
Abstract
Introduction
Two Spirit and Native LGBTQ people have unique health risks and cultural strengths.
Method
This study analyzes 28 reports published since 1980 examining the health and identity–formation experiences of Two Spirit or Native LGBTQ individuals.
Results
The majority (68%) of the articles focus on urban populations. Few employ a strengths-based approach. Less than half capture information about gender identity.
Conclusion
Findings suggest that Two Spirit and Native LGBTQ individuals are underrepresented in current health research. Existing research prioritizes a disease-specific perspective. Future research focused on intersectional identity formation, connectedness, and culture as a protective factor is needed.
Introduction
Note: There are over 574 Federally recognized Tribes in the United States, and even more state recognized and unrecognized Tribes. Each of these Tribes have their own culture, history, knowledge and way of referring to themselves. Throughout this article, we will be using the term Native to refer to the Indigenous people of the United States and Canada.
Prior to colonization, concepts of gender identity in Native communities were diverse and the acceptance of gender diversity was high. Two Spirit people, “whose behaviors or beliefs may be interpreted by others to be uncharacteristic of their sex,” were often expected to take on roles as medicine people, mentors, teachers, and healers (Jacobs, Citation1997). This practice of diverse gender acceptance in Native communities has been dramatically altered through colonization and the forced assimilation process. However, the history of Native acceptance of Two Spirit and LGBTQ identities remains in the teachings and wisdom of Native ancestors and Two Spirit Elders living today. Many Two Spirit and Native LGBTQ people credit their Elders as sources of affirmation and support (Walters et al., Citation2006). This combination of historical acceptance and contemporary marginalization is unique to Two Spirit and Native LGBTQ communities.
Despite this unique intersectional identity, studies which examine the effects of Two Spirit identity on health are extremely uncommon. Studies examining the impacts of Native identity, or non-Native LGBTQ identity, on health are rare as well. Studies focused on LGBTQ health generally focus on White European populations, and studies focused on Native health rarely capture sexual orientation or gender identity (Huang, Citation2010; Sarche & Spicer, Citation2008).
While both Native and LGBTQ communities experience unique cultural strengths, traditions, and histories that promote good health and wellness, research on both populations generally focuses on health disparities. From this research, we know that LGBTQ individuals are more likely to experience homelessness, unemployment, and lack of access to appropriate healthcare and housing services (Office of Disease Prevention and Health Promotion, Citation2020). These social determinants lead to health disparities including higher rates of sexually transmitted infections, substance use, mood disorders, and suicide (Office of Disease Prevention and Health Promotion Citation2020). Native people are more likely to experience homelessness, poverty, and a lack of targeted education and employment services (Sarche & Spicer, Citation2008). These social determinants lead to health disparities including higher rates of sexually transmitted infections, substance use, diabetes, and suicide (Indian Health Service Disparities, Citation2019).
Discrimination has been consistently linked to adverse health effects for both Native and LGBTQ people (Gates, Citation2013; Shavers et al., Citation2012). Two Spirit and Native LGBTQ people face layers of discrimination—heterosexism and cisnormativity within some Native communities, racism and stereotyping within non-Native LGBTQ communities. Initial surveys, including the 2015 U.S. Transgender Survey’s Report on the Experiences of American Indian/Alaska Native Respondents, report disparities affecting Native trans individuals. Fifty-seven percent of Native trans people had experienced homelessness. Twenty-one percent had lost a job because of their trans identity. One in two trans people who had accessed healthcare in the last year reported a negative experience related to their trans identity (USTS, Citation2015). However, as there has never been a systematic review of literature focused on Native Two Spirit and LGBTQ individuals, it is difficult to know what disparities—and what resiliencies—are being effectively recorded and which may be overlooked.
To describe that gap, we aim to systematically review and report the scope and findings of existing studies in which a majority of participants are Native and Two Spirit or LGBTQ. Through this work, we hope to better understand the health of Two Spirit and Native LGBTQ individuals and better determine the necessary direction of future research and programmatic work to achieve health equity in Two Spirit and Native LGBTQ communities.
Materials and methods
Inclusion criteria
To be included in the analysis, studies had to (a) be available in English, (b) include at least 10% Native American, Alaska Native, or Indigenous persons, (c) include at least 10% Two Spirit or LGBTQ persons, (d) report out results specifically for Native and Two Spirit or LGBTQ individuals, (e) be published between January 1980 and December 2019, and (f) focus on health disparities, health risk, health inequities, social determinants, community health, discrimination, or equity. All relevant records came from the USA or Canada. Though we did not limit our search by country, searches were conducted in English.
Search strategy
Search terms included (Native OR American Indian OR Alaska Native OR indigenous OR Native Hawaiian) AND (Two Spirit OR LGBTQ OR lesbian OR gay OR bisexual OR transgender OR queer OR genderqueer OR sexuality OR pansexual OR nonbinary OR trans* OR indigiqueer OR gender identity OR sexual orientation) AND (health disparity OR health risk OR health inequity OR social determinants of health OR Community Health OR CBPR OR protective factors OR equity OR discrimination OR health). Several databases were searched, including CINAHL Complete, Academic Search Ultimate, Alt HealthWatch, Family and Society Studies Worldwide, Family Studies Abstracts, Gender Studies Database, Health Policy Reference Center, Health Source: Nursing/Academic Edition, MEDLINE Complete, PsycINFO, Public Administration Abstracts, Public Affairs Index, and Women's Studies International.
The original search, completed in November 2019, yielded 42 unique articles. Double-blind coding by two researchers determined article exclusion/inclusion. Any discrepancies in inclusion between the two researchers were discussed until they came to consensus.
Additionally, a review of references from the 17 initially included articles was performed by two researchers. This review resulted in an additional 11 articles, which met the inclusion criteria.
Coding strategy
Two researchers independently (double-blind) coded each of the 28 finally included articles with specific focus on three categories outlined below. The information retrieved from each article included: year of the study, percent of participants who are Two Spirit or LGBTQ, percent of participants who are Native, Indigenous, or Aboriginal, setting, country, sampling method, sample size, population age, subject, research framework, CBPR or not, qualitative or quantitative, rural or urban focus, and key results. Any discrepancies in coding were reviewed and discussed by the researchers to come to consensus.
