
ABSTRACT
Aims: In 2018, the 11th version of the International Classification of Diseases (ICD-11) recognized a new diagnosis in addition to Posttraumatic Stress Disorder (PTSD), that of Complex Posttraumatic Stress Disorder (C-PTSD). A new measurement tool was developed to assess both disorders: the International Trauma Questionnaire. The objectives of this study were (a) to conduct a French translation of the tool, (b) to confirm the factorial structure of the tool, (c) to verify its convergent and divergent validity, (d) and finally to ensure its temporal stability.
Method: The ITQ was translated into French using a committee approach, bringing together experts and bilingual individuals with a dual French-English culture. It was then completed by 750 people residing in France and having been exposed to potentially traumatic events, recruited from the general population. Other measures were also completed (HADS, ITEM, PCL-5, WHO-5, DERS).
Results: Confirmatory factor analysis confirmed that the French version of the ITQ had the same factor structure as the original version. The scale showed satisfactory convergent and divergent validity, as well as good stability over time.
Conclusion: Our study suggests that the French version of the ITQ is a good measurement tool for assessing PTSD and C-PTSD according to the ICD-11 diagnostic criteria.
HIGHLIGHTS
This study provides the first translation and validation of the International Trauma Questionnaire in the French population.
Confirmatory factor analysis confirmed that the French version of the ITQ had the same factor structure as the original version.
The French version of the ITQ showed good convergent and divergent validity, as well as good test-retest reliability.
Objetivos: En el 2018, la versión 11.° de la Clasificación Internacional de Enfermedades (CIE-11) reconoció un nuevo diagnóstico además del Trastorno de Estrés Postraumático (TEPT), el de Trastorno de Estrés Postraumático Complejo (TEPT-C). Se desarrolló un instrumento de medición nuevo para evaluar ambos trastornos: el Cuestionario Internacional de Trauma (ITQ, en sus siglas en inglés). Los objetivos de este estudio fueron (a) realizar una traducción al francés del instrumento, (b) confirmar la estructura factorial del instrumento, (c) verificar su validez convergente y divergente, (d) y finalmente asegurar su estabilidad temporal.
Método: El ITQ se tradujo al francés utilizando un enfoque de comité, reuniendo expertos e individuos bilingües con una cultura dual Francesa-Inglesa. Luego fue completado por 750 personas residentes en Francia y que habían estado expuestas a eventos potencialmente traumáticos, reclutados de la población general. También se completaron otras medidas (HADS, ITEM, PCL-5, WHO-5. DERS).
Resultados: El análisis factorial confirmatorio confirmó que la versión francesa del ITQ tenía la misma estructura factorial que la versión original. La escala mostró una validez convergente y divergente satisfactoria, así como una buena estabilidad en el tiempo.
Conclusión: Nuestro estudio sugiere que la versión francesa del ITQ es un buen instrumento de medición para evaluar TEPT y TEPT-C según los criterios diagnósticos de la CIE-11.
目的:2018 年,第 11 版国际疾病分类 (ICD-11) 采纳了除创伤后应激障碍 (PTSD) 外的一种新诊断,即复杂性创伤后应激障碍 (C-PTSD) 。开发了一种新的测量工具来评估这两种疾病:国际创伤问卷。本研究旨在 (a) 对该工具进行法语翻译,(b) 确认其因子结构,(c) 验证其聚合效度和区分效度,(d) 最后确定其时间稳定性。
方法:ITQ 通过汇集具有法英双重文化的专家和双语人士的委员会方法被翻译成法语。然后 750 名从一般人群中招募的居住在法国并曾经历过潜在创伤事件的人填写问卷。还完成了其他测量问卷(HADS、ITEM、PCL-5、WHO-5、DERS)。
结果:验证性因子分析证实,法语版ITQ 与原始版本具有相同的因子结构。该量表表现出令人满意的聚合和区分效度,以及良好的时间稳定性。
结论:我们的研究表明,法语版 ITQ 是根据 ICD-11 诊断标准评估 PTSD 和 C-PTSD 的良好测量工具。
1. Introduction
In 2018, the eleventh version of the International Classification of Diseases (ICD-11) was released (World Health Organization, Citation2018). ICD-11 changes the diagnosis of Post-Traumatic Stress Disorder (PTSD) in a major way, replacing it with two twin diagnoses: PTSD and Complex Post-Traumatic Stress Disorder (C-PTSD). This change address a concern that has been raised by clinicians and researchers for decades (Cloitre et al., Citation2013; Cloitre et al., Citation2018), while also providing some continuity with previous classifications. As Brewin (Citation2020) notes, previous classifications had already attempted to operationalize complex trauma, whether it was the DSM-IV (American Psychiatric Association, Citation1994) with its proposition of ‘Disorder of Extreme Stress Not Otherwise Specified » (DESNOS) or the ICD-10 (WHO, Citation1992) with the diagnosis of ‘Enduring Personality Change After Catastrophic Experience’ (EPCACE). C-PTSD as defined in ICD-11 is a disorder that can occur as a result of exposure to one or more events of an extremely threatening or horrific nature that take place in a prolonged or repetitive manner and from which escape is difficult or impossible (e.g. torture, genocide, prolonged domestic violence, repeated sexual or physical abuse during childhood) (World Health Organization, Citation2018). It has been established in the literature that C-PTSD is generally consequential to events that are interpersonal in nature, i.e. caused by humans rather than nature (e.g. earthquakes, tornadoes, tsunamis) or by accidents (e.g. transportation accidents) (Brewin, Citation2020). In line with DSM-IV’s DESNOS or ICD-10’s EPCACE, the ICD-11’s C-PTSD emphasizes changes in self-organization, but without the personality changes of the EPCACE and with a much smaller number of identified symptoms than the DESNOS.
