
ABSTRACT
Background: Enamel defects (EDs) are commonly reported dental findings in preterm/low birthweight children. EDs potentially increase caries susceptibility.
Aim: To assess the prevalence of EDs and dental caries in a group of preterm children (aged 5–10 years) in Dubai, United Arab Emirates (UAE).
Methodology: A retrospective cohort study of medical records of 62 preterm children (mean age 8.1 ± 1.54) and 62 full-term children (mean age 8.1 ± 1.73) of both genders born in a UAE children’s hospital were studied. These children were dentally assessed for EDs and caries by a calibrated examiner.
Results: EDs were 4.34 times more prevalent among preterm children [odd ratio (OR) = 4.338, CI 95% [2.010–9.366]. The prevalence of EDs in the pre-term group was 58.15%, significantly higher (P < 0.01) than the full-term control group (24.2%). Birth weight, intubation and type of delivery were statistically significant factors contributing to EDs. In the primary dentition, the mean dmft was 4.61 ± 4.30, while in the permanent dentition DMFT was 0.38 ± 0.99. There was a statistically significant difference in permanent teeth caries experience amongst pre-term children compared to the full-term control as measured by DMFT (P = 0.008).
Conclusion: EDs and dental caries in permanent dentition in the pre-term group were significantly higher than the full-term group.
1. Introduction
A premature infant as defined by the World Health Organization (WHO) is any newborn with less than 37 weeks’ gestation or fewer than 259 days after the last menstrual period with a birthweight less than 2500 g [Citation1]. Preterm birth prevalence is increasing and is estimated to be 15 million per year worldwide [Citation2]. Pre-term and/or low birthweight deliveries affect many aspects of health and increase the economic, social, and individual demands impacting the quality of life of these children [Citation3]. In recent years, the improvement of perinatal care aided by significant medical advances resulted in the reduction of mortality and morbidity in pre-term children. However, some complications will inevitably be present especially with a lower gestational age [Citation4].
Primary teeth development starts early in pregnancy (week 12) and the whole process of enamel formation and maturation is completed around 12 months postnatally [Citation5]. While, enamel development of first permanent teeth starts at week 28 with the mineralization commencing at the time of birth and is completed during the first 3 years of life. During this process, any disturbance in amelogenesis will result in either a quantitative or a qualitative defect [Citation6]. The qualitative defects result in molar-incisor hypomineralization (MIH) in the permanent dentition or hypomineralized second primary molars (HSPM) in the primary dentition [Citation7].
Multiple possible etiological factors for the enamel defects have been suggested. Prenatal susceptibility (like illness during pregnancy), perinatal susceptibility (like premature or prolonged birth, low birth weight, cesarean delivery, and birth complications) and postnatal susceptibility (like early childhood illness or medication or breastfeeding) are all reported etiological factors related to enamel defects [Citation8]. Enamel defects might also occur due to the early disturbances in the metabolism of calcium exaggerated by the fact that calcium and phosphorus accumulate mainly during the third trimester of pregnancy [Citation9]. Enamel disturbances have many clinical implications such as esthetic concerns and social embarrassment due to the dental appearance, associated symptoms and sensitivity, increased caries susceptibility, altered occlusal function and treatment challenges. Moreover, enamel defects in the primary dentition might be predictive of similar defects in the permanent one [Citation10,Citation11].
Hypoplastic enamel is associated with increased susceptibility to dental caries due to the reduction in mineralization, increased porosity, thinner enamel, increased tooth breakdown, and irregular surfaces allowing more bacterial aggregation. This is compounded by long-term intake of sucrose-containing medications and associated inaccurate feeding practices [Citation12,Citation13]. Therefore, more attention needs to be given to premature children including early diagnosis and preventive care especially in the United Arab Emirates (UAE), a country with a high prevalence of dental decay [Citation14,Citation15]. Thus, this study aimed to assess the prevalence of enamel defects and caries status in preterm born children in Dubai, UAE and compare them with their full-term healthy counterparts.
