
ABSTRACT
Background: Although symptoms of posttraumatic stress disorder (PTSD) have been associated with the COVID-19 pandemic experiences, no study has explored yet the association of specific COVID-19 narratives with peritraumatic distress, the precursor of PTSD.
Objective: To explore the worst experiences associated with peritraumatic distress during the first wave of the COVID-19 pandemic.
Method: Adult residents (N = 1098), from the US (n = 741) and Italy (n = 357), completed an online survey including socio-demographic data, COVID-19-related experiences, the Peritraumatic Distress Inventory and an open question on their worst experiences during the first period of the COVID-19 pandemic (April–May 2020). A thematic content analysis (TCA) was conducted on the answers to the open question and a classification and regression tree (CART) analysis was used to identify the themes that best predicted the clinical levels of peritraumatic distress.
Results: The main TCA themes related to participants’ worst COVID-19 experiences were anxiety, threat, loss, anger, stress and constriction. Threat was the most prevalent theme and correlated with experiences such as being quarantined, being infected and a loved one receiving the diagnosis. US participants’ descriptions of their worst experiences related more to life-threat and loss, while Italians reported more threat to the world, stress, social isolation, and feeling trapped. In the CART analysis, the main predictor (79.9%) was perceiving negative effects from the COVID-19 crisis. Among them, a COVID-related threat to self-experience was the most robust predictor. In its absence, being deprived of resources or experiencing high levels of anxiety were other robust predictors.
Conclusions: The study provided evidence of the utility of a mixed-method approach in conceptualizing experiences associated with the COVID-19 pandemic and the risk of traumatic symptoms. Its findings may inform healthcare interventions and policies for tackling the new challenges posed by the COVID-19 pandemic.
HIGHLIGHTS
Clinically significant levels of peritraumatic distress symptoms were prevalent during the COVID-19 pandemic.
Clinically significant levels of peritraumatic distress during the COVID-19 pandemic were related to experiences of life-threat, resource deprivation, and anxiety, cross-cutting the themes articulated by the thematic content analysis of anxiety, threat, loss, anger, stress and constriction.
The US and Italian participants’ descriptions of their worst experiences differed in subtle but important ways, with Americans reporting more life-threat and losses compared to Italians reporting more threat to the world, stress, social isolation, and feelings of being trapped.
Antecedentes: Aunque los síntomas del trastorno de estrés postraumático (TEPT) se han asociado con las experiencias de la pandemia de COVID-19, ningún estudio ha explorado aún la asociación de las narrativas específicas de COVID-19 con el distres peritraumático, el precursor del TEPT.
Objetivo: Explorar las peores experiencias asociadas al distres peritraumático durante la primera ola de la pandemia COVID-19.
Método: Adultos residentes (N = 1098), de los EE.UU. (n = 741) e Italia (n = 357), completaron una encuesta en línea que incluía datos sociodemográficos, experiencias relacionadas con la COVID-19, el Inventario de Distrés Peritraumático y una pregunta abierta sobre sus peores experiencias durante el primer período de la pandemia de la COVID-19 (abril-mayo de 2020). Se realizó un análisis de contenido temático (TCA, en sus siglas en inglés) sobre las respuestas a la pregunta abierta y se utilizó un análisis de árbol de clasificación y regresión (CART, en sus siglas en inglés) para identificar los temas que mejor predecían los niveles clínicos de distres peritraumático.
Resultados: Los principales temas del TCA relacionados con las peores experiencias de COVID-19 de los participantes fueron la ansiedad, la amenaza, la pérdida, la ira, el estrés y la constricción. La amenaza fue el tema más prevalente y se correlacionó con experiencias como estar en cuarentena, estar infectado y que un ser querido recibiera el diagnóstico. Las descripciones de los participantes estadounidenses de sus peores experiencias estaban más relacionadas con la amenaza a la vida y la pérdida, mientras que los italianos informaron más de la amenaza al mundo, el estrés, el aislamiento social y la sensación de estar atrapados. En el análisis CART, el principal predictor (79,9%) fue la percepción de efectos negativos de la crisis COVID-19. Entre ellos, la experiencia de amenaza a sí mismo relacionada con la COVID fue el predictor más sólido. En su ausencia, estar privado de recursos o experimentar altos niveles de ansiedad fueron otros predictores sólidos.
Conclusiones: El estudio aportó pruebas de la utilidad de un abordaje de métodos mixtos para conceptualizar las experiencias asociadas a la pandemia de COVID-19 y el riesgo de síntomas traumáticos. Sus hallazgos pueden servir de base a las intervenciones y políticas sanitarias para afrontar los nuevos retos que plantea la pandemia de COVID-19.