According to ICD-11, C-PTSD is composed of six symptom clusters (Brewin et al., Citation2017). Three clusters with two symptoms each correspond to PTSD: (1) re-experiencing (i.e. dissociative flashbacks and nightmares), (2) avoidance (i.e. avoidance of external reminders and avoidance of thoughts and feelings associated with the traumatic event), and (3) persistent sense of threat (i.e. hypervigilance, exaggerated startle response). Three other clusters correspond to the complex dimension, named Disturbances in Self-Organization (DSO), with two symptoms each: (4) affective dysregulation (i.e. emotional hyperactivation and/or hypoactivation), (5) negative self-concept (i.e. feeling like a failure or feeling worthless, diminished, defeated, or worthless, with feelings of shame, guilt, or failure), and (6) interpersonal disturbances (i.e. having difficulty maintaining relationships and feeling close to others) (Maercker et al., Citation2013; WHO, Citation2018). The diagnostic guidelines for C-PTSD are summarized in three main points (Brewin, Citation2020). First, the presence of a traumatic event should be noted. The presence of exposure to a stressor typically of an extreme or prolonged nature and from which escape is difficult or impossible such as torture, concentration camps, slavery, genocide campaigns and other forms of organized violence, domestic violence, and childhood sexual or physical abuse is identified as a risk factor. However, it must be remembered that the nature of the trauma is not a diagnostic criterion and C-PTSD can be diagnosed following any traumatic event. Second, symptoms of PTSD are present (i.e. re-experiencing, avoidance of reminders of the trauma, perception of constant threat). Third, symptoms consistent with DSO (i.e. problems with affect regulation, persistent negative beliefs about self, persistent difficulties in developing and maintaining relationships) must be noted. These symptoms could generate persistent and pervasive impairment in one or more spheres of life (i.e. relational, personal, professional), and have been present for at least one month (Cloitre et al., Citation2013; Maercker et al., Citation2013; WHO, Citation2018).
To address the need for a specific measure for the diagnosis of C-PTSD, Cloitre et al. (Citation2018) developed the International Trauma Questionnaire (ITQ). The ITQ is a brief self-administered questionnaire created to assess symptoms of PTSD and C-PTSD, consistent with the ICD-11 nomenclature of maximizing clinical utility and ensuring international applicability (Cloitre et al., Citation2018; First et al., Citation2015). The ITQ includes a ‘PTSD’ scale referencing the three dimensions identified in the ICD-11 (i.e. re-experiencing, avoidance, and feeling constantly threatened), as well as a ‘DSO’ scale referencing the three dimensions of C-PTSD (i.e. affective dysregulation, disruption in relationships, and negative self-concept) (Cloitre et al., Citation2018). In order to develop the ITQ items, Cloitre et al. (Citation2018) relied on the work of Brewin et al. (Citation2009) for the PTSD portion (Redican et al., Citation2021). For the DSO portion, item selection was based on the results of clinical studies using the DSM-IV that examined the most frequently reported symptoms in C-PTSD (Van der Kolk et al., Citation2005), guided by considerable empirical analysis of the performance of a large set of potential items (Cloitre et al., Citation2021; Shevlin et al., Citation2018) as well as results of a survey of experts and clinicians (Cloitre et al., Citation2011; Redican et al., Citation2021).
The original version of the ITQ has proven to be a clinically useful measure with good psychometric properties (Cloitre et al., Citation2018; Citation2021), and numerous translations have been published in Europe (Karatzias et al., Citation2017a; Murphy et al., Citation2020; Somma et al., Citation2019; Vang et al., Citation2021), the Middle East (Cloitre et al., Citation2018; Gilbar et al., Citation2018; Vallières et al., Citation2018), Asia (Ho et al., Citation2019; Citation2020; Mordeno et al., Citation2019), Africa (Owczarek et al., Citation2020), North America (Cloitre et al., Citation2019; Cyr et al., Citation2022) and South America (Donat et al., Citation2019). A recent systematic review of the literature (Redican et al., Citation2021) shows that two models fit the ITQ factor structure correctly. The first, modelled with 2 s-order factors reflecting PTSD and DSO, appears to be more appropriate in studies of highly traumatized individuals recruited in clinical populations. The second, modelled with 6 first-order factors correlated with each other, seems to be more appropriate in studies in the general population. Multiple psychometric studies conducted show good internal consistency of the ITQ (e.g. Cloitre et al., Citation2018; Vang et al., Citation2021). In terms of convergent validity, it has been established that the ITQ score is positively correlated with the number of aversive events experienced (Karatzias et al., Citation2017b; Murphy et al., Citation2020), difficulties in maintaining a coherent sense of self (Cyr et al., Citation2022), or anxiety and depression (Gilbar, Citation2020). Where some symptoms appear to be more associated with PTSD (panic disorder, generalized anxiety disorder), others appear to be more associated with C-PTSD (depression, post-traumatic cognitions, emotion regulation) (Hyland et al., Citation2021b). In terms of divergent validity, the ITQ has been shown to be negatively correlated with quality of life (Cyr et al., Citation2022). Finally, in a recent network analysis of the interconnection between PTSD/DSO and Borderline Personality Disorder (BPD) in polytrauma patients, Owczarek et al. (Citation2022) showed that C-PTSD symptoms as measured by the ITQ were well distinguished from BPD symptoms. Recent studies conducted with the ITQ in the general population have shown cumulative prevalence rates ranging from about 7-12%. For example, the prevalences of PTSD and C-PTSD are respectively 3.4% and 3.8% in the United States (Cloitre et al., Citation2019), 5% and 7.7% in Ireland (Hyland et al., Citation2021b), or 5.1% and 2.7% in Canada (Cyr et al., Citation2022). Where some studies find a higher prevalence of PTSD than C-PTSD (Ben-Ezra et al., Citation2018; Rossi et al., Citation2022), others find the opposite (Møller et al., Citation2020; Hyland et al., Citation2021b).
1.1. Objectives of the study
In order to facilitate research on psychotrauma in France, validated measurement tools should be available. To date and to our knowledge, the ITQ is the only standardized self-administered questionnaire for assessing C-PTSD. Although the ITQ has already been translated into more than 20 languages, no validation in French existed at the time of this study. Recently, a Quebecan French version has been published (Cyr et al., Citation2022), validated with a sample of 335 French-speaking Quebecers. Given the sometimes important differences in formulations, it seemed necessary to propose a French version adapted to the French context. The objective of our study is to propose a French adaptation of the ITQ to a sample of people living in France. The aim is (a) to produce a French (trans-cultural) translation of the tool, (b) to confirm, in the French population, the factorial structure revealed in the original version as well as the internal consistency of the tool and its various dimensions, (c) to ensure that the tool has good convergent and divergent validity with other measures, (d) and to verify its temporal stability (reliability). Based on the existing literature, we determined the following 5 hypotheses: (1) the ITQ has good internal consistency, as measured by Cronbach’s alphas; (2) the best-fitting confirmatory factor model for the ITQ is a model with two second-order factors correlated with each other (PTSD and DSO), each grouping three first-order factors; (3) The ITQ score is positively correlated with measures of trauma exposure, the DSM-5's PTSD, emotional dysregulation, anxiety and depression; (4) The ITQ score is negatively correlated with the measure of perceived quality of life; (5) The reliability of the tool is satisfactory (significant and positive correlations of the ITQ scores at T1 (test) and at T2 (retest)).
