
ABSTRACT
Background: Psychological resilience has grown in popularity as a topic of study in psychotraumatology research; however, this concept remains poorly understood and there are several competing theories of resilience.
Objective: This study sought to assess the support for one proposed theory of resilience: the flexibility sequence.
Method: This study use secondary data analysis of panel survey data (N = 563). Participants were aged 18 years or over and based in the UK. A series of sequential mediation models was used to test the flexibility sequence theory as a proposed pathway of resilience on mental health outcomes (post-traumatic stress disorder, anxiety, and depression) among a trauma-exposed sample from the UK.
Results: The ‘feedback’ component of the proposed flexibility sequence components was associated with reduced symptom severity with all outcomes, whereas ‘context sensitivity’ and ‘repertoire’ were significantly associated only with depression as an outcome. When indirect mediation pathways were modelled via the flexibility sequence, statistically significant effects were observed for all outcomes under investigation.
Conclusions: These findings support the theorized flexibility sequence pathway of resilience, suggesting that the combination of these skills/processes performs more favourably as a framework of resilience than any in isolation. Further research into more elaborate associations and feedback loops associated with this pathway is warranted.
HIGHLIGHTS
The components of the flexibility sequence were not uniformly associated with reduced psychopathology.
The path model of following the proposed flexibility sequence was associated with reduced psychopathology, and therefore is more than the sum of its parts in predicting resilience.
The flexibility sequence is a promising framework for understanding and promoting resilience in a trauma-exposed sample.
Antecedentes: La resiliencia psicológica ha ganado popularidad como tema de estudio en la investigación en psicotraumatología, sin embargo este concepto sigue siendo poco comprendido. Hay varias teorías de resiliencia que compiten entre sí, sin embargo este estudio buscó evaluar el apoyo para una teoría propuesta: la Secuencia de Flexibilidad.
Metodología: Este estudio utilizó análisis de datos secundarios de datos de encuestas de panel (N=563, los participantes tenían más de 18 años y residían en el Reino Unido). Se utilizaron una serie de modelos secuenciales para probar la teoría de Secuencia de Flexibilidad como una vía propuesta de Resiliencia en los resultados de salud mental (TEPT, Ansiedad y Depresión) entre una muestra del Reino Unido expuesta a traumas.
Resultados: Se encontró que el componente de Retroalimentación de los componentes de la Secuencia de Flexibilidad propuesta se asoció con una reducción de la gravedad de los síntomas en todos los resultados y la Sensibilidad al Contexto y Repertorio se asociaron significativamente solo con Depresión como resultado. Cuando las vías de mediación indirecta se modelaron a través de la Secuencia de Flexibilidad, se observaron efectos estadísticamente significativos para todos los resultados bajo investigación.
Discusión: Estos hallazgos respaldan el camino de Resiliencia teorizado de Secuencia de Flexibilidad, lo que sugiere que la combinación de estas habilidades/procesos funciona más favorablemente como una estructura de resiliencia que cualquiera de forma aislada. Se justifica una mayor investigación sobre asociaciones más elaboradas y circuitos de retroalimentación asociados con esta vía.
背景:心理韧性作为心理创伤学研究的一个主题越来越受欢迎,然而对这个概念的了解甚浅。有几种心理韧性竞争理论,但是本研究试图评估对一个推荐理论:灵活性序列的支持。
方法:本研究利用面板调查数据的二级数据分析(N=563,参与者年龄在 18 岁以上,居住在英国)。在一个来自英国的创伤暴露样本中,使用一系列顺序中介模型检验灵活性序列理论是否可作为心理健康结果(PTSD、焦虑和抑郁)到心理韧性的一条推荐途径。
结果:发现推荐的灵活性序列成分的反馈成分与所有结果的症状严重程度降低相关,背景敏感性和技能仅与作为结果的抑郁显著相关。通过灵活性序列作为间接中介路径建模后,观察到所有考查结果都有统计学显著效应。
讨论:这些发现支持心理韧性的理论化灵活性序列路径,表明这些技能/过程的组合作为心理韧性框架比任何孤立的框架都更有利。有必要进一步研究与该路径相关的更精细的关联和反馈循环。
PALABRAS CLAVE:
1. Introduction
Historically, research has focused on negative outcomes following trauma and adversity; in particular, research has focused on the development of maladaptive conditions post-trauma, including both mental and physical disorders (Southwick et al., Citation2014). For decades, psychological research has fallen into this ‘trauma trap’, suggesting that pathological outcomes, including post-traumatic stress disorder (PTSD), depression, and anxiety, are the most prevalent or most pertinent following traumatic stress. The burden of evidence highlights that this is not the case, with the majority of those exposed to potentially traumatizing events (PTEs) reporting an absence of mental ill-health conditions and relatively healthy functioning (Bonanno et al., Citation2011).
Contemporary literature has sought to better understand post-traumatic resilience, with several competing concepts of resilience having emerged, and thus no unanimous understanding of this process (Bonanno et al., Citation2011; Southwick et al., Citation2014). Despite the lack of a unified definition, it remains important to explore the processes underpinning resilience following adversity and trauma to promote more favourable post-trauma outcomes. This is particularly pertinent given that 70.4% of individuals worldwide report exposure to PTEs, with many individuals often reporting multiple PTEs across their lifetime (Kessler et al., Citation2017).
