

ABSTRACT
Instant Blood-Mediated Inflammatory Reaction (IBMIR) is a major cause of graft loss during pancreatic islet transplantation, leading to a low efficiency of this treatment method and significantly limiting its broader clinical use. Within the procedure, transplanted islets obstruct intrahepatic portal vein branches and consequently restrict blood supply of downstream lying liver tissue, resulting typically in ischemic necrosis. The extent of ischemic lesions is influenced by mechanical obstruction and inflammation, as well as subsequent recanalization and regeneration capacity of recipient liver tissue. Monitoring of immediate liver perfusion impairment, which is directly related to the intensity of post-transplant inflammation and thrombosis (IBMIR), is essential for improving therapeutic and preventive strategies to improve overall islet graft survival. In this study, we present a new experimental model enabling direct quantification of liver perfusion impairment after pancreatic islet transplantation using ligation of hepatic arteries followed by contrast-enhanced magnetic resonance imaging (MRI). The ligation of hepatic arteries prevents the contrast agent from circumventing the portal vein obstruction and enables to discriminate between well-perfused and non-perfused liver tissue. Here we demonstrate that the extent of liver ischemia reliably reflects the number of transplanted islets. This model represents a useful tool for in vivo monitoring of biological effect of IBMIR-alleviating interventions as well as other experiments related to liver ischemia. This technical paper introduces a novel technique and its first application in experimental animals.
1. Introduction
After the introduction of the Edmonton protocol in 2000, transplantation of isolated pancreatic islets has become a clinically applicable alternative to solid pancreas transplantation for the therapy of type-1 diabetic patients, especially those prone to hypoglycemia unawareness syndrome.Citation1,Citation2 In most cases, transplantation is performed as an infusion of islet suspension into the hepatic portal vein, thus allowing the islets to settle spontaneously in its peripheral branches. Transplanted islets cause mechanical obstruction and significantly reduce blood perfusion of downstream-lying liver tissue. The simple mechanical obstruction is intensified by the Instant Blood-Mediated Inflammatory Reaction (IBMIR), which is characterized by platelet aggregation, activation of clotting cascade and complement system, infiltration of leukocytes into the islets, and formation of thrombi as a consequence of direct contact of islet cells with recipient blood. IBMIR starts within minutes and culminates about 120 min after islet transplantation.Citation3,Citation4 Focal discolorations, which develop in suboptimally/insufficiently perfused liver tissue, are clearly visible immediately after islet transplantation with subsequent progression into focal necrosis of liver cells in order of hours. The consequent inflammation and thrombosis lead to a significant loss of transplanted islets early after infusion. It is estimated that 50–70% of transplanted islets are subject to destruction, i.e., less than half of the islets successfully engraft.Citation3-Citation7 Taken together, IBMIR contributes significantly to the fact that islet grafts isolated from more than one donor are required to achieve insulin independence of a diabetic patient in clinical practice.Citation4,Citation7-Citation9
Several intervention strategies improving islet engraftment by inhibition of coagulation and/or inflammation have been reported,Citation8-Citation14 however, a technique for quantification of ischemic liver tissue is still missing despite its critical need for the evaluation of efficiency of the diverse therapeutic interventions. Until now, IBMIR monitoring was based merely on the measurement of the level of thrombin-antithrombin complex after pancreatic islet transplantation or in vitro using the blood loop system.Citation8-Citation11,Citation13 To our best knowledge, only one paper focused on morphological quantification of necrotic liver tissue after islet transplantation was published.Citation15 The reported study was performed using a mouse animal model, a high number of transplanted islets (≳30 islets/g of body weight), and subsequent ex vivo examination of recipient liver using magnetic resonance imaging (MRI) with 11.7T scanner lasting for 80 min. Necrosis detected in sacrificed animals is characteristic for the late state of liver damage, but the obtained data does not enable the quantification of the actually non-perfused but still vital tissue. Therefore, this study proved the ability of MRI to examine the late liver impairment after islet transplantation in principle; nevertheless, the employed methodology cannot be used for in vivo monitoring of interventions aimed at modulating IBMIR.
The main aim of this study was to prepare a novel de-arterialized liver model for visualization of liver ischemia after pancreatic islet transplantation, which would be applicable for in vivo evaluation of efficiency of different experimental approaches focused on inhibition of IBMIR, and to test the sensitivity of this novel method using transplantation of islet grafts of different sizes (increasing number of islets).