2. Material and methods
2.1. Study sample
This was a retrospective cohort study of UAE and non-UAE children who were born prematurely before the 37th gestational week in Latifa hospital, a governmental hospital in Dubai, UAE. Latifa hospital is the major referral centre for most complicated pregnancies and premature births in Dubai and the Northern Emirates of the UAE. The medical records in Latifah hospital were reviewed for all births between January 2007 and December 2012 (current age 5–10 years). The total number of preterm children included in the records was 2640. A sample size calculation was conducted prior to data collection. For every birth year, 100 children were randomly selected by a computer randomization software as per the serial number. Children with special health-care needs were excluded. A total of 600 families were contacted through the phone with a pre-set script. Out of the families who expressed their interest to participate, only 62 preterm children attended the clinic for their examination appointment. The control group comprised of age- and gender-matched full-term healthy children who were born in Latifah Hospital and attended Dubai Dental Hospital for their regular treatment. This study was approved by the Mohammed Bin Rashid University of Medicine and Health Sciences (MBRU) Institutional Review Board and the Ethics and Research Committee at the Dubai Health Authority (DHA) (DSREC-10/2017_09).
2.2. Examiner’s calibration
The principal examiner was trained and calibrated to use the recently proposed standardized scoring method by the European Academy of Paediatric Dentistry (EAPD) for enamel defects by Ghanim et al. (2015) [Citation16]. Intra- and inter-examiner reliability with an expert consultant was done and calculated using Kappa statistics prior to starting the data collection. The results were as follows: Intra-examiner (Kappa) was 100% concordance. While for Inter-examiner (McNemar’s test) there was high agreement (kappa = 0.92–0.94).
2.3. Clinical examination
Data were collected using clinical data recording sheet through dental examination. The list of the participants from Latifa hospital was coded anonymously and all references to the identity of the child were eliminated by one of the co-investigators who invited the participants in the study via phone call. The participants' list which consisted of participant’s serial number, name and phone number was provided to the main investigator who was blinded of their status of birth.
A pilot study conducted for the clinical examination sheet including 10 individuals to evaluate the study methodology. These records were not included in the final sample. Participants of the study who attended the clinic and signed the consent form were first examined intra-orally for enamel defects and decayed missing filled teeth (dmft/DMFT). Once the examination was completed, mothers were then asked to fill the questionnaire and the details of their child’s birth. A pilot study for the questioner was conducted also with 10 of the mothers of the children attending our clinics regularly to ensure the accuracy and clarity of the questionnaire. The results of this pilot study were excluded from the study results. The clinical examination was performed at the dental clinics of Dubai Dental Hospital/Hamdan Bin Mohammed College of Dental Medicine of MBRU.
The following indices were recorded:
1) Enamel defects index (MIH/HSPM) by Ghanim et al. (2015). This index was used to record enamel defects in both primary and permanent dentitions for each participant [Citation16]. The number of teeth along with the type of defects were recorded together with the total number of erupted teeth (primary and permeant teeth) in the data recording sheet. The following key features, as agreed by the EAPD were used to identify teeth affected by enamel defects, MIH and HSPM: (Demarcated opacities, Post-eruptive enamel breakdown (PEB), atypical restorations, atypical carious lesions, extraction of molar due to MIH/HSPM). These key features along with a further breakdown of each feature are explained in .
Table 1. European academy of pediatric dentistry enamel defects index (Ghanim et al. 2015)
In order for a surface to be included in the examination, at least 1/3 of the surface or the crown length of the incisor must be visible. When two or more MIH/HSPM lesions exist per surface (example, creamy and brown opacities) the most severe score is assigned. The tooth was considered normal if there was any doubt about the presence of the defect.
2) Caries Index: DMFT\dmft index according to WHO criteria (WHO 1997) was recorded after the dental examination of the children in both groups [Citation17]. Both primary and permanent teeth (t/T) were examined and given a specific code as in d/D (decayed), m/M (missing) and f/F (filled).