Unfortunately, the current understanding of post-traumatic resilience is muddied by ‘uncertain evidence’ and variable theories that are not well founded and tested (Mahdiani & Ungar, Citation2021). Indeed, there have been several transient conceptualizations of resilience presented beyond those ‘resistance’ and ‘bounce-back’ themes, adding more elaborate considerations of the processes and precursors to resilience and adaptation following trauma (Mahdiani & Ungar, Citation2021). These competing and disparate concepts of resilience often yield studies that produce small effects which, in turn, fail to qualify post-traumatic resilience in its full complexity. Bonanno (Citation2021b) discussed ‘making peace with small effects’ in post-traumatic resilience research, noting that these are common in psychological research and may be expected. Key to this rationale is the idea that resilience, like many other psychological concepts, is a complex and transient phenomenon which, by its very nature, is hard to qualify and, in turn, quantify. In addition, because resilience following potential trauma is typically the most prevalent outcome (Galatzer-Levy et al., Citation2018), membership in this group is likely to have multiple determinants.
Given the need to better understand resilience outcomes following exposure to traumatic stress, the current study seeks to test a model of psychological resilience among those with a history of trauma exposure, based on a contemporary model with theoretical grounding, combining several aspects of resilience’s estimated ‘small effects’. More specifically, we aim to test the flexibility sequence theory (Bonanno, Citation2021b; Bonanno & Burton, Citation2013). This theory rejects the concept of resilience as a trait and, instead, views resilience as an ever-changing, adaptive process. The driving mechanism of that process is flexible responding, more specifically the flexibility sequence, where individuals determine which strategies might best apply to a specific aversive circumstance, and then monitor and modify strategy use as needed in order to overcome and thrive. The flexibility sequence was postulated to unfold in three sequential components: (1) context sensitivity, (2) repertoire, and (3) feedback.
Context sensitivity is defined as the ability to perceive contextual cues that indicate the demands of a situation. Doing so permits an individual to then employ an appropriate and probably effective coping or regulation strategy (Bonanno et al., Citation2020). This initial appraisal of external cues and threats is the interface by which stressors interact with and influence the individual (Lazarus, Citation1966). However, as the outcomes for regulatory strategies have been found to vary widely, it is apparent that some flexible approach, i.e. identifying contextual cues of what to do and in what situation, is necessary to be resilient (Aldao et al., Citation2015). In the face of post-traumatic stress, accurate perception of contextual cues becomes even more vital to initiate and guide subsequent processes that might mitigate that stress (Bonanno et al., Citation2020).
Repertoire may be understood as an individual’s bank of regulation strategies that they can utilize to cope with stressful stimuli (Bonanno & Burton, Citation2013). In many cases, it is considered preferable to have access to a larger number of strategies; however, the diversity of these strategies may be as important as their number (Bonanno & Burton, Citation2013). Indeed, possessing a greater number of coping strategies has been associated with psychopathological outcomes regardless of how often each is actually implemented (Heffer & Willoughby, Citation2017). This is not unambiguously observed, however, as meta-analytical evidence has shown that a broader repertoire of coping strategies has only a modest effect on global resilience. Therefore, consistent with the flexibility sequence concept, the greatest importance should be placed on identifying strategies that are effective in situ (Cheng et al., Citation2014).
Feedback monitoring speaks to a skill which involves the evaluation of the regulation strategy, and a decision as to whether to maintain or adjust this based on its effectiveness in that particular context (Bonanno & Burton, Citation2013). Feedback is central to flexible adaptation, as during this stage individuals are engaging in self-evaluation and regulation to cope more effectively, ultimately improving the chance of post-traumatic resilience (Aldao et al., Citation2015; Cheng et al., Citation2014). Previous evidence has supported this idea, showing that greater evaluation and adaptation skills related to coping strategies are significantly associated with a reduced risk of depressive symptomology (Kato, Citation2012, Citation2015).
The flexibility sequence presents a novel unified theory of resilience that links concepts in a proposed process. Indeed, when individuals can proficiently assess their present situation, identify a coping strategy, and review or adjust these strategies until an effective strategy is employed, it is hypothesized that they will show greater probability of resilience after adversity (Bonanno, Citation2021b; Bonanno & Burton, Citation2013). Although a previous study has shown that a majority of individuals have at least moderate proficiency in all three components (Chen & Bonanno, Citation2021), no research has yet examined their interface. To address this deficit, in the current study we aimed to examine the proposed pathways between context sensitivity, repertoire, and feedback using sequential mediation modelling. The value of this type of analysis lies in evaluating the viability of this proposed causal/temporal pathway or sequence as a theory-driven model of post-traumatic psychological resilience. Likewise, this approach adopts a variable-centred approach complementing other emerging evidence adopting person-centred approaches (Chen & Bonanno, Citation2021).
