

ABSTRACT
Background
Understanding the implications of aging on endodontic treatment is important to appropriately care for patients with increasingly complex and diverse health needs in conjunction with increasingly intact and complex dentition.
Types of Studies Reviewed
Content from existing studies and literature on aging, oral health and endodontics was reviewed and integrated to present a holistic approach to endodontics for older adults. The full spectrum of need and ability of older adults, from well to frail elders, was taken into consideration.
Results
Age-related changes in the dentition present challenges to endodontic diagnosis and treatment that are compounded by physical or cognitive impairments that alter presentation of disease and response to treatment. Communication may need to extend beyond the patient and the referring provider to establish a diagnosis, clear expectations and goals of treatment.
Practical Implications
It is important to understand the complexities unique to aging and aging’s potential impact on clinical outcomes to ensure the appropriate inclusion and delivery of endodontic care to older adults.
Continuing Education Credit Available
The practice worksheet is available online in the supplementary material tab for this article. A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20.
Introduction
Projections show that the population aged 60 and older in California will grow more than three times as fast as the total population from 2010–2060. More than 50% of the state’s counties will experience more than a 100% increase, over 40% of the counties will increase by more than 150%, and four counties, Merced, Riverside, San Bernardino, San Joaquin, and Santa Clara, are expected to increase their population of adults aged 60 and older by more than 200%. The fastest increases, however, are occurring in the population that is 85 and older, with more than 40% of counties at more than 400% increase during this time period.Citation1 This significant shift toward an aging population will invariably result in an increase in older patients seeking dental care.
The current generation of those over 60 has benefited from improved oral health care. As a result, they have maintained more of their dentition than any generation before. They have different expectations and values around oral health as they age, with a greater focus on maintenance, prevention, minimally invasive care and restoration of their existing dentition instead of opting for extractions and replacement of teeth with prostheses.Citation2 Root canal therapy will be essential for many older adults to retain their natural dentition into old age.
Despite the significant decrease in edentulism, significant risks to oral health remain for aging older adults. Many of the chronic diseases and medications common to older adults also place oral health at risk. For example, caries can result from many medications that cause diminished salivary flow and physical and cognitive disabilities that may impair daily oral hygiene or routine access to care. Lack of money or insurance for routine care (which is a reality for many older adults, particularly those in retirement) can also place patients at risk, with diagnosis delayed until some acute event occurs.Citation3 Delayed treatment of caries can result in the need for endodontics. Some older adults may have increased risk of falls due to systemic conditions,Citation4 and unfortunately, some may experience abuse or neglect. Both of these situations could potentially result in maxillofacial trauma with pulpal involvement.Citation5
While we have constructs to assign someone as being older or old, such as landmark birthdays (50 years), retirement age (65 years) and advanced age (85-plus years), the number itself often has less relevance to oral health needs and ability to receive and tolerate dental care than health status and the presence of any level of dependence.Citation6 There is no typical older person, as there is great variability in physical and cognitive ability among older adults. So-called well-elders may benefit from and tolerate root canal therapy, as well as young people, but someone with multiple co-morbidities and/or moderate-to-high dependency may be less able to tolerate and respond to dental care including endodontic treatment, regardless of age.Citation6 Chronological age alone should not be the basis for treatment planning. Considering age and life expectancy alone, root canal therapy and restoration for an 80-year-old patient could be perceived by some as superfluous. However, if the patient reaches 90 years old and the tooth remains functional and disease free, then the previously considered extraneous treatment would be demonstrably valuable. By the same token, a frail individual who was able to receive treatment may derive a great deal of value, benefit to overall health and quality of life from the opportunity to retain their own dentition and be pain- and disease-free.Citation7 The value of oral health care cannot be viewed solely from the lens of expected or even actual longevity.Citation8 All older adults deserve the most appropriate care to achieve ideal treatment outcomes that meet their oral health needs and values. This article will review the implications for endodontics that result from or in tandem with normal age-related changes and commonly occurring diseases and conditions as well as strategies to overcome challenges in diagnosis, treatment planning and patient care.
Benefits of Root Canal Therapy Across the Spectrum: Well-To-Frail Older Adults
Retaining teeth with root canal therapy allows for the restoration of oral function and maintenance of proprioception for optimal oral motor function.Citation9,Citation10 Tooth extraction and removable prostheses is often a default treatment plan for older adults, especially those who are viewed as elderly or frail. However, tooth loss significantly impairs masticatory performance, and proprioception may be lost.Citation7 Maintenance of proprioception and functional dentition is especially beneficial to those with oral motor dysfunction that may arise from a history of stroke or the presence of progressive diseases such as multiple sclerosis or Parkinson’s Disease.Citation11 Furthermore, the long-term success of both fixed and removable prostheses relies on sound and adequate numbers of abutment teeth that may also be dependent on the receipt of appropriate endodontic treatment. In some cases, teeth that may otherwise be extracted in a younger patient may be functionally important and essential to retain. For example, endodontic treatment of a third molar may not normally be considered. However, if it is essential for the retention of a prosthesis, saving it with root canal therapy would be of great functional importance. The option for endodontics to maintain over-denture abutments or to maintain a shortened dental arch should not be overlooked, especially for individuals who cannot, do not want or cannot afford to have implants.Citation12 Root canal therapy may also be necessary for patients with endodontically involved teeth that cannot be extracted due to a high risk of osteoradionecrosis or medication-related osteonecrosis of the jaws (MRONJ).
