
ABSTRACT
Background: Significant numbers of individuals leave the military and experience symptoms of posttraumatic stress disorder (PTSD). Veterans with PTSD symptoms rarely experience them in isolation, more commonly they are co-morbid with a range of other difficulties.
Objective: Latent profile analysis (LPA) was used to explore the heterogeneity of PTSD symptom presentation. Following this, regression analysis was used to examine variables that predicted membership to the identified PTSD profiles.
Methods: Data on childhood adversity, socio-demographic characteristics and mental health outcomes was collected from 386 male veterans who had engaged with mental health services in the UK.
Results: LPA identified a six-profile model to best describe the sample. There was a Low symptom profile, a Severe symptom profile and four Moderate symptom profiles. The Severe symptom profile was the largest one, accounting for 37.57% of the sample. Five out of the six profiles had mean PTSD scores above the cut-off for probable PTSD. Higher rates of common mental health difficulties were associated with more symptomatic profiles.
Discussion: As the vast majority of veterans met criteria for probable PTSD, the finding of six different profiles differing primarily quantitatively, but to some extent also qualitatively, suggests the importance of moving away from a ‘one-size fits all’ approach when it comes to treatments, towards developing interventions that are tailored to meet the specific PTSD and co-morbid symptoms profiles.
HIGHLIGHTS
• Six PTSD profiles were identified in UK treatment-seeking military veterans.• The differences between the profiles were primarily quantitative.• Qualitative differences between profiles emerged in relation to the PTSD avoidance symptoms.• Common mental health difficulties were consistently associated with more symptomatic profiles.
Antecedentes: Un número significativo de individuos deja el servicio militar y experimenta síntomas de trastorno de estrés postraumático (TEPT). Los veteranos con síntomas de TEPT rara vez los experimentan de forma aislada, más comúnmente son comórbidos con una variedad de otras dificultades.
Objetivo: Se utilizó el análisis de perfiles latentes (LPA, en sus siglas en inglés) para explorar la heterogeneidad de la presentación de síntomas del TEPT. A continuación se usó análisis de regresión para examinar variables que predijeran la pertenencia a los perfiles de TEPT identificados.
Método: Se obtuvieron datos sobre la adversidad infantil, las características sociodemográficas y los resultados de salud mental de 386 veteranos varones que habían consultado en servicios de salud mental en el Reino Unido.
Resultados: LPA identificó un modelo de seis perfiles que mejor describen la muestra. Hubo un perfil de síntomas bajos, un perfil de síntomas graves y cuatro perfiles de síntomas moderados. El perfil de síntomas severos fue el más grande, representando el 37.57% de la muestra. Cinco de los seis perfiles tenían puntajes promedio de TEPT por encima del puntaje de corte para probable TEPT. Tasas más altas de dificultades de salud mental comunes se asociaron con más perfiles sintomáticos.
Discusión: Como la gran mayoría de los veteranos cumplieron con los criterios de probable TEPT, el hallazgo de seis perfiles diferentes que se distinguen principalmente de forma cuantitativa, pero en cierta medida también cualitativamente, sugiere la importancia de alejarse de un enfoque ‘de una sola talla’ para todos cuando se trata de tratamientos, hacia el desarrollo de intervenciones que se adapten a los perfiles específicos de TEPT y síntomas comórbidos.
背景: 大量人员离开军队后经历了创伤后应激障碍(PTSD)的症状。退伍军人患有的PTSD症状的很少孤立地出现,常见它们与其他一系列障碍共病。
目的:使用潜剖面分析(LPA)来探索PTSD症状表现的异质性。然后使用回归分析考查PTSD剖面的预测变量。
方法:在英国收集了使用过精神卫生服务的386名男性退伍军人的童年不幸、社会人口学特征和心理健康结果的数据。
结果:LPA识别一个六维剖面模型可以最好地描述该样本:低症状,严重症状和四种中度症状剖面。严重症状剖面比例最高,占样本的37.57%。其中五个剖面的PTSD分数高于潜在PTSD的临界值。常见心理健康问题的较高发生率与更多的症状表现有关。
讨论:绝大多数退伍军人符合可能的创伤后应激障碍的标准。六种不同的剖面的发现主要是量化上的差异,但在某种程度上也是性质上的差异。这提示应在治疗中放弃‘普适’方法,针对有共病的PTSD的特异症状定制开发干预措施。
1. Introduction
Approximately 15,000 individuals leave the UK military each year (Defence Analytical Services Agency, Citation2017). The majority of UK veterans make successful transitions into civilian life, however, a minority either leave with, or later develop, mental health difficulties. Of veterans in this group, those suffering from posttraumatic stress disorder (PTSD) have been shown to be at the greatest risk of experiencing social exclusion, have higher associated health costs and are less likely to seek support than veterans suffering from other mental health conditions (Brunello et al., Citation2017; Iversen et al., Citation2005, Citation2011; Pinder, Murphy, Iversen, Wessely, & Fear, Citation2011). Evidence shows that PTSD is rarely experienced in isolation, but more frequently with at least one or more co-morbidities (Murphy, Ashwick, Palmer, & Busuttil, Citation2017a).