The current study considered the relative absence of psychopathological symptoms, specifically PTSD, anxiety, and depression symptoms, as the endpoint of resilience, and the flexibility sequence as the process that leads to this. Emergent evidence has been supportive of this theory, suggesting that people adhering to this concept of being flexible regulators are less likely to experience such psychopathological symptoms (Chen & Bonanno, Citation2021). We therefore adopted a hypothesis-testing approach grounded in the flexibility sequence theory, asserting that (1) each component of the sequence would be associated with a significant reduction in psychopathological symptomology (PTSD, depression, and anxiety), and (2) the sequential variable model in accordance with this theory would be associated with significantly reduced PTSD, depression, and anxiety symptomology.
2. Methodology
2.1. Data and procedure
This study analysed data collected from an online panel survey of Prolific users. Survey questions were administered using Qualtrics survey software. Ethical approval for this study was sought and obtained from the Queen’s University Belfast Engineering and Physical Sciences Faculty Research Ethics Committee (approval ref.: EPS 21_292). Informed consent was obtained from all participants prior to survey administration.
All participants identified through the Prolific panel were resident in the UK and proficient in English, leading to n > 59,000 potential respondents being identified. Because of resource constraints, the first n = 1,000 respondents were screened for lifetime experience of potential traumatic life events and compensated for this (effective survey rate £0.13). Those who endorsed one or more potentially traumatic life events were invited to respond to the main survey. Of those participants screened initially, n = 715 met the eligibility criteria and were invited to take part in this study. Of those invited, n = 152 (21.3%) did not respond to the invitation, yielding a final effective sample size of n = 563. All respondents to the main survey were compensated at a rate of £1.88 each.
Within this final dataset, there was 1.2% item-level missingness. These data were not missing at random, as responses to survey items were required to progress; thus, where participants declined to respond to any item the following variable responses were necessarily missing. Imputation methods were therefore not appropriate and complete case analysis was used across analyses, maximizing the utility of collected data. This procedure has been shown to be an acceptable approach and not to bias the results of analyses in cases with low levels of missingness (Allison, Citation2001).
2.2. Measures
Trauma exposure was measured using the Life Events Checklist for DSM-5 (LEC-5) (Weathers, Blake, et al., Citation2013). This scale asked participants for dichotomous (Yes/No) responses to 16 recognized potentially traumatic life events qualifying for PTSD diagnosis under Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) guidelines (APA, Citation2013). The LEC-5 has demonstrated excellent psychometric properties and robust association with PTSD and psychological distress (Gray et al., Citation2004).
PTSD was assessed using the PTSD Checklist for DSM-5 (PCL-5) (Weathers, Litz, et al., Citation2013). The PCL-5 is a 20-item measure of PTSD symptomology where participants rate the degree to which they have been distressed by symptoms, from 0 ‘Not at all’ to 4 ‘Extremely’; thus, total scores range from 0 to 80. Higher scores on this scale are indicative of greater PTSD symptomology, with a score of 33 determining a robust indicator of potential PTSD caseness, i.e. probable diagnosis (Bovin et al., Citation2016). This scale demonstrated excellent internal reliability in the current study (α = .949).
Generalized anxiety disorder (GAD) was assessed using the Generalized Anxiety Disorder 7-item questionnaire (GAD-7) (Spitzer et al., Citation2006). Major depressive disorder (MDD) was assessed using the 9-item Patient Health Questionnaire (PHQ-9) (Kroenke et al., Citation2001). Both scales ask participants to rate the extent to which they have experienced anxiety and depression symptoms in the previous 2 weeks, on a scale from 0 to 3 (0 ‘Not at all’, 1 ‘Several days’, 2 ‘More than half the days’, 3 ‘Nearly every day’). A cut-off score of 10 for each measure is considered to provide an adequate sensitivity and specificity to screen for caseness of GAD and MDD (Kroenke et al., Citation2001; Spitzer et al., Citation2006). Both scales demonstrated good internal reliability in the current study: GAD-7 (α = .915) and PHQ-9 (α = .881).
The flexibility sequence was measured using the same scales outlined in the study by Chen and Bonanno (Citation2021).
Context sensitivity was measured by the Context Sensitivity Index (CSI) (Bonanno et al., Citation2020). The CSI presents six vignettes (e.g. ‘You are walking alone down a street when you see a person slip and fall. They hit their head when they land’),each with a series of items assessing respondent appraisals of the perceived control, urgency, potential co-operation, and threat in the scenario presented. Each response is recorded on a scale from 1 ‘Not at All’ to 7 ‘Very Much’. This study applied the same procedure as Chen and Bonanno (Citation2021), using a sum of the ‘cue absence’ items reverse scores and ‘cue presence’ items; thus, higher scores were considered indicative of greater context sensitivity. Internal consistency was not computed for the CSI as the items in this scale are causal indicators rather than effect indicators (Bonanno et al., Citation2020).
Repertoire was measured by the Flexible Regulation of Emotional Expression (FREE) scale (Burton & Bonanno, Citation2016). The FREE scale presents 16 scenarios, to which respondents are asked to rate their perceived ability to cope with adversity by employing strategies enhancing or suppressing affective responses, on a scale from 1 ‘Not at all’ to 6 ‘Very Much’. The summed score of this scale was used as a measure representing the repertoire construct. Good internal reliability was demonstrated in the current sample (α = .790).