Natural dentition allows for the maintenance of chewing function and the ability to eat nutritious food such as fresh fruits and vegetables. With diminished chewing function, food choices often become less healthy as individuals choose more highly processed foods that are easier to chew but also pose a systemic and oral health risk.Citation13 The maintenance of a patient’s natural dentition is also beneficial for psychosocial well-being. Loss of self-confidence and the stigma of aging as a consequence of tooth loss can affect older adults, potentially contributing to social isolation and withdrawal.Citation14,Citation15 Maintenance of the dentition with endodontics can improve health, emotional well-being and quality of life for many older adults.Citation16,Citation17
Goals of Endodontic Treatment
The goal of root canal therapy for older and younger patients is to retain the natural tooth by eliminating the source of infection, preventing reinfection and creating an environment that will allow healing of the peri-radicular tissue.Citation18 The success rate of root canal therapy for older patients is the same as for younger patients. Two systematic reviews found that age had no effect on the outcome of root canal therapy.Citation19,Citation20
Considerations in Root Canal Therapy for Older Adults
Although the steps and goals of root canal therapy are similar between young and old, dependency or advanced age may result in treatment challenges unique to these populations. The stress and anxiety associated with dental treatment, especially root canal therapy, should be minimized for every patient, but this consideration is of particular importance in frail elderly patients and patients with medical problems who have a decreased capacity to cope with stress.Citation21 A critical factor in providing an anxiety-free situation is the relationship established among the dentist, the office staff, and the patient. Good communication establishes trust and tends to reduce patient anxiety. This often leads to better patient experiences and fewer misunderstandings, complaints, and potential legal issues.Citation22,Citation23 Age-related changes in hearing and vision are normal and can result in older adults needing more time to process information. An estimated one-third of those between 65 and 74 years have some degree of hearing loss.Citation24 For those patients who read lips, making eye contact, removing the face mask (if possible), and facing the patient when speaking improves communication. (). For patients with hearing and vision impairment, be aware of issues such as excessive noise, distractions, glare, or poor lighting that may hamper communication.Citation23
Figure 1. Take the time to communicate with the patient speak directly to patients and maintain eye contact. Remove mask if possible as patients may read lips. Picture courtesy of Jon Draper, Dugoni School of Dentistry.

Some 16–20% of older adults experience mild cognitive impairment.Citation25 Those with short-term memory issues will benefit from written materials to review in between visits. They may also benefit from someone accompanying them who can act as an advocate and reservoir of information. As with any patient, confirm with them a mutual understanding of the procedure to be performed. Whether an older adult has full physical and cognitive capacity, mild cognitive or physical impairments or are highly dependent, they should be spoken to directly.Citation26 Do not speak over them to a family member, friend, caregiver or even surrogate decision-maker who may accompany them to their appointment. If it is not clear to you if the patient has capacity to consent and/or who may give consent, consult with their primary care provider.Citation11
Older patients with some kinds of physical of cognitive impairments such as altered speech from a stroke or Parkinson’s disease may require more time to listen and respond to your questions. Do not attempt to finish sentences or try to guess what they will say.Citation23 While these kinds of actions may seemingly save time in the moment, they undermine establishing a connection and sense of trust. Extra time spent establishing clear communication and conveying understanding, empathy and compassion is critical, so schedule accordingly.
Diagnosis
The first step of any treatment is to arrive at a diagnosis. Challenges with the diagnostic process are due to communication challenges, the presence of heavily restored teeth, and age-related changes in the pulp. Cognitive deficits can further complicate diagnosis. Someone with dementia may not be able to articulate their symptoms and may not understand how to respond to the objective tests performed by the dentist.Citation11
Clinicians use the results of pulp sensibility tests (thermal and electric tests) to determine whether the pulp is normal, inflamed, or necrotic.Citation27 The results are based on feedback received from the patient. The results are therefore only as good as the patient’s cooperation and accurate reporting of sensation or lack of sensation. In addition to communication challenges, sensibility tests have been shown to be less accurate for patients who are over age 50.Citation28 Normal age-related changes in the pulp tissue resulting in more fibrous and less cellular composition may diminish sensation in the dentition and contribute to the diagnostic challenge. Using a combination of tests, clinicians need to combine the subjective and all objective data and integrate this with their clinical expertise and experience to arrive at an accurate diagnosis. A study by Weisleder et al. concluded that the use of both the cold test and EPT resulted in a more accurate pulpal diagnosis.Citation29 Unfortunately, the use of EPT may be unsuitable in many cases as teeth may be restored with full coverage restorations and tooth structure may be unavailable for placement of the probe directly on tooth structure.
