
Abstract
Introduction: Research into disordered eating in men paints a mixed picture regarding the relationship to sexual orientation and muscularity. Method: Participants completed the Eating Disorder Examination Questionnaire 6.0 and Drive for Muscularity scale via Qualtrics. Results: Gay men experience more symptoms related to body attitudes and shape and weight concerns. Heterosexual men experience more muscularity and restricting related symptoms. Bisexual men generally score lower than the other groups, so should be considered independently. Conclusion: Sexual orientation relates to both rates of eating disorders in men and also the kind of symptoms they experience. This should be taken into account in treatment and diagnostic approaches.
Introduction
Eating disorders (EDs) are serious psychiatric conditions with high mortality (5.9%) (Smink et al., Citation2012) and relapse (11–30%) (Fairburn et al., Citation2000) rates. The DSM V specifies that anorexia nervosa involves a restriction of energy intake, intense fear of gaining weight, and a disturbance in how body shape/weight are experienced (APA, Citation2013). Historically, EDs are associated with young, thin, heterosexual, white women (NEDA, Citation2016) and research investigating ED etiology in other groups, including men and sexual orientation minorities, is lacking despite men making up at least one in four diagnosed cases (Cohn et al., Citation2016). Much of the prior research in EDs has excluded men, considering them atypical despite EDs being reported in men for as long as they have been reported in women (Murray et al., Citation2017). Tools used in ED research and for clinical ED assessment have typically been developed in female samples, and their use has not always been validated in male participants (Carey et al., Citation2019; Lavender et al., Citation2010). Alongside such inappropriate measures, much of the previous research that has focused on men is also limited by the use of small sample sizes (Smith et al., Citation2017). This bias in reporting and researching male EDs is reflected in the many anecdotal experiences of men who do receive a diagnosis, reporting that they feel invisible because EDs are seen as a “female problem” (Robinson et al., Citation2013).
Although clinical EDs are thought to present with similar symptoms for men and women (Feldman & Meyer, Citation2007), significant differences have been identified between genders in community samples. For example, men generally score lower on all attitudinal aspects of ED symptomatology compared to women (Lavender et al., Citation2010; Carey et al., Citation2019). This difference in prevalence of ED symptomatology may represent a qualitative difference in the way that men and women interpret assessment questions rather than a quantitative difference (Smith et al., Citation2017; Carey et al., Citation2019). It is not surprising that common ED assessment tools do not fully capture the male symptomology due to these measures being developed in women, and the majority not having been adapted for more current DSM ED diagnoses, such as binge eating disorder (Smith et al., Citation2017; Carey et al., Citation2019; Murray et al., Citation2016). Understanding and addressing body-related disorders in men requires the ability to correctly identify its presence, which calls for more accurate, validated measures (Talbot et al., Citation2019).
A key symptom thought to be of increased importance for men in evaluating male attractiveness, is drive for muscularity (Duggan & McCreary, Citation2004; Murray et al., Citation2017). The internalization of muscularity as well as thinness ideals are associated with body dissatisfaction and eating concerns in men (Klimek et al., Citation2018). Muscle dysmorphia (misestimation of own muscularity) is considered to be the male equivalent of body size overestimation, which is frequently linked to EDs in women (Boehm et al., Citation2016; Slade & Russell, Citation1973; Keizer et al., Citation2013). Both the drive for muscularity and the drive for thinness are relevant in eating disorders, particularly in men (Klimek et al., Citation2018). Research indicates that men who internalize the muscular ideal have a higher level of drive for muscularity when they do not internalize the thin ideal; however, the internalization of both together is considered as most relevant to men developing eating disorders (Klimek et al., Citation2018).
A specific factor thought to mediate vulnerability to EDs in men is sexual orientation (Feldman & Meyer, Citation2007; Morrison et al., Citation2004). Although being gay and male is not in itself predictive of developing an ED, being in a sexual minority group seems to be an indication of increased risk (Strother et al., Citation2012; Calzo et al., Citation2017). Gay men report higher overall levels of body dissatisfaction and display more negative, thinness-oriented eating attitudes and behaviors compared to heterosexual men (Duggan & McCreary, Citation2004), demonstrating equivalent concern for physical attractiveness as heterosexual women (Harvey & Robinson, Citation2003). Men identifying as gay are less satisfied with their bodies and show more distress about body dissatisfaction compared to heterosexual men (Harvey & Robinson, Citation2003). Gay men have a greater risk of a range of disordered eating behaviors, including binge eating, purging, restrictive dieting, steroid misuse, and using diet pills (Murray et al., Citation2017).
Body dissatisfaction in gay men specifically may be linked to the experiences of living in a heteronormative society, and the stigma that comes along with this (Brennan, Crath, Hart, Gadalla & Gillis, Citation2011). Gay subculture seems to value attractiveness especially highly, such that concerns about the body are particularly salient for gay men (Drummond, Citation2005; Citation2010). Unlike women, who it is suggested primarily experience pressure to a thin ideal, gay men experience a pressure to be simultaneously lean (devoid of fat) and muscular (Drummond, Citation2005; Citation2010). Physical power and prowess, and thus muscularity, are seen as vitally important in our conception of masculinity in general, however some suggest that muscularity serves a different purpose for gay men. Muscularity for gay men does not just relate to dominance or the ability to physically overpower, but is increasingly related to attractiveness and the ability to form relationships with sexual partners, as well as having access to the social capital that it confers (Drummond, Citation2005; Citation2010; Brennan, Craig & Thompson, Citation2012). Although it may also be a way to reject femininity and demonstrate masculinity, given the way that being gay is conflated with femininity (Brennan et al., Citation2011). Drummond (Citation2005) also highlights the possibility of “protest muscularity,” that which demonstrates physical health and virility against the stigma related to with the frailer bodies associated with HIV/AIDS, something that gay men have borne the brunt of. However, given the changing health landscape, this may not have such a big influence at present. If muscularity has become the normative body for men in general, gay and bisexual men might attempt to develop this kind of body to display masculinity, in order to counteract possible homophobia (Tiggemann et al., Citation2007). The attempt to look a certain way to avoid negative experience linked to stigma and homophobia, could in itself have a damaging impact on the individual’s health, given that it is related to depression and experiences of disordered eating (Brennan et al., Citation2012; Blashill, Citation2010).