Feedback was measured by the Coping Flexibility Scale – Revised (CFS-R) (Kato, Citation2012). The CFS-R is a 12-item measure of perceived ability to evaluate and adapt coping strategies in response to external cues. Each item is rated in relation to how much each statement applies to the respondent, on a scale from 0 ‘Not at all’ to 3 ‘Very applicable’. The sum of responses was used to represent the ‘feedback’ construct, with higher scores reflecting heightened feedback. Excellent reliability was demonstrated for the summative CFS-R scale in the current sample (α = .904).
2.3. Data analytic plan
The primary goal of these analyses was to test Bonanno’s (Citation2021a, Citation2021b) proposal that the flexibility sequence is the underlying mechanism leading to resilient outcomes among trauma-exposed adults. To do this, a series of mediation path models was specified estimating the direct and indirect effects between the concepts of this theory (context sensitivity, repertoire, and feedback) and scores on self-report measures of PTSD, anxiety, and depression symptomology. This technique is used to examine the role of intervening or causal variables in a relationship (Hayes, Citation2009). In its simplest terms, mediation path modelling involves estimating direct and indirect influences of an independent variable on an outcome via mediating variable(s). Sequential mediation adds to this analysis by examining the indirect effect of a variable on some outcome via two or more mediating variables (Tofighi & Kelley, Citation2020); more specially, a temporal or causal chain is proposed by which variables influence each other. practically, this means that simple mediation models estimate indirect effects through one variable (predictor to mediator to outcome) and sequential mediation models estimate effects through the additive effect of two intermediary variables (predictor to mediator 1 to mediator 2 to outcome) (Tofighi & Kelley, Citation2020).
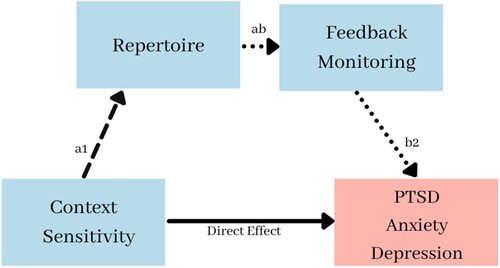
In the current study, context sensitivity was considered the independent variable and a series of sequential mediation models was used to evaluate the indirect pathways between this and the mental health outcomes under investigation. These specified models used the flexibility sequence (Bonanno, Citation2021a) as a framework, specifying a theory-informed sequential pathway of these variables. These mediation models are illustrated graphically in . While, historically, approaches to mediation such as the causal steps approach (Baron & Kenny, Citation1986) require that a significant direct relationship be observed prior to testing mediation, this approach has been widely criticized and contemporary researchers argue that it is valuable to estimate model indirect effects testing mediation even in the absence of significant associations (Hayes, Citation2009). Direct pathways were estimated for each variable within the mediation model, along with the theorized indirect pathways.
Figure 1. Post-traumatic stress disorder (PTSD), depression, and anxiety sequential mediation model diagram.
Primary analyses controlled for age, gender, ethnicity, educational attainment, relationship status, and employment status, as these demographic variables have been shown to influence the risk of adverse mental health outcomes (WHO, Citation2014). Each outcome was modelled as a continuous variable representing the sum score of each of the screening measures used.
All analyses were performed using Jamovi statistical software (Gallucci, Citation2020; Jamovi Project, Citation2021). Mediation models for each outcome were estimated using bias-corrected bootstrapping with 1000 iterations. Model fit for direct and indirect models was compared using adjusted R-squared values, which provide a robust indicator of a model’s improved ability to predict outcomes while penalising for the addition of predictor variables (Fairchild et al., Citation2009).
3. Results
3.1. Descriptive statistics
The majority of respondents identified as female (n = 453, 80.5%), were of white ethnicity (n = 518, 92.0%), married or living with a partner (n = 325, 57.7%), had attained a bachelor’s degree (n = 190, 33.7%), and were employed (n = 416, 73.9%). Full information on the demographics of this sample may be found in .
Table 1. Participant demographic information.
The total number of potentially traumatic life events experienced in this sample ranged from 1 to 12. On average, participants reported experiencing 3.29 lifetime potentially traumatic experiences (SD = 2.03). Across all endorsements, ‘transportation accident’ was the most frequently reported (n = 309, 54.9%). This was followed by ‘other unwanted sexual experience’ (n = 279, 49.6%) and ‘physical assault’ (n = 273, 48.5%). When asked to rate which of their experiences was the most distressing, the most frequently endorsed experience was ‘sexual assault’ (n = 122, 21.7%), followed by ‘witnessing a fire or explosion’ (n = 96, 17.1%) and ‘physical assault’ (n = 72, 12.8%). Total and most distressing trauma endorsements are detailed for the full study sample in .
Table 2. Participant endorsements of any and most distressing life events.