Demographics
The percentage of the study population which was Two Spirit or LGBTQ was noted. For studies which provided further information about sexual orientation or gender identity of participants (i.e. percentage lesbian, gay, bisexual, trans, or Two Spirit), those percentages were broken out, as seen in . In addition, the percentage of Native American, Alaska Native, Indigenous, or Aboriginal participants was recorded.
Table 1. Demographic information for retrieved and included articles.
Population age was recorded as child (12 years or under), adolescent/youth (12–18 years), and adult (over 18 years).
In addition, the study’s focus on rural or urban participants was recorded.
Study characteristics
Study characteristics, such as sampling method, sample size, research framework (i.e. focus groups, cross-sectional, or semi-structured interviews), place where research was conducted, quantitative or qualitative data type, and study type were recorded, as shown in .
Table 2. Summary of methods and results for retrieved and included articles.
When recording sampling method, studies which were a part of a larger study were designated as subset analyses.
Subject and results
Using an inductive approach, studies were coded by subject (HIV/AIDs, sexual health, mental/behavioral health, violence prevention, health equity, substance use, or overall health).
Key results and conclusions of the studies were recorded, as shown in .
Results
Exclusion
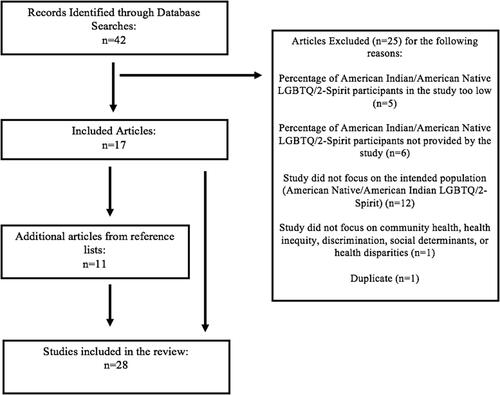
Seventeen of the original 42 articles met the inclusion criteria. Of the 25 excluded articles, five were excluded because they had less than 10% Two Spirit and LGBTQ or Native participants. Six were excluded because they did not report the percentage of Two Spirit and LGBTQ or Native participants. Twelve were excluded because they did not report out results specifically for Two Spirit and LGBTQ or Native participants, one was excluded because it did not focus on health, and one was a duplicate article ().
Figure 1. PRISMA diagram depicting article inclusion and exclusion.
Article characteristics
Of the 28 included articles, the majority (67.9%) examined health of urban Two Spirit and Native LGBTQ populations. Four articles (14.2%) focused on adolescent populations (12–18 years old). No articles focused specifically on children (<12 years old). No articles focused specifically on elder populations (>65 years old). Nine (32.1%) of the articles examined Canadian communities. The remaining 19 (67.9%) were based in the United States. shows the demographic qualities of each article.
A majority (75%) of the articles had study populations comprised exclusively of Native people. All 28 studies reported demographic data about sexual orientation and gender identity. Fifteen (55.6%) had study populations which were exclusively Two Spirit or LGBTQ.
Only 18 (60.7%) of the studies broke down their participant populations beyond general headings, such as “Two Spirit” or “LGBT.” Of those, ten (39%) reported the percentage of their study participants which were transgender. Only two studies focused on a population which had a majority of trans participants. The other six studies which reported their transgender participant percentages showed a range from 0% to 14% transgender, with an average percentage of nine percent. None of the studies provided information about gender identities beyond the binary of transgender or cisgender, such as nonbinary, genderqueer, or agender.
Regarding sexual orientation, nine (32%) studies reported the percentage of participants who identified as bisexual. Of these, percentages ranged from 2% to 45%, with an average of 23%. None of the studies offered sexual orientations beyond straight (heterosexual), gay (homosexual), lesbian, bisexual, or queer.
Of the 18 (71.4%) studies which reported the number of participants who identified as Two Spirit, 11% (n = 2) recorded Two Spirit as a gender identity; 44% (n = 8) recorded it as a sexual orientation, and 44% (n = 8) did not distinguish between the two. Of these final studies, several defined Two Spirit as a term that went beyond sexual orientation or gender identity, encompassing both of those things as well as activism, traditional tribal roles, and spirituality. Other studies, which did not define Two Spirit as specially a sexual orientation or gender identity, used the term as an umbrella heading for Native LGBTQ individuals.
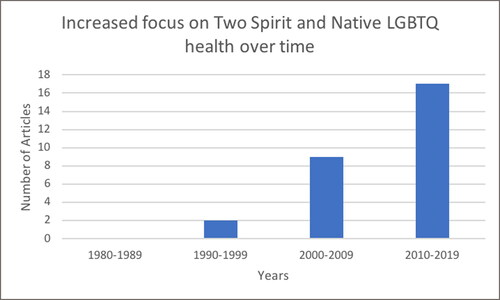
The number of articles surveying the health of Two Spirit and Native LGBTQ populations has steadily increased since 1980 ().
Figure 2. Volume of research in Two Spirit and Native LGBTQ health over time from 1980 to 2019.
Sample size varied widely across reports (mean 329; median 107; SD 755; range 6:3748). Just under half of the reports (n = 10; 42.9%) had a sample size greater than 100, and four articles (14.3%) had a sample size less than 20.
Four articles (14.3%) employed a community-based participatory research (CBPR) methodological design. These included a survey of service access and self-reported health for Aboriginal trans people in Canada (Scheim et al., Citation2013), the development of a research agenda with youth in the Northwest Territories (Logie et al., Citation2015), a survey of barriers to HIV prevention among Native men who have sex with men in Oklahoma City (Burks et al., Citation2011), and a survey of the effects of migration on the health of Aboriginal Two Spirit and LGBTQ people in Canada (Ristock et al., Citation2010).
Ten (35.7%) of the articles included secondary or subset analysis of data from the HONOR (Honoring Our Nations and Our Relations) Project, a large-scale, cross-sectional survey of Two Spirit and Native LGBTQ people completed in 2006 by Dr. Karina Walters at the University of Washington. Of the 18 articles which did not use data from the HONOR Project, 11 used targeted sampling. Two used network sampling. Two used respondent driven sampling. One used convenience sampling. Two were literature reviews that did not include new data.
