
Abstract
We assessed Knowledge Attitude and Practice (KAP) regarding occupational noise exposure, Noise-induced hearing loss, audiometry and use of hearing protection devices among iron and steel factory workers exposed to high noise level. A modified, validated, structured questionnaire was used to collect information from 253 male workers randomly selected from the four factories. The sum scores for each domain of KAP were computed. Scores above 75% were defined as good knowledge and positive attitude. For practice, scores of >50% were defined as good. Independent samples t-test and Chi-squared test were used to analyze association between KAP and continuous/categorical variables respectively. Majority of workers displayed poor knowledge and poor practice (94%), but 76% displayed a positive attitude. Most of the workers (86%) had never been provided with hearing protection devices. The mean scores for attitude and practice differed significantly between the four factories (one-way ANOVA, p < 0.001). Implementation of hearing conservation program with provision of hearing protection devices are suggested.
Introduction
Noise-induced hearing loss (NIHL) is a public health problemCitation1 that has been increasing in developing countries (including Tanzania), as compared with other parts of the world.Citation2 The estimated prevalence of NIHL in studies in the field of mining and in iron and steel factories in Tanzania was 47% and 48% respectively,Citation3,Citation4 which is above the average global prevalence of NIHL, that ranges from 7%–21%.Citation5 A high prevalence of NIHL has been linked to increased industrialization coupled with governing institutions’ low capacity for provision of adequate preventive measures against noise, effective programs to prevent NIHL,Citation6,Citation7 poor data collection systemsCitation8,Citation9 and limited research to document the magnitude of the problem.Citation2 In addition, the coverage of occupational health services in the working population has been low,Citation7,Citation10 and this might in turn have affected workers’ knowledge of occupational noise exposure and prevention of hearing loss.
NIHL (with a permanent threshold shift) is irreversible once it has occurred, thus effective preventive solutions are necessary.Citation11 Various noise-control measures exist, namely engineering control (elimination, substitution, targeting of noise-source manipulation), administrative control (changing work practices and schedules, policy-making and enforcing regulations that target workers’ behavior) and use of personal protective equipment (PPE) to protect individual workers, with regular surveillance.Citation12,Citation13 Evaluation of the effectiveness of the interventions implemented has yielded varied results.Citation14 Nevertheless, studies suggest that a comprehensive hearing conservation program, including provision and use of hearing protection devices (HPDs), may be effective, even when administrative and engineering methods of noise control are not feasible,Citation15,Citation16 and such intervention has been found to be associated with less NIHL.Citation17 In countries with limited resources like Tanzania it would be feasible to advocate establishment and implementation of hearing conservation programs. To achieve this, it is necessary to establish and document workers’ Knowledge, Attitude and Practice (KAP) as a prerequisite for effective planning of interventions. This study is thus being conducted to document the level of KAP in iron and steel workers.
There are interactions between various aspects of individuals’ knowledge of health and their attitude to it that may affect practices at work.Citation18 A high prevalence of NIHL has been associated with a low level of KAP in workers. For example, a cross-sectional study of 97 Malaysian quarry workers found a high prevalence of NIHL (57%), while the KAP scores were low, i.e. 11% for knowledge, 10% for attitude and 28% for practice.Citation19 Other KAP studies have documented varying results about KAP. Two studies, one in Malaysia and the other in Nigeria, found good knowledge, a positive attitude but poor practice among workers.Citation20,Citation21 In addition, two other studies in Nigeria have reported good knowledge with poor practice.Citation22,Citation23
Practice can also be influenced by factors such as non-availability of hearing protection devices, high financial costs, poorly fitting of hearing protection devices, and maintenance, though regular training and supervision improve usage.Citation20,Citation21,Citation23,Citation24 Also, KAP scores differ among workers in different sectors, necessitating the documentation of sectoral related findings for effective planning and implementation of preventive interventions.