Diagnosis can further be complicated by age-prevalent diseases or conditions. For example, someone who had a stroke and lost sensation in some part of their mouth would not have the usual sensation to pathosis of endodontic origin or to pulp testing.Citation11 Individuals with chronic pain who regularly take pain medications may be at risk for covering their symptoms. The pain medication may also interfere with the diagnostic testing.Citation30 Additionally, the incidence of orofacial pain is higher in the elderly. When the symptoms and objective tests are inconclusive, orofacial pain should be on the list of differential diagnosis and the patient may need referral to an orofacial pain specialist.Citation31
Treatment Planning
Once a diagnosis is established, there are several considerations in treatment planning. Issues of dependency should be considered along with any complications or treatment modifications that will be needed as a result of any diseases or treatment the patient may be receiving. The AAE Endodontic Case Difficulty Assessment Form and GuidelinesCitation32 serves as a valuable resource for assessing preoperative cases and identifying the likelihood of complication during endodontic treatment. Conditions listed on this form, such as a complex medical history, limited ability to open the mouth, and canal visibility, are potential risk factors that may complicate treatment and lead to a diminished prognosis or adverse outcome.
Restorability of the tooth and proper isolation with a rubber dam are required for successful and safe root canal therapy. If the ability to achieve this is questionable, then root canal therapy may not be a feasible option. If the patient was referred to a specialist, this needs to be discussed with the referring dentist, as the goals of treatment and the final restoration are critical components of the treatment following root canal therapy.Citation33 A holistic approach to patient care is essential.Citation34
Other factors that impact a patient’s ability to tolerate or benefit from endodontic treatment may be less definitive or obvious and can present a challenge when determining an appropriate course of treatment. The Seattle Care Pathway (SCP) is an evidence-based approach to treatment planning for older adults.Citation6 This approach is based not just on medical complexity, but also on dependency. The elements of risk assessment, prevention, treatment considerations and communication are considered in detail and can be applied to endodontic treatment planning, case selection and delivery of care. Integrating the level of difficulty from the AAE Case Difficulty Form with the considerations addressed in SCP can enhance a clinician’s ability to consider the patient’s total needs. As an example, endodontic cases that are determined to be of low complexity in a patient assessed to be in no dependency or pre-dependent status would likely qualify for all endodontic and restorative treatment options; those patients with a high complexity endodontic case who are also highly dependent are likely be managed by palliative measuresCitation6 (See for applications).
Table 1. Endodontic considerations using the Seattle Care Pathway (SCP) as a Framework.(Petty et al, Robbins, Innes, deBaat, Murphy, Baumgartner, Rajeswari)
Patient Comfort
If a decision is made to proceed with treatment, consider that cognitive decline is often associated with apprehension and anxiety when patients are subjected to unfamiliar treatment, which could result in the patients becoming resistant to care and difficult to treat.Citation35
Benzodiazepines are often used to achieve anxiolysis to allow the provision of necessary care. In the elderly, triazolam, lorazepam, and oxazepam have properties that are most desirable. They are all short acting and have no active metabolites.Citation36 Inhalation sedation has been shown to also be very effective in reducing anxiety and stress in the elderly patient.Citation37
Many older patients require a semi-supine position and cannot be placed in a supine position.Citation34,Citation38 This may be due to systemic issues, such as COPD or congestive heart failure, or arthritis and joint pain. Providing patients with pillows or a bite block for support and comfort, shorter appointments and frequent breaks may allow root canal therapy to proceed comfortably. A dental office may be too cold for some older individuals. Offering blankets or other coverings to keep help keep the patient warm is a simple measure to ensure comfort and reduce disruptions in treatment. Some patients taking diuretics or with prostate issues may require frequent bathrooms breaks. Communicating with the patient during the procedure to assure they are comfortable and able to continue will reduce the patient’s emotional and physical stress.
Intra-Operative Pain Management
Pain control during and after an endodontic procedure is a vital aspect of patient care. The anticipation of pain and the actual experience of pain and discomfort during treatment can be detrimental in the elderly patient population as their capacity to cope with stress can be diminished. Notably, patients with significant cardiovascular disease (hypertension, dysrhythmias, heart failure, valvular insufficiency, or congestive heart disease) require excellent pain control to avoid the release of endogenous epinephrine in response to stress from pain or anxiety.Citation39
Profound local anesthesia is essential in dental treatment. However, for elderly patients, this should be achieved with consideration of lower doses than for otherwise healthy adult patients. Older patients may be at increased risk for excessive, and thereby toxic, local anesthetic blood levels due to decreased liver function, lowered plasma protein binding, and other age-related changes that affect drug distribution and biotransformation of the local anesthetic.Citation38 As the elimination half-life of amide local anesthetics is usually significantly increased in the presence of decreased liver function, it is advisable to stay well below the FDA-published maximum dosing recommendation.Citation40 This is especially important for elderly patients weighing less than a normal adult patient or less than 100 pounds. The “rule of 25” from pediatric dentistry is easy to remember for determining a safe dose of anesthetics intended for the older patient population who may present with a body weight below ideal: 1 cartridge (1.7 ml) of any anesthetic formulation can be administered safely for every 25 pounds of a child’s body weight.Citation41 The maximum recommended dose by weight should always be calculated for pediatric patients, medically compromised patients, and elderly patients.Citation42