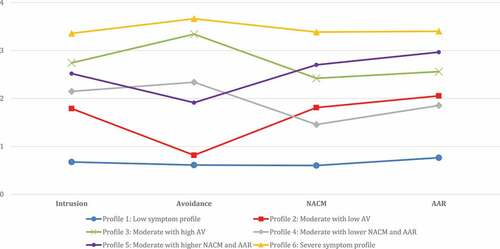
Figure 1. Mean PTSD symptom cluster scores in the six latent profiles.
Another important concern is that veterans with PTSD appear to respond less favourably to treatments than civilian groups (Bisson et al., Citation2007; Bisson, Roberts, Andrew, Cooper, & Lewis, Citation2013). Furthermore, treatment outcome studies from a range of veteran populations suggest the presence of differing treatment trajectories and the negative influence of a range of co-morbidities, such as depression, anxiety, dissociation and functional impairment, on treatment efficacy (Currier, Holland, Drescher, Elhai, & Elhai, Citation2014; Murphy & Smith, Citation2018; Murphy et al., Citation2016; Phelps et al., Citation2018; Richardson et al., Citation2014). Understanding the heterogeneity of PTSD profiles may therefore help inform better interventions.
The majority of research focussed on PTSD has used psychometric measures to either define the presence/absence of PTSD or explore severity of PTSD symptoms as a composite score to measure the burden of PTSD symptomology. These approaches allow for inferences to be made about the prevalence or severity of PTSD within populations, but not about the variation of PTSD symptom presentations within these populations. Latent profile analysis (LPA) is a statistical technique that aims to overcome this by assessing for the presence of heterogeneous subgroups within a population of interest including veterans with PTSD symptoms. Heterogeneity may stem from differences in endorsement and/or severity of individual symptoms, thus yielding qualitative and/or quantitative differences in PTSD symptoms between the subgroups. In LPA, individuals are categorized into profiles based on their responses to a set of continuous indicators (e.g. PTSD symptoms rated on a five-point Likert scale). In contrast, latent class analysis (LCA) utilizes categorical indicators (e.g. symptom endorsed or not endorsed).
Studies that have utilized LPA and LCA have demonstrated the presence of different PTSD subgroups within various veteran populations. For example, using the 17 PTSD items from the DSM-IV version of the PTSD-Checklist (PCL) as indicators, a study of a clinical sample of Canadian veterans presenting for psychiatric assessment identified a more symptomatic PTSD class and a less symptomatic PTSD class. The differences were predominantly quantitative (i.e. PTSD item severity), but the latter class scored lower primarily on the emotional numbing and dysphoria symptoms of PTSD (Naifeh, Richardson, Del Ben, & Elhai, Citation2010). Additionally, the authors found that membership of the more symptomatic, as opposed to the less symptomatic, class was more common in those with a depression diagnosis. In another LCA study conducted with Vietnam veterans and using the 17 PTSD items from the Structured clinical interview for the DSM-III-R, three classes characterized by no disturbance, intermediate disturbance and pervasive disturbance were identified (Steenkamp et al., Citation2012). The differences in PTSD symptoms between the classes were primarily quantitative, but the authors also reported some qualitative differences with avoidance and hypervigilance symptoms being most elevated in the pervasive disturbance class relative to the other two classes. Individuals in the pervasive disturbance class also reported greater exposure to war-zone stressors, more dissociation and lower education.
