

ABSTRACT
Background
As dentistry became a profession it crafted aspirational values to announce the highest standards for the relationship between individual practitioners and those who sought their care and of professional etiquette among colleagues. These standards evolved as dentistry underwent dramatic development in technique, scientific knowledge, commercial ownerships of practice, a shift toward insurance and the government paying for most of the dental bill, and an increasing voice for the public. Dentistry borrowed some of the principles from the bioethics movement in the 1970s and ‘80s.
Objective
Evidence is presented in this paper for six areas showing that measures of ethical impact such as public trust, disciplined licenses, teaching of ethics, and membership in organized dentistry suggest that further adjustments are needed to make the profession responsive to the current expectations of society and the profession itself.
Conclusion
An alternative to the descriptive lists of aspirational principles is presented. This involves two imperatives or expected types of behavior that close the gap between ideal images and typical behavior.
Practical Highlights
Moral action and professionalism (MAP) means not cheating, which is taking unjustified personal advantage of others, and being stewards of the common good that is the mark of a profession.
MAP
Here are two suggestions for strengthening dentistry’s capacity to thrive while advancing oral health: Don’t cheat. Be professional.
This is something different from the familiar sets of ethical principles. Less cheating and more professionalism are imperatives for action rather than general ideals. Publishing and lecturing on abstractions where several principles might be applied is no assurance that good behavior will follow. The focus here is turning attention to making a difference. The abbreviation MAP is used to designate “moral action and professionalism.” As the Harvard healthcare ethicist Norman Daniels said in Just Health Care, “We learn much about the adequacy of moral theories by attempting to apply them.”Citation1p. xi
Cheating is defined as profiting personally at the expense of others in ways that are not justified.Citation2–4 Being paid for providing appropriate dental care; requiring that patients take time from work and travel and endure some pain and cost; collecting insurance reimbursements; selling one’s practice; and so forth are examples of benefiting from exchanges where others give up something. But they are not cheating if there is a plausible expectation that others would act the same way in similar situations. Examples of cheating include upcoding, overtreatment, false advertising, controlling patient choices through misinformation or lack of informed consent, overlooking gross or continuous faulty treatment by colleagues, and any other behavior one would not publicly defend or be happy to see one’s colleagues engaged in.
Cheating is never a solo act. At the basic level, it turns on how we treat others.Citation5–8 In the secondary sense cheating includes how we justify our behavior to colleagues. We resent it when we have been cheated or when policies are imposed to our disadvantage; we disapprove, to some extent, when others get away with cheating, unless we can do the same ourselves. As psychologist Danile Ariely shows, the boundary between relative personal gain that is allowable and what is not is open to interpretation based on feeling overlaid with justifications.Citation5 The border zone varies from person to person, across circumstances, and even in response to external factors such as situational stress. Most cases of cheating are justified by one of three excuses: (a) “I am entitled to it because of my special position,” (b) “others deserve the short end of what they get,” and (c) “no one will notice or bother to correct the problem because it is not worth it to them.” Examples include the following: (a) “My educational debt, my service to the community, and the wisdom I have acquired though practice give me greater credibility on determining what is right here.” (b) “Insurance companies are getting wealthy at my expense and they dictate treatment options, so it is appropriate that I ‘make a few compensatory adjustments.’” (c) “I practice alone and accept full responsibility for what I do and would not say anything about those I know are cutting corners and I expect them to extend the same courtesy to me.”
Professionalism means contributing one’s fair share to the common good and not taking more than one is entitled to.Citation9,Citation10 The public trust and patronage of dentistry are dependent on more than the reputation of any individual dentist. It is more than the average of what happens in individual offices. There is a substantial body of literature showing that humans thrive as social beings and that moral interactions accumulate over time as a surplus of skill, technology, trust, health, status, economic security, and general thriving. This is the common good that we share.Citation11–15 The Painless Parkers who took a few bucks from the public because they were quick with extractions have been replaced in just a century with a sound body of evidence-based research knowledge; equipment and delivery systems created, funded, and supported by industry; private and public sharing of the costs of care; lobbying by organized dentistry to ensure fair regulations; and dental schools that teach the knowledge, skills, and values to begin practice in the equivalent of four years or more rather than a year or two, plus apprenticeship. Professionals and the public they serve benefit from the collective and cumulative contributions of many who have contributed to the common good. The stronger the profession, the better oral health.