2. Method
2.1. ITQ French translation
The ITQ has been translated according to Vallerand’s (Citation1989) recommendations for the translation and cross-cultural validation of tests. Three preliminary versions were produced by 6 bilingual translators with a dual French/Anglo-Saxon culture. Three of them translated the original version of the ITQ into French, and the other three performed a reverse translation from French into English. Then, we proceeded with an expert committee group, gathering translators and three PTSD experts, to develop the first French version of the tool. A pre-test was conducted within a community sample and psychologists aware of PTSD who were asked to evaluate the correct understanding of each item on a scale to 1 of 7. A new committee meeting was then organized to review the lowest rated items and to reformulate them if necessary. The final version of the French-ITQ was then included in the online protocol to assess its psychometric qualities. The table outlining the differences in translation between the Quebecan French version and the French version is available as supplementary material.
2.2. ITQ psychometric evaluation
2.2.1. Procedure
An online survey with LimeSurvey was conducted in the adult general French population between January 11th and March 08th 2022. Respondents were recruited from social networks using a snowball sampling method. Inclusion criteria were age ≥ 18 years, able to communicate fluently in French, and consenting to participate in the study. Participants had to report at least one potentially traumatic event to answer ITQ. Participants were informed of the objectives of the study and potential risks associated. Suicide prevention hotlines and resource centres dedicated to PTSD treatment were specified at the end of the survey. At the first assessment, respondents were invited to provide their email address if they agreed to be contacted again for a follow-up study. Participants who agreed were contacted three weeks after initial survey completion for completion of the ITQ retest. The research protocol met the General Data Protection Regulation criteria and was approved by the local ethics committee (Comité de Protection des Personnes Nord Ouest 1 – N°21.02325.000023).
2.2.2. Measures
2.2.2.1. The International Trauma Questionnaire (ITQ)
In the present study, the French version of the ITQ was used and examined. The ITQ (Cloitre et al., Citation2018) is an 18-item self-report measure of ICD-11 PTSD and C-PTSD symptoms among adults. Six items represent the three clusters of PTSD (re-experiencing, avoidance and sense of threat) and six others represent the three clusters of Disorders in Self Organization (DSO; ‘Affective dysregulation’, ‘disturbances in relationships’ and ‘negative self-concept’). Six other items measure functional impairment (social, occupational and other important areas of life) for the PTSD and DSO clusters. Items are scored on a five-point scale from 0 (‘Not at all’) to 4 (‘Extremely’). Respondents indicate how much each symptom has bothered them in the past month. Probable PTSD diagnosis is indicated by endorsement (score ≥ 2) of at least one symptom in each PTSD cluster and associated functional impairment. Probable C-PTSD diagnosis is indicated by endorsement of at least one symptom in each DSO cluster and associated impairment in addition to a diagnosis of PTSD. The full French version of the ITQ is available in supplementary material.
2.2.2.2. The International Trauma Exposure Measure (ITEM)
Traumatic exposure was assessed using the French Version of the ITEM (Hyland et al., Citation2021a) which is a freely available checklist measuring 21 threatening life events among the three developmental periods (0-12 years, 13–18 years, and older than 18 years). Sixteen events reflect the DSM-5 definition of trauma exposure, the other five events are psychologically threatening events that can be considered traumatic in line with ICD-11 guidelines (i.e. being stalked, bullied, neglected or humiliated). We previously translated a French version of the ITEM, using the same process as the French version of the ITQ (Peraud et al., Citation2022).
2.2.2.3. The post-traumatic checklist for DSM-5 (PCL-5)
Convergent validity was assessed using the PCL-5 (Weathers et al., Citation2013; French version by Ashbaugh et al., Citation2016). The PCL-5 is a 20-item self-report measure of DSM-5 PTSD symptoms among adults, reflecting the four clusters of PTSD (Intrusions, Avoidance, Negative alterations in cognitions and mood, and Alteration in arousal and reactivity). Items are scored on a five-point scale from 0 (‘not at all’) to 4 (‘extremely’). Respondents indicate how much each symptom has bothered them in the past month. Reliability in the sample was satisfactory (α = .93).
2.2.2.4. Difficulties in Emotion Regulation Scale (DERS)
The DERS (Gratz & Roemer, Citation2004; French version by Dan-Glauser & Scherer, Citation2013) is a 36-item self-report measure which assesses six dimensions of emotion regulation problems: Non acceptance (difficulty accepting negative emotions); Goals (difficulty in goal-directed behaviour when distressed); Impulse (problems controlling behaviours when distressed); Strategies (limited access to adaptive emotion regulation skills); Clarity (problems differentiating emotional states); Awareness (limited ability to identify emotions). Each item is rated on a 5-point scale. Reliability in the sample was satisfactory (α = .94).
2.2.2.5. The 5-item World Health Organization well-being index (WHO 5)
The WHO-5 is a short and generic global rating scale measuring subjective well-being, widely used over the world (Topp et al., Citation2015). Respondents indicate how well each item applies to them during the last 14 days on a five-point likert scale going from 0 (‘none of the time’) to 5 (‘all of the time’). Reliability in the sample was satisfactory (α = .90).
2.2.2.6. The Hospital Anxiety and Depressionscale (HADS)
The HADS (Zigmond & Snaith, Citation1983) is a 14-item self-report measure used to assess states of anxiety and depression. Items are scored on a 4-point scale rating from 0 to 3. The French version of this scale has been introduced by Lépine et al. (Citation1985) and has since been validated in clinical (Razavi et al., Citation1989; Untas et al., Citation2009) and non clinical samples (Bocéréan & Dupret, Citation2014). Reliability in the sample was acceptable for anxiety (α = .75) and depression (α = .81) subscales.
