
ABSTRACT
Objective
To explore the efficacy and safety of binaural beats (BB) for stress management in non-clinical contexts.
Method
Embase, Medline, PsycINFO, CINAHL, Web of Science and Cochrane databases were searched for RCTs that administered BB and reported ≥1 stress-related outcome in subjects with pre-existing stress, or in participants with laboratory-induced stress (PROSPERO registration: CRD42023428623). The risk of bias was assessed using the JBI critical appraisal tool and a purpose-designed tool to explore stress-specific methodological quality. Effects between groups were synthesised thematically, exploring physiological and psychological outcomes, duration of exposure and frequency (Hz).
Results
Twelve studies were included for review. Half of the studies used a single-session BB intervention and half used longer-term home-based protocols. Seven involved participants with pre-existing stress and five exposed healthy subjects to stressors. Eight studies reported ≥1 significant effect favouring intervention over control while four found no group effects. However, methodological heterogeneity, unclear randomisation and blinding procedures, and lack of oversight of stress mediators and moderators were found.
Discussion
BBs have promise as a self-care stress-management tool. However, evidence is not strongly in favour of widespread recommendation, there is little known about adverse effects, and there is not yet a clear optimal protocol (frequency and schedule) for stress-buffering effects.
Introduction
Stress is a subjective term used to describe both situations and feelings, with definitions varying by research discipline (Epel et al., Citation2018). In psychology, it is traditionally defined as when the perceived demands of an environment exceed an individual’s ability to meet or control them (Lazarus et al., Citation1985). These demands or stressors, real or imagined, can induce adaptive physiological change in the body (Selye, Citation2013). Briefly, in the short-term, there is mobilisation of sympathetic, parasympathetic, and neuromuscular nervous systems. This is followed by activation of the neuroendocrine axis, commonly known as the ‘fight-or-flight’ response (Everly & Lating, Citation2019), with associated feelings of tension or worry often referred to as anxiety (APA, Citation2023). Stress is often used interchangeably with the term ‘anxiety’, which also has multiple meanings. ‘State anxiety’ best describes feelings triggered by a stressor, while ‘trait anxiety’ may represent one’s tendency to experience these feelings even in the absence of a stressor (Gidron, Citation2013). Furthermore, anxiety is also used as an umbrella term for a number of diagnoses such as generalised anxiety disorder and panic disorder (Mind, Citation2021).
Excessive stress and anxiety – in intensity and chronicity – can have long-acting impacts on the body with resulting physiological changes leaving some individuals at higher risk of physical and mental illness (Everly & Lating, Citation2019; Miller et al., Citation2011). Globally, some of the most prevalent morbidities such as cardiovascular disease, type 2 diabetes mellitus, and depression are associated with unmanaged stress and anxiety (Cohen et al., Citation2007; Ingrosso et al., Citation2023; Stojanovich & Marisavljevich, Citation2008). This is a growing problem with levels of mental health disorders – such as anxiety – rising 13% in the decade up to 2017 (WHO, Citation2023), with reports of significant further increases following the covid-19 pandemic (Salari et al., Citation2020). However, managing stress and maintaining mental wellbeing can buffer against these effects (Pressman & Cohen, Citation2005).
Currently, stress-management approaches involve pharmacological, psychological and lifestyle interventions. Approaches may vary depending on whether there is any clinical diagnosis, cause, and severity of stress. Drug treatments (i.e. benzodiazepines) have utility but come with the risk of adverse effects, rendering them less acceptable for long-term use (Bandelow, Citation2020). Psychological therapies (i.e. cognitive behavioural therapy) may be appropriate in some contexts, but the effectiveness depends on patient receptibility, while therapist access and costs can be barriers (Olthuis et al., Citation2016; Ruotsalainen et al., Citation2015). General lifestyle and self-care advice aim to equip the wider population with proactive self-stress-management tools such as exercise, social support and mindfulness (Cohen, Citation2004; Gordon et al., Citation2017; Gu et al., Citation2015). However, reduced capacity for self-care in the highly stressed, alongside skills and lifestyles can impede one’s ability to apply such strategies effectively (Luis et al., Citation2021). Expanding the stress self-care toolkit to include accessible, low-harm methods may allow more users to find an approach that suits their circumstances and needs.
Binaural beats (BB) are two tones presented at slightly different frequencies to both ears from which the brain perceives a third tone equal to the frequency difference of the two tones, inducing a phenomenon known as brainwave entrainment (Ross et al., Citation2014). Brainwave entrainment has been observed using electroencephalogram (EEG) (Schwarz & Taylor, Citation2005) with five frequency bands associated with different arousal states: delta (0.5–4 Hz), theta (4–7 Hz), alpha (7–13 Hz), beta (13–30 Hz) and gamma (30–50 Hz), with lower frequencies linked to lower arousal and greater relaxation, and the opposite for higher frequencies (Jirakittayakorn & Wongsawat, Citation2018). Since Oster (Citation1973) first described BB’s potential clinical value, reviews of studies using BB as a therapeutic intervention for health and wellbeing have found evidence supporting its efficacy as an intervention for pain, cognition and anxiety (Basu & Banerjee, Citation2020; Chaieb et al., Citation2015; Garcia-Argibay et al., Citation2019; Maddison et al., Citation2022). Furthermore, several clinical trials have reported reductions in peri-operative anxiety associated with BB exposure (Isik et al., Citation2017; Loong et al., Citation2022; Parodi et al., Citation2021). However, most stressors exist outside of clinical settings such as at work or in the home (Harvey et al., Citation2017; Marsh et al., Citation2020), and the efficacy for the use of BB in these contexts is unknown despite there already being a population already self-prescribing them for relaxation (Barratt et al., Citation2022).
BB have potential as an accessible, low-harm, non-pharmacological approach to stress management in the general population. However, there are currently no systematic reviews that collate the findings on this subject. The following systematic review aims to address this gap by describing and critiquing evidence from randomised control trials (RCTs) with a focus on BB effects on both short-term stress reactivity and chronic stress in non-clinical contexts. In response to concerns surrounding the quality, appropriateness and consistency of stress research methodology (Crosswell & Lockwood, Citation2020; Epel et al., Citation2018), the review will also explore the use of stress-related methodologies with a discussion of implications.
Materials and methods
The protocol for this review was registered with PROSPERO (CRD42023428623). Reporting was conducted in adherence to the Preferred Reporting Items for Systematic Reviews (PRISMA) statement (Appendix 1) (Page et al., Citation2021) using EndNote (The EndNote Team, Citation2013) and Covidence (Covidence, Citation2023) platforms.