The experience of body dissatisfaction may manifest as drive for muscularity in gay and bisexual men, particularly given that muscularity is privileged in gay culture (Brennan et al., Citation2012). It is suggested that as well as helping gay men to access the spaces and benefits of belonging to this group by conforming to group norms, alongside the way in which masculinity is objectified via muscularity, being muscular also enables gay men to attract a partner of at least equal level of desirability (Swami & Tovée, Citation2008). It should be noted that on occasions, due to the possible complexities of recruiting a specific sample, research in the area sometimes uses samples from the same place repeatedly (such as Brennan et al.’s recruitment in the 2008 Toronto LGBT festival). This could limit the generalizability of these claims, and reminds us of the importance of recruiting diverse samples (Filiault & Drummond, Citation2009).
Most studies examining the influence of sexual orientation in ED psychopathology focus primarily on being gay. Gay men in particular may experience similar pressures to women in terms of being physically attractive due to the male preference for attractive partners (Siever, Citation1994; Legenbauer et al., Citation2009; Lippa, Citation2007). Preliminary research suggests that bisexual men are also at risk for eating disorders when compared to heterosexual men (Feldman & Meyer, Citation2007). One explanation for this is that both gay and bisexual men aim to sexually attract men, which may put them under the same body image pressures as heterosexual women (Hatfield & Sprecher, Citation1986; Siever, Citation1994; Duggan & McCreary, Citation2004). Empirical support for this idea comes from a study suggesting that lesbians were the least concerned about physical attractiveness, whereas gay men and heterosexual women showed the highest concern for physical attractiveness (Siever, Citation1994). The authors concluded that heterosexual men and lesbian women may be less concerned about physical attractiveness due to a lack of pressure to sexually attract men, and thus are less dissatisfied with their bodies (Siever, Citation1994).
Men who identify as bisexual are often not included in the research that focuses on eating disorders and sexuality (Russell & Keel, Citation2002), either being excluded because of small sample sizes (Duggan & McCreary, Citation2004) or being considered as a single group with gay men (Gigi et al., Citation2016; Brown & Keel, Citation2015). There is little empirical justification available for grouping gay and bisexual men together in one heterogeneous group. Therefore, it is important that research going forward considers how bisexual men experience disordered eating and in what ways this may differ from men of other sexualities. Further exploration of how bisexual men experience eating disorders may also enable a fuller understanding of how sexuality itself influences these symptoms. The majority of research focuses on gay or heterosexual men’s experiences, so the inclusion of bisexual men will allow a more detailed picture of the link between sexual orientation and eating disorders, given that bisexual men may be trying to attract people of multiple genders instead of just one.
This study aimed to explore whether identifying as gay, bisexual, or heterosexual is related to prevalence of ED symptoms and drive for muscularity attitudes in a community sample of men. We examined the appropriateness of the standard EDE-Q as a measure of male disordered eating by testing model fit in a large community sample. Our previous research suggests that a three-factor assessment is more suitable for men compared to the original 22-item four-factor structure (Carey et al., Citation2019). Therefore, we predicted that the original four-factor structure would be a poor fit for male responses, whereas the three-factor model will be more appropriate. We then examined, through measurement invariance analysis, whether there is evidence that the EDE-Q is measuring equivalent constructs for men of different sexualities. We consider the prevalence of attitudes and behaviors relating to disordered eating and drive for muscularity in gay, bisexual, and heterosexual men. The majority of previous research has focused on either muscularity or ED attitudes, and has not considered bisexual men as a group in their own right. Because of the pressures on physical appearance for attracting men and the increased pressure to conform to masculine muscular ideals, we predicted that both gay and bisexual men would show greater prevalence of ED related attitudes compared to heterosexual men across all measures. Finally, we examined how drive for muscularity and sexual orientation interact in relation to disordered eating attitudes and behaviors. We predict that drive for muscularity in gay and bisexual men, who are aiming to attract other men, may have a stronger link to restrictive and eating behaviors compared to drive for muscularity in heterosexual men.
Methods
Participants
Participants were recruited via local community groups, university societies, social media, and online/print advertising. Responses were received from 185 bisexual men, 230 gay men, and 203 heterosexual men. Age and Body Mass Index (BMI) of participants can be found in . 43 participants chose not to disclose their height and weight for BMI calculation, meaning we had BMI information from 93.04% of participants. Men were identified as White (N = 381), Hispanic (N = 3), Black (N = 5), Asian (N = 31), and other (N = 20). The study gained ethical approval from the departmental ethics board.
Table 1. Demographic information for participants in the study.
Measures
Eating disorder examination questionnaire (EDE-Q) 6.0
The EDE-Q is a 28-item self-report questionnaire that assesses eating disorder symptoms (Fairburn & Beglin, Citation1994; Citation2008). It assesses disordered eating behaviors and attitudes in the last 28 days and has four subscales (Restraint, Eating Concern, Shape Concern, Weight Concern) as well as a global score, which is calculated from the averages of the four subscale scores. Participants rate items on a seven-point Likert scale, with higher scores indicating higher eating disorder psychopathology. There are six items that relate to the frequency of eating disorder attitudes and behaviors in the past 28 days, which do not contribute to the subscale or global scores but provide information on some eating disorder behaviors such as laxative use and self-induced vomiting. Research has established acceptable levels of internal consistency for global and subscale scores in men and women, alongside the reliability of the scale (Berg et al., Citation2011; Peterson et al., Citation2007; Lavender et al., Citation2010; Rose et al., Citation2013; Hilbert et al., Citation2012). Traditionally the EDE-Q uses a three-factor structure, but our previous research suggests that a brief, 16-item, three factor assessment is more suitable for men compared to the original 22-item four factor structure (Carey et al., Citation2019). This model includes a factor around restricting (restriction), one about worries around one’s body shape and weight (shape and weight concern), and finally a factor focused on how much an individual is worried about and preoccupied by their eating (Preoccupation and Eating Concern).