The articles were almost evenly split between qualitative (n = 13; 46.4%) and quantitative (n = 15, 53.6%) analysis. Among qualitative articles, semi-structured interviews and focus groups were the major research framework (n = 11). Two articles reported findings from literature reviews. Quantitative articles drew from cross-sectional surveys. No articles included information from longitudinal surveys. No articles included evaluation of a specific intervention or training program designed for Two Spirit or Native LGBTQ people.
The majority of the articles focused on disparities-based health outcomes. The most common focus was sexual health (n = 11, 39.3%). Of articles focused on sexual health, seven focused specifically on HIV/AIDS prevention, intervention, or treatment. Articles also focused on mental health (n = 5; 17.9%), substance use (n = 5; 17.9%), violence prevention (n = 3, 10.7%), or overall health (n = 3, 10.7%). A minority of studies (n = 8; 28.6%) focused on health equity, intersectionality, and/or identity formation as it relates to health outcomes. The central results and conclusions of the articles appear in .
Only a few of the reports examined their research questions or hypotheses from an explicitly intersectional lens. For example, Walters et al. (Citation2006) analyzed transcripts from five interviews with Two Spirit women to explore identity formation, connectedness, and pride as they relate to self-rated health. None of the articles approached their research questions or hypotheses from an explicitly strengths-based framework.
Discussion
As shown in , nearly all of the articles sampled in this analysis were published within the last 10 years. This reflects a growing interest in Two Spirit and Native LGBTQ health. The vast majority of included studies focus exclusively on Two Spirit or Native LGBTQ populations, which allows survey instruments to be tailored to these communities. Further, the HONOR Project, from which many of these articles drew data, remains an ongoing source of robust information gathering and reporting. Conducted in 2002 to 2007 by Dr. Karina Walters at the University of Washington in Seattle, the HONOR Project is a multi-site national study which collected 452 survey interviews and completed 65 qualitative interviews with Two Spirit and Native LGBTQ individuals from urban sites (Town et al., Citation2018). The researchers are deeply indebted to the individuals who conducted and published the research reflected in this literature review. Their work has laid a foundation for the necessary future work, which will update the data they captured, reflecting the current strengths and health disparities of Two Spirit and Native LGBTQ people.
Importantly, findings from this review suggest that within this increased interest and focus, gaps remain. Specifically, the existing literature on the health and wellness of Two Spirit and Native LGBTQ people focuses on sexual health, mental health, and substance use, at the possible expense of broader measures of holistic health and wellbeing required to determine necessary interventions to achieving health equity. Also lacking is a dialogue about strengths unique to this subpopulation, protective qualities of Two Spirit and Native LGBTQ identities, and the importance of cultural practices for health maintenance.
A majority of the sampled articles focus on sexual health, and HIV/AIDS in particular. While this research was indelibly driven by the HIV epidemic and infections in Native communities and the near total lack of robust treatment and prevention options available to Native people until very recently (like in the rural southwest), the absence of research on other key health indicators within this population can largely be attributed to the lack of resources for Two Spirit- or LGBTQ-specific health research (Iralu et al., Citation2010). This deficiency remains in spite of advocacy efforts by Native researchers to secure funding streams to address Two Spirit and LGBTQ health. Researchers interested in Two Spirit or Native LGBTQ research are left largely dependent on disease- or disparities-based funding, such as that available for studying HIV/AIDS. By narrowing Two Spirit and Native LGBTQ research to the study of HIV/AIDS among this community, an unintended cycle of stigma also emerges, wherein Two Spirit or Native LGBTQ people become conflated with HIV/AIDS research. Early research on non-Native gay men in the United States perpetuated the same cycle (Herek et al., Citation2003).
This emphasis on specific disease topics also leads to a lack of data on social supports, networking, and relationship structures within Two Spirit and Native LGBTQ communities. For instance, only a few of the previous researchers ask participants about their levels of disclosure to their social contacts regarding their gender identity and sexual orientation, though we know social transition and acceptance is key to Two Spirit and LGBTQ health overall (Durwood et al., Citation2017). None of the previous research explores relationship structures (polyamorous, ethically nonmonogamous, monogamous) or the roles that either conventional or nonconventional social contacts play in the maintenance of health and wellbeing as Two Spirit and Native LGBTQ people interact with each other, the Native community at large, or mainstream society. One recent study conducted with mostly white older gay men examined the importance of social network ties for maintenance of both physical and social health by demonstrating ways that gay men construct families and social protection for themselves (Tester & Wright, Citation2017). Similar research would be helpful for understanding social networks and health maintenance among Two Spirit and Native LGBTQ populations.
A shift away from a disparities-centered focus also provides opportunities to explore unique protective factors experienced by a group, particularly in health research. DeBruyn et al. (Citation2020) well describes the promise offered by investigating integration of cultural practices into public health strategies for decreasing the incidence of Type II Diabetes in an among American Indian Tribal Nations. Similarly, given Two Spirit people employ a wide variety of understandings of Two Spirit histories, roles, and practices, those roles and practices could serve as cultural protective factors, but this potential has yet to be investigated.
Representation
This review further identifies several notable gaps among the subpopulations represented in articles focused on health within Two Spirit and Native LGBTQ communities. In the broader literature, Native and LGBTQ populations are often not reflected in demographic surveys, as is emphasized by the exclusion of several of the original 42 articles, because they did not report percentages of LGBTQ or Native participants. Given these well-known data limitations, scant data describes the intersection of Indigeneity and gender identity or sexual orientation diversity. Within each community—LGBTQ, Native, and Two Spirit/Native LGBTQ—further limitations regarding representation within datasets are discussed below.
Tribal affiliation
The majority of included reports that draw on Native-specific data employed non-descript, pan-ethnic labels (like Native American, Indigenous, or American Indian) to describe respondents, and did not include tribal affiliation or homelands. This prevents the assessment of the impacts of regional variation on Two Spirit and Native LGBTQ health. This is of consequence because reservation, rural non-reservation, and urban Native people often face their own unique challenges with regard to social and institutional racism (Jeffries, Citation2018). It also obscures diverse tribal understandings of gender identity and sexual orientation, and the wide variation in acceptance of Two Spirit identities and/or roles among different tribal communities.
