

ABSTRACT
Beginning in the 1970s and 1980s, risk management principles were adapted to healthcare from other industries to help address the proliferation of medical malpractice settlements and judgments. Efforts focused on Identifying and mitigating legal vulnerabilities. As dentists continue to refine and expand services offered to their patients, they must assess and proactively address potential risks for the benefit of patients and professional liability mitigation. This article will consider the recent past and status of patient safety and risk management in dentistry, as well as immediate opportunities for safety improvements and risk mitigation in professional dental practice. Although individual dentists and dental practices may identify and implement methods to improve safety and risk management, cooperative dental professional and cross-professional initiatives will help to foster change more broadly, benefitting both dental patients and all dental professionals.
Risk Management and Patient Safety in Dentistry
A 52 year-old male patient sought care for a faulty bridge from tooth 29 to 31. The abutment teeth were non-restorable, and the patient agreed to implant therapy. After extractions and implant placement, the patient complained of pain and paresthesia. The doctor monitored the situation for two weeks, taking no other action. The patient then sought a second opinion and later filed a lawsuit asserting negligent care. Expert review indicated standard of care concerns including inadequate pre-surgical planning/imaging, no documented implant length planning, no intra-operative images, absence of follow-up diagnostic images, failure to remove implants to prevent permanent nerve injury, and missing treatment/follow-up care records. A CBCT image indicated clear evidence of mandibular nerve impingement. The patient suffered permanent nerve damage.
The case study demonstrates patient safety and risk management concerns that are all too common in dental professional liability claims.Citation1 Although professional malpractice involving serious patient harm may never be asserted during an individual dentist’s career, malpractice claims and lawsuits involving injuries (e.g., nerve injury, jaw fracture, laceration), and other adverse events (e.g., wrong tooth treatment/extraction, swallowed/aspirated objects, failed implants, failure to diagnose/refer for oropharyngeal cancer, or infection/sepsis) are reported frequently to professional liability insurers.
Similar to clinical, operational, and financial risks associated with dentistry and health care, errors, adverse events and undesirable outcomes are inevitable. Nevertheless, dental professionals must adhere to ethical standards – beneficence and non-malfeasance – as part of preventing harm.Citation2 Furthermore, all members of the dental community must challenge the status quo and continually improve both treatment quality and patient safety.
The practicing dentist and all dental team members are critical to the delivery of safe patient care. Moreover, each dental team is responsible for sharing its experiences (both positive and negative) through networking, educational programs, adverse event reports, the dental literature and through other available mechanisms. These resources can enable dental professionals to learn from their peers about real-world risks and preventive measures without experiencing an adverse event or litigation.
Dental researchers, academia, professional organizations, governmental agencies and others play a key role in funding and development/dissemination of evidence-based clinical guidelines, recommendations, and best practices to support safe and effective patient care.
Governmental agencies, professional organizations, professional liability insurance companies, and others may provide information on, and analysis of, adverse events on an aggregate basis, quality and/or patient safety data and criteria.
The dental products industry and the FDA are responsible for developing and assessing the safety and effectiveness of dental products – another important part of providing safe dental care.
Background and Status
Although many definitions exist that apply to specific situations, risk management and patient safety are complementary terms for purposes of this discussion. They share a common goal – preventing harm – as demonstrated in the following definitions
Patient Safety- the absence of preventable harm to a patient and reduction of risk of unnecessary harm associated with health care to an acceptable minimum.Citation3
Risk Management- the attempt to identify, evaluate and deal with problems which may cause harm to patients, to file complaints about malpractice and to avoid unnecessary economic losses for health care providers.Citation4
In today’s dental practice, implementation of strategies and processes that support the interrelated concepts of risk management and patient safety will help to ensure an environment in which to deliver safe, quality dental care that will benefit the patient and provider.
Beginning in the 1970s and 1980s, the principles of risk management were adapted to healthcare from other industries as a strategy to address the proliferation of medical malpractice settlements and judgments. The focus centered on identifying and mitigating areas of legal vulnerability, such as the absence of informed consent and professional negligence.Citation5 A few years later, another perspective presented risk management as a unifying principle between legal responsibilities and sound clinical practice.Citation6 Two common themes emerged in the reviewed cases. These factors remain at the core of dental risk management today: transparent communication and comprehensive documentation.
Notwithstanding the importance of communication and documentation to effective risk management and harm prevention over many decades, inadequate communication and documentation remain as key elements associated with patient harm and consequent malpractice claims, as in the following claim case study.