A LCA study of US female veterans with PTSD, which utilized the 17 items from the DSM-IV version of the PCL, identified four latent classes; a high symptom class, two intermediate symptom classes and a low symptom class (Hebensteit, Madden, & Maguen., Citation2014). The differences in PTSD symptoms between the four classes were primarily quantitative. Qualitative differences were revealed between the two intermediate classes, one of which had a very high probability of endorsing the emotional numbing symptoms of PTSD. The classes could be further differentiated based on socio-demographic and military-related variables, such as age, race/ethnicity, time since deployment and distance from a treatment centre. Using another sample of US Iraq and Afghanistan veterans meeting the criteria for full or sub-threshold PTSD and utilizing the 17 PTSD items from the DSM-IV version of the PCL, Maguen et al. (Citation2013) revealed four latent classes characterized by high, intermediate (2x) and low PTSD symptomology. Again, the differences in PTSD symptoms between the latent classes were primarily quantitative, but the two intermediate classes differed in the endorsement of several emotional numbing and irritability symptoms. Additionally, those who reported having killed were more likely to be categorized into the high symptomology class than those who did not kill. Examining differences between the classes/profiles on external variables is important as it provides external validation of the distinctiveness of the classes and, additionally, it may help to highlight important risk factors for the higher severity classes, which in turn may inform early interventions.
As highlighted above, LCA and LPA can help move away from a binary understanding of PTSD based on prevalence or caseness to allow for the understanding about the variance between individuals experiencing symptoms of PTSD. This could have important implications for the development of more tailored interventions to move away from a ‘one-size fits all’ approach that may lead to attrition from treatment or less favourable outcomes as has been recently advocated (Steenkamp, Citation2016).
To date, no studies have used LCA/LPA to explore the heterogeneity of PTSD profiles in UK veterans and, to the best of our knowledge, no veteran studies have used the DSM-5 (as opposed to DSM-IV) PTSD symptoms as indicators in the analysis. The current study aimed to address this by using data from a sample of veterans who had sought support for mental health difficulties and who were assessed with the DSM-5 version of the PCL (PCL-5). The DSM-IV and DSM-5 criteria for PTSD differ in the number of symptoms (17 vs. 20) as well as the wording of some symptoms and it is therefore important to examine the heterogeneity in PTSD symptom presentation using these updated criteria. The current study used an LPA to explore for the presence of different PTSD typologies and logistic regressions were used to examine a range of health outcomes and socio-demographic factors as predictors of latent profile membership. The inclusion of these covariates served two purposes: (1) to validate the resulting profiles, and (2) to examine whether any of these are specifically related to certain PTSD profiles. As this is the first LPA study of PTSD conducted with UK treatment-seeking veterans, no specific hypotheses were made about the number of profiles to be found. However, based on previous research with this sample (Murphy et al., Citation2017a), we expected several external variables to differentially predict membership in the latent profiles. These variables included history of childhood adversities, common mental health problems, hazardous drinking, time taken to seek help after leaving the military and several demographic variables (age, relationship status, employment status), all of which were previously found to be associated with PTSD caseness and/or increasing PTSD severity (Murphy et al., Citation2017a).
2. Methods
2.1. Design
Data for this study was extracted from a cross-sectional study exploring the health and wellbeing of a sample of treatment-seeking UK veterans (Murphy et al., Citation2017a). This study sampled from a national veteran-specific mental health charity in the UK called Combat Stress (CS) that offers clinical services to veterans. CS receives approximately 2500 new referrals per annum from across the UK.
2.2. Participants
A 20% sample of veterans who had engaged with CS over a 12-month period was randomly selected to be contacted as potential participants for the study (n = 600). Inclusion criteria were being a veteran (defined in the UK as having completed at least one full day of military service) and having attended one or more appointments (other than an initial assessment) between January 2015 and December 2016. A response rate of 403/600 (67.2%) was achieved. We have previously demonstrated that no differences were present between individuals who returned completed questionnaires and those who did not (Murphy et al., Citation2017a).
2.3. Procedure
Data was collected through an eight-page questionnaire. A three-wave mail out strategy and follow up telephone tracing was employed to elicit a response. Data collection was conducted between March and August 2017.
