
Abstract
Scaphoid and lunate mobility has been suggested to be minimal during the dart-throwing motion in studies based on serial computed tomography (CT) scans and cadaver studies. This study analyzes the direct motion between the scaphoid and the lunate during the dart-throwing motion in vivo. We examined nine individuals with standard CT scans of the wrist in radial extension and ulnar flexion. The paired CT scans were analyzed with a volume registration technique. The lunate was registered as fixed and the scaphoid as the mobile element. The motion of the scaphoid relative the lunate between the positions of radial extension and ulnar flexion was measured. There was considerable motion between the scaphoid and the lunate with both a distal to proximal translation and rotation during the dart-throwing motion, regardless of whether the scapholunate ligament was intact or not. These results suggest that aggressive dart-throwing exercises should not be implemented early on during rehabilitation following scapholunate repair.
Introduction
The dart-throwing motion is the most frequent wrist axis of movement during activities of daily living [Citation1]. Scaphoid and lunate motion has been suggested to be minimal during the dart-throwing motion in studies based on serial in vivo computed tomography (CT) and cadaver studies [Citation2–4]. For this reason, dart-throwing exercises have been proposed to be safe after repair of the scapholunate ligament. On the other hand, using dynamic four-dimensional computerized tomography (4 D-CT), Garcia-Elias et al. [Citation5] showed that the scaphoid moves considerably more than the lunate radially towards the radial styloid during the dart-throwing motion in patients with a torn scapholunate ligament, inducing a scapholunate gap.
Motion between carpal bones can be analyzed with volume registration technique of paired CT scans [Citation6]. In comparison to 4 D-CT, this technique requires only two regular CT scans, does not generate extensive data volumes and implies less radiation.
The aim of this study was to analyze the direct motion between the scaphoid and the lunate during the dart-throwing motion, i.e. from radial extension to ulnar flexion in wrists with no signs of scapholunate injury using a volume registration technique of paired CT scans.
Methods
Patients
Nine patients from a previous study [Citation6] that had been operated with a unilateral lunocapitate fusion and for the purpose of that study had a CT scan of the contralateral non-operated side, were included. The median age at surgery was 54 years (range: 28–62 years), and the patients were 8 men and 1 woman. None of the patients described any symptoms of pain in the non-operated wrist. Wrist range of motion had been measured with a goniometer ().
The study was approved by the Regional Ethical Review Board. All patients provided their written informed consent.
CT scans
CT scans were obtained with the wrist in two wrist positions: radial extension and ulnar flexion, i.e. opposing positions of the dart-throwing motion. In the CT scanner, the wrist was held in position with adjustable plastic splints that were adjusted for each patient to achieve the anticipated wrist position and to reduce motion artefacts.
The data volumes were acquired according to the protocol used for standard imaging of the wrist, i.e. a helical scan, 0.6 mm collimation, pitch 0.8, 1.0 revolutions/s at approximately 75 mA (dose regulation) and 120 kV. Slices were reconstructed at 1.0 mm thickness with 1.0-mm increment using a bone reconstruction algorithm in three planes (axial, coronal, sagital).
Motion analysis
The images were analyzed using a volume registration tool (CT-based Implant Micromotion Analysis (CTMA) by SectraTM, Linköping, Sweden). The scaphoid was registered as the moving object and the lunate as fixed. Three reference points on the scaphoid were defined manually, the center of mass (COM) of the scaphoid was computed by the software (). The motion of these points on the scaphoid in relation to the lunate was analyzed. The scaphoid reference points would shift position relative the lunate between the two scans only if motion had occurred between the two bones from radial extension to ulnar flexion. The motion of each of the four scaphoid reference points in relation to the lunate was tracked in six degrees of freedom (translation and rotation around and along three orthogonal cardinal axes) (). Motion was expressed as translation of the COM along the three axes and the total degree of rotation in space (). The total degree of rotation in space was calculated by computing the screw axis between the two wrist positions and the angle of rotation about the screw axis. The intra-observer reliability was evaluated by repeating the test. It was excellent; intraclass correlation coefficient was 0.999 (CI 0.999–1.000).
Figure 1. Bone volume registration technique analysis. The lunate is the fixed segment with green and yellow areas indicating no motion. Translation and total rotation in space of the scaphoid relative the lunate are measured in four points (COM: center of mass; SLP: scapholunate proximal; SLD: scapholunate distal; SDU: scapholunate distal-ulnar). The XYZ coordinate system is used to show translation and rotation axis orientation.
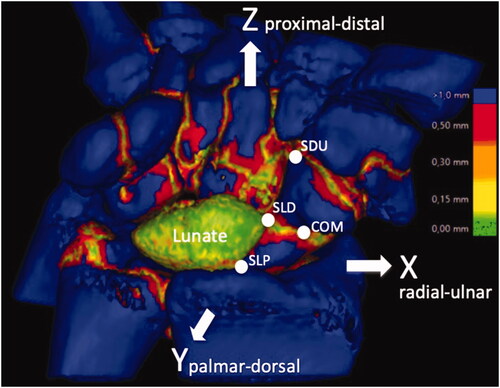
Table 2. Scaphoid motion relative the lunate.