The non-descript nature of the data on Two Spirit and Native LGBTQ people also allows for a situation where Two Spirit is only referred to broadly, and is rarely discussed in the context of any particular tribal nation which may further mystify the concept and implicitly reinforce the stigmatization of Two Spirit individuals within their own tribal communities. That is, if Two Spirit remains a vague and largely urban concept in the literature, Two Spirit individuals who reside within their tribal lands may struggle to disclose that identity for fear of being perceived as an outsider. Two Spirit is, of course, an umbrella term used to refer to many different traditional roles and practices, recognizing wide tribal diversity in areas including but not limited to gender, each with its own original roles and corresponding language used to describe it. As one of Walters’ et al. (Citation2006) Two Spirit respondents points out, “the word Two-Spirit, as you may know, is really just a contemporary marker … for lack of a yet-to-be-found better word” (p. 135). However, if Two Spirit research were to capture unique tribal experiences and diversity, the concept and resulting data could become more relatable and therefore useful to people who may identify with the term in diverse and complex ways that are not limited to a single definition.
Gender
More comprehensive measurements and reports on sexual orientation and gender identity are needed. Many of the sampled studies fail to capture gender identity altogether. None of the studies provided gender identities beyond the binary of transgender or cisgender (such as nonbinary, genderqueer, or agender). With one exception, none of the previous researchers specified whether trans respondents identified as transwomen, transmen, or trans nonbinary, conflating groups who are likely to experience discrimination very differently and have very different health risks and needs. Further, several studies used the descriptor “men who have sex with men” to apply to transwomen, conflating entirely different groups of people and inaccurately assuming the gender identities, sexual orientations, and sexual behaviors of trans women. Allowing respondents more options for self-identifying, even and especially qualitative measures that allow them to describe their own gender identities and sexual orientations, diminishes the perpetuation of unintentional microaggressions and misgendering by the researchers themselves.
Sexual orientation
None of the sampled studies offered sexual orientation options broader than straight (heterosexual), gay (homosexual), lesbian, bisexual, or queer. Individuals who identify as asexual, pansexual, graysexual, or other identities may therefore be misrepresented. Response rates are not always reported, but some individuals interacting with surveys that do not allow them to represent themselves adequately may fail to complete the survey or have their responses rejected. The same is true for gender identity.
Youth and elders
None of the studies sampled in this review cite datasets that include Elder Two Spirit and Native LGBTQ individuals. Elder Two Spirit and LGBTQ individuals may access services and experience discrimination differently than those who are younger or who were raised in a different generation (Choi & Meyer, Citation2016). Many Native Elders experienced Indian Boarding or Residential Schools firsthand, or are only one to two generations removed from them, so there is likely to be a unique relationship with stigma, assimilation, and other factors that may prevent disclosure, affect social supports, foster urban displacement, or facilitate additional impacts on health and wellbeing (Evans-Campbell et al., Citation2012; Grayshield et al., Citation2015).
Further, none of the sampled studies include data from interviews nor surveys with Two Spirit or LGBTQ youth under 12 years of age. Relying on allies or parents to report on the experiences of Two Spirit and LGBTQ youth does not offer an accurate portrayal of youth experiences, especially since the most vulnerable youth are those not able to be open with parents or trusted adults about their sexual orientation or gender identity (Katz-Wise et al., Citation2016).
Setting
The majority of these articles cite data reflective of participants recruited from urban settings. While it is the case that over seventy percent of the Native population resides off reservations, this feature of existing data means that we know little of the experiences of Native people who reside in rural and/or reservation settings (Norris et al., Citation2012). While obtaining statistically significant numbers of participants from relatively small reservation populations may be an incredible challenge, capturing cross-reservation data as well as applying meaningful qualitative assessments would provide useful insight for future health interventions (Walls et al., Citation2019).
Further, studies that sample both rural and urban populations rely heavily on clinics and community organizations for recruitment. The data, then, represents only the Two Spirit and Native LGBTQ individuals who are linked to care and/or to supportive community. Individuals in rural areas who are not accessing LGBTQ organizations or healthcare providers remain unsampled and invisible. Within that neglected subset may be the largest level of need.
Exemplary study
Of the studies sampled in this analysis, that reported by Scheim et al. (Citation2013) is a review of data from the cross-sectional survey completed as part of the Trans PULSE Project. This study is the most comprehensive that we found. The article captures complete gender identity and sexual orientation information for participants, including non-binary gender identities, distinguishes between trans-masculine and trans-feminine respondents, and includes a range of sexual orientations, including asexual, bisexual, and pansexual. This study further captures social demographic information for participants, including social transition status and access to services like housing or education. This study, we believe, sheds light on the potential for future Two Spirit and Native LGBTQ research.
Two Spirit term and identity
In these articles, the term Two Spirit is used in different ways. In some, the author states that the term Two Spirit is used throughout as an umbrella term to describe any Native LGBTQ-identifying person. While this clarity is useful, this use of Two Spirit is disputed. A survey of Native LGBTQ individuals in Canada found that only 44% identify as Two Spirit (Scheim et al., Citation2013). While we don’t know what percentage of Native LGBTQ people in the United States identify with the term, we suspect similar proportions, because it is a recent term and its use differs with regard to specific tribal teachings and is largely absent in some areas.
Authors of these articles use Two Spirit differently, sometimes employing it as a sexual orientation, a gender identity, or both. Within Two Spirit and distinct tribal communities, differences exist in terms of how this term is understood. While some do, in fact, consider it as a sexual orientation or gender identity, others may see it as a community role, a spiritual identity, or all/none of the above (Jacobs, Citation1997; Walters et al., Citation2006). The very nature of this diversity is important, and one centralized pan-Indian definition could overshadow tribal diversity. With that said, it is important that researchers either clearly define how they use and define the term or ask respondents to qualitatively define it for themselves as Walters et al. did in their 2006 study.