With regard to the mental health outcomes under investigation, the most common probable diagnosis was MDD, with 42.4% of the study sample (range = 0–27, M = 9.26, SD = 6.02) meeting the criteria. This was followed by PTSD, with 34.5% of the sample meeting the criteria for probable diagnosis (range = 0–80, M = 27.20, SD = 17.80), and finally GAD, with 32.7% of the sample qualifying caseness for this disorder (range = 0–21, M = 7.62, SD = 5.46). While these rates may be considered high, it should be noted that this is a trauma-exposed sample (for more on this issue, see Section 4.1).
3.2. Primary analyses
3.2.1. PTSD
When direct effects of the proposed flexibility sequence components were estimated, only feedback had a significant relationship with PTSD (β = −0.251, p < .001), and, as expected, was associated with reduced symptom severity. While the direct relationship between context sensitivity and PTSD was found to be non-significant (p = .559), the indirect model was estimated in line with suggested practices for mediation analysis (Hayes, Citation2009).
There was a significant improvement in model fit observed for the indirect sequential mediator model relative to the direct model (adjusted R2 = .10, ΔR2 = .06, F2,550 = 18.9, p < .001). Of the indirect models tested, only the full sequential mediation model (context sensitivity to repertoire to feedback monitoring to mental health outcomes) was found to have a statistically significant effect on PTSD symptom severity (β = −0.200, p < .001), and explained 11% of the variance in this outcome.
Full results for the direct and indirect models for PTSD may be found in .
Table 3. Mediation model results.
3.2.2. Depression
The direct association between context sensitivity and depression symptomology was found to be marginally significant (p = 0.51). The indirect model was once again estimated in line with best practices in contemporary mediation analysis (Hayes, Citation2009).
The indirect model via feedback (β = −0.030, p < .05) and the full sequential mediator model (β = −0.001, p < .05) were found to be significantly associated with reduced depression symptomology. Again, a significant improvement was found for the sequential mediator model relative to the direct model (adjusted R2 = .11, ΔR2 = .10, F2,537 = 33.5, p < .001). The full mediation model was found to explain 20% of the outcome variance.
Full results for the direct and indirect models for depression may be found in .
3.2.1. Anxiety
The direct association between context sensitivity and anxiety symptomology was found to be statistically significant (β = −0.010, p < .05), as was the association with feedback (β = −0.127, p < .001). In both instances, these direct relationships were in the expected direction, being associated with reduced anxiety symptomology.
As with depression, the indirect model via feedback (β = −0.026, p < .05), and the full sequential mediator model (β = −0.001, p < .001) were found to be significantly associated with reduced anxiety symptomology. Once again, a significant improvement was found for the sequential mediator model relative to the direct model (adjusted R2 = .17, ΔR2 = .07, F2,537 = 22.6, p < .001), with the indirect model explaining 18% of outcome variance.
Full results for the direct and indirect models for anxiety may be found in .
4. Discussion
This study aimed to validate the theorized flexibility sequence underlying resilience in a trauma-exposed sample by applying sequential mediation path modelling to the hypothesized conceptual chain within this theory. Statistically significant pathways were identified for this model for each mental health outcome under investigation; greater context sensitivity was associated with reduced mental health symptomology via repertoire and feedback skills. These findings suggest that the flexibility sequence presents a viable conceptualization of psychological resilience in a trauma-exposed community sample. The supported model illustrates that the proposed sequence of context identification, regulatory strategy repertoire, and review of its effectiveness is a viable way of understanding psychological resilience.
While the overall study results were found to support the proposed flexibility sequence, the first hypothesis that the intrinsic components of the flexibility sequence would be associated with reduced psychopathology was not supported. In historic causal steps approaches to mediation analysis, researchers might be discouraged from further interrogating such a relationship; however, this negates the possibility that important intermediary variables exist in this relationship (Hayes, Citation2009). Failure to examine potential mediating relationships under such conditions may lead to researchers’ failure to uncover interesting and valuable mechanisms, particularly where a theory-informed explanation is to be explored (Fairchild & McDaniel, Citation2017; Hayes, Citation2009). Likewise, the individual components of the flexibility sequence are not considered salient indicators of resilience; rather, the sum of their effect is (Bonanno, Citation2021a).
Following these principles, when the indirect models were estimated for each outcome, the study hypothesis that the flexibility sequence would be associated with reduced symptom severity was supported. The association between these skills may therefore be understood as the mechanism underlying resilient outcomes, as individuals apply these in sequence to identify and mitigate stressors. This finding supports the theoretical assertion that the flexibility sequence is more than the sum of its parts, as no one constituent skill was associated with resilient outcomes, but their additive effect yielded statistically significant results. This may be useful to practically understand how an individual may successfully adapt to adversity, identifying potential strengths and weaknesses in this process as targets for intervention.
Bonanno (Citation2021b) suggested that owing to the disparate nature of studies attempting to identify resilience factors, researchers must make peace with the often small effects arising from research criticized for limited concept and measurement of resilience factors. Indeed, this assertion partly informed the conceptualization of the flexibility sequence as a more elaborate understanding of individual reactions to trauma and adversity, combining several constructs previously evidenced to be associated with well-being and resilience. The approach of the current study, using path analysis to assess the additive effects of multiple influencing factors, may therefore be a valuable approach to mitigating the issues of small effects and understanding the wider processes underpinning psychological resilience.