2.4. Questionnaire interview
A structured questionnaire, slightly modified from the questionnaire previously used by Cruvinel et al. [Citation18] was used to obtain the demographic details (date of birth, gender, mother education and occupation). The medical history was obtained from Latifah hospital medical records to determine the possible association with the dental defects. The following information was obtained from the medical histories: (preterm or full-term birth/weight at birth/type of delivery (caesarean, vaginal)/any aided respiratory device used for the infant).
In addition, the following related information were obtained from the mothers by the questionnaire: (Diseases during pregnancy/hospitalization in the first years of life/systemic infectious diseases occurred in the first 3 years of life [such as: pneumonia, tonsillitis, ear infections, chickenpox, rubella, measles, systemic antibiotic medication]/history of trauma).
2.5. Statistical analysis
Data were entered into the computer using SPSS for windows version 20.0 (SPSS Inc., Chicago, IL 2009). Results were cross-tabulated to examine the independency between variables. Statistical analysis was performed using χ2-square for the test of association and Fisher’s exact test as appropriate. Where two or more continuous independent variables examined, t-test and analysis of variance were used. Frequency tables’ bar and lines graphs were utilized as descriptive statistics. A P-value of less than 0.05 was considered significant in all statistical analyses.
3. Results
The ages of the children in each group (n = 62) ranged from five to 10 years, with a mean of 8.1 (±1.54) in the preterm-group, compared to 8.1 (±1.73) in the full-term group (P = 0.913). For gender distribution, 32 (51.6%) of pre-term children were males compared to 30 (48.4%) females, and in the full-term group, 34 (54.8%) were males compared to 28 (45.2%) females (P = 0.429). No statistically significant differences existed between age, gender, mothers’ education and occupation in the pre-term and full-term group (P > 0.05).
Regarding the medical history there was a statistically significant difference between the two groups in relation to their weight at birth, need for intubation, diseases during pregnancy, systemic diseases and admissions early in life (P < 0.05). History of traumatic dental injuries was the only variable with no statistically significant difference between the pre-term and full-term group (P = 0.301).
3.1. Enamel defects prevalence
The collected data revealed that the overall prevalence of the enamel defects in both groups was 41%. The preterm group prevalence was 58.15% and was significantly higher (P < 0.001) compared with the full-term group 24.2%. There was an association between being preterm and enamel defects in such a way that the enamel defects were 4.34 times more prevalent among preterm children compared with full-term children [odd ratio (OR) = 4.338, CI 95% [2.010–9.366]].
3.2. Enamel defects and birthweight
shows the distribution of birthweight among the two groups. More than half of the pre-term group [37 (59.7%)] had low birth weights, followed by very low birth weights [22 (35.5%)] while only 3 (4.8%) had normal birth weights. On the other hand, full-term group were mostly of normal birth weight [58 (93.5%)], 4 (6.5%) had low birth weights and none of them had a very low birth weight (P < 0.001).
Figure 1. Distribution of participants’ birthweight
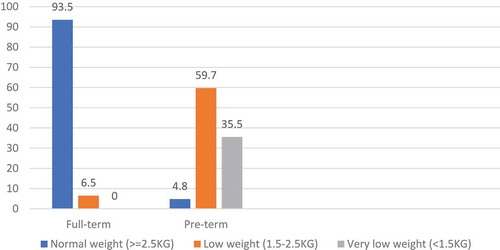
The highest proportion of enamel defects was found in the pre-term infants with abnormal birth weights (low and very low birth weights; 94.4%). No enamel defects presented in the majority of the full-term infants who had a normal birth weight (95.7%). Birth weight was found to be a statistically significant factor contributing to enamel defects (P < 0.001).
3.3. Potential causes of enamel defects
This study also investigated the other possible causes of enamel defects – presented in - such as type of delivery, intubation, diseases during pregnancy, hospitalization and systemic disease early in life as recalled by the mothers.