2.2.3. Statistical analysis
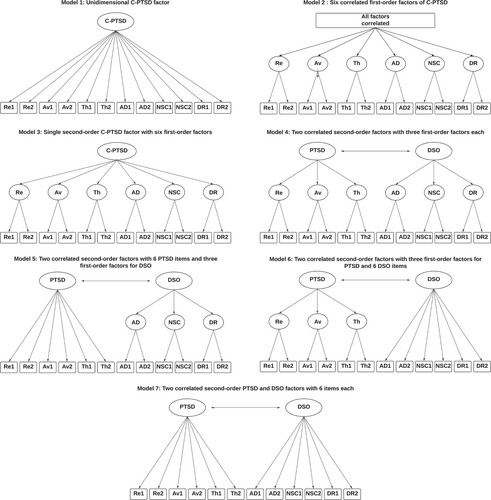
To test the psychometric properties of the French ITQ version, we tested internal consistency, factor structure, convergent and discriminant validities, and test-retest reliability. Internal consistency was tested by calculating Cronbach's α, setting the acceptability threshold at .70 (Tavakol & Dennick, Citation2011). For the factorial structure of the French version of the ITQ, we compared different theoretical models based on the ICD-11 definitions of PTSD and C-PTSD, using confirmatory factor analyses (CFA) with Maximum likelihood with robust standard errors (MLR) as the estimation method. We tested 7 models which are compiled from previous research concerning the factorial structure of the ITQ (Armour et al., Citation2021; Haselgruber et al., Citation2020). The 7 models used in this study are shown in . Model 1 estimates a single-factor model, with all symptoms loading on a single latent variable (CPTSD). Model 2 estimates a six-factor model with six correlated first-order factors (Av, Re, Th, AD, NSC and DR). Model 3 estimates six first-order factors, with one single second-order factor (CPTSD). Model 4 estimates six first-order factors, with two correlated second-order factors (PTSD and DSO). Av, Re and Th load on the second-order factor PTSD, AD,NSC and DR load on the second-order factor DSO. Model 5 estimates PTSD symptoms loading directly on the PTSD factor, while DSO symptoms load on their respective first-order factors (AD, NSC, DR), which load on the DSO factor. In model 6, PTSD symptoms load on their respective first-order factors (Av, Re, Th), which load on the PTSD factor, while DSO symptoms load directly on the DSO factor. In model 7, PTSD and DSO symptoms load directly on their respective factors (PTSD and DSO).
Figure 1. Seven models tested with ITQ scores. Note: Re = Re-experiencing; Av = Avoidance; Th = Sense of Threat; AD = Affective Dysregulation; NSC = Negative Self Concept; DR = Disturbances in Relationships; DSO = Disturbances in Self-Organization.
The selected fitting statistics and acceptability thresholds are those established by Hooper et al. (Citation2008) and Steiger (Citation2007): Comparative fit index (CFI) > .95; Root Mean Square Error of Approximation (RMSEA) < .07; Standardized root mean square residual (SRMR) < .08; Adjusted Goodness-of-Fit statistic (AGFI) > .90. We chose the Bayesian Information Criterion (BIC) as a comparison index between models, so that a decrease in the BIC corresponds to a better fit and a difference of 10 indicates a significant difference (Raftery, in Bauldry, Citation2015). For convergent and discriminant validity, Spearman correlations were performed between the total scores and the different symptom clusters of the ITQ and the scores obtained on the PCL-5, the DERS, the WHO-5, and the HADS. Finally, test-retest reliability was verified by Spearman correlations between the ITQ scores obtained at T1 and those obtained at T2, and also by calculation of the Intraclass Correlation Coefficient (ICC) between the two measurement times.
2.2.4. Characteristics of the sample
Of the 750 people who responded to the French version of the ITQ, 669 (89.2%) were women, 68 (9.07%) were men and 13 (1.73%) belonged to gender minorities. The mean age was 34.40 years (SD = 12.90). Among study participants, most were single (n = 223, 29.73%), in a couple or common-law couple (n = 296, 39.47%), and married or in a civil union (n = 178, n = 23.73%). The sample was mainly composed of executives and knowledge workers (n = 232, 30.93%), students (n = 224, 29.87%) and employees (n = 137, 18.27%). Education levels were mostly Bachelor degree (n = 266, 35.47%), Master degree (n = 260, 34.67%) and High School degree (n = 160, 21.33%).
presents the descriptive statistics of exposure to aversive experiences during childhood, adolescence and adulthood. The mean of aversive experiences experienced by our sample was 7.92 events. 458 participants (61.07%) in the sample had aversive experiences in childhood, 596 (79.47%) in adolescence, and 637 (84.93%) as adults. The full description of every aversive experience measured in this study by the ITEM is available in supplementary material.
Table 1. Descriptive statistics of aversive experiences measured (n = 750).
3. Results
3.1. ITQ descriptive statistics
presents descriptive statistics and Cronbach’s α for each dimension and total score of the ITQ. The means of the ITQ scores were 15.87 (SD = 10.53) for the total score, 7.74 (SD = 6.02) for the PTSD scale, and 8.12 (SD = 5.83) for DSO.
Table 2. ITQ French version descriptive statistics and internal consistency (n = 750).
3.2. Factorial structure
presents every fitting statistic for each model tested with CFA. Models 2 and 4 are both well-adjusted. When comparing the two models, the BIC value for Model 4 is lower than Model 2 and the difference between the two BIC values is 10, indicating a significantly better adjustment for Model 4. represents a graphical modelling of the factor structure of model 4.
Figure 2. Graphical modeling of the factor structure of Model 4. Note: Re = Re-experiencing; Av = Avoidance; Th = Sense of Threat; AD = Affective Dysregulation; NSC = Negative Self Concept; DR = Disturbances in Relationships; DSO = Disturbances in Self-Organization.
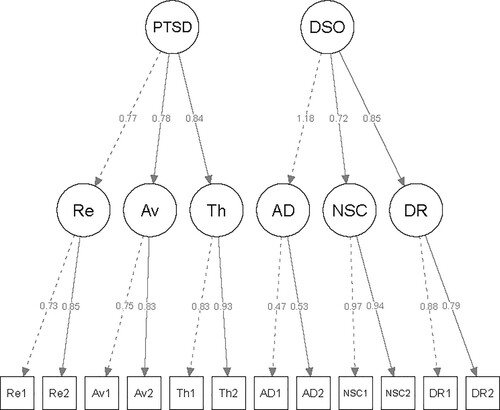
Table 3. Comparison of alternative models of ICD-11 based on ITQ French version‘s results.
According to , all items loaded significantly and positively into the first-order factors representative of their respective symptom clusters, ranging from 0.73–0.93 for the PTSD indicators and 0.47–0.97 for the DSO indicators. All of the second-order loadings for the PTSD and DSO latent variables were high, positive and significant at p < .01. As expected, in Model 4, PTSD and DSO were highly correlated (r = .74; p < .01).
Table 4. Standardized factor loadings for Model 4 (six first-order factors, with two correlated second-order factors) (N = 750).