A patient with a history of oropharyngeal cancer treatment retired from work, moved to a different state, and sought dental care. Due to specific patient complaints, limited exams and treatment were performed at the new office. These visits led to a treatment plan for several implants and restorations, without benefit of a comprehensive evaluation. Extraction of a lower molar at the start of the planned case resulted in pain and delayed healing. Upon further questioning, the patient confirmed that he had previously received chemotherapy and radiation therapy to treat the oral cancer. The dentist then prescribed an antibiotic, which was ineffective. The patient then sought care from an oral surgeon. The diagnosis: osteoradionecrosis and infection. The patient’s disease course included multiple debridement procedures, pathologic fracture and eventually, reconstructive surgery. Concerns included missing records (including the medical history and letter regarding the patient’s cancer treatment from the prior dentist), inadequate informed consent and failure to initiate a timely referral for specialty care.
In this case study, transparent and effective communication may have prevented the oversight of the patient’s radiation therapy history. The patient and the dentist play an essential role in the communication process. Unfortunately, the patient failed to disclose this critical part of his medical history, and the dentist failed to probe for further details about cancer therapy. The office had recently implemented an electronic record system and had not yet established a procedure and audit process for the integration of external records. Otherwise, effective documentation management may have averted the adverse outcome.
Perea-Pérez et al.Citation4 proposed a multi-part dental care risk management plan (), since “no available bibliography exists regarding any ‘plan for health care risk management’ specific to dentistry.” Citation4(p806) Part of the plan proposes that measures be established to reduce risk, which may include sound clinical practice recommendations.Citation4 Consistent with this proposal, a risk management plan should include the consideration of evidence-based clinical guidelines for the procedure at hand, if available.
Table 1. Components of “the Plan for Health Care Risk Prevention in Dentistry.”4(p807)
In the absence of evidence-based clinical guidelines, practitioners should implement and follow clinical protocols and safety measures consistent with the principles of evidence-based practice, designed to meet the standard of care (). Although deviation from guidelines or protocols may be appropriate or necessary for an individual patient’s condition and circumstances, in the author’s experience as a risk control professional, a supporting rationale for deviation often fails to be reflected in clinical documentation.
Table 2. Standard of care in dentistry.*
Essential risk management steps for today’s dental practice may be proposed that closely align with the Agency for Healthcare Research and Quality (AHRQ) elements of a patient safety initiative.Citation7 Whether a practice plans to offer a new patient service or reevaluate current treatments and procedures, follow a methodical risk management/patient safety process that minimally incorporates these key points:
Identify and analyze potential risks/adverse events related to the treatment or process.
Evaluate possible risk management/patient safety methods or techniques.
Implement selected methods and techniques.
Track results, then reassess and improve methods and techniques, as necessary.
In addition to patient safety and risk management processes, an important third component of rendering safe and effective care is the quality improvement process (continuous improvement). A useful, dental practice-focused resource describes quality assurance and improvement in the context of dental clinic services.Citation8 For example, the Plan-Do-Check (or Study)-Act quality improvement process (PDCA or PCSA cycle) aligns well with the steps described in a patient safety initiative and the risk management process.Citation9
Consider the previous case studies. What risks and adverse events should be prioritized for mitigation for the procedures that were performed? Were sufficient risk mitigation and patient safety techniques considered and implemented to help ensure safe, quality patient care? What steps would a prudent dentist take to do so? What protocols and procedures does your practice implement to ensure safe, quality patient care?
Patient injuries and other adverse events may occur even when the standard of care is fulfilled. On the other hand, certain actions and decisions during the course of patient care may result from a number of factors that conflict with risk management and patient safety principles – as in the two case examples – potentially leading to patient injuries and adverse outcomes.
Are We Improving?
Researchers discovered that there were more than 1500 dental malpractice claims per year in the National Practitioner Data Bank (NPDB) dataset between September 1990 and December 2018.Citation10 The majority of claims involved minor injuries. However, in the years studied, it was noted that minor claims decreased in number while claims involving major injuries increased.Citation10
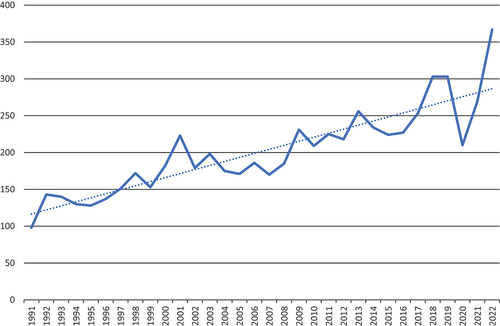
The NPDB online data analysis tool demonstrates that this trend continues, with data now available through December 2022. Less severe dental incidents with settlement payments below $100,000 () have trended down over three decades, while at the same time more severe incidents with payments of $100,000 or more () have increased in number.Citation11 Interestingly, the average dentist malpractice payment reported to the NPDB in 1991 was $23,178. Correcting for inflation, this amount represents approximately $49,800 in 2022 dollars. However, in 2022, the average dentist malpractice payment reported to the NPDB was $113,188, approximately 2.25 times more than in 1991.
