
ABSTRACT
Background: The International Trauma Questionnaire (ITQ) is a self-report assessment focused on the core features of Post-Traumatic Stress Disorder (PTSD) and complex Post-Traumatic Stress Disorder (CPTSD). It is consistent with the organizing principles of the 11th revision to the WHO's International Classification of Diseases (ICD-11). Since the 1990s, the number of North Korean defectors (NKD) entering South Korea to escape human rights violations has been increasing rapidly, with 33,815 NKD settled by 2021. The South Korean government faces an important challenge in supporting NKD to successfully adapt and settle in South Korean society. NKD experience various traumatic events during the process of defecting and repatriation. Therefore, it is essential to understand the psychological disorders of NKD, especially PTSD and CPTSD.
Objective: This study aimed to test the validity of the ITQ assessment and explore the differences in symptoms and quality of life between PTSD and CPTSD.
Method: The study sample comprised 503 trauma-exposed NKD. Confirmatory factor analysis (CFA) and latent class analysis (LCA) were used to evaluate the validity of ITQ. One-way analysis of variances and post-hoc analyses revealed the difference in the Depression and Somatic Symptoms Scale (DSSS) and WHOQOL-BREF results among PTSD and CPTSD symptom LCA classes.
Results: The CFA and LCA results supported the ICD-11 conceptualization of PTSD and CPTSD in NKD. The CFA results confirmed that both the first- and second-order models were statistically fit, but for community-dwelling NKD the first-order model had better model fit than the second-order model. The LCA findings revealed a four-class model with ‘PTSD’, ‘CPTSD’, ‘DSO’, and ‘low symptom’ classes. Compared to the PTSD class, CPTSD class had higher levels of depression and somatic symptoms and a lower quality of life.
Conclusion: This study provided evidence that ITQ is a valid tool to assess PTSD or CPTSD in community-dwelling NKD.
HIGHLIGHTS
First study to test validity of ICD-11 PTSD and CPTSD for NKD with a Korean version of the ITQ.
Provided evidence that ITQ is a valid tool to assess PTSD or CPTSD in NKD.
Results revealed that depression and somatic symptoms and quality of life were different for PTSD and CPTSD, and that CPTSD was worse than PTSD.
Antecedentes: El Cuestionario Internacional de Trauma (ITQ en su sigla en inglés) es una evaluación de autoreporte focalizado en las características principales del Trastorno de Estrés Postraumático (TEPT) y del Trastorno de Estrés Postraumático complejo (TEPT-C). Es consistente con los principios organizadores de la onceava revisión de la Clasificación International de las Enfermedades (CIE-11) de la OMS. Desde 1990, ha aumentado rápidamente el número de desertores de Corea del Norte (NKD en su sigla en inglés) que han entrado a Corea del Sur para escapar de las violaciones a los derechos humanos, con 33,815 NKD instalados hasta 2021. El gobierno de Corea del Sur enfrenta un desafío importante en apoyar a los NKD para adaptarse e instalarse en la sociedad de Corea del Sur. Los NKD experimentan varios eventos traumáticos durante el proceso de deserción y repatriación. Por lo tanto, es esencial entender los trastornos psicológicos de NKD, especialmente TEPT y TEPT-C.
Objetivo: Este estudio busca evaluar la validez de la evaluación ITQ y explorar las diferencias en los síntomas y la calidad de vida entre TEPT y TEPT-C.
Método: La muestra del estudio estuvo compuesta de 503 NKD expuesto a trauma. Se usaron el análisis factorial confirmatorio (CFA en su sigla en inglés) y análisis de clases latentes (LCA en su sigla en inglés) para evaluar la validez de ITQ. Los análisis de una vía de las varianzas y los análisis post-hoc revelaron la diferencia en los resultados de la Escala de los Síntomas somáticos y Depresión (DSSS en su sigla en inglés) y WHOQOL-BREF entre los síntomas TEPT y TEPT-C de las clases de los LCA.
Resultados: Los resultados de CFA y LCA apoyan la conceptualización del TEPT y TEPT-C de la CIE-11 en NKD. Los resultados del CFA confirmaron que tanto los modelos de primer y de segundo orden fueron estadísticamente adecuados, pero para los NKD viviendo en residencias comunitarias, el modelo de primer orden tuvo un mejor ajuste que el modelo de segundo orden. Los hallazgos del LCA revelaron un modelo de cuatro clases con las clases ‘TEPT’, ‘TEPT-C’, ‘DSO’, y ‘baja sintomatología’. En comparación con la clase TEPT, la clase TEPT-C tuvo niveles más altos de síntomas somáticos y depresión y una calidad de vida más baja.
Conclusión: Este estudio proporciona evidencia que el ITQ es una herramienta válida para evaluar TEPT o TEPT-C en NKD viviendo en residencias comunitarias.
背景:国际创伤问卷(ITQ)是一项自我报告评估,关注创伤后应激障碍(PTSD)和复杂性创伤后应激障碍(CPTSD)的核心特征。这与WHO国际疾病国际疾病分类(ICD-11)第11修订版的组织原则是一致的。自1990年代起,为逃脱人权侵害进入韩国的朝鲜叛逃者人数一直在增长,到2021年,有33,815 NKD定居。韩国社会。在叛逃和遣返过程中,NKD经历了各种创伤事件。因此,必须了解NKD的心理障碍,尤其是PTSD和CPTSD。目的:本研究旨在检验ITQ评估的有效性,并探讨PTSD和CPTSD之间症状和生活质量的差异。方法:本研究样本包括503个创伤暴露的NKD。验证性因素分析(CFA)和潜在类别分析(LCA)用于评估ITQ的有效性。单向方差分析和事后分析显示出ICD-11 PTSD和CPTSD症状LCA类别中抑郁和躯体症状量表(DSS)和WHOQOL-BREF结果的差异。结果:CFA和LCA结果支持NKD中PTSD和CPTSD的ICD-11概念化。 CFA结果验证了一阶和二阶模型都可在统计上拟合,但是对于居住在社区的NKD中,一阶模型比二阶模型具有更好的模型拟合度。 LCA结果揭示了一个具有“ PTSD”,“ CPTSD”,“ DSO”和“低症状”类别的四类模型。与PTSD类别相比,CPTSD类具有更高水平的抑郁和躯体症状和更低的生活质量。结论:本研究为ITQ是评估居住社区的NKD中PTSD或CPTSD的有效工具提供了证据。
Introduction
In 2018, the World Health Organization (WHO) published the 11th version of the International Classification of Diseases (ICD-11) that proposed a novel model of psychotraumatology to differentiate between Post-traumatic Stress Disorder (PTSD), and Complex PTSD (CPTSD), under a general parent category of traumatic stress disorders (Maercker et al., Citation2013). CPTSD is a broader diagnosis intended to describe the complex and diverse psychological characteristics in multiple domains, including somatic, cognitive, affective, behavioural, and relational (Herman, Citation1992). CPTSD includes symptoms of PTSD and three additional symptoms of Disturbance of Self-Organization (DSO). PTSD is characterized by three symptoms: 1) re-experiencing the traumatic event here and now (RE); 2) avoidance of thoughts and memories of the event (AV); and 3) persistent perceptions of heightened current threat (TH). DSO is characterized by severe and persistent: 1) affective dysregulation (AD); 2) negative self-concept (NSC), accompanied by feelings of shame, guilt, or failure associated with the traumatic event; and 3) disturbance in relationships (DR).