2. Results
In our study, we have introduced a modification of the reported model to a more sensitive variant, which enables the comparison of different intervention approaches in vivo (heparinization and other coating of islets, islet preconditioning by RNA interference, preculturing of islets with different substances or cells, etc.). In order to improve the discrimination threshold between hypo-perfused and control liver tissue, we injected a contrast agent into the lateral tail vein of islet recipients at the start of the MRI examination 2 h after transplantation, i.e., at the time of presumed IBMIR culmination. The contrast agent increases the difference in signal intensity of perfused and non-perfused liver tissue, thus increasing the sensitivity of MRI. In addition, we have ligated hepatic arteries prior to islet transplantation. Without this intervention, hepatic arteries provide a way for the contrast agent to bypass the obstruction in portal vein blood flow. Previously, it was repeatedly reported that in case of liver transplantation in rodents, arterial reconstruction is better but not necessary for a long-term graft function and animal survival.Citation16,Citation17 In contrary to the study described above, we have used a significantly lower number of islets (0, 4, −4 islets per gram), and a less powerful MRI scanner (4.7T vs 11.7T).
2.1. Macroscopic visualization of intraportal thrombosis
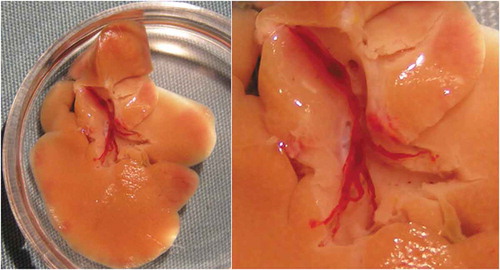
Immediately after pancreatic islet transplantation into the rat liver, ischemic areas appear which are clearly visible in a macroscopic view (). Inside the liver, a large thrombus can be found filling the branches of the portal vein tree (). Two days after transplantation, non-perfused liver areas turn into necrotic lesions. In 28 d, lesions are completely healed (data not shown).
Figure 1. Ischemic areas in rat liver 2 h after transplantation of 1000 syngeneic pancreatic islets without ligation of hepatic arteries. Dark brown/violet areas represent the non-perfused liver tissue.

Figure 2. Large thrombus filling the branches of portal vein inside of an ischemic rat liver 2 h after transplantation of 1000 syngeneic pancreatic islets.
2.2. Intravital staining with patent blue dye
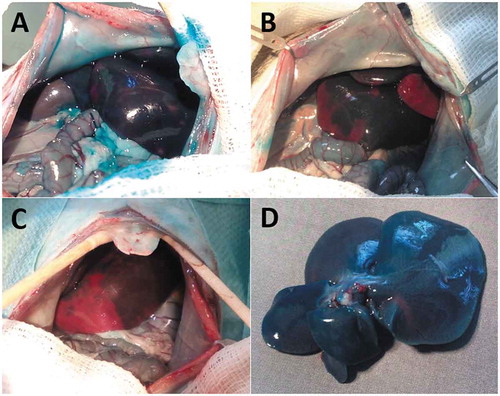
Two hours after transplantation of 100, 500 and 1000 pancreatic islet with ligation of hepatic arteries, the areas of non-perfused liver tissue were demonstratively visualized by injection of patent blue intravital contrast dye (). In case of 100 islets transplantation, ischemia was macroscopically almost indeterminable, whereas transplantation of 500 and 1000 islets led to a formation of extensive ischemic areas. Transplantation of islets without ligation of hepatic arteries caused the obstruction of several portal vein branches detectable only as temporarily delayed distribution of blue dye into these areas. Within 2 min, the hepatic arterial bloodstream bypassed the obstruction and spread out the contrast dye over the whole liver volume ().
Figure 3. Non-perfused areas of liver tissue 2 h after transplantation of 100 (A), 500 (B) and 1000 (C) syngeneic pancreatic islets with ligation and excised liver after transplantation of 1000 syngeneic pancreatic islets without ligation of hepatic arteries (D) 2 min after application of patent blue intravital contrast dye. Without ligation, the contrast dye perfuses quickly into the temporally ischemic areas through the arterial circulation.
2.3. Magnetic resonance imaging and quantification of ischemic tissue volume
The mean total volume of recipient liver measured using MRI in combination with a specific contrast agent was 9.50 ± 1.04 ml. The volume of ischemic tissue varied from 0.55 ± 0.01 ml in Group A, to 2.09 ± 0.11 ml in Group B, and 2.88 ± 0.01 ml in Group C, yielding in the proportion of ischemic tissue raising from 6.3% to 20.7%, and 28.1%, respectively, of the total liver volume ().