Figure 1. Dental malpractice payments ≤ $99,999.
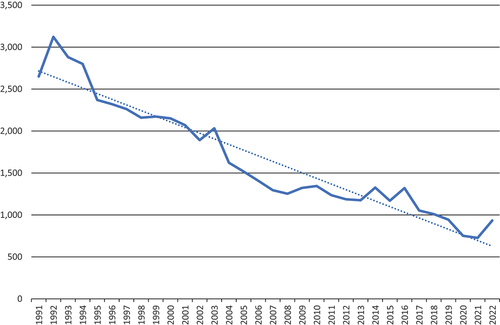
Figure 2. Dental malpractice payments ≥ $100,000.
Data from one insurer’s dental professional liability claim report comparing two datasets demonstrates a similar trend, with the percentage of claims over $100K on the rise and a decreased percentage for claims under $100K (),Citation1
Figure 3. Paid indemnity range comparison: 2016 claim dataset vs 2020 claim dataset.
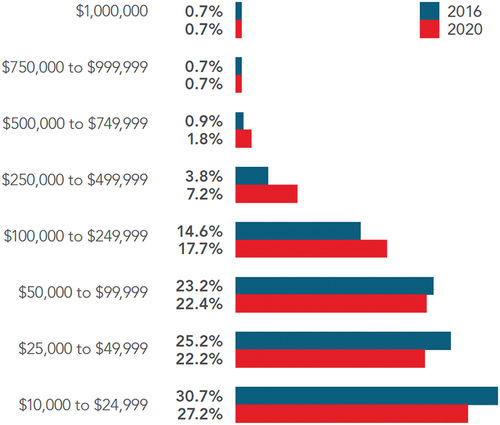
Other key findings of this claim report, which compared closed claims with settlement payments from $10,000 to $1,000,000 over two time periods, 2016 and 2020, include:
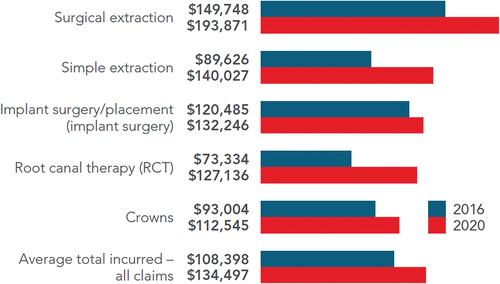
The average total incurred (total of a settlement payment or judgment at trial, plus claim expenses) for dental closed claims increased more than 24% to $134,497 from the previous report.
The top five dental procedures most often associated with malpractice claims all demonstrated increases in average total incurred since the previous report ().
Figure 4. Average total incurred of top dental procedures associated with all professional liability claims.
Claims associated with nerve injury have increased and the average total incurred has risen by 43.6% to $210,568.
Incidents of swallowed-aspirated object and wrong tooth treatment/extraction continue to be an important safety concern. In total, these claims have increased in frequency and now represent 8.6% of closed claims with settlements of $10,000 or more.
These findings help to clarify the types of dental procedures most often associated with costly malpractice claims in dental practice. Periodically publishing this information is intended to “help dentists enhance their practice and minimize professional liability exposure by identifying loss patterns and trends.” Citation1(p5)
Only a portion of errors and adverse outcomes result in professional liability claims or lawsuits. Moreover, many near misses involve situations where the conditions indicated the likeliness of an error or injury, but none occurred. In the absence of these data over many years, it is difficult or impossible to state whether dentistry is improving with respect to risk management and patient safety. However, the question of progress and improvement is multifaceted for this complex topic.
On the positive side of the equation, the professional literature on dental patient safety and clinical guidelines is expanding. The resulting information and the development of associated tools will increase practitioners’ awareness and facilitate advances in dental-specific patient safety initiatives, including at the practice level.Citation12–18 Organized dentistry also is becoming proactive on policies, recommendations, quality of care and continuing education.Citation19–24 Dentistry has a patient safety organization (PSO) – the Dental Patient Safety Foundation (DPSF) – which meets the criteria established by the Patient Safety Rule of the U.S. Department of Health and Human Services.Citation25 Finally, dental licensing boards across the country exist primarily to protect the public. Licensing boards help to ensure the delivery of safe patient care through the promulgation of rules and regulations, as well as through their oversight and compliance activities.
