

ABSTRACT
Background
Solitary oral mucosal xanthogranuloma, previously termed juvenile xanthogranuloma, is exceedingly rare in adults. Extracutaneous lesions are similarly rarely seen; and the condition generally affects infants and children.
Methods
This case report documents only the second occurrence of an adult oral xanthogranuloma on the palatal mucosa. For the clinician, a differential diagnosis is presented to include several disease categories, including traumatic, infectious/inflammatory, and neoplastic.
Conclusions
General dentists, dental specialists, and pathologists should be cognizant of this disease, and xanthogranuloma should be considered in the differential diagnosis of benign tumors of the palatal and oral mucosa, especially when a histiocytic entity is being considered.
Practical Implications
Dentists, dermatologists, and general practitioners may be the first to recognize this rare condition during inspection of the oral cavity.
Continuing Education Credit Available: The practice worksheet is available online in the supplemental material tab for this article.
A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20
Introduction
Juvenile xanthogranuloma (JXG) is the most common type of non-Langerhans cell histiocytosis (nonLCH) whose cell of origin, etiology, and molecular pathogenesis are not fully understood. The presence of single or multiple raised cutaneous lesions characterizes this benign and self-healing disorder. Extracutaneous sites are rare; and the condition generally affects infants and children, frequently in those younger than 1 year of age.Citation1 In a review of the English literature, reports of oral mucosal adult JXGs are exceedingly rare, having been only eight previously reported cases.Citation1–8 We present a case of solitary oral xanthogranuloma, previously termed juvenile xanthogranuloma, in a 53-year-old Hispanic male on the palatal mucosa. The current case report documents, to our knowledge, only the second occurrence of an adult oral JXG in the palatal mucosa.Citation2 This report presents a differential diagnosis of this palatal lesion to include several disease categories, including traumatic, infectious/inflammatory, and neoplastic. The clinical characteristics of adult oral JXGs are also reviewed. JXG may present variable clinical and microscopic aspects, which leads to a diversity of clinical misdiagnoses. A precise diagnosis of these lesions requires an accurate evaluation of clinical, microscopic, and immunohistochemical features. Dentists, dermatologists, and general practitioners may be the first to recognize this rare condition during the inspection of the oral cavity.
Clinical Presentation
A 53-year-old Hispanic male was referred for evaluation of a lesion on his palate located approximately half-way between the palatal midline and his canine. He reported first noticing the lesion several months prior but attributed it to eating spicy foods. He had noticed the lesion enlarging over the past three months, and denied any history of local pain, trauma, alcohol use, tobacco use, or recreational drug use. The patient’s past medical history was noncontributory; he was not taking any medications and reported no known drug or seasonal allergies. He reported discomfort upon palpation and was concerned with the recent enlargement.
A systemic examination was unremarkable without signs of distress or abnormal vital signs. Intraorally, a solitary, firm, painless, non-tender 8 mm irregularly circumscribed, round, variegated yellow-tan to red-pink smooth-surfaced papule was noted in the space between palatal rugae immediately medial to the right maxillary canine (). The right maxillary lateral incisor was slightly malpositioned, but all the teeth in the quadrant responded normally to both percussion and palpation. Compression of the lesion did not result in pain or exudation, and no sinus tracts or fistulas were noted in the area. Radiographic and periodontal evaluation in the quadrant revealed normal findings, and all teeth tested vital to cold and electric pulp testing.
Figure 1. Clinical photo demonstrating anterior palatal soft tissue lesion filling the space between palatal rugae medial to the right maxillary canine.

Differential Diagnosis
Raised palatal soft tissue masses may originate from a variety of tissue types. Such a palatal swelling likely resulted from focally increased cells and/or extracellular matrix. The cells could represent inflammatory cells (lymphocytes, histiocytic cells, granulomatous inflammation) or neoplastic cells (such as peripheral nerve sheath cells). A nodule of extracellular matrix could feature collagen, elastin, ground substance, or amyloid.