Table 2. Potential causes of enamel defects
Regarding the type of the delivery, in the pre-term group, the majority, 69.4%, of those whom had a caesarean delivery had enamel defects. Most of the full-term group were through vaginal delivery and 76.6% did not develop any enamel defects (P = 0.02), indicating that the type of delivery was a statistically significant factor contributing to enamel defects.
Intubation was among the most significant factors contributing to enamel defects (P-value <0.001). In the full-term group, we had only two (13.3%) children who were intubated and both of them developed enamel defects. While in the pre-term group we had 29 (80.6%) of children who were intubated and had enamel defects as a result.
For complications during pregnancy: antibiotic exposure, hospitalization, systemic disease in the first 3 years of life and history of previous dental trauma (P > 0.05) indicating that there was no statistically significant relationship between these factors and enamel defects.
3.4. Types of enamel defects
demonstrates the different types of enamel defects. The most common type of enamel defects reported in both full and pre-term groups was white or creamy demarcated opacities, accounting for 22.6% of the defects in the full-term and 41.9% in the pre-term group with a statistically significant difference between the two groups (P = 0.017). [odd ratio (OR) = 2.476, CI 95% [1.135,5.403]. The second most common type of defect in the preterm group was post-eruptive breakdown (PEB) with a statistically significant difference between the two groups (P = 0.017). [OR = 3.847, CI 95% [1.178, 12.562]].
Table 3. Types of enamel defects in study participants
The presence of all the yellow or brown demarcated opacities, atypical restorations, diffuse opacities, hypoplasia and hypomineralization defects (not MIH/HSPM) was not statistically significantly different between the pre-term and full-term group (P-values: 0.5, 0.372, 0.5, 0.248, 0.122, respectively).
3.5. Prevalence of dental caries
The prevalence of caries in the primary dentition among preterm children was 72.6% while for the full-term control it was 69.4%. In the same context, the prevalence of caries in the permanent teeth among pre-term children was 38.7% while for the full-term controls it was 17.7%.
3.6. Decayed, missing and filled teeth (DMFT/dmft) caries indices
Permanent (DMFT) and primary (dmft) dentitions’ caries status is summarized in . There was a statistically significant difference in permanent teeth caries experience amongst pre-term children compared to the full-term control as measured by DMFT (1.00 ± 1.55 vs 0.38 ± 0.99, P = 0.008).
Table 4. Permanent dentition (DMFT) and primary caries status (dmft)
4. Discussion
The prevalence of enamel defects and caries status in preterm born children in Dubai has not been investigated yet. Therefore, this study provided an opportunity to assess these oral health problems among those who were born prematurely in Latifa hospital in Dubai and compare them to a matched full-term control. The preterm children in the study and control groups were matched in age and gender. No significant differences existed in mothers’ education and occupation.
The recent proposed standardized scoring method by the EAPD for enamel defects by Ghanim et al. (2015) was used to identify and record enamel defects [Citation16]. This method was introduced to enable the researcher to use a standardized tool and criteria which would lead to consistent results and allow proper comparison between different studies. In the present study, enamel defects’ prevalence in the preterm group was significantly higher (58.15%) compared with the full-term group (24.2%). This was similar to findings in other studies such as Takaoka et al. from Brazil [Citation19] who reported an 87% prevalence of enamel defects in the preterm group compared to 44% in the full-term group. Similarly, Aine et al. from Finland [Citation9] reported a 78% prevalence of enamel defects in the primary dentition of preterm children compared to 20% in the full-term group and 83% prevalence in the permanent dentitions of preterm children compared to 36% in the full-term group.
In our study, we found that being preterm increases the risk of developing enamel defects by 4.34 times. In comparison, Arrow et al. in Australia [Citation20] found that prematurity increases the risk of enamel defects 2.75 times. A possible explanation of the high prevalence of enamel defects among the pre-term infant group can be explained by the different chemical and the microscopic properties of the dental hard tissues of the pre-term infants [Citation21,Citation22], although this aspect was not assessed in our study.
