

ABSTRACT
Background
Aging, uninsured, underserved, ethnic/racial minority groups and residents of rural areas are most vulnerable to suffering from a lack of access to health care. These populations experience delays in diagnosis and treatment, making treatment more difficult and expensive.
Case Description
In as much as the mouth is critical to overall health and quality of life, resources are needed to reduce these disparities and find ways to integrate the practice of dentistry and medicine. The specialty of oral medicine is one venue of opportunity. This paper aims to share the importance of oral medicine specialists in bridging the gap between medicine and dentistry and managing patients using a safety-net dental clinic.
Practical Implications
The authors present a case that provides insights into “vulnerable” populations, access to care, the importance of early diagnosis, and how safety-net clinics play an important role, especially during the Coronavirus disease 2019 (COVID-19) pandemic, in providing oral health care to a community in need.
Continuing Education Credit Available: The practice worksheet is available as supplemental material for this article: https://doi.org/10.1080/19424396.2023.2174659.
A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20
Oral medicine is the 11th recognized dental specialty by the American Dental Association (ADA) in the United States.Citation1 Oral medicine specialists diagnose and manage a wide range of conditions of the maxillofacial region and the oral cavity, such as oral mucosal diseases, orofacial pain conditions, temporomandibular disorders, salivary gland disorders, oral complications related to cancer treatments and diagnosis and management of patients with complex medical problems.Citation2 Through their unique education and training, these specialists are able to help integrate oral health care into the medical health care model.Citation3,Citation4 Accordingly, oral medicine specialists play significant roles in bridging the gap between the medical health and the oral health of people who are less fortunate, given the state of the current health care system.Citation5–7
Oral health has a direct impact on an individual’s overall health and life quality.Citation3 Therefore, inadequate access to dental care is a barrier to good oral health.Citation8 Across all ages and income levels, dental care costs are the most significant cited barrier to care.Citation9 The coronavirus 2019 (COVID-19) pandemic exacerbated these issues, especially among individuals at elevated risk for oral diseases.Citation10 The extent and duration of this pandemic led to greatly reduced access to care and greatly reduced hours of routine dental office operation, except for dental emergency services.Citation10
Federally qualified health centers (FQHC), community-based clinics, hospitals and dental schools serve as safety-net dental clinics for underserved and low-income populations.Citation11,Citation12 However, these clinics and centers may not be readily available or known to the communities that need them or employ dental specialists such as oral medicine practitioners to diagnose and manage complex oral diseases. Another safety net for the marginalized and underserved populations is foundation grant-based clinics. Extramurally funded grants can help ease the high costs of oral health care and the burden of oral and dental disease in uninsured and underserved populations. One example is the extramural Delta Dental Community Care Foundation (DDCCF) biopsy grant. This grant helps to support oral health care providers, such as oral medicine specialists, in the performance of clinical examinations, imaging studies, biopsies and laboratory testing analyses at no cost for qualified patients.
This case report presents a patient referred to an oral medicine practice at a safety-net dental clinic utilizing the DDCCF biopsy grant. Given the patient’s challenges associated with limited financial resources, lack of dental insurance and delayed access to care due to the COVID-19 pandemic, the authors were inspired to share this resource as an example of how they can help uninsured and low-income individuals who have diagnostically challenging diseases receive care.
Case Report
In 2021, a 39-year-old Hispanic female was referred to the oral medicine clinic at the Western University of Health Sciences in Pomona with chief complaints of worsening dry mouth and rampant cervical dental caries. These problems occurred despite the patient’s good home oral hygiene for the past 4 years. Due to her financial constraints, newly established dental coverage and the COVID-19 pandemic, the patient had not received routine dental care for how many months. In addition, the patient could not request time off work, which created another barrier to her oral health care. She reported difficulty in speech due to xerostomia and intermittent feeling of “sand” in her eyes for the past two years. In 2019, she established care with a rheumatologist for her positive antinuclear antibody (ANA), negative anti-Sjögren’s syndrome SSA (Ro) and SSB (La) antibodies lab finding and intermittent fatigue. Her family history was significant for her mother who has systemic erythematous lupus and Sjögren’s syndrome (SS). The patient’s medical history was significant for gastroesophageal reflux disease (GERD), controlled with omeprazole 20 mg daily.