Drive for muscularity scale (DMS)
The DMS is a 15-item self-report questionnaire that assesses how important being muscular is to participants, and how they act to develop their muscularity. Participants answer each item on a five-point Likert scale anchored by “Always” and “Never.” The scale uses reverse-scoring on all items. Higher scores indicate higher drive for muscularity. In men, the DMS can give muscularity-driven behaviors and muscularity-oriented body image attitude scores individually, as well as an overall drive for muscularity score. The item has shown acceptable reliability and validity in male samples (McCreary, Citation2007).
Procedure
Participants were invited to take part through social media adverts, adverts posted through local community groups, and adverts in Attitude magazine. Participants followed a link to an online questionnaire, delivered via Qualtrics software (Qualtrics, Provo, UT). The questionnaire included demographic information (age, gender, sexual orientation, and ethnicity), followed each time by the EDE-Q and then the DMS. The survey took approximately 20 minutes to complete. Height and weight were also voluntarily self-reported (not forced entry) in order to calculate BMI. The questionnaires were presented in a way that meant participants could not skip past questions in an effort to limit missing data.
Data analysis
A Confirmatory factor analysis (CFA) was conducted using RStudio software, to assess the goodness of fit for the factor structure in the full sample. A model may be regarded as an acceptable fit if the Goodness of Fit Index (GFI), Normed Fit Index (NFI) and Comparative Fit Index (CFI) are all above .90; if the Adjusted Goodness of Fit Index (AGFI) is above .80 (Byrne, Citation1994), and if the Root Mean Square Error of Approximation (RMSEA) is below .10 (Browne & Cudeck, Citation1993). If the chi square test is not significant then the model can be accepted, although there are problems with chi square statistics in larger samples. We also calculated measurement invariance between sexual orientation groups, to explore if the factor structure was the same across sexualities. For this we used the criteria of a less than .01 change in CFI to signify measurement invariance (Cheung & Rensvold, Citation2002). Any items found to be invariant were then omitted from subsequent analysis.
In order to examine the relationship between sexual orientation and ED symptomatology we first conducted a MANOVA, to consider the impact of multiple sexualities on multiple components simultaneously and thereby control for Type II error. The independent variable was sexual orientation (bisexual, gay, or heterosexual). The dependent variables were the individual EDE-Q subscale scores (preoccupation and eating concern, shape and weight concern, restraint, and global score). Significant differences identified in the MANOVA were then followed up with separate ANOVAs examining the effect of sexual orientation on each of the subscales and global scores separately.
Multiple moderated regression was subsequently carried out for each EDE-Q sub-component identified as significantly different between sexual orientation groups, in order to explore whether drive for muscularity moderates the relationship between sexual orientation and eating disorder symptoms. In separate hierarchical regressions, we used EDE-Q score (global or sub-component) as the outcome variable, with BMI and age entered as control or nuisance variables (Step 1), followed by sexual orientation and drive for muscularity as our main predictor variables of interest (Step 2), and finally the interaction between these two predictor variables (Step 3). Significant interactions were followed up by comparing each sexual orientation in terms of the relationship (correlation coefficient using Fisher’s Z transformation) between drive for muscularity and eating disorder symptomology, in a pairwise manner applying a Bonferroni correction for multiple comparisons. Following the results of the measurement invariance testing, follow up ANOVAs were carried out on EDE-Q subscales without the items that were shown to be variant.
Results
Confirmatory factor analysis
We conducted CFA on the traditional four-factor model of the EDE-Q, and found that this was not a good fit based on accepted thresholds. We then conducted a CFA on the more recent three-factor model, and found this to be an acceptable fit for this data. This model includes a factor around restricting (restriction), one about worries around one’s body shape and weight (Shape and Weight Concern), and finally a factor focused on how much an individual is worried about and preoccupied by their eating (Preoccupation and Eating Concern). Based on these acceptable fit indices, we used the three-factor model in all future analysis. Further details on these analyses can be found in the supplementary data.
Measurement invariance
We carried out measurement invariance analysis to consider whether the items of the EDE-Q contributed in the same way to each scale across the sexual orientation groups. Results indicate that the scale is invariant across groups up to the residuals level, where there is variance. Based on this, we removed certain items from subsequent analysis. Further details about this analysis can be found in the supplementary data.
Eating disorder examination questionnaire (EDE-Q) scores
Global score
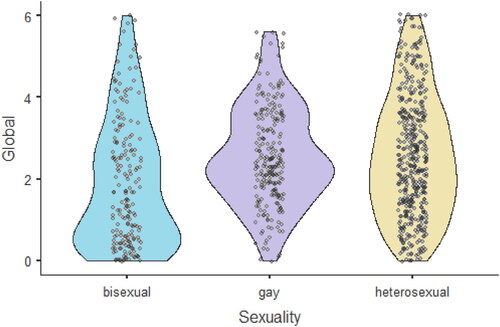
We ran ANOVAs without the items shown to be variant at the residuals level. A one-way ANOVA showed a significant difference in global scores between sexual orientation groups (F(2,636) = 14.96, p < .001). shows the pattern of results. Bonferroni post-hoc tests revealed that bisexual men scored the lowest on this subscale (p < .001) whereas there was no difference between gay and heterosexual men (p = 1.00). This scale is an aggregate of the three other scales, so gives information on overall disordered eating thoughts and behaviors, indicating that bisexual men showed the lowest disordered eating thoughts and behaviors in general.
Figure 1. A figure showing the results of ANOVAs for Global EDE-Q score and each subscale score, respectively.
Preoccupation and eating concern (PEC)
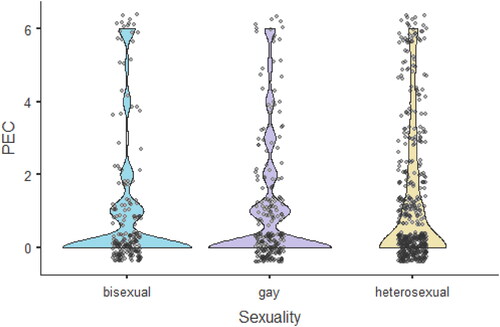
A one-way ANOVA did not show a significant difference in PEC scores between groups (F(2,636) = 2.61, p < .074) (). PEC scores relate to how concerned an individual is with what and how they eat, as well as whether they are seen eating by other people, and these results indicate that gay, bisexual, and heterosexual men experience similar rates of these thoughts and behaviors.
Figure 2. ANOVA results for PEC score. There were no significant differences between groups.