Similar to any new clinical discovery, method or treatment, the progression from research to broad-based acceptance and implementation can be tortuously slow. Dentists must apply the principles of evidence-based practice and remain aware of advances as new information is validated, published, and disseminated. Moreover, participating in the dissemination process – and implementing strategies that will enhance safety – represent actions within each practitioner’s scope and ability. Now is the time to consider the steps that every dentist/dental team immediately may implement to advance patient safety, risk management and facilitate continuous improvement to make a difference in patient care.
Opportunities for Improvement
Understanding Obstacles
Modern society places significant demands on an individual’s time and attention. Dentists and their team members are not exempt from these pressures. Consequently, a perceived obstacle to re-thinking the approach of a dental practice to risk management and patient safety is the time necessary to do so. Dentists often ask patients who are grappling with a treatment plan decision about their personal priorities. Is their smile and oral function more important than other products or services competing for disposable income? Establishing priorities may quickly clarify a decision to proceed with dental care.
Similarly, every dental office has a philosophy, mission, and priorities, whether documented in writing or visible through its actions. Typically, risk management and patient safety activities are already consistent with the practice philosophy. Re-assessing philosophy and mission and, if necessary, making thoughtful adjustments will permit the practice to re-set its focus and integrate high-priority risk management and patient safety activities.
Other obstacles which may explain delays in the development of programs organized specifically for promoting patient safety have been describedCitation4 including:
Relatively minor incidents. Dental adverse events and injuries are often minor and less severe compared to other healthcare settings. However, recall the trend toward more severe malpractice claims. Furthermore, consider an adverse event such as swallowed/aspirated objects in dental practice. Although most incidents do not result in grave outcomes, every such incident has the potential to cause serious morbidity, even death.
Outpatient setting. In an ambulatory/outpatient setting capturing and following up on injuries and adverse events may be more challenging and inconsistent.
Dental practice variety. Differences in size, complexity, business practices, computer systems and other factors present challenges to safety data collection/sharing.
Reputational risk. In a competitive private practice environment, dentists may fear potential repercussions and reputational risks associated with reported adverse events. While reports to a PSO, such as the DPSF can be safely, voluntarily, and confidentially submitted, this concern persists.Citation25
These and other obstacles may be effectively addressed by collaboration with and understanding solutions implemented by our medical colleagues and other healthcare professions. In addition, working together as a dental community with government agencies, vendors, professional organizations, insurers, and others will help to address safety infrastructure requirements.
Risk Management and Safety-Focused Actions, Educational Opportunities, and Other Resources
Dental academic and continuing education involves didactic, experiential, and social/observational learning. Learning by doing (experiential) occupies the core of clinical education, whether in dental schools, community-based clinics/externships, or hands-on continuing education programs. However, there is no need to experience a professional liability claim or patient adverse outcome for effective learning. Seeking opportunities to learn from collective patient safety reports and/or claim data and individual adverse event experiences of other dentists will facilitate and improve the assessment, mitigation, and management of risk exposures in dental practice. Consider the following approaches to promote a culture of safety and expand your dental team’s awareness of and focus on risk management and mitigation.
Importance of the dental team. The ability of staff to help manage risk is critical to an effective risk management and patient safety program.
A team approach to corrective action development helps eliminate bias in the process and maximize effectiveness and buy-in for new or modified policies or procedures.
Develop a culture based upon open communication and being receptive to constructive feedback and recommendations from team members, other providers, and patients. These tenets are critical to realizing procedural and patient safety improvements.
Hold regular staff meetings and incorporate risk management/patient safety into the agenda of each session.
Appoint a Patient Safety Officer to lead internal safety efforts, preferably, an individual other than the office infection control officer.Citation26
Consider in-office or external educational and career-expanding opportunities for the Patient Safety Officer – and all team members. These may include: TeamSTEPPS®,Citation27,Citation28 general patient safety and/or risk management courses, certificates, and certifications,Citation29–31 dental-specific risk management and safety courses/certifications.Citation32–34
Establish team processes for identification and review of near misses and adverse events, development of corrective actions and ongoing monitoring, as well as for reporting incidents to the DPSF.Citation25 Readers may learn more about the reporting process and the DPSF Reporting Tool by accessing the organization’s website (https://www.dentalpatientsafety.org) and clicking on “Report An Incident”.