The International Trauma Questionnaire (ITQ) is a self-reported assessment focusing solely on the core features of PTSD and CPTSD. The ITQ was developed to be consistent with the organizing principles of the ICD-11 (Ben-Ezra et al., Citation2018; Cloitre et al., Citation2018; Hyland et al., Citation2017; Redican et al., Citation2022). Recent studies have tested the construct validity of ITQ assessment using the confirmatory factor analysis (CFA) (Choi et al., Citation2021a; Hyland et al., Citation2017; Redican et al., Citation2022; Vallières et al., Citation2018) and latent class/profile analysis (LCA/LPA) (Ben-Ezra et al., Citation2018; Haselgruber et al., Citation2020; Redican et al., Citation2022; Tian et al., Citation2020). LCA and LPA were used to cluster individuals in unobserved groups using items of the ITQ, which verified the construct validity. Results of the CFA studies have consistently shown that the latent structure of the ITQ is identified by the first- and second-order models. The results of the LCA/LPA indicate that most studies demonstrated symptom endorsement patterns of a three-class model, comprising PTSD, CPTSD, and low symptom classes (Haselgruber et al., Citation2020; Kazlauskas et al., Citation2018; Murphy et al., Citation2016). Several studies found a four-class model, comprising DSO, PTSD, CPTSD, and low symptom classes (Ben-Ezra et al., Citation2018; Liddell et al., Citation2019; Redican et al., Citation2022; Tian et al., Citation2020). Although there were divergent findings, over 30 different language versions confirmed that the ITQ could distinguish PTSD and CPTSD symptoms as proposed by ICD-11.
The United Nations High Commissioner for Refugees (UNHCR) defines refugees as people who have suffered human rights violations and fled across the borders of their home countries to seek protection elsewhere (Betts et al., Citation2013). Under the authority of the UNHCR, North Koreans who have illegally left their country of origin receive refugee protection. However, most countries in Northeast and Southeast Asia rarely guarantee refugee status to North Korea defectors (NKD), and the U.S. and European countries also implement very selective NKD acceptance policies (Kang, Citation2013). In South Korea, which has been divided as two nations for over half a century, the government positively accepts NKD from the viewpoint of human rights since the late 1990s (Kim, Citation2012b). NKD attain South Korean citizenship automatically once they have proved their identity irrespective of the refugee status determination based on the ‘North Korean Refugees Protection and Settlement Support Act.’ The number of NKD has been rapidly increasing since the 1990s, and 33,815 NKD (24,340 women and 9,475 men) had settled in South Korea by 2021 (Ministry of Unification, Citation2022). Therefore, the South Korean government faces an important task of supporting NKD to successfully adapt and settle in South Korean society.
NKD experience several traumatic events during the process of defecting and repatriation. They cannot deal with the effects of the long-term and chronic traumatic events by themselves. NKD have severe disabilities in key functional areas such as individual, familial, societal, educational, and occupational (Chang & Son, Citation2014; Chung & Kim, Citation2014). According to the 2021 Social Integration Survey of North Korean defectors in South Korea (Korea Hana Foundation, Citation2022), 59% of the NKD experienced stress in general life, 57.8% at work, 51% at school, and 13.3% reported having suicidal thoughts, which was more than twice that of South Koreans (5.2%). NKD still struggle with mental health challenges in South Korea, which affects their settlement in South Korea. However, there are only a few studies on CPTSD symptoms among this population (Hu et al., Citation2008; Jeong & Kim, Citation2014; Kim, Citation2012a).
Revised questionnaires have been used to assess Complex Trauma and Disorder of Extreme Stress (DESNOS) (Van der Kolk et al., Citation2005) among NKD. The results showed high scores of DESNOS subcategories: alterations in the regulation of affect and impulses; alterations in attention or consciousness; somatization; and alterations in relationships with others (Hu et al., Citation2008; Jeong & Kim, Citation2014). CPTSD symptoms of NKD related to psychological disorders include anxiety, helplessness, and retrospection (Hu et al., Citation2008). Furthermore, NKD, classified as having CPTSD, had difficulty adjusting to South Korea (Jeong & Kim, Citation2014). Although several studies demonstrated CPTSD symptoms in NKD, they have limited use for non-standardized questionnaires similar to those assessing the CPTSD construct. Therefore, it is crucial to test the utility of validated assessments to measure ICD-11 PTSD and CPTSD symptoms that are more representative of the symptoms of NKD.
Thus, this study aims to examine the validity of ICD-11 PTSD and CPTSD in a trauma-exposed sample of NKD using the Korean version of ITQ (Choi et al., Citation2021b). Based on previous studies, we performed (1) CFA to test the factorial validity; (2) LCA to support the construct validity; and (3) One way analysis of variances (ANOVAs) and post-hoc analyses to reveal the difference in psychological state and quality of life among the ITQ-11 PTSD and CPTSD symptom LCA classes. This study would help clarify the concepts of PTSD and CPTSD and, subsequently, provide a basis for developing a suitable diagnostic tool for NKD.
Methods
Participants and procedures
The participants comprised trauma-exposed North Korean defectors over the age of 19 living in South Korea (N = 503). Participants of the study were recruited with the assistance of key personnel in online and offline communities for North Korean defectors and centres proving psychological counselling. All participants signed an electronic informed consent form before accessing the questionnaire. The online survey was completed (in approximately 33 min) by 537 participants between August 25 and October 1. Out of the 537 participants, 17 were excluded owing to the survey response time of less than 10 min (N = 8) and data quality (N = 9). An additional 17 participants with no exposure to trauma were excluded, bringing the final number of participants to 503.
In the final sample, the mean age was 46 years (SD = 13.2; range 19-77) and the proportion of age groups was 19–39 years old (32.8%), 40–49 years old (27.6%), 50–59 years old (24.7%), and 60 years or older (14.9%). Most of the participants were women (84.5%), which is reflective of the higher proportion of women (72%) settlers among NKD in South Korea than men (28%) (Ministry of Unification, Citation2022). Participants’ educational attainment levels were as follows: high school graduate (52%), college or higher (31%), and middle school or lower (17%). The employed, not employed and student participants comprised 50.5%, 37.2%, and 12.3%, respectively. Their average economic satisfaction was 2.1 points (SD = 0.9; range 0-5, where a higher score indicates a higher level of satisfaction). The average number of years spent in South Korea was 10.7 (SD = 5.1; range 0-21), the average of traumatic event experiences was 8.9 (SD = 4.6, range 1-20) and the proportion of participants taking psychiatric medication was 23%.