Shape and weight concern (SWC)
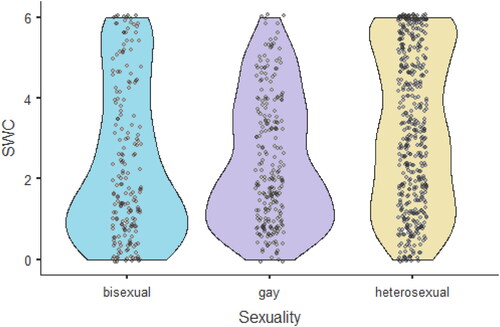
A one-way ANOVA showed a significant difference in SWC scores between groups (F(2,636) = 19.28, p < .001). shows the pattern of results. Bonferroni post-hoc tests showed that heterosexual men scored the highest on this subscale (p < .001) but there were no differences between bisexual and gay men (p = 1.00). This indicates that heterosexual men engage in more behaviors related to changing and monitoring their body shape and weight than gay and bisexual men.
Figure 3. ANOVA results for SWC score. Heterosexual men had higher scores compared to both gay and bisexual men.
Restriction
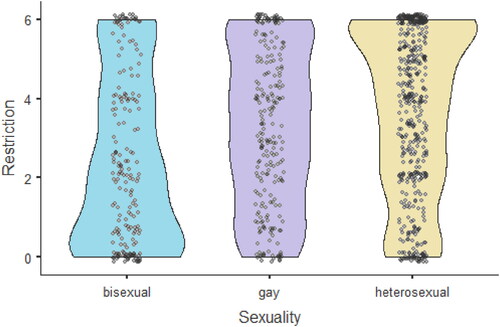
A one-way ANOVA showed a significant difference in restriction scores between groups (F(2,636) = 39.02, p < .001) (see ). Bonferroni post-hoc tests showed that scores in each group were significantly different from each other (p < .001). This indicates that heterosexual men engage more in behaviors around limiting and controlling their diet than gay men, but gay men engage more in these behaviors than bisexual men.
Figure 4. ANOVA results for restriction score. Heterosexual men had the highest score for restriction subscale, followed by gay men with bisexual men having the lowest scores.
Regression
Four, three-stage hierarchical moderated multiple regressions were carried out with Global EDE-Q score, PEC, SWC and restriction as dependent variables, respectively, following the removal of variant items.
Global score
For the moderated multiple regression with Global score as the dependent variable (see ) BMI and age were added at stage one of the regression as noise variables. The model was not significant, neither age nor BMI contributed significantly to the global EDE-Q score. Sexual orientation and DMS score were entered at stage two, explaining an additional 2.2% of variation. The model was significant; however, only sexual orientation significantly contributed to this. The interaction between sexual orientation and DMS score was added at stage three, explaining an additional 0.1% of the variance. The model was significant with only sexual orientation identified as a significant predictor.
Table 2. Results of a moderated hierarchical regression of global scores.
SWC
For the moderated multiple regression with SWC score as the dependent variable (see ). BMI and age were added at stage one of the regressions as noise variables. The model was not significant, although age was identified as a significant predictor to SWC. Sexual orientation and DMS scores were entered at stage two, explaining an additional 5.2% of variation in SWC. The model was significant and both sexual orientation and DMS score significantly contributed to this. The interaction between sexual orientation and DMS score was added at stage three which did not explain any additional variance. The model was significant, with sexual orientation and DMS as significant predictors.
Table 3. Results of a moderated hierarchical regression of SWC subscale scores.
PEC
For the moderated multiple regression with PEC score as the dependent variable (see ) at stage one, BMI and age were added as noise variables. The model was not significant and neither BMI nor age contributed significantly to PEC score. Sexual orientation and DMS score were entered at stage two explaining an additional 1.3% of the variance. The model was significant but only DMS score was a significant predictor. The interaction between sexual orientation and DMS score was added at stage three, which did not explain any additional variance. The model was significant, with DMS as the only significant predictor.
Table 4. Results of a moderated hierarchical regression of PEC subscale scores.
Restriction
For the model with restriction as the dependent variable (see ), BMI and age were added at stage one as noise variables and explained 0.3% of the variance in restraint scores, but neither were significant predictors. At stage two sexual orientation and DMS scores were added, explaining an additional 17.5% of the variance in Restriction, with age, sexual orientation, and DMS scores all as significant predictors. At stage three the interaction between DMS score and sexual orientation was added, which explained an additional 0.7% of the variance, representing a significant change in R2. At stage three, age, sexual orientation, DMS, and the interaction were all significant predictors.
Table 5. Results of a moderated hierarchical regression of restraint subscale scores, where the interaction is sexual orientation x drive for muscularity.
The significant interaction between DSM and sexual orientation on restriction scores was further examined by calculating and comparing correlations between DMS and restraint scores for each sexual orientation. Restriction and DMS scores were significantly correlated for bisexual men (r = 0.38, p < .001) and gay men (r = 0.21, p = .001), with increased drive for muscularity being related to greater Restriction, however, there was no such correlation in heterosexual men (r = 0.08, p = .285). Pairwise comparison of these correlation coefficients indicated that bisexual and heterosexual men were significantly different (z = 3.12, p = .002), while the correlations were not significantly different for gay and heterosexual men (z = 1.37, p = .170), or bisexual and gay men (z = 1.88, p = .060); however, the non-significant difference between bisexual and gay men indicated a possible tendency for these two groups to differ in terms of the magnitude of the relationship between drive for muscularity and restriction (p < .10).
Discussion
This study aimed to examine how eating disorder symptoms differ in men of different sexual orientations. In doing so, we set out specifically to examine disordered eating behavior in two under-represented populations: namely, (i) men and (ii) sexual minorities—especially bisexual men who are often neglected or specifically excluded from eating disorder research (Bankoff et al., Citation2016). Additionally, we investigated how eating disorder symptoms in men with different sexual orientations might be related to the desire for a muscular physique. We aimed to provide novel insight into the varying reasons that underlie men of different sexual orientations developing eating disorder symptoms. In a large sample of gay, bisexual, and heterosexual men, we found significant differences in self-reported eating disorder behavior and the contribution of drive for muscularity across groups. We also confirmed previous findings suggesting that eating disorder symptoms in men are best described by a three-factor (component) structure (Carey et al., Citation2019). However, this may not be suitable for men of all sexualities, as can be seen by our measurement invariance analysis results indicating we should omit many items.