The vasoconstrictor epinephrine is added to local anesthetics to increase the duration and depth of anesthesia. It also reduces the blood level of the anesthetic by slowing the rate of absorption from the area of injection into the surrounding vasculature from adrenergic-mediated vasoconstriction. However, the safe use of epinephrine for patients with cardiovascular disease due to the vasoconstrictor’s transient effect on increasing arterial pressure and heart rate must be considered for patients unable to tolerate these stressors. Balancing the risk of epinephrine with the importance of profound anesthesia is essential. Malamed recommends the use of epinephrine up to 0.040 mg as generally safe for elderly patients and those with cardiovascular disease, although specific patient considerations may preclude the use altogether of local anesthetics formulated with epinephrine.Citation43,Citation44 In most instances, the enhanced clinical effect of local anesthesia with the addition of epinephrine will help prevent increased stress and the release of endogenous catecholamines in amounts that exceed those in the local anesthetic. Frequently, angina, arrhythmias, and acute stress reactions (tremor, nausea and vomiting, and shortness of breath) have a higher incidence in the stressed, poorly anesthetized patient with cardiovascular disease. These events are less likely to occur in relaxed well-anesthetized patients with cardiovascular disease.Citation45
In situations where the dental provider is concerned about the use of epinephrine in local anesthetics, a consultation with the patient’s physician is warranted to gather information on formulating an appropriate clinical treatment plan. Providing relevant and sufficient therapeutic information to the consultant physician, such as the amount of epinephrine to be administered and reason for use, are critical. For example, a dentist may send a consultation to inquire if an elderly patient’s condition is stable enough to tolerate transient increases in heart rate and blood pressure for 5–10 minutes with anywhere from 0.017 mg to 0.040 mg of epinephrine used in dentistry. The consultant may also be able to recommend strategies for peri-operative stress reduction as well as postoperative pain control recommendations.
Access
Coronal access represents the most challenging treatment aspect of a calcified tooth. Access into the pulp chamber of teeth of older patients is challenging due to the receded pulps and presence of full coverage restorations () Reviewing a cone beam computed tomography image (CBCT) prior to treatment can assist in finding the location of calcified canals or a calcified pulp chamber. The three-dimensional CBCT information guides the operator in the approach, depth, and direction of the access.Citation46
Figure 2. Note calcified chamber of #19. Difficult case to access.

Figure 3. Teeth #24 and #25 are necrotic. Canal is visible toward apical third. Consider guided access.
Although a rubber dam must be used during root canal therapy, in cases where access will be difficult, it is beneficial to place the rubber dam after access has been achieved. The orientation of adjacent teeth may help guide the access, and the absence of a clamp will make any radiographs necessary for guidance with access easier to evaluate and to direct the access. In certain instances, an intra-appointment CBCT may also be necessary to assess the approach of the access.Citation47
A few tips on locating calcified canals are listed below. All of these techniques require magnification and illumination, and most will require the use of various burs and ultrasonic tips that are designed for performing the deep troughing required to locate and enter calcified pulp chambers and canals.
Use a sharp DG16 Endo Explorer to detect small canal orifices. The canal orifice is often softer to the probing than the surrounding dentin.Citation48
Place NaOCl in the chamber to detect bubbles emerging from a calcified canal.Citation47 The bubbles are due to the oxygenation of the pulp tissue when it reacts with NaOCl.Citation48,Citation49
Use a fiberoptic light at the level of the CEJ to transilluminate the tooth from the buccal or lingual, which can help discriminate between the dentinal color of the orifice and the floor of the pulp chamber and help in locating the canal.Citation47 It is beneficial to turn off any overhead light source during transillumination.
Use methylene blue dye to identify canals.Citation49
For an efficacious approach in a multi-canal tooth, enlarge the orifice of any canal found before searching for the other canals. The enlarged orifice helps with the orientation, and the now discernable dentinal map (the dark developmental lines connecting canal orifices) helps guide the operator to the other canals.Citation48
To assure a canal was located while searching as opposed to the creation of a perforation, a small file can be attached to the apex locator and placed a few millimeters inside the canal. A reading of “apex” would indicate a perforation.Citation50,Citation51 A smaller perforation that can be quickly repaired improves the prognosis for the tooth.Citation47 However, before any files are used, the rubber dam must be placed if it was not placed prior to access.
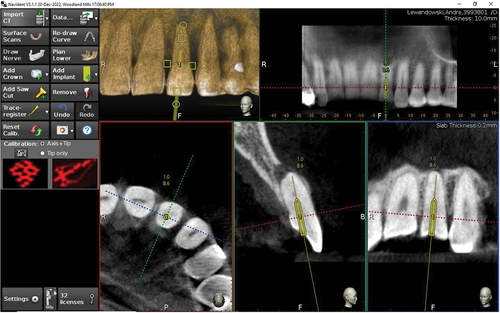
Guided Access
Guided endodontics is a relatively new approach to access calcified teeth. There are currently two methods for guided access, both utilizing CBCT images.Citation52 The static guided approach uses a 3D printed guide that covers the tooth to be accessed and is designed with a drill hole that allows direct access to the calcified canal. () The dynamic navigation system provides real time visualization and guidance during endodontic access preparation utilizing the CBCT and spatial positioning technology. () Once the canal is accessed with the aid of either technique, conventional root canal treatment can continue.
Figure 4. Splint for guided access. Arrow points to guide for bur. Picture courtesy of Dr. David Kelliny.