Study club activities.
Encourage the integration of risk management and patient safety programming at local study clubs.
Start a new study club focusing on risk management and patient safety. Use this safe space to share information about adverse events, near misses and corrective actions. Consider periodic submission of study club-authored papers to professional journals.
Encourage internal patient safety officers to share their expertise via local and regional study club or dental society meetings.
Seek out cross-professional content for study clubs to learn from medical colleagues and other professionals. Medical providers, hospitals and other healthcare facilities have actively pursued safety improvements and initiatives for many years.Citation23 Brainstorm on strategies to leverage their knowledge to reduce risk and improve safety in the dental setting.
Other educational activities and content.
Seek out presentations, webinars and on-demand content related to risk management and patient safety available from multiple professional liability insurers.
Teach others: share your knowledge via local, state, or national professional meetings.
Learn more about staying up to date on evidence-based clinical guidelines; evidence-based dentistry and evidence assessmentCitation35–47
Regularly incorporate training focused on patient and team communications as part of risk management/patient safety CDE plans (workshop/role-play format preferred).
Documentation best practices – paper or electronic records. Reassess office documentation practices and implement or enhance internal dental record audit procedures to improve documentation. Minimally, confirm compliance with state documentation requirements. This information should be readily available on state dental board websites as part of board position statements, the state dental practice act and/or in state board promulgated regulations. Assistance also may be available from state dental societies, external consultants and/or professional liability insurers.
As part of assessing office communication and documentation practices, review and improve the office’s informed consent process ().
Table 3. Informed consent^.
Accreditation by independent and recognized third-party organizations is customary and often required in healthcare fields other than dentistry. Although less common, dental practices may seek accreditation voluntarily from such organizations.Citation48,Citation49 The accreditation process provides another opportunity for dentists and dental team members to remain focused on methods and practices to improve quality, reduce risk and promote patient safety.
Summary and Considerations
Dentistry is a fulfilling professional endeavor, leading to personal, professional, and financial rewards for dentists and all dental team members. Most importantly, millions of patients benefit from dental services through improved self-esteem and better oral/overall health. In order to deliver quality care and improve patient health, dentists routinely monitor patient home care, health/disease status, and recommend appropriate preventive actions and treatments, and assess outcomes. To help ensure a healthy dental business, they regularly monitor financial metrics, hire business and marketing consultants, implement financial improvement strategies, and determine results.
Similarly, in the interest of ethical care, patient safety – and in dentistry’s enlightened self-interest – the dental community must continue to improve and implement methods to collect, analyze and disseminate patient safety information to fully understand the scope and nature of errors, injuries, and other adverse events in dentistry. These data will help to expose gaps in safety systems, treatment protocols and office procedures to facilitate risk mitigation and reduce harm. Although dental researchers and organized dentistry have made progress to identify and overcome barriers, and to develop methods, strategies, and goals toward broad realization of a dental culture of safety, every practicing dentist and dental team member represents the catalyst necessary to accomplish this goal.
Practice reassessment and change implementation can be a daunting endeavor in the best of circumstances. Remember that a journey of a thousand miles begins with a single step. Choose one protocol or technique that your team can implement tomorrow, choose three protocols or techniques (or more) that your team can implement in the coming year. Take action and begin to establish a culture of safety in your dental practice and within the local/regional dental community. Then take a breath, assess, and recognize your successes. In addition, dentists and team members must understand and realize that risk management and patient safety are partners in a continuing journey—not a destination. In this journey, challenges will arise and errors will occur. Responding to these events with honesty, transparency, and empathy, rather than blame and shame, will help to ensure development and continuation of an effective culture of safety.
By carefully examining policies and processes, sharpening the focus on patient safety, and developing effective communication, documentation and risk prevention protocols, dental professionals can elevate their practice to the next level, benefiting all parties.