Our recent findings show that workers in the iron and steel factories in Tanzania were exposed to personal mean equivalent noise exposure (LEX,8h) of 92.0 dB (A).Citation3 Several processes contributed to the recorded sound level such as various operating machines, manual handling of metal scraps and steel billets and feeding metal scraps into furnace.Citation3 The prevalence of NIHL in these workers was 48%,Citation25 suggesting an urgent need for effective noise-control intervention. To our knowledge, there is no published information from iron and steel factories in Tanzania that would inform policy and decision makers and might be useful in the formulation and implementation of preventive measures seeking to improve the situation of workers. The purpose of this study was thus to assess KAP in iron and steel factory workers in Tanzania exposed to a high level of noise.
Materials and methods
Study population
We conducted a cross-sectional study of 253 randomly selected male participants working in steel-bar production lines in four iron and steel factories in Dar es Salaam, Tanzania between June 2016 and June 2017. The main study also comprised audiometry to examine hearing loss among the workers and measurement of noise exposure in the factories. The details of noise levels and the characteristics of the studied factories are presented elsewhere.Citation3
The sample size calculation was based on the estimated prevalence of hearing loss among workers exposed to loud noise at work. Since there was no available information about hearing loss among noise exposed workers or among the general population in Tanzania, the sample size was calculated based on a community baseline survey conducted in Uganda that found the prevalence of hearing loss among adults to be 12%.Citation26 In our study the effect of noise on hearing loss was hypothesized to be doubled i.e. 24%. To achieve 90% power and be able to detect a difference in hearing loss between noise exposed workers and a non-exposed group at a significance level of 0.05 (Using Open-Epi online calculator Version 3.3a),Citation27 totally 230 exposed workers was needed. We added 10% to account for non-responders, providing total sample size of 253 workers.
Study participants
The research team held meetings with the management of each factory, explained the purpose of the research and requested permission to conduct the project. All four factories agreed to participate. The managements of these factories each assigned a contact personnel to help the research team with the planning and implementation of the research activities. We included permanent production line workers who consented to participate and excluded workers in other sections without occupational noise exposure. A list of permanent workers was provided, and 253 workers were randomly selected from a total of 588 production workers of four factories. These workers were contacted and informed about the project objectives and were required to give written consent. All workers selected agreed to participate in the project. This study was ethically cleared by Ethical committees in Norway and Tanzania and all workers participated gave informed consent prior to their inclusion into the study.
Interview questionnaire
A modified, validated, structured KAP questionnaire from a study of Malaysian sawmill workers was used to collect information from 253 workers through an interview.Citation20,Citation28 This Malaysian questionnaire was modified to suit the local context, e.g. the statement in the knowledge-assessment part asking for hobbies was modified to omit the word ‘scuba’, adding ‘listening to loud music for long time’. A statement involving specific legislation in Malaysia was modified and remained as a neutral statement unrelated to any country. The word ‘sawmill’ was omitted, and the word ‘deafness’ was translated into ‘hearing loss’ (HL). The English version of the questionnaire was translated into Swahili and then back into English once to check for logical consistency and meaning. No changes were made after translation.
Workers’ knowledge regarding NIHL was assessed using 18 statements, each with a score of ‘1’ for correct response and a maximum score of 18 points, equivalent to 100%. The 18 statements in the knowledge domain were for collection of information on the causes, symptoms, treatment and prevention of NIHL.
Workers’ attitudes to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices were assessed by 13 statements, using a five-point scale ranging from ‘strongly disagree’, ‘disagree’ and ‘neither disagree or agree’ to ‘agree’ and ‘strongly agree’, each with a corresponding score of between one and five. The maximum score was 65 points, equivalent to 100%.
Workers’ practice regarding provision and use of hearing protection devices, health and safety training and audiometry were assessed using 12 statements with the three possible responses ‘always’, ‘sometimes’ and ‘never’, and with scores of 3, 2 and 1, respectively. The maximum score was 36 points, equivalent to 100%.
Information regarding participants’ socio-demographics, i.e. age in years, duration of work (in years) and educational level (no formal education, primary education, secondary and tertiary education) was also collected. All information was collected by a research assistant trained for the study.