The differential diagnosis of this palatal lesion might include several disease categories: traumatic, infectious/inflammatory, and neoplastic. If there was a history of surgery or trauma, consideration could be made for fibrosis. If infectious, one must consider a bacterial or fungal etiology, such as tuberculosis, syphilis, or Valley Fever. For an inflammatory cause, entities to be considered include a histiocytosis; granulomatous inflammation (orofacial sarcoidosis); or lymphoid. A neoplastic source could include granular cell tumor; schwannoma; neurofibroma; amelanotic melanoma; or lymphoma; and a matrix accumulation consideration might include elastofibroma and amyloid.Citation9–11
Disorders such as Langerhans cell histiocytosis (LCH) are rare but can present as enlargements of the mucosa with greater hyperplasticity in the palatal variants.Citation12 Soft tissue tumors such as a granular cell tumor (GCT) or neurofibroma are infrequent benign neoplasms, but approximately 10% have demonstrated malignant behavior with presentations within the submucosa of the palate.Citation13 Peripheral ossifying fibroma (POF) is a relatively common, reactive inflammatory lesion that can present as hyperplastic soft tissue masses of both the young and old age groups.Citation14 Our lesion’s small size, relative stability, as well as a lack of neurovascular symptoms or surface ulcerations are inconsistent with malignancies; and since palatal mucosa in the area with rugae is devoid of salivary glands, glandular tumors are not included in the differential diagnosis (metastatic adenocarcinoma excluded).
Langerhans cells histiocytosis (LCH) is an abnormal proliferation of dendritic cells and macrophages with a distinct predilection for males.Citation12,Citation15 Although it is frequently an osseous lesion, a significant number of LCH cases have been discovered as erythematous swelling of the maxilla and palate mimicking periodontal disease, mucosal ulcerations, or granulomatous lesions.Citation16,Citation17 LCH frequently can also mimic malignancies with cortical penetration and multifocal co-presentations in skin, lungs, and distal bones.Citation18 Birbeck granules and positive immunohistochemistry for S100 and CD1a are recognized as standard histological diagnostic factors for LCH.Citation12 While some palatal LCH may be visually similar to the lesion present in this patient, LCH is typically a lesion of young age and the lack of osseous involvement here makes it an unlikely candidate.
Soft tissue lesions such as the granular cell tumor (GCT) arise from the submucosal region and, in most cases, present as small, slowly enlarging growths with pain.Citation13 GCT was initially described by Abrikossoff as a glandular cell myoblastoma in 1926 because its cells were thought to derive from myoblasts.Citation19 However, investigators have demonstrated that GCT originates from Schwann cells via S-100 staining, which indicates a neural crest lineage.Citation20 Histopathology shows polygonal cells with eosinophilic granular cytoplasm and small nuclei.Citation21 The most common location for GCT lesions is the head and neck region – especially in the oral cavity including the tongue – which accounts for 50% of cases.Citation21 Still, despite its prevalence in the head and neck, GCTs are uncommonly reported on the palate itself. GCT is also more closely associated with the female gender and African ancestry.
Similarly, neurofibroma is a benign peripheral nerve sheath tumor of irregularly mixed Schwann cells, fibroblasts, and perineural cells.Citation22 They often present in the oral cavity as non-tender, submucosal masses of the tongue, buccal mucosa, vestibule, and gingiva. Neurofibromas occur either as a component of a syndrome (such as von Recklinghausen’s disease of skin and neurofibromatosis type 1 or as isolated entities.Citation23 The current patient did not demonstrate any of the common findings typically seen in patients with neurofibromatosis type 1.
Peripheral ossifying fibroma (POF) is a common, painless, well-demarcated nodule consisting of fibrous tissue and variable amounts of mineralized material mimicking bone.Citation24 POFs can occur at any age but are frequently seen in the maxilla during the second and third decades of life.Citation25 Though painless, they can be caused by irritation from faulty dental restorations, irritating dental appliances, calculus, and plaque. There may also be a genetic predisposition to POF as well. They are nonetheless typically found in female patients and rarely form in the non-tooth-bearing areas such as the palate.