背景: 尽管创伤后应激障碍 (PTSD) 的症状与 COVID-19 疫情经历有关,但尚无研究探讨特定 COVID-19 叙述与创伤后精神痛苦(创伤后应激障碍的前兆)之间的关联。
目的: 探讨在 COVID-19 疫情第一波期间与创伤后精神痛苦相关的最糟糕经历。
方法: 来自美国 (n = 741) 和意大利 (n = 357) 的成年居民 (N = 1098) 完成了一项在线调查,包括社会人口数据、COVID-19 相关经历、创伤后精神痛苦清单和一个关于他们在 COVID-19 疫情第一阶段(2020 年 4 月至 5 月)最糟糕经历的开放式问题。对开放式问题的答案进行了主题内容分析 (TCA),并使用分类和回归树 (CART) 分析来确定最能预测创伤后精神痛苦临床水平的主题。
结果: 与参与者最糟糕的 COVID-19 经历相关的主要 TCA 主题是焦虑、威胁、丧失、愤怒、压力和压迫。威胁是最普遍的主题,并且与被隔离、被感染和亲人接受诊断等经历相关。美国参与者对他们最糟糕经历的描述更多与生命威胁和丧失有关,而意大利人则报告了更多世界的威胁、压力、社会隔离和感到被困住。在 CART 分析中,主要预测因素 (79.9%) 是感知到 COVID-19 危机的负面影响。其中自我经历的COVID 相关威胁是最有力的预测因素。在没有它的情况下,被剥夺资源或经历高度焦虑是其他强有力的预测因素。
结论: 该研究提供了混合方法在概念化与 COVID-19 疫情和创伤症状风险相关的经历方面有效性的证据。其研究结果可能会为应对 COVID-19 疫情带来的新挑战的医疗干预措施和政策提供信息。
1. Introduction
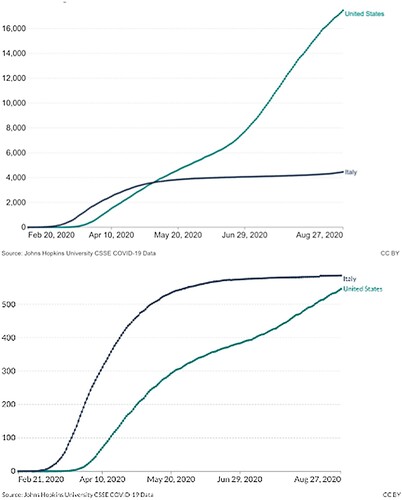
The coronavirus disease 2019 (COVID-19) was first detected in December 2019 in Wuhan (China) and was defined in March 2020 by the World Health Organization as a global pandemic, a decision that urged governments to establish infection control measures such as social distancing, hygiene practices and lockdowns. As of the beginning of May 2020, more than 3.5 million cases of COVID-19 were confirmed worldwide, with almost 250,000 deaths being reported, figures steadily increasing in some countries (Hu et al., Citation2020). The USA and Italy were among the most severely impacted countries, although they differed by the evolution of cases, how the pandemic was managed by their governments, and how they faced the first wave of the COVID-19 pandemic. The cumulative number of new confirmed cases per million people between 19 April and 26 May 2020, when this study was conducted, in the US (2266.84–4988.76) became higher than in Italy (3021.12–3891.86) and the number of deaths remained lower (US 127.40–303.92 vs Italy 399.39–556.29) (John Hopkins University, Citation2020), but the limited testing in US and the subsequent changes in cumulative numbers should also be taken into account (see ). From May, these numbers remained stable in Italy whereas they increased in the USA. This might also be attributed to the different measures adopted to contain the contagion. Italy was in a complete lockdown from 8 March to 3 May and kept very strict anti-contagion measures after May whereas USA only started to shut down activities and schools and to introduce social distancing measures from mid-March to the end of April.
Figure 1. Cumulative number of new confirmed cases (top) and deaths (bottom) per million people in the US and Italy during the first wave of COVID-19 pandemic.
Although human society had been confronted with various forms of infectious diseases from the earliest days, it can be said that it has never before, on such a global level, been faced with restrictions that fundamentally changed their everyday lives and social relationships (Hu et al., Citation2020). The pandemic was associated with an increase in anxiety, depression, and trauma- and stress-related symptoms (Brunet et al., Citation2022; Liu et al., Citation2020), that are estimated will be long lasting and far more intense than those experienced with previous pandemics (Boyraz & Legros, Citation2020).
A number of authors have described extremely high rates of self-reported symptoms of posttraumatic stress disorder (PTSD) in the general population (Bo et al., Citation2020; Sun et al., Citation2020) during the pandemic and in specific groups such as people hospitalized due to COVID-19 (Boyraz & Legros, Citation2020) and among those exposed to continuous and intense stress such as healthcare workers (Blekas et al., Citation2020), especially those working directly with COVID-19 patients (Yin et al., Citation2020). This is also the case for those close to individuals infected by the virus (Sun et al., Citation2020) and those who experienced the unexpected death of a loved one due to COVID-19 together with the impossibility to attend the funeral (Boyraz & Legros, Citation2020; Cipolletta, Andreghetti, et al., Citation2022). There were also favourable life changes (e.g. more frequent physical exercise, increased fruit and vegetable intake) (Hu et al., Citation2020), and instances of people who were not distressed or even experienced positive psychological changes due to lifestyle adjustments, social support and meaning making (Brülhart et al., Citation2021; Lu et al., Citation2022; Todorova et al., Citation2021).
In addition to the factors explored in the above-mentioned studies, no study has yet attempted to understand how personal meanings attributed to crises may be relevant to understand peritraumatic distress symptoms, a more proximal measure of distress than PTSD symptoms, and one of its most robust predictors according to meta-analytic work (e.g. Thomas et al., Citation2012). A useful framework to understand these meanings is personal construct theory (PCT), which was first introduced by George Kelly (Citation1955). Kelly (Citation1955) identifies some transitions, which are diagnostic constructs used to define the meanings that people give to changes in their own construct systems. Three of these transitions that may be of particular relevance to a situation of major change such as a pandemic are anxiety, threat, and guilt. Anxiety essentially involves an inability to anticipate events, since they are ‘outside the range of convenience’ of the person’s construct system. Threat is the awareness of an imminent comprehensive change to core structures, those central to one’s identity, and guilt is defined as dislodgement from one’s core role, one’s characteristic way of being. Transitions have been used to understand the illness experience (Cipolletta et al., Citation2017; Citation2020) and the present pandemic (Cipolletta & Ortu, Citation2020; Tomaino et al., Citation2021; Winter et al., Citation2022; Winter & Reed, Citation2021) but not peritraumatic distress.
1.1. Study aim and questions
The aim of this study was to explore US and Italian participants’ narratives of their worst experiences during the first wave of the COVID-19 pandemic and analyse the association between these narratives and peritraumatic distress symptoms by combining qualitative and quantitative data. More specifically, the research questions were: What were the prevalent negative experiences during the first period of the COVID-19 outbreak? How can they be understood in terms of PCT and of Kellian transitions in particular? How are they associated with such events as COVID-19 tests, diagnosis, and being quarantined? Which of these experiences are associated with clinically significant levels of peritraumatic distress symptoms? Were there differences between US and Italian people’s experiences and levels of peritraumatic distress?
2. Method
2.1. Participants and procedure
A convenience sample of 1098 respondents from the US (N = 741) and Italy (N = 357) took part in a cross-sectional web-based survey on the psychosocial effects of COVID-19. They were primarily Caucasians who identified as women with a mean age of 42.80 years (SD = 16.09). provides detailed demographic and clinical information.
Table 1. Demographic and clinical information.