Exemplary study
In Walters et al. (Citation2006) the term Two Spirit is defined in multiple ways by participants themselves. Their definitions include descriptions of Two Spirit that entail intricate and nuanced meanings. For example, Two Spirit as a spiritual identity is evidenced by this quote from one of their respondents:
Being Two-Spirited, kind of goes beyond my sexuality. I am attracted to women, prefer to be with a woman, but it also is more about who I am as a person … there’s a spiritual side to it. (p. 128)
According to another, it is largely a community role:
I just feel like I have this responsibility to community that I have to fulfill and that’s just a part of me. (p. 129)
In their 2018 dissertation project, Jeffries also asked Two Spirit respondents to define Two Spirit identity. In the following quote, Isaiah Brokenleg (Sicangu Lakota) describes winkte, their Lakota Two Spirit way of being, as both a spiritual calling and a community role simultaneously. He says:
The word winkte is actually short for the word (he sounds out) wi-i-inkte, which basically means “talks like a woman” because in Lakota men talk one way and women talk a different way. … Based on what I was taught by my grandparents [it means] that you’re expected to live your life in a good way, and you’re expected to imbue the values of the community, their values and virtues as yours. You are a highly respected member of the community but at the same time, you’re viewed as a leader. In the Indian way, or at least in my culture, leaders lead by example, it’s really more of a servant leadership, so although you might be highly respected, you’re also expected to do whatever you’re asked. If it’s like 3-o’clock in the morning and some says, "come over, my baby is sick, I need you to pray for my baby," then you’re getting up at 3-o’clock in the morning and going over there and praying for someone’s baby who is sick at 3-o’clock in the morning. It’s not like a leadership where you’re sitting on a throne reigning over people. Your job is that you are there to serve the community in the ways that they ask you to, and to live your life in a good way. (Jeffries, Citation2018, p. 204)
Work like that conducted by Walters et al. (Citation2006) provides a foundation for nuanced uses of the term Two Spirit to be connected to concepts of health and wellbeing in a way that does not limit respondents to Westernized categories, making room for individuals like Brokenleg to explore their impacts of their history or social connections on their self-rated health. It also reminds us that Two Spirit, like any word describing sexual orientation or gender identity, should be used only as a term of self-identification, not as a term that is assumed to apply to all Native LGTBQ individuals.
Research framework
The majority of the articles referring to research conducted in the United States draw from a single cross-sectional survey conducted through the HONOR Project. This demonstrates the general lack of information about Two Spirit and Native LGBTQ communities in the United States and the near total absence of accessible datasets that include this population.
None of the studies provided longitudinal data. The absence of longitudinal data prohibits rigorous causal inferences, which could assess how structural determinants of health—for example, loss of a job, loss of housing, family rejection, or migration—impact the self-reported health and identity of Two Spirit and Native LGBTQ individuals. For example, a longitudinal study completed with majority White European trans adolescents found that social transition significantly improved mental health, limiting anxiety and depression to levels comparable to that of their cisgender peers (Durwood et al., Citation2017). Similar studies, which focus on Native LGBTQ communities, are needed to better understand how situational and social factors impact Two Spirit and Native LGBTQ health and wellness.
Exemplary study
Ristock et al. (Citation2010) offers a qualitative evaluation of narratives of migration among Canadian Two Spirit and First Nations LGBTQ individuals. Although this is not a longitudinal study, the research framework, which emphasizes narratives of migration with descriptions of health, self-esteem, and social support before and after migration allows some insight into the effects of movement (from tribal/rural to urban centers, across national borders, etc.) on health. Research on urban Native people and on border towns well demonstrates the fluidity of the notorious urban-reservation divide, and the maintenance of social networks across both spheres, so such narratives may be useful to future researchers, especially if longitudinal data collection is undertaken (Iralu et al., Citation2010; Jeffries, Citation2018; Ramirez, Citation2007).
Limitations
For purposes of conducting this analysis, we limited our sampling method to articles that included health-specific search terms. It is possible that some published articles focus on elements of identity, pride, and connectedness, which directly impact the health of Native Two Spirit and LGBTQ people, may not have been returned given those search terms. This may have led to an increased apparent emphasis on disparities and disease outcomes.
The way in which demographic information is categorically, not holistically, reported creates a second limitation—it is possible certain surveys captured information from at least 10% of LGBTQ people and 10% of Native people, but that these two groups did not overlap (there was not 10% of Two Spirit and Native LGBTQ individuals). If this occurred, that particular study is not in fact relevant to this literature review.
Further, due to both the diversity of research focus as well as the small number of articles included here, our ability to complete more rigorous statistical analyses of these articles—for instance, determining causal relationships between funding streams and research focus—is extremely limited.
Conclusion
Most of the included articles are recent, completed in the last 10 years (2009–2019). This suggests research in Two Spirit and Native LGBTQ populations is increasing, which we see especially with the HONOR Project, a comprehensive and promising dataset still undergoing secondary subset analysis. This makes the findings in this review timely and significant.
In light of the findings above, we would especially like to emphasize the importance of:
appropriate and nuanced use of the term Two Spirit in future research;
comprehensive and diverse inclusion of gender identity and sexual orientation to avoid misclassification of Two Spirit and Native LGBTQ individuals;
appropriate recruitment strategies to fully sample Two Spirit and Native LGBTQ individuals across a variety of demographic strata; and
increased training and support for Native researchers and health professionals.
This last recommendation is especially key, as one component of addressing structural inequalities which lead to the health disparities so commonly enumerated in research centering Native and LGBTQ populations is ensuring that those communities themselves determine the scope and questions of research which concerns them. As Linda Smith writes in Indigenizing the Academy, “To imagine self-determination…. is to imagine a world in which indigenous people become active participants [in research] to prepare for the possibilities and challenges that lay ahead” (Citation1999, p. 124).
We offer this literature review as a foundational point and hope that a similar review, conducted in 10 years, will find not only more complete demographic representation, but also a more robust system of evidence-based programs designed to ensure Two Spirit and Native LGBTQ people have the support they need to achieve health equity.
Ethics Statement
No ethical approval was required for this review.
| Abbreviations | ||
| 2SLGBTQ | = | Two Spirit, Lesbian, gay, bisexual, transgender, queer |
| LGBQ | = | Lesbian, Gay, Bisexual, Queer |
| 2S | = | Two Spirit |
| SO | = | Sexual orientation |
| GI | = | Gender identity |
| T | = | Transgender |
| MSM | = | Men who have sex with men |
| AI/AN | = | American Indian/Alaska Native |
| NA | = | Not applicable |
Acknowledgments
The authors acknowledge the Minority HIV/AIDS Fund from the HHS Office of Infectious Disease and HIV/AIDS Policy within the Office of the Assistant Secretary for Health, which supported this research.