Diagnosis and Management
An excisional scalpel biopsy and curettage of the soft tissue lesion was performed under local anesthesia. Hemostasis was obtained with pinpoint electrocautery. A resorbable collagen dressing was applied, and sutures were placed over the wound. The specimen was then submitted to oral and maxillofacial pathology for histopathologic analysis.
Hematoxylin and eosin sections demonstrated palatal connective tissue with infiltrates of foamy mononuclear macrophages consistent with atypical histiocytes containing xanthomatous cytoplasm and scattered Touton giant cells (). Each Touton giant cell exhibited a wreath of nuclei surrounding a central ellipsoid of pink cytoplasm in a pattern resembling “blueberries stuck on a pink cheese ball” (). Abundant pale foamy cytoplasm also surrounded the wreath of nuclei. Immunohistochemistry was negative for S-100 and CD1a.
Figure 2. Photomicrograph demonstrating foamy histiocytes and scattered Touton giant cells in the lamina propria (hematoxylin & eosin [H&E] x 200).
![Figure 2. Photomicrograph demonstrating foamy histiocytes and scattered Touton giant cells in the lamina propria (hematoxylin & eosin [H&E] x 200).](/cms/asset/87ba4818-1a4b-47a8-a190-76101de22d5e/ucda_a_2221397_f0002_oc.jpg)
Figure 3. Photomicrograph demonstrating a Touton giant cell showing nuclei forming a wreath around a central spherule of pink cytoplasm (“blueberries stuck on a pink cheese ball”). Abundant pale “foamy” cytoplasm surrounds the wreath of nuclei (H&E x 400).
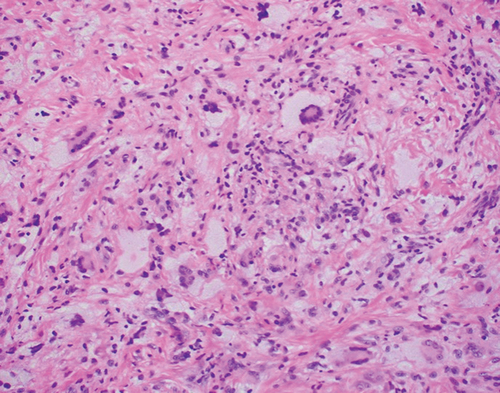
Touton giant cells are characteristic of solitary xanthogranuloma (XG), previously termed juvenile xanthogranuloma. Because the patient lacked evidence of disease elsewhere, a diagnosis of solitary XG was established.
Following complete excision of the lesion, the patient healed uneventfully and has remained disease free for over two years. Recurrence is unlikely as these lesions, once excised, do not tend to recur.
Discussion
XG belongs to a class of rare entities known as non-Langerhans cell histiocytoses (NLCH).Citation26 NLCH are characterized by proliferation of multinucleated Touton giant cells and foamy histiocytes. Out of the NLCHs, extraoral XG may be the most common form present in children.Citation27 XG was commonly called juvenile xanthogranuloma due to its prevalence in early childhood and infancy, with adult cases seldomly noted after the fourth decade.Citation26,Citation28 Touton giant cells can also be seen in Erdheim-Chester disease, a multi-organ myeloid neoplasm that most often affects bone, but can also manifest as cardiac, retro-orbital, retroperitoneal pulmonary, or central nervous system masses. In fact, Erdheim-Chester disease masses of the skull base have resulted in diabetes insipidus as well.Citation29
XG lesions in adults are typically solitary which often go unrecognized. The most common presentations occur on the skin of the face, neck, and upper torso.Citation28 Oral lesions are extremely rare, with approximately thirty histologically proven cases documented in the literature.Citation1,Citation30 They can arise as yellow nodules on the tongue, buccal mucosa, gingiva, or near the midline of the hard palate, and are often associated with bleeding especially upon palpation.Citation28
The etiology of XG is unclear, though the lesion is thought to develop in reaction to unknown external stimuli.Citation31,Citation32 In the current case, the patient reported that the lesion seemed to slowly grow after contact with spicy foods, which may be consistent with this notion. Treatment of choice is excisional biopsy and recurrence is unlikely. Proper and timely recognition of non-pediatric palatal XG may nonetheless prove to be difficult because of its rarity both in the oral cavity and in adulthood. XG should be considered in a differential diagnosis of benign tumors of the buccal mucosa and the palatal region, especially when an entity involving histiocytes is to be considered.