Participants were recruited through snowball sampling. Emails were sent to various associations and advertisements were placed on social media (i.e. Facebook, Twitter) to involve different populations (students, healthcare professionals and general population) and reach as many people as possible. Since the main purpose of the study was a quantitative one, the criterion of convenience was dominant in the choice of sampling procedure: a more appropriate procedure for qualitative research such as theoretical sampling could not be used because the qualitative analysis of data started only after all data were collected and the criterion of theoretical saturation could not be applied.
Ethics approval for the research project was obtained from the Douglas Mental Health University Institute, Montreal, Canada (#IUSMD-20-13). The survey was hosted on SurveyMonkey and administered between 19 April and 26 May 2020. The methodology of this survey has been further described elsewhere (see Brunet et al., Citation2022). Potential participants opening the survey link were directed to an informed consent form and completed the 15-minute survey in one sitting.
2.2. Measures
The survey measures included:
– socio-demographic data;
– COVID-19-related experiences (having been tested for or diagnosed with COVID-19 and experiences of social isolation or quarantine);
– an open question asking participants to describe their worst experience with the COVID-19 crisis;
– the Peritraumatic Distress Inventory (PDI; Brunet et al., Citation2001; Carmassi et al., Citation2021). The PDI assesses life-threat and other physical and emotional immediate responses (e.g. fear, helplessness, and horror) experienced with respect to an index event, in this case, the most difficult event occurring during the first period of the pandemic. A cut-off of 14 on its total score, which ranges between 0 (no distress) and 52, represents clinically significant levels of peritraumatic distress likely to elicit symptoms of trauma- and stressor-related disorders (Guardia et al., Citation2013), such as adjustment disorder or posttraumatic stress disorder (PTSD).
2.3. Analysis
A mixed-method approach was used to combine quantitative and qualitative measures by following a sequential approach to quantify the qualitative data and connect them to the quantitative data derived by the socio-demographic measures and PDI. To this aim a thematic content analysis (TCA, Vaismoradi et al., Citation2013) was employed, proceeding in two steps. The first step was the thematic analysis that combined an inductive and deductive approach: each response to the open question was inductively categorized in terms of one or more codes that were then grouped in themes and deductively viewed in terms of the diagnostic constructs of PCT. This process led to the creation of a codebook, which was applied to all the responses. The second step was quantitative: the subthemes were given a code one or zero, according to the presence or absence of each one. The count of the frequency of theme presence led to the quantification of the themes. Two coders independently conducted the analysis on the Italian dataset and two on the US dataset. Disagreements between them were resolved by discussion and through reference to a third researcher (the same for the two datasets), who helped to refine codes and create a common dataset.
Less than 5% of the quantitative data were missing. Little’s (Citation1988) MCAR test suggested that the data were missing at random (χ2 = 15,480.5, df = 13,558, p < .001). Data were therefore imputed using the k-Nearest-Neighbour imputation method with k = 5 in the VIM package for the statistical software R (Kowarik & Templ, Citation2016). All other analyses were performed using SPSS v23 (IBM Corp., Armonk, NY). All tests were two-tailed and used an alpha level of .05.
Descriptive analyses, ANOVAs, chi-squares and correlations were conducted on the socio-demographic data and to compare them with the major themes identified by the TCA of participants’ narratives of their worst COVID-related experiences and PDI data. A classification and regression tree (CART; Breiman et al., Citation1984) analysis was used to identify the themes that better predicted clinically significant peritraumatic distress derived by the PDI data dichotomized using the cut-off score. CART analysis uses recursive partitioning to split populations into mutually exclusive subgroups and uncover complex interactions, not easily discoverable with traditional regression methods, in addition to considering the importance of each independent variable in isolation to the model (Breiman et al., Citation1984; Lemon et al., Citation2003). The CART procedure yields a classification tree by progressively splitting in two the sample until no further splits improve classification. The minimum number of cases required in the intermediary node and in the terminal node was set to 50 people (approximately 5% of the sample) and 30, respectively. Splitting stopped when the Gini improvement score was <.001 (Lemon et al., Citation2003). To assess the model’s stability, the data were divided into 10 subsets and the classification, produced with 90% of the data, was applied to the remaining 10%.
3. Results
In this section, the results of the qualitative analysis will be briefly presented (a more extensive presentation of the qualitative analysis of US data can be found in Winter et al., Citation2022) followed by a more extensive presentation of the quantitative analysis of the qualitative and quantitative data.
3.1. Qualitative analysis
The themes and codes derived by the TCA of participants’ narratives of their worst experiences will be reported with illustrative quotations from US or Italian participants identified by US or I, a numeric code, gender (M, F) and age. Some of the themes and subthemes (anxiety, threat, guilt and constriction) refer to transitions as defined within the PCT perspective, others (loss experienced by the self or other, anger, stress, absence of negative effects, positive effects and coping strategies) are more descriptive of participants’ experiences in their own terms.
3.1.1. Anxiety
Anxiety refers to statements about uncertainty and the difficulty to understand what is going on: ‘It has been the uncertainty for the future that worried me the most: not to know how things would have gone’ (I_960, F, 26); ‘Sometimes my anxiety makes it hard to breathe. Hard to move. I just took a nap that was LONG. Maybe/probably too long. Getting up, I felt like I had been drugged. Like I didn't know what time it was. Unmoored’ (US_666, F, 53).
3.1.2. Threat
This category was applied to statements involving major concerns about the possible death or illness of oneself or significant others: ‘My best friend telling me that her dad and her brother had gotten COVID-19. That was the moment when I realized it had reached personal circles and that the threat was pretty big’ (US_563, F, 21).
Some participants described a broader sense of threat involving a dismantling of their fundamental and trusted ways of seeing the world: ‘Fear, fear of the future and of not going back to normality or to what I used to call so before’ (I_990, F, 29).
3.1.3. Loss
This category was applied to statements concerning experiences of not carrying out one’s expected role or not behaving in accordance with how one characteristically sees oneself (guilt) or is seen by others (shame), ‘The worst experience was when I saw vanishing all my projects for the next months, personal ones, work ones, educational ones … Everything’ (I_961, F, 27); ‘I felt shame afterward. This was my lowest moment – that I reacted not with compassion and solidarity’ (US_315, F, 41).