Figure 4. Calibration curve establishing a direct correlation between the number of transplanted islets and volume of ischemic liver tissue 2 h after transplantation of 100 (Group A), 500 (Group B) and 1000 (Group C) pancreatic islet into the portal vein of healthy rats (n = 6 in each group) with hepatic arteries ligated prior to transplantation. Graph shows the mean values (± standard deviation).
2.4. Serum examination
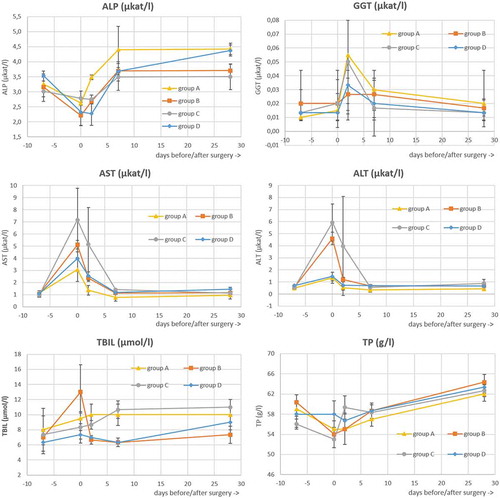
shows that ligation of hepatic arteries does not have any detrimental effect on rat liver cells. A temporary increase of liver enzymes activity in blood indicating the impairment of hepatocytes was detected early after islet transplantation (day +2) and was normalized until day 7 after surgery. The evaluated biochemical parameters remained in physiological range until the end of study.Citation18
Figure 5. Changes in standard biochemical parameters of rats during the experiment. Serum was collected from rat tail vein 7 d prior the surgery, 4 h after the surgery, and then 2, 7, and 28 d after the surgery. Group A, B, and C – transplantation of 100, 500, and 1000 isolated pancreatic islets, respectively, with ligation of hepatic arteries; Group D – only ligation of hepatic arteries without islet transplantation. For all groups n = 6; graph shows the mean values (± standard deviation). ALP – alkaline phosphatase, GGT – gamma-glutamyltransferase, AST – aspartate transaminase, ALT – alanine transaminase, TBIL – total bilirubin, TP – total protein.
3. Discussion
During the last two decades, extensive research was conducted focusing on the improvement of pancreatic islets engraftment in order to increase the efficiency of pancreatic islet transplantation as a therapeutic method. A large number of studies focused on alleviating IBMIR was publishedCitation8-Citation14; however, no method allowing the direct assessment of individual intervention efficiency in vivo has been available so far. Indirect laboratory parameters were reported indicating but not quantifying liver impairment caused by islet transplantation such as temporary increase of liver enzymes activity or presence of coagulation markers in blood.Citation8-Citation11,Citation13 Several papers also describe the decrease of islet number detected by MRI or positron-emission tomography during early posttransplant period,Citation5,Citation6,Citation19,Citation20 but the possibility of measuring the liver damage directly was missing. The only work reporting the range of posttransplant ischemic necrosis was focused on the late, fully matured consequences of portal vein micro-thrombosis but not on the acute post-transplant disturbances of blood flow.Citation15 These conditions are not commutable as the ultimate extent of the liver necrosis is, in addition to interruption of blood supply, influenced also by other factors including the timing of examination, the activity of plasminogen system, the individual resistance to ischemia, etc. The direct quantification of blood circulation defect can accurately reflect the extent and magnitude of portal vein micro-thrombosis and so the level of IBMIR early after islet transplantation.
In our study, we have combined the injection of MRI contrast agent into the tail vein with the ligation of hepatic arteries in order to prevent double perfusion of liver tissue from portal vein and hepatic arteries. First, we have tested the visualization of liver perfusion impairment using intravital dye patent blue or using MRI in combination with contrast agent. Due to double perfusion of liver through portal vein and hepatic arteries, the contrast agent is able to penetrate the ischemic liver tissue in a short time. Some delay of hypo-perfused regions was visible (up to 2 min), but not detectable using MRI due to standard time needed for technical preparation of animal inside the scanner. Therefore, we proceeded to the ligation of hepatic arteries, making the portal vein the only blood supply for liver. Our results demonstrate that de-arterialized liver can survive with good function and without any side effects for at least 30 d. The biochemical values returned to the physiological range within 1 week after surgery. Animals healed the operating wound normally and increased the body weight in time in the same manner as healthy animals. This is consistent with published data reporting a good long-term function even in case of transplanted liver without arterial anastomosis in rat.Citation16,Citation17 Using the interruption of the hepatic arterial blood flow, we prevented the intravenously injected contrast agent from penetrating the tissue behind the islets previously settled in peripheral branches of portal vein, thus enabling to “preserve” the areas of ischemic liver tissue for the subsequent imaging.