3.3. Internal consistency
Cronbach’s α of the various dimensions and total ITQ scores are above the .70 acceptability threshold: from .77 to .95 for ITQ symptoms clusters, .85 for the six PTSD items, .84 for the six DSO items and .89 for the total ITQ score. The only exception was for the ‘Affective Dysregulation’ cluster (α = .40). Descriptive statistics and Cronbach’s α for every scale used in this study are available in .
Table 5. Descriptive statistics for every scale used (n = 750).
3.4. Convergent and discriminant validities
shows the different correlations between the ITQ scores and dimensions and the other scales used. PTSD and DSO subscales were positively correlated with the HADS Anxiety subscale (.60, p < .01 vs .57, p < .01), the HADS Depression subscale (.49, p < .01 vs .64, p < .01), the PCL-5 (.87, p < .01 vs .75, p < .01), the DERS Impulse subscale (.12, p < .01 vs .07, p = .07), the DERS Strategies subscale (.34, p < .01 vs .45, p < .01), the DERS Clarity subscale (.43, p < .01 vs .57, p < .01), and the DERS Awareness subscale (.18, p < .01 vs .29, p < .01). The only exception was the non-significant correlation between the AD symptom cluster and the DERS Impulse subscale (−.008, p = .83). PTSD and DSO subscales were negatively correlated with the WHO-5 (−.50, p < .01 vs –.65, p < .01), the DERS Goals subscale (−.27, p < .01 vs –.35, p < .01), and the DERS Non acceptance subscale (−.35, p < .01 vs –.42, p < .01). The strongest relationship was found between the PTSD subscale and the PCL-5 (.87, p < .01) and the weakest between the AD symptom cluster and the DERS Impulse subscale (−.008, p = .83).
Table 6. Correlations between ITQ scores and subscales and HADS, WHO-5, PCL-5 and DERS using Spearman’s ρ.
3.5. Test-retest reliability
Three hundred and thirty-two people responded to the second step of the study, approximately three weeks later. presents the various Spearman correlations and intraclass correlation coefficients between the two measurement times on the scores obtained on the ITQ. The correlations between the two measurement times are .77 for the PTSD subscale and .83 for the DSO subscale, and range from .68 to .83 for the symptom clusters. The overall intraclass correlation coefficients are significant at p < .01, are .767 and .830 for the PTSD and DSO scales, respectively, and range from .582 to .838 for the symptom clusters.
Table 7. Spearman's ρ correlations and intraclass correlation coefficient between the two measurement times at the ITQ scores and subscales (n = 332).
4. Discussion
The objective of this study was to propose a Francophone validation of the ITQ, in France. Overall, the French version of the ITQ showed satisfactory psychometric qualities. Its factorial structure was equivalent to the original version and the scale and its different subscales showed good internal consistency overall. The French version of the ITQ showed good convergent and divergent validity, as well as good test-retest reliability.
In this study, both the second-order two-factor model and the correlated first-order six-factor model had good fits. When comparing the two models using the BIC, the two-factor second-order model had the lowest value with a difference greater than 10, indicating a significantly better fit compared to the six-factor first-order correlated model. These two explanatory models of ICD-11 PTSD and C-PTSD measured by the ITQ are the best fit in the majority of previous studies, as explained in a literature review based on the factor structure analysis of the ITQ (Redican et al., Citation2021). According to this review, the two-factor second-order model would be more appropriate for clinical population studies, whereas the six-factor first-order correlated model would be preferred in general population studies. Although this hypothesis has been confirmed in many studies, the two-factor second-order model was the best fit in some general population research (Cyr et al., Citation2022; Redican et al., Citation2021). In comparison with the Quebecan French version (Cyr et al., Citation2022), both studies retained the second-order two-factor model as the best fit, and the fit indices are satisfactory for both the Quebecan French version (RMSEA = .045, SRMR = .034, CFI = .975) or the French version (RMSEA = .064, SRMR = .043, CFI = .971). This research provides further evidence on the need for more studies to get as close as possible to the concepts of PTSD and C-PTSD as defined by the ICD-11 when choosing ITQ factor structure.
The internal consistency of the French version of the ITQ is good, except for the Affective Dysregulation subdimension (α = .40). This is found in several studies (Cyr et al., Citation2022; Redican et al., Citation2021) and is consistent both theoretically and clinically. The ‘AD’ subdimension measures two opposing aspects of affective dysregulation reflecting affective under – and over-regulation (hyper-activation and hypo-activation), two modalities that are frequently and separately found in trauma patients.
4.1. Strengths and interests of the research
To our knowledge and to date, this study is the first to propose a version of the ITQ adapted to the French population, and thus makes available a first valid measurement tool for PTSD and C-PTSD according to the ICD-11 in France, with the advantage of being an economical scale in terms of time and therefore easily usable in clinical routine. The contributions of this tool are numerous, where the prevalence data of C-PTSD are still very limited or even non-existent in France and while this disorder seems to affect a significant part of the general and clinical population (Karatzias et al., Citation2017a). In this sense, this study is, to our knowledge, the first to provide data on C-PTSD as defined by the ICD-11 in France. It can also be observed in clinical practice that some patients sometimes present erroneous or incomplete diagnoses, in the absence of validated identification tools. This new tool will help research on this disorder, facilitate its identification in the field, and consequently help raise awareness among health professionals for a more appropriate care of patients.
4.2. Limits
As our sample is largely composed of young women with a rather high level of education, it is clear that certain profiles of people may have been missed in our study, such as elderly, precarious or marginalized people. As our study was conducted on a general population recruited via social networks, it is likely that the profile of our population is directly attributable to our methodology. Studies conducted via social networks have multiple biases that may influence both the population reached (limited to social network consumers and favouring profiles of young, white, and rather privileged women) (Peraud et al., Citation2021; Whitaker et al., Citation2017) and the rate of engagement (ability to leave the questionnaire at any time). It is also possible that those most impacted by their traumas were unable to complete the questionnaire. However, the meta-analysis by Jaffe et al. (Citation2015) blunted this idea by highlighting that online protocols would be less likely to generate distress related to the recall of events compared to interviews, and this distress seems to be compensated by other positive aspects such the feeling of helping other victims by having participated in the survey.
This validation study was conducted with a general population exposed to potentially traumatic events. It is therefore not representative of the French population and does not constitute a snapshot of patients who may be found in trauma centres, limiting the generalization of our results. In the future, it seems necessary that the French version of the ITQ be validated in different contexts, and particularly in the general population, with lower exposure to PTSD/C-PTSD (Hyland et al., Citation2017b; Wolf et al., Citation2015), and in the clinical population where the prevalences seem higher and the symptoms more intense (Cloitre et al., Citation2018; Hyland et al., Citation2017a; Karatzias et al., Citation2016).