Data analysis
Descriptive statistics were presented as means and standard deviation for continuous variables and frequencies or percentages for categorical variables.
The variable age in years was categorized as tertiles, with almost equal percentages of participants. Duration of work was arbitrarily categorized in accordance with three groups (≤2 years, 3–10 years, 11–24 years). The educational-level variable was dichotomized (primary education = 0 vs secondary and tertiary education = 1), as there were no participants without any formal education.
The sum scores for the KAP domains were computed, converted into percentages of the total score and then dichotomized, with knowledge and attitude scores of ≥75% being defined as good knowledge and positive attitude, respectively,Citation20 whilst the practice score of ≥50% was defined as good practice.
In the sum scores for KAP, the differences between age and duration of work were explored using one-way Analysis of Variance (ANOVA), whilst an independent samples t-test was used to analyze the association between KAP and the continuous variables, i.e. age, duration of work and educational level. Chi-squared test was used to analyze the association between dichotomized KAP and categorical variables, i.e. age group, duration of work and educational level. Two multiple linear regression analysis was used to explore the relationship between attitude and practice scores as dependent variables, respectively and the significant variables from the preliminary analyses, i.e. educational level and the factory. In this analysis, three dummy variables were used for factory B, factory C and factory D. Factory A was used as reference.
Internal consistency in distinct items in each domain of knowledge, attitude and practice was evaluated using Cronbach’s Alpha coefficient (α), the results being α = 0.74, 0.70 and 0.72, respectively.
The IBM SPSS statistics, Version 25 was used for data analysis and a parameter of p < 0.05 was set as statistical significance.
Ethical consideration
This study was completed in accordance with the Helsinki Declaration of 1975 and its subsequent revisions. The ethical clearance for this study was issued by The Regional Committee of Medical and Health Research Ethics (REK-VEST) in Norway number 2016/635/REK sør-øst dated 20th May 2016; and The Muhimbili University of Health and Allied Sciences (MUHAS) Ethics Committee in Tanzania with Institutional Review Board (IRB) number 2016-06-24/AEC/Vol. XI/38 dated 24th June 2016. Permission to conduct the study was granted by each iron and steel factory. The information collected was treated as confidential. Each individual participant was contacted and informed about the research objectives and activities to be conducted and gave written consent prior to inclusion into the study.
Results
The participants’ mean age (in years) was 32 (range: 18-64), and 68% of them were under 35. The mean age for Factory A was 29 (SD = 6), for Factory B 36 (9), for Factory C 29 (8) and for Factory D 33 (7). Sixty-seven per cent had received primary education, 33% had received secondary and tertiary education and 88% had worked for 3 to 10 years (). The participation was 100%.
Table 1. Descriptive characteristics of the participants and their association with KAP in the study among Tanzanian iron and steel workers (N = 253).
The mean scores for attitude and practice differed significantly between the four factories (one-way ANOVA, p < 0.001) (). Factory A had a significantly lower mean attitude score than the other three factories, whilst there was no significant difference between those other three factories. The mean practice score for Factory D was significantly lower than for the other three factories (A, B and C), whilst there was no significant difference in mean practice scores between those three factories. The mean knowledge scores did not differ between any of the four factories (one-way ANOVA, p > 0.05).
Overall the mean score for knowledge did not differ significantly between the subgroups for age, duration of work and educational level (). Only 23% of participants had a good knowledge (score ≥ 75%) of occupational noise-exposure hearing loss ().
There was a significant difference in attitude scores between participants who had received primary education and those who had received secondary and tertiary education (independent samples t-test, p = 0.01) (). The participants who had received primary education had a significantly more positive attitude than those who had received secondary and tertiary education (chi-square test, p < 0.05) (). In the practice domain, participants who had received primary education had significantly lower scores than their counterparts (independent samples t-test, p = 0.03) (). The overall mean scores for practice was low ().
In the multiple linear regression model for the attitude domain, factory B, factory C and factory D had higher scores than factory A, while secondary/tertiary education was associated with lower score than primary education. This regression model explained 28% of the total variance in attitude score ().