ICD-11 PTSD and CPTSD
The ITQ is a self-report diagnostic scale for PTSD and CPTSD as per the definition in ICD-11. An 18-item version of the ITQ for the ICD-11 PTSD and CPTSD disorders was used in this study (Cloitre et al., Citation2018). This version was translated into Korean and validated by Choi et al. (Citation2021b). The ITQ responses were assessed in relation to the participants’ most distressing traumatic event. The ITQ included six questionnaires in three clusters to assess PTSD symptoms: re-experiencing (RE as measured by RE1, RE2); avoidance (AV as measured by AV1, AV2); and sense of threat (TH as measured by TH1, TH2). DSO symptoms were assessed using six questionnaires comprising the following three clusters: affective dysregulation (AD as measured by AD1, AD2); negative self-concept (NSC as measured by NSC1, NSC2); and disturbance in relationships (DR as measured by DR1, DR2). Additionally, there were three items measuring functional impairment for PTSD and DSO symptoms. The effect of each symptom over the past month was measured by the participants using a five-point Likert scale ranging from 0 (Not at all) to 4 (Extremely). Internal reliability (Cronbach’s α) was satisfactory in our sample for the RE (α = 0.89), AV (0.91), and TH (0.80) PTSD clusters and the AD (α = 0.86), NSC (α = 0.94), and DR (α = 0.92) DSO clusters.
For CFA analyses, each of the six items of PTSD and DSO symptoms was used as continuous variable ranging from 0 to 4. For LCA analyses, each of the three clusters of PTSD (RE, AV, and TH) and DSO (AD, NSC, and DR) symptoms was used based on dichotomized variables. Based on the clinical practice of ICD-11 PTSD and CPTSD, a dichotomous cluster variable was created when at least one of the two items constituting the cluster was greater than or equal to 2 (moderate).
Lifetime traumatic exposures
The Traumatic Event Checklist for NKD, a revised version approved by the previous NKD PTSD researchers (Yoon et al., Citation2007), is a 22-item self-report measure designed to screen for potentially traumatic events in a NKD’s lifetime. The 22 items were organized into 6 categories: (1) disaster and accident-related trauma (natural disaster, serious accident); (2) family-related trauma (divorce of parents in childhood, divorce, unwanted separation from a spouse, parent or sibling, unwanted separation from a child, caring for a family member with a serous illness); (3) trauma related to illness and death (sudden death of a family member or close friend, witnessing death of a family member of close friend, witnessing death of someone, extreme hardship that can risk one’s life, life-threatening illness); (4) trauma related to violence (domestic violence, physical/emotional abuse and neglect by parents in childhood, verbal abuse, physical assault, sexual assault); (5) threats and culture shock (threats to personal security, imprisonment, torture); and (6) social stressors (betrayal, discrimination). The last category was added after the literature review, which suggested unexpected betrayal by a trusted person as a traumatic event for NKD in South Korea during defection (Jeon et al., Citation2005). Additionally, NKD’s mental health was related to the perceived discrimination due to cultural differences in language use, lifestyle, and attitudes (Lee et al., Citation2017). Participants responded dichotomously to experiences of potential traumatic event, and the number of traumatic experiences variable was calculated on a scale of 0–22. In this study, the average number of traumatic events experienced was 8.9 (±4.6) and ranged from 1 to 20.
DSSS and WHOQOL-BREF
DSSS
The Depression and Somatic Symptoms Scale (DSSS; Hung et al., Citation2006b) comprised 22 items with two major subscales: the depression subscale (DS) and the somatic subscale (SS). The DS comprised 12 items, including three vegetative symptoms (insomnia, poor appetite, and loss of interest in sex) and fatigue. The SS consisted of 10 items, with five pain subscales (headache, back pain, chest pain, neck or shoulder soreness, and soreness in more than half of the body's muscles) (Hung et al., Citation2006a). Each question was scored from 0 (absent) to 3 (severe) according to its severity over the past week. The total scores ranged from 0 to 36 for the DS and 0–30 for the SS, with higher scores indicating higher levels of symptoms. This study used the Korean version of DSSS, which was validated in a Korean clinical population (Kim et al., Citation2011). The sample’s internal reliability was adequate, with Cronbach’s alpha values DS (α = 0.91) and SS (α = 0.93).
WHOQOL-BREF
The WHO Quality of Life scale (WHOQOL-BREF), comprising 26 questions, examines two separate items: overall perception of quality of life and overall perception of health, over the previous two weeks. The four domains of 24 items represent an individual’s perception of quality of life in each particular domain: 7 items of physical capacity (PC), 6 items of psychological well-being (PW), 3 items of social relationships (SR), and 8 items of environmental health (EN). The specific information about WHOQOL-BREF was documented by the Whoqol Group (Citation1998). The items were measured on a response scale of 1 (disagree) to 5 (extremely agree), with higher scores indicating a higher the quality of life. The domain scores were calculated by multiplying the average scores of all items in each domain by four. All domain scores have a potential score range of 4–20. The study used the Korean version of WHOQOL-BREF developed by Min et al. (Citation2000). The internal reliability calculated by Cronbach’s alpha ranged from acceptable to good for each domain of PC (α = 0.88), PW (α = 0.87), SR (α = 0.71), and EN (α = 0.81).
Analysis
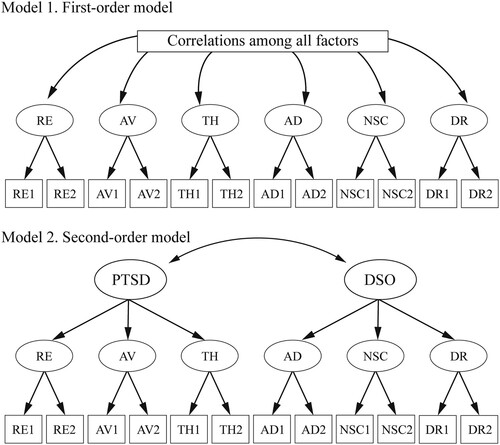
This study used three methods to conduct the statistical analysis. First, CFA was performed to test the symptom structure and factorial validity of PTSD and CPTSD among NKD, wherein the first- and second-order models were tested. The first-order model was a correlated six-factor model based on the ICD-11 specifications of the three PTSD (RE, AV, and TH) and three DSO (AD, NSC, and DR) symptom clusters, each measured by two items. The second-order model was a correlated two-factor model in which the RE, AV, and TH clusters were loaded on a second-order PTSD symptom and the AD, NSC, and DR clusters were loaded on a second-order DSO symptom. The structures of the two models are shown in . The model fit of CFA was estimated as acceptable using a non-significant chi-square (χ2), the Comparative Fit Index (CFI) (Bentler, Citation1990), the Tucker-Lewis Index (TLI) (Tucker & Lewis, Citation1973) with a value greater than 0.90, the Root-Mean-Square-Error of Approximation (RMSEA) with a value less than 0.05 considered excellent and values up to 0.08 considered reasonable (Steiger, Citation1990), and the Standard Root-Mean-Square (SRMR) with a value of 0.08 or less. The statistics of chi-square (χ2), with p-value higher than .05, indicated a better model fit and that the covariance matrix derived from the model represents the population covariance. However, it is sensitive to sample size, with larger sample sizes decreasing the p-value (Babyak & Green, Citation2010).