Acknowledgments
The author would like to recognize the efforts of Mr. Scott Sellers for management of the NPDB malpractice payment data and generation of and . Mr. Sellers also managed and analyzed claim data supporting publication of the CNA/Dentist’s Advantage Dental Professional Liability Claim Report: 2nd Edition, including exhibits 1 and 5 of the Claim Report which appear this manuscript as and , respectively.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Ronald R. Zentz
Ronald R. Zentz joined CNA in 2012 and serves as Consulting Director, Industry Leader, Healthcare Risk Control. His primary responsibilities include risk management resource development, customer support and continuing education for dentist and pharmacist professional liability programs. Dr. Zentz practiced pharmacy and general dentistry, followed by professional and clinical affairs positions with a major dental manufacturer. His responsibilities included product development, clinical research, regulatory affairs and continuing education for device and pharmaceutical products. Dr. Zentz later joined the American Dental Association (ADA) staff, serving as Senior Director, ADA Council on Scientific Affairs. The Council advances the science of dentistry through research, product evaluations and standards, and development of evidence-based clinical recommendations. His education includes a Bachelor of Science in Pharmacy (Butler University), Doctor of Dental Surgery (Indiana University School of Dentistry) and a General Practice Residency Certificate (Veterans Administration Medical Center, Indianapolis). Dr. Zentz is a member of the American Dental Association, the American Pharmacists Association, and is a Fellow of the Academy of General Dentistry and the American College of Dentists. He is certified in healthcare risk management (CPHRM) by the American Society of Healthcare Risk Management and has completed the TeamSTEPPS® Master Trainer program.
References
- CNA, Dentist’s Advantage. Dental professional liability claim report: 2nd edition. CNA Specialty Risk Control and Dentist’s Advantage. https://www.dentists-advantage.com/Prevention-Education/Claim-Reports. Published February, 2021. Accessed September 18, 2023.
- American Dental Association (ADA). Principles of ethics and code of professional conduct. ADA. https://www.ada.org/ethics. Updated March, 2023. Accessed March 1, 2024.
- World Health Organization (WHO). Patient safety. WHO. https://www.who.int/news-room/fact-sheets/detail/patient-safety. Updated September 11, 2023. Accessed March 1, 2024.
- Perea Pérez B, Santiago Sáez A, García Marín F, Labajo González E, Villa Vigil A. Patient safety in dentistry: dental care risk management plan. Med Oral Patol Oral Cir Bucal. 2011;6:e805–10. doi:10.4317/medoral.17085.
- Pollack BR. Risk management in the dental office. Dent Clin North Am. 1985;29(3):557–580. https://pubmed.ncbi.nlm.nih.gov/3861400/. PMID: 3861400.
- Dunne M, Brown JL. Risk management in dentistry. Curr Opin Dent. 1991;1(5):668–671. https://pubmed.ncbi.nlm.nih.gov/1807467/. PMID: 1807467.
- Agency for Healthcare Research and Quality. Ahrq’s Patient Safety Initiative: Building Foundations, Reducing Risk. An Interim Report to the United States Senate Committee on Appropriations. Rockville, MD: AHRQ; 2003.
- Unit 5: quality assurance and quality improvement—quality improvement process. In: Doherty M, Bingham D, Kislak R, Kolo S, Barzel R, Holt K, eds. Safety Net Dental Clinic Manual. 2nd ed. Westborough, MA: DentaQuest Partnership for Oral Health Advancement; Washington, DC: National Maternal and Child Oral Health Resource Center; 2018.https://www.dentalclinicmanual.com/5-quality/. Accessed October 31, 2023.
- Unit 5: quality assurance and quality improvement—quality improvement process, section 1, the vision for quality. In: Doherty M, Bingham D, Kislak R, Kolo S, Barzel R, Holt K, eds. Safety Net Dental Clinic Manual. 2nd ed. Westborough, MA: DentaQuest Partnership for Oral Health Advancement; Washington, DC: National Maternal and Child Oral Health Resource Center; 2018.https://www.dentalclinicmanual.com/5-quality/sec1-04.php#. Accessed October 31, 2023.
- Cui W, Finkelstein J. Using big data analytics to identify dentists with frequent future malpractice claims. Stud Health Technol Inform. 2020;270:489–493. doi:10.3233/shti200208.
- Division of Practitioner Data Bank, Bureau of Health Workforce, Health Resources and Services Administration. Online data analysis tool, practitioner type-dentist, medical malpractice payment reports. Data source: National Practitioner Data Bank (2023). https://www.npdb.hrsa.gov/analysistool/. Updated June 30, 2023. Accessed September 20, 2023.
- Carrasco-Labra A, Polk DE, Urquhart O, Aghaloo T, Claytor WJ, et al. Evidence-based clinical practice guideline for the pharmacologic management of acute dental pain in children. J Am Dent Assoc. 2023;154(9):814–825.e2. doi:10.1016/j.adaj.2023.06.014.
- Dhar V, Pilcher L, Fontana M, Gonzalez-Cabezas C, Keels MA, Mascarenhas AK, et al. Evidence-based clinical practice guideline on restorative treatments for caries lesions. J Am Dent Assoc. 2023;154(7):551–566.e51. doi:10.1016/j.adaj.2023.04.011.