Search strategy
A search of Medline, Embase, PsycINFO, Cochrane, Web of Science and CINAHL for all peer-reviewed articles available in the English language and published from the inception of the database up until the search date was conducted on 6 June 2023. Additionally, reference lists of retrieved articles were manually searched for further studies.
The search strategy consisted of two elements: the intervention (BB) AND outcome (stress), utilising a range of specific and related terms to capture the anticipated disparate methodologies and language ().
Table 1. Example search strategy (Embase). Full strategy can be found in Appendix 2.
Retrieved articles were imported into EndNote and duplicates were removed digitally. The remaining articles were then uploaded to Covidence online software for title and abstract and full text screening, data extraction and quality assessment.
Inclusion and exclusion criteria
Two reviewers independently screened all titles and abstracts, and full texts, with any conflicts resolved through discussion. Inclusion and exclusion criteria were altered from those outlined in the study protocol (Platt & Hammond, Citation2023). During the screening phase, it was apparent that the included studies were too heterogenous to meaningfully review. Therefore, a decision was taken to further limit the review to RCTs and to remove EEG measurement as an outcome to focus on physically and psychologically felt stress and anxiety (see for the eligibility criteria).
Table 2. Article inclusion and exclusion criteria. Italics denote criteria that were changed from the protocol.
Data extraction
One author completed data extraction with a second author independently checking the results. The following information and data were extracted from included studies into a pre-set template: author and year, journal name, study location, trial design (randomised control or randomised crossover trial), participant characteristics (sample size, age, sex, ethnicity, comorbidities and group characteristic), intervention details (setting, stressor type/description, BB source (i.e. commercially available or purpose-created), frequency, duration, schedule and delivery method), control conditions, outcome type, measurement, results, any reported side effects and intervention completion rate.
Quality appraisal for risk of bias
One author conducted a quality appraisal of all included articles while a second author independently checked the results. The JBI (Citation2020) ‘Checklist for randomized control trials’ was used for this process. This tool comprises 13 methodology-based questions regarding topics such as randomisation, blinding and outcome measurement with results used to inform evidence synthesis and interpretation. No studies were excluded on a quality basis.
A second quality appraisal approach was employed by one author to explore further methodological questions for stress-related studies. No published quality appraisal tool for this was found. Therefore, a new form was devised to question whether authors have clearly described replicable methods and if these methods account for the intricacies of stress definition, induction and measurement raised by Epel et al. (Citation2018) and Crosswell and Lockwood (Citation2020). Results were summarised descriptively, and quality implications were discussed. However, it should be noted that this was exploratory and not an exhaustive or validated measure of quality.
Data synthesis
Results were assessed for meta-analysis suitability and due to methodological heterogeneity deemed unsuitable. Therefore, extracted data were synthesised narratively overall and using the following thematic groups: physiological and psychological outcomes (tabulated), duration of exposure, and BB frequency (Hz) in line with questions of optimal timing, duration and frequency raised by Maddison et al. (Citation2022) and Garcia-Argibay et al. (Citation2019). Effects were presented as significant or non-significant mean differences between groups.
Results
Study characteristics
From a total of 1131 retrieved articles, 12 met the inclusion criteria, of which seven were RCTs and five were randomised crossover trials (RXT) (see PRISMA flow chart in and study characteristics in ). The evidence had a wide geographic scope, however, with one exception (Thanyawinichkul et al., Citation2022), and all studies were conducted in high-income countries such as the USA, UAE, and South Korea. Seven studies focused on people with a pre-existing stressor such as chronic pain, and five induced a stressor such as the ‘Trier Social Stress Test’ on healthy subjects. Healthy participants were often recruited from universities (Al-Shargie et al., Citation2021; Hautus et al., Citation2021; Katmah et al., Citation2023; Kelton et al., Citation2021), while studies on pre-existing stress had more varied groups such as clinical outpatients (Gkolias et al., Citation2020; Thanyawinichkul et al., Citation2022), military (Gantt et al., Citation2017) and again, students (Shalforoushan et al., Citation2021).
Figure 1. PRISMA flow chart detailing the screening process.
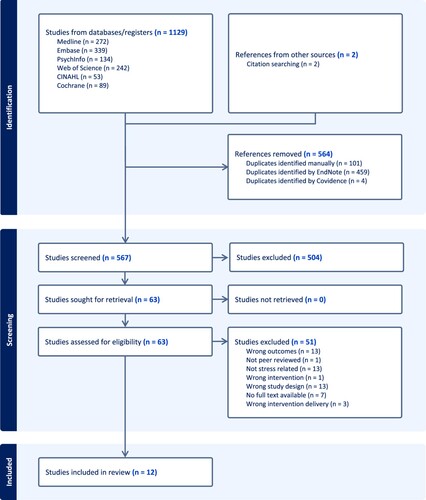
Table 3. Study characteristics.
Six studies involved a longer-term home-based BB protocol, six used a single BB session (four laboratory-based and two online) and one study included both approaches (). Generally, single sessions induced a stressor, while longer protocols did not. Two exceptions were the study by Mallik and Russo (Citation2022), which exposed a single BB session to participants with pre-existing anxiety, and the study by Gantt et al. (Citation2017), which tested the effectiveness of a home-based protocol with a laboratory-induced stressor.
Most studies investigated a single BB frequency – most commonly theta – with a music-only condition as the most used control (). Eight studies used sound-embedded BB (i.e. with music), two studied pure-tone BB, while two did not clarify the content of the BB stimuli. Similarly, sources of BB varied with five assessing a commercially available BB (i.e. Monroe Institute file), and six using purpose-created BB for the study. One study failed to describe the BB stimuli source. In the studies testing commercially available BB stimuli, all provided source references indicating some reproducibility. However, it was unclear whether they were verified as true BB. In the studies that used purpose-created BB, sound characteristics and generation procedures were described with varying detail. For example, Katmah et al. (Citation2023) described the BB frequency only, while Al-Shargie et al. (Citation2021) detailed frequency (for each ear and the BB), sampling rate and sound pressure level. Furthermore, there was no clear reporting of any pilot or third-party testing of purpose-created BB stimuli.
Quality of studies
Overall, studies were of mixed quality (see ) with numbers of criteria met ranging from 2 to 12/13. Note for RXTs and one-session experiments, not all criteria were applicable. The main limitations of the included studies were unclear group allocation and blinding procedures. For example, five studies clearly used true randomisation methods, and only one study evidently blinded their outcome assessors. Oppositely, most studies maintained equal treatment between groups or conditions, and with three exceptions, were judged to have used appropriate methods.