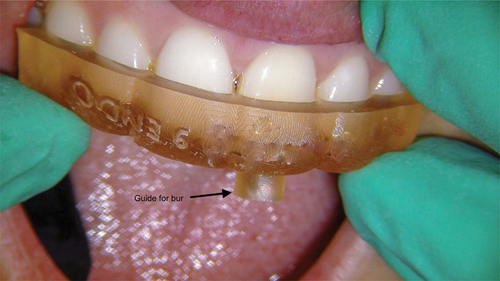
Figure 5. Real time orientation of bur drill path with a dynamic navigation system. Picture courtesy of Dr. Sameer Jain.
Rubber Dam Placement
The rubber dam is the standard of care when performing root canal therapy.Citation53 The placement of the rubber dam may be challenging on some teeth, but below are some tips to simplify the process.
Place the rubber dam as one unit, together with the clamp and frame, to minimize the risk of the clamp falling into the patient’s mouth. In addition to safety, this approach is also easier because the dam remains taut and is thus easier to place.
For teeth that are prepped for crowns or badly broken down, use a butterfly clamp with the beaks close together to easily secure the tooth.
Add composite or GI to the buccal and lingual of teeth to help secure the clamp when there is no height of contour (undercut) on the crown.
Use cyanoacrylate to secure the rubber dam when it is not possible to place a clamp on a tooth.Citation54
Establishing Working Length
Cementum continues to be formed throughout life, especially in the apical half of the root, resulting in a gradual increase in thickness. The increased thickness of cementum results in increased distance between the foramen and the radiographic apex. This alteration in the apical anatomy associated with aging affects the radiographic perception of the working length. In advanced age, there may be a discrepancy between the location of the apical constriction as determined by the electronic apex locator (EAL) and the radiographic appearance. Although the working length may appear to be short of the apical constriction, the EAL should be trusted to avoid over instrumentation and extrusion of material due to the known anatomical changes in the apical area.Citation55
A CBCT may also eliminate the need for intraoperative radiographs, expediting the treatment, decreasing radiation exposure and alleviating challenges posed by intra-appointment radiographs, especially with the elderly.Citation56,Citation57,Citation58
Restoring the Endodontically Treated Tooth
The type of final restoration of the endodontically treated tooth is at the discretion of the restorative dentist. The endodontic referral should be as clear and informative as possible to minimize any misunderstanding regarding the proposed treatment plan. If new information affecting outcome is elucidated during treatment, a recommendation for the final restoration can be made by the endodontist upon consultation with the referring dentist. Both the endodontic treatment and restorative treatment are necessary to maintain the tooth, and this requires coordination and good communication between both providers.
Postoperative Pain Management
Postoperative pain management should be carefully evaluated relative to potential drug-drug interactions and the physiological effect of aging on drug pharmacokinetics. Hepatic and renal function can be significantly decreased with age and may affect the ability to metabolize and eliminate medications. Some drug interactions may hinder or augment enzymatic activity of the liver too. NSAIDs are commonly prescribed to treat acute pain associated with inflammation. However, NSAIDS should be used with caution in the elderly and for limited duration (<5 days). Common adverse effects in the elderly associated with NSAIDs include gastrointestinal bleeding, renal impairment, and even heart failure with the reduction in circulating prostaglandins.Citation58
Acetaminophen is considered the drug of choice for mild to moderate dental pain in the elderly.Citation59 Generally considered to have minimal side effects with low to usual dosing, acetaminophen is associated with few drug interactions. However, patients with significant hepatic compromise should be carefully evaluated before acetaminophen administration as even normal adult dosing can cause liver damage. Opioid analgesics should be used sparingly for dental pain management in elderly patients. Opioid analgesics are associated with common side effects such as sedation, nausea, constipation, and most significantly, respiratory depression. These side effects are often exaggerated in the geriatric patient.Citation59
Antibiotics
When antibiotics are indicated, comorbidities and potential drug interactions must be considered. Beta-lactam-based antibiotics (primarily 500 mg amoxicillin three times per day) are the first choice for adjunct treatment of endodontic infections. For patients with a penicillin allergy, the primary alternative is now azithromycin.Citation60 Clindamycin is only indicated if there is a contraindication to azithromycin. Fortunately, azithromycin has less drug interactions than other macrolides such as clarithromycin or erythromycin.Citation38 However, caution should be used when prescribing azithromycin to patients on statins as azithromycin may increase the plasma level of the statin drugs.Citation61 There is also a potential for an increase in digoxin levels when a macrolide is prescribed. The anti-coagulant effect of warfarin may be increased by several antibiotic classes, but cephalosporins, macrolide antibiotics, and metronidazole have the most effect. Penicillin combined with a beta lactamase inhibitor such as Augmentin has a much higher incidence of increasing the risk of bleeding than penicillin with a narrower spectrum.Citation61
Conclusion
With increasing retention of teeth and greater expectations for oral health among baby boomers and the generations that follow, endodontic treatment is increasingly necessary and valuable for older adults and even some frail older adults. Dental prognoses must be considered in terms of both the prognosis for the tooth to be treated as well as the patient’s ability to tolerate, and the likelihood of benefitting from, the treatment provided. Rather than considering age alone, the patient’s general health, the presence or absence of physical or cognitive disability, and the potential impact on their ability to receive treatment should be the principle determinants for treatment planning. Effective communication, high level of clinical skills, and patient-centric treatment planning are critical for successful outcomes of endodontic treatment for patients with increasing dental and medical complexity at any age.