It also includes statements indicating that the person is helpless or powerless, as reported by a nurse who felt a loss in her helping role: ‘Seeing all those people in the medical unit dying and being unable to do anything to save them’ (I_995, F, 24).
Finally, this category is applied to statements concerning the emotional effects of losses experienced by the self or others: ‘Losing two friends, another two in the hospital. Another one is self-quarantine’ (US_15, F, 70) and ‘Hearing about young friends of friends in the intensive care unit dying’ (US_716, 7, 58).
3.1.4. Anger
This category was applied to statements concerning anger with the government and anger or interpersonal conflict with other people: ‘People around us are dying and we feel betrayed and abandoned by institutions (especially regional ones) that should have protected us instead’ (I_895, M, 42); ‘anger about an elderly friend who died and wasn’t able to have family visit or even attend her funeral’ (US_442, F, 45).
3.1.5. Stress
This category refers to statements concerning general stress, due to an accumulation of pressure and invalidation; exposure to potentially threatening information or events; or forms, or symptoms, of psychological distress (e.g. panic attacks; generalized anxiety; depression; suicidal ideation; alcohol abuse; sleep disturbance; concentration or memory difficulties; emotional liability; exhaustion; traumatic memories) that are not covered by other categories: ‘I had anxiety attacks and palpitations for a week, probably due to the stress of quarantine’ (I_915, M, 31). In this quotation, as in similar ones, no specific transition in PCT terms could be inferred, thereby the more descriptive category of stress was applied.
3.1.6. Constriction
Constriction refers to people’s narrowing of their worlds that has resulted from ‘lockdown’ restrictions. The subtheme of social isolation is applied to statements concerning the person’s isolation from other people in general or from significant others: ‘[…] during isolation while living alone in the epicenter of New York City with family on the other coast and no access to physical touch support like a hug which is what I needed most’ (US_516, F, 30).
The subtheme of deprivation of other resources refers to statements concerning the person being deprived of particular resources or activities: ‘I had to assist my father at the hospital and I had to help my mother, who has a disability, exactly in this period, without receiving any help from my brothers, especially from one that decided to interrupt all contact for precaution’ (I_823, F, 45).
Being trapped in an intolerable situation concerns experiences of feeling stuck in a difficult or intolerable environment because of lockdown: ‘My room in which I have always lived for more than two months has now become my prison’ (I_1053, F, 21); ‘My worst experiences involve me feeling trapped at home with my family’ (US_406, F, 24).
3.1.7. Absence of negative effects
This theme is applied to any statements that for the individual there have been no bad effects of the pandemic: ‘I have been lucky to be quite sheltered from actual experiences with COVID-19’ (US337, M, 47); ‘Honestly, I had no problems. I have always been at ease and I had no emotional problems or similar ones’ (I_840, M, 18).
3.1.8. Positive effects
Some participants described the positive effects of the lockdown, and the sense of certainty which it entailed: ‘The shelter in place provided clarity, rules, and a new routine, and was in some ways a relief’ (US_663, F, 27); ‘Isolation made me crave to do things that in the past seemed ordinary to me, simple things’ (I_995, F, 73).
3.1.9. Coping strategies
Coping strategies refer to ways in which the person has coped with the crisis and its associated invalidations: ‘worrying about these anxieties was a coping mechanism to avoid worrying about my stress surrounding COVID’ (US_242, F, 25); ‘I look at the positive side’ (I_880, F, 33).
3.2. Quantitative analysis
3.2.1. Prevalence of the variables and associations between them
Threat was the prevalent theme, followed by constriction, stress, loss and anxiety. Only a few participants reported no negative effects or even positive experiences. The frequencies of each theme are reported in .
Table 2. Frequency of themes endorsed in the worst experiences narratives and comparison by country.
A total of 859 participants (78.2%) reported peritraumatic distress levels above the clinical cut-off score in reaction to their worst COVID-related event, identifying a large proportion of our sample as being potentially at risk of current or later trauma- and stressor-related disorder. A one-way ANOVA suggested that there is a statistically significant difference in PDI total score across gender, F(3, 1094) = 29.75, p < .001. More specifically, male participants reported significantly lower levels of peritraumatic distress than female or prefer not to disclose/other (respectively M = 17.89, SD = 9.78, M = 23.13, SD = 9.93, and M = 24.96, SD = 8.29). Moreover, PDI scores significantly correlated with age (r = −.21, p < .001). No other significant associations between PDI and demographics were found. As regards COVID-related experiences, PDI scores significantly correlated with being separated from loved ones (rpbis = .18, p < .001), being quarantined (rpbis = .13, p < .001), being confined (rpbis = .11, p < .001), being diagnosed with COVID-19 (rpbis = .11, p < .001), a loved one being diagnosed with COVID-19 (rpbis = .11, p <.001), and having lost a loved one (rpbis = .12, p = .002).
Finally, there was a statistically significant difference in total scores on PDI between countries of residence, t(1096) = 4.80, p < .001, with higher levels of peritraumatic distress in US than in Italian residents (respectively, M = 23.13, SD = 10.18 and M = 20.04, SD = 9.68). As reported in , US residents’ descriptions of their worst experiences also indicated more threat to self and others and loss of others, while Italian residents’ descriptions indicated more threat to the world, stress, social isolation and being trapped.
Other significant associations were found between some themes and participants’ age, marital status, education and occupation: age negatively correlated with anxiety (r = −.10, p = .001), constriction (r = −.08, p = .009) and loss (r = −.07, p = .020). Constriction was associated with marital status, χ²(3, N = 1098) = 10.75, p = .013, with endorsement in 32.9% of single participants, 25% of separated/widowed participants, 39.3% of people dating, and 27% of married people. Additionally, threat was statistically significantly associated with education and occupation respectively, χ²(2, N = 1098) = 26.10, p < .001, and χ²(3, N = 1098) = 11.41, p = .010. Threat was endorsed in 21.7% of individuals with seven years or less of education (pre-university) compared to 37.7% of individuals with an undergraduate level of education and 46.1% of individuals with a graduate level of education. Regarding occupation, threat was endorsed by 51.6% of healthcare workers, 40.4% of the general employees (other categories than healthcare), 35.1% of the unemployed, and 44.3% of other employment status. There was no significant association between any of the themes and gender. The most relevant associations between the themes and COVID-related experiences were the following: threat was positively correlated with being quarantined (phi = .08, p = .007), being tested for COVID-19 (phi = .11, p < .001), a loved one being tested (phi = .10, p < .001), being diagnosed with COVID-19 (phi = .09, p = .002), and a loved one receiving the diagnosis (phi = .12, p < .001). The main association of the loss theme was with the experience of having lost a loved one (phi = .092, p = .002). Constriction was positively correlated with separation from loved ones (phi = .09, p = .003).