Birth weight in our study group was a statistically significant factor contributing to enamel defects in primary and permanent dentition combined. Pre-term infants with low birth weight had the highest incidence of enamel defects (94.4%). In comparison, Wagner et al. [Citation23] found that being pre-term with low birth weight makes the child 4.9 times more at risk of developing enamel defects compared to full-term children with normal birth weight. While, Lunardelli et al. reported slightly more than double the risk of enamel defects in the primary dentition of low birth-weight children (OR = 2.6) compared to full term-born children [Citation24]. The higher prevalence of enamel defects in low birth-weight children can be explained by the increased morbidity of these children with more complications and interventions needed in the short and long term which might leave an impact on the dental tissues [Citation25].
Mode of delivery in the current study group was a significant factor contributing to an increased risk of enamel defects. Most of the pre-term delivery mode was by a caesarean section (73.3%), while in the full-term group vaginal deliveries were the most common (71.9%). This was in agreement with a Brazilian study [Citation18] where the type of birth was significantly associated with the occurrence of hypoplasia. These findings could be because caesarean sections are usually prone to more complications which might be reflected as enamel defects in the developing dentition. In contracts, a study by Allazzam et al. [Citation26] in Saudi Arabia [Citation26] did not find any association between mode of delivery and the presence of enamel defects.
Infants’ intubation was significantly related to enamel defects in this study. Takaoka et al. in Brazil also reported similar findings [Citation19]. Another Brazilian study by Gravina et al. found all the children who were intubated and received ventilatory support developed hypoplasia [Citation27]. Mechanical trauma from intubation in pre-term infants was reported to have an effect on the oral structures [Citation28]. Endotracheal and oral-gastric intubation can create an excessive force on the developing crowns of the teeth in the palate disturbing the amelogenesis process resulting in enamel defects [Citation29]. Although all the preterm intubated infants in our sample were nasally intubated instead of the oral intubation, enamel defects still exist in the majority of the intubated infants which could be linked to the associated respiratory distress and the hypoxia rather than a direct physical effect of the tube into the oral tissue.
We did not find any association between enamel defects and the following factors: complications and diseases during pregnancy, hospitalization early in life and systemic infectious diseases and antibiotic exposure during the first 3 years of life. Allazzam et al. in Saudi Arabia had similar findings in their study [Citation26]. Wuollet et al. in 2016 in Finland [Citation30] studied the association between childhood illness and antibiotic exposure as possible risk factors of MIH. They found that most types of childhood illness were not associated with MIH, except for acute otitis media; however, this association was not statistically significant. Regarding antibiotic usage, they found that children who had at least one course of amoxicillin or penicillin had a higher risk for MIH; however, other antibiotic did not increase the risk. Wagner et al. in their study in 2017 found that children with systemic diseases had double the risk of developing enamel defects (OR 2.45), similarly, does the antibiotic exposure (OR 2.21), while hospitalization early in life increase the risk of enamel defects to fourfold (OR 4.44) [Citation23].
In our study, demarcated opacities were the most common type of enamel defects with a statistically significant difference between the two groups. The least common type of defect observed was diffuse opacities affecting only one pre-term child and none of the full-term children. Similar findings were reported in a cohort study in 2017 by Wagner et al. in Germany [Citation23] who found that the demarcated opacity was the most common type of defect affecting 75.0% of the studied population and the diffuse opacity was the least occurring type of defect (5.0%). Allazzam et al. in Saudi Arabia reported the same findings [Citation26].
In the present study, there was a statistically significant difference in the DMFT index between pre-term and full-term groups. Nelson et al. [Citation31] studied dental caries in very low birth-weight adolescents and reported a similar finding. Kumar et al. [Citation32] in India [Citation32] studied the presence of dental caries in pre-term children aged 2–8 years with enamel defects. They reported an increased risk of dental caries in the preterm group compared to the full-term.