Disclosure statement
The authors report no conflicts of interest.
Additional information
Funding
References
- Choi, S. K., & Meyer, I. H. (2016). LGBT aging: A review of research findings, needs, and policy implications. The Williams Institute. https://williamsinstitute.law.ucla.edu/publications/lgbt-aging/
- DeBruyn, L., Fullerton, L., Satterfield, D., & Frank, M. (2020). Integrating culture and history to promote health and help prevent type 2 diabetes in American Indian/Alaska Native communities: Traditional foods have become a way to talk about health. Prevention of Chronic Diseases, 17, 190–213. https://doi.org/10.5888/pcd17.190213externalicon
- Durwood, L., McLaughlin, K. A., & Olson, K. R. (2017). Mental health and self-worth in socially transitioned transgender youth. Journal of the American Academy of Child & Adolescent Psychiatry, 56(2), 116–123. e112. https://doi.org/10.1016/j.jaac.2016.10.016
- Gates, G. J. (2013). Demographics and LGBT health. Journal of Health & Social Behavior, 54(1), 72–74. https://doi.org/10.1177/0022146512474429
- Grayshield, L., Rutherford, J. J., Salazar, S. B., Mihecoby, A. L., & Luna, L. L. (2015). Understanding and healing historical trauma: The perspectives of Native American elders. Journal of Mental Health Counseling, 37(4), 295–307. https://doi.org/10.17744/mehc.37.4.02
- Herek, G. M., Capitanio, J. P., & Widaman, K. F. (2003). Stigma, social risk, and health policy: Public attitudes toward HIV surveillance policies and the social construction of illness. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 22(5), 533–540. https://doi.org/10.1037/0278-6133.22.5.533
- Huang, Y.-P., Brewster, M. E., Moradi, B., Goodman, M. B., Wiseman, M. C., & Martin, A. (2010). Content analysis of literature about LGB people of color: 1998–2007. The Counseling Psychologist, 38(3), 363–396. https://doi.org/10.1177/0011000009335255
- Indian Health Service Disparities. (2019). Indian Health Service. https://www.ihs.gov/newsroom/factsheets/disparities/
- Jacobs, S. E. (1997). Two-Spirit people: Native American gender identity. Sexuality, and spirituality. University of Illinois Press.
- Jeffries, M. (2018). Whole Indian: Racism, resistance, and (re)membering Turtle Island [Dissertation, Georgia State University]. https://scholarworks.gsu.edu/sociology_diss/110
- Katz-Wise, S. L., Rosario, M., & Tsappis, M. (2016). Lesbian, gay, bisexual, and transgender youth and family acceptance. Pediatric Clinics of North America, 63(6), 1011–1025. https://doi.org/10.1016/j.pcl.2016.07.005
- Norris, T., Vines, P. L., & Hoeffel, E. M. (2012). The American Indian and Alaska Native Population: 2010. 2010 Census Briefs C2010BR-10. US Census.
- Office of Disease Prevention and Health Promotion. (2020). Lesbian, Gay, Bisexual, and Transgender Health Office of Disease Prevention and Health Promotion. https://www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health
- Ramirez, R. (2007). Native hubs: Culture, community, and belonging in Silicon Valley and beyond. Duke University Press.
- Report on the Experiences of American Indian and Alaska Native Respondents. (2015). US Transgender Report: National Center for Transgender Equality. https://transequality.org/sites/default/files/USTS%20AIAN%20Report.pdf
- Sarche, M., & Spicer, P. (2008). Poverty and health disparities for American Indian and Alaska Native children: Current knowledge and future prospects. Annals of the New York Academy of Sciences, 1136, 126–136. https://doi.org/10.1196/annals.1425.017
- Shavers, V. L., Klein, W. M. P., & Fagan, P. (2012). Research on race/ethnicity and health care discrimination: Where we are and where we need to go. American Journal of Public Health, 102(5), 930–932. https://doi.org/10.2105/AJPH.2012.300708
- Smith, L. (1999). Indigenizing the academy. University of Nebraska Press.
- Tester, G., & Wright, E. R. (2017). Older gay men and their support convoys. The Journals of Gerontology. Series B, Psychological Sciences & Social Sciences, 72(3), 488–497. https://doi.org/10.1093/geronb/gbw052.
- Walls, M. L., Whitesell, N. R., Barlow, A., & Sarche, M. (2019). Research with American Indian and Alaska Native populations: Measurement matters. Journal of Ethnicity in Substance Abuse, 18(1), 129–149. https://doi.org/10.1080/15332640.2017.1310640. Epub 2017 Apr 25.