Table 4. Quality appraisal results (reproduced from JBI, Citation2020).
In the stress-specific quality appraisal, studies were also judged to be of mixed quality (see ). In the six stress induction studies, the numbers of criteria met ranged from 3 to 9/11. Only two studies met all ‘stressor’ criteria including justification of stressor selection. In the seven pre-existing stress studies, the numbers of criteria met ranged from 2 to 8/9. Of these, four were judged to adequately describe the stressor (i.e. for comparability and replicability). For all studies, the main area of concern was the lack of consideration of potential stress mediators and moderators in their designs.
Table 5. Results of a purpose-designed tool to explore methodological quality in the context of stress research. Adapted from comments made by Crosswell and Lockwood (Citation2020) and Epel et al. (Citation2018).
Summaries of effects
Outcomes of BB intervention on 15 unique stress-related outcomes are reported in (physiological) and (psychological). Overall, eight studies reported at least one significant effect in favour of BB intervention, and four reported no significant differences between groups. One study assessed both pure-tone and music-combined theta BB finding significant effects in favour of combined but reported pure-tone BB as the least effective condition for short-term anxiety reduction (Mallik & Russo, Citation2022). Note for this synthesis, the combined condition in this study is counted as having an effect in favour of BB.
Table 6. Effects of physiological outcomes.
Table 7. Effects of psychological outcomes.
Physiological and psychological outcomes
Two RCTs examined the effect of theta BB on heart rate variability (HRV) both finding significantly higher high-frequency HRV during stress tasks in intervention conditions than controls (pink noise and music) indicating higher parasympathetic activity (Gantt et al., Citation2017; Kelton et al., Citation2021). Two RXTs reported salivary hormone levels (cortisol and alpha-amylase) to significantly reduce with beta BB exposure during a stressful task (Al-Shargie et al., Citation2021; Katmah et al., Citation2023). However, there is limited confidence in both studies due to the high risk of carryover effects and lack of blinding. One RXT measured skin conductance and found a reduction in subjects exposed to 4 minutes of delta and beta BB during stressor recovery, when compared with silent control (Hautus et al., Citation2021). No significant effects between groups were reported in any of the remaining autonomic indicators: pulse rate, respiration rate and depth, and blood pressure (Gkolias et al., Citation2020; Hautus et al., Citation2021).
Psychological outcomes were all measured using self-report methods. Five studies assessed anxiety using measures including State-Trait Anxiety Inventory (STAI) (Bang et al., Citation2019; Gkolias et al., Citation2020; Lee et al., Citation2022), State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA) (Mallik & Russo, Citation2022) and Hospital Anxiety and Depression Scale-Anxiety (HADS-A) (Thanyawinichkul et al., Citation2022) questionnaires reporting mixed results. For example, Gkolias et al. (Citation2020) reported a significant reduction in STAI scores in chronic pain outpatients following a 1-week on-demand theta BB protocol but not in the sham control group. However, Thanyawinichkul et al. (Citation2022) used the Thai-HADS-A also in subjects with chronic pain finding no significant effects. Alternatively, one study measured pre-sleep rumination (Rumination Response Scale) as a proxy for anxiety in students with poor sleep quality (Shalforoushan et al., Citation2021) and reported significant reductions and group effects with pre-bedtime alpha BB exposure.
Perceived stress was also evaluated in several ways. Two studies used the Perceived Stress Scale (PSS) and both reported scores to reduce pre–post-intervention (Lee et al., Citation2022; Shalforoushan et al., Citation2021). This effect was significant when compared to a waiting-list control by Shalforoushan et al. (Citation2021) but similarly effective when compared to an ASMR control by Lee et al. (Citation2022). Studies using the Visual Analogue Scale (VAS) and a mental states questionnaire reported no significant effects (Kelton et al., Citation2021; Leistiko et al., Citation2023). Finally, Gantt et al. (Citation2017) used an unvalidated questionnaire that asked participants to reflect on the previous day’s stress observing consistently lower stress reporting in the intervention group.
Effects by duration of exposure
In the studies examining the effects of single-session BB interventions, total durations ranged from 5 minutes (10 × 30 seconds) to 24 minutes (continuous) and were mostly around 20 minutes. Of these studies, all except Leistiko et al. (Citation2023), who presented gamma BB during an attention task, found significant reductions in stress/anxiety. Comparing two studies with similar designs, Al-Shargie et al. (Citation2021) presented a total of 5-minute beta BB, and Katmah et al. (Citation2023), 20 minutes. While both achieved significant reductions in salivary stress hormones, the 20-minute protocol yielded more significant results (p < 0.05 vs p < 0.0001 & p < 0.01).
Longer protocols ranged from 1 week (on-demand) to 30 days (1 × 30 minutes every day). No dose–response effect was apparent with significant effects found in both the shortest (1 week) and longest (30 days) interventions. Demographic differences limit comparability between single-session and longer protocols. However, Gkolias et al. (Citation2020) studied both a theta BB brief 30-minute and 1-week application in an RXT design. Both groups had reduced anxiety (STAI) following the brief application, but after a week, only the intervention significantly reduced anxiety levels.
Effects by BB frequency (Hz)
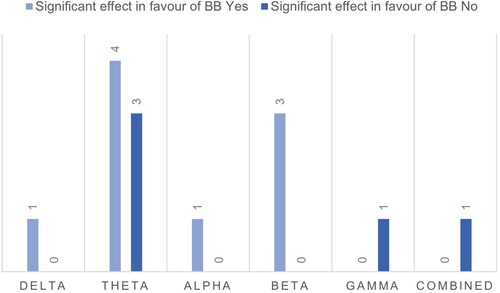
The distribution of studies for each BB frequency is shown in . There were insufficient numbers of studies across frequency bands with only single papers for delta, alpha, gamma and combined (alpha-theta) protocols. Thus, it was not possible to make any conclusions on effectiveness by frequency. Furthermore, of seven studies examining a theta protocol, four reported results in favour of BB intervention while similarly, three reported no significant effects, which is again inconclusive. One study compared multiple BB frequencies (delta, theta, alpha and beta) and silence for short-term stressor recovery (Hautus et al., Citation2021) finding only delta (lowest Hz) and beta (highest Hz) BBs to significantly reduce skin conductance compared to silence. However, no patterns in frequency effectiveness were apparent.
Figure 2. Distribution of studies per BB frequency band (Hz) with numbers reporting and not reporting one or more significant effects favouring BB intervention.