Suggested possible factors besides enamel defects that can contribute to a higher risk of caries among the pre-term children could be, increased consumption of sugary medications due to increased morbidity rate, xerostomia as a result of some medications, high caloric diet to gain more weight and higher reflexes among the pre-term children [Citation33]. Moreover, the rough surfaces of the enamel defects can be easily occupied by dental biofilm and streptococcus mutans species, this early colonization of the cariogenic bacteria increases the risk of developing dental caries [Citation34].
In the present study, a lower mean dmft was found in the pre-term group compared to the full-term group; however, the difference was not statistically significant. Another study carried out in Thailand in 2016 reported that the preterm children had lower dmfs compared to full-term children (12.9 ± 15.1 versus 14.4 ± 12.3), respectively [Citation35]. A possible explanation of the above findings could be due to enhanced care from the parents of their prematurely born child [Citation31,Citation35]. Another possible reason reported by Ramos et al. that pre-term children with very low birthweight had a significant delay in the eruption of the deciduous dentition when compared to full-term infants considering their chronological age [Citation36].
As most questionnaire-based studies, an inevitable possible limitation of this study is the accuracy of the information given by mothers who some of them might not be recall pre-, peri- and post-natal information. In addition, having a prospective cohort design will allow more accurate assessment of possible influencing early life factors and their relationship with enamel defects.
In summary in the present study, enamel defects were significantly higher and four times more common in the preterm group compared to the full-term control. Birth weight, mode of child delivery and intubation were significantly related to the occurrence of enamel defects. DMFT index was significantly higher amongst pre-term group compared to the control.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Acknowledgments
The authors would like to thank the participants, Dr. Mahmoud ElHalik in Latifah Children’s Hospital and Dubai Health Care Authority for their great cooperation, which made this study achievable.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- World Health Organization [WHO]. International classification of diseases and related health problems. 10th Revision ed. Geneva: WHO Library Cataloguing-in-Publication Data; 2010.
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth bates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–7.
- Lai PY, Seow WK, Tudehope DI, et al. Enamel hypoplasia and dental caries in very-low birthweight children: a case-controlled, longitudinal study. Pediatr Dent. 2000;19:42–49.
- Franco KMD, Line SRP, de Moura-ribeiro MVL. Prenatal and neonatal variables associated with enamel hypoplasia in deciduous teeth in low birth weight preterm infants. J Appl Oral Sci. 2007;15(6):518–523.
- Suckling GW. Developmental defects of enamel-historical and present-day perspectives of their pathogenesis. Adv Dent Res. 1989;3(2):87–94.
- A review of the developmental defects of enamel index (DDE Index). Commission on oral health, research & epidemiology. Report of an FDI working group. Int Dent J. 1992;42:411–426.
- Elfrink MEC, Ten Cate JM, Jaddoe VWV, et al. Deciduous molar hypomineralization and molar incisor hypomineralization. J Dent Res. 2012;91(6):551–555.
- Silva MJ, Scurrah KJ, Craig JM, et al. Etiology of molar incisor hypomineralization – a systematic review. Community Dent Oral Epidemiol. 2016;44(4):342–353.
- Aine L, Backström MC, Mäki R, et al. Enamel defects in primary and permanent teeth of children born prematurely. J Oral Pathol Med. 2000;29(8):403–409.
- Seow WK. Enamel hypoplasia in the primary dentition: a review. ASDC J Dent Child. 1991;58(6):441–452.
- Rodd HD, Abdul-Karim A, Yesudian G, et al. Seeking children’s perspectives in the management of visible enamel defects. Int J Paediatr Dent. 2011;21(2):89–95.
- Kowash MB. Severity of early childhood caries in preschool children attending Al-Ain dental center, United Arab Emirates. Eur Arch Paediatr Dent. 2015;16:319–324.
- Law V, Seow WK. A longitudinal controlled study of factors associated with streptococcus mutans infection and caries lesion initiation in children 21 to 72 months old. Pediatr Dent. 2006;28(1):58–65.
- Alayyan W, Al Halabi M, Hussein I, et al. A systematic review and meta-analysis of school children’s caries studies in gulf cooperation council states. J Int Soc Prev Community Dent. 2017;7(5):234–241.