A detailed extraoral and intraoral clinical examination was notable for erythematous and dry palatal tissue, multiple carious lesions on the buccal and lingual surfaces of 15 teeth (). Her parotid gland salivary flow was diminished bilaterally. Measured unstimulated whole saliva was <0.1 mL/min (normal: ranging from 0.3–0.4 mL/min) indicative of hyposalivation.Citation13,Citation14 She had visited two general dental practitioners for oral dryness and dental caries. Due to her limited financial resources, rampant carious lesions and dental insurance coverage, she was referred to the university for evaluation and management of her oral complaints and restorations. Meanwhile, she was being monitored via synchronous telehealth visits with her rheumatologist and had been referred to an otolaryngologist for reported dysphagia and chronic oral dryness symptoms. Her medical specialty consultation was delayed due to medical insurance authorization and the pandemic. Her visit to an otolaryngologist was uneventful, and it was recommended for the patient to establish a dental home since her complaints seemed better managed with an oral health care provider.
Figure 1. Dry oral mucosa, extensive cervical caries on posterior maxillary and mandibular dentitions and dry, erythematous palatal tissue.

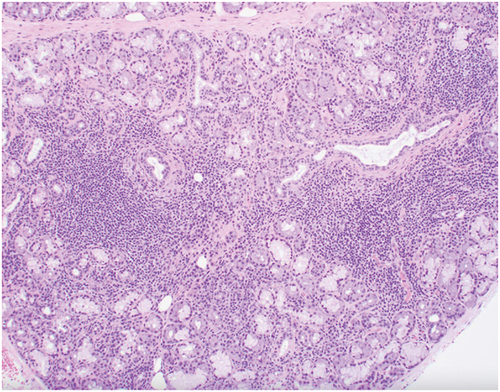
Based on her hyposalivation, chronic oral symptoms, laboratory values and recent ocular symptoms, a labial minor salivary gland biopsy was recommended and performed under the DDCCF biopsy grant.Citation15 The histology and histopathology report confirmed focal lymphocytic sialadenitis consistent with the salivary component of SS (). The findings were discussed with her rheumatologist, and further medical management was arranged with the physician specialist, including referral to an ophthalmologist. The authors provided a dry mouth protocol including topical fluoride and prescribed a parasympathomimetic medication, pilocarpine 5 mg three times a day.Citation12 At the six-month oral medicine follow-up visit, caries control had been achieved and her oral hygiene and diet were greatly improved. The patient also reported significantly positive outcomes with her oral and general health care. The most positive aspects of her care are reported to be:
Figure 2. Focal lymphocytic sialadenitis consistent with the salivary component of Sjögren’s syndrome. (Image courtesy of Gretchen Folk, DDS, MS. Scripps Oral Pathology Services, San Diego).
She has a better understanding of her chronic systemic disease process.
She is not living with the uncertainty of not having a diagnosis
Her medical and dental care is being better communicated and coordinated with her health care providers.
She understands and applies recommended techniques to manage her dry mouth, which has resulted in disease control.Citation13
Discussion
Oral diseases pose significant health issues, create a heavy economic burden and associate with reduced quality of life for people in the U.S. and globally.Citation16,Citation17 Poor oral health not only affects an individual’s income and the economy by disabling the workforce but also elevates health care costs by increasing the number of emergency dental care visits for palliative treatments instead of definitive oral health care.Citation4 Annually, palliative care related to dental pain visits at the emergency departments costs $1 billion dollars.Citation3 Of note, oral diseases continue to be highly prevalent in low- and middle-income countries, mainly due to social and economic inequalities and barriers to funding for prevention and management.Citation17
Per the Centers for Disease Control and Prevention(CDC), people with chronic diseases such as heart disease, diabetes, autoimmune disease and obesity are at risk of losing their dentition and developing poor overall health. As in the above case example, SS is one of the most challenging chronic and multisystem autoimmune rheumatic disorders to evaluate and treat.Citation15,Citation18 SS is characterized by oral and ocular dryness from salivary and lacrimal glandular tissue damage.Citation15 SS affects approximately 3 million of Americans,Citation14 reducing their oral and overall quality of a patient’s lifeCitation19 and leading to costly oral health complications.Citation20 Currently, there is no cure for the disease, and delays in diagnosis are common since oral and ocular dryness can have an insidious onset. SS is a risk factor for the development of hematological disorders and malignancies such as mucosa-associated lymphoid tissue (MALT) lymphoma, a subtype of low-grade B cell non-Hodgkin lymphomasCitation21; therefore, close patient monitoring is essential. Oral medicine specialists play an important role in the diagnosis and management of this condition through collaboration with medical specialists i.e., rheumatologists and ophthalmologists and the oral health care providers.Citation15
Access to Oral Health Care Barriers