3.2.2. Experience determinants of peritraumatic distress
The overall classification prediction accuracy achieved by the CART analysis was 79.9%. Similar classification accuracy was obtained when variables appearing on the final tree model were fitted in a binary logistic regression model. There was only 1% increase in risk estimate (i.e. 21%) in the validation model using 10-fold cross-validation, suggesting that the model produced was stable. The independent variables included in the model were anxiety, threat to self, threat to others, threat to world, guilt, helplessness, loss experienced by self, loss experienced by others, anger, stress, social isolation, deprivation of other resources, being trapped in an intolerable situation, no negative effect experienced, coping strategies and positive experiences.
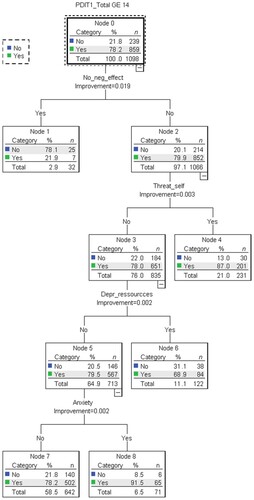
The CART analysis revealed the importance of specific TCA variables. As shown in , the perceived negative effects of the COVID-19 crisis were the strongest predictor of clinically elevated peritraumatic distress (node 2, 852 of 1066, or 79.9%). This group was further split according to whether one experienced a personal life-threat, with a ‘yes’ response improving the predicting power to 87% (node 4). In the absence of a life-threat, elevated peritraumatic distress was predicted by reporting resource deprivation (node 6, 68.9%), or else by endorsing a narrative of anxiety (node 8, 91.5%).
Figure 2. Classification and regression tree (CART) analysis of COVID-19 experiences predicting clinically significant levels of peritraumatic distress.
4. Discussion
The aim of this study was to analyse narratives about the worst experiences of the US and Italian population during the first wave of the COVID-19 pandemic and relate them to the probability of endorsing clinically elevated peritraumatic distress symptoms, the precursor of trauma- and stressor-related symptoms.
The results showed that the descriptions of worst experiences in terms of the negative effects of the pandemic, life-threat, deprivation of resources and anxiety were prevalent in those experiencing elevated peritraumatic distress. Threat was also the prevalent transition among participants and was associated with their worst experience. In PCT terms threat is represented by experiences that endanger one’s identity, certainties and values (Kelly, Citation1955) and one of the main reasons why the COVID-19 pandemic represented a threat was because it exposed people and their significant others to the risk of death, thus promoting PTSD-like symptomatology (Dutheil et al., Citation2021). In line with the DSM-5 definition of trauma as ‘the exposure to actual or threatened death, serious injury, or sexual violence’ (American Psychiatric Association, Citation2013, p. 271), in PCT formulation a traumatic experience implies the exposure to events – such as death and serious injuries – that are outside the realm of usual human experience (Sewell, Citation2003). Not surprisingly, threat was associated with being (or a loved one being) tested for or diagnosed with COVID-19.
Moreover, among the different occupations, healthcare workers were those who reported more narratives of threatening events, probably due to the frequent exposure to their own or others’ potential death (González-Gil et al., Citation2021; Gorini et al., Citation2020; Puci et al., Citation2020). Indeed, it has been documented that the healthcare workers represent a particularly at-risk group, given the inadequacy of protection despite their high level of exposure (Brophy et al., Citation2021), which could add further distress regarding the risks of infection they themselves, and their loved ones, face. The concern of being infected while working was found also among other workers who had a job outside home (Mansilla Dominguez et al., Citation2020). However, healthcare workers are also subject to stigmatization during the pandemic, such as being avoided and feared by the population, due to their high level of exposure to the virus and fear of contamination (Taylor et al., Citation2020). The social isolation created by the stigmatization, along with increased exposure to the virus without proper protective equipment, could create precarious situations in which healthcare workers are faced with potentially life-threatening situations without obtaining the social support that they require, thus putting them at higher risks for developing trauma- and stressor-related symptoms. Threat also was more frequent in more educated participants, which might be explained in terms of a higher COVID-19 awareness (Ciancio et al., Citation2020; Cipolletta, Entilli, et al., Citation2022; Ding et al., Citation2020; Kabito et al., Citation2020; Wise et al., Citation2020).
Participants also described their worst experiences in terms of anxiety. Kelly (Citation1955) defined the transition of anxiety as a situation in which an event – usually experienced as unknown or unprecedented – cannot be construed within an individual’s personal system of constructs. As pandemics fortunately are not events typical of Western people’s life experience, it is not difficult to think that reacting to a virus might be beyond our usual system of constructions. Thus, the pandemic provoked anxiety, especially in its first months, when many aspects of it were unknown and difficult to construe (and still are at the time of writing), including such questions as: When will herd immunity be achieved? Will the vaccine work effectively? How much will the virus mutate? The results of the present study do not show relevant associations of anxiety with the demographic variables apart from age, that was lower in participants who reported experiences described in terms of anxiety, as already pointed out by previous studies (Germani et al., Citation2020).
Another prevalent narrative dealt with loss on the part of oneself or others but also with a loss of personal role (guilt) or a general sense of helplessness. Many participants experiencing guilt felt that the pandemic had stolen their plans and future and that they could not recognize themselves. For example, healthcare workers felt that they could not help others or save people as they were used to doing. Indeed, healthcare workers were recognized at higher risk to develop psychopathological disorders such as adjustment disorder, PTSD, severe depression, and substance abuse (Brooks et al., Citation2020). The results of the present study do not find the same association between peritraumatic distress and occupation but found that peritraumatic distress was more frequent among those who had lost a loved one by COVID-19.