Figure 1. First- and second-order models of ICD-11 PTSD and CPTSD using the ITQ.
Second, the latent class analysis (LCA) method was performed to identify the number of classes based on the diagnostic thresholds for the three PTSD (RE, AV, and TH) and DSO (AD, NSC, and DR) symptom clusters (McCutcheon, Citation1987). The model solutions were evaluated on the Akaike Information Criterion (AIC) (Akaike, Citation1974), the Bayesian Information Criterion (BIC) (Schwarz, Citation1978), sample-size adjusted BIC (SABIC) (Sclove, Citation1987), entropy, the Lo-Mendell-Rueben Test (LMRT) (Lo et al., Citation2001), and the Bootstrap Likelihood Ratio Test (BLRT) (Peel & McLachlan, Citation2000). Lower BIC values indicate a better model fit. The LMRT and BLRT provide a p-value, indicating whether the model should be rejected in favour of a model with one less class (Lo et al., Citation2001). Entropy is a measure of the quality of classification, with values closer to 1 indicating greater classification accuracy (Ramaswamy et al., Citation1993) and 0.8 a commonly used cutoff point (Lubke & Muthén, Citation2007). In LCA, there is a sensitivity of the likelihood function to converge on a local solution. To avoid this problem, we used 500 random start values in the initial stage and 100 optimizations in the last stage (McLachlan & Peel, Citation2000; Nylund-Gibson & Choi, Citation2018). Six latent class models were assessed to find the best fit model. The CFA and LCA were conducted using Mplus, Version 6.12 (Muthén & Muthén, Citation2013). All models in the CFA and LCA were estimated using robust maximum likelihood estimation (MLR; Wang & Wang, Citation2019).
Third, multinominal logistic regression analyses were used to investigate significant predictors of PTSD and CPTSD symptom LCA classes, which included socio-economic status, psychiatric medication taking, and traumatic event experiences. The multinominal logistic regression models calculated odds ratios for the predictors of PTSD and CPTSD classes, taking the low-symptom class as the reference group. Finally, one-way ANOVAs and pairwise post hoc comparisons utilizing the Bonferroni correction were conducted to compare mean scores on DSSS and WHOQOL-BREF across PTSD and CPTSD symptom LCA classes. As latent class interpretation should include practical knowledge to avoid reaching a solely analytical solution (Xi, Citation2016), latent class membership was introduced as an independent variable in subsequent analyses. The multinominal logistic regression analyses, ANOVAs, and post hoc comparisons were performed in STATA 15.0 (StataCorp., College Station, TX, USA), and p-values less than .05 were considered statistically significant.
Results
The model fit statistics of the CFA are presented in . The results showed that the first- and second-order models showed excellent fit regarding CFI (0.984 in the first-order model and 0.964 in the second-order model) and TLI (0.973 in the first-order model and 0.950 in the second-order model). In RMSEA and SRMR, the first-order model was excellent (0.058 in RMSEA and 0.023 in SRMR), and the second-order model was acceptable (0.080 in RMSEA and 0.065 in SRMR). Moreover, factor loadings of the first- and second-order models were all positive and statistically significant (p-value <.001). A comprehensive interpretation of the statistical results proved the first-order model to be a better model fit than the second-order model. Factor loadings for the two models are reported in Supplementary Table 1.
Table 1. Fit statistics for CFA of the ITQ.
The model fit statistics of the LCA are shown in . The five- and six-class models were not considered to be the final models as they did not yield a significant LMRT. The two-, three-, and four-class models had a significant LMRT. However, the Pearson and Log-likelihood Chi-square tests of fit are non-significant only in the four-class model. In addition, the four-class model yielded the lowest AIC, BIC, and SABIC values, which strongly supported its statistical superiority. Based on the fit indices, the four-class model was selected as the most appropriate.
Table 2. Fit statistics for latent class analysis.
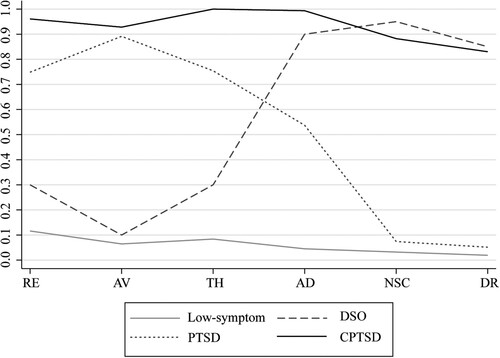
The four classes were labelled based on the pattern of PTSD and DSO. The six symptom clusters for PTSD and DSO are presented in . Class 1 (30.8%, n = 155) was characterized by a low diagnostic threshold in both PTSD and DSO symptom clusters and was labelled as ‘low-symptom.’ Class 2 was the smallest (4.0%, n = 20) and characterized by a low diagnostic threshold in the PTSD symptom clusters but a relatively high diagnostic threshold in the DSO symptom clusters. This class was labelled the ‘DSO.’ Class 3 (34.8%, n = 175) was labelled ‘PTSD’, as people in this class had a high diagnostic threshold in the PTSD symptom clusters but a low diagnostic threshold in the DSO symptom clusters. Class 4 (30.4%, n = 153) was characterized by a high diagnostic threshold in both PTSD and DSO symptom clusters and was labelled the ‘CPTSD.’ The Supplementary Table 2 shows the rates of PTSD and DSO symptom clusters by PTSD and CPTSD symptom LCA classes.
Figure 2. Mean scores on ICD-11 PTSD and CPTSD symptom LCA classes in North Korean defectors who were exposed to traumatic events (N = 503).
Note: Re: re-experiencing; AV: avoidance; TH: sense of current threat; AD: affective dysregulation; NSC: negative self-concept; DR: disturbances in relationship.