5. Conclusion
Our study provides a French version of the ITQ with satisfactory psychometric qualities and in conformity with the original version of the ITQ. The factorial structure of the tool supports the distinction between PTSD and DSO symptoms provided by the ICD-11, even if model 2 also presents good statistical indices. The validation of the French ITQ is a first step towards having a PTSD and C-PTSD assessment tool adapted to the ICD-11 criteria in France. It is important that this scale be tested both in research and in clinical settings, with other populations, so that our results can be replicated or not. Although this scale is a significant contribution, like any self-questionnaire on post-traumatic symptoms, it is not sufficient on its own to make a diagnosis. Other tools need to be developed and validated in France, such as the International Trauma Interview (ITI) (Gelezelyte et al., Citation2022), a clinical interview for the assessment of PTSD and C-PTSD according to the ICD-11. These new perspectives should facilitate screening and thus promote earlier and more optimal treatment of these disorders.
Supplemental Material
Download MS Word (38.5 KB)Acknowledgements
We than Maria Karimov-Zwienenberg, Chloe Salway, Pascale Swedsen and Dr. Erwan Dieu for their help in translating this tool.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author [WP], upon reasonable request.
Additional information
Funding
References
- American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th edn) (DSM-IV). APA.
- Armour, C., Robinson, M., & Ross, J. (2021). Factor structure of the international trauma questionnaire in UK armed forces veterans residing in northern Ireland. European Journal of Psychotraumatology, 12(1), 1924954. https://doi.org/10.1080/20008198.2021.1924954
- Ashbaugh, A. R., Houle-Johnson, S., Herbert, C., El-Hage, W., & Brunet, A. (2016). Psychometric validation of the English and French versions of the posttraumatic stress disorder checklist for DSM-5 (PCL-5). PloS one, 11(10), e0161645. https://doi.org/10.1371/journal.pone.0161645
- Bauldry, S. (2015). Structural Equation Modeling. In J. D. Wright (Ed.), International encyclopedia of the social & behavioral sciences (Second Edition) (pp. 615–620). Elsevier. https://doi.org/10.1016/B978-0-08-097086-8.44055-9.
- Ben-Ezra, M., Karatzias, T., Hyland, P., Brewin, C. R., Cloitre, M., Bisson, J. I., Roberts, N. P., Lueger-Schuster, B., & Shevlin, M. (2018). Posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) as per ICD-11 proposals: A population study in Israel. Depression and Anxiety, 35(3), 264–274. https://doi.org/10.1002/da.22723
- Bocéréan, C., & Dupret, E. (2014). A validation study of the hospital anxiety and depression scale (HADS) in a large sample of French employees. BMC Psychiatry, 14(1), 1–11. https://doi.org/10.1186/s12888-014-0354-0
- Brewin, C. R. (2020). Complex post-traumatic stress disorder: A new diagnosis in ICD-11. BJPsych Advances, 26(3), 145–152. https://doi.org/10.1192/bja.2019.48
- Brewin, C. R., Cloitre, M., Hyland, P., Shevlin, M., Maercker, A., Bryant, R. A., Humayun, A., Jones, L. M., Kagee, A., Rousseau, C., & Somasundaram, D. (2017). A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clinical Psychology Review, 58, 1–15. https://doi.org/10.1016/j.cpr.2017.09.001
- Brewin, C. R., Lanius, R. A., Novac, A., Schnyder, U., & Galea, S. (2009). Reformulating PTSD for DSM-V: Life after criterion A. Journal of Traumatic Stress, 22(5), 366–373. https://doi.org/10.1002/jts.20443
- Cloitre, M., Courtois, C. A., Charuvastra, A., Carapezza, R., Stolbach, B. C., & Green, B. L. (2011). Treatment of complex PTSD: Results of the ISTSS expert clinician survey on best practices. Journal of Traumatic Stress, 24(6), 615–627. https://doi.org/10.1002/jts.20697
- Cloitre, M., Garvert, D. W., Brewin, C. R., Bryant, R. A., & Maercker, A. (2013). Evidence for proposed ICD-11 PTSD and complex PTSD: A latent profile analysis. European Journal of Psychotraumatology, 4(1), 20706. https://doi.org/10.3402/ejpt.v4i0.20706
- Cloitre, M., Hyland, P., Bisson, J. I., Brewin, C. R., Roberts, N. P., Karatzias, T., & Shevlin, M. (2019). ICD-11 posttraumatic stress disorder and complex posttraumatic stress disorder in the United States: A population-based study. Journal of Traumatic Stress, 32(6), 833–842. https://doi.org/10.1002/jts.22454
- Cloitre, M., Hyland, P., Prins, A., & Shevlin, M. (2021). The international trauma questionnaire (ITQ) measures reliable and clinically significant treatment-related change in PTSD and complex PTSD. European Journal of Psychotraumatology, 12(1), 1930961. https://doi.org/10.1080/20008198.2021.1930961
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., Karatzias, T., & Hyland, P. (2018). The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546. https://doi.org/10.1111/acps.12956
- Cyr, G., Belanger, C., & Godbout, N. (2022). French translation and validation of the international trauma questionnaire in a Canadian community sample. Child Abuse & Neglect, 128, 105627. https://doi.org/10.1016/j.chiabu.2022.105627
- Dan-Glauser, E. S., & Scherer, K. R. (2013). The difficulties in emotion regulation scale (DERS). Swiss Journal of Psychology, 72(1), 5–11. https://doi.org/10.1024/1421-0185/a000093
- Donat, J. C., Lobo, N. D. S., Jacobsen, G. D. S., Guimarães, E. R., Kristensen, C. H., Berger, W., & Nascimento, E. (2019). Translation and cross-cultural adaptation of the international trauma questionnaire for use in Brazilian Portuguese. Sao Paulo Medical Journal, 137(3), 270–277. https://doi.org/10.1590/1516-3180.2019.0066070519
- First, M. B., Reed, G. M., Hyman, S. E., & Saxena, S. (2015). The development of the ICD-11 clinical descriptions and diagnostic guidelines for mental and behavioural disorders. World Psychiatry, 14(1), 82–90. https://doi.org/10.1002/wps.20189
- Gelezelyte, O., Roberts, N. P., Kvedaraite, M., Bisson, J. I., Brewin, C. R., Cloitre, M., Kairyte, A., Karatzias, T., Shevlin, M., & Kazlauskas, E. (2022). Validation of the international trauma interview (ITI) for the clinical assessment of ICD-11 posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) in a Lithuanian sample. European Journal of Psychotraumatology, 13(1), 2037905. https://doi.org/10.1080/20008198.2022.2037905