Constriction was the main transition experienced in terms of the social isolation and deprivation of resources that lockdown implied and correlated with the experience of being separated from participants’ loved ones. Not surprisingly, those who experienced more constriction were single/separated/widowed or dating people. Moreover, the deprivation of resources predicted peritraumatic distress. The lockdown and general restrictions imposed to limit the infection produced for many participants the forced experience of a confined interpersonal space, that was reported as lonely and imprisoning, with a negative impact on psychological wellbeing (Boyraz & Legros, Citation2020; Brooks et al., Citation2020).
These data might explain some differences between the US and the Italian sample in this study: peritraumatic distress symptoms and the experience of threat were higher in the US population whereas threat to the world, stress, and social isolation were higher in the Italian population. At the time the present study was conducted (April–May 2020), Italy had already imposed very strict anti-contagion measures and lockdown that probably generated more boredom; compared to the USA, where people kept going to work and were more exposed (Milman et al., Citation2020), thus experiencing especially a life-threat towards self and others.
The weak correlations of the demographic variables and the COVID-related experiences with peritraumatic distress and the themes identified in participants’ descriptions of their worst experiences suggest that the meanings (as described by the themes) given to specific conditions (e.g. being married or a healthcare worker) or experiences (e.g. being tested or diagnosed) may vary from one person to another and that trauma-related symptoms may be better understood in terms of the personal meanings of these experiences than in terms of ‘objective variables’ (Sewell, Citation2003).
4.1. Limitations
The main limitation of the present study is its cross-sectional nature. Symptoms reported by participants could have been generated by the pandemic or have pre-existed in the individuals as risk factors (DiGangi et al., Citation2013) that were able to enhance the negative response to the pandemic and vulnerability to the development of PTSD. Nevertheless, the exploration of personal narratives allows us to overcome this limitation and focus on the narratives currently associated to trauma-related symptoms. However, only a longitudinal study might assess the association between the identified transitions and trauma-related symptoms in the long term.
Another limitation of the present study is the method of data collection. Since the main aim of the study was to collect as much data as possible in a short time and in the pandemic situation when it was particularly difficult to reach people in person, data were collected online through snowball sampling, favouring a quantitative procedure of sampling at the expense of a qualitative one. This choice prevented the authors from reaching a more thorough and comprehensive understanding of participants’ experiences. Moreover, an online survey together with convenience sampling presents the risk of collecting data from a limited part of the population. The authors tried to overcome this limitation by spreading the survey through a variety of channels (e.g. media advertisements) in order to reach as many different people as possible. Nonetheless, the respondents were primarily Caucasian, female and well-educated. Future studies might test the results of the present study through a more controlled procedure of data collection (e.g. an epidemiological sample) that might either consist in a more randomized administration of the survey or its integration with data collected face-to-face, maybe through semi-structured interviews to deepen the qualitative data.
5. Conclusions
The present study used a mixed-method approach to the conceptualization of experiences associated with the COVID-19 pandemic and the risk of symptoms of peritraumatic distress. The narratives reported by our participants are important resources to contextualize and enrich quantitative data and understand the personal determinants of peritraumatic distress symptoms. The early detection of those symptoms, together with the understanding of the personal experiences associated with them, is fundamental to the ability to respond with personalized interventions focusing on risks and protective factors (Brooks et al., Citation2020; Shah et al., Citation2020) and to prevent the long-term effects of the pandemic. Even though differences between Italy and the USA have been underlined, results are in line with previous studies in pointing out the need to detect situations of COVID-19 yielding trauma and stressor-related symptoms to address them appropriately, by orienting healthcare interventions and policies for tackling the new challenges posed by the COVID-19 pandemic.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
- Blekas, A., Voitsidis, P., Athanasiadou, M., Parlapani, E., Chatzigeorgiou, A. F., Skoupra, M., Syngelakis, M., Holeva, V., & Diakogiannis, I. (2020). COVID-19: PTSD symptoms in Greek health care professionals. Psychological Trauma: Theory, Research, Practice, and Policy, 12(7), 812–819. https://doi.org/10.1037/tra0000914
- Bo, H.-X., Li, W., Wang, Y., Zhang, Q., Cheung, T., Wu, X., & Xiang, Y.-T. (2020). Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychological Medicine, 51(6), 1052–1053. https://doi.org/10.1017/S0033291720000999
- Boyraz, G., & Legros, D. N. (2020). Coronavirus disease (COVID-19) and traumatic stress: Probable risk factors and correlates of posttraumatic stress disorder. Journal of Loss and Trauma, 25(6-7), 503–522. https://doi.org/10.1080/15325024.2020.1763556
- Breiman, L., Friedman, J., Stone, C. J., & Olshen, R. A. (1984). Classification and regression trees. CRC press.
- Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. https://doi.org/10.1016/S0140-6736(20)30460-8
- Brophy, J. T., Keith, M. M., Hurley, M., & McArthur, J. E. (2021). Sacrificed: Ontario heaelthcare workers in the time of COVID-19. NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy, 30(4), 267–281. https://doi.org/10.1177/1048291120974358
- Brunet, A., Rivest-Beauregard, M., Lonergan, M., Cipolletta, S., Rasmussen, A., Meng, X., Jaafari, N., Romero, S., Superka, J., Brown, A. D., & Sapkota, R. P. (2022). PTSD is not the emblematic disorder of the COVID-19 pandemic; adjustment disorder is. BMC Psychiatry, 22(1), 300. https://doi.org/10.1186/s12888-022-03903-5
- Brunet, A., Weiss, D. S., Metzler, T. J., Best, S. R., Neylan, T. C., Rogers, C., Fagan, J., & Marmar, C. R. (2001). The peritraumatic distress inventory: A proposed measure of PTSD criterion A2. The American Journal of Psychiatry, 158(9), 1480–1485. https://doi.org/10.1176/appi.ajp.158.9.1480
- Brülhart, M., Klotzbücher, V., Lalive, R., & Reich, S. (2021). Mental health concerns during the COVID-19 pandemic as revealed by helpline calls. Nature, 600(7887), 121–126. https://doi.org/10.1038/s41586-021-04099-6
- Carmassi, C., Bui, E., Bertelloni, C. A., Dell’Oste, V., Pedrinelli, V., Corsi, M., Baldanzi, S., Cristaudo, A., Dell’Osso, L., & Buselli, R. (2021). Validation of the Italian version of the peritraumatic distress inventory: Validity, reliability and factor analysis in a sample of healthcare workers. European Journal of Psychotraumatology, 12(1), 1. https://doi.org/10.1080/20008198.2021.1879552
- Ciancio, A., Kampfen, F., Kohler, I., Bennett, D., de Bruin, W. B., Darling, J., Kapteyn, A., Maurer, J., & Kohler, H.-P. (2020). Know your epidemic, know your response: Early perceptions of COVID-19 and self-reported social distancing in the United States. PLoS One, 15(9), e0238341. https://doi.org/10.1371/journal.pone.0238341
- Cipolletta, S. (2020). Understanding illness experience from the perspective and practice of personal construct psychology. Journal of Constructivist Psychology, 35(4), 1140–1153. https://doi.org/10.1080/10720537.2020.1805072
- Cipolletta, S., Andreghetti, G. R., & Mioni, G. (2022). Risk perception towards COVID-19: A systematic review and qualitative synthesis. International Journal of Environmental Research and Public Health, 19(8), 8. https://doi.org/10.3390/ijerph19084649
- Cipolletta, S., Entilli, L., & Filisetti, S. (2022). Uncertainty, shock and anger: Recent loss experiences of first-wave COVID-19 pandemic in Italy. Journal of Community and Applied Social Psychology, 32, 983–997. https://doi.org/10.1002/casp.2604
- Cipolletta, S., Gammino, G. R., & Palmieri, A. (2017). Illness trajectories in patients with amyotrophic lateral sclerosis: How illness progression is related to life narratives and interpersonal relationships. Journal of Clinical Nursing, 26(23-24), 5033–5043. https://doi.org/10.1111/jocn.14003
- Cipolletta, S., & Ortu, M. C. (2020). COVID-19: Common constructions of the pandemic and their implications. Journal of Constructivist Psychology, 34(3), 278–294. https://doi.org/10.1080/10720537.2020.1818653
- DiGangi, J. A., Gomez, D., Mendoza, L., Jason, L. A., Keys, C. B., & Koenen, K. C. (2013). Pretrauma risk factors for posttraumatic stress disorder: A systematic review of the literature. Clinical Psychology Review, 33(6), 728–744. https://doi.org/10.1016/j.cpr.2013.05.002
- Ding, Y., Xu, J., Huang, S., Li, P., Lu, C., & Xie, S. (2020). Risk perception and depression in public health crises: Evidence from the COVID-19 crisis in China. International Journal of Environmental Research and Public Health, 17(16), 5728. https://doi.org/10.3390/ijerph17165728
- Dutheil, F., Mondillon, L., & Navel, V. (2021). PTSD as the second tsunami of the SARS-Cov-2 pandemic. Psychological Medicine, 51(10), 1773–1774. https://doi.org/10.1017/S0033291720001336
- Germani, A., Buratta, L., Delvecchio, E., Gizzi, G., & Mazzeschi, C. (2020). Anxiety severity, perceived risk of COVID-19 and individual functioning in emerging adults facing the pandemic. Frontiers in Psychology, 11, 567505. https://doi.org/10.3389/fpsyg.2020.567505
- González-Gil, M. T., González-Blázquez, C., Parro-Moreno, A. I., Pedraz-Marcos, A., Palmar-Santos, A., Otero-García, L., Navarta-Sánchez, M. V., Alcolea-Cosín, M. T., Argüello-López, M. T., Canalejas-Pérez, C., Carrillo-Camacho, M. E., Casillas-Santana, M. L., Díaz-Martínez, M. L., García-González, A., García-Perea, E., Martínez-Marcos, M., Martínez-Martín, M. L., Palazuelos-Puerta, M. D. P., Sellán-Soto, C., & Oter-Quintana, C. (2021). Nurses’ perceptions and demands regarding COVID-19 care delivery in critical care units and hospital emergency services. Intensive and Critical Care Nursing, 62, Article 102966. https://doi.org/10.1016/j.iccn.2020.102966
- Gorini, A., Fiabane, E., Sommaruga, M., Barbieri, S., Sottotetti, F., La Rovere, M. T., Tremoli, E., & Gabanelli, P. (2020). Mental health and risk perception among Italian healthcare workers during the second month of the covid-19 pandemic. Archives of Psychiatric Nursing, 34(6), 537–544. https://doi.org/10.1016/j.apnu.2020.10.007
- Guardia, D., Brunet, A., Duhamel, A., Ducrocq, F., Demarty, A. L., & Vaiva, G. (2013). Prediction of trauma-related disorders: A proposed cutoff score for the peritraumatic distress inventory. The Primary Care Companion for CNS Disorders, 15(1), PCC.12l01406. https://doi.org/10.4088/PCC.12l01406
- Hu, Z., Lin, X., Chiwanda Kaminga, A., & Xu, H. (2020). The impact of coronavirus disease (COVID-19) epidemic on lifestyle behaviors and their association with subjective wellbeing among the general population in the Mainland China: A cross-sectional study. Journal of Medical Internet Research, 22(8), e21176. https://doi.org/10.2196/21176
- John Hopkins University. (2020). Mortality analyses. Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/data/mortality
- Kabito, G. G., Alemayehu, M., Mekonnen, T. H., Wami, S. D., Azanaw, J., Adane, T., Azene, Z. N., Merid, M. W., Muluneh, A. G., Geberu, D. M., Kassa, G. M., Yenit, M. K., Tilahun, S. Y., Gelaye, K. A., Mekonnen, H. S., Azagew, A. W., Wubneh, C. A., Belay, G. M., Assimamaw, N. T., … Gashaye, K. T. (2020). Community’s perceived high risk of coronavirus infections during early phase of epidemics are significantly influenced by socio-demographic background, in Gondar City, Northwest Ethiopia: A cross-sectional-study. PLoS One, 15(11), e0242654. https://doi.org/10.1371/journal.pone.0242654
- Kelly, G. A. (1955). The psychology of personal constructs (Vols. 1-2). W. W. Norton.