- Kalenderian E, Lee JH, Obadan-Udoh EM, Yansane A, White JM, Walji MF. Development of an inventory of dental harms. J Patient Saf. 2022;18(6):559–564. doi:10.1097/PTS.0000000000001033.
- Walji MF, Yansane A, Hebballi NB, Ibarra-Noriega AM, Kookal KK, Tungare A, et al. Finding dental harm to patients through electronic health record-based triggers. JDR Clin Trans Res. 2020;5(3):271–277. doi:10.1177/2380084419892550.
- Kalenderian E, Obadan-Udoh E, Yansane A, Kent K, Hebballi NB, Delattre V, et al. Feasibility of electronic health record–based triggers in detecting dental adverse events. Appl Clin Inform. 2018;9(3):646–653. doi:10.1055/s-0038-1668088.
- Obadan EM, Ramoni RB, Kalenderian E. Lessons learned from dental patient safety case reports. J Am Dent Assoc. 2015;146(5):318–326.e2. doi:10.1016/j.adaj.2015.01.003.
- Maramaldi P, Walji MF, White J, Etolue J, Kahn M, Vaderhobli R, et al. How dental team members describe adverse events. J Am Dent Assoc. 2016;147(10):803–811. doi:10.1016/j.adaj.2016.04.015.
- American Academy of Pediatric Dentistry. Policy on patient safety. In: The Reference Manual of Pediatric Dentistry. Chicago, IL: American Academy of Pediatric Dentistry; 2023:27–31. https://www.aapd.org/media/Policies_Guidelines/P_PatientSafety.pdf. Accessed September 25, 2023.
- American Academy of Oral and Maxillofacial Surgeons. Culture of safety in the OMS office. American Academy of Oral and Maxillofacial Surgeons. https://myoms.org/why-choose-an-oms/culture-of-safety. Updated May, 2021. Accessed September 25, 2023.
- American Dental Association. Dental quality alliance (DQA)TM. American Dental Association ©2023. https://www.ada.org/resources/research/dental-quality-alliance. Accessed September 26, 2023.
- Morath J, Gallagher T. Communicating with patients when things go wrong in dentistry (recorded webinar). https://ebusiness.ada.org/education/viewcourse.aspx?id=635. Updated January, 2022. Accessed September 26, 2023.
- Bosack R, Rollert M, Lieblich S, Stevens R, Brady J. My view: improving safety in dentistry. American Dental Association. https://adanews.ada.org/ada-news/viewpoint/my-view/2020/november/improving-safety-in-dentistry. Updated December 13, 2021. Accessed September 26, 2023.
- American Dental Association. ADA guidelines for practice successTM. Managing professional risks: best practices. American Dental Association ©2019. https://engage.ada.org/p/pb/guidelines-for-practice-success-managing-professional-risks-best-practices-1413. Accessed September 20, 2023.
- Dental Patient Safety Foundation (DPSF). Website home page. https://www.dentalpatientsafety.org. Accessed September 20, 2023.
- American Society for Healthcare Risk Management. The growing role of the patient safety officer: implications for risk managers. Agency for Healthcare Research and Quality. https://psnet.ahrq.gov/issue/growing-role-patient-safety-officer-implications-risk-managers. Updated March 6, 2005. Accessed September 26, 2023.
- Agency for Healthcare Research and Quality. TeamSTEPPS® 3.0 Curriculum. Agency for healthcare research and quality. Free-to-use materials for instructor-led or self-paced training. Rockville, MD. https://www.ahrq.gov/teamstepps-program/index.html and https://www.ahrq.gov/teamstepps-program/curriculum/index.html. Updated July, 2023. Accessed September 27, 2023.
- American Hospital Association (AHA). AHA team training—getting started with TeamSTEPPS. American Hospital Association. On-site or virtual education options for beginner, intermediate and advanced learner levels. https://www.aha.org/center/team-training/getting-started-teamstepps. Accessed September 27, 2023.
- American Society for Healthcare Risk Management (ASHRM). ASHRM education opportunities. American society for healthcare risk management ©2023. https://www.ashrm.org/education-ashrm. Accessed September 27, 2023.
- American Society for Healthcare Risk Management (ASHRM). CPHRM Certification. American Society for Healthcare Risk Management ©2023. https://www.ashrm.org/education/cphrm. Accessed September 27, 2023.
- IHI—Institute for Healthcare Improvement. Career growth & professional development. Institute for Healthcare Improvement ©2023. https://www.ihi.org/education/Pages/default.aspx. Accessed September 27, 2023.