Table 2. Determinants for attitude and practice in a KAP study among 253 iron and steel factory workers in Tanzania.
For the practice domain, factory D had lower score than factory A (reference), while secondary/tertiary education was associated with higher score than primary education (). These two determinants (educational level and factory D) explained 12% of the total variance in practice.
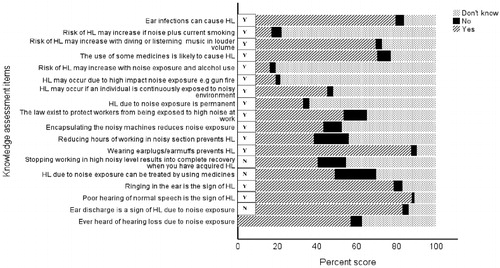
A high proportion of the participants had a poor overall knowledge of the specific causes of NIHL (). For example, only 16% responded correctly to the statement ‘HL may occur due to high-impact noise exposure, e.g. gunfire, and 45% to the statement ‘HL may occur if an individual is continuously exposed to a noisy environment’. Regarding NIHL symptoms, 88% responded correctly to the statement ‘Poor hearing of normal speech is a sign of HL’ and 79% to the statement ‘Ringing in the ear is the sign of HL’. Nevertheless, only 33% responded correctly to the statement ‘HL due to noise exposure is permanent’, 21% to the statement ‘HL due to noise exposure can be treated by using medicines’ and only 14% to the statement ‘Stopping working in high noise level results into complete recovery when you have acquired HL’ (). With regard to prevention, 87% responded correctly to the statement ‘Wearing earplugs/earmuffs prevents HL’, 43% to the statement ‘Encapsulating the noisy machines reduces noise exposure’, 38% to the statement ‘Reducing hours of working in a noisy section prevents HL’ and 53% to the statement ‘Laws exist to protect workers from being exposed to high noise at work’ ().
Figure 1. Knowledge score (as a percentage) regarding noise-induced hearing loss (NIHL) (causes, symptoms, treatment and prevention) for various items in 253 iron and steel workers in Tanzania. The correct answer for each item is indicated by Y = yes and N = no.
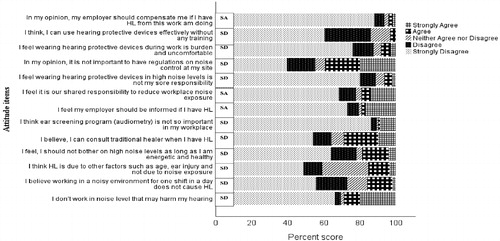
Overall 76% of the participants had a positive attitude to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices. Findings from specific items show that about 86% of the participants ‘strongly disagreed’ with the statement ‘I think ear-screening program (audiometry) is not so important at my workplace’, 80% with the statement ‘I feel wearing hearing protection devices during work is a burden and is uncomfortable’ and about 66% with the statement ‘I don’t work in noise level that may harm my hearing’ (). However, about 78% ‘strongly disagreed’ with the statement ‘I feel my employer should be informed if I have HL’ and about 61% with the statement ‘I feel it is our shared responsibility to reduce workplace noise exposure’ ().
Figure 2. Attitude score (as a percentage) for noise exposure and control, noise-induced hearing loss (NIHL), audiometry and wearing of hearing protection devices for various items in 253 iron and steel workers in Tanzania. The correct answer is indicated in a box following each statement, where SD = Strongly disagree and SA = Strongly agree.
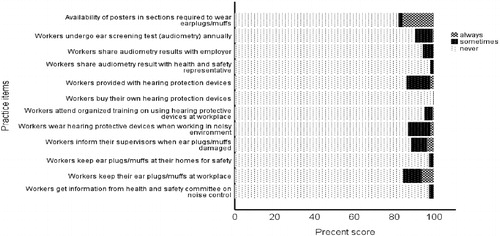
About 94% of the participants displayed poor practice regarding provision and use of hearing protection devices, health and safety training and audiometry (). The majority of the participants responded ‘Never’ to most of the statements. For example, 82% responded ‘Never’ to the statement ‘availability of posters in sections required to wear earplugs/muffs’, 95% to the statement ‘Workers attend organized trainings on using hearing protection devices at the workplace’ and 91% to the statement ‘Workers undergo ear-screening test (audiometry) annually’. In addition, 86% of the participants responded ‘Never’ to ‘Workers provided with hearing protection devices at work’, and a similar percentage responded likewise to ‘Workers wear hearing protection devices when working in a noisy environment’ ().
Figure 3. Percentage score for 13 items used for assessment of workers’ practice in a study among 253 iron and steel workers in Tanzania.
Discussion
Overall few workers in the four iron and steel factories had a good knowledge of NIHL. In addition, a majority of them displayed poor practice regarding use of hearing protection devices and a considerable number of them reported non-availability of these devices at their workplaces. However, the majority were found to have a positive attitude to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices. This suggests limited availability of education and training and a lack of hearing protection devices for workers.
A study of Malaysian quarry workers found a high prevalence of NIHL (57%), with a low level of knowledge (11%) among workers.Citation19 The present study found a fairly similar result, with the majority of our study participants displaying poor knowledge, and in these workers, the prevalence of NIHL was found to be high, i.e. 48%.Citation25 A study of Ghanaian mill workers also reported similar findings, with a high prevalence of NIHL (44%) and a relatively low level of knowledge (55%).Citation29 Thus, in these three studies there is an association between a low level of knowledge and a high prevalence of NIHL among noise exposed workers. Contrastingly, a study of Nigerian steel-mill workers found a good level of knowledge in workers (93%),Citation22 but a high prevalence of NIHL (57%),Citation30 indicating that a good level of knowledge may not be sufficient to prevent NIHL, and that there may be other contributory factors.Citation31
Our study participants displayed less knowledge of specific items, e.g. whether noise exposure may cause NIHL, than workers in Malaysian sawmills (78%) and Nigerian steel-mills (93%).Citation20,Citation22 The high knowledge score in those studies was presumably the result of personal experience of work in a noisy environment.Citation22,Citation32 In addition, the majority of our participants were not aware that stopping work in a high noise level will not result in complete recovery if NIHL has already been acquired, compared with 54% and 22% among workers in Malaysian sawmills and quarries respectively. One explanation may be the lack of an effective education and training program regarding occupational noise hazards and related hearing loss among iron and steel workers. An integrated education and training program for workers may thus be appropriate to improve workers’ knowledge of NIHL.Citation14,Citation15,Citation29
Our findings indicate that the majority of our study participants had a positive attitude to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices. One explanation may be what they perceive to be the risk of working in noisy environment. Our finding is in line with two studies of Malaysian sawmill and quarry workers, whose attitude scores were 61% and 70% respectively.Citation19,Citation20 The positive attitude of our study participants may be regarded as an intention to change their behavior,Citation33 and is likely to be a good sign for future preventive work.
The attitude of our participants regarding specific items was analogous to that ascertained in the studies of Malaysian sawmill and quarry workers.Citation19,Citation20 Most workers had a positive attitude to use of hearing protection devices. For example, 80% of our participants had a positive attitude, whilst in Malaysian sawmill and quarry workers the proportional of the participants were 92% and 94% respectively. This may indicate the potential success of noise-preventive measures, including provision of hearing protection devices. In addition, 86% of our participants had a positive attitude to ear screening, comparable to that in Malaysian sawmill and quarry workers, ie 84% and 89% respectively. However, 78% had a negative attitude to sharing their ear-screening (audiometry) results with their employers – an attitude quite similar to that displayed by Malaysian quarry workers (87%).Citation19 This careful attitude may be due to a fear of losing their job. It may also be due to a lack of knowledge of the effect of occupational noise exposure on hearing.