- Kowarik, A., & Templ, M. (2016). Imputation with the R package VIM. Journal of Statistical Software, 74(7), 1–16. https://doi.org/10.18637/jss.v074.i07
- Lemon, S. C., Roym, J., Clark, M. A., Friedmann, P. D., & Radowski, W. (2003). Classification and regression tree analysis in public health: Methodological review and comparison with logistic regression. Annals of Behavioral Medicine, 26(3), 172–181. https://doi.org/10.1207/S15324796ABM2603_02
- Little, R. J. (1988). A test of missing completely at random for multuvariate data with missing values. Journal of American Statistical Association, 83(404), 1198–1202. https://doi.org/10.1080/01621459.1988.10478722
- Liu, C. H., Zhang, E., Wong, G. T., Hyun, S., & Hahm, H. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U. S. young adult mental health. Psychiatry Research, 290, 113172. https://doi.org/10.1016/j.psychres.2020
- Lu, L., Contrand, B., Dupuy, M., Ramiz, L., Sztal-Kutas, C., Lagarde, E.. (2022). Mental and physical health among the French population before and during the first and second COVID-19 lockdowns: Latent class trajectory analyses using longitudinal data. Journal of Affective Disorders, 309, 95–104. https://doi.org/10.1016/j.jad.2022.04.095
- Mansilla Dominguez, J. M., Font Jimenez, I., Belzunegui Eraso, A., Pena Otero, D., Diaz Perez, D., & Recio Vivas, A. M. (2020). Risk perception of COVID-19 community transmission among the Spanish population. International Journal of Environmental Research and Public Health, 17(23), 8967. https://doi.org/10.3390/ijerph17238967
- Milman, E., Lee, S. A., & Neimeyer, R. A. (2020). Social isolation and the mitigation of coronavirus anxiety: The mediating role of meaning. Death Studies, 46(1), 1–13. https://doi.org/10.1080/07481187.2020.1775362
- Puci, M. V., Nosari, G., Loi, F., Puci, G. V., Montomoli, C., & Ferraro, O. E. (2020). Risk perception and worries among health care workers in the COVID-19 pandemic: Findings from an Italian survey. Healthcare, 8(4), 535. https://doi.org/10.3390/healthcare8040535
- Sewell, K. W. (2003). An approach to post-traumatic stress. In F. Fransella (Ed.), International handbook of personal construct psychology (pp. 223–233). John Wiley & Sons.
- Shah, K., Kamrai, D., Mekala, H., Mann, B., Desai, K., & Patel, R. S. (2020). Focus on mental health during the coronavirus (COVID-19) pandemic: Applying learnings from the past outbreaks. Cureus, 12, e7405. https://doi.org/10.7759/cureus.7405
- Sun, L., Sun, Z., Wu, L., Zhu, Z., Zhang, F., Shang, Z., Shang, Z., Jia, Y., Gu, J., Zhou, Y., Wang, Y., Liu, N., & Liu, W. (2020). Prevalence and risk factors of acute posttraumatic stress symptoms during the COVID-19 outbreak in Wuhan, China. Journal of Affective Disorders, 283, 123–129. https://doi.org/10.1016/j.jad.2021.01.050
- Taylor, S., Landry, C. A., Rachor, G. S., Paluszek, M. M., & Asmundson, G. J. (2020). Fear and avoidance of healthcare workers: An important, under-recognized form of stigmatization during the COVID-19 pandemic. Journal of Anxiety Disorders, 75, Article 102289. https://doi.org/10.1016/j.janxdis.2020.102289
- Thomas, É, Saumier, D., & Brunet, A. (2012). Peritraumatic distress and the course of posttraumatic stress disorder symptoms: A meta-analysis. The Canadian Journal of Psychiatry, 57(2), 122–129. https://doi.org/10.1177/070674371205700209
- Todorova, I., Albers, L., Aronson, N., Baban, A., Benyamini, Y., Cipolletta, S., del Rio Carral, M., Huang, Q., John, L., Kaneva, M., Khan, S., Kostova, Z., Kotzeva, T., Fathima, M. A., Dimitrova, E., Dudley, C., Guzzardo, M., Hammoud, R., Fadil Azim, D. H., Hilverda, F., … Zlatarska, A. (2021). “What I thought was so important isn't really that important”: International perspectives on making meaning during the first wave of the COVID-19 pandemic. Health Psychology and Behavioural Medicine, 9(1), 830–857. http://doi.org/10.1080/21642850.2021.1981909
- Tomaino, S. C. M., Cipolletta, S., Kostova, Z., & Todorova, I. (2021). Stories of life during the first wave of the COVID-19 pandemic in Italy: A qualitative study. International Journal of Environmental Research and Public Health, 18(14), 7630. https://doi.org/10.3390/ijerph18147630
- Vaismoradi, M., Turunen, H., & Bondas, T. (2013). Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing & Health Sciences, 15(3), 398–405. https://doi.org/10.1111/nhs.12048
- Winter, D. A., Brunet, A., Rivest-Beauregard, M., Hammoud, R., & Cipolletta, S. (2022). Construing worst experiences of the COVID-19 pandemic in the USA: A thematic analysis. Journal of Constructivist Psychology, https://doi.org/10.1080/10720537.2021.2012544
- Winter, D. A., & Reed, N. (2021). Unprecedented times for many but not for all: Personal construct perspectives on the COVID-19 pandemic. Journal of Constructivist Psychology, 34(3), 254–263. https://doi.org/10.1080/10720537.2020.1791291
- Wise, T., Zbozinek, T. D., Michelini, G., Hagan, C. C., & Mobbs, D. (2020). Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. Royal Society Open Science, 7(9), 200742. https://doi.org/10.1098/rsos.200742
- Yin, Q., Sun, Z., Liu, T., Ni, X., Deng, X., Jia, Y., Shang, Z., Zhou, Y., &Liu, W. (2020). Posttraumatic stress symptoms of health care workers during the corona virus disease 2019. Clinical Psychology and Psychotherapy, 27(3), 384–395. https://doi.org/10.1002/cpp.2477