Comparing the 22 traumatic event exposure rates by ICD-11 PTSD and CPTSD symptoms LCA classes, excluding three events (natural disaster, parental divorce, and separation from family), the exposure rates of 19 traumatic experiences were significantly different among the four LCA classes. The CPTSD class had the highest exposure rate for 17 traumatic experiences (fire or explosion, the sudden death of family or close person, witnessing a sudden death of family or close person, witnessing a sudden death of others, severe difficulty, severe illness, forced imprisonment, torture, violence by others, violence by family, divorce, separation from children, caring for sick family, betrayal, discrimination, verbal violence and sexual assault). The life-threatening traumatic experience rate was the highest in the PTSD class, and the child abuse rate by parents was the highest in the DSO class. The results are shown in Supplementary Table 3.
shows the significant predictors of socio-economic status, psychiatric medication taking, and traumatic event experiences for ICD-11 PTSD and CPTSD symptom LCA classes with multinomial logistic regression analysis. Taking the low symptom class as the reference group, the PTSD and CPTSD classes were more likely to be in the age groups of 40–49 years (OR = 2.13, 95% CI: 1.22–3.71 for PTSD and OR = 2.53, 95% CI: 1.43–4.68 for CPTSD), 50–59 years (OR = 3.05, 95% CI:1.68–5.55 for PTSD and OR = 4.04, 95% CI: 2.16–7.56 for CPTSD), and 60–79 years (OR = 3.13, 95% CI: 1.52–6.43 for PTSD and OR = 4.17, 95% CI: 1.98–8.80 for CPTSD). The predictors of PTSD and CPTSD classes included the participants who had high school education, or had college or higher education in North Korea (OR = 2.70, 95% CI: 1.48–4.90 for PTSD and OR = 3.47, 95% CI: 1.80–6.72 for CPTSD), (OR = 2.13, 95% CI: 1.13–4.03 for PTSD and OR = 2.79, 95% CI: 1.39–5.60 for CPTSD), and experienced traumatic experiences. (OR = 1.18, 95% CI: 1.12–1.23 for PTSD and OR = 1.28, 95% CI: 1.21–1.37 for CPTSD). Women were more likely to be classified in the CPTSD than the low-symptom class (OR = 2.25, 95% CI: 1.20–4.23). The CPTSD class was also associated with non-employment status (OR = 2.90, 95% CI: 1.83–4.61) and lower economic satisfaction (OR = 0.40, 95% CI: 0.30–0.53). The DSO (OR = 10.64, 95% CI: 3.03–37.42), PTSD (OR = 5.99, 95% CI: 2.44–14.7), and CPTSD (OR = 20.94, 95% CI: 8.72–50.29) classes were more likely to take psychiatric medication than the low-symptom class. The number of years spent in South Korea was not associated with the DSO, PTSD, and CPTSD classes.
Table 3. Unadjusted multinomial regression for PTSD and CPTSD symptom LCA classes (N = 503).
shows the significant differences in the mean score of depression and somatic symptoms and WHOQOL-BREF across ICD-11 PTSD and CPTSD classes. These differences were compared using one-way ANOVAs and post hoc analyses. Results of one-way ANOVAs showed significant differences among the LCA classes on all psychological states and quality of life. Specifically, the average score of depression was 18.3 (SD = 7.3) in CPTSD, 14.6 (SD = 5.7) in DSO, 11.8 (SD = 5.9) in PTSD, and 7.5 (SD = 4.6) in low-symptom classes. The average score of somatic symptoms was 15.0 (SD = 7.1) in CPTSD, 10.6 (SD = 5.2) in DSO, 9.9 (SD = 5.7) in PTSD, and 5.7 (SD = 5.3) in low-symptom classes. The results from the post hoc analyses revealed that NKD in the CPTSD class had significantly higher level of depression and somatic symptoms, followed by DSO, PTSD, and lastly the low-symptom class. The mean WHOQOL-BREF score for all aspects was the lowest in the CPTSD class: overall quality of life 2.6 (SD = 0.3), overall quality of health 2.2 (SD = 0.8), physical health 9.6 (SD = 2.8), psychological state 10.3 (SD = 2.9), social relationship 10.6 (SD = 2.6), and environment 10.6 (SD = 2.2). The post hoc analyses of WHOQOL-BREF showed that the CPTSD class had consistently poorer quality of life than the PTSD and low-symptom classes in all aspects. The differences between CPTSD and DSO classes were not significant in the post hoc results of overall quality of life, psychological state, and social relationships.
Table 4. Difference on psychological state and quality of life across ICD-11 PTSD and CPTSD symptom LCA classes (N = 503)
Discussion
This is the first study to test the validity of the ICD-11 PTSD and CPTSD for NKD using a Korean version of the ITQ. The CFA and LCA methods were used to test the construct validity, and the two main results were as follows: 1) the CFA findings confirmed that both the first- and second-order models were statistically fit; however, the first-order model had better model fit than the second-order model for community-dwelling NKD; 2) the LCA findings revealed a four-class model (PTSD, CPTSD, DSO, and low-symptom). The overall findings supported the distinction between PTSD and CPTSD, which has important implications for recognizing CPTSD among NKD. Lastly, the results revealed that depression and somatic symptoms and quality of life were more severe in CPTSD compared to PTSD, based on the ICD-11 PTSD and CPTSD symptoms LCA classes.
Contrary to our results, ICD-11 finds/states that the second-order model reflects the distinction between PTSD and DSO symptoms better than the first-order model. To date, several studies support the second-order model from CFA results in clinical samples (Hyland et al., Citation2017; Karatzias et al., Citation2016; Kazlauskas et al., Citation2018). However, our results were also consistent with the prior studies that examined community-dwelling participants exposed to trauma events (Ben-Ezra et al., Citation2018; Haselgruber et al., Citation2020; Ho et al., Citation2020; Li et al., Citation2021). An important feature of our sample was that they were non-clinical participants who experienced diverse types of traumatic events.
The LCA results indicated that the four-class model showed the best fitting model, which supported the ICD-11 conceptualization of PTSD and CPTSD. They were in line with previous studies conducted on the general population (Ben-Ezra et al., Citation2018; Liddell et al., Citation2019; Redican et al., Citation2022; Tian et al., Citation2020). The LCA results from a study on 112 refugees with diverse backgrounds resettled in Australia also identified the four-class model as the best fit (Liddell et al., Citation2019). In our study, there was a small ‘DSO class’ (4%), in contrast to the clinical sample results classified into three classes (low-symptom, PTSD, and CPTSD). This class had relatively low symptoms in PTSD but was vulnerable to self-concept or relationships (Ho et al., Citation2020).