Adverse effects and acceptability
Ten studies did not explicitly report any adverse effects associated with the intervention ( and ). One study stated that there were no adverse events (Bang et al., Citation2019) and one reported mild headache, which improved without treatment (Lee et al., Citation2022). However, this also occurred in the control condition, so it was not attributed to BB specifically. Additionally, all studies reported that above 90% completion rate inferring BB intervention was acceptable for involved populations.
Discussion
Excessive stress is a recognised threat to health and wellbeing (Everly & Lating, Citation2019; Selye, Citation2013). In contrast, subjective wellbeing has been associated with longevity and health (Diener & Chan, Citation2011), and studies have shown potential for physiological improvement from stress-management interventions such as meditation (Carlson et al., Citation2004; Jacobs et al., Citation2011). BB is now a widely available technology for which existing evidence also suggests potential for wellbeing (Basu & Banerjee, Citation2020). Yet, this review is the first to explore the efficacy of BB as a self-care stress-management tool.
Non-clinical use of BB appears to be safe and acceptable with no harms attributed to exposure and high (>90%) intervention completion rates. However, reporting of adverse effects was largely overlooked, as it was in other reviews on BB interventions (Basu & Banerjee, Citation2022; Garcia-Argibay et al., Citation2019; Maddison et al., Citation2022) perhaps indicating an assumption of safety. Given that concerns have been raised elsewhere for potential adverse effects on hearing (Musiek et al., Citation2012) and mental health (Wahbeh et al., Citation2007a; Wahbeh et al., Citation2007b), readers should be cognisant of this lack of reporting.
Overall, the evidence for efficacy was equivocal with a third of studies not finding BB to be associated with any significant reductions in stress or anxiety and inconsistent results within some studies. For example, Hautus et al. (Citation2021) reported reductions in skin conductance associated with 2 and 24 Hz BB but no other physiological measures or BB frequencies. Methodological heterogeneity contributed to difficulties in making conclusions with 15 unique outcomes used, inconsistent application of BB stimuli and intervention schedules, and varied methodological quality. Moreover, it was generally unclear whether the BB stimuli were verified as true BB with no clear reporting of any pilot or third-party testing procedures. Nonetheless, there were some interesting findings as discussed below.
BB and the stress-response
All five studies that measured physiological responses to stressors found a significant effect between BB and non-BB groups, indicating that BB can have acute effects on the stress response. The strongest evidence comes from two studies that found significantly higher HRV with theta BB exposure (Gantt et al., Citation2017; Kelton et al., Citation2021). Higher HRV represents a balanced autonomic nervous system able to respond to stressors, while lower HRV indicates that the body is working to adapt to or recover from a stressor, and it has clinical relevance as a predictor of illness such as cardiac mortality (Kim et al., Citation2018; Sztajzel, Citation2004). Apart from some questions surrounding blinding procedures by Kelton et al. (Citation2021), these studies were judged as having a lower risk of bias and their findings are consistent with evidence from relaxation studies exposing healthy subjects also to theta BB (Bakaeva et al., Citation2022; Chockboondee et al., Citation2023).
Significant effects on salivary stress-indicators (alpha-amylase and cortisol) were found by two similarly designed studies that mitigated against induced stress with beta BB (Al-Shargie et al., Citation2021; Katmah et al., Citation2023). Alpha-amylase is a recognised surrogate marker of sympathetic nervous system activation (Petrakova et al., Citation2015), while cortisol is released, circulates in response to stressors, and is a well-used measure of stress reactivity (Everly & Lating, Citation2019). These effects were interesting as beta BB is usually associated with enhanced arousal and cognition rather than relaxation (Garcia-Argibay et al., Citation2019). One possible explanation is that the perception of good or bad performance may influence stress-reactivity in a similar way to active and passive coping (Everly & Lating, Citation2019). However, the above should be interpreted with caution due to the high risk of bias in both studies.
Apart from some findings for skin conductance (Hautus et al., Citation2021), BB had no effects on the remaining physiological outcomes in the included studies. However, effects have been seen in clinical contexts with several studies reporting reductions in blood pressure and pulse rate in patients exposed to BB peri-operatively (i.e. cataract surgery) (Loong et al., Citation2022; Opartpunyasarn et al., Citation2022; Wiwatwongwana et al., Citation2016). This contrast in findings may reflect contextual differences. For example, experiments conducted in clinical settings where that type of data collection is routine and environments are naturalistic have higher ecological validity (Andrade, Citation2018). For example, an unfamiliar laboratory environment could interfere with stress responses and participants’ abilities to relax as they might at home. In contrast, laboratory studies may have more relevance for less routine situations such as public speaking and job interviews.
BB for chronic stress management
While the above results indicate the potential effectiveness of BB on stress, to address the question of its efficacy as a personal stress-management tool, it is useful to look to longer duration, home-based interventions for more ecologically valid studies that explore if effects persist beyond initial exposure.
One week of BB exposure was sufficient to observe significant differences in STAI scores in chronic pain outpatients (Gkolias et al., Citation2020) while a daily intervention of 30 days also significantly reduced perceived stress and rumination in students with poor sleep quality (Shalforoushan et al., Citation2021). However, interventions of 2 weeks reported no significant group effects (Bang et al., Citation2019; Thanyawinichkul et al., Citation2022). Similar inconsistencies exist throughout the literature with significant reductions in trait anxiety recorded during a pilot trial of a 60-day delta BB intervention (Wahbeh et al., Citation2007) and only slight, non-significant effects found in a 4-week study (Le Scouarnec et al., Citation2001). Thus, it is unclear what duration of exposure one should aim towards for meaningful outcome assessment.
The limited available evidence for exposure schedule suggests daily listening may not be necessary, but exposures should be within 1-week of each other to maintain stress-buffering effects. A washout period analysis by Gkolias et al. (Citation2020) indicated effects from a 1-week intervention did not persist for more than 1-week afterwards. Gantt et al. (Citation2017) observed significant differences in HRV up to 1-week post-intervention where the protocol did not involve daily exposure (>3 times/week). Longer post-intervention follow-ups could explore this further.
Stress-methodology implications
The issues highlighted in the stress-specific methodology were consistent with those raised in the wider stress literature and limit the trustworthiness of some of the reviewed studies (Crosswell & Lockwood, Citation2020; Epel et al., Citation2018). Changes in physiological stress-markers have been observed alongside variables including sleep quality, caffeine consumption and life events such as bereavement (Al-Amin et al., Citation2016; Fagundes et al., Citation2018; van Dalfsen & Markus, Citation2018). Yet, not accounting for these was the largest concern drawn from the stress-method exploration. Controlling for these, either by exclusion, or recording and reporting as characteristics would strengthen findings in future BB stress research.