- Walters, K. L., Evans-Campbell, T., Simoni, J. M., Ronquillo, T., & Bhuyan, R. (2006). My spirit in my heart: Identity experiences and challenges among American Indian Two-Spirit women. Journal of Lesbian Studies 10(1–2), 125–149. https://doi.org/10.1300/J155v10n01_07
Appendix A:
Included articles
- Arguello, T. M., & Walters, K. (2018). They tell us “we don't belong in the world and we shouldn't take up a place”: HIV discourse within Two-Spirit communities. Journal of Ethnic & Cultural Diversity in Social Work, 27(2), 107–123. https://doi.org/10.1080/15313204.2017.1362616 <!--${if: isGetFTREnabled}-->
- Balsam, K. F., Huang, B., Fieland, K. C., Simoni, J. M., & Walters, K. L. (2004). Culture, trauma, and wellness: A comparison of heterosexual and lesbian, gay, bisexual, and Two-Spirit Native Americans. Cultural Diversity & Ethnic Minority Psychology, 10(3), 287–301. https://doi.org/10.1037/1099-9809.10.3.287 <!--${if: isGetFTREnabled}-->
- Brotman, S., Ryan, B., Jalbert, Y., & Rowe, B. (2002). Reclaiming space-regaining health. Journal of Gay & Lesbian Social Services, 14(1), 67–87. https://doi.org/10.1300/J041v14n01_04 <!--${if: isGetFTREnabled}-->
- Burks, D. J., Robbins, R., & Durtschi, J. P. (2011). American Indian gay, bisexual and Two-Spirit men: A rapid assessment of HIV/AIDS risk factors, barriers to prevention and culturally-sensitive intervention. Culture, Health & Sexuality, 13(3), 283–298. https://doi.org/10.1080/13691058.2010.525666 <!--${if: isGetFTREnabled}-->
- Cassels, S., Pearson, C. R., Walters, K., Simoni, J. M., & Morris, M. (2010). Sexual partner concurrency and sexual risk among gay, lesbian, bisexual, and transgender American Indian/Alaska natives. Sexually Transmitted Diseases, 37(4), 272–278. https://doi.org/10.1097/OLQ.0b013e3181c37e3e <!--${if: isGetFTREnabled}-->
- Chae, D. H., & Walters, K. L. (2009). Racial discrimination and racial identity attitudes in relation to self-rated health and physical pain and impairment among Two-Spirit American Indians/Alaska natives. American Journal of Public Health, 99(S1), S144–S151. https://doi.org/10.2105/AJPH.2007.126003 <!--${if: isGetFTREnabled}-->
- Evans-Campbell, T., Walters, K. L., Pearson, C. R., & Campbell, C. D. (2012). Indian boarding school experience, substance use, and mental health among urban Two-Spirit American Indian/Alaska natives. The American Journal of Drug and Alcohol Abuse, 38(5), 421–427. https://doi.org/10.3109/00952990.2012.701358 <!--${if: isGetFTREnabled}-->
- Fieland, K. C., Walters, K. L., & Simoni, J. M. (2007). Determinants of health among Two-Spirit American Indians and Alaska natives. In I. H. Meyer, & M. E. Northridge (Eds.), The health of sexual minorities. Springer. https://doi.org/10.1007/978-0-387-31334-4_11 <!--${if: isGetFTREnabled}-->
- Iralu, J., Duran, B., Pearson, C. R., Jiang, Y., Foley, K., Harrison, M. (2010). Risk factors for HIV disease progression in a rural southwest American Indian population. Public Health Reports (1974–), 125–143. http://proxy.library.tamu.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=edsjsr&AN=edsjsr.41434919&site=eds-live <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 web Risk+factors+for+HIV+disease+progression+in+a+rural+southwest+American+Indian+population author%3DJ.+Iralu%26author%3DB.+Duran%26author%3DC.+R.+Pearson%26author%3DY.+Jiang%26author%3DK.+Foley%26author%3DM.+Harrison 2010 Iralu%2C+J.%2C+Duran%2C+B.%2C+Pearson%2C+C.+R.%2C+Jiang%2C+Y.%2C+Foley%2C+K.%2C+Harrison%2C+M.+%282010%29.+Risk+factors+for+HIV+disease+progression+in+a+rural+southwest+American+Indian+population.+Public+Health+Reports+%281974%E2%80%93%29%2C+125%E2%80%93143.+ %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_5_1_3_9_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dweb%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DIralu%26rft.aufirst%3DJ.%26rft.date%3D2010%26rft.atitle%3DRisk%2520factors%2520for%2520HIV%2520disease%2520progression%2520in%2520a%2520rural%2520southwest%2520American%2520Indian%2520population%26rft.spage%3D125%26rft.epage%3D143 %00empty%00}-->
- Johnson-Jennings, M., Belcourt, A., Town, M., Walls, M. L., & Walters, K. L. (2014). Racial discrimination's influence on smoking rates among American Indian Alaska native Two-Spirit individuals: Does pain play a role? Journal of Health Care for the Poor and Underserved, 25(4), 1667–1678. https://doi.org/10.1353/hpu.2014.0193 <!--${if: isGetFTREnabled}-->
- Lehavot, K., Walters, K. L., & Simoni, J. M. (2009). Abuse, mastery and health among lesbian, bisexual and Two-Spirit American Indian and Alaska native women. Cultural Diversity Ethnic Minor Psychology, 15(3). https://doi.org/10.1037/a0013458 <!--${if: isGetFTREnabled}-->
- Logie, C. H., Lys, C. L., Fujioka, J., MacNeill, N., Mackay, K., & Yasseen, A. S. III (2019). Sexual practices and condom use among a sample of Northern and Indigenous adolescents in northern Canada: Cross-sectional survey results. BMJ Sexual & Reproductive Health, 45(2), 147–154. https://doi.org/10.1136/bmjsrh-2018-200174 <!--${if: isGetFTREnabled}-->
- Logie, C. H., Lys, C. L., Mackay, K., MacNeill, N., Pauchulo, A., & Yasseen, A. S. I. I. I. (2019). Syndemic factors associated with safer sex efficacy among Northern and Indigenous adolescents in Arctic Canada. International Journal of Behavioral Medicine, 26(4), 449–453. https://doi.org/10.1007/s12529-019-09797-0 <!--${if: isGetFTREnabled}-->
- Logie, C. H., & Lys, C. (2015). The process of developing a community-based research agenda with lesbian, gay, bisexual, transgender and queer youth in the Northwest Territories. International Journal of Circumpolar Health, 74(1), 28188. https://doi.org/10.3402/ijch.v74.28188 <!--${if: isGetFTREnabled}-->