In the United States, several barriers contribute to access to care and navigation of the oral health care system in the underserved, vulnerable, and aging patients with chronic diseases.Citation22,Citation23 Some of these barriers include cost, oral health care service reimbursement issues, variation in the scope of practice or expertise and oral health care provider shortage areas and the COVID-19 pandemic.Citation8,Citation23–25 The cost of dental care remains the single most cited barrier to access to care for all individuals regardless of income, insurance and age.Citation9 It is why free annual events in California, such as CDA Cares, Care Harbor Los Angeles and Give Kids Smile events nationwide, have turnouts in the thousands.Citation26–31 However, these events happen throughout the weekend and many patients who attend lack continuity of care. The actual cost of dental care goes beyond treatment expenses. It includes the cost of time, transportation, proximity to dental offices, busy work schedules and ability to take time off for dental care.Citation30,Citation31 These factors are compounded in the elderly who are often retired, live on a fixed income, uninsured and suffer a greater prevalence of periodontal disease, tooth loss and dry mouth associated with polypharmacy.Citation32 Moreover, 56 million Americans live in areas with a shortage of dentists,Citation33 and California, which has the highest number of dentists compared to other states in the U.S., still has 2.2 million Californians who live in areas with dental workforce shortages.Citation25
Are Dental Benefit Plans the Solution?
Historically, dental benefit plans differ from medical insurance plans due to differences between medical-dental diseases and an existing divergent health care system.Citation34 Medi-Cal Dental Program, California’s Medicaid program, pays up to $1,800 annually for covered dental services for adults over 18. In the U.S., 70% of older adults don’t have dental insurance.Citation32 The remaining 30% have coverage through their employer, Medicaid, or self-purchased supplemental dental plans.Citation32 Dental care services’ reimbursement rate through Medi-Cal is lower than those paid by private dental insurers, leading to many private dental practitioners declining to treat Medi-Cal beneficiaries or limiting the number of Medi-Cal patients treated in dental practices.Citation25 Integration of dental-medical screening for chronic diseases could aid the health care system and help save an estimated $102.6 million annually.Citation33 The underserved would also benefit by increasing the number of providers in underserved areas, expanding public dental insurance programs and incentivizing providers by addressing reimbursement rates from public insurance.Citation35
The Role of FQHCs and Partnerships
FQHCs provide important dental care to the most vulnerable, communities of color, Medicaid and Medicare enrollees and underserved populations in America.Citation36,Citation37 These clinics help fill the gap between private practice-sector dental care and vulnerable populations who need timely care and a dental home.Citation12,Citation38 One method that could help improve access to care involves partnering with dental schools across the U.S. Dental schools actively provide students and residents with experiences in underserved communities by partnering with FQHCs. Dental schools also tend to offer reduced prices, diagnostic equipment beyond the scope of FQHC personnel and access to dental specialty services such as oral medicine. Thus, partnerships between dental schools and FQHCs may increase access to care for vulnerable populations and help coordinate care with dental specialists, e.g., oral medicine specialists who can help integrate oral health care and coordinate overall health care with the required medical providers.Citation4
COVID-19 Pandemic Impact on Access to Care
As illustrated in the case report, the COVID-19 pandemic created disproportional limited access to routine dental care, especially for “vulnerable” populations such as people who have medical, physical, financial and/or learning disabilities.Citation39 The unforeseen evolution of the COVID-19 pandemic not only drastically altered the normalcy of everyday life but also further negatively impacted individuals who were already experiencing difficulties with access to dental care within the U.S.Citation10 The pandemic helped change the role of dental workforces in the health system and provided an opportunity to evaluate how oral health care providers interacted with the health system in helping to end the pandemic.Citation40 Many dental practices, including safety-net dental clinics, incorporated telehealth visits into their routine workflow.Citation41 These visits included initial or reevaluation of oral mucosal lesions, accompanied by the limitations for evaluating important features of oral lesions.Citation41 The ADA Health Policy Institute survey reported that during the week of March 23, 2020, of the pandemic, 76% of dental offices saw only emergency patients, 19% were completely closed and 5% saw a reduced volume of patients.Citation42 Moreover, the extent of the COVID-19 pandemic, patients’ financial limitations and loss of dental insurance have contributed to access to care, especially in vulnerable populations.Citation10 This case report highlights multiple access to care issues that millions across the U.S. may have faced when confronted with a pandemic and the other barriers the authors have reported.
Extramural Grant at Western University College of Dental Medicine
The DDCCF biopsy grant provides oral medicine specialty services for uninsured and underserved populations. The grant utilized at the author’s patient care clinic is a dentist-led initiative that delivers low-cost or free screening and testing to medically underserved dental patients who face language, cultural, and financial barriers to diagnosing lesions, tumors and oral cavity cysts. As such, it creates opportunities for interprofessional collaborations between dental and medical providers. This grant is awarded annually based on the safety-net clinic’s eligibility. Qualified patients receive diagnostic evaluation, imaging studies, biopsies, and laboratory testing analysis at no cost. Biopsy results are prompt, can save lives and patients get a chance to discuss management options and coordinate care with their oral and medical health care providers.
Conclusion
Safety-net dental clinics are a critical component of providing oral health care to vulnerable populations.Citation4 These clinics help to create access to affordable care, connect medicine to dentistry, and increase collaborations amongst healthcare providers. Programs such as these should be considered for expansion or other innovative ideas promoted if oral health care providers are to serve as advocates for their patients to receive the basic rights of affordable healthcare, equity, dignity, and ultimate respect they genuinely deserve, no matter their socioeconomic status.
Overall, oral health care providers are in a unique position to detect oral signs and symptoms associated with chronic systemic disorders and promptly refer patients to oral medicine specialists, and coordinate care with physicians for diagnosis, monitoring, prevention of complications, and management.Citation18 The author’s case features the importance of oral medicine specialists in disease diagnosis, educating patients regarding their disease process and management modalities, collaboration with medical health care providers to provide better care, in addition to utilizing safety-net clinics to address the needs of a vulnerable population. Barriers to access care, such as cost of care, need for oral/dental specialty care services and the COVID-19 pandemic, led this patient to be without care for many years. Dentistry, however, has ways to help and continues to help using several of the approaches illustrated here; yet more are needed to help those in need.
Supplemental Material: January 2023 CE
Download MS Word (25.8 KB)Supplemental data
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2174659.
Additional information
Notes on contributors
Sahar Mirfarsi
Sahar Mirfarsi, DDS, is an assistant professor and the co-coordinator of the advanced oral diagnosis workgroup at the Western University of Health Sciences, College of Dental Medicine in Pomona, California. She’s a diplomate of the American Board of Oral Medicine. She focuses her research on oral medicine-related topics and is dedicated to remove access to oral health care barriers for the uninsured, underserved and vulnerable populations.
Aaron Bacha
Aaron Bacha, is a 2023 DMD candidate in the College of Dental Medicine at Western University of Health Sciences with an interest in community-based clinical practice and research in public health dentistry.
Vineza Saraza Reduta
Vineza Saraza Reduta, BA, is a 2023 DMD candidate in the College of Dental Medicine at Western University of Health Sciences with an interest in pursuing pediatric dentistry, especially providing a dental home to those with special needs and disabilities.
Mark Mintline
Mark Mintline, DDS, is an assistant professor and co-coordinator of the advanced oral diagnosis workgroup in the College of Dental Medicine at Western University of Health Sciences. He is a diplomate of the American Board of Oral and Maxillofacial Pathology and the laboratory director of WesternU Health Oral Pathology Laboratory. He oversees diagnostic testing for the College and is dedicated to increasing access to oral health services to underserved dental patients who face language, cultural and financial barriers.
Craig S. Miller
Craig S. Miller, DMD, MS, is the Alvin L. Morris professor of oral health research, university research professor, and director of the Nudge Unit at University of Kentucky College of Dentistry. He oversees the oral medicine curriculum for the College and focuses his research on risk assessment, decision-making and medically complex dental care.
References
- National Commission on Recognition of Dental Specialties and Certifying Boards. ADA recognized dental specialties. Accessed August 8, 2022.
- Sollecito TP, Rogers H, Prescott-Clements L, et al. Oral medicine: defining an emerging specialty in the United States. J Dent Educ. April 2013;77(4):392–5. doi:10.1002/j.0022-0337.2013.77.4.tb05484.x.
- Simon L. Overcoming historical separation between oral and general health care: interprofessional collaboration for promoting health equity. AMA J Ethics. September 1, 2016;18(9):941–949. doi:10.1001/journalofethics.2016.18.9.pfor1-1609.
- Fellows JL, Atchison KA, Chaffin J, Chávez EM, Tinanoff N. Oral health in America: implications for dental practice. J Am Dent Assoc. July 2022;153(7):601–609. doi:10.1016/j.adaj.2022.04.002. Epub 2022 May, 25. PMCID: PMC9637008.
- Vujicic M, Fosse C. Time for dental care to be considered essential in U.S. health care policy. AMA J Ethics. January 2022;24(1):E57–63. doi:10.1001/amajethics.2022.57.
- Scully C, Miller CS, Aguirre Urizar JM, et al. Oral medicine (stomatology) across the globe: birth, growth, and future. Oral Surg Oral Med Oral Pathol Oral Radiol. February 2016;121(2):149–157.e5. doi:10.1016/j.oooo.2015.10.009. Epub 2015 October 19.
- Miller CS, Peterson DE. Oral medicine: today’s future can become tomorrow’s reality. Oral Surg Oral Med Oral Pathol Oral Radiol. November 2018;126(5):409–414. doi:10.1016/j.oooo.2018.07.001. Epub 2018 August 22.
- U.S. Department of Health and Human Services, National Institutes of Health and National Institute of Dental and Craniofacial Research. Oral health in America: advances and challenges.
- Vujicic M, Buchmueller T, Klein R. Dental care presents the highest level of financial barriers, compared to other types of health care services. Health Aff (Millwood). December 1, 2016; 35(12):2176–2182. doi:10.1377/hlthaff.2016.0800.
- Brian Z, Weintraub JA. Oral health and COVID-19: increasing the need for prevention and access. Prev Chronic Dis. August 13, 2020; 17:E82. doi:10.5888/pcd17.200266. PMCID: PMC7458118.
- Byck GR, Cooksey JA, Russinof H. Safety-net dental clinics. J Am Dent Assoc. July 2005;136(7):1013–1021. doi:10.14219/jada.archive.2005.0296.
- Beazoglou T, Heffley D, Lepowsky S, Douglass J, Lopez M, Bailit H. The dental safety net in connecticut. J Am Dent Assoc. October 2005;136(10):1457–1462. doi:10.14219/jada.archive.2005.0061.
- Navazesh M, Kumar SKS. Measuring salivary flow: challenges and opportunities. J Am Dent Assoc. May 2008;139(35S–40S):35S–40S. doi:10.14219/jada.archive.2008.0353.
- Navazesh M. How can oral health care providers determine if patients have dry mouth? J Am Dent Assoc. May 2003;134(5):613–620. doi:10.14219/jada.archive.2003.0229. quiz 633.
- Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome. Arthritis Rheumatol. January 2017;69(1):35–45. doi:10.1002/art.39859. Epub 2016 October 26. PMCID: PMC5650478.
- Pourat N, Andersen RM, Marcus M. Assessing the contribution of the dental care delivery system to oral health care disparities. J Public Health Dent. 2015 Winter;75(1):1–9. doi:10.1111/jphd.12064. Epub 2014 June 25. PMCID: PMC4276727.
- Peres MA, Macpherson LMD, Weyant RJ, et al. Oral diseases: a global public health challenge. Lancet. July 20, 2019;394(10194):249–260. doi:10.1016/S0140-6736(19)31146-8.
- Vivino FB, Carsons SE, Foulks G, et al. New treatment guidelines for Sjögren’s disease. Rheum Dis Clin North Am. August 2016;42(3):531–551. doi:10.1016/j.rdc.2016.03.010. PMCID: PMC5812283.
- Center for Disease Control and Prevention. CDC Facts About Adult Oral Health. Adult Oral Health. 2020. Accessed May 2022.
- Zero DT, Brennan MT, Daniels TE, et al. Clinical practice guidelines for oral management of Sjögren disease. J Am Dent Assoc. April 2016;147(4):295–305. doi:10.1016/j.adaj.2015.11.008. Epub 2016 January 5.