Supplemental Material
Download MS Word (38.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary data
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2263937.
Additional information
Notes on contributors
Yaara Berdan
Yaara Berdan, DDS, MBA, is an associate professor of clinical dentistry and Co-Chair of the Department of Endodontics and Periodontics at the Herman Ostrow School of Dentistry of USC. Following graduation from the University of California, San Francisco (UCSF), she completed a Pediatric Residency Program at Children’s Hospital Boston and practiced pediatric dentistry in the Boston area for a couple of years. She earned her certificate in endodontics from the University of Illinois at Chicago and returned to Los Angeles where she practiced endodontics until 2008 when she began teaching at Ostrow. She is active in the American Dental Education Association (ADEA) where she represents the Endodontics Section on the Council of Sections and is the Chair of the Sustainability in Dentistry Special Interest Group. She has lectured locally and nationally in the field of endodontics. She is a fellow of the American College of Dentists and the International College of Dentists. She received her MBA from the USC Marshall School of Business.
Elisa M. Chávez
Elisa M. Chávez, DDS, is a Professor in the Department of Diagnostic Sciences at the Arthur A. Dugoni School of Dentistry, San Francisco. She graduated from The University of California San Francisco, School of Dentistry and earned her certificate in Geriatric Dentistry from The University of Michigan, Ann Arbor. Dr. Chávez has practiced in private, community health, long-term care and hospital settings including Centro de Salud Familiar La Fe in her hometown of El Paso Texas, The Veteran’s Administration in Ann Arbor, Michigan, The Jewish Home for the Aged in San Francisco and On Lok PACE in the Bay Area. She has served on the California Dental Association Medicare Task Force and as a member of The Santa Fe Group she is an advocate for the oral health needs of older adults nationwide. She currently serves as the Director of the Pacific Center for Equity in Oral Health Care. (https://dental.pacific.edu/dental/faculty-and-research/research-facilities/pc)
References
- California Department of Aging. Facts about california’s elderly. California Department of Aging. https://aging.ca.gov/Data_and_Reports/Facts_About_California%27s_Elderly/. Accessed April 9, 2023.
- Innes NPT, Chu CH, Fontana M, et al. A century of change towards prevention and minimal intervention in cariology. J Dent Res. 2019;98(6):611–10. doi:10.1177/0022034519837252.
- A report from the National Institutes of Health: oral Health in America: advances and challenges, section 3B: oral Health Across the Lifespan: older adults. 3B–83. 2021. https://www.nidcr.nih.gov/sites/default/files/2021-12/Oral-Health-in-America-Advances-and-Challenges.pdf#page=411.
- de Baat C, de Baat P, Gerritsen AE, Flohil KA, van der Putten GJ, van der Maarel-Wierink CD. Risks, consequences, and prevention of falls of older people in oral healthcare centers. Spec Care Dent. 2017;37(2):71–77. doi:10.1111/scd.12212.
- Murphy K, Waa S, Jaffer H, Sauter A, Chan A. A literature review of findings in physical elder abuse. Can Assoc Radiol J. 2013;64(1):10–14. doi:10.1016/j.carj.2012.12.001.
- Pretty IA, Ellwood RP, Lo EC, et al. The Seattle care pathway for securing oral health in older patients. Gerodontology. 2014;31(Suppl 1):77–87. doi:10.1111/ger.12098.
- Baumgartner W, Schimmel M, Müller F. Oral health and dental care of elderly adults dependent on care. Swiss Dent J. 2015;125(4):417–426. PMID: 26169068.
- Hall A. Quality of life and value assessment in health care. Health Care Anal. 2020;28(1):45–61. doi:10.1007/s10728-019-00382-w.
- Peyron MA, Woda A, Bourdiol P, Hennequin M. Age-related changes in mastication. J Oral Rehabil. 2017;44(4):299–312. doi:10.1111/joor.12478.
- González-Gil D, Flores-Fraile J, López-Marcos J. Tactile sensibility thresholds in implant prosthesis, complete dentures and natural dentition: review about their value in literature. Medicina (Kaunas). 2022;58(4):501. doi:10.3390/medicina58040501.
- Robbins MR. Neurologic diseases in special care patients. Dent Clin North Am. 2016;60(3):707–735. doi:10.1016/j.cden.2016.03.002.
- Kapadia A, Wankhade S, Khalikar A, et al. Comparing the functional efficiency of tooth-supported overdentures and implant-supported overdentures in patients requiring oral rehabilitation: a systematic review. Dent Res J (Isfahan). 2022;19:94
- Kossioni AE. The association of poor Oral Health parameters with malnutrition in older adults: a review considering the potential implications for cognitive impairment. Nutrients. 2018;10(11):1709. doi:10.3390/nu10111709.
- Muhammad T, Srivastava S. Tooth loss and associated self-rated health and psychological and subjective wellbeing among community-dwelling older adults: a cross-sectional study in India. BMC Public Health. 2022;22(1):7. doi:10.1186/s12889-021-12457-2.