- Emergency Care Research Institute—ECRI. Dental risk management training program. Emergency Care Research Institute ©2023. https://www.ecri.org/components/PPRM/Pages/EduTrain7.aspx. Accessed September 27, 2023. Login required for access.
- Dental Compliance Institute. A comprehensive curriculum for OSHA and HIPAA regulations and dental risk management. Dental Compliance Institute ©2023. https://dentalcomplianceinstitute.com/curriculum/. Accessed September 27, 2023.
- OSAP—Organization for Safety, Asepsis and Prevention. Education and training. Organization for Safety, Asepsis and Prevention ©2023. https://www.osap.org/education-training. Accessed September 27, 2023.
- ADA Science and Research Institute. Introduction to evidence-based dentistry (video series). American Dental Association ©2023. https://www.ada.org/resources/research/science-and-research-institute/evidence-based-dental-research/tutorials. Accessed September 27, 2023.
- ADA Science and Research Institute home page. Access clinical practice guidelines (see “evidence-based dentistry”) and other topics. American Dental Association ©2023. https://www.ada.org/resources/research/science-and-research-institute. Accessed September 27, 2023.
- Carrasco-Labra A, Urquhart O, Glick M. A. practitioner’s guide to developing critical appraisal skills. J Am Dent Assoc. 2023;154(9):836–841. doi:10.1016/j.adaj.2023.06.005.
- Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry-understanding and applying the principles of EBD. J Am Dent Assoc. 2014;145(11):1105–1107. doi:10.14219/jada.2014.102.
- Brignardello-Petersen R, Carrasco-Labra A, Booth HA, Glick M, Guyatt GH, Azarpazhooh A, et al. A practical approach to evidence-based dentistry-how to search for evidence to inform clinical decisions. J Am Dent Assoc. 2014;145(12):1262–1267. doi:10.14219/jada.2014.113.
- Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry: III-How to appraise and use an article about therapy. J Am Dent Assoc. 2015;146(1):42–49. doi:10.1016/j.adaj.2014.11.010.
- Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry: IV-How to use an article about harm. J Am Dent Assoc. 2015;146(2):94–101. doi:10.1016/j.adaj.2014.12.002.
- Brignardello-Petersen R, Carrasco-Labra A, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry: V-How to appraise and use an article about diagnosis. J Am Dent Assoc. 2015;146(3):184–191. doi:10.1016/j.adaj.2015.01.011.
- Carrasco-Labra A, Brignardello-Petersen R, Glick M, Guyatt GH, Azarpazhooh A. A practical approach to evidence-based dentistry: VI-How to use a systematic review. J Am Dent Assoc. 2015;146(4):255–265. doi:10.1016/j.adaj.2015.01.025.
- Carrasco-Labra A, Brignardello-Petersen R, Glick M, Guyatt GH, Neumann I, Azarpazhooh A. A practical approach to evidence-based dentistry: VII-How to use patient management recommendations from clinical practice guidelines. J Am Dent Assoc. 2015;146(5):327–336. doi:10.1016/j.adaj.2015.03.015.
- Sale J, Amin M, Carrasco-Labra A, Brignardello-Petersen R, Glick M, Guyatt GH, et al. A practical approach to evidence-based dentistry: VIII-How to appraise an article based on a qualitative study. J Am Dent Assoc. 2015;146(8):623–630. doi:10.1016/j.adaj.2015.06.010.
- Abrahamyan L, Pechlivanoglou P, Carrasco-Labra A, Brignardello-Petersen R, Glick M, Guyatt GH, et al. A practical approach to evidence-based dentistry: IX-How to appraise and use an article about economic analysis. J Am Dent Assoc. 2015;146(9):679–689. doi:10.1016/j.adaj.2015.06.021.
- Carrasco-Labra A, Brignardello-Petersen R, Azarpazhooh A, Glick M, Guyatt GH. A practical approach to evidence-based dentistry: X-How to avoid being misled by clinical studies’ results in dentistry. J Am Dent Assoc. 2015;146(12):919–924. doi:10.1016/j.adaj.2015.08.008.
- AAAHC—Accreditation Association for Ambulatory Health Care. Accreditation for primary care providers (dental group practices). Accreditation Association for Ambulatory Health Care, Inc. ©2023. https://www.aaahc.org/accreditation/primary-care. Accessed September 28, 2023.
- ACHC—Accreditation Commission for Health Care. Programs—dentistry accreditation. Accreditation Commission for Health Care, Inc. ©2023. https://www.achc.org/dentistry. Accessed September 28, 2023.