There is a relationship between moral action and professionalism. Cheaters gain relative personal advantage doing things that are not credited by their colleagues when their abuses are overlooked. In the case of dentists, one of the “others” with the potential for significantly justifying behavior is the profession. Being professional is more than a collection of individual behaviors by those with a common title or membership.
Generally, there are four kinds of agents in the professional mix. Solid professionals maintain a fair balance between positive contributions and personal benefits relative to their colleagues. They do not seek leadership positions or awards, nor do they embarrass themselves or their peers. There is no reason not to consider them to be ethical. They participate in the common good in a passive way. There are also leaders who are willing to invest in building the profession. The third type is commonly known as “free riders.”Citation16 They contribute less than they should or take more than is fair. They deplete the common good. In that sense they are “unethical,” not because they violated a principle but because they cheat and take what really belonged to others collectively. The fourth group is the entire set of external communities. No profession functions in isolation or has complete control over how they thrive or decline. Patients have some voice. More is heard and more forcefully from state licensing agencies, government regulators, industry, and insurance companies. An outsized influence that has rapidly and powerfully gained influence is the commercial structure of dental practices with its infusion of capital. The dental profession as an entire community interacts with other related communities and as such does so in terms of moral actions. It is simply inadequate to consider dental ethics to be only a matter of how individual dentists practice relative to each other and how they treat that segment of the population that agrees to be patients. The dental profession collectively is a moral agent, among other collective moral agents. To cite just one example of how profession-to-context relationship twist practice within the dentistry consider the case of those dentists who “game” the insurance industry. Insurers impose general requirements and restrictions in response. These fall on all dentists so the moral ones must pay the costs for the free riders.
Six examples will be given suggesting that MAP is better positioned to take up the slack in dependence on ethical theory and better meet the emerging challenges facing dentistry.
Isn’t it Enough to Tell Others About Ethical Theory?
Voluntary endorsement by individual practitioners of claims regarding high aspirational standards defined professionalism two hundred years ago. The first “Code of Professional Etiquette” of the American Dental Association urged consultation to fix prices, ruled out advertising, and lectured young dentists that they “should show proper deference to their seniors.”Citation17 Significant changes in how professionals related to each other and to patients started in the middle of the last century as the complexity and interaction of multiple, specialized parts showed its advantages.Citation18 Bioethics became a specialty in its own right in the 1970sCitation19 that thrives today in medicine to some extent because bioethicists can bill independently for their services. Dentistry took advantage of this resource, inviting ethics experts to suggest principles and teach the proper argot. The ADA added a superstructure for the Principles of Professional Conduct borrowed and modified from the Kennedy Institute of Ethics in the 1990s.Citation20 A standard on teaching ethical principles in dental schools was created by the Commission on Dental Accreditation at the same time.Citation21 States and specialties have various codes and require continuing education certification on ethics (largely knowledge of the dental practice act). About a dozen textbooks appeared. The American College of Dentists was a leader in this field, establishing a standing Ethics Committee in the 1970s.
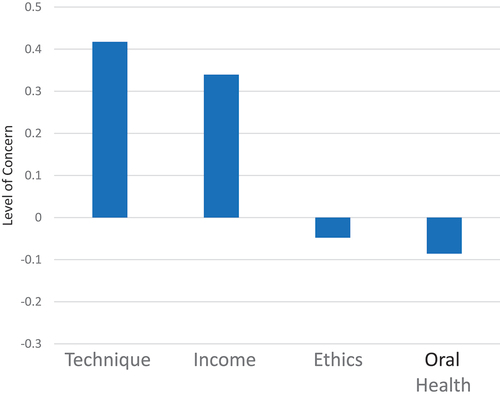
But attention to dental ethics is waning.Citation22 Continuing education ethics offerings at state dental meetings are rare. The number of ethics articles in peer-reviewed publications has fallen by 20% in the past decade, as has the number of hours devoted to ethics in school curricula. The dominant approach to teaching dental ethics in schools now is a guest lecture in the practice management course, on the assumption that ethics is modeled by all faculty members at all times. The ACD disbanded its Ethics Committee and states such as California have suspended their Judicial Councils and peer review programs. There are no full-time dental ethicists. In the American Dental Education Association Annual Survey of Seniors, ethics and biomedical theory vie with each other as the discipline that is given too much curriculum time.Citation23 Dentistry is the only profession, including all of health care, business, engineering and the like, that does not have a journal devoted to ethics. Commercial organizations offer “alternative ethical standards” for good and appropriate behavior, and membership in organized dentistry has declined. Dentists are just no longer that interested in ethics. displays the results of a study where dentists were asked which topics they would like to learn more about.Citation24 Distance above or below the 0-line on the vertical axis indicates degree of interest. Scores above the 0-line indicate preference for hearing positive information. Scores below the line represent interest in learning about negative situations. This pattern is probably reflected in the distribution of lectures presented at dental conventions. Discussion of ethics has remained largely on matters of dentists chairside values.