- Gilbar, O. (2020). Examining the boundaries between ICD-11 PTSD/CPTSD and depression and anxiety symptoms: A network analysis perspective. Journal of Affective Disorders, 262, 429–439. https://doi.org/10.1016/j.jad.2019.11.060
- Gilbar, O., Hyland, P., Cloitre, M., & Dekel, R. (2018). ICD-11 complex PTSD among Israeli Male perpetrators of intimate partner violence: Construct validity and risk factors. Journal of Anxiety Disorders, 54, 49–56. https://doi.org/10.1016/j.janxdis.2018.01.004
- Gratz, K. L., & Roemer, L. (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. https://doi.org/10.1023/B:JOBA.0000007455.08539.94
- Haselgruber, A., Sölva, K., & Lueger-Schuster, B. (2020). Validation of ICD-11 PTSD and complex PTSD in foster children using the International Trauma Questionnaire. Acta Psychiatrica Scandinavica, 141(1), 60–73. https://doi.org/10.1111/acps.13100
- Ho, G. W., Hyland, P., Shevlin, M., Chien, W. T., Inoue, S., Yang, P. J., Chen, F. H., Chan, A. C., & Karatzias, T. (2020). The validity of ICD-11 PTSD and complex PTSD in east Asian cultures: Findings with young adults from China, Hong Kong, Japan, and Taiwan. European Journal of Psychotraumatology, 11(1), 1717826. https://doi.org/10.1080/20008198.2020.1717826
- Ho, G. W., Karatzias, T., Cloitre, M., Chan, A. C., Bressington, D., Chien, W. T., Hyland, P., & Shevlin, M. (2019). Translation and validation of the Chinese ICD-11 international trauma questionnaire (ITQ) for the assessment of posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD). European Journal of Psychotraumatology, 10(1), 1608718. https://doi.org/10.1080/20008198.2019.1608718
- Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modelling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6(1), 53–60.
- Hyland, P., Karatzias, T., Shevlin, M., McElroy, E., Ben-Ezra, M., Cloitre, M., & Brewin, C. R. (2021a). Does requiring trauma exposure affect rates of ICD-11 PTSD and complex PTSD? Implications for DSM–5. Psychological Trauma: Theory, Research, Practice, and Policy, 13(2), 133. https://doi.org/10.1037/tra0000908
- Hyland, P., Murphy, J., Shevlin, M., Vallieres, F., McElroy, E., Elklit, A., Christoffersen, M., & Cloitre, M. (2017a). Variation in post-traumatic response: The role of trauma type in predicting ICD-11 PTSD and CPTSD symptoms. Social psychiatry and psychiatric epidemiology, 52(6), https://doi.org/10.1007/s00127-017-1350-8
- Hyland, P., Shevlin, M., Brewin, C. R., Cloitre, M., Downes, A. J., Jumbe, S., Karatzias, T., Bisson, J. I., & Roberts, N. P. (2017b). Validation of post-traumatic stress disorder (PTSD) and complex PTSD using the international trauma questionnaire. Acta Psychiatrica Scandinavica, 136(3), 313–322. https://doi.org/10.1111/acps.12771
- Hyland, P., Vallières, F., Cloitre, M., Ben-Ezra, M., Karatzias, T., Olff, M., & Shevlin, M. (2021b). Trauma, PTSD, and complex PTSD in the republic of Ireland: Prevalence, service use, comorbidity, and risk factors. Social Psychiatry and Psychiatric Epidemiology, 56(4), 649–658. https://doi.org/10.1007/s00127-020-01912-x
- Jaffe, A. E., DiLillo, D., Hoffman, L., Haikalis, M., & Dykstra, R. E. (2015). Does it hurt to ask? A meta-analysis of participant reactions to trauma research. Clinical Psychology Review, 40, 40–56. https://doi.org/10.1016/j.cpr.2015.05.004
- Karatzias, T., Cloitre, M., Maercker, A., Kazlauskas, E., Shevlin, M., Hyland, P., & Brewin, C. R. (2017a). PTSD and complex PTSD: ICD-11 updates on concept and measurement in the UK, USA, Germany and Lithuania. European Journal of Psychotraumatology, 8(sup7), 1418103. https://doi.org/10.1080/20008198.2017.1418103
- Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D., Roberts, N., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of PTSD and complex PTSD (ICD-TQ): evidence of construct validity. Journal of Anxiety Disorders, 44, 73–79. https://doi.org/10.1016/j.janxdis.2016.10.009
- Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D., Roberts, N., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2017b). Evidence of distinct profiles of posttraumatic stress disorder (PTSD) and complex posttraumatic stress disorder (CPTSD) based on the new ICD-11 trauma questionnaire (ICD-TQ). Journal of Affective Disorders, 207, 181–187. https://doi.org/10.1016/j.jad.2016.09.032
- Lépine, J. P., Godchau, M., Brun, P., & Lempérière, T. H. (1985). Évaluation de l'anxiété et de la dépression chez des patients hospitalisés dans un service de médecine interne [Anxiety and depression evaluation in patients hospitalized in an internal medicine unit]. Annales Médico-Psychologiques, 143(2), 175–189.
- Maercker, A., Brewin, C., Bryant, R., Cloitre, M., & Reed, G. (2013). Proposals for mental disorders specifically associated with stress in the international classification of diseases-11. The Lancet, 381(9878), https://doi.org/10.1016/S0140-6736(12)62191-6
- Mordeno, I. G., Nalipay, M. J. N., & Mordeno, E. R. (2019). The factor structure of complex PTSD in combat-exposed Filipino soldiers. Psychiatry Research, 278, 65–69. https://doi.org/10.1016/j.psychres.2019.05.035
- Møller, L., Augsburger, M., Elklit, A., Søgaard, U., & Simonsen, E. (2020). Traumatic experiences. ICD-11, PTSD, ICD-11 complex PTSD, and the overlap with ICD-10 diagnoses. Acta Psychiatrica Scandinavica, 141(5), 421–431. https://doi.org/10.1111/acps.13161
- Murphy, D., Shevlin, M., Pearson, E., Greenberg, N., Wessely, S., Busuttil, W., & Karatzias, T. (2020). A validation study of the international trauma questionnaire to assess post-traumatic stress disorder in treatment-seeking veterans. The British Journal of Psychiatry, 216(3), 132–137. https://doi.org/10.1192/bjp.2020.9
- Owczarek, M., Ben-Ezra, M., Karatzias, T., Hyland, P., Vallieres, F., & Shevlin, M. (2020). Testing the factor structure of the international trauma questionnaire (ITQ) in African community samples from Kenya, Ghana, and Nigeria. Journal of Loss and Trauma, 25(4), 348–363. https://doi.org/10.1080/15325024.2019.1689718
- Owczarek, M., Karatzias, T., McElroy, E., Hyland, P., Kratzer, L., Knefel, M., Grandison, G., Ho, G. W., Morris, D., & Shevlin, M. (2022). Borderline personality disorder (BPD) and complex post traumatic stress disorder (CPTSD): A network analysis in a highly traumatised clinical sample. Journal of Personality Disorders.