Our CFA of the EDE-Q supported the recently proposed three-factor model of Carey et al. (Citation2019), with above acceptable fit levels found for all groups in the current data. This supports the idea that the three-factor model of the EDE-Q (combining shape and weight concern into a single factor) is useful for assessing men’s eating disorder symptoms and attitudes, whereas the traditional four-factor model might not be suitable for measuring these traits in men. For this reason, we used the three-factor model for all subsequent analysis. Measurement invariance analysis further indicated a difference in how participants responded to the questions based on their sexual orientation, indicating that the way men interpret and respond to the questions within the EDE-Q may differ depending on their sexual orientation.
We found that gay men showed the highest levels of eating disorder symptoms, specifically global scores, preoccupation and eating concern, and shape and weight concern. By contrast, bisexual men had some of the lowest eating disorder symptom scores, but often scored similarly to heterosexual men. Heterosexual men scored the highest for the restricting subscale only. This pattern of results was confirmed by sexual orientation being a significant predictor, either by itself or as part of an interaction with drive for muscularity, for every regression model. In addition, gay men reported the highest instances of bingeing, purging and excessive exercise, while heterosexual men also reported high levels of regular excessive exercise.
Drive for muscularity was a significant predictor of eating disorder symptoms; its impact on eating disorder symptoms depended on sexual orientation. Drive for muscularity was associated with greater global scores but not dietary restricting in heterosexual men. Conversely, for gay men drive for muscularity was associated with dietary restricting but not global scores. For bisexual men, a greater drive for muscularity was associated with both increased restricting and global scores, despite the fact that this group has the lowest levels of symptoms overall. It seems that for heterosexual men, muscularity affects general attitudes to their bodies and foods, whereas for gay men muscularity is specifically related to restricting behaviors. For bisexual men, muscularity seems to influence both attitudes to their bodies and eating as well as restricting behaviors. This complex interaction between sexual orientation, drive for muscularity, and eating/dieting behaviors may explain the very mixed results in the literature. For example, there are mixed results regarding how sexual orientation is related to experiences of eating disorder symptoms, with some saying gay men specifically focus on thinness as opposed for muscularity, and others suggesting that all men suffer from the consequences of high drive for muscularity (Carlat et al., Citation1997; Duggan & McCreary, Citation2004; Murray et al., Citation2017). It may also be that the way in which drive for muscularity influences ED symptoms are linked to the kind of ED symptoms being measured as well as the sexual orientation of the participants.
Measurement invariance analysis indicates that some items of the EDE-Q are variant at the level of the residuals (errors). Based on this, we isolated those items that showed variance and re-ran the ANOVAs and multiple moderated regressions without these items included. This somewhat changed the pattern of results (see supplementary material for analysis without the items removed). The small amount of variance in shape and weight concern that our model explained remained significantly predicted by sexual orientation and drive for muscularity; however, sexual orientation becomes the key predictor for global score and drive for muscularity the key predictor for how preoccupied participants were with eating. When variant items were omitted, there were no differences between gay and heterosexual participants’ scores on the global score, but bisexual men continued to score the lowest on this scale. For the preoccupation and eating concern, no significant differences were found once variant items were removed. For shape and weight concern, heterosexual men became the highest scoring after variant items were removed. As these differences were found solely at the level of the residuals, it may not be necessary to completely remove these items from analysis. It could be sufficient to simply be aware that error terms for these items are likely to be bigger than for other items.
Often, bisexual men are grouped with gay men when examining eating disorder symptoms (e.g., Carlat et al., Citation1997; Austin et al., Citation2004; Bankoff et al., Citation2016). However, our results suggest that this is not an effective or accurate way to group participants when considering disordered eating. We positioned bisexual men as a separate group, and found that their patterns of results in EDE-Q scores were different to both gay and heterosexual men, and sexual orientation influenced regression models differently. This underlines that bisexual men should not be grouped with gay men when exploring experiences of body image and eating disorders, but should be considered as a group in their own right. The practice of grouping people by fixed sexual orientation groups may be unhelpful in itself. There has been considerable change in our understanding of both gender and sexual identity fluidity over the past decade or so (Nicholson, Citation1990; Katz-Wise, Citation2015; Diamond, Citation2014). These concepts are not universally accepted, as this has impacted the way many individual self-identify it is important that researchers and clinicians are aware of how these experiences might affect clients and participants. It is likely that the pressures of being a bisexual man attracting people of various genders are very different from the pressures of being a heterosexual or gay man attracting people of only one gender, and thus are linked to different facets of the relationship with their bodies.
Measurement invariance analysis indicated that several of the EDE-Q items should be removed due to being variant at the error level. These items tended to focus on feelings around shape and weight, as well as dieting behaviors like limiting food. Our analysis indicates that the items that showed higher amounts of variance are related to feelings around shape, weight, and traditional dieting behaviors specifically. This is in line with prior research indicating that muscularity (linked to both shape and weight) is a key driver for men in their disordered eating behavior, and the dual pressures of being lean and muscular (Drummond, Citation2002; Duggan & McCreary, Citation2004; Murray et al., Citation2017). It is also worth noting that the restricting subscale did not show variance in any items, but all other subscales did.
Based on these results, we support previous findings that men’s experience of disordered eating is related to their sexual orientation. It is already established that gay men experience higher rates of eating disorders compared to heterosexual men, however this is not the complete picture (Duggan & McCreary, Citation2004). Our results demonstrate that drive for muscularity influences men in different ways related to their sexual orientation. For gay men, drive for muscularity links to greater dietary restraint, and for heterosexual men it is linked more to other disordered eating symptoms. This contradicts previous research finding that gay men had a higher drive for thinness coupled with muscularity and thus focused on a thin but muscular body ideal (Yelland & Tiggemann, Citation2003), which may predict a tighter link between drive for muscularity and shape and weight concern. The current study recruited a much larger sample size compared to Yelland and Tiggemann (Citation2003). However, it is possible that the body ideals within each community are changing in response to sociocultural trends; and that our results may indicate a shift in these ideals in comparison to previous research. Awareness of current body ideals for different sexual orientation groups is likely to help clinicians identify disordered eating thoughts and behaviors across these clients. Anecdotal comments from participants refer to the difference between “heterosexual thin” and “gay thin,” suggesting that the gay body ideal is even slimmer than the typical thin ideal seen in heterosexual communities. Our results similarly indicate that gay men experience more body shape and weight concern focusing on thinness than heterosexual men.