- Lyons, T., Shannon, K., Pierre, L., Small, W., Krüsi, A., & Kerr, T. (2015). A qualitative study of transgender individuals' experiences in residential addiction treatment settings: Stigma and inclusivity. Substance Abuse Treatment, Prevention, and Policy, 10, 17. https://doi.org/10.1186/s13011-015-0015-4 <!--${if: isGetFTREnabled}-->
- Newman, P. A., Woodford, M. R., & Logie, C. (2012). HIV vaccine acceptability and culturally appropriate dissemination among sexually diverse aboriginal peoples in Canada. Global Public Health, 7(1), 87–100. https://doi.org/10.1080/17441692.2010.549139 <!--${if: isGetFTREnabled}-->
- Pearson, C. R., Walters, K. L., Simoni, J. M., Beltran, R., & Nelson, M. K. (2013). A cautionary tale: Risk reduction strategies among urban American Indian/Alaska Native men who have sex with men. AIDS Education and Prevention: Official Publication of the International Society for AIDS Education, 25(1), 25–37. https://doi.org/10.1521/aeap.2013.25.1.25 <!--${if: isGetFTREnabled}-->
- Ristock, J., Zoccole, A., & Passante, L. (2010). Aboriginal Two-Spirit and LGBTQ migration, mobility, and health research project: Final report. University of Manitoba. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 book Aboriginal+Two-Spirit+and+LGBTQ+migration%2C+mobility%2C+and+health+research+project%3A+Final+report author%3DJ.+Ristock%26author%3DA.+Zoccole%26author%3DL.+Passante 2010 Ristock%2C+J.%2C+Zoccole%2C+A.%2C+%26+Passante%2C+L.+%282010%29.+Aboriginal+Two-Spirit+and+LGBTQ+migration%2C+mobility%2C+and+health+research+project%3A+Final+report.+University+of+Manitoba. %00empty%00 %00null%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_5_1_3_18_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dbook%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DRistock%26rft.aufirst%3DJ.%26rft.date%3D2010%26rft.btitle%3DAboriginal%2520Two-Spirit%2520and%2520LGBTQ%2520migration%252C%2520mobility%252C%2520and%2520health%2520research%2520project%253A%2520Final%2520report%26rft.pub%3DUniversity%2520of%2520Manitoba %00empty%00}-->
- Ryan, B., Brotman, S., & Rowe, B. (2000). Access to care: Exploring the health and well-being of gay, lesbian, bisexual, and Two-Spirit people in Canada. McGill Centre for Applied Family Studies. <!--${if: isGetFTREnabled}--><!--${/if:}--> <!--${ifNot: isGetFTREnabled}--><!--${/ifNot:}--><!--${if: isGetFTREnabled}--><!--${/if:}--><!--${googleScholarLinkReplacer: %00empty%00 book Access+to+care%3A+Exploring+the+health+and+well-being+of+gay%2C+lesbian%2C+bisexual%2C+and+Two-Spirit+people+in+Canada author%3DB.+Ryan%26author%3DS.+Brotman%26author%3DB.+Rowe 2000 Ryan%2C+B.%2C+Brotman%2C+S.%2C+%26+Rowe%2C+B.+%282000%29.+Access+to+care%3A+Exploring+the+health+and+well-being+of+gay%2C+lesbian%2C+bisexual%2C+and+Two-Spirit+people+in+Canada.+McGill+Centre+for+Applied+Family+Studies. %00empty%00 %00null%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 %00empty%00 getFTREnabled FULL_TEXT %00empty%00}--><!--${sfxLinkReplacer: e_1_3_5_1_3_19_1 %00empty%00 url_ver%3DZ39.88-2004%26rft.genre%3Dbook%26rfr_id%3Dinfo%3Asid%2Fliteratum%253Atandf%26rft.aulast%3DRyan%26rft.aufirst%3DB.%26rft.date%3D2000%26rft.btitle%3DAccess%2520to%2520care%253A%2520Exploring%2520the%2520health%2520and%2520well-being%2520of%2520gay%252C%2520lesbian%252C%2520bisexual%252C%2520and%2520Two-Spirit%2520people%2520in%2520Canada%26rft.pub%3DMcGill%2520Centre%2520for%2520Applied%2520Family%2520Studies %00empty%00}-->
- Saewyc, E. M., Skay, C. L., Bearinger, L. H., Blum, R. W., & Resnick, M. D. (1998). Sexual orientation, sexual behaviors, and pregnancy among American Indian adolescents. Journal of Adolescent Health, 23(4), 238–247. https://doi.org/10.1016/S1054-139X(98)00016-0 <!--${if: isGetFTREnabled}-->
- Scheim, A. I., Jackson, R., James, L., Dopler, T. S., Pyne, J., & Bauer, G. R. (2013). Barriers to well-being for aboriginal gender-diverse people: Results from the trans PULSE project in Ontario. Ethnicity and Inequalities in Health and Social Care, 6(4), 108–120. https://doi.org/10.1108/EIHSC-08-2013-0010 <!--${if: isGetFTREnabled}-->
- Simoni, J. M., Walters, K. L., Balsam, K. F., & Meyers, S. B. (2006). Victimization, substance use, and HIV risk behaviors among gay/bisexual/Two-Spirit and heterosexual American Indian men in New York City. American Journal of Public Health, 96(12), 2240–2245. https://doi.org/10.2105/AJPH.2004.054056 <!--${if: isGetFTREnabled}-->
- Town, M. A., Walters, K. L., & Orellana, E. R. (2021). Discriminatory distress, HIV risk behavior, and community participation among American Indian/Alaska native men who have sex with men. Ethnicity & Health, 26(5), 646–658. 557858.2018.1557115 https://doi.org/10.1080/13 <!--${if: isGetFTREnabled}-->
- Walters, K. L. (1997). Urban lesbian and gay American Indian identity: Implications for mental health service delivery. Journal of Gay and Lesbian Social Services, 6(2). https://doi.org/10.1300/J041v06n02_05 <!--${if: isGetFTREnabled}-->
- Walters, K. L., Horwath, P. F., & Simoni, J. M. (2001). Sexual orientation bias experiences and service needs of gay, lesbian, bisexual, transgendered, and Two-Spirited American Indians. Journal of Gay & Lesbian Social Services, 13(1–2), 133–149. https://doi.org/10.1300/J041v13n01_10 <!--${if: isGetFTREnabled}-->
- Willging, C. E., Israel, T., Ley, D., Trott, E. M., DeMaria, C., Joplin, A., & Smiley, V. (2016). Coaching mental health peer advocates for rural LGBTQ people. Journal of Gay & Lesbian Mental Health, 20(3), 214–236. https://doi.org/10.1080/19359705.2016.1166469 <!--${if: isGetFTREnabled}-->
- Yuan, N. P., Duran, B. M., Walters, K. L., Pearson, C. R., & Evans, T. A. (2014). Alcohol misuse and associations with childhood maltreatment and out-of-home placement among urban Two-Spirit American Indian and Alaska Native people. International Journal of Environmental Research and Public Health, 11(10), 10461–10479. https://doi.org/10.3390/ijerph1010461 <!--${if: isGetFTREnabled}-->