The support of the flexibility sequence offered through this method of analysis should be considered in relation to the variable structure of this theory. These results support the sequence of flexible regulation proposed by Bonanno and Burton (Citation2013) predicting psychopathological outcomes; therefore, this theory should be considered a framework for understanding the processes by which individuals may exhibit resilience. This sequence of appraisal, strategy repertoire, and evaluation may therefore be used in the development of training and interventions, with a view to promoting psychological resilience in groups exposed to traumatic stress.
It has been argued that ill-defined and ill-applied processes of resilience may include negative and maladaptive practices (Mahdiani & Ungar, Citation2021). For instance, in response to traumatic life events, individuals may employ emotional suppression strategies (repertoire) and, finding this approach effective (feedback), go on to apply it in situations more generally (context sensitivity), thus becoming callous and distant in more contexts. In this example, an individual might be said to have exhibited resilience through the flexibility sequence and adapted to future stressors; however, they may also be considered to have incorporated antisocial tendencies in their behaviour. It is therefore important that a continuum of resilience be understood. It is extremely unlikely that a ‘one size fits all’ approach to post-traumatic resilience will ever have full applicability. Indeed, the feedback stage of the flexibility sequence, by its very nature, is about the ability to ‘adapt and flex’ in a particular context.
These results speak to the adaptation of flexibility sequence skills among those with a history of trauma exposure. This should not be confused with a causative link from potentially traumatic stress to mental ill-health; rather, these results illustrate the development of resilience using the flexibility sequence framework in this at-risk group.
The current study’s conceptualization of resilience as the relative absence of psychopathology should be acknowledged. It would be worthwhile in future studies to examine positive outcomes, such as positive emotion, satisfying relationships, and meaning in life or, beyond that, post-traumatic growth, where individuals may fare even better than they had prior to the experience of traumatic stress (Westphal & Bonanno, Citation2007). In the context of the current findings, flexible coping may be a growth concept as individuals develop adaptive traits in response to potentially traumatic experiences that benefit them in exposure to future adversity. The lack of a unified understanding of resilience and growth following trauma contributes to the disparate evidence around these concepts. Indeed, review evidence has suggested that, despite their conceptual similarity, the growth and resilience research areas fail to capitalize on each other’s strengths (Infurna & Jayawickreme, Citation2019). Future research codifying the flexibility sequence theory should seek to integrate perspectives of post-traumatic growth as well as resilience dynamics.
These findings specifically support the pathway to resilient coping, but point to the clinical utility of the flexibility sequence as a framework in the alleviation of psychopathology in both therapeutic assessment and intervention. For example, clinicians may consider using this as a framework for evaluating aspects of resilience and coping. Likewise, clinicians may consider the use of the flexibility sequence as a means by which they can train resilience behaviours (Bonanno, Citation2021a). Indeed, existing therapeutic treatments, such as dialectical behaviour therapy, include clients recognizing emotions and coping strategy effectiveness as a route to resilience and recovery.
While this study sought to assess the flexibility sequence as a pathway to resilience, it should be noted that this theory posits that an individual may engage in a cycle of assessment, regulation, and revision in response to adversity (Bonanno & Burton, Citation2013). This study presents a snapshot of this process, assessing the relationship of a single sequence of these steps. Future research may consider more granular assessment of the strategies and feedback loops present in the flexibility sequence, and how these may influence individual traits and behaviour in the longer term. One potential approach to understanding this may be the application of network analysis, which models complex relationships both cross-sectionally and longitudinally, allowing for a granular examination of psychological items and the capture of between- and within-variable (e.g. feedback loops) associations (Fried, Citation2017).
It would likewise be pertinent to examine the effects of different types and contexts of traumatic stress on the development of flexibility sequence skills. It may be useful to understand whether exposure to interpersonal traumatic stressors contributes differently to context-sensitivity development (the identification and appraisal of stressors) compared to non-interpersonal stressors. To best understand this, future research could employ prospective and longitudinal measurement to examine individual evaluations of trauma experiences and skills development trajectories following different trauma types. For instance, methodological innovations that capture real-time data [ecological momentary assessment (EMA)] may prove useful in capturing more granular detail on trauma typology, appraisals, and time-series nuances that represent the flexibility sequence and development of its underpinning skills in response to adversities, as and when they occur.
4.1. Limitations
These results should be considered in light of some notable limitations. First, self-report screening measurement of mental health outcomes was used for study outcomes. This method has been suggested to overestimate prevalence rates (Charlson et al., Citation2019); however, validated measures have been demonstrated to have moderate concordance with clinician diagnostic interviews (Roberts et al., Citation2021; Stuart et al., Citation2014). Nonetheless, while this survey was administered with a non-clinical sample, it may be the case that ratings of mental ill-health are inflated by this method of administration.