Further to the above, outcome selection (particularly of self-report methods) in stress measurement requires careful consideration of population characteristics and circumstances, and the mechanisms of stress in those contexts (Crosswell & Lockwood, Citation2020). For example, overwhelm may be relevant to student stress during exam periods.
Similarly, cultural norms in definitions and expressions of mental health in China lean towards the use of somatic measures whereby headache may be a better stress indicator (Ryder & Chentsova-Dutton, Citation2012). This is a consideration for global studies such as that by Leistiko et al. (Citation2023). However, the comparability of variable outcomes is limited as relationships between measures are weak (Epel et al., Citation2018). Thus, context-specific measures limit comparability between populations.
Strengths and limitations
This review was rigorously conducted, harnessing the strengths of a double-reviewer process and the thoroughness of a sensitive search strategy. However, there were some limitations. Primarily, it was difficult to define stress due to there being many related constructs (i.e. relaxation) and closely linked topics such as sleep quality (van Dalfsen & Markus, Citation2018). Papers on closely linked topics were included as stress management was considered pertinent in these contexts. However, this contributed to methodological heterogeneity, and it was difficult to disentangle the effects of stress from these other factors. Secondly, in the absence of an existing tool, the review used an unvalidated measure of stress-specific methodological quality. While this provided awareness of challenges in stress research, its findings should be interpreted within context. Finally, the review was altered from protocol to limit to RCTs. Excluding quasi-experimental studies potentially misses findings, which may have provided desired evidence on efficacy, frequency and dose–response effects of BB. However, it would have been challenging to meaningfully review that scope of evidence with the resources available.
Several limitations of the included studies may impact the interpretation of this review’s conclusions. Firstly, reporting of randomisation and blinding procedures was generally unclear. Thus, the risk of exaggerated effect reporting was unclear (Forbes, Citation2013). Secondly, all studies except one had modest sample sizes (<100). High variability in stress responses due to factors including personality and childhood experiences (Bibbey et al., Citation2013; Brindle et al., Citation2022) may be problematic for clinical studies with small samples. Finally, there was a methodological and demographic divide in studies. Healthy subjects were only exposed to single sessions while subjects with a pre-existing stressor tended to partake in home-based protocols with no physiological outcome measurement. This meant it was not meaningful to compare effectiveness between healthy and ‘stress’ subjects. Moreover, healthy subjects tended to be younger. Some evidence suggests BB elicits a greater response in younger people (Grose & Mamo, Citation2012). Therefore, results cannot be generalised to older populations.
Recommendations for future research
The findings of this review could be quantified with meta-analyses with a narrower methodological focus (for example, laboratory assessments of BB on physiological stress outcomes). Future primary research should address the limited knowledge of adverse effects with a systematic approach to identification, analysis and reporting of harms associated with BB exposure, such as that outlined in ‘CONSORT Harms 2022’ (Junqueira et al., Citation2023). Research should also aim to define and verify BB stimuli (i.e. embedded vs pure-tone, frequency (Hz), and intervention schedule) to work towards standardised methodologies with empirically validated stimuli. Recruitment of larger and more diverse samples could offer better generalisability and account for large variability in stress responses. This would also allow for more subgroup analyses of different characteristics (i.e. trait anxiety) and enable testing of multiple BB stimuli and intervention schedules, to disentangle methodological and demographic variables from effects. These samples could be achieved with the use of online applications. Two studies provided proof of this concept successfully by adapting to remote/online evaluations following COVID restrictions (Leistiko et al., Citation2023; Mallik & Russo, Citation2022). Additionally, the use of wearable technologies could enhance remote studies with the inclusion of objective physiological outcomes such as HRV (Hinde et al., Citation2021). Finally, as part of this review, we developed a stress-specific quality assessment tool. However, the development of a validated tool could address many of the concerns raised here, and in the wider stress literature. This could provide guidance around procedures, outcomes and stressor selection to minimise the impact of external factors such as acute stressful events.
Implications for practice
Globally, there is a growing burden of stress and stress-related disease, despite awareness and existing stress-management strategies. BB may have some stress-buffering effects, but there is currently no evidence for adverse effects, and they are widely accessible on mainstream media platforms. However, this review did not find strong evidence for their efficacy in non-clinical contexts, and it is unclear what protocol may be optimal to see benefits. On this evidence, they are not yet recommended for widespread use for stress management but may have use complementary to more evidence-based approaches.
Conclusion
Unmanaged stress is a growing problem with significant public health implications; however, some evidence indicates that BB has a stress-buffering effect. This review explored the effects of BB interventions on non-clinical stress to ascertain their efficacy as a self-care stress-management strategy. Twelve included studies provided equivocal results with promising findings weakened by unclear randomisation and blinding procedures and oversight of the intricacies of stress measurement. Furthermore, methodological heterogeneity led to difficulties in making conclusions. Online and wearable technologies may allow future research to access larger, more diverse samples to address questions surrounding optimal frequencies and schedules and generate more robust results.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Al-Amin, M., Kawasaki, I., Gong, J., & Shim, Y. H. (2016). Caffeine induces the stress response and up-regulates heat shock proteins in Caenorhabditis elegans. Molecules and Cells, 39(2), 163–168. https://doi.org/10.14348/molcells.2016.2298
- Al-Shargie, F., Katmah, R., Tariq, U., Babiloni, F., Al-Mughairbi, F., Al-Nashash, H. & IEEE (2021). Stress assessment and mitigation using fNIRS and binaural beat stimulation.
- Andrade, C. (2018). Internal, external, and ecological validity in research design, conduct, and evaluation. Indian Journal of Psychological Medicine, 40(5), 498–499. https://doi.org/10.4103/IJPSYM.IJPSYM_334_18
- APA. (2023). APA dictionary of psychology. Retrieved March 7, 2023, from https://dictionary.apa.org/anxiety
- Bakaeva, Z. V., Shumov, D. E., Yakunina, E. B., Starshinov, Y. P., Sveshnikov, D. S., Torshin, V. I., Dorokhov, V. B., & Karpov, V. I. (2022). The influence of music with the binaural beat effect on heart rate during daytime sleep in humans. Neuroscience and Behavioral Physiology, 52(2), 218–222. https://doi.org/10.1007/s11055-022-01227-1
- Bandelow, B. (2020). Current and novel psychopharmacological drugs for anxiety disorders. In Y.-K. Kim (Ed.), Anxiety disorders: Rethinking and understanding recent discoveries (pp. 347–365). Springer Singapore.