- Negrini S, Emmi G, Greco M, et al. Sjögren’s syndrome: a systemic autoimmune disease. Clin Exp Med. February 2022;22(1):9–25. doi:10.1007/s10238-021-00728-6. Epub 2021 June 7. PMCID: PMC8863725.
- Donoff RB, Daley GQ. Oral health care in the 21st century: it is time for the integration of dental and medical education. J Dent Educ. September 20, 2020; 84(9):999–1002. doi:10.1002/jdd.12191.
- Bersell CH. Access to oral health care: a National crisis and call for reform. J Dent Hyg. February 2017;91(1):6–14.
- de Lazaro SS, Durben AN, Kline J. Oral health for older adults: policy barriers and opportunities. Innov Aging. December 17, 2021; 5(Suppl 1):954–955. doi:10.1093/geroni/igab046.3420.
- Kwong C, Coffman JM. Oral health workforce and education in California. HealthForce Center at UCSF. July 31, 2020. Accessed May 19, 2022.
- Oral Health Workforce Research Center. Consumer survey of barriers to and facilitators of access to oral health services 2019.
- Emerson S. San bernardino county plan aims to get more residents into the dentist’s chair. The Sun October 7, 2019. Accessed May 19, 2022.
- CDA Cares Treats 1,626 at San Bernardino Clinic. Dent today. October 7, 2019. Accessed May 19, 2022.
- Khairzada Z. 200 UCLA health volunteers hope to bring access to health care in LA. Spectrum News 1. Los Angeles. March 5, 2022. Accessed May 19, 2022.
- Gupta N, Vujicic M. Main barriers to getting needed dental care all relate to affordability. November 2019.
- Yarbrough C, Nasseh K, Vujicic M. Why adults forgo dental care: evidence from a new national survey. ADA Health Policy Institute, November 2014.
- Raphael C. Oral health and aging. Am J Public Health. 2017;107(S1):S44–45. doi:10.2105/AJPH.2017.303835.
- National Institute for Health Care Management Foundation. Oral Health & Health Equity. September 14 2021.
- Mertz EA. The dental-medical divide. Health Aff (Millwood). December 1, 2016;35(12):2168–2175. doi:10.1377/hlthaff.2016.0886.
- Elani HW, Kawachi I, Sommers BD. Dental outcomes after Medicaid insurance coverage expansion under the Affordable Care Act. JAMA Netw Open. September 1, 2021;4(9):e2124144. doi:10.1001/jamanetworkopen.2021.24144. PMCID: PMC8485174.
- California Health Care Foundation. Holding on: how California’s health centers adapted operations and care for patients during the pandemic. February 2021.
- Grisanti SM, Boyd LD, Rainchuso L. An assessment model for evaluating outcomes in federally qualified health centers’ dental departments: results of a 5 year study. J Dent Hyg. August 2015;89(4):247–257.
- Jones E, Shi L, Hayashi AS, Sharma R, Daly C, Ngo-Metzger Q. Access to oral health care: the role of federally qualified health centers in addressing disparities and expanding access. Am J Public Health. March 2013;103(3):488–493. doi:10.2105/AJPH.2012.300846. Epub 2013 January 17. PMCID: PMC3673494.
- Dziedzic A, Tanasiewicz M, Tysiąc-Miśta M. Dental care provision during coronavirus disease 2019 (COVID-19) pandemic: the importance of continuous support for vulnerable patients. Medicina (Kaunas). June 12, 2020;56(6):294. doi:10.3390/medicina56060294. PMCID: PMC7353858.
- London SD, Fontelo P, Boroumand S, Dye BA. COVID-19 provides an opportunity for integration of dentistry into the health informatics system. J Am Dent Assoc. January 2022;153(1):3–8. doi:10.1016/j.adaj.2021.11.003. PMCID: PMC8599016.
- Shanti RM, Stoopler ET, Weinstein GS, et al. Considerations in the evaluation and management of oral potentially malignant disorders during the COVID-19 pandemic. Head Neck. July 2020;42(7):1497–1502. doi:10.1002/hed.26258. Epub 2020 May 16. PMCID: PMC7276902.
- American Dental Association. HPI poll examines impact of COVID-19 on dental practices. April 1, 2020.