Clinical significance
These results indicate that clinicians should be mindful of a client’s sexual orientation when assessing and treating disordered eating thoughts and behaviors. The kinds of symptoms that clients present with might differ based on their sexual orientation. Heterosexual men may show more restriction around food, and their general disordered eating behaviors might be more strongly influenced by desire for a muscular body. Gay men may show more concern around thinness as well as muscularity, particularly showing restricting behaviors that link to wanting a muscular body. Clinicians should not assume that bisexual men will show the same kinds of behaviors as gay men, but should consider the influence of their sexual orientation in its own right. As such, bisexual men may show lower rates of these kinds of thoughts and behaviors.
Knowledge of the different disordered eating symptoms that different groups of men may experience can help clinicians provide more tailored interventions. Traditional treatment for disordered eating is unlikely to consider restricting in order to build muscularity (often referred to as shredding and bulking by the individuals taking part in these behaviors). However, for gay and bisexual men, in particular, this may be important. Heterosexual men, on the other hand, may benefit from awareness of drive for muscularity and its links to overall disordered eating thoughts and behaviors.
Limitations
We only considered the experiences of people identifying as heterosexual, bisexual, and gay; however, we also received responses from individuals identifying as, among others, asexual and pansexual. There were not sufficient participants in these groups to consider them alongside the others but based on our results it is possible that they would also experience different pressures and thus have different patterns of eating disorder and muscularity-related symptoms (Carlat et al., Citation1997). It would be useful for future research to recruit from other sexual orientation groups to consider how they demonstrate risk factors for eating disorders, and how this might help inform theories regarding the mechanisms of how sexual orientation relates to disordered eating. Many people identifying as genders other than cisgender men, including trans*, agender, and non-binary people, participated in the survey. Research into the impact of gender identity on the experiences of eating disorders should explore the experiences of these individuals in more depth, an area that is currently inadequately addressed in the literature.
Participants in this study were predominantly White. This issue is widespread in disordered eating research (Sonneville & Lipson, Citation2018). Similarly to the stereotypical picture of who gets an eating disorder being a slim, cisgender, heterosexual young woman, the typical eating disorder patient is also seen as White. However, research suggests that belonging to a racially minoritized community is a risk factor for development of disordered eating as well as being less likely to receive treatment for those symptoms (Sonneville & Lipson, Citation2018; Bodell et al., Citation2018). Even less of the available research explores the experiences of men of color, which is concerning given that one recent study suggests that Black men show different patterns of symptoms than Asian, Hawaiian, and Pacific Islander men, and Asian men usually scoring the highest (Goel et al., Citation2022). This study had similar limitations to previous research in the area, by not ensuring accessibility for a wider range of participants in terms of race. Given that both race and sexual orientation seem to have an effect on the kind of disordered eating thoughts and experiences that men have, further research should consider how these identities may intersect and have differing effects on men’s experiences and eating disorder vulnerability as this has impacted the way many individual self-identify.
Participants self-selected to participate in the study, responding to adverts placed on a range of social and traditional media channels. This means that those who chose to respond may be predisposed to have an interest in body image. All the participants that were included in our study were healthy and not currently diagnosed with an eating disorder, and thus our results do not generalize to people experiencing a clinical eating disorder. Studies exploring the relationships sexual orientation and clinical eating disorders in men are needed in the future. We asked participants in our study to define their own sexual orientation by clicking which group they felt they belonged to from a list, as well as an option of “other” with a self-identification box. Allowing participants to select their own sexual orientation instead of us assigning them to a group based on a scale ensured that we accurately captured how participants felt their sexual orientation was best explained. However, it may be that we missed out on some nuance by not adopting a spectrum approach to sexual orientation and instead placing participants in discrete groups. Overall the amount of variance that was explained by the regression models was small, aside from for the restricting scale (17.8%), but all were significant. This suggests that there are many more factors significantly linked to eating disorders in men aside from sexual orientation and drive for muscularity, and that the picture is much more complex than just being influenced by a handful of factors.
Conclusions
These results underline that sexual orientation is related to rates and types of eating disorder symptoms in healthy men, and also how those eating disorder symptoms are linked to the drive for muscularity. Disordered eating symptoms for a heterosexual man are different to those which a gay man experiences under the label of an eating disorder. These symptoms are related in different ways to drive for muscularity depending on sexual orientation, and drive for muscularity itself is experienced by a wide range of men. In gay men, greater drive for muscularity is linked to greater dietary restraint, in heterosexual men it is linked with other ED symptoms. Considering sexual orientation as a risk factor linked with different manifestations of eating disorders in men may allow preventative strategies to be tailored to different groups, allowing a focus on the most pertinent elements of disordered eating for that person.
Ethics statement
Ethical approval for this study was gained from the departmental ethics board at the Department of Psychology, University of York.
Disclosure statement
The authors report there are no conflicting interests to declare.
Data availability statement
The data that support the findings of this study are available from the corresponding author, Ruth Knight, upon reasonable request.
Additional information
Funding
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association.
- Austin, S. B., Ziyadeh, N., Kahn, J. A., Camargo, C. A., Jr, Colditz, G. A., & Field, A. E. (2004). Sexual orientation, weight concerns, and eating-disordered behaviors in adolescent girls and boys. Journal of the American Academy of Child & Adolescent Psychiatry, 43(9), 1115–1123. https://doi.org/10.1097/01.chi.0000131139.93862.10
- Bankoff, S. M., Richards, L. K., Bartlett, B., Wolf, E. J., & Mitchell, K. S. (2016). Examining weight and eating behavior by sexual orientation in a sample of male veterans. Comprehensive Psychiatry, 68, 134–139. https://doi.org/10.1016/j.comppsych.2016.03.007
- Berg, K. C., Peterson, C. B., Frazier, P., & Crow, S. J. (2011). Convergence of scores on the interview and questionnaire versions of the eating disorder examination: A meta-analytic review. Psychological Assessment, 23(3), 714–724. https://doi.org/10.1037/a0023246
- Blashill, A. J. (2010). Elements of male body image: Prediction of depression, eating pathology and social sensitivity among gay men. Body Image, 7(4), 310–316. https://doi.org/10.1016/j.bodyim.2010.07.006
- Bodell, L. P., Wildes, J. E., Cheng, Y., Goldschmidt, A. B., Keenan, K., Hipwell, A. E., & Stepp, S. D. (2018). Associations between race and eating disorder symptom trajectories in black and white girls. Journal of Abnormal Child Psychology, 46(3), 625–638.