- Qi X, Pei Y, Wang K, Han S, Wu B. Social isolation, loneliness and accelerated tooth loss among Chinese older adults: a longitudinal study. Community Dent Oral Epidemiol. 2023;51(2):201–210. doi:10.1111/cdoe.12727.
- Niesten D, McKenna G. Quality of life and oral health in older people. In: Kossioni A, ed. Gerodontology Essentials for Health Care Professionals. Switzerland, AG: Springer Nature; 2020: 101–112. doi:10.1007/978-3-030-41468-9_6.
- Zilinskaite-Petrauskiene I, Haug SR. A comparison of endodontic treatment factors, operator difficulties, and perceived oral health-related quality of life between elderly and young patients. J Endod. 2021;47(12):1844–1853. doi:10.1016/j.joen.2021.08.017.
- Hulsmann M, Peters O, Dummer P. Mechanical preparation of root canals: shaping goals, techniques and means. Endo Topics. 2005;10(1):30–76. doi:10.1111/j.1601-1546.2005.00152.x.
- Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature – part 2. Influence of clinical factors. Int Endod J. 2008;41(1):6–31. doi:10.1111/j.1365-2591.2008.01484.x.
- Shakiba B, Hamedy R, Pak JG, Barbizam JV, Ogawa R, White SN. Influence of increased patient age on longitudinal outcomes of root canal treatment: a systematic review. Gerodontology. 2017;34(1):101–109. doi:10.1111/ger.12231.
- Rajeswari K, Kandaswamy D, Karthick S. Endodontic management of patients with systemic complications. J Pharm Bioallied Sci. 2016;8(Suppl 1):S32–S35. doi:10.4103/0975-7406.191962.
- Kwon SR, Lee S, Oyoyo U, et al. Oral health knowledge and oral health related quality of life of older adults. Clin Exp Dent Res. 2021;7(2):211–218. doi:10.1002/cre2.350.
- Dougall A, Fiske J. Access to special care dentistry, part 2 Communication. Br Dent J. 2008;205(1):11–21. doi:10.1038/sj.bdj.2008.533.
- University of Washington School of Dentistry. Oral health fact sheet for dental professionals. dental.washington.edu/oral-medicine/special-needs/Patients-with-special-needs. Accessed June 9, 2016.
- Roberts R, Knopman DS. Classification and epidemiology of MCI. Clin Geriatr Med. 2013;29(4):753–772. doi:10.1016/j.cger.2013.07.003.
- Chalmers JM. Behavior management and communication strategies for dental professionals when caring for patients with dementia. Spec Care Dent. 2000;20(4):147–154. doi:10.1111/j.1754-4505.2000.tb01152.x.
- Chen E, Abbott PV. Dental pulp testing: a review. Int J Dent. 2009;2009:365785. doi:10.1155/2009/365785.
- Jespersen JJ, Hellstein J, Williamson A, Johnson WT, Qian F. Evaluation of dental pulp sensibility tests in a clinical setting. J Endod. 2014;40(3):351–354. doi:10.1016/j.joen.2013.11.009.
- Weisleder R, Yamauchi S, Caplan DJ, Trope M, Teixeira FB. The validity of pulp testing: a clinical study. J Am Dent Assoc. 2009;140(8):1013–1017. doi:10.14219/jada.archive.2009.0312. ISSN 0002-8177.
- Read JK, McClanahan SB, Khan AA, Lunos S, Bowles WR. Effect of Ibuprofen on masking endodontic diagnosis. J Endod. 2014;40(8):1058–1062. doi:10.1016/j.joen.2014.05.004.
- Derafshi R, Rezazadeh F, Ghapanchi J, Basandeh Sharif D, Farzin M. Prevalence of chronic orofacial pain in elderly patients referred to Shiraz Dental School from 2005 to 2017. Anesth Pain Med. 2019;9(6):e91182. doi:10.5812/aapm.91182.
- AAE Endodontic Case Difficulty Assessment Form and Guidelines. Chicago, IL: American Association of Endodontists; 2006.
- Coronal Leakage: Clinical and Biological Implications in Endodontic Success. ENDODONTICS: Colleagues for Excellence, Fall/Winter. Chicago, IL: American Association of Endodontists; 2002.
- Chavez EM, Wong LM, Subar P, Young DA, Wong A. Dental care for geriatric and special needs populations. Dent Clin North Am. 2018;62(2):245–267. doi:10.1016/j.cden.2017.11.005.
- Chalmers JM, Levy SM, Buckwalter KC, Ettinger RL, Kambhu PP. Factors influencing nurses’ aides’ provision of oral care for nursing facility residents. Spec Care Dent. 1996;16(2):71–79. doi:10.1111/j.1754-4505.1996.tb00837.x.
- Matear DW, Clarke D. Considerations for the use of oral sedation in the institutionalized geriatric patient during dental interventions: a review of the literature. Spec Care Dent. 1999;19(2):56–63. doi:10.1111/j.1754-4505.1999.tb01369.x.
- Nicolas E, Lassauzay C. Interest of 50% nitrous oxide and oxygen premix sedation in gerodontology. Clin Interv Aging. 2009;4:67–72. doi:10.2147/CIA.S4381. PMID: 19503768.