The ligation of hepatic arteries was followed by intraportal transplantation of pancreatic islets immediately and injection of patent blue dye 2 h later. Transplanted islets settle randomly in terminal branches of different liver lobes and patent blue clearly indicates the non-perfused regions, however, the quantification of ischemic tissue in vivo is impossible as it varies significantly inside the liver mass.
The MRI is considered as a safe, non-invasive method, which minimally burdens the patient and can be used repeatedly. Using proper coils and sequences in combination with gadolinium-based contrast agents, MRI can discriminate small lesions and enable even visualization of individual islets transplanted into liver of mice and rats and their localization in 3D reconstruction of whole animal.Citation19-Citation26 The gadolinium-based contrast increases the signal intensity of tissue and enhances the sensitivity of the scanner to distinguish among enhanced (perfused), non-enhanced (= non-perfused), and tissues influenced with negative (iron-based) contrast agents.Citation27 Therefore, we concluded that this method should be sensitive enough for visualization of focal disturbances in liver perfusion.
In order to have fully developed thrombi at the time of measurement, the MRI procedure was started 2 h after islet transplantation (culmination of IBMIR). Using MRI sequences described above, the abdominal cavity was scanned and individual abdominal organs were visualized. Immediately after intravenous injection of contrast agent, regions with an enhanced signal are clearly distinguishable from those, which signal intensity remained on basic, non-enhanced level. It is possible to outline non-perfused liver regions and after multiplying by layer thickness to quantify the total liver volume as well as the volume of non-perfused tissue. Two days later, the ischemic necrosis is macroscopically visible in the same location where it was detected by MRI before. Using this experimental protocol, it is possible to detect the liver perfusion impairment immediately after transplantation of pancreatic islets into the portal vein in vivo.
The other set of experiments was focused on the sensitivity of this novel technique. The ultimate goal is the evaluation of therapeutic inhibition of IBMIR by various methods. To estimate the extent of ischemic liver tissue related to different levels of IBMIR intensity, we decided simply to transplant an increasing number of islets. Using the same experimental design, three groups of animal recipients were prepared and transplanted by 100, 500 and 1000 islets. The larger extent of non-perfused liver was expected and confirmed for a higher number of transplanted islets. The identical processing of data obtained from MR scanner was applied and the final extent of non-perfused tissue was recalculated to total liver volume. There was a significant difference in the extent of non-perfused liver tissue after transplantation of 100, 500 and 1000 pancreatic islets into the portal vein. In addition to that, the extent of non-perfused tissue correlates with a number of transplanted islets precisely (with small standard deviation between individual animals).
The study has several limitations, the first of all being its non-translatability into the clinical practice. Because of the ligation of hepatic arteries, it is impossible to use this model in humans. However, the main purpose of this study is an introduction of an experimental model, which allows comparing the efficiency of different experimental approaches focused on alleviation of IBMIR, which contribution to islet death after transplantation is indisputable and present in human as well as animal models. Thus, the transfer of this model into clinical practice is not suitable nor requested as its main purpose is the evaluation of the therapeutic approach in general, but not the monitoring of each patient. The interruption of hepatic arteries prevents the method from the use even in large animals. Nevertheless, we believe that outcomes obtained using rodent models can considerably contribute to the improvement of islet pretreatment protocols and their establishment in routine clinical practice without the necessity of clinical trials based on this method. Although the microenvironment is very different in the case of rodent and human islet transplantation, the extent of liver ischemia serves in this case only as an “instrument” for demonstration/visualization of IBMIR intensity and its possible alleviation through the experimental interventions. Therefore, although this model cannot be directly transferred to clinical practice, it represents the only model for the evaluation of the effects of IBMIR-alleviating therapeutic interventions on liver perfusion in vivo and immediately after pancreatic islet transplantation.