Among the LCA classes, PTSD and CPTSD had higher rates in almost all of the traumatic events compared to the low-symptom class. However, in three traumatic events — physical/emotional abuse and neglect by parents in childhood, discrimination, and verbal abuse — the DSO class had similar rates of exposure to the CPTSD class. Previous NKD studies have classified interpersonal trauma events into physical and verbal violence and sexual assault by acquaintances or strangers. NKD with interpersonal trauma experience were more likely to have problems in emotional regulation, negative perception, and distrust of themselves and others (Kim, Citation2012a). These three traumatic events could be considered more important factors for the development and maintenance of DSO symptoms than that of PTSD symptoms (Paetzold & Rholes, Citation2021). These results also indicated that the DSO symptoms were distinct from the PTSD symptoms, which seemed reasonable for the conceptualization of CPTSD (Knefel et al., Citation2019).
This study further revealed the difference in depression and somatic symptoms and quality of life among PTSD and CPTSD symptom LCA classes for NKD. Individuals in the CPTSD class reported significantly higher levels of depression and somatic symptoms than those in the PTSD class (Murphy et al., Citation2016; Palic et al., Citation2016; Redican et al., Citation2022; Tian et al., Citation2020). One previous paper presented examples of somatic symptoms among NKD, including indigestion, constipation, and cystitis, but the general practitioner could not diagnose the symptoms (Ahn et al., Citation2007). In this study, we revealed that somatic symptoms were highly associated with PTSD and CPTSD symptoms and that NKD with CPTSD were more likely to have somatic symptoms. Therefore, in clinical practice, the physical suffering of NKD should be examined with the simultaneous possibility of PTSD and CPTSD and the approach to treating the physical and psychological pain of NKD should be meticulous.
Complementing previous studies, this study demonstrated that individuals with CPTSD have lower levels of multidimensional quality of life, including positive aspects of life (Fortin et al., Citation2021; Huijts et al., Citation2012; Redican et al., Citation2022). Individuals with CPTSD are traumatized repeatedly and cumulatively in specific situations over time, which results in an impaired psychological state and overall quality of life. However, a study found that the quality of life of refugees was related not only to their experiences during their refugee status but also to the settlement period (Hu et al., Citation2013). Additionally, a study on the quality of life among NKD diagnosed with PTSD indicated that their quality of life was associated with poor language comprehension, difficulty interacting with South Koreans, and discrimination (Han et al., Citation2015). Moreover, these difficulties in adapting to South Korea were also higher in NKD diagnosed with PTSD. The results of the present study revealed that the quality of life among the CPTSD class was worse than the low-symptom and PTSD classes. These results have implications for psychiatric intervention strategies to improve the overall quality of life and adaptation in South Korea, with a focus on PTSD and CPTSD symptoms.
Additionally, we found that individuals in the DSO class had poorer quality of life with regard to psychological state and social relationships than individuals in the PTSD class. Also, the DSO class had higher levels of depression and similar levels of somatic symptoms compared to the PTSD class. Similar to the CPTSD, the DSO class had challenges in terms of their psychological state and quality of life. DSO symptoms engender psychological disorders and, in the current study, the DSO class had a higher proportion of individuals taking psychiatric medication (30%) compared to the PTSD class (19.4%). Similarly, in a study of community-dwelling Chinese college students, students in the DSO class had higher levels of depression and dissociation than those in the PTSD class (Tian et al., Citation2020). Therefore, although the DSO class was classified as the low-symptom class in the clinical context, we carefully suggested that DSO symptoms could be interpreted as a variant of CPTSD symptoms and that individuals with DSO symptoms be clinically examined for comorbidities such as depression and anxiety for healing and recovery of their symptoms.
Limitations
In the present study, there were three primary limitations. First, because our respondents voluntarily participated online, it is possible that individuals who do not access North Korean online sites or communities were not included in this study. Second, in contrast to clinician-administered diagnostic interviews, the use of self-reported assessments may overestimate diagnostic rates. Lastly, a relatively small percentage of men (15.5%) participated in our study. Even though the proportion of men among NKD is already small (28%), our sample was still disproportionate.
Conclusion
The results of this study provide additional evidence of the factorial and construct validity of ICD-11 PTSD and CPTSD for the refugee population, specifically North Korean defectors settled in South Korea. These results suggest the first empirical evidence that ITQ is applicable to both PTSD and CPTSD in community-dwelling NKD and that it is a useful tool to identify PTSD and CPTSD symptoms. Furthermore, the results reveal that depression and somatic symptoms and quality of life were different for PTSD and CPTSD and that CPTSD was worse than PTSD. Especially considering somatic symptoms, both clinical psychologists and physicians should pay careful attention to PTSD and CPTSD symptoms for NKD. Due to differences in the symptoms, severity, and mental status between PTSD and CPTSD in NKD, treatment approaches, interventions, and duration may differ, which should be examined in future research.
Ethics approval
The Severance Hospital Institutional Review Board approved this study (IRB number 4-2021-0897).
Supplemental Material
Download MS Word (37.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are not publicly available due to privacy and sensitive information of the participants. Moreover, the data contain potentially identifiable participants. The restricted data are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Ahn, E. M., Song, J. I., Kang, H. S., Park, J. J., Yoo, S. H., & Huh, B. R. (2007). The symptom expression and the illness behavior of North Korean defectors: Toward an effective therapeutic relationships. Journal of the Korean Academy of Family Medicine, 28(5), 352–358.