Secondly, the demographics of the study sample may not be considered representative of the population at large. For instance, this sample being mostly female, white, educated, and employed may limit the generalizability of these results to wider groups. It is therefore recommended that analyses be repeated with diverse clinical and general populations. It is pertinent to emphasize, however, that representativeness is less of a concern when investigating mechanisms across psychological constructs compared to studies which focus on prevalence and associated outcomes.
These results may also have been limited by the use of non-specific measurement of the flexibility sequence components. The FREE scale and CFS were not developed to directly assess these concepts; however, they have been recognized as viable measures for these constructs (Chen & Bonanno, Citation2021). Although precedent is established using these scales as measures of flexibility sequence constructs, future research could consider the use of purpose-built measurement to best capture these constructs.
Likewise, the trauma events endorsed by participants may not be specifically linked to the current flexibility sequence skills expression. The statistical models used in the current study assess the sequential relationship between the components of the sequence linked to the vignette scenarios presented in the CSI. These results should therefore be interpreted as support for the application of these skills in a sample exposed to traumatic stress, rather than specifically related to the trauma event(s) experiences. These results would be strengthened by future analyses assessing the use of repertoire and feedback monitoring skills in relation to real stressors.
The cross-sectional design and limited detail of traumatic exposure in this study mean that time since trauma exposure and temporal causality may not be definitively established for the constructs in primary analyses. The outcomes in this study should therefore be considered to be associated with the trauma exposure in the sample; however, the effects of traumatic stress on flexibility sequence skills development are not fully realized. The mediation models specified were, however, grounded using an a priori theoretical framework, and thus suggest the validity of this theorized pathway in the current study sample. Where constructs occur near-instantly and are implicative of ordering by their definition, mediational pathways may be valuable using cross-sectional data (Fairchild & McDaniel, Citation2017). Nonetheless, these results should be interpreted with caution and considered in light of the hypothesis-testing context in which they were formulated.
Future research may strengthen these findings by applying repeated, longitudinal, or real-time measurement of individual coping processes, such as EMAs (Shiffman et al., Citation2008) and time-series network analyses (Fried, Citation2017). Such measurement would allow for better understanding of the causal chain of the flexibility sequence, directly linking this to experiences of adversity and how this may be exhibited in different contexts. Likewise, future studies of the flexibility sequence focusing on post-traumatic resilience may benefit from taking a more nuanced look at trauma. For example, asking questions such as whether time since trauma exposure, or type of potentially traumatic event experienced, results in changes to the underlying mechanisms of the flexibility sequence.
4.2. Conclusions
These results suggest that psychological resilience is more than the sum of its parts. The findings support the specified pathway of the flexibility sequence theory; that resilience is better understood as an adaptive process consisting of multiple functional parts rather than any single element. Further examination of latent and path models might be used to understand psychological resilience, as a flexible concept is warranted to better understand how individuals navigate this pathway.
Data availability
Data are not made publicly available as consent for this was not sought from participants during initial data collection. The data that support the findings of this study are available from the corresponding author, C. A., upon reasonable request.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Aldao, A., Sheppes, G., & Gross, J. J. (2015). Emotion regulation flexibility. Cognitive Therapy and Research, 39(3), 263–278. https://doi.org/10.1007/s10608-014-9662-4
- Allison, P. D. (2001). Missing Data. Sage Publications.
- APA. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th ed.). American Psychiatric Association.
- Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
- Bonanno, G. A. (2021a). The End of Trauma: How the New Science of Resilience is Changing How We Think About PTSD (1st ed.). Basic Books.
- Bonanno, G. A. (2021b). The resilience paradox. European Journal of Psychotraumatology, 12(1), 1942642. https://doi.org/10.1080/20008198.2021.1942642
- Bonanno, G. A., & Burton, C. L. (2013). Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspectives on Psychological Science, 8(6), 591–612. https://doi.org/10.1177/1745691613504116
- Bonanno, G. A., Maccallum, F., Malgaroli, M., & Hou, W. K. (2020). The context sensitivity index (CSI): Measuring the ability to identify the presence and absence of stressor context cues. Assessment, 27(2), 261–273. https://doi.org/10.1177/1073191118820131
- Bonanno, G. A., Westphal, M., & Mancini, A. D. (2011). Resilience to loss and potential trauma. Annual Review of Clinical Psychology, 7(1), 511–535. https://doi.org/10.1146/annurev-clinpsy-032210-104526