Conclusion
A clinical diagnosis of oral JXG is difficult due to its rare occurrence. Additionally, oral lesions may present a wide range of clinical features, leading to various misdiagnoses, such as a salivary gland tumor. Therefore, a definitive diagnosis of oral JXG relies on a biopsy of the lesion and subsequent histological and immunohistochemical examinations. A biopsy is the treatment of choice for oral JXGs. Spontaneous regression is commonly noted for JXGs of the skin; however, spontaneous regression has not yet been reported for oral JXGs, which may further indicate that surgical excision is the correct treatment modality.
JXGs of the skin are associated with various systemic disorders, including neurofibromatosis type 1, juvenile chronic myeloid leukemia, acute lymphocytic leukemia, LCH, urticaria pigmentosa, diabetes mellitus, solitary mastocytosis, hepatomegaly with anemia and thrombocytopenia, and Neumann-Pick disease.Citation1
To our knowledge, oral JXGs have not been found to be associated with any systemic disorders, as was the case in the current patient. General dentists, dental specialists, and pathologists should be cognizant of this disease, and JXGs should be considered in the differential diagnosis of benign tumors of the palatal and oral mucosa, especially when a histiocytic entity is being considered. Adult oral JXGs are an unusual but recognized condition in which various clinical and histological features may manifest, resulting in a clinical misdiagnosis. A correct diagnosis of this lesion is therefore dependent upon thorough clinical, histological, and immunohistochemical examinations.
Dentists, dermatologists, and general practitioners may be the first to recognize this rare condition during the inspection of the oral cavity. Clinicians and pathologists must recognize JXG to avoid misdiagnoses with oral benign or malignant lesions.
Supplemental Material
Download MS Word (26 KB)Acknowledgments
The authors wish to thank Lee J. Slater, DDS, MS (Staff Pathologist, Scripps Oral Pathology Service, San Diego, CA) and Mario Flores, DDS, MS (Assistant Professor, Department of Periodontics, Loma Linda University School of Dentistry, Loma Linda, CA) for their assistance in the histopathologic evaluation and preparation of the manuscript.
Supplemental data
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2221397.
Additional information
Notes on contributors
Hardev M. Singh
Hardev M. Singh, DMD, MS is an adjunct associate professor of periodontics at the Western University of Health Sciences College of Dental Medicine in Pomona, California. He also maintains a private periodontics practice in Los Angeles County. Conflict of Interest Disclosure: None reported.
Jeffrey A. Elo
Jeffrey A. Elo, DDS, MS is a professor of oral and maxillofacial surgery at the Western University of Health Sciences College of Dental Medicine in Pomona, California; and is a clinical assistant professor in the department of oral and maxillofacial surgery at the Loma Linda University School of Dentistry in Loma Linda, California. He is a fellow in the American College of Surgeons, American College of Dentists, and International College of Dentists. Conflict of Interest Disclosure: None reported.
Yoon-Jeong Kim
Yoon-Jeong Kim, DDS, MS is a professor and chair of the department of periodontics and is the program director for advanced education in periodontics at the Loma Linda University School of Dentistry in Loma Linda, California. Conflict of Interest Disclosure: None reported.