- Akaike, H. (1974). A new look at the statistical model identification. IEEE Transactions on Automatic Control, 19(6), 716–723. https://doi.org/10.1109/tac.1974.1100705
- Babyak, M. A., & Green, S. B. (2010). Confirmatory factor analysis: An introduction for psychosomatic medicine researchers. Psychosomatic Medicine, 72(6), 587–597. https://doi.org/10.1097/PSY.0b013e3181de3f8a
- Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238–246. https://doi.org/10.1037/0033-2909.107.2.238
- Ben-Ezra, M., Karatzias, T., Hyland, P., Brewin, C. R., Cloitre, M., Bisson, J. I., Roberts, N. P., Lueger-Schuster, B., & Shevlin, M. (2018). Posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) as per ICD-11 proposals: A population study in Israel. Depression and Anxiety, 35(3), 264–274. https://doi.org/10.1002/da.22723
- Betts, A., Loescher, G., & Milner, J. (2013). The United Nations High Commissioner for Refugees (UNHCR): The politics and practice of refugee protection. Routledge, https://doi.org/10.4324/9780203146651
- Chang, M. S., & Son, E. J. (2014). Complex PTSD symptoms and psychological problems of the North Korean defectors. The Korean Journal of Health Psychology, 19(4), 973–999. https://doi.org/10.17315/kjhp.2014.19.4.006
- Choi, H., Kim, N., & Lee, A. (2021a). ICD-11 posttraumatic stress disorder (PTSD) and complex PTSD among organized violence survivors in modern South Korean history of political oppression. Anxiety, Stress, & Coping, 34(2), 203–214. https://doi.org/10.1080/10615806.2020.1839889
- Choi, H., Lee, W., & Hyland, P. (2021b). Factor structure and symptom classes of ICD-11 complex posttraumatic stress disorder in a South Korean general population sample with adverse childhood experiences. Child Abuse & Neglect, 114, 104982. https://doi.org/10.1016/j.chiabu.2021.104982
- Chung, Y. K., & Kim, H. J. (2014). The relationship between traumatic incidents and social adaptation among North Korean refugees: Focusing on the mediating effect of complex post traumatic stress disorder. Korean Journal of Social Welfare Studies, 45(4), 143–167. https://doi.org/10.16999/kasws.2014.45.4.143
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., Karatzias, T., & Hyland, P. (2018). The international trauma questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546. https://doi.org/10.1111/acps
- Fortin, M., Fortin, C., Savard-Kelly, P., Guay, S., & El-Baalbaki, G. (2021). The effects of psychotherapies for posttraumatic stress disorder on quality of life in the civilian population: A meta-analysis of RCTs. Psychological Trauma: Theory, Research, Practice, and Policy, 13, 673–683. https://doi.org/10.1037/tra0000992
- Han, N. Y., Lee, S. H., Yoo, S. Y., Kim, S. J., Jun, J. Y., Won, S. D., & Shin, M. N. (2015). Predictors of PTSD among north Korean defectors visited psychiatric department of North Korean defectors treatment center. Journal of Korean Neuropsychiatric Association, 54(1), 105–111. https://doi.org/10.4306/jknpa.2015.54.1.105
- Haselgruber, A., Sölva, K., & Lueger-Schuster, B. (2020). Validation of ICD-11 PTSD and complex PTSD in foster children using the international trauma questionnaire. Acta Psychiatrica Scandinavica, 141(1), 60–73. https://doi.org/10.1111/acps.13100
- Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377–391. https://doi.org/10.1002/jts.2490050305
- Ho, G. W., Hyland, P., Shevlin, M., Chien, W. T., Inoue, S., Yang, P. J., Chen, F. H., Chan, A. C., & Karatzias, T. (2020). The validity of ICD-11 PTSD and complex PTSD in East Asian cultures: Findings with young adults from China, Hong Kong, Japan, and Taiwan. European Journal of Psychotraumatology, 11(1), 1717826. https://doi.org/10.1080/20008198.2020.1717826
- Hu, S., Choi, Y. J., & Jung, T. (2008). Diagnosis of complex post traumatic stress disorder for North Korean refugees. Korean Journal of Stress Research, 16(4), 379–386.
- Hu, S., Park, E., Park, J., & Jung, T. (2013). Social adaptation of college students from North Korea: A case study with focus on complex-PTSD. Korean Journal of Stress Research, 21, 193–202.
- Huijts, I., Kleijn, W. C., van Emmerik, A. A., Noordhof, A., & Smith, A. J. (2012). Dealing with man-made trauma: The relationship between coping style, posttraumatic stress, and quality of life in resettled, traumatized refugees in the Netherlands. Journal of Traumatic Stress, 25(1), 71–78. https://doi.org/10.1002/jts.21665
- Hung, C. I., Su, Y. J., Weng, L. J., & Liu, C. Y. (2006a). Preliminary study of a scale measuring depression and somatic symptoms. Psychological Reports, 99(2), 379–389. https://doi.org/10.2466/pr0.99.2.379-389
- Hung, C. I., Weng, L. J., Su, Y. J., & Liu, C. Y. (2006b). Depression and somatic symptoms scale: A new scale with both depression and somatic symptoms emphasized. Psychiatry and Clinical Neurosciences, 60(6), 700–708. https://doi.org/10.1111/j.1440-1819.2006.01585.x
- Hyland, P., Shevlin, M., Brewin, C. R., Cloitre, M., Downes, A., Jumbe, S., Karatzias, T., Bisson, J. I., & Roberts, N. P. (2017). Validation of post-traumatic stress disorder (PTSD) and complex PTSD using the international trauma questionnaire. Acta Psychiatrica Scandinavica, 136(3), 313–322. https://doi.org/10.1111/acps.12771
- Jeon, W., Hong, C., Lee, C., Kim, D. K., Han, M., & Min, S. (2005). Correlation between traumatic events and posttraumatic stress disorder among North Korean defectors in South Korea. Journal of Traumatic Stress, 18(2), 147–154. https://doi.org/10.1002/jts.20017
- Jeong, Y., & Kim, H. (2014). The relationship between traumatic incidents and social adaptation among North Korean refugees: Focusing on the mediating effect of complex post traumatic stress disorder. Korean Journal of Social Welfare Studies, 45(4), 143–167. https://doi.org/10.16999/kasws.2014.45.4.143
- Kang, J. W. (2013). Human rights and refugee status of the North Korean diaspora. North Korean Review, 9(2), 4–17. https://www.jstor.org/stable/43908916. https://doi.org/10.3172/NKR.9.2.4
- Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D., Roberts, N., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of PTSD and complex PTSD (ICD-TQ): Evidence of construct validity. Journal of Anxiety Disorders, 44, 73–79. https://doi.org/10.1016/j.janxdis.2016.10.009
- Kazlauskas, E., Gegieckaite, G., Hyland, P., Zelviene, P., & Cloitre, M. (2018). The structure of ICD-11 PTSD and complex PTSD in Lithuanian mental health services. European Journal of Psychotraumatology, 9(1), 1414559. https://doi.org/10.1080/20008198.2017.1414559
- Kim, H. K. (2012a). Difference on complex PTSD and PTSD symptoms according to types of traumatic events in North Korean refugees. The Korean Journal of Psychology : General, 31(4), 1003–1022.
- Kim, K. W., Hong, J. P., Park, S. J., Choi, J. H., & Choi, H. R. (2011). Reliability and validity of Korean version of depression and somatic symptom scale (DSSS). Anxiety and Mood, 7(1), 9–15. https://doi.org/10.30773/pi.2020.0112
- Kim, S. K. (2012b). “Defector,” “Refugee,” or “Migrant”? North Korean settlers in South Korea's changing social discourse. North Korean Review, 8(2), 94–110. https://www.jstor.org/stable/43910315. https://doi.org/10.3172/NKR.8.2.94
- Knefel, M., Lueger-Schuster, B., Karatzias, T., Shevlin, M., & Hyland, P. (2019). From child maltreatment to ICD-11 complex post-traumatic stress symptoms: The role of emotion regulation and re-victimisation. Journal of Clinical Psychology, 75(3), 392–403. https://doi.org/10.1002/jclp.22655
- Korea Hana Foundation. (2022). 2021 Social Integration Survey of North Korea Defectors.