Figure 1. Level of interest (value) in representative dental topics.
Placebos are effective interventions for relieving the symptoms of disease and trauma, for a limited period of time and to the extent that trust can be maintained. But there are ethical issues even when they work.Citation25 Accurate diagnosis and engagement with the best actual therapeutic interventions might be postponed.
Perhaps the initial enthusiasm for attention to ethical theory in dentistry has passed its point of maximum impact.
There is No Need: Dentistry is Doing Well
A convincing case can be made for astounding advances in the technical accomplishments of dentistry over the past 75 years. Dentists are in the top 2 or 3% of American income earners, although there is a growing spread between the top performers and the bottom earners who are now losing ground when taking adjustments for inflation.Citation26 In 2023 dentists regained a top position as one of the “Best Jobs” in the country in the U.S. News & World Reports.Citation27 (Note emphasis on “jobs.”) The number of dental schools and thus the number of dentists has grown by about a third in the past few decades, mostly private schools.Citation28 Patients no longer report fear of pain as a deterrent to seeking care.Citation29 (Cost is the major barrier for about three-quarters of the population.) Roughly 60% of America’s dental bill is now picked up by insurance and the government.Citation26 We have moved from a public image of treating disease to one of providing cosmetic services. A scan of the fictitious business names of practices in California shows that, after the owner’s name, the location, or the specialty, “smiles” is the next most common designation, and the word “health” only appears a few times.
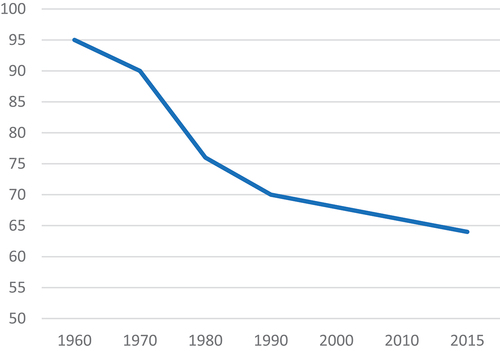
There are many positive indications that dentistry is thriving. But it is not obvious that the profession is making comparable strides in morality. Per the Gallup Survey of Honesty and Ethics in the Professions,Citation30 dentistry ranks lowest among the health professions. See . Dentists are comparable to grade school teachers and those serving in the armed forces. As shown in , membership in the American Dental Association has fallen from the high-90% range in the 1970s to currently about 65% of active practitioners.Citation31 In his aptly titled The Logic of Collective Action: Public Goods and the Theory of Groups, Mancur Olson reminds us that membership is a cardinal sign of the moral health of an organization.Citation32 Fellows of the American College of Dentists scored just 50% on a test of the contents of the American Dental Association’s Principles of Ethics and Code of Professional Conduct.Citation33 (Dental students scored a few points better.)
Figure 2. Gallup survey of public trust in health professions.
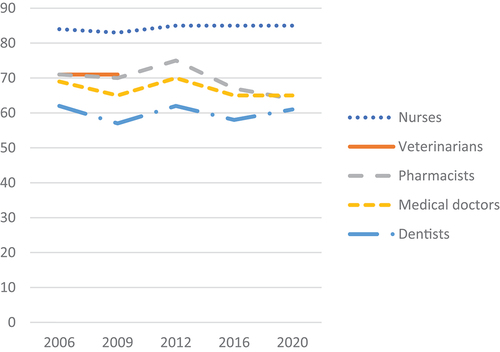
Figure 3. Membership in the American Dental Association.