Ho-Hyun (Brian) Sun
Ho-Hyun (Brian) Sun, DMD, MS is a clinical assistant professor of oral and maxillofacial surgery at the Western University of Health Sciences College of Dental Medicine in Pomona, California, and a clinical instructor in the department of oral and maxillofacial surgery at the University of the Pacific Arthur A. Dugoni School of Dentistry. He practices in an oral surgery private practice in San Jose, California. Conflict of Interest Disclosure: None reported.
References
- Consolaro A, Sant’ana E, Lawall MA, et al. Gingival juvenile xanthogranuloma in an adult patient: case report with immunohistochemical analysis and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(2):246–5. doi:10.1016/j.tripleo.2008.09.032.
- Takeda Y, Suzuki A, Fujioka Y, et al. Xanthogranuloma of the oral cavity in adult. A case report and review of the literature. Acta Pathol Jpn. 1986;36(10):1565–1570. doi:10.1111/j.1440-1827.1986.tb02827.x.
- Satow SJ, Zee S, Dawson KH, et al. Juvenile xanthogranuloma of the tongue. J Am Acad Dermatol. 1995;33(2):376–379. doi:10.1016/0190-9622(95)91438-2.
- Tanyeri H, Weisenberg E, Friedman M. Juvenile xanthogranuloma of the tongue. Otolaryngol Head Neck Surg. 2000;123(5):641–642. doi:10.1067/mhn.2000.109661.
- Fabrizi G, Massi G. Mononuclear variant of juvenile xanthogranuloma in the oral cavity of an adult patient. Br J Dermatol. 2001;144(4):909–911. doi:10.1046/j.1365-2133.2001.04161.x.
- Usmani N, Yung A, Merchant W. An unusual nodular lesion. Clin Exp Dermatol. 2006;31(4):607–608. doi:10.1111/j.1365-2230.2006.02156.x.
- Costa F, Cian R, Robiony M, et al. Unilateral swelling of the cheek. J Oral Maxillofac Surg. 2008;66(2):342–348. doi:10.1016/j.joms.2007.04.030.
- Chen C-Y, Sung C-L, Hsieh M-Y, et al. An adult juvenile xanthogranuloma in the buccal mucosa. J Dent Sci. 2015;10(3):334–337. doi:10.1016/j.jds.2013.02.028.
- Darling MR, Kutalowski M, MacPherson DG, Jackson-Boeters L, Wysocki GP. Oral elastofibromatous lesions: a review and case series. Head Neck Pathol. 2011;5(3):254–258. doi:10.1007/s12105-011-0274-y.
- Nonaka CFW, Rêgo DM, da Costa Miguel MC, et al. Elastofibromatous change of the oral mucosa: case report and literature review. J Cutan Pathol. 2010;37(10):1067–1071. doi:10.1111/j.1600-0560.2010.01576.x.
- Pontes HAR, de Souza LL, Rodrigues-Fernandes CI, et al. A nodule in the palatal mucosa. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130(5):473–477. doi:10.1016/j.oooo.2019.05.006.
- Altay MA, Sindel A, Özalp Ö, et al. Langherhans cell histiocytosis: a diagnostic challenge in the oral cavity. Case Rep Pathol. 2017;2017:1691403. doi:10.1155/2017/1691403.
- Boulos R, Marsot-Dupuch K, De Saint-Maur P, et al. Granular cell tumor of the palate: a case report. Am J Neuroradiol. 2002;23(5):850–854.
- Cuisia ZE, Brannon RB. Peripheral ossifying fibroma–a clinical evaluation of 134 pediatric cases. Pediatr Dent. 2001;23:245–248.
- Divya KS. Oral manifestation of Langherans cell histiocytosis mimicking inflammation. Indian J Dent Res. 2014;25(2):228–230. doi:10.4103/0970-9290.135930.
- Morimoto A, Oh Y, Shioda Y, et al. Recent advances in Langerhans cell histiocytosis. Pediatr Int. 2014;56(4):451–461. doi:10.1111/ped.12380.