2.4. Measures
The questionnaire collected data on socio-demographic characteristics, information on exposure to childhood adversity, military history and included a number of health and wellbeing outcome measures. The variables used for the current study are described below.
2.5. Primary health outcome
PTSD symptoms were assessed using the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., Citation2013). The PCL-5 consists of 20 items that are scored on a five-point Likert scale. The 20 items map onto the fifth edition of the Diagnostic and Statistical Manual (DSM-5) diagnosis for PTSD. Accordingly, they assess symptoms of intrusion, reexperiencing, negative alterations in cognitions and mood (NACM) and alterations in arousal and reactivity (AAR). Participants are asked to endorse the frequency of each symptom over the last month. Responses range from ‘not at all’ to ‘extremely’ and are scored from 0 to 4. Total scores range from 0 to 80 and in UK veterans scores of 34 or more have been shown to be indicative of probable PTSD (Murphy, Ross, Ashwick, Armour, & Busuttil, Citation2017b).
2.6. Demographic characteristics and life experiences
Demographic details were collected about age, sex, relationship status (single/divorced/separated/widowed/in a relationship) and employment status (working or not). Time taken between leaving the military and first contact with CS was calculated and dichotomized between taking greater or less than five years to contact CS.
Adverse childhood experiences were recorded by asking respondents to endorse a list of 16 true or false statements related to difficult early life events. These items were taken from a longitudinal epidemiological study exploring the health and wellbeing of the UK military (Iversen et al., Citation2007). For the purposes of the current study, a sum score was calculated and used as a continuous variable indicating exposure to various types of childhood adversities.
2.7. Health and wellbeing outcomes
Common mental health difficulties (CMD) were assessed with the General Health Questionnaire (GHQ-12; Goldberg & William, Citation1998). The GHQ-12 has 12 items asking about the frequency of mental health symptoms related to anxiety and depression. Total scores on the GHQ-12 range from 0 to 12. Meeting case criteria on the GHQ-12 has been defined as a score of 4 or more.
The World Health Organization’s Alcohol Use Disorders Identification Test (AUDIT; Babor, Higgins-Biddle, Saunders, & Monteiro, Citation2001) was used to explore alcohol difficulties. This is a 10-item measure that is scored from 0 to 40. Scores of 8 or above have been used to indicate the presence of hazardous drinking (Babor et al., Citation2001).
2.8. Data analysis
Prior to conducting the LPA, the 20 PCL-5 symptoms were converted into mean symptom cluster scores corresponding to the DSM-5 PTSD criteria B (intrusion), C (avoidance), D (NACM) and E (AAR). The aim of using this reduced number of indicators was to account for the relatively small sample size and to facilitate interpretation. Models with increasing number of latent profiles were estimated. The analysis was conducted in Mplus 8 (Muthén & Muthén, Citation2007) using the default settings for LPA, including the robust maximum likelihood estimator, but each model was estimated with two different sets of starting values (200 and 400) to achieve model convergence and avoid local maxima solutions. The Akaike’s Information Criterion (AIC), Bayesian Information Criterion (BIC) and the Sample-Size-Adjusted BIC (SSABIC) were used to compare models with different numbers of profiles. Lower relative values of these three fit indices indicate better model fit. The Lo-Mendell-Rubin-Adjusted likelihood ratio test and the Bootstrapped likelihood ratio test were used to compare models with adjacent numbers of profiles. A significant p-value associated with these two tests indicates that a particular model fits better than another with one fewer profile. When deciding on the optimal number of profiles, parsimony, meaningfulness and ease of interpretation were also considered (Nylund, Asparouhov, & Muthén, Citation2007; Nylund, Bellmore, Nishina, & Graham, Citation2007).
Once the optimal model was decided upon, we conducted Analyses of Variance (ANOVAs) in SPSS 24 to examine the differences between the latent profiles in the mean PTSD symptom cluster scores, as well as the total PCL-5 scores. To do so, each participant was assigned to their most likely profile. This procedure is associated with some degree of classification error, however, if entropy values are high, the error is minimal.
Finally, we examined the predictors of the latent profiles using the 3-step approach for conducting multinomial logistic regressions in Mplus (Asparouhov & Muthén, Citation2014). The AUXILIARY statement in Mplus was used to specify the covariates. The 3-step approach takