
Abstract
A participatory-based intervention was performed in Sweden, aimed at improving the sound environment in one preschool (n = 20) and one obstetric ward (n = 50), with two controls each (n = 28, n = 66). Measured sound levels, and surveys of noise annoyance, hearing-related symptoms and emotional exhaustion were collected before, and three and nine months after the interventions, comparing intervention and control groups over time. The results of this first implementation in a limited number of workplaces showed significantly worsening of hyperacusis, sound-induced auditory fatigue, emotional exhaustion and increased sound levels in the preschool, and worsening of noise annoyance in both intervention groups. Increased risk awareness, limited implementation support and lack of psychosocial interventions may explain the worsening in outcomes, as might the worse baseline in the intervention groups. The complexity of the demands in human-service workplaces calls for further intervention studies.
Introduction
Noise exposure is one of the major causes of occupational disease.Citation1 The European Work Authorities highlights a lack of risk assessments in female-dominated sectors.Citation2 In human-service settings, such as education and health care, traditional interventions such as attenuating or removing noise sources are inadequate, as the noise arise mainly from intense speech communication, children playing or medical alarms.Citation3 Indoor noise levels in Swedish preschools may reach 80 decibel A-weighted equivalent levels (dB LAeq), often intermittently exceeding 85 dB LAeq(1 min), with maximum A-weighted levels (dB LAFmax) close to or even exceeding 115 dB.Citation4–6 In a Swedish obstetrics ward, 46% of 61 work-shifts exceeded 80 dB LAeq(7-10 h), and 5% exceeded 85 dB LAeq(7-10 h), with several instances above 115 dB LAFmax.Citation7 Exceeding these levels pose a risk of hearing damage.
A Swedish study found increased risk ratios (RR) for sound-induced auditory fatigue (RR 2.4, 95% confidence interval CI 2.2–2.5), hyperacusis (RR 2.3, 95% CI 2.1–2.5), difficulty perceiving speech (RR 1.9, 95% CI 1.7–2.0), tinnitus (RR 1.7, 95% CI 1.5–1.9) and hearing loss (RR 1.6, 95% CI 1.5–1.8) in female preschool teachers (n = 4718), compared to randomly selected women (n = 4122).Citation8 Increased hazard ratio (HR) of hyperacusis (HR 3.4, 95% CI 3.0–3.7) has also been found in Swedish preschool teachers compared to women working in low noise exposure (<75 dB LAeq(8h)).Citation9 One study on obstetrics personnel in Sweden found increased odds ratio (OR) for sound-induced auditory fatigue (OR 1.04, 95% CI 1.00–1.07) and tinnitus (OR 1.04, 95% CI 1.00–1.09) in relation occupational noise.Citation7
Swedish and Danish studies have shown that stress-related disorders (e.g. burnout and emotional exhaustion) are common in preschool personnel and midwives.Citation10,Citation11 The noise-stress model outline how noise cause physiological arousalby activating the sympathetic nervous system and the endocrine system.Citation12 Interestingly, studies have indicated an association between stressand hearing,Citation13 such as increased hyperacusis during an acute stress test among women with emotional burnout.Citation14 High working demands is pervasive in human-service work,Citation15 andmay thus also be important to reduce to prevent hearing disorder. Consistent with the noise-stress model, noise annoyance may modify or mediate the risk of hearing-related symptoms.Citation7,Citation16 Notably, 70% of preschool teachers and 49% of obstetrics personnel in Sweden report noise annoyance at work,Citation7,Citation17 compared to 27% in the general female population.Citation17
There is a lack of noise intervention studies in communication-intense human-service settings. While studies in the obstetrics care are lacking, a few studies in preschools in Sweden and Germany have found small or non-significant effects from acoustic or organizational measures on outcomes including noise annoyance and burnout.Citation6,Citation18–21 Small or absent effects may result from a lack of “measure-to-challenge correspondence” (the interventions do not target the existing problems).Citation22Compared to top-down implementation (e.g.from management), which can lack relevance and motivation among employees, employee-driven change is often focused on actual problems and realistic solutions,Citation23 and may achieve a sustainable change by integration with the ordinary systematic work environment work.Citation24 This emphasizes the possibilities of noise intervention studies using a participatory-based approach.
This study aims to assess the effects on hearing-related outcomes, noise annoyance and emotional exhaustion of context-specific interventions developed using a participatory-based approach in one preschool and one obstetrics ward in Sweden. The hypothesis was an improved sound environment, and a decreased reporting of hearing-related outcomes, noise annoyance and emotional exhaustion.
Methods and materials
Study design, setting and selection of participants
The study was designed as a non-randomized non-blinded intervention aimed at improving the sound environment in female-dominated human-service communication-intense settings (preschools and obstetrics care) by implementing context-specific interventions developed using a participatory approach.
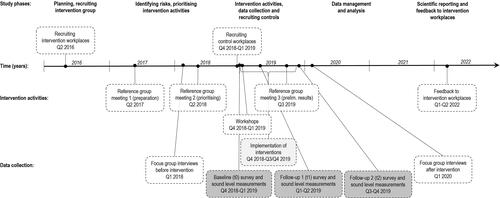
shows the timeline, the study phases and intervention activities. A purposive selection was used to ensure that the intervention workplaces had the necessary characteristics of female-dominated human-service communication-intense settings, and that they had resources to engage in the participatory approach. All workplaces were located in the Västra Götaland County, Sweden. One intervention preschool was selected via the head of schools in one municipality. The preschool principal had the resources and motivation to participate. One intervention obstetrics ward was selected after having participated in a previous study, which informed the researchers of the workplace characteristics. They also had resources to renovate the department as part of the intervention. Two control workplaces were recruited for each intervention workplace, closely matching size and building characteristics. All preschools were in suburban medium sized municipalities. The number of children ranged from around 50 in one control preschool to around 80-90 in the intervention preschool and the other control. In the obstetrics, the low-risk labor wards were included. The intervention ward was located at a university hospital in a larger city, with approximately 4000 births per year. The controls were among the next largest wards in in smaller neighboring cities, with around 3000 births per year each. One larger obstetrics ward and two preschools initially declined participation. One control preschool was excluded due to plans of a stress-reducing intervention.
Figure 1. Timeline of the study phases, the intervention activities, and the data collection. The control workplaces participated only in the data collection (dark grey), while the intervention workplaces participated in all the intervention activities and the data collection.
All employees were invited to participate. Managers were not considered participants but were involved in the intervention process.
The study was approved by the Regional Ethical Review Board, Gothenburg Sweden, No. 659-18. Participants received written information and signed a written informed consent form.
The intervention processes
shows the intervention process, initiating with a reference group meeting in May 2017 including researchers, representatives from the intervention workplaces, and key stakeholders, explaining the study aim, and giving presentations on noise, stress and organizational interventions. Then, separate qualitative interviews, reported elsewhere,Citation3 were conducted to assess the needs, opportunities, and ideas for interventions. These results fed into the intervention via a second reference group meeting held in May 2018, including the intervention workplaces, where selection and priority ofinterventions was initiated. Then, baseline measurements were collected, after which implementation of interventions begun. To support the implementation process, a workshop (1.5-2 h) was held at each intervention workplace, including results from the qualitative interviews.Citation27 In accordance with the participatory method, the workshops encouraged active participation from the personnel.Citation25,Citation26 Two additional meetings were held with managers and one union representative at the obstetrics intervention to support the implementation. In September 2019, a third reference group meeting was held focussing on following through with the implementation, and included evaluation of the process and descriptive data on the implementation so far. Adaptations of the interventions after this point were slight. After the final data collection, follow-up qualitative interviews were performed, reported elsewhere.Citation25 Finally, results were reported back to the workplaces.
The intervention content
details the intervention content, which included changes to the physical environment, and organizational and psychosocial changes. All employees who were not on leave of absence were considered to have received theseworkplace level interventions.
Table 1. The selected and prioritized context-specific intervention contents implemented in the obstetrics care and the preschool setting.
Data collection
Questionnaire surveys
Survey data was collected at three timepoints: baseline (t0), and two follow-ups approximately 3-4 months (t1), and 9 months (t2) after baseline. The first follow-up was performed after the workshop, during the implementation process, as per the participatory approach.Citation28
All personnel received a questionnaire and two reminders attheir home address or at work. Including items on hearing loss, tinnitus, difficulty perceiving speech at work, sound sensitivity (hyperacusis) and sound-induced auditory fatigue, previously diagnostically validated in the obstetrics care (except for difficulty perceiving speech at work previously assessed as a combination of work and leisure time),Citation29 and in Think Aloud interviews on preschool teachers.Citation8 Noise annoyance at work was assessed using an item adapted for the workplace, based on the ISO/TS 15666:2003.Citation30 Emotional exhaustion was assessed using the five items from the emotional exhaustion subscale of the Maslach Burnout Inventory general survey (MBI-GS),Citation31 in Swedish,Citation32 with a modified 6-point response scale,excluding the alternative “A few times each week”. For MBI-GS, internal missing were replaced by the mean if three or more items were reported. All response alternatives and the categorization defining the analyzed variables (binary, ordinal or scale) are detailed in . The survey also included items measuring potential confounders, for example age, noise at work, manager support, general health, as detailed in supplement A.
Table 2. Baseline values for the outcome variables with categories or scale as analyzed, shown as valid column percentages (%*), or mean and standard deviation (SD), within the obstetrics setting and the preschool setting, separating the intervention workplace from the controls.
Sound level measurements
Sound levels were measured each timepoint during one work week (five days in preschools and seven days in the obstetrics). The SVANTEK SV 104 (IEC 61252 − 2002, Class 2, IEC 61672-1 – 2013, range 43 to 141 dBA Peak) dosimeters were used, except at baseline in the obstetrics intervention where the Larson Davis 705+ (IEC 61252 − 1993, Class 2, range 40 to 143 dBA Peak) was used. Sound levels were logged every 30 s. Personnel wore the dosimeter on the right shoulder close to the ear and wrote a log including start and stop times and work activities.
Equivalent daily A-weighted decibel level (dB LAeq), minimum two hours, and the highest A-weighted fast maximum decibel level (dB LAFmax) per measurement, were calculated from eight dosimeters per day in preschool and from ten dosimeters in obstetrics care. Work shifts in obstetrics (day, evening, and night) were similar and thus combined. Calculations were done in Python, after data managing in excel to exclude loggings when the dosimeter was not reported to be worn orwhen the personnel left the workplace (e.g., being outside, or at a nearby ward) was excluded. Coffee and lunch breaks were included to reflect the individual dose.
Statistical analysis
Baseline characteristics and prevalence are presented as valid percentages for categorical variables, and as mean and standard deviation (SD) for continuous variables. Repeatedly measured outcomes were analyzed using the generalized estimating equation (GEE), including participants who responded at baseline and at least one of the two follow-ups. Each workplace setting was analyzed separately. Response categories from the survey were merged if there were few responses, and assessed as either binary or ordinal, as detailed in . Each outcome was analyzed in separate models, controlling for its baseline value. Potential confounders were selectedusinga theoretical approach, then assessed statistically (forward stepwise) and kept if beta changed ≥15%. A timepoint variable (follow-up 1 or follow-up 2) was analyzed to assess change over time, and included if beta changed ≥15%. Dosimeter data was analyzed for each setting separately by comparing the group average equivalent (dB LAeq) and maximum (dB LAFmax) sound levels between the intervention and the control group at each timepoint using t-test with Bonferroni correction, and over timepoints within each group using One-way ANOVA with post hoc pairwise comparisons using Bonferroni. All tests were two-sided, with p-value <0.05 considered statistically significant. Analyses were performed using IBM SPSS Statistics 28.0 and Stata/SE 17.0.
Results
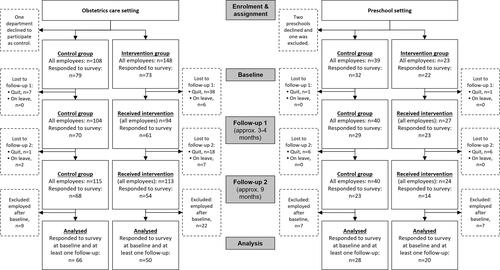
details the number of participants responding to the survey at each timepoint. The response rate at baseline in preschool was 96% in the intervention group and 82% in the control group, and in obstetrics (including hourly employees) 49% in the intervention group and 73% in the control group. The response rates decreased over time. The preschool intervention group was slightly older (mean 49 years) than the controls (mean 38 years). In the obstetrics the mean age was 50 years in both groups.
Figure 2. Participant flow diagram detailing number of personnel enrolled, lost to follow-up, responding at each timepoint, and the final study sample included in the analysis.
shows that baseline outcomes were slightly more prevalent and with more frequently occurring symptoms in both intervention groups compared to their control. The results from the GEE analysis () did not show any significant improvement from the intervention (a negative β would indicate an improvement in the outcome, whereas a positive β indicates a worsening in the outcome). Hyperacusis changed in a direction toward improvement in the obstetrics setting, but the model was not significant. A similar trend was seen for difficulty perceiving speech in obstetrics and tinnitus in preschool. In contrast, a significant worsening was found for noise annoyance in both settings, although descriptive data for the intervention group in the obstetrics care showed less worsening than the control group (). Hyperacusis, sound-induced auditory fatigue, and emotional exhaustion also showed a significant worsening in preschool. There was no significant effect of time.
Figure 3. Descriptive data of the individual change in the outcomes as valid percentages reporting improvement (green), worsening (orange) or remaining unchanged (grey) from baseline to follow up (merging results from t1 and t2) within the intervention group (I) and control group (C) respectively, in the obstetrics care setting (left) and in the preschool setting (right).
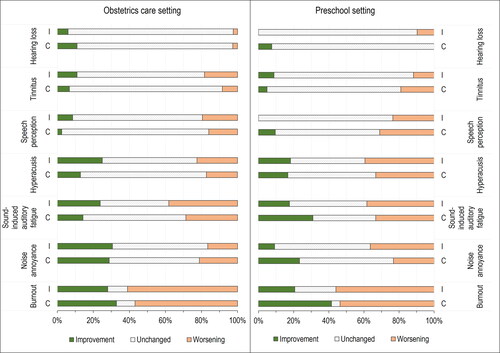
Table 3. Generalized estimating equation (GEE) analyzing the effect of intervention by comparing outcomes at follow-up in the intervention versus the control group in the obstetrics and the preschool setting respectively (control group as reference).
shows that equivalent sound levels was slightly higher in the preschools compared to the obstetric wards, and that in the preschool setting the mean equivalent levels increased significantly in the intervention group from baseline to follow-up 2 with a medium effect size of the overall model (ANOVA p = 0.005, post hoc t0-t2 p = 0.004). As shown in , there were no other significant differences.
Figure 4. Boxplots of daily A-weighted equivalent sound levels (dB LAeq) from dosimeter measurements in the obstetrics care (left) and in the preschools (right).
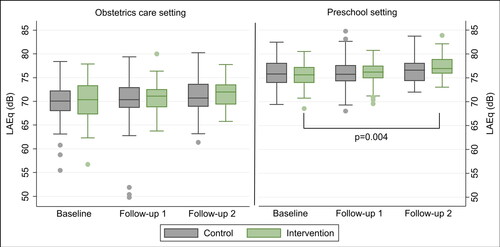
Table 4. Descriptive data and analysis of average sound levels within each group over timepoints and between control and intervention group at each timepoint.
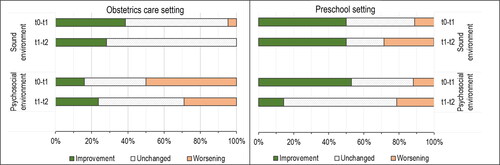
illustrates that a larger proportion reported improvements in sound environment than in psychosocial work environment in both intervention groups. Notably, at the final follow-up a third of the preschool group and a third of the obstetrics group perceived a worsening of sound environment and psychosocial environment respectively.
Figure 5. Descriptive responses of perceived changes in the work environment within the intervention groups, showing improvement (green), worsening (orange) or remaining unchanged (grey) from baseline (t0) to the first follow-up (t1), and between the two follow-ups (t1 and t2) in the obstetrics care setting (left) and in the preschool setting (right).
Discussion
The main result was the significant worsening after the intervention in some outcomes, instead of the hypothesized improvement. In the obstetrics, only noise annoyance worsened significantly. In the preschool, worsening of hyperacusis, sound-induced auditory fatigue, noise annoyance and emotional exhaustion, and increased equivalent sound levels was found. The worsening is partly explained by a larger improvement in the control groups. If starting with worse values makes it harder to improve, the effect could also be partly explained by worse baseline values in the intervention groups. Control workplaces were selected to match the intervention workplaces and analyses were adjusted for potential confounding differences, but differences may still have influenced. The significantly increased sound levels in preschool supports the hypothesis of a causal relationship with health outcomes, but the worsening may also be a result of the intervention raising awareness of the health risks of noise exposure.
A lack of resources and support for implementation may have decreased the intervention effect. This is supported by a concurrent qualitative evaluation,Citation27 where personnel expressed positive attitudes toward the changes but also described hindering factors. An earlier study in the same population highlighted that improvements were much wanted,Citation3 which may have increased the expectations of improvement. Blinded or double-blinded occupational interventions are nearly impossible,Citation33 and high expectations have been suggested to explain worsening of outcomes in participatory interventions,Citation26 as have employee disappointment due to poor implementation.Citation12
While there are studies aimed at improving the sound environment in hospital settings such as intensive care,Citation34 we have found no studies from the obstetrics care. Previous interventions in preschool have shown divergent results, but we still expected improvement particularly in noise annoyance,Citation18 and sound-induced auditory fatigue,Citation35 and decreased sound levels.Citation6,Citation19,Citation20 The sound levels were comparable to previous studies both in preschools and obstetrics care,Citation7,Citation18 and may be high enough to pose a risk to hearing. Previous interventions did not assess hearing-related symptoms, but one assessed whether hearing protection devices decreased personnel burnout.Citation21 Similar to our study, they found a non-significant increase in burnout, while another preschool study found significant increased stress after interventions aimed at improving the sound environment.Citation20
It has previously been suggested that organizational needs will be prioritized over needs of a research intervention study.Citation36 We argue that high work demands may impact particularly participatory-based interventions where personnel and managers are responsible for implementation. Fewer intervention measures were directed at the psychosocial work environment, despite of, or due to, the increasingly demanding work environment with cutbacks, lay-offs, and increased workload.Citation3,Citation27 This may have overshadowed improvements from the sound environment interventions, and it could explain the increased emotional exhaustion. The personnel have described that noise causes stress but also that stressful working conditions made the noise more difficult to handle,Citation3 which potentially explain the increased noise in the preschool. We hypothesize that stress and noise have a synergistic effect on health, as reported for environmental noise and job strain,Citation37 partly through noise annoyance causing a stress reaction,Citation38 as described in the noise-stress model.Citation12
Strengths and limitations
A limited sample size may cause type-II errors. Confidence intervals were wide and estimates uncertain, but descriptive data of individual change generally supported the statistical analysis. The limited sample motivated analysis of both follow-ups, although implementation was ongoing at the first follow-up, and motivated including individuals responding at only one follow-up. This may mean that the full or final intervention effect was not analyzed, though no significant time effect was found. The limited number of intervention sites and the purposive selection could introduce bias and hinder generalization. Hence, further studies could confirm or counter the results from this first trial using these participatory-developed interventions.
There were fundamental similarities in the interventions in the two settings, matching the similar work environments. A strength of the participatory methodis context-specific interventions,Citation26 and high measure-to-challenge correspondence.Citation22 The approach is however limited in estimating effects of specific measures. Randomized controlled trials (RCTs) are still considered gold standard, but are difficult to implement in occupational settings and has limitations in real-world effectiveness.Citation33
The participatory method requires consideration of the personnel’s influence over and involvement in the intervention process.Citation28 Involvement was mainly representative via the reference group. Representative involvement has however not been shown to result in less influence or participation.Citation28 The workplaces had limited influence over the process. It is common,Citation28 and it may have influenced the results since process participation is associated with the perception of change and thus with the intervention outcome.Citation39 Another potential weakness is that organizational influence was not a goal in itself. It has been suggested important for sustainable change.Citation28
The accompanying qualitative evaluation reported elsewhere,Citation27 is an important strength of the overall project as it provides a nuanced and multifaceted analysis of the personnel’s perceptions of the intervention process and outcome. It showed that the overall experience was positive.Citation27 Hence, we suggest further studies using the participatory approach to develop innovative, context-specific, and comprehensive interventions, to meet the complex issues in these communication-intense settings. These should consider and analyze the process and degree of implementation, personnel participation and expectations, and the potentially hindering effect of concurrent work-related factors such as stress and high workload. Although difficult, follow-up studies should evaluated the interventions in larger samples, and ideally at more intervention sites with randomized assignment to the intervention group.
Conclusions
This study could not show significant improvement from the intervention. Contrary, a significant worsening in hyperacusis, sound-induced auditory fatigue, emotional exhaustion and noise annoyance, and increased equivalent sound levels was found in preschool, and worsening noise annoyance was found in obstetrics. The results may be explained by larger improvements in controls, and if starting with worse values makes it harder to improve, the effect could also be partly explained by worse baseline values in the intervention groups. Raised awareness of risks in the intervention group may initially inflated the outcomes, but the increase in sound levels and concurrent worsening in outcomes also supports a causal relationship. A lack of psychosocial interventions may explain the worsening of emotional exhaustion. The complexity of the demands in communication-intense human-service workplaces calls for further studies on sustainable interventions.
Supplemental Material
Download MS Word (44.5 KB)Acknowledgements
The authors acknowledge the contribution of Mikael Ögren, PhD, and Fiona Starke, MSc, in the management of the dosimeter data.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The participants of this study did not give consent for data to be shared. However, anonymised data is available upon reasonable request and providing approval from an ethical review board.
Additional information
Funding
References
- Themann CL, Masterson EA. Occupational noise exposure: A review of its effects, epidemiology, and impact with recommendations for reducing its burden. J Acoust Soc Am. 2019;146(5):3879–3905. doi:10.1121/1.5134465.
- EU-OSHA. New Risks and Trends in the Safety and Health of Women at work - European Risk Observatory: Literature Review. Luxembourg: Publications Office of the European Union; 2013.
- Gyllensten K, Fredriksson S, Widen S, et al. The experience of noise in communication-intense workplaces: a qualitative study. PLoS One. 2023;18(1):e0280241. doi:10.1371/journal.pone.0280241.
- Sjödin F, Kjellberg A, Knutsson A, et al. Noise exposure and auditory effects on preschool personnel. Noise Health. 2012;14(57):72–82. doi:10.4103/1463-1741.95135.
- Neitzel RL, Svensson EB, Sayler SK, et al. A comparison of occupational and nonoccupational noise exposures in Sweden. Noise Health. 2014;16(72):270–278. doi:10.4103/1463-1741.140503.
- Persson Waye K, Karlberg J. Sound quality characteristics of importance for preschool children’s perception and wellbeing after an acoustic intervention. Front Built Environ. 2021;7:91. doi:10.3389/fbuil.2021.688836.
- Fredriksson S, Hammar O, Torén K, et al. The effect of occupational noise exposure on tinnitus and sound-induced auditory fatigue among obstetrics personnel: a cross-sectional study. BMJ Open. 2015;5(3):e005793. doi:10.1136/bmjopen-2014-005793.
- Fredriksson S, Kim J-L, Torén K, et al. Working in preschool increases the risk of hearing-related symptoms: a cohort study among Swedish women. Int Arch Occup Environ Health. 2019;92(8):1179–1190. doi:10.1007/s00420-019-01453-0.
- Fredriksson S, Hussain-Alkhateeb L, Torén K, et al. The impact of occupational noise exposure on hyperacusis: a longitudinal population study of female workers in Sweden. Ear Hear. 2022;43(4):1366–1377. doi:10.1097/AUD.0000000000001194.
- Wieclaw J, Agerbo E, Mortensen PB, et al. Risk of affective and stress related disorders among employees in human service professions. Occup Environ Med. 2006;63(5):314–319. doi:10.1136/oem.2004.019398.
- Hildingsson I, Westlund K, Wiklund I. Burnout in Swedish midwives. Sex Reprod Healthc. 2013;4(3):87–91. doi:10.1016/j.srhc.2013.07.001.
- Babisch W. The noise/stress concept, risk assessment and research needs. Noise and Health. 2002;4(16):1–11.
- Canlon B, Theorell T, Hasson D. Associations between stress and hearing problems in humans. Hear Res. 2013;295:9–15. doi:10.1016/j.heares.2012.08.015.
- Hasson D, Theorell T, Bergquist J, Canlon B. Acute stress induces hyperacusis in women with high levels of emotional exhaustion. PLoS One. 2013;8(1):e52945. doi:10.1371/journal.pone.0052945.
- Dollard MF, Dormann C, Boyd CM, Winefield HR, Winefield AH. Unique aspects of stress in human service work. Australian Psychologist. 2003;38(2):84–91. doi:10.1080/00050060310001707087.
- Fredriksson S, Hussain-Alkhateeb L, Persson Waye K. The effect of occupational noise on hearing-related symptoms-exploring mediating and modifying effect of annoyance and stress. In: 12th ICBEN Congress on Noise as a Public Health Problem, Zurich Schweitz; 2017:1–9.
- Fredriksson S. Hearing-Related Symptoms among Women - Occurrence and Risk in Relation to Occupational Noise and Stressful Working Conditions. Gothenburg, Sweden: Department of Occupational and Environmental Medicine, Institute of Medicine at Sahlgrenska Academy, University of Gothenburg; 2018.
- Persson Waye K. Perception and measurements of the pre-school sound environment-before and after acoustic improvements. In: INTER-NOISE and NOISE-CON Congress and Conference Proceedings. Institute of Noise Control Engineering; 2009.
- Gerhardsson L, Nilsson E. Noise disturbances in daycarecenters before and after acoustical treatment. J Environ Health. 2013;75(7):36–40.
- Sjödin F, Kjellberg A, Knutsson A, et al. Measures against preschool noise and its adverse effects on the personnel: an intervention study. Int Arch Occup Environ Health. 2014;87(1):95–110. doi:10.1007/s00420-012-0833-x.
- Koch P, Stranzinger J, Kersten JF, et al. Use of moulded hearing protectors by child care workers-an interventional pilot study. J Occup Med Toxicol. 2016;11(1):50. doi:10.1186/s12995-016-0138-1.
- Severin J, Björk L, Corin L, et al. Process evaluation of an operational-level job stress intervention aimed at decreasing sickness absence among public sector employees in Sweden. Int J Environ Res Public Health. 2021;18(4):1778. doi:10.3390/ijerph18041778.
- Ekman M, et al. Innovationer i vårdens vardag: de små stegens väg till förändring. Lund, Sweden: Studentlitteratur AB; 2007.
- von Thiele Schwarz U, Lundmark R, Hasson H. The dynamic integrated evaluation model (DIEM): achieving sustainability in organizational intervention through a participatory evaluation approach. Stress Health. 2016;32(4):285–293. doi:10.1002/smi.2701.
- Augustsson H, Richter A, Hasson H, et al. The need for dual openness to change: a longitudinal study evaluating the impact of employees’ openness to organizational change content and process on intervention outcomes. J Appl Behav Sci. 2017;53(3):349–368. doi:10.1177/0021886317691930.
- Framke E, Sørensen OH, Pedersen J, et al. Effect of a participatory organizational workplace intervention on workplace social capital: post-hoc results from a cluster randomized controlled trial. BMC Public Health. 2019;19(1):693. doi:10.1186/s12889-019-6903-1.
- Gyllensten K, Fredriksson S, Widen S, et al. Nurses’ and preschool teachers’ experiences of taking part in a participatory intervention project in communication-intense working environments. Work. 2022;73(3):857–869. doi:10.3233/WOR-211009.
- Abildgaard JS, Hasson H, von Thiele Schwarz U, et al. Forms of participation: The development and application of a conceptual model of participation in work environment interventions. Econ Ind Democracy. 2020;41(3):746–769. doi:10.1177/0143831X17743576.
- Fredriksson S, Hammar O, Magnusson L, et al. Validating self-reporting of hearing-related symptoms against pure-tone audiometry, otoacoustic emission, and speech audiometry. Int J Audiol. 2016;55(8):454–462. doi:10.1080/14992027.2016.1177210.
- ISO. Acoustics – Assessment of Noise Annoyance by Means of Socio-Acoustic or Social Surveys. Geneva; 2003.
- Schaufeli, W, Leiter, M, Maslach, C, & Jackson, S. Maslach Burnout Inventory–General Survey (GS). In: Maslach, C., Jackson, S. E. and Leiter, M. P. (eds.), The Maslach Burnout Inventory: Test Manual, Palo Alto, California: Consulting Psychologists Press; 1996.
- Magnusson Hanson LL, Theorell T, Oxenstierna G, et al. Demand, control and social climate as predictors of emotional exhaustion symptoms in working Swedish men and women. Scand J Public Health. 2008;36(7):737–743. doi:10.1177/1403494808090164.
- Schelvis RMC, Oude Hengel KM, Burdorf A, et al. Evaluation of occupational health interventions using a randomized controlled trial: challenges and alternative research designs. Scand J Work Environ Health. 2015;41(5):491–503. doi:10.5271/sjweh.3505.
- Hagerman I, Rasmanis G, Blomkvist V, et al. Influence of intensive coronary care acoustics on the quality of care and physiological state of patients. Int J Cardiol. 2005;98(2):267–270. doi:10.1016/j.ijcard.2003.11.006.
- Persson Waye K, et al. God ljudmiljö i förskola - samband mellan ljudmiljö, hälsa och välbefinnandeföre och efter åtgärdsprogram. Gothenburg, Sweden: Rapportserie AMM Göteborgs Universitet; 2011.
- von Thiele Schwarz U, Nielsen K, Edwards K, et al. How to design, implement and evaluate organizational interventions for maximum impact: the Sigtuna Principles. Eur J Work Organ Psychol. 2021;30(3):415–427. doi:10.1080/1359432X.2020.1803960.
- Selander J, Bluhm G, Nilsson M, et al. Joint effects of job strain and road-traffic and occupational noise on myocardial infarction. Scand J Work Environ Health. 2013;39(2):195–203. doi:10.5271/sjweh.3324.
- Kjellberg A. Subjective, behavioral and psychophysiological effects of noise. Scand J Work Environ Health. 1990;16(Suppl 1):29–38. doi:10.5271/sjweh.1825.
- Nielsen K, Randall R. The importance of employee participation and perceptions of changes in procedures in a teamworking intervention. Work Stress. 2012;26(2):91–111. doi:10.1080/02678373.2012.682721.