Summarizing the presented results, we conclude that this model provides a unique and helpful technique for evaluation of the effect of different experimental interventions aimed at the inhibition of IBMIR in vivo. The main contribution of this study is the introduction of a visualization technique allowing the identification of liver ischemia extent in living animals without any detrimental effects on their health conditions.
4. Materials and methods
4.1. Study design
Isolated pancreatic islets in three different doses – 100 (Group A), 500 (Group B), and 1000 (Group C) – were transplanted into the portal vein of healthy rats (n = 6 in each group) with hepatic arteries ligated prior to transplantation. In Group D, only the ligation of hepatic arteries was performed. Two hours after islet transplantation (Group A, B and C), contrast-enhanced MRI of rat liver was performed and the volume of non-perfused liver tissue was quantified. Alternatively, for macroscopic evaluation, the distribution of intravital contrast dye patent blue (animals not included in experimental groups) was examined 2 h after islet transplantation. In order to confirm the safety of hepatic ligation, tail vein blood was collected for subsequent analysis 7 d prior the surgery, 4 h after the surgery, and then 2, 7 and 28 d after the surgery (all groups).
4.2. Animals
Male Brown Norway rats weighting 250–300 g (Velaz, Czech Republic) were used as both islet donors and recipients. All protocols related to this study were approved by the Animal Care Committee of the Institute for Clinical and Experimental Medicine and the Ministry of Health of Czech Republic. Experimental animals were maintained according to the European Convention on Animal Care in a controlled temperature, humidity, and 12/12 light/dark regimen with free access to food pellets and water. All surgical procedures were performed under total anesthesia induced by intramuscularly injected mixture of ketamine (Narketan, Vétoquinol S.A., France; 1,5 mg/100 g), dexmedetomidine (Dexdomitor, Orion Pharma, Czech Republic; 0,005 mg/100 g) and butorphanol (Torbugesic Vet, Zoetis, Spain; 0,05 mg/100 g).
4.3. Pancreatic islet isolation
Pancreatic islets were isolated using collagenase digestion followed by Ficoll discontinuous density gradient separation as previously described.Citation28 Briefly, pancreata of deeply anesthetized rats were filled through the bile duct with 15 ml of collagenase solution (Sigma-Aldrich, cat. # C9407; 1 mg/ml in HBSS, Hank´s balanced salt solution, Sigma-Aldrich, cat. # H8264). Excised pancreata were incubated for 10–15 min at 37°C with gentle shaking. Digested tissue was sieved through a 500 μm stainless steel mesh and islets were separated from exocrine tissue using Ficoll 400 discontinuous density gradient (Sigma-Aldrich, cat. # F9378; 1.108 g/ml, 1.096 g/ml, 1.069 g/ml, 1.037 g/ml). Purified islets were cultured overnight in CMRL-1066 (Biotech, cat. # P04-84600) based medium supplemented with 10% fetal bovine serum, 5% HEPES (both Sigma-Aldrich, cat. # F9665 and H0887, respectively) and 1% Penicillin/Streptomycin/L-Glutamine (Thermo Fisher Scientific, cat. # 10378-016), at 37°C in 5% CO2 atmosphere, and manually counted using dissection microscope prior to transplantation.
4.4. Liver ischemia model preparation
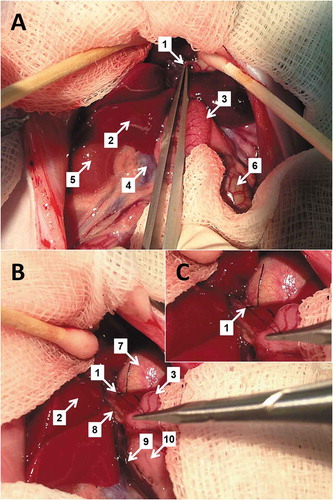
In order to increase the difference in MRI signal intensity of perfused and non-perfused liver tissue, the parallel arterial blood perfusion of the recipient liver was interrupted. Hepatic arteries (arteria hepatica propria and arteria hepatoesophagica) of Brown Norway rats were ligated ( and ) using Mersilk 7–0 non-absorbable material (Ethicon, cat. # W817) just before islet transplantation.
Figure 6. Preparation of arteria hepatica propria (A) and its ligation (B) in a detail (C). 1 – a. hepatica propria, 2 – duodenum, 3 – ductus choledochus, 4 – liver, 5 – v. cava caudalis, 6 – v. portae, 7 – v. pylorica.