- Boehm, I., Finke, B., Tam, F. I., Fittig, E., Scholz, M., Gantchev, K., Roessner, V., & Ehrlich, S. (2016). Effects of perceptual body image distortion and early weight gain on long-term outcome of adolescent anorexia nervosa. European Child & Adolescent Psychiatry, 25(12), 1319–1326. https://doi.org/10.1007/s00787-016-0854-1
- Brennan, D. J., Crath, R., Hart, T. A., Gadalla, T., & Gillis, L. (2011). Body dissatisfaction and disordered eating among men who have sex with men in Canada. International Journal of Men’s Health, 10(3), 253–268. https://doi.org/10.3149/jmh.1003.253
- Brennan, D. J., Craig, S. L., & Thompson, D. E. (2012). Factors associated with a drive for muscularity among gay and bisexual men. Culture, Health & Sexuality, 14(1), 1–15.
- Brown, T. A., & Keel, P. K. (2015). A randomized controlled trial of a peer co-led dissonance-based eating disorder prevention program for gay men. Behaviour Research and Therapy, 74, 1–10.
- Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. Sage Focus Editions, 154, 136–136.
- Byrne, B. M. (1994). Structural equation modeling with EQS and EQS/Windows: Basic concepts, applications, and programming. Sage.
- Calzo, J. P., Blashill, A. J., Brown, T. A., & Argenal, R. L. (2017). Eating disorders and disordered weight and shape control behaviors in sexual minority populations. Current Psychiatry Reports, 19(8), 49. https://doi.org/10.1007/s11920-017-0801-y
- Carey, M. A., Kupeli, N., Knight, R. E., Troop, N., Jenkinson, P. M., & Preston, C. E. J. (2019). Eating disorder examination questionnaire (EDE-Q): Norms and psychometric properties in UK females and males. Psychological Assessment, 31(7), 839–850. https://doi.org/10.1037/pas0000703
- Carlat, D. J., Camargo, C. A., & Herzog, D. B. (1997). Eating disorders in males: A report on 135 patients. The American Journal of Psychiatry, 154(8), 1127–1132.
- Cohn, L., Murray, S. B., Walen, A., & Wooldridge, T. (2016). Including the excluded: Males and gender minorities in eating disorder prevention. Eating Disorders, 24(1), 114–120.
- Cheung, G. W., & Rensvold, R. B. (2002). Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255.
- Diamond, L. M. (2014). I was wrong! Men are pretty darn sexually fluid too [Paper presentation].Presentation at the Sexuality Preconference of the Society for Personality and Social Psychology, Austin, TX.
- Drummond, M. J. (2002). Men, body image, and eating disorders. International Journal of Men’s Health, 1(1), 89–103.
- Drummond, M. J. (2005). Men’s bodies: Listening to the voices of young gay men. Men and Masculinities, 7(3), 270–290. https://doi.org/10.1177/1097184X04271357
- Drummond, M. J. (2010). Younger and older gay men’s bodies. Gay and Lesbian Issues and Psychology Review, 6(1), 31–41.
- Duggan, S. J., & McCreary, D. R. (2004). Body image, eating disorders, and the drive for muscularity in gay and heterosexual men: The influence of media images. Journal of Homosexuality, 47(3–4), 45–58.
- Fairburn, C. G., & Beglin, S. J. (1994). Assessment of eating disorders: Interview or self‐report questionnaire? The International Journal of Eating Disorders, 16(4), 363–370.
- Fairburn, C. G., Cooper, Z., Doll, H. A., Norman, P., & O’Connor, M. (2000). The natural course of bulimia nervosa and binge eating disorder in young women. Archives of General Psychiatry, 57(7), 659–665.
- Fairburn, C. G., & Beglin, S. J. (2008). Eating disorder examination questionnaire. Cognitive Behaviour Therapy and Eating Disorders, 309, 313.
- Feldman, M. B., & Meyer, I. H. (2007). Eating disorders in diverse lesbian, gay, and bisexual populations. The International Journal of Eating Disorders, 40(3), 218–226.
- Filiault, S. M., & Drummond, M. J. (2009). Methods and methodologies: Investigating gay men’s body image in Westernized cultures. Critical Public Health, 19(3–4), 307–323. https://doi.org/10.1080/09581590802626463
- Gigi, I., Bachner-Melman, R., & Lev-Ari, L. (2016). The association between sexual orientation, susceptibility to social messages and disordered eating in men. Appetite, 99, 25–33.
- Goel, N. J., Burnette, C. B., Weinstock, M., & Mazzeo, S. E. (2022). Eating disorder examination‐questionnaire: Evaluating factor structures and establishing measurement invariance with Asian/Hawaiian/Pacific Islander, Black, and White American college men. International Journal of Eating Disorders, 55(4), 481–493. https://doi.org/10.1002/eat.23696
- Harvey, J. A., & Robinson, J. D. (2003). Eating disorders in men: Current considerations. Journal of Clinical Psychology in Medical Settings, 10(4), 297–306. https://doi.org/10.1023/A:1026357505747
- Hatfield, E., & Sprecher, S. (1986). Mirror, mirror: The importance of looks in everyday life. Suny Press.
- Hilbert, A., De Zwaan, M., & Braehler, E. (2012). How frequent are eating disturbances in the population? Norms of the eating disorder examination-questionnaire. PloS One, 7(1), e29125.