- Bang, Y. R., Choi, H., & Yoon, I. Y. (2019). Minimal effects of binaural auditory beats for subclinical insomnia a randomized double-blind controlled study. Journal of Clinical Psychopharmacology, 39(5), 499–503. https://doi.org/10.1097/JCP.0000000000001097
- Barratt, M. J., Maddox, A., Smith, N., Davis, J. L., Goold, L., Winstock, A. R., & Ferris, J. A. (2022). Who uses digital drugs? An international survey of ‘binaural beat’ consumers. Drug and Alcohol Review, 41(5), 1126–1130. https://doi.org/10.1111/dar.13464
- Basu, S., & Banerjee, B. (2020). Prospect of brainwave entrainment to promote well-being in individuals: A brief review. Psychological Studies, 65(3), 296–306. https://doi.org/10.1007/s12646-020-00555-x
- Basu, S., & Banerjee, B. (2022). Potential of binaural beats intervention for improving memory and attention: Insights from meta-analysis and systematic review. Psychological Research, 87(4), 951–963. https://doi.org/10.1007/s00426-022-01706-7
- Bibbey, A., Carroll, D., Roseboom, T. J., Phillips, A. C., & de Rooij, S. R. (2013). Personality and physiological reactions to acute psychological stress. International Journal of Psychophysiology, 90(1), 28–36. https://doi.org/10.1016/j.ijpsycho.2012.10.018
- Brindle, R. C., Pearson, A., & Ginty, A. T. (2022). Adverse childhood experiences (ACEs) relate to blunted cardiovascular and cortisol reactivity to acute laboratory stress: A systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews, 134, 104530. https://doi.org/10.1016/j.neubiorev.2022.104530
- Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2004). Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress and levels of cortisol, dehydroepiandrosterone sulfate (DHEAS) and melatonin in breast and prostate cancer outpatients. Psychoneuroendocrinology, 29(4), 448–474. https://doi.org/10.1016/S0306-4530(03)00054-4
- Chaieb, L., Wilpert, E. C., Reber, T. P., & Fell, J. (2015). Auditory beat stimulation and its effects on cognition and mood states. Frontiers in Psychiatry, 6, 70. https://doi.org/10.3389/fpsyt.2015.00070
- Chockboondee, M., Jatupornpoonsub, T., Lertsukprasert, K., & Wongsawat, Y. (2023). Long and short durations of binaural beats differently affect relaxation: A study of HRV and BRUMS. IEEE Access, 11, 84842–84851. https://doi.org/10.1109/ACCESS.2023.3303183
- Cohen, S. (2004). Social relationships and health. American Psychologist, 59(8), 676–684. https://doi.org/10.1037/0003-066X.59.8.676
- Cohen, S., Janicki-Deverts, D., & Miller, G. E. (2007). Psychological stress and disease. JAMA, 298(14), 1685–1687. https://doi.org/10.1001/jama.298.14.1685
- Covidence. (2023). Covidence systematic review software.
- Crosswell, A. D., & Lockwood, K. G. (2020). Best practices for stress measurement: How to measure psychological stress in health research. Health Psychology Open, 7(2), 205510292093307. https://doi.org/10.1177/2055102920933072
- Diener, E., & Chan, M. Y. (2011). Happy people live longer: Subjective well-being contributes to health and longevity. Applied Psychology: Health and Well-Being, 3(1), 1–43. https://doi.org/10.1111/j.1758-0854.2010.01045.x
- The EndNote Team. (2013). EndNote.
- Epel, E. S., Crosswell, A. D., Mayer, S. E., Prather, A. A., Slavich, G. M., Puterman, E., & Mendes, W. B. (2018). More than a feeling: A unified view of stress measurement for population science. Frontiers in Neuroendocrinology, 49, 146–169. https://doi.org/10.1016/j.yfrne.2018.03.001
- Everly, G. S., & Lating, J. M. (2019). The anatomy and physiology of the human stress response. In J. G. S. Everly & J. M. Lating (Eds.), A clinical guide to the treatment of the human stress response (pp. 19–56). Springer New York.
- Fagundes, C. P., Murdock, K. W., LeRoy, A., Baameur, F., Thayer, J. F., & Heijnen, C. (2018). Spousal bereavement is associated with more pronounced ex vivo cytokine production and lower heart rate variability: Mechanisms underlying cardiovascular risk? Psychoneuroendocrinology, 93, 65–71. https://doi.org/10.1016/j.psyneuen.2018.04.010
- Forbes, D. (2013). Blinding: An essential component in decreasing risk of bias in experimental designs. Evidence Based Nursing, 16(3), 70. https://doi.org/10.1136/eb-2013-101382
- Gantt, M. A., Dadds, S., Burns, D. S., Glaser, D., & Moore, A. D. (2017). The effect of binaural beat technology on the cardiovascular stress response in military service members With postdeployment stress. Journal of Nursing Scholarship, 49(4), 411–420. https://doi.org/10.1111/jnu.12304
- Garcia-Argibay, M., Santed, M. A., & Reales, J. M. (2019). Efficacy of binaural auditory beats in cognition, anxiety, and pain perception: A meta-analysis. Psychological Research, 83(2), 357–372. https://doi.org/10.1007/s00426-018-1066-8
- Gidron, Y. (2013). Trait anxiety. In M. D. Gellman & J. R. Turner (Eds.), Encyclopedia of behavioral medicine (pp. 1989–1989). Springer New York.