Wrong Question
The standard presentation in schools and editorial and guest lectures focuses on ethical theory. Principles are reviewed and examples of indefensible behavior are used to illustrate the importance of identifying the good. This may include made-up dilemmas that pit one principle against another to build ethical reasoning skill. The cases are almost entirely focused on the relationship between a single dentist and a person who has sought the dentist’s care, and seldom involve all those who need oral health care or dentist-to-dentist relationships. Cases of disciplined licenses, which are public records, identifying patterns in practice and policy that would build public trust, and interventions to help colleagues are seldom part of the program for improving moral action and professionalism. It appears to be assumed that knowledge of principles translates into moral behavior. The principles may be self-evident but they are not self-activating.
By contrast, MAP focuses on actions that change the way dentists act and the way the profession adjusts to changes in society. There is a difference between aspiration standards and what the behavior groups are prepared to enforce. There are just too many principles. The nine characteristics of good dentists in the California Dental Association code have more common principles with the National Association of RealtorsCitation34 than with the five advanced by the American Dental Association. For the most part, these principles are descriptions of hoped-for member characteristics; adjectival descriptions of the best motives of the best members. Most dentists can point to examples where their behavior exemplifies these descriptions. We should celebrate the high points, but a broader look might prove valuable.
Principles are not action-generating, they are aprirationally descriptive. Although framed “Top Dentist” certificates are sometimes seen in dental office waiting rooms, the same cannot be said for lists of ethical standards. Criminals, mean and selfish people, and those who occasionally just bend the rules usually have a pretty good understanding of what principles they are violating. For example, UC Irvine behavioral philosopher Eric SchwitzgebelCitation35 surveyed libraries at elite universities such as Oxford, Harvard, and Michigan regarding missing books on topics in philosophy. Those dealing with ethics were half again up to one and a half times more likely to be taken. Ethics books were simply stolen more often. Usually, it is agreed that moral action is a separate question from ethical aspirations or what is said by a group about what it would like to see among its members.Citation36–40 To the extent that professional codes of conduct are written to highlight behavior for own’s colleagues, without input in their creation, monitoring, or response of others participating in the process, they may qualify as self-descriptions rather than moral standards elevating the common good of those who are licensed and those they serve.
Kelly and McPherson emphasize this gap between principles and behavior: “A cognitive analysis of the content of ethics cannot on its own provide an account of moral motivation.”Citation41, p. 197 Harvard professor of philosophy Hilary Putnum puts the matter more directly: “The idea that it should be the task of philosophy to deliver ex cathedra resolution of all our moral disagreements is absurd.Citation42 Principles tell others how a group sees itself at its best. It is third-party work. Charles Bertolami’s 2004 paper, “Why our ethics curricula don’t work,”Citation43 provoked a defensive reaction from those who teach ethics, but no evidence has been presented that Bertolami was wrong.
Just as there is confusion between knowing principles and acting morally, licensure and professionalism are sometimes mistakenly interchanged. Licensure is a privilege granted by state agencies to classes of individuals (not all of whom are professionals) to engage in commercial services for customers who are not normally able to recognize when they are being well served. Operational standards are set and enforced by the state, and not by licensed occupations. The late bioethicist Bernard GertCitation2,Citation3 was direct in stating that behavior cannot be judged to be moral without the full, informed consent and participation of all those affected. Expert knowledge and control are important, but insufficient. We cannot be moral on behalf of others; only with them. Third-party payers, government, as well as state bodies that regulate commercial activities of all who must have a license to provide public services in a commercial setting, each have important areas of concern in promoting morally sound oral health outcomes. So do patients. It is reasonable to assume that the best outcomes will be the result of harmonious cooperation among those involved by standards they all agree to.
The discussions in schools, in CE presentations, prizes for essay competitions, and in notes in the newsletters have been about ethical reasoning: giving an example of bad behavior and associating that with the proper principle. James Rest offers a broader view in his Four Component Model.Citation44 In addition to ethical reasoning, he says that those who make positive contributions also have skills in moral sensitivity (awareness that problems exist), moral integrity (willingness to engage in addressing problems), and moral courage (skill in effectively engaging others in building the good). ChambersCitation45 surveyed small groups of dental students, faculty members, and officers in the American College of Dentists, asking two questions: (a) how do you rate yourself on each of Rest’s four components? and (b) how do you rate others in the group? There was a modest but statistically significant association (r = .391) between self-ratings for reasoning on ethical theory and recognition by one’s colleagues as being adept at that. But there was no association between self-rating of ethical reasoning and being aware that moral problems exist (r = .075). The most disappointing finding was that the better one thinks he or she is at ethical reasoning the less likely colleagues are to perceive them as engaging in addressing moral problems (r = −.226) and the less effective they were seen to be in doing so (r = −.126).