Our results show that participants who have received secondary and tertiary education displayed better practice than those who have received primary education. Our findings are in line with a study of Malaysian quarry workers, where workers who had received education below secondary level displayed ignorance of the use of personal protective equipment.Citation19 This is probably because of the increased knowledge gained in school, which can sometimes be translated into the way people think and act. Surprisingly, in our study workers who had received primary education had a more positive attitude to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices. than those who had received secondary and tertiary education. These findings differ from those for Malaysian quarry workers. One of the explanations may be that formal education does not necessarily change human perception of workplace hazards such as noise. Also, the difference between our study and the Malaysian quarry study might lie in the methodology, whereby workers who had not received any formal education were compared with those who had received a formal education, whilst there were no workers who had not received a formal education in our present study.
In our study the overall practice was poor, as only 14% of the participants had been provided with and used hearing protection devices. In addition, factory D has the lowest practice score among others. This is analogous to the Malaysian sawmill and quarry studies, where 12% and 14% of workers respectively used hearing protection devices.Citation20 This may in part be explained by the non-availability of these devices in iron and steel factories. Although we did not find any information regarding provision of hearing protection devices for workers in the Malaysian studies, it is likely that non-provision of personal protective equipment by employers at the workplaces was the reason for a low level of utilization of the protective measures, or even non-utilization.Citation34 A study of Nigerian steel mill workers reported provision of hearing protection devices for only 27% of workers, indicating that non-provision of these devices for workers was a problem.Citation22 This provides a clue as to why only a very low proportion of workers (<10%) in these studies reported having attended training on occupational safety and health issues, including the use of hearing protection devices. This underlines the importance of provision of hearing protection devices at workplaces where workers are exposed to harmful noise. On the other hand, the non-availability of ear-screening programs for workers in our present study is analogous to the situation in the two studies of Malaysian sawmill and quarry workers, where only 6% and 2%, respectively, of workers reported having undergone ear screening, which might be interpreted as either poor coverage and/or ineffective implementation of reported in developing countries.Citation2,Citation7
The strengths of this study include a high participation rate. In addition, items within the three KAP domains displayed a high internal consistency, and we used a previously validated questionnaire. However, interview-based questionnaires may be subjected to a socially desirable reporting bias. We explained the objective of the project, and the interview was carried out in private. This reduces the fear of disclosing confidential information, hence we have no reason to suspect any motivation that might have influenced the result. Also, the research team was available in the factories during data collection, and this was probably good as regards obtaining the correct information from participants. We used a large sample size, and our participants were randomly selected from the list of workers provided by the administration, thereby minimizing the selection bias.
Our study participants were male workers in the production line in large-scale iron and steel factories exposed to a high noise level, thus our findings may be valid for other groups of workers with similar workplace characteristics.
In Tanzania the Occupational Safety and Health Act (OSHA) No. 5 of 2003 requires the employer to provide and maintain effective personal protective equipment (hearing protection devices) for the use of employees, and to conduct a thorough pre-placement as well as periodic medical examinations (including ear screening in this case). However, our findings indicate that the practical implementation of these requirements was poor. This might be the case for other low- and middle-income countries.Citation7,Citation10 Thus, results from this study may be used by stakeholders at all levels, as a reflection of the status of implementation of occupational safety and health policy, legislation and noise control-related regulations in the countries facing similar challenges. This will help in the formulation and effective implementation of workplace noise-control measures including comprehensive hearing conservation programs to protect workers from developing hearing loss.
Conclusions
This study found that the majority of workers in the studied iron and steel factories had a poor knowledge of NIHL, a positive attitude to the importance of noise reduction at the workplace, NIHL, audiometry and wearing of hearing protection devices, as well as poor practice regarding provision and use of hearing protection devices, health and safety training. With a high noise level present, noise-control measures entailing the formulation and implementation of comprehensive hearing conservation program and improved provision of hearing protection devices are suggested, to avoid NIHL.
Acknowledgments
The authors are grateful to the four iron and steel factory managements for permission to host the project and for consenting to the participation of workers. We would like to thank the workers for their participation. Our appreciation also goes to the field research assistant (Ms Judith A. Haule), Muhimbili University of Health and Allied Sciences and the Occupational Safety and Health Authority in Tanzania for their helpful contribution to this work. This work was financially supported by the Norwegian State Educational Loan Fund (Lånekassen).
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Rabinowitz PM. The public health significance of noise-induced hearing loss. In: Le Prell CG, Henderson D, Fay RR, Popper AN, eds. Noise-Induced Hearing Loss: Scientific Advances. New York: Springer Science + Business Media, LLC; 2012:13–25. doi:10.1007/978-1-4419-9523-0_2.
- Smith AW. The World Health Organization and the prevention of deafness and hearing impairment caused by noise. Noise Health. 1998;1:6–12.
- Nyarubeli IP, Tungu AM, Bratveit M, Sunde E, Kayumba AV, Moen BE. Variability and determinants of occupational noise exposure among iron and steel factory workers in Tanzania. Ann Work Expo Health.2018;62(9):1109–1122. doi:10.1093/annweh/wxy071.
- Musiba Z. The prevalence of noise-induced hearing loss among Tanzanian miners. OCCMED. 2015;65(5):386–390. doi:10.1093/occmed/kqv046.
- Nelson DI, Nelson RY, Concha-Barrientos M, et al. The global burden of occupational noise-induced hearing loss. Am J Ind Med. 2005;48(6):446–458. doi:10.1002/ajim.20223.
- Concha-Barrientos M, Campbell-Lendrum D, Steenland, K. Occupational Noise: assessing the Burden of Disease from Work-Related Hearing Impairment at National and Local Levels. Geneva: World Health Organization; 2004, (WHO Environmental Burden of Disease Series, No. 9), ISBN 9241591927.
- Mrema EJ, Ngowi AV, Mamuya SH. Status of occupational health and safety and related challenges in expanding economy of Tanzania. Ann Glob Health. 2015;81(4):538–547. doi:10.1016/j.aogh.2015.08.021.
- Nuwayhid IA. Occupational health research in developing countries: a partner for social justice. Am J Public Health. 2004;94(11):1916–1921. doi:10.2105/AJPH.94.11.1916.
- Christiani DC, Durvasula R, Myers J. Occupational health in developing countries: review of research needs. Am J Ind Med. 1990;17(3):393–401. doi:10.1002/ajim.4700170311.
- Rantanen J, Lehtinen S, Valenti A, Iavicoli S. A global survey on occupational health services in selected international commission on occupational health (ICOH) member countries. BMC Public Health 2017;17(1):787. doi:10.1186/s12889-017-4800-z.
- Basner M, Babisch W, Davis A, et al. Auditory and non-auditory effects of noise on health. Lancet 2014;383(9925):1325–1332. doi:10.1016/S0140-6736(13)61613-X.
- National Institute for Occupational Safety and Health (NIOSH). Criteria For A Recommended Standard: Occupational Noise Exposure Revised Criteria 1998:105. NIOSH, Ed. Cincinnati, Ohio; 1998.
- Health and Safety Executive (HSE). Controlling noise at work. The Control of Noise at Work Regulations 2005 no. 1643. Guidance on Regulations; 2005.
- Verbeek JH, Kateman E, Morata TC, Dreschler WA, Mischke C. Interventions to prevent occupational noise-induced hearing loss: a Cochrane systematic review. Int J Audiol. 2014;53(Supp. 2):S84–S96. doi:10.3109/14992027.2013.857436.
- Okpala NC. Knowledge and attitude of infantry soldiers to hearing conservation. Mil Med. 2007;172(5):520–522.
- Dobie RA. Cost-effective hearing conservation: regulatory and research priorities. Ear Hear.2018;39(4):621–630. doi:10.1097/AUD.0000000000000523.
- Tikka C, Verbeek JH, Kateman E, Morata TC, Dreschler WA, Ferrite S. Interventions to prevent occupational noise-induced hearing loss. Cochrane Database Syst Rev. 2017;7:Cd006396. doi:10.1002/14651858.