- Lee, Y., Lee, M., & Park, S. (2017). Mental health status of North Korean refugees in South Korea and risk and protective factors: A 10-year review of the literature. European Journal of Psychotraumatology, 8(sup2), 1369833. https://doi.org/10.1080/20008198.2017.1369833
- Li, J., Wang, W., Hu, W., Yuan, Z., Zhou, R., Zhang, W., & Qu, Z. (2021). Validation of posttraumatic stress disorder (PTSD) and complex PTSD in Chinese children as per the ICD-11 proposals using the international trauma questionnaire. European Journal of Psychotraumatology, 12(1), 1888525. https://doi.org/10.1080/20008198.2021.1888525
- Liddell, B. J., Nickerson, A., Felmingham, K. L., Malhi, G. S., Cheung, J., Den, M., Askovic, M., Coello, M., Aroche, J., & Bryant, R. A. (2019). Complex posttraumatic stress disorder symptom profiles in traumatized refugees. Journal of Traumatic Stress, 32(6), 822–832. https://doi.org/10.1002/jts.22453
- Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88(3), 767–778. https://doi.org/10.1093/biomet/88.3.767
- Lubke, G., & Muthén, B. O. (2007). Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Structural Equation Modeling, 14(1), 26–47. https://doi.org/10.1080/10705510709336735
- Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., Reed, G. M., Van Ommeren, M., Humayun, A., Jones, L. M., Kagee, A., & Llosa, A. E. (2013). Proposals for mental disorders specifically associated with stress in the international classification of diseases-11. The Lancet, 381(9878), 1683–1685. https://doi.org/10.1016/S0140-6736(12)62191-6
- McCutcheon, A. L. (1987). Latent Class Analysis. Sage.
- McLachlan, G., & Peel, D. (2000). Finite Mixture Modeling. Wiley.
- Min, S. K., Lee, C. I., Kim, K. I., Suh, S. Y., & Kim, D. K. (2000). Development of Korean version of WHO quality of life scale abbreviated version (WHOQOL-BREF). Journal of Korean Neuropsychiatric Association, 39(3), 571–579.
- Ministry of Unification. (2022). Manual for the Resettlement Support for North Korean Refugees.
- Murphy, S., Elklit, A., Dokkedahl, S., & Shevlin, M. (2016). Testing the validity of the proposed ICD-11 PTSD and complex PTSD criteria using a sample from Northern Uganda. European Journal of Psychotraumatology, 7(1), 32678. https://doi.org/10.3402/ejpt.v7.32678
- Muthén, L., & Muthén, B. (2013). Mplus User's Guide. Muthén & Muthén.
- Nylund-Gibson, K., & Choi, A. Y. (2018). Ten frequently asked questions about latent class analysis. Translational Issues in Psychological Science, 4(4), 440–461. https://doi.org/10.1037/tps0000176
- Paetzold, R. L., & Rholes, W. S. (2021). The link from child abuse to dissociation: The roles of adult disorganized attachment, self-concept clarity, and reflective functioning. Journal of Trauma & Dissociation, 22(5), 615–635. https://doi.org/10.1080/15299732.2020.1869654
- Palic, S., Zerach, G., Shevlin, M., Zeligman, Z., Elklit, A., & Solomon, Z. (2016). Evidence of complex posttraumatic stress disorder (CPTSD) across populations with prolonged trauma of varying interpersonal intensity and ages of exposure. Psychiatry Research, 246, 692–699. https://doi.org/10.1016/j.psychres.2016.10.062
- Peel, D., & McLachlan, G. J. (2000). Robust mixture modelling using the t distribution. Statistics and Computing, 10(4), 339–348. https://doi.org/10.1023/A:1008981510081
- Ramaswamy, V., DeSarbo, W. S., Reibstein, D. J., & Robinson, W. T. (1993). An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Marketing Science, 12(1), 103–124. https://doi.org/10.1287/mksc.12.1.103
- Redican, E., Cloitre, M., Hyland, P., McBride, O., Karatzias, T., Murphy, J., & Shevlin, M. (2022). The latent structure of ICD-11 posttraumatic stress disorder (PTSD) and complex PTSD in a general population sample from USA: A factor mixture modelling approach. Journal of Anxiety Disorders, 85, 102497. https://doi.org/10.1016/j.janxdis.2021.102497
- Schwarz, G. (1978). Estimating the dimension of a model. The Annals of Statistics, 6(2), 461–464. https://doi.org/10.1214/aos/1176344136
- Sclove, S. L. (1987). Application of model-selection criteria to some problems in multivariate analysis. Psychometrika, 52(3), 333–343. https://doi.org/10.1007/BF02294360
- Steiger, J. H. (1990). Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research, 25(2), 173–180. https://doi.org/10.1207/s15327906mbr2502_4
- Tian, Y., Wu, X., Wang, W., Zhang, D., Yu, Q., & Zhao, X. (2020). Complex posttraumatic stress disorder in Chinese young adults using the international trauma questionnaire (ITQ): A latent profile analysis. Journal of Affective Disorders, 267, 137–143. https://doi.org/10.1016/j.jad.2020.02.017
- Tucker, L. R., & Lewis, C. (1973). A reliability coefficient for maximum likelihood factor analysis. Psychometrika, 38(1), 1–10. https://doi.org/10.1007/BF02291170
- Vallières, F., Ceannt, R., Daccache, F., Abou Daher, R., Sleiman, J., Gilmore, B., Byrne, S., Shevlin, M., Murphy, J., & Hyland, P. (2018). ICD-11 PTSD and complex PTSD amongst Syrian refugees in Lebanon: The factor structure and the clinical utility of the international trauma questionnaire. Acta Psychiatrica Scandinavica, 138(6), 547–557. https://doi.org/10.1002/jts.20047
- Van der Kolk, B. A., Roth, S., Pelcovitz, D., Sunday, S., & Spinazzola, J. (2005). Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. Journal of Traumatic Stress: Official Publication of the International Society for Traumatic Stress Studies, 18(5), 389–399. https://doi.org/10.1111/acps.12973
- Wang, J., & Wang, X. (2019). Structural Equation Modeling: Applications Using Mplus. John Wiley & Sons.
- Whoqol Group. (1998). Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychological Medicine, 28(3), 551–558. https://doi.org/10.1017/s0033291798006667
- Xi, J. (2016). Types of integration and depressive symptoms: A latent class analysis on the resettled population for the three gorges dam project, China. Social Science & Medicine, 157, 78–86. https://doi.org/10.1016/j.socscimed.2016.03.045
- Yoon, Y. S., Kim, H. A., & Han, S. Y. (2007). Validation and development of a post-traumatic stress symptom scale for dislocated North Koreans in South Korea. The Korean Journal of Counseling and Psychotherapy, 19(3), 693–718.