This is Someone Else’s Problem
Those in the best position to influence the conduct of the profession are tempted to identify the problem as flowing from the questionable behavior of others. Tolstoy remarked on this human failing: “When people behave badly, they always invent a philosophy of life which represents their bad actions to be not bad actions at all, but merely results of unalterable laws beyond their control.Citation46, p. 34 It is easier to solve ethical problems when they are presented as hypotheticals or the concrete actions of others. A recent paperCitation47 reported that, in the opinion of those dentists interviewed, overtreatment is an ethical dilemma to be managed by individual dentists as they see fit.
Sometimes it is easier to complain about rather than confront supposed bad actors. Insurance companies and government regulations are seen as examples of those who “should know better” than to behave as they do. Or perhaps it is the students. Issues of academic integrity (cheating) are currently on the decline, having peaked in the 1980s.Citation48 The average age for disciplined licenses is the same for medicine and dentistry: 57.Citation49 Young dentists have the highest proportion of active practitioners as members of the ADA and research shows that their value profile more nearly resembles that of the American population than does the older cohort that undervalues caring and places more emphasis on authority, individualism, and only caring for those who “deserve to be treated.”Citation50
It is human nature to shift the blame, as documented in Tavis and Aronson’s book, Mistakes Were Made (but not by me).Citation51 Research by Papadakis and colleaguesCitation52 found that physicians with disciplined licenses were more likely to have engaged in “independent, personally advantageous behavior” (cheating?) while in medical school. The response in the profession to these studies tended to be negative regarding students but silent on what schools did not do as a result. Sometimes the profession fails to act professionally, preferring to consider bad behavior an individual matter. “We set the rules; they should follow them.”
The way questionable ethical behavior is handled is sometimes an example of a logical fallacy with the colorful name “No True Scotsman.”Citation53 The basic form of the tangled logic is as follows: “No true Scotsman would flee from a fight. McBumble fled. Therefore, he was no true Scotsman, thus proving again that all Scotsmen are brave.” Or “No ethical dentist would overtreat or abridge patient autonomy or violate a do-not-compete clause. There is a rumor that Dr. Slippery might have done something some would disapprove of. But if so, Slippery is not a true ethical dentist.” The net effect of such logic is to maintain the position that all true Scotsmen are fearless and that all dentists are ethical. But no program has been put in place to improve actual behavior.
Yes, but …
“We should let others try to fix issues regarding the voluntary bad behavior of colleagues” is an argument against professionalism. The red herring fallacy accepts the reality of shortcomings but excuses anyone from addressing them because they cannot be managed perfectly. At a recent city council meeting, dentists opposed to county water fluoridation outnumbers those supporting it. The matter was resolved in favor of a city resolution opposing fluoridation led by a council member saying that he understood the problem better than the professionals with their “evidence-based” research falderal. He reached under the table and pulled out a can of coke. He explained, “This is causing more problems than fluoridation can prevent. And we certainly aren’t going to tell kids what they can and cannot drink.”
The red herring argument goes something like this:Citation54 “A and B are both problems. B is worse than A, but we can’t do much about B. Therefore, we should not do anything about A either.” The correct argument is whether doing A is worthwhile on its own merits, all things considered. In the case of dentistry, red herring arguments might take any of the following forms. “Attitudes toward ethics are determined at an early age, so it would be a waste of time to teach ethics in dental schools. And certainly, it would be a poor allocation of resources to work on the problem among practitioners.” “Teledentistry or dental care provided by licensed ancillaries is not of the same quality as that which could be provided by dentists, so they should be prohibited.” “The dentists most in need of reading an article about dental ethics are the least likely to read one, therefore, we should not waste time publishing a paper talking about something like this.”