- Kowash MB, Alkhabuli JO, Dafaalla SA, et al. Early childhood caries and associated risk factors among preschool children in Ras Al-Khaimah, United Arab Emirates. Eur Arch Paediatr Dent. 2017;18(2):97–103.
- Ghanim A, Silva MJ, Elfrink MEC, et al. Molar incisor hypomineralisation (MIH) training manual for clinical field surveys and practice. Eur Arch Paediatr Dent. 2017;18(4):225–242.
- World Health Organization [WHO]. Oral health surveys: basic methods. 4th ed. Geneva: World Health Organization; 1997.
- Cruvinel VRN, Gravina DBL, Azevedo TDPL, et al. Prevalence of enamel defects and associated risk factors in both dentitions in preterm and full term born children. J Appl Oral Sci. 2012;20(3):310–317.
- Takaoka LAMV, Goulart AL, Kopelman BI, et al. Enamel defects in the complete primary dentition of children born at term and preterm. Am Acad Pediatr Dent. 2011;33:171–176(6).
- Arrow P. Risk factors in the occurrence of enamel defects of the first permanent molars among school children in Western Australia. Community Dent Oral Epidemiol. 2009;37(5):405–415.
- Rythén M, Norén JG, Sabel N, et al. Morphological aspects of dental hard tissues in primary teeth from preterm infants. Int J Paediatr Dent. 2008;18(6):397–406.
- Rythén M, Sabel N, Dietz W, et al. Chemical aspects on dental hard tissues in primary teeth from preterm infants. Eur J Oral Sci. 2010;118(4):389–395.
- Wagner Y. Developmental defects of enamel in primary teeth - findings of a regional German birth cohort study. BMC Oral Health. 2017;17(1):10.
- Lunardelli SEPM. Breast-feeding and other mother-child factors associated with developmental enamel defects in the primary teeth of Brazilian children. J Dent Child. 2006;73:70–78.
- Whatling R, Fearne JM. Molar incisor hypomineralization: a study of aetiological factors in a group of UK children. Int J Paediatr Dent. 2008;18(3):155–162.
- Allazzam SM, Alaki SM, El Meligy OAS. Molar incisor hypomineralization, prevalence, and etiology. Int J Dent. 2014;2014:234508.
- Gravina DBL, Cruvinel VRN, Azevedo TDPL, et al. Enamel defects in the primary dentition of preterm and full-term children. J Clin Pediatr Dent. 2013;37(4):391–395.
- Alves PVM, Luiz RR. The influence of orotracheal intubation on the oral tissue development in preterm infants. Oral Health Prev Dent. 2012;10(2):141–147.
- Seow WK. Effects of preterm birth on oral growth and development. Aust Dent J. 1997;42(2):85–91.
- Wuollet E, Laisi S, Salmela E, et al. Molar–incisor hypomineralization and the association with childhood illnesses and antibiotics in a group of finnish children. Acta Odontol Scand. 2016;74(5):416–422.
- Nelson S, Albert JM, Lombardi G, et al. Dental caries and enamel defects in very low birth weight adolescents. Caries Res. 2010;44(6):509–518.
- Kumar R, Thomas AM. Evaluation of dental caries in preterm born children with enamel defects. Dent J. 2017;19(3):1–5.
- Casey PH. Growth of low birth weight preterm children. Semin Perinatol. 2008;32(1):20–27.
- Seow WK, Young WG, Tsang AKL, et al. A study of primary dental enamel from preterm and full-term children using light and scanning electron microscopy. Pediatr Dent. 2005;27(5):374–379.
- Nirunsittirat A, Pitiphat W, McKinney CM, et al. Adverse birth outcomes and childhood caries: a cohort study. Community Dent Oral Epidemiol. 2016;44(3):239–247.
- Ramos SRP, Gugisch RC, Fraiz FC. The influence of gestational age and birth weight of the newborn on tooth eruption. J Appl Oral Sci. 2006;14(4):228–232.