- Gkolias, V., Amaniti, A., Triantafyllou, A., Papakonstantinou, P., Kartsidis, P., Paraskevopoulos, E., Bamidis, P. D., Hadjileontiadis, L., & Kouvelas, D. (2020). Reduced pain and analgesic use after acoustic binaural beats therapy in chronic pain - A double-blind randomized control cross-over trial. European Journal of Pain, 24(9), 1716–1729. https://doi.org/10.1002/ejp.1615
- Gordon, B. R., McDowell, C. P., Lyons, M., & Herring, M. P. (2017). The effects of resistance exercise training on anxiety: A meta-analysis and meta-regression analysis of randomized controlled trials. Sports Medicine, 47(12), 2521–2532. https://doi.org/10.1007/s40279-017-0769-0
- Grose, J. H., & Mamo, S. K. (2012). Electrophysiological measurement of binaural beats: Effects of primary tone frequency and observer age. Ear and Hearing, 33(2), 187–194. https://doi.org/10.1097/AUD.0b013e318230bbbd
- Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindfulness-based cognitive therapy and mindfulness-based stress reduction improve mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12. https://doi.org/10.1016/j.cpr.2015.01.006
- Harvey, S. B., Modini, M., Joyce, S., Milligan-Saville, J. S., Tan, L., Mykletun, A., Bryant, R. A., Christensen, H., & Mitchell, P. B. (2017). Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occupational and Environmental Medicine, 74(4), 301. https://doi.org/10.1136/oemed-2016-104015
- Hautus, M. J., Shepherd, D., Giang, E., & Landon, J. (2021). Can binaural beats facilitate autonomic recovery following exposure to an acute stressor? Complementary Therapies in Clinical Practice, 45, 101485. https://doi.org/10.1016/j.ctcp.2021.101485
- Hinde, K., White, G., & Armstrong, N. (2021). Wearable devices suitable for monitoring twenty four hour heart rate variability in military populations. Sensors, 21(4), 1061. https://doi.org/10.3390/s21041061
- Ingrosso, D. M. F., Primavera, M., Samvelyan, S., Tagi, V. M., & Chiarelli, F. (2023). Stress and diabetes mellitus: Pathogenetic mechanisms and clinical outcome. Hormone Research in Paediatrics, 96(1), 34–43. https://doi.org/10.1159/000522431
- Isik, B. K., Esen, A., Buyukerkmen, B., Kilinc, A., & Menziletoglu, D. (2017). Effectiveness of binaural beats in reducing preoperative dental anxiety. British Journal of Oral and Maxillofacial Surgery, 55(6), 571–574. https://doi.org/10.1016/j.bjoms.2017.02.014
- Jacobs, T. L., Epel, E. S., Lin, J., Blackburn, E. H., Wolkowitz, O. M., Bridwell, D. A., Zanesco, A. P., Aichele, S. R., Sahdra, B. K., MacLean, K. A., King, B. G., Shaver, P. R., Rosenberg, E. L., Ferrer, E., Wallace, B. A., & Saron, C. D. (2011). Intensive meditation training, immune cell telomerase activity, and psychological mediators. Psychoneuroendocrinology, 36(5), 664–681. https://doi.org/10.1016/j.psyneuen.2010.09.010
- JBI. (2020). Critical appraisal tools. Retrieved March 6, 2023, from https://jbi.global/critical-appraisal-tools
- Jirakittayakorn, N., & Wongsawat, Y. (2018). A novel insight of effects of a 3-Hz binaural beat on sleep stages during sleep. Frontiers in Human Neuroscience, 12, 387. https://doi.org/10.3389/fnhum.2018.00387
- Junqueira, D. R., Zorzela, L., Golder, S., Loke, Y., Gagnier, J. J., Julious, S. A., Li, T., Mayo-Wilson, E., Pham, B., Phillips, R., Santaguida, P., Scherer, R. W., Gøtzsche, P. C., Moher, D., Ioannidis, J. P. A., & Vohra, S. (2023). CONSORT harms 2022 statement, explanation, and elaboration: Updated guideline for the reporting of harms in randomised trials. BMJ, 381, e073725.
- Katmah, R., Al-Shargie, F., Tariq, U., Babiloni, F., Al-Mughairbi, F., & Al-Nashash, H. (2023). Mental stress management using fNIRS directed connectivity and audio stimulation. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 31, 1086–1096. https://doi.org/10.1109/TNSRE.2023.3239913
- Kelton, K., Weaver, T. L., Willoughby, L., Kaufman, D., & Santowski, A. (2021). The efficacy of binaural beats as a stress-buffering technique. Alternative Therapies in Health & Medicine, 27(4), 28–33.
- Kim, H. G., Cheon, E. J., Bai, D. S., Lee, Y. H., & Koo, B. H. (2018). Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investigation, 15(3), 235–245. https://doi.org/10.30773/pi.2017.08.17
- Lazarus, R. S., DeLongis, A., Folkman, S., & Gruen, R. (1985). Stress and adaptational outcomes. The problem of confounded measures. American Psychologist, 40(7), 770–779. https://doi.org/10.1037/0003-066X.40.7.770
- Lee, M., Lee, H. J., Ahn, J., Hong, J. K., & Yoon, I.-Y. (2022). Comparison of autonomous sensory meridian response and binaural auditory beats effects on stress reduction: A pilot study. Scientific Reports, 12(1), 19521. https://doi.org/10.1038/s41598-022-24120-w
- Leistiko, N. M., Madanat, L., Yeung, W. K. A., & Stone, J. M. (2023). Effects of gamma frequency binaural beats on attention and anxiety. Current Psychology, 43(6), 5032–5039. https://doi.org/10.1007/s12144-023-04681-3
- Le Scouarnec, R., Poirier, R., Owens, J. E., Gauthier, J., Taylor, A. G., & Foresman, P. A. (2001). Use of binaural beat tapes for treatment of anxiety: A pilot study of tape preference and outcomes. Alternative Therapies in Health & Medicine, 7(1), 58–63.
- Loong, L. J., Ling, K. K., Tai, E. L. M., Kueh, Y. C., Kuan, G., & Hussein, A. (2022). The effect of binaural beat audio on operative pain and anxiety in cataract surgery under topical anaesthesia: A randomized controlled trial. International Journal of Environmental Research and Public Health, 19(16), 10194. https://doi.org/10.3390/ijerph191610194
- Luis, E., Bermejo-Martins, E., Martinez, M., Sarrionandia, A., Cortes, C., Oliveros, E. Y., Garces, M. S., Oron, J. V., & Fernández-Berrocal, P. (2021). Relationship between self-care activities, stress and well-being during COVID-19 lockdown: A cross-cultural mediation model. BMJ Open, 11(12), e048469. https://doi.org/10.1136/bmjopen-2020-048469
- Maddison, R., Nazar, H., Obara, I., & Vuong, Q. C. (2022). The efficacy of sensory neural entrainment on acute and chronic pain: A systematic review and meta-analysis. British Journal of Pain, 17(2), 126–141. https://doi.org/10.1177/20494637221139472
- Mallik, A., & Russo, F. A. (2022). The effects of music & auditory beat stimulation on anxiety: A randomized clinical trial. PLoS ONE, 17(3), e0259312. https://doi.org/10.1371/journal.pone.0259312
- Marsh, S., Dobson, R., & Maddison, R. (2020). The relationship between household chaos and child, parent, and family outcomes: A systematic scoping review. BMC Public Health, 20(1), 513. https://doi.org/10.1186/s12889-020-08587-8
- Miller, G. E., Chen, E., & Parker, K. J. (2011). Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving toward a model of behavioral and biological mechanisms. Psychological Bulletin, 137(6), 959–997. https://doi.org/10.1037/a0024768
- Mind. (2021). Anxiety and panic attacks. Retrieved August 10, 2023, from https://www.mind.org.uk/information-support/types-of-mental-health-problems/anxiety-and-panic-attacks/anxiety-disorders/
- Musiek, F., Atcherson, S., Kennett, S. W., & Nicholson, N. (2012). The dangers of eDosing with binaural beats. Hearing Journal, 65(10), 9–10. https://doi.org/10.1097/01.HJ.0000421132.06215.20
- Olthuis, J. V., Watt, M. C., Bailey, K., Hayden, J. A., & Stewart, S. H. (2016). Therapist-supported internet cognitive behavioural therapy for anxiety disorders in adults. Cochrane Database of Systematic Reviews, 3(3), Cd011565.