Reluctance of dentists to follow through in cases of justifiable criticism as required by the ADA Code of Professional Conducts under standard C.4 or the CDA Behavioral Principles 1.F.1 might involve red herring thinking. Some might say, “It is clear that we are acting unethically to offer unsubstantiated criticism of colleagues. So we should do nothing about possible cases of gross or continual faulty treatment we observe.” The number of disciplined licenses is small, and most complaints come from patients, with a few from staff. Benjamin Enke is one who would not criticize dentists as being “unethical” when overlooking bad practice. “People differ, not necessarily in how moral they are, but toward whom they are moral.”Citation55, p. 10 Among interviews with dentists on this topicCitation55 the most common response when poor work was identified was to tell the patient they had some problems that needed attention and then offering to perform that work themselves provided that the originally treating dentist was not involved.
A few decades ago the ADA established an ethical hotline to advise practitioners. The project was terminated for lack of participation. Dentists phoned for legal advice: staff and employee dentists phoned to report questionable ethical behavior of their employers. In a study of vignettes regarding moral challenges, such as former associates opening a nearby practice, the question was raised among members of the American College of Dentists: “Where would you turn for help in making an ethical decision?” Ninety percent of respondents answered that they would not involve anyone else: their personal understanding of ethics was sufficient.Citation56 A few said they would consult a code of ethics principles, but virtually none would involve a trained ethicist.
This is Not Your Concern
Decades ago it was popular to refer to the “silent contract” between professionals and the societies they served.Citation8,Citation9 The agreement was that a group having special knowledge and skills might be granted monopoly power over certain services and admission to the group in exchange for the promise to police performance among its members. In dentistry, this contract takes two forms.
As an ethical ideal this is explicit in both the California and American Dental Association’s codes of professional conduct: “Dentists shall be obliged to report … instances of gross or continual faulty treatment by other dentists.” It is not clear whether this applies to cases of overtreatment, fraudulent billing, and other non-technical behavior or just to technical quality. Approximately two-thirds of cases of disciplined licenses in California do not involve technical matters and among those that do, inadequate records and failure to diagnose are the largest “technical” problems.Citation49 Instances of dentists losing their ADA membership as a consequence of failing to report colleagues have not been documented. Enforcement of the implied contract is generally passed to state departments of consumer affairs or to third-party payers who are not part of the professional community.
Licensure of professionals extends beyond the implied contract because it is governed as a commercial privilege by the state. In 2015 the U. S. Supreme Court decided this matter in a case involving the Federal Trade Commission and the North Carolina Board of Dental Examiners,Citation57 Dentists serving on boards were defined as representatives of the state, not the profession. In its presentation before the Supreme Court, the Dental Board of North Carolina argued that dentists may be unwilling to serve unless they have controlling interest. The court scolded the board, citing the ADA Principles of Ethics and Code of Professional Conduct which calls, in the court’s opinion, on professionals to “follow high ethical standards including honesty, compassion, kindness, integrity, fairness, and charity.”
Each group establishes and maintains the margin of “cheating” it will accept. The West Point Honor Code states “I will not lie, cheat, or steal or tolerate anyone who does.” It is the second part about not tolerating dishonesty among colleagues that distinguished a profession from a group that pays dues for mutual gain. Research has shown that the existence of codes of integrity make little difference to moral behavior. But enforcement of them by one’s peers (professionalism) certainly does.Citation4, Citation6, Citation7
Summary
Evidence, sometimes uncomfortable evidence, has been presented that the moral tone of dentistry has declined somewhat during the half century that the profession has looked to bioethical theory and lists of principles as the way it talks about theory. During this period important changes have occurred in dental technique and the commercial aspects of oral health and smile care. Dentists have been asked to reflect on what they do at chairside. It is logically possible that the erosion of public trust and the invasion of nonprofessional values would have been worse had dentistry not embraced principles as a way of talking about ethics.
An alternative positon has been developed here. MAP (moral action and professionalism) are behaviors that lead directly to strengthening the profession and those it serves. They are operational definitions of bringing about the good rather than abstract intentions an individual can consider while deciding what to do. Those who do not cheat by gaining in unjustified ways at others’ expense, or who do so less often than they did in the past, are moral. Being professional means contributing one’s fair share to the common good and not taking more of it than one is entitled to. The two imperatives are related. We look to our professional colleagues to define how much cheating is permitted and the more individual cheating that occurs, the weaker the profession. The individual dentist is responsible to others; the profession is responsible to society. It is the behavioral interactions, not the good intentions, that count.