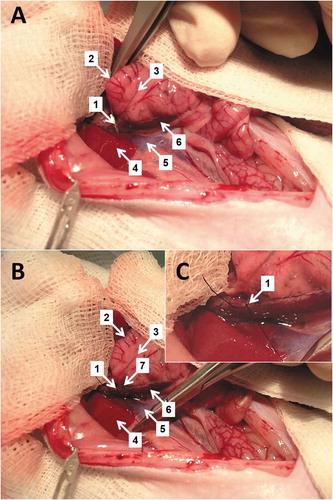
Figure 7. Preparation of arteria hepatoesophagica (A) and its ligation (B) in a detail (C). 1 – a. hepatoesophagica, 2 – liver, 3 – duodenum, 4 – v. cava caudalis, 5 – right kidney, 6 – cecum, 7 – stomach, 8 – ductus choledochus, 9 – v. portae, 10 – pancreas.
4.5. Pancreatic islet transplantation
After overnight cultivation, pancreatic islets (100, 500 or 1000) were transplanted into the portal vein using standard technique.Citation29 Briefly, the midline laparotomy was performed in deeply anesthetized animal. Then, the large intestine was spread out off the abdominal cavity on a wet gauze in order to visualize the ileocecal vein. Islets were collected into the 27G butterfly catheter and injected into the ileocecal vein in total volume of 300 μl of saline. Bleeding was stopped by Avitene® flour (Bard Inc., cat. # 1010020) and mechanic press on the puncture. The abdominal cavity was then sutured in two layers using Vicryl 5–0 absorbable material (Ethicon, cat. # W9501).
4.6. Macroscopic visualization of intraportal thrombosis
One thousand of syngeneic pancreatic islets were transplanted into the portal vein of a healthy animal as described above, without ligation of hepatic arteries. Two hours after transplantation, the liver was excised, gently washed with saline and the portal vein tree was dissected and photographed. In another animal, the liver was examined macroscopically 2 and 28 d after transplantation.
4.7. Intravital staining with patent blue dye
For macroscopic evaluation of liver ischemia, 100 μl of intravital contrast patent blue dye (Bleu Patenté V, Sodique Guerbet 2,5%, France) was equally diluted in saline and injected into the portal vein 2 h after transplantation of 500 or 1000 pancreatic islet with or without ligation of hepatic arteries and a macroscopic picture was taken.
4.8. Magnetic resonance imaging
MRI was carried out on a 4.7 T Bruker BioSpec scanner (Bruker, Germany) using a resonator coil with a diameter of 7 cm (Bruker, Germany). For anatomical localization of liver tissue, T2*-weighted MR images were acquired by a gradient echo sequence with the following parameters: repetition time (TR) = 111 ms, echo time (TE) = 3.7 ms, spatial resolution 0.254 × 0.254 × 1 mm3 and scan time of 4 min. For imaging of ischemic lesions, MRI contrast agent MultiHance® (gadobenate dimeglumine, Bracco, cat. # 0270–5164; 0,1 mmol/kg) was administered into the rat tail vein through a catheter. Then, T1-weighted MR images of liver were acquired by a gradient echo sequence: TR = 94.5 ms, TE = 3.7 ms, spatial resolution 0.23 × 0.23 × 1 mm3, number of acquisition (NA) = 16 and scan time of 6 min. Liver was usually covered by two stacks consisting of 11 slices.
4.9. Quantification of ischemic tissue volume
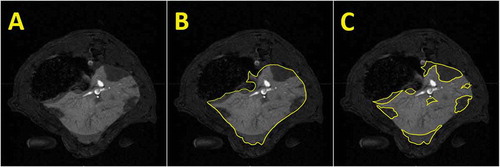
The volume of non-perfused liver tissue 2 h after transplantation was quantified based on magnetic resonance images using digital image analysis with ImageJ software (freely available at https://imagej.net/Welcome). Demonstration of the procedure is shown in . Three trained experts evaluated pictures independently with the final result combining all three individual assessments.
Figure 8. Illustrative picture of original magnetic resonance images of a rat abdominal cavity (A) with outlined liver (B) and ischemic areas within the liver tissue (C) after transplantation of 1000 syngeneic pancreatic islets using the MRI contrast agent to enhance the difference in the signal intensity of well-perfused and non-perfused liver tissue.
4.10. Serum examination
To prove that ligation of hepatic arteries does not have any detrimental effect on animal health, rat blood was collected from the tail vein 7 d prior to, at day of (4 h after), and then 2, 7 and 28 d after the surgery in experimental groups A, B, C and D. The serum was prepared and examined for following biochemical parameters: alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT), aspartate transaminase (AST) and alanine transaminase (ALT), total bilirubin (TBIL), and total protein (TP) level, using DRI-CHEM NX500i automated clinical chemistry analyzer (Fujifilm, Japan).
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Additional information
Funding
References
- Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, Warnock GL, Kneteman NM, Rajotte RV. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343(4):230–238. doi:10.1056/NEJM200007273430401.
- Shapiro AM, Ricordi C, Hering BJ, Auchincloss H, Lindblad R, Robertson RP, Secchi A, Brendel MD, Berney T, Brennan DC, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med. 2006;355(13):1318–1330. doi:10.1056/NEJMoa061267.
- Moberg L, Korsgren O, Nilsson B. Neutrophilic granulocytes are the predominant cell type infiltrating pancreatic islets in contact with ABO-compatible blood. Clin Exp Immunol. 2005;142(1):125–131. doi:10.1111/j.1365-2249.2005.02883.x.
- Delaune V, Berney T, Lacotte S, Toso C. Intraportal islet transplantation: the impact of the liver microenvironment. Transpl Int. 2017;30(3):227–238. doi:10.1111/tri.12919.
- Eich T, Eriksson O, Lundgren T. Visualization of early engraftment in clinical islet transplantation by positron-emission tomography. N Engl J Med. 2007;356:2754–2755. doi:10.1056/NEJMc070201.
- Eich T, Eriksson O, Sundin A, Estrada S, Brandhorst D, Brandhorst H, Langstrom B, Nilsson B, Korsgren O, Lundgren T. Positron emission tomography: a real-time tool to quantify early islet engraftment in a preclinical large animal model. Transplantation. 2007;84:893–898. doi:10.1097/01.tp.0000284730.86567.9f.
- Korsgren O, Lundgren T, Felldin M, Foss A, Isaksson B, Permert J, Persson NH, Rafael E, Ryden M, Salmela K, et al. Optimising islet engraftment is critical for successful clinical islet transplantation. Diabetologia. 2008;51(2):227–232. doi:10.1007/s00125-007-0868-9.
- Johansson H, Lukinius A, Moberg L, Lundgren T, Berne C, Foss A, Felldin M, Källen R, Salmela K, Tibell A, et al. Tissue factor produced by the endocrine cells of the islets of Langerhans is associated with a negative outcome of clinical islet transplantation. Diabetes. 2005;54:1755–1762. doi:10.2337/diabetes.54.6.1755.
- Moberg L, Johansson H, Lukinius A, Berne C, Foss A, Källen R, Østraat Ø, Salmela K, Tibell A, Tufveson G, et al. Production of tissue factor by pancreatic islet cells as a trigger of detrimental thrombotic reactions in clinical islet transplantation. Lancet. 2002;360:2039–2045. doi:10.1016/s0140-6736(02)12020-4.
- Ozmen L, Ekdahl KN, Elgue G, Larsson R, Korsgren O, Nilsson B. Inhibition of thrombin abrogates the instant blood-mediated inflammatory reaction triggered by isolated human islets: possible application of the thrombin inhibitor melagatran in clinical islet transplantation. Diabetes. 2002;51(6):1779–1784. doi:10.2337/diabetes.51.6.1779.
- Moberg L, Olsson A, Berne C, Felldin M, Foss A, Källen R, Salmela K, Tibell A, Tufveson G, Nilsson B, et al. Nicotinamide inhibits tissue factor expression in isolated human pancreatic islets: implications for clinical islet transplantation. Transplantation. 2003;76(9):1285–1288. doi:10.1097/01.TP.0000098905.86445.0F.
- Nilsson B, Ekdahl KN, Korsgren O. Control of instant blood-mediated inflammatory reaction to improve islets of Langerhans engraftment. Curr Opin Organ Transplant. 2011;16(6):620–626. doi:10.1097/MOT.0b013e32834c2393.
- Cabric S, Sanchez J, Lundgren T, Foss A, Felldin M, Källen R, Salmela K, Tibell A, Tufveson G, Larsson R, et al. Islet surface heparinization prevents the instant blood-mediated inflammatory reaction in islet transplantation. Diabetes. 2007;56(8):2008–2015. doi:10.2337/db07-0358.