- Opartpunyasarn, P., Vichitvejpaisal, P., & Oer-areemitr, N. (2022). The effect of binaural beat audio on anxiety in patients undergoing fiberoptic bronchoscopy: A prospective randomized controlled trial. Medicine, 101(24), e29392–e29392. https://doi.org/10.1097/MD.0000000000029392
- Oster, G. (1973). Auditory beats in the brain. Scientific American, 229(4), 94–102. https://doi.org/10.1038/scientificamerican1073-94
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Parodi, A., Fodde, P., Pellecchia, T., Puntoni, M., Fracchia, E., & Mazzella, M. (2021). A randomized controlled study examining a novel binaural beat technique for treatment of preoperative anxiety in a group of women undergoing elective caesarean section. Journal of Psychosomatic Obstetrics & Gynecology, 42(2), 147–151. https://doi.org/10.1080/0167482X.2020.1751607
- Petrakova, L., Doering, B. K., Vits, S., Engler, H., Rief, W., Schedlowski, M., & Grigoleit, J. S. (2015). Psychosocial stress increases salivary alpha-amylase activity independently from plasma noradrenaline levels. PLoS ONE, 10(8), e0134561. https://doi.org/10.1371/journal.pone.0134561
- Platt, J., & Hammond, L. (2023). Is non-clinical use of binaural beats audio an effective stress-management strategy? A systematic review. PROSPERO 2023 CRD42023428623. Retrieved August 6, 2023, from https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023428623
- Pressman, S. D., & Cohen, S. (2005). Does positive affect influence health? Psychological Bulletin, 131(6), 925–971. https://doi.org/10.1037/0033-2909.131.6.925
- Ross, B., Miyazaki, T., Thompson, J., Jamali, S., & Fujioka, T. (2014). Human cortical responses to slow and fast binaural beats reveal multiple mechanisms of binaural hearing. Journal of Neurophysiology, 112(8), 1871–1884. https://doi.org/10.1152/jn.00224.2014
- Ruotsalainen, J. H., Verbeek, J. H., Mariné, A., & Serra, C. (2015). Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews, 2015(4), Cd002892.
- Ryder, A. G., & Chentsova-Dutton, Y. E. (2012). Depression in cultural context: “Chinese somatization,” revisited. Psychiatric Clinics of North America, 35(1), 15–36. https://doi.org/10.1016/j.psc.2011.11.006
- Salari, N., Hosseinian-Far, A., Jalali, R., Vaisi-Raygani, A., Rasoulpoor, S., Mohammadi, M., Rasoulpoor, S., & Khaledi-Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Globalization and Health, 16(1), 57. https://doi.org/10.1186/s12992-020-00589-w
- Schwarz, D. W., & Taylor, P. (2005). Human auditory steady state responses to binaural and monaural beats. Clinical Neurophysiology, 116(3), 658–668. https://doi.org/10.1016/j.clinph.2004.09.014
- Selye, H. (2013). Stress in health and disease. Butterworth-Heinemann.
- Shalforoushan, S., Mohamadreza, G., & Zahra, B. (2021). The effectiveness of alpha binaural beats in reducing stress and rumination and promoting sleep quality in university students with poor sleep quality. Journal of Sleep Sciences, 6(3/4), 67–73.
- Stojanovich, L., & Marisavljevich, D. (2008). Stress as a trigger of autoimmune disease. Autoimmunity Reviews, 7(3), 209–213. https://doi.org/10.1016/j.autrev.2007.11.007
- Sztajzel, J. (2004). Heart rate variability: A noninvasive electrocardiographic method to measure the autonomic nervous system. Swiss Medical Weekly, 134(35-36), 514–522.
- Thanyawinichkul, K., Tontisirin, N., Mahawan, R., Kumdang, S., Yamsa-Ard, T., Maneepairoj, M., & Nakawiro, D. (2022). The efficacy of binaural beat stimulation mixed with acoustic music in chronic Low back pain management: A randomized controlled trial. Journal of the Medical Association of Thailand, 105(9), 806–814. https://doi.org/10.35755/jmedassocthai.2022.09.13598
- van Dalfsen, J. H., & Markus, C. R. (2018). The influence of sleep on human hypothalamic–pituitary–adrenal (HPA) axis reactivity: A systematic review. Sleep Medicine Reviews, 39, 187–194. https://doi.org/10.1016/j.smrv.2017.10.002
- Wahbeh, H., Calabrese, C., & Zwickey, H. (2007). Binaural beat technology in humans: A pilot study to assess psychologic and physiologic effects. The Journal of Alternative and Complementary Medicine, 13(1), 25–32. https://doi.org/10.1089/acm.2006.6196
- Wahbeh, H., Calabrese, C., Zwickey, H., & Zajdel, D. (2007b). Binaural beat technology in humans: A pilot study to assess neuropsychologic, physiologic, and electroencephalographic effects. The Journal of Alternative and Complementary Medicine, 13(2), 199–206. https://doi.org/10.1089/acm.2006.6201
- WHO. (2023). Mental health. Retrieved July 23, 2023, from https://www.who.int/health-topics/mental-health#tab=tab_2
- Wiwatwongwana, D., Vichitvejpaisal, P., Thaikruea, L., Klaphajone, J., Tantong, A., & Wiwatwongwana, A. (2016). The effect of music with and without binaural beat audio on operative anxiety in patients undergoing cataract surgery: A randomized controlled trial. Eye, 30(11), 1407–1414. https://doi.org/10.1038/eye.2016.160