- Katz-Wise, S. L. (2015). Sexual fluidity in young adult women and men: Associations with sexual orientation and sexual identity development. Psychology & Sexuality, 6(2), 189–208. https://doi.org/10.1080/19419899.2013.876445
- Keizer, A., Smeets, M. A., Dijkerman, H. C., Uzunbajakau, S. A., van Elburg, A., & Postma, A. (2013). Too fat to fit through the door: First evidence for disturbed body-scaled action in anorexia nervosa during locomotion. PloS One, 8(5), e64602. https://doi.org/10.1371/journal.pone.0064602
- Klimek, P., Murray, S. B., Brown, T., Gonzales, M.IV, & Blashill, A. J. (2018). Thinness and muscularity internalization: Associations with disordered eating and muscle dysmorphia in men. The International Journal of Eating Disorders, 51(4), 352–357.
- Lavender, J. M., De Young, K. P., & Anderson, D. A. (2010). Eating disorder examination questionnaire (EDE-Q): Norms for undergraduate men. Eating Behaviors, 11(2), 119–121.
- Legenbauer, T., Vocks, S., Schäfer, C., Schütt-Strömel, S., Hiller, W., Wagner, C., & Vögele, C. (2009). Preference for attractiveness and thinness in a partner: Influence of internalization of the thin ideal and shape/weight dissatisfaction in heterosexual women, heterosexual men, lesbians, and gay men. Body Image, 6(3), 228–234.
- Lippa, R. A. (2007). The preferred traits of mates in a cross-national study of heterosexual and homosexual men and women: An examination of biological and cultural influences. Archives of Sexual Behavior, 36(2), 193–208.
- McCreary, D. R. (2007). The drive for muscularity scale: Description, psychometrics, and research findings. In J. K. Thompson & G. Cafri (Eds.), The muscular ideal: Psychological, social, and medical perspectives (pp. 87–106). American Psychological Association.
- Morrison, M. A., Morrison, T. G., & Sager, C. (2004). Does body satisfaction differ between gay men and lesbian women and heterosexual men and women? A meta-analytic review. Body Image, 127–138.
- Murray, S. B., Griffiths, S., & Mond, J. M. (2016). Evolving eating disorder psychopathology: conceptualising muscularity-oriented disordered eating. British Journal of Psychiatry, 208, 414–415.
- Murray, S. B., Nagata, J. M., Griffiths, S., Calzo, J. P., Brown, T. A., Mitchison, D., Blashill, A. J., & Mond, J. M. (2017). The enigma of male eating disorders: A critical review and synthesis. Clinical Psychology Review, 57, 1–11.
- NEDA. (2016). Identity and eating disorders. Retrieved from https://www.nationaleatingdisorders.org/identity-eating-disorders
- Nicholson, L. (1990). Feminism/postmodernism (thinking gender). Routledge.
- Peterson, C. B., Crosby, R. D., Wonderlich, S. A., Joiner, T., Crow, S. J., Mitchell, J. E., Bardone-Cone, A. M., Klein, M., & le Grange, D. (2007). Psychometric properties of the eating disorder examination‐questionnaire: Factor structure and internal consistency. The International Journal of Eating Disorders, 40(4), 386–389. https://doi.org/10.1002/eat.20373
- Robinson, K. J., Mountford, V. A., & Sperlinger, D. J. (2013). Being men with eating disorders: Perspectives of male eating disorder service-users. Journal of Health Psychology, 18(2), 176–186.
- Rose, J. S., Vaewsorn, A., Rosselli-Navarra, F., Wilson, G. T., & Weissman, R. S. (2013). Test-retest reliability of the eating disorder examination-questionnaire (EDE-Q) in a college sample. Journal of Eating Disorders, 1(1), 1–10.
- Russell, C. J., & Keel, P. K. (2002). Homosexuality as a specific risk factor for eating disorders in men. The International Journal of Eating Disorders, 31(3), 300–306.
- Siever, M. D. (1994). Sexual orientation and gender as factors in socioculturally acquired vulnerability to body dissatisfaction and eating disorders. Journal of Consulting and Clinical Psychology, 62(2), 252–260. https://doi.org/10.1037/0022-006X.62.2.252
- Slade, P. D., & Russell, G. F. M. (1973). Experimental investigations of bodily perception in anorexia nervosa and obesity. Psychotherapy and Psychosomatics, 22(2), 359–363.
- Smink, F. R., Van Hoeken, D., & Hoek, H. W. (2012). Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Current Psychiatry Reports, 14(4), 406–414.
- Smith, K. E., Mason, T. B., Murray, S. B., Griffiths, S., Leonard, R. C., Wetterneck, C. T., Smith, B. E. R., Farrell, N. R., Riemann, B. C., & Lavender, J. M. (2017). Male clinical norms and sex differences on the eating disorder inventory (EDI) and eating disorder examination questionnaire (EDE‐Q). The International Journal of Eating Disorders, 50(7), 769–775.
- Sonneville, K. R., & Lipson, S. K. (2018). Disparities in eating disorder diagnosis and treatment according to weight status, race/ethnicity, socioeconomic background, and sex among college students. International Journal of Eating Disorders, 51(6), 518–526. https://doi.org/10.1002/eat.22846
- Strother, E., Lemberg, R., Stanford, S. C., & Turberville, D. (2012). Eating disorders in men: Underdiagnosed, undertreated, and misunderstood. Eating Disorders, 20(5), 346–355.
- Swami, V., & Tovée, M. J. (2008). The muscular male: A comparison of the physical attractiveness preferences of gay and heterosexual men. International Journal of Men’s Health, 7(1), 59–71. https://doi.org/10.3149/jmh.0701.59
- Talbot, D., Smith, E., Cass, J., & Griffiths, S. (2019). Development and validation of the new somatomorphic matrix–male: A figural rating scale for measuring male actual–ideal body discrepancy. Psychology of Men & Masculinities, 20(3), 356–367. https://doi.org/10.1037/men0000165
- Tiggemann, M., Martins, Y., & Kirkbride, A. (2007). Oh to be lean and muscular: Body image ideals in gay and heterosexual men. Psychology of Men & Masculinity, 8(1), 15–24. https://doi.org/10.1037/1524-9220.8.1.15
- Yelland, C., & Tiggemann, M. (2003). Muscularity and the gay ideal: Body dissatisfaction and disordered eating in homosexual men. Eating Behaviors, 4(2), 107–116.