- Bovin, M. J., Marx, B. P., Weathers, F. W., Gallagher, M. W., Rodriguez, P., Schnurr, P. P., & Keane, T. M. (2016). Psychometric properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-fifth edition (PCL-5) in veterans. Psychological Assessment, 28(11), 1379–1391. https://doi.org/10.1037/pas0000254
- Burton, C. L., & Bonanno, G. A. (2016). Measuring ability to enhance and suppress emotional expression: The Flexible Regulation of Emotional Expression (FREE) scale. Psychological Assessment, 28(8), 929–941. https://doi.org/10.1037/pas0000231
- Charlson, F., van Ommeren, M., Flaxman, A., Cornett, J., Whiteford, H., & Saxena, S. (2019). New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. The Lancet, 394(10194), 240–248. https://doi.org/10.1016/s0140-6736(19)30934-1
- Chen, S., & Bonanno, G. A. (2021). Components of emotion regulation flexibility: Linking latent profiles to depressive and anxious symptoms. Clinical Psychological Science, 9(2), 236–251. https://doi.org/10.1177/2167702620956972
- Cheng, C., Lau, H. P., & Chan, M. P. (2014). Coping flexibility and psychological adjustment to stressful life changes: A meta-analytic review. Psychological Bulletin, 140(6), 1582–1607. https://doi.org/10.1037/a0037913
- Fairchild, A. J., Mackinnon, D. P., Taborga, M. P., & Taylor, A. B. (2009). R2 effect-size measures for mediation analysis. Behavior Research Methods, 41(2), 486–498. https://doi.org/10.3758/BRM.41.2.486
- Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
- Fried, E. I. (2017). What are psychological constructs? On the nature and statistical modelling of emotions, intelligence, personality traits and mental disorders. Health Psychology Review, 11(2), 130–134. https://doi.org/10.1080/17437199.2017.1306718
- Galatzer-Levy, I. R., Huang, S. H., & Bonanno, G. A. (2018). Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clinical Psychology Review, 63, 41–55. https://doi.org/10.1016/j.cpr.2018.05.008
- Gallucci, M. (2020). jAMM: Jamovi advanced mediation models. https://jamovi-amm.github.io/
- Gray, M. J., Litz, B. T., Hsu, J. L., & Lombardo, T. W. (2004). Psychometric properties of the life events checklist. Assessment, 11(4), 330–341. https://doi.org/10.1177/1073191104269954
- Hayes, A. F. (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76(4), 408–420. https://doi.org/10.1080/03637750903310360
- Heffer, T., & Willoughby, T. (2017). A count of coping strategies: A longitudinal study investigating an alternative method to understanding coping and adjustment. PLoS One, 12(10), e0186057. https://doi.org/10.1371/journal.pone.0186057
- Infurna, F. J., & Jayawickreme, E. (2019). Fixing the growth illusion: New directions for research in resilience and posttraumatic growth. Current Directions in Psychological Science, 28(2), 152–158. https://doi.org/10.1177/0963721419827017
- Jamovi Project. (2021). Jamovi. Version 1.6. www.jamovi.org
- Kato, T. (2012). Development of the coping flexibility scale: Evidence for the coping flexibility hypothesis. Journal of Counseling Psychology, 59(2), 262–273. https://doi.org/10.1037/a0027770
- Kato, T. (2015). The impact of coping flexibility on the risk of depressive symptoms. PLoS One, 10(5), e0128307. https://doi.org/10.1371/journal.pone.0128307
- Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., Degenhardt, L., de Girolamo, G., Dinolova, R. V., Ferry, F., Florescu, S., Gureje, O., Haro, J. M., Huang, Y., Karam, E. G., Kawakami, N., Lee, S., Lepine, J. P., Levinson, D., … Koenen, K. C. (2017). Trauma and PTSD in the WHO World Mental Health Surveys. European Journal of Psychotraumatology, 8(sup5), 1353383. https://doi.org/10.1080/20008198.2017.1353383
- Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
- Lazarus, R. S. (1966). Psychological Stress and the Coping Process. McGraw-Hill.
- Mahdiani, H., & Ungar, M. (2021). The dark side of resilience. Adversity and Resilience Science, 2(3), 147–155. https://doi.org/10.1007/s42844-021-00031-z
- Roberts, N. P., Kitchiner, N. J., Lewis, C. E., Downes, A. J., & Bisson, J. I. (2021). Psychometric properties of the PTSD checklist for DSM-5 in a sample of trauma exposed mental health service users. European Journal of Psychotraumatology, 12(1), 1863578. https://doi.org/10.1080/20008198.2020.1863578
- Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4(1), 1–32. https://doi.org/10.1146/annurev.clinpsy.3.022806.091415
- Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5(1), 25338. https://doi.org/10.3402/ejpt.v5.25338
- Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
- Stuart, A. L., Pasco, J. A., Jacka, F. N., Brennan, S. L., Berk, M., & Williams, L. J. (2014). Comparison of self-report and structured clinical interview in the identification of depression. Comprehensive Psychiatry, 55(4), 866–869. https://doi.org/10.1016/j.comppsych.2013.12.019
- Tofighi, D., & Kelley, K. (2020). Indirect effects in sequential mediation models: Evaluating methods for hypothesis testing and confidence interval formation. Multivariate Behavioral Research, 55(2), 188–210. https://doi.org/10.1080/00273171.2019.1618545
- Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., & Keane, T. M. (2013). The Life Events Checklist for DSM-5 (LEC-5). Instrument available from the National Center for PTSD. www.ptsd.va.gov
- Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD Checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD. www.ptsd.va.gov
- Westphal, M., & Bonanno, G. A. (2007). Posttraumatic growth and resilience to trauma: Different sides of the same coin or different coins? Applied Psychology, 56(3), 417–427. https://doi.org/10.1111/j.1464-0597.2007.00298.x
- WHO. (2014). Social Determinants of Mental Health. World Health Organization.