- Peraud, W., Hebrard, L., Lavandier, A., Brennstuhl, M. J., & Quintard, B. (2022). French cross-cultural adaptation and validation of the international trauma exposure measure (ITEM) in a French community sample. Manuscript in preparation.
- Peraud, W., Quintard, B., & Constant, A. (2021). Factors associated with violence against women following the COVID-19 lockdown in France: Results from a prospective online survey. PLoS one, 16(9), e0257193. https://doi.org/10.1371/journal.pone.0257193
- Razavi, D., Delvaux, N., Farvacques, C., & Robaye, E. (1989). Validation de la version française du HADS dans une population de patients cancéreux hospitalisés. Revue de psychologie appliquée.
- Redican, E., Nolan, E., Hyland, P., Cloitre, M., McBride, O., Karatzias, T., Murphy, J., & Shevlin, M. (2021). A systematic literature review of factor analytic and mixture models of ICD-11 PTSD and CPTSD using the international trauma questionnaire. Journal of Anxiety Disorders, 79, 102381. https://doi.org/10.1016/j.janxdis.2021.102381
- Rossi, R., Socci, V., Pacitti, F., Carmassi, C., Rossi, A., Di Lorenzo, G., & Hyland, P. (2022). The Italian version of the international trauma questionnaire: Symptom and network structure of post-traumatic stress disorder and complex post-traumatic stress disorder in a sample of late adolescents exposed to a natural disaster. Frontiers in Psychiatry, 13, https://doi.org/10.3389/fpsyt.2022.859877
- Shevlin, M., Hyland, P., Roberts, N. P., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2018). A psychometric assessment of disturbances in self-organization symptom indicators for ICD-11 complex PTSD using the international trauma questionnaire. European Journal of Psychotraumatology, 9(1), 1419749. https://doi.org/10.1080/20008198.2017.1419749
- Somma, A., Maffei, C., Borroni, S., Gialdi, G., & Fossati, A. (2019). Post traumatic reactions as individual differences: Latent structure analysis of the international trauma questionnaire in Italian trauma-exposed and non-trauma exposed adults. Mediterranean Journal of Clinical Psychology, 7, 1. https://doi.org/10.6092/2282-1619/2019.7.2058
- Steiger, J. H. (2007). Understanding the limitations of global fit assessment in structural equation modeling. Personality and Individual Differences, 42(5), 893–898. https://doi.org/10.1016/j.paid.2006.09.017
- Tavakol, M., & Dennick, R. (2011). Making sense of cronbach's alpha. International Journal of Medical Education, 2, 53. https://doi.org/10.5116/ijme.4dfb.8dfd
- Topp, C. W., Østergaard, S. D., Søndergaard, S., & Bech, P. (2015). The WHO-5 well-being index: A systematic review of the literature. Psychotherapy and Psychosomatics, 84(3), 167–176. https://doi.org/10.1159/000376585
- Untas, A., Aguirrezabal, M., Chauveau, P., Leguen, E., Combe, C., & Rascle, N. (2009). Anxiété et dépression en hémodialyse: Validation de l’Hospital Anxiety and Depression Scale (HADS). Néphrologie & Thérapeutique, 5(3), 193–200. https://doi.org/10.1016/j.nephro.2009.01.007
- Vallerand, R. J. (1989). Vers une méthodologie de validation trans-culturelle de questionnaires psychologiques: Implications pour la recherche en langue française. Canadian Psychology/Psychologie Canadienne, 30(4), 662. https://doi.org/10.1037/h0079856
- Vallières, F., Ceannt, R., Daccache, F., Abou Daher, R., Sleiman, J., Gilmore, B., Byrne, S., Shevlin, M., Murphy, J., & Hyland, P. (2018). ICD-11 PTSD and complex PTSD amongst Syrian refugees in Lebanon: The factor structure and the clinical utility of the International Trauma Questionnaire. Acta Psychiatrica Scandinavica, 138(6), 547–557. https://doi.org/10.1111/acps.12973
- Van der Kolk, B. A., Roth, S., Pelcovitz, D., Sunday, S., & Spinazzola, J. (2005). Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. Journal of Traumatic Stress: Official Publication of the International Society for Traumatic Stress Studies, 18(5), 389–399. https://doi.org/10.1002/jts.20047
- Vang, M. L., Dokkedahl, S. B., Løkkegaard, S. S., Jakobsen, A. V., Møller, L., Auning-Hansen, M. A., & Elklit, A. (2021). Validation of ICD-11 PTSD and DSO using the international trauma questionnaire in five clinical samples recruited in Denmark. European Journal of Psychotraumatology, 12(1), 1894806. https://doi.org/10.1080/20008198.2021.1894806
- Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The ptsd checklist for dsm-5 (pcl-5). Scale available from the National Center for PTSD at www.Ptsd.va.gov, 10(4), 206. https://doi.org/10.1002/jts.22059
- Whitaker, C., Stevelink, S., & Fear, N. (2017). The use of Facebook in recruiting participants for health research purposes: A systematic review. Journal of Medical Internet Research, 19(8), e290. https://doi.org/10.2196/jmir.7071
- Wolf, E. J., Miller, M. W., Kilpatrick, D., Resnick, H. S., Badour, C. L., Marx, B. P., Keane, T. M., Rosen, R. C., & Friedman, M. J. (2015). ICD–11 complex PTSD in US national and veteran samples: Prevalence and structural associations with PTSD. Clinical Psychological Science, 3(2), 215–229. https://doi.org/10.1177/2167702614545480
- World Health Organization. (1992). The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. WHO.
- World Health Organization. (2018). ICD-11: International classification of diseases 11th revision. WHO. (https://icd.who.int/en/). Accessed 19 Jul 2022.
- Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67(6), 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x