- Little JW, Miller CS, Rhodus NL. Little and Falace’s Dental Management of the Medically Compromised Patient. 9th ed. St. Louis, MO: Elsevier; 2018.
- Logothetis D 2017. Local anesthesia for the dental hygienist. 2nd ed. Elsevier.
- Haas DA. An update on local anesthetics in dentistry. J Can Dent Assoc. 2002;68(9):546–551. PMID: 12366885.
- Moore PA, Hersh EV. Local anesthetics: pharmacology and toxicity. Dent Clin North Am. 2010;54(4):587–599. doi:10.1016/j.cden.2010.06.015.
- Malamed SF. Handbook of Local Anesthesia. 7th ed. St. Louis, MO: Elsevier; 2020.
- Brown RS, Rhodus NL. Epinephrine and local anesthesia revisited. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4):401–408. doi:10.1016/j.tripleo.2005.05.074.
- Godzieba A, Smektała T, Jędrzejewski M, Sporniak-Tutak K. Clinical assessment of the safe use local anaesthesia with vasoconstrictor agents in cardiovascular compromised patients: a systematic review. Med Sci Monit. 2014;20:393–398. doi:10.12659/MSM.889984.
- Coke JM, Edwards MD. Minimal and moderate oral sedation in the adult special needs patient. Dent Clin North Am. 2009;53(2):221–230, viii. doi:10.1016/j.cden.2008.12.005.
- Yang YM, Guo B, Guo LY, et al. CBCT-Aided microscopic and ultrasonic treatment for upper or middle thirds calcified root canals. Biomed Res Int. 2016;2016:4793146. doi:10.1155/2016/4793146.
- Johnson BR. Access related complications. In: Jain P, ed. Common Complications in Endodontics; 2018: 67–85. doi:10.1007/978-3-319-60997-3_4.
- Gutmann JL, Lovdahl PE. Problem solving in tooth isolation, access openings, and identification of orifice locations. In: Gutmann J, Lovdahl P, eds. Problem Solving in Endodontics; 2011: 150–176.
- McCabe PS, Dummer PMH. Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J. 2012;45(2):177–197. doi:10.1111/j.1365-2591.2011.01963.x.
- Marroquín BB, Fernández CC, Schmidtmann I, et al. Accuracy of electronic apex locators to detect root canal perforations with inserted metallic posts: an ex vivo study. Head Face Med. 2014;10(1):57. doi: 10.1186/s13005-014-0057-2.
- Zmener O, Grimberg F, Banegas G, et al. Detection and measurement of endodontic root perforations using a newly designed apex-locating handpiece. Endod Dent Traumatol. 1999;15(4):182–185. doi:10.1111/j.1600-9657.1999.tb00798.x.
- Kulinkovych-Levchuk K, Pecci-Lloret MP, Castelo-Baz P, Pecci-Lloret MR, Oñate-Sánchez RE. Guided endodontics: a literature review. Int J Environ Res Public Health. 2022;19(21):13900. doi:10.3390/ijerph192113900.
- American Association of Endodontists. AAE position statement: dental dams. https://www.aae.org/specialty/wpcontent/uploads/sites/2/2017/06/dentaldamstatement.pdf. Accessed August 14, 2023.
- Roahen JO, Lento CA. Using cyanoacrylate to facilitate rubber dam isolation of teeth. J Endod. 1992;18(10):517–519. doi:10.1016/S0099-2399(06)81356-7.
- Stein TJ, Corcoran JF. Anatomy of the root apex and its histologic changes with age. Oral Surg Oral Med Oral Pathol. 1990;69(2):238–242. doi:10.1016/0030-4220(90)90334-o.
- de Morais AL, de Alencar AH, Estrela CR, et al. Working length determination using cone-beam computed tomography, periapical radiography and electronic apex locator in teeth with apical periodontitis: a clinical study. Iran Endod J. 2016;11(3):164–168. doi:10.7508/iej.2016.03.003
- Jeger FB, Janner SF, Bornstein MM, et al. Endodontic working length measurement with preexisting cone-beam computed tomography scanning: a prospective, controlled clinical study. J Endod. 2012;38(7):884–888. doi:10.1016/j.joen.2012.03.024.
- Rochon P. Drug prescribing for older adults. In: Post TW. Ed, UpToDate. Waltham, MA: Wolters Kluwer; 2022:1–60. https://org/www.uptodate.com. Accessed April 9, 2023.
- Ouanounou A, Haas DA. Pharmacotherapy for the elderly dental patient. J Can Dent Assoc. 2015;80:f18. PMID: 26679331.
- Lockhart PB, Tampi MP, Abt E, et al. Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal- and periapical-related dental pain and intraoral swelling: a report from the American dental Association. J Am Dent Assoc. 2019;150(11):906–921.e12. doi:10.1016/j.adaj.2019.08.020.
- Baillargeon J, Holmes HM, Lin YL, Raji MA, Sharma G, Kuo YF. Concurrent use of warfarin and antibiotics and the risk of bleeding in older adults. Am J Med. 2012;125(2):183–189. doi:10.1016/j.amjmed.2011.08.014.