Ethical approval
No individual provided private information with respect to this manuscript, thus no IRB approval was required
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
David W. Chambers
Dr. David W. Chambers is the director of the Clinical Judgment Laboratory at the University of the Pacific dental school and editor emeritus of the American College of Dentists. He compiled Dental Ethics:The New Professionalism for the ACD and authored a monthly column on ethics in this journal from 2009 to 2019.
References
- Daniels N. Just Health Care. Cambridge, UK: Cambridge University Press; 1985.
- Bryan V, Sanders S, Kaplan LE. The Helping Professional’s Guide to Ethics: Theory and Practice. 2nd ed. New York: Oxford University Press; 2022.
- Gert B. Common Morality: Decision What to Do. Oxford, UK: Oxford University Peress; 2004.
- Gert B. Morality: Its Nature and Justification. New York: Oxford University Press; 1998.
- Ariely D. The (Honest) Truth About Dishonesty. How We Lie to Everyone – Especially Ourselves. New York: Harper Collins; 2012.
- Bok S. Lying: Moral Choice in Public and Private Life. New York: Vintage Books; 1978.
- Callahan D. The Cheating Culture: Why More Americans are Doing Wrong to Get Ahead. New York: Harvest; 2004.
- Rhode DL. Cheating: Ethics in Everyday Life. New York: Oxford University Press; 2018.
- Brody H, Doukas D. Professionalism: a framework to guide medical education. Med Educ. 2014;48(10):980–8. doi:10.1111/medu.12520.
- Welie JVM. Is dentistry a profession? Part 3. Future challenges. J Can Dent Assoc. 2004;70:675–678.
- Boehm C. Moral Origins: The Evolution of Virtue, Altruism, and Shame. New York: Basic Books; 2012.
- Gauthier D. Morals by Agreement. Oxford, UK: Oxford University Press; 1986.
- Heinrich J. The Secret of Our Success. Princton: Princeton University Press; 2016.
- Sober E, Wilson DS. Unto Others: The Evolution and Psychology of Unselfish Behavior. Cambridge, MA: Harvard University Press; 1998.
- Ostrom E. Governing the Commons: The Evolution of Institutions for Collective Action. Cambridge, UK: Cambridge University Press; 1990.
- Wilson DS. Does Altruism Exist? Culture, Genes, and the Welfare of Others. New Haven: Yale University Press; 2015.
- American Dental Association. Transactions of the American dental association sixth annual meeting, Boston, July 31, 1866.
- Nuland SB. Doctors: The Biography of Medicine. New York: Vintage; 1988.
- Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 6th ed. New York: Oxford University Press; 2009.
- American Dental Association. Principles of Ethics and Code of Professional Conduct. Chicago: The Association; 2005.
- Predoctoral dental education accreditation standards. https://coda.ada.org/-/media/project/ada-organization/ada/coda/files/predoc_standards.pdf?rev=20eabc229d4c4c24a2df5f65c5ea62c8&hash=B812B8A2FAF6D99F37703EE081B48E58. Published December 2023.
- Chambers DW. Survey of dental ethics education: 2018. J Am Coll Dent. 2020;87:48–58.
- Istrate EC, Cooper BL, Singh R, Gül G, West KP. An analysis of the results of the ADEA 2023 survey of U.S. Dental school seniors. J Dent Educ. 2023;87(11):110607–111620. doi:10.1002/jdd.13392.
- Chambers DW. Dentists’ values: actual and projected. J Am Coll Dent. 2019;86:32–43.
- Cheah PY, Steinkamp N, von Seidlein L, Price RN. The ethics of using placebo in randomised controlled trials: a case study of a Plasmodium vivax antirelapse trial. BMC Med Ethics. 2018;19(1). doi:10.1186/s12910-018-0259-4.
- Chambers DW. Factors driving recent changes in dentists’ incomes. J Cal Dent Assoc. 2014;42(5):331–337. doi:10.1080/19424396.2014.12221361.
- Dentistry among top U.S. jobs. https://adanews.ada.org/ada-news/2023/january/dentistry-rises-to-top-10-in-best-jobs-list/. Published December 2023.