Results
presents individual patient data. Seven patients had a radiologically intact scapholunate ligament (i.e. there was no widening of the scapholunate distance between radial extension and ulnar flexion). Two patients had a scapholunate advanced collapse (SLAC) with a static scapholunate dissociation. Six patients had a type 1 lunate, three patients a type 2.
Table 1. Individual patient data.
Considerable motion of the COM occurred between the scaphoid and the lunate in all patients. There were a distal to proximal translation as well as rotation between the bones during dart-throwing motion (). The SLAC wrists had a higher degree of rotation in space of the scaphoid relative the lunate compared to the patients with radiologically healthy wrists (). One patient had a congenital osseous coalition between the lunate and triquetrum. The degree of rotation in space of the scaphoid in this patient did not differ from the patients with radiologically intact scapholunate ligaments.
Discussion
Using volume registration technique of paired CT scans, we could demonstrate motion between the scaphoid and lunate during dart-throwing motion. There was a tendency of more pronounced scapholunate motion in wrists with scapholunate dissociation.
It had been postulated that exercises along the path of the dart-throwing motion after scapholunate injury repair might be safe. This is based on the assumption that scapholunate motion is minimal during dart-throwing motion according to studies on serial CT scans and cadavers [Citation1–4]. In contrast, we found that the scaphoid both rotated and translated relative the lunate during the dart-throwing motion even in patients with an intact scapholunate ligament. Garcia-Elias et al. [Citation5] demonstrated that in normal wrists, the scaphoid and lunate do not extend or flex but translate relative the radius along the frontal plane during dart-throwing motion. It was also shown that if the scapholunate ligament was torn, the scaphoid shifted towards the radial styloid considerably more than the lunate, inducing a scapholunate gap. Accordingly, we observed that in the two wrists with scapholunate dissociation, a higher degree of total motion in space of the scaphoid relative the lunate ().
We observed that the magnitude of motion between the scaphoid and lunate varied among patients with intact scapholunate ligaments (). Possible explanations could be the presence of dynamic scapholunate instability in some wrists or a varying degree of laxity of the carpal ligaments between patients, or both. Garcia-Elias et al. [Citation7] have shown that joint laxity affects the scaphoid motion during radioulnar deviation of the wrist. In lax joints, the scaphoid rotates along a sagittal axis of flexion-extension whereas in more stiff wrists the scaphoid rotates along the frontal plane of radioulnar deviation with minimal flexion-extension.
Beside the small sample size, a limitation of this study is the uncertainty as to whether there were anatomical variances between patients or scapholunate injuries that were not diagnosed by the clinical and radiological examination. Diagnostic arthroscopy of the examined wrists would have been of great value. Our results reflect the motion changes between the extremes of wrist motion. In a setting with smaller dart throw range of motion these changes might be less.
Volume registration of serial CT scans may have potential as a cheap and non-invasive tool to diagnose scapholunate injuries, reducing the need for diagnostic wrist arthroscopy. An implication for further research is to compare volume registration of paired CT scans with arthroscopy for scapholunate injury diagnostics.
We conclude that there is motion between the scaphoid and the lunate during the dart-throwing motion and consequently, during rehabilitation after scapholunate injury and reconstruction surgery, caution is recommended and if early mobilization is performed, maximal range of dart throw motion should be avoided.
Ethical statement
The study was approved by the local Ethics Committee of Stockholm (2017/26-31/4).
Written informed consent was obtained from all subjects before the study.
Author contributions
TS and MW researched literature and conceived the study, gained ethical approval and recruited patients. HO was involved in protocol development and data analysis. TS wrote the first draft of the manuscript and the revisions. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Disclosure statement
Dr Olivecrona is occasionally engaged by Sectra as an independent consultant for software development. The authors declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Funding
References
- Brigstocke GH, Hearnden A, Holt C, et al. In-vivo confirmation of the use of the dart thrower's motion during activities of daily living. J Hand Surg Eur Vol. 2014;39(4):373–378.
- Werner FW, Green JK, Short WH, et al. Scaphoid and lunate motion during a wrist dart throw motion. J Hand Surg Am. 2004;29(3):418–422.
- Crisco JJ, Coburn JC, Moore DC, Akelman E, et al. In vivo radiocarpal kinematics and the dart thrower's motion. J Bone Joint Surg Am. 2005; 87:2729–2740.
- Werner FW, Sutton LG, Basu N, et al. Scaphoid tuberosity excursion is minimized during a dart-throwing motion: a biomechanical study. J Hand Ther. 2016;29(2):175–182.
- Garcia-Elias M, Alomar Serrallach X, Monill Serra J. Dart-throwing motion in patients with scapholunate instability: a dynamic four-dimensional computed tomography study. J Hand Surg Eur Vol. 2014;39(4):346–352.
- Schriever TU, Olivecrona H, Wilcke MT. Triquetral motion is limited in vivo after lunocapitate fusion. J Hand Surg Global Online. 2020;2(1):42–45.
- Garcia-Elias M, Ribe M, Rodriguez J, et al. Influence of joint laxity on scaphoid kinematics. J Hand Surg Br. 1995;20(3):379–382.