- Aricò M, Girschikofsky M, Généreau T, et al. Langherhans cell histiocytosis in adults. Report from the international registry of the histiocyte society. Eur J Cancer. 2003;39(16):2341–2348. doi:10.1016/S0959-8049(03)00672-5.
- Pan Z, Xu ML. Histiocytic and dendritic cell neoplasms. Surg Pathol Clin. 2019;12(3):805–829. doi:10.1016/j.path.2019.03.013.
- Kamal SA, Othman EO. Granular cell tumour of the larynx. J Laryngol Otol. 1998;112(1):83–85. doi:10.1017/S0022215100139970.
- Holland RS, Abaza N, Balsara G, et al. Granular cell tumor of the larynx in a six-year-old child: case report and review of the literature. Ear Nose Throat J. 1998;77(8):652–4,656,658. doi:10.1177/014556139807700814.
- Victoria LV, Hoffman HT, Robinson RA. Granular cell tumour of the larynx. J Laryngol Otol. 1998;112(4):373–376. doi:10.1017/S0022215100140502.
- Messersmith L, Krauland K. Neurofibroma. [Updated 2022 Aug 15] In: StatPearls. Treasure Island (FL): StatPearls Publishing; January, 2023.
- Marocchio LS, Oliveira DT, Pereira MC, et al. Sporadic and multiple neurofibromas in the head and neck region: a retrospective study of 33 years. Clin Oral Investig. 2007;11(2):165–169. doi:10.1007/s00784-006-0096-6.
- Buchner A, Hansen LS. The histomorphologic spectrum of peripheral ossifying fibroma. Oral Surg Oral Med Oral Pathol. 1987;63(4):452–461. doi:10.1016/0030-4220(87)90258-1.
- Agarwal P, Chug A, Kumar S, et al. Palatal peripheral ossifying fibroma: a rare occurrence. Int J Health Sci (Qassim). 2019;13(4):63–66.
- Weitzman S, Jaffe R. Uncommon histiocytic disorders: the non-Langerhans cell histiocytoses. Pediatr Blood Cancer. 2005;45(3):256–264. doi:10.1002/pbc.20246.
- Janssen D, Harms D. Juvenile xanthogranuloma in childhood and adolescence: a clinicopathologic study of 129 patients from the kiel pediatric tumor registry. Am J Surg Pathol. 2005;29(1):21–28. doi:10.1097/01.pas.0000147395.01229.06.
- Collins L, Banks R, Robinson M. Juvenile xanthogranuloma: unusual intraoral finding. Br J Oral Maxillofac Surg. 2015;53(1):86–88. doi:10.1016/j.bjoms.2014.09.014.
- Estrada-Veras JI, O’Brien KJ, Boyd LC, et al. The clinical spectrum of Erdheim-Chester disease: an observational cohort study. Blood Adv. 2017;1(6):357–366. doi:10.1182/bloodadvances.2016001784.
- Sánchez-Romero C, Cuenca Arriaga AI, de Almeida OP, et al. Oral juvenile xanthogranuloma in a child: clinical, histological and immunohistochemical profile of a rare entity. J Cutan Pathol. 2018;45(7):515–521. doi:10.1111/cup.13152.
- Paxton CN, O’Malley DP, Bellizzi AM, et al. Genetic evaluation of juvenile xanthogranuloma: genomic abnormalities are uncommon in solitary lesions, advanced cases may show more complexity. Mod Pathol. 2017;30(9):1234–1240. doi:10.1038/modpathol.2017.50.
- Mota CP, Silva Cunha JL, Magalhães MCSV, et al. Oral Juvenile Xanthogranuloma: a clinicopathological, immunohistochemical and BRAF V600E study of five new cases, with literature review. Head Neck Pathol. 2022;16(2):407–415. doi:10.1007/s12105-021-01373-x.