- U.S. dental schools. http:///2012%20Dental%20Schools%20list.pdf. Published December, 2023.
- Reasons for avoiding dental care. https://www.ada.org/resources/research/health-policy-institute/coverage-access-outcomes/oral-health-and-well-being. Published December, 2023.
- Gallup Survey of Public Trust in Professions. https://news.gallup.com/poll/1654/Honesty-Ethics-Professions.aspx. Published December, 2023.
- Chambers DW. ADA News and ADA membership. J Am Coll Dent. 2018;85(3):38–43. doi:10.1145/3375408.3375411.
- Olson M. The Logic of Collective Action: Public Goods and the Theory of Groups. Cambridge, M: Harvard University Press; 1965.
- Chambers DW. Dentists’ knowledge of ADA code. J Am Coll Dent. 2020;87:26–34.
- American Association of Realtors Code of Ethics. https://www.nar.realtor/about-nar/governing-documents/code-of-ethics/2024-code-of-ethics-standards-of-practice. Published April 2024.
- Schwitzgebel E. Do ethicists steal more books? Phil Psych. 2009;22(6):711–725. doi:10.1080/09515080903409952.
- Griffin J. Value Judgment: Improving Our Ethical Beliefs. Oxford: Clarendon Press; 1996.
- Railton P. Facts, Values, and Norms: Essays Toward a Morality of Consequence. Cambridge, UK: Cambridge University Press; 2003.
- Scanlon TM. What We Owe to Each Other. Cambridge, MA: Belknap Press; 1998.
- Singer P. The Most Good You Can Do. New Haven: Yale University Press; 2015.
- Williams B. Ethics and the Limits of Philosophy. Cambridge, MA: Harvard University Press; 1985.
- Kelly RJ, McPherson LK. The naturalist gap in ethics. In: Caro MD Macarthur D, eds. Naturalism and Normativity. New York: Columbia University Press; 2010: 193–204.
- Putnam H. Values and norms. In: The Collapse of the Fact/Value Dichotomy and Other Essays. Cambridge, MA: Harvard University Press; 2002.
- Bertolami CN. Why our ethics curricula don’t work. J Dent Educ. 2004;68(4):414–425. doi:10.1002/j.0022-0337.2004.68.4.tb03758.x.
- Rest JR, Narváez D, Eds. Moral Development in the Professions: Psychology and Applied Ethics. Hillsdale, NJ: Lawrence Erlbaum; 1994.
- Chamber DW. Developing a self-scoring comprehensive instrument to measure rest’s four-component model of moral behavior: the moral skills inventory. J Dent Educ. 2011;7(1):23–35. doi:10.1002/j.0022-0337.2011.75.1.tb05019.x.
- Tolstoy L. The Slavery of Our Times. Christ Church, UK: Free Age Press; 1901.
- Holden ACL, Adam L, Thomson WM. Dentists’ perspectives on commercial practice in private dentistry. JDR Clin Trans Res. 2022;7(1):29–40. doi:10.1177/2380084420975700.
- Chambers DW. A primer on dental ethics: part II. Moral behavior. J Am Coll Dent. 2007;74:38–51.
- Chambers DW. Disciplined licenses. J Am Coll Dent. 2018;85:30–39.
- Chambers DW. The values of dentists. J Am Coll Dent. 2019;86:32–43.
- Tavris C, Aronson E. Mistakes Were Made (But Not by Me). New York: Mariner Books; 2007.
- Papadakis MA, Hodgson CS, Teherani A, Kohhatsu ND. Unprofessional behavior in medical school is associated with subsequent disciplinary action by a state medical board. J Med Reg. 2004;90(1):16–23. doi:10.30770/2572-1852-90.1.16.
- Pinker S. Rationality: What it is, Why it Seems Scarce, Why it Matters. New York: Penguin; 2021.
- Tindale CW. Fallacies and Argument Appraisal. Cambridge, UK: Cambridge University Press; 2007.
- Enke B. Values and voting parties. Harv Mag. January–February 2024;125:10–12.
- Chambers DW. What dentists do when they recognize faulty treatment: to tattle or build a moral community? J Am Coll Dent. 2017;84:32–66.
- Chambers DW. Ethical touchstones. J Am Coll Dent. 2020;87:35–40.