- Badran IG. Knowledge, attitude and practice the three pillars of excellence and wisdom: a place in the medical profession. East Mediterr Health J. 1995;1(1):8–16.
- Ismail AF, Daud A, Ismail Z, Abdullah B. Noise-induced hearing loss among quarry workers in a north-eastern state of Malaysia: a study on knowledge, attitude and practice. Oman Med J. 2013;28(5):331–336. doi:10.5001/omj.2013.9.
- Razman Mohd R, Daud A, Musa KI, Naing L. Knowledge, attitude and practice of sawmill workers towards noise-induced hearing loss in Kota Bharu, Kelantan. Malays J Med Sci. 2008;15(4):28–34.
- Okafoagu NC, Oche M, Awosan KJ, et al. Determinants of knowledge and safety practices of occupational hazards of textile dye workers in Sokoto, Nigeria: a descriptive analytic study. J Public Health Afr. 2017;8 (1):664. doi:10.4081/jphia.2017.664.
- Ologe FE, Akande TM, Olajide TG. Noise exposure, awareness, attitudes and use of hearing protection in a steel rolling mill in Nigeria. Occup Med (Lond). 2005;55(6):487–489. doi:10.1093/occmed/kqi089.
- Sogebi OA, Amoran OE, Iyaniwura CA, Oyewole EA. Awareness and attitudes to noise and its hazards in motor parks in a sub-urban Nigerian town. Niger Postgrad Med J. 2014; 21(1):40–45.
- Sayapathi SB, Su TA, Koh D. Knowledge, attitude and practice in relation to noise - induced hearing loss in two factories. Res J Biol Sci. 2014;9(6):197–2014.
- Nyarubeli IP, Tungu AM, Moen BE, Bråtveit M. Prevalence of Noise-Induced Hearing Loss Among Tanzanian Iron and Steel Workers: A Cross- Sectional Study.Int J. Environ. Res. Public Health 2019;16:1367; doi:10.3390/ijerph16081367
- Westerberg BD, Lee PK, Lukwago L, Zaramba S, Bubikere S, Stewart I. Cross-sectional survey of hearing impairment and ear disease in Uganda. J Otolaryngol Head Neck Surg. 2008;37(6):753–758.
- Dean AG, Soe MM. OpenEpi: Open source epidemiologic statistics for public health, version 3.03a. http://www.openepi.com/. Last accessed March 7, 2019.
- Razman MR, Naing L, Azian D, Kamarul IM. Validation of noise induced hearing loss questionnaire among Malay sawmill workers in Kelantan Malaysia. Int Med J Malaysia. 2010;9(2):51–56.
- Kitcher ED, Ocansey G, Abaidoo B, Atule A. Occupational hearing loss of market mill workers in the city of Accra, Ghana. Noise Health. 2014;16(70):183–188. doi:10.4103/1463-1741.134919.
- Ologe FE, Akande TM, Olajide TG. Occupational noise exposure and sensorineural hearing loss among workers of a steel rolling mill. Eur Arch Otorhinolaryngol. 2006;263(7):618–621. doi:10.1007/s00405-006-0043-9.
- Rashaad Hansia M, Dickinson D. Hearing protection device usage at a South African gold mine. Occup Med (Lond). 2010;60(1):72–74. doi:10.1093/occmed/kqp114.
- Kahan E, Ross E. Knowledge and attitudes of a group of South African mine workers towards noise induced hearing loss and the use of hearing protective devices. S Afr J Commun Disord. 1994;41:37–47.
- World Health Organization (WHO). Health education: theoretical concepts, effective strategies, and core competencies: a foundation document to guide capacity development of health educators. Eastern Mediterranean Health; 2012:1–82.
- Haldiya KR, Sachdev R, Mathur ML, Saiyed HN. Knowledge, attitude and practices related to occupational health problems among salt workers working in the desert of Rajasthan, India. J Occup Health. 2005;47(1):85–88. doi:10.1539/joh.47.85.