- Teramura Y, Iwata H. Islets surface modification prevents blood-mediated inflammatory responses. Bioconjug Chem. 2008;19(7):1389–1395. doi:10.1021/bc800064t.
- Sakata N, Hayes P, Tan A, Chan NK, Mace J, Peverini R, Sowers L, Pearce WJ, Chinnock R, Obenaus A, et al. MRI assessment of ischemic liver after intraportal islet transplantation. Transplantation. 2009;87:825–830. doi:10.1097/TP.0b013e318199c7d2.
- Lee S, Charters AC, Orloff MJ. Simplified technic for orthotopic liver transplantation in the rat. Am J Surg. 1975;130:38–40. doi:10.1016/0002-9610(75)90453-5.
- Hori T, Gardner LB, Chen F, Baine AM, Hata T, Uemoto S, Nguyen JH. Impact of hepatic arterial reconstruction on orthotopic liver transplantation in the rat. J Invest Surg. 2012;25(4):242–252. doi:10.3109/08941939.2011.636476.
- Quesenberry KE, Carpenter JW. Ferrets, rabbits, and rodents: clinical medicine and surgery. St. Louis (MO): Elsevier; 2012.
- Saudek F, Jirak D, Girman P, Herynek V, Dezortova M, Kriz J, Peregrin J, Berkova Z, Zacharovova K, Hajek M. Magnetic resonance imaging of pancreatic islets transplanted into the liver in humans. Transplantation. 2010;90(12):1602–1606. doi:10.1097/tp.0b013e3181ffba5e.
- Jirak D, Kriz J, Strzelecki M, Yang J, Hasilo C, White DJ, Foster PJ. Monitoring the survival of islet transplants by MRI using a novel technique for their automated detection and quantification. MAGMA. 2009;22(4):257–265. doi:10.1007/s10334-009-0172-4.
- Evgenov NV, Medarova Z, Dai G, Bonner-Weir S, Moore A. In vivo imaging of islet transplantation. Nat Med. 2006;12(1):144–148. doi:10.1038/nm1316.
- Evgenov NV, Medarova Z, Pratt J, Pantazopoulos P, Leyting S, Bonner-Weir S, Moore A. In vivo imaging of immune rejection in transplanted pancreatic islets. Diabetes. 2006;55(9):2419–2428. doi:10.2337/db06-0484.
- Kriz J, Jirak D, White D, Foster P. Magnetic resonance imaging of pancreatic islets transplanted into the right liver lobes of diabetic mice. Transplant Proc. 2008;40(2):444–448. doi:10.1016/j.transproceed.2008.02.018.
- Berkova Z, Jirak D, Zacharovova K, Kriz J, Lodererova A, Girman P, Koblas T, Dovolilova E, Vancova M, Hajek M, et al. Labeling of pancreatic islets with iron oxide nanoparticles for in vivo detection with magnetic resonance. Transplantation. 2008;85(1):155–159. doi:10.1097/01.tp.0000297247.08627.ff.
- Kriz J, Jirak D, Girman P, Berkova Z, Zacharovova K, Honsova E, Lodererova A, Hajek M, Saudek F. Magnetic resonance imaging of pancreatic islets in tolerance and rejection. Transplantation. 2005;80(11):1596–1603. doi:10.1097/01.tp.0000183959.73681.b9.
- Jirak D, Kriz J, Herynek V, Andersson B, Girman P, Burian M, Saudek F, Hajek M. MRI of transplanted pancreatic islets. Magn Reson Med. 2004;52(6):1228–1233. doi:10.1002/mrm.20282.
- Herynek V, Berkova Z, Dovolilova E, Jirak D, Kriz J, Girman P, Saudek F, Hajek M. Improved detection of pancreatic islets in vivo using double contrast. Contrast Media Mol Imaging. 2011;6(4):308–313. doi:10.1002/cmmi.432.
- Girman P, Kriz J, Balaz P. Rat experimental transplantation surgery: a practical guide. Basel (CH): Springer; 2015.
- Kriz J, Jirak D, Berkova Z, Herynek V, Lodererova A, Girman P, Habart D, Hajek M, Saudek F. Detection of pancreatic islet allograft impairment in advance of functional failure using magnetic resonance imaging. Transpl Int. 2012;25(2):250–260. doi:10.1111/j.1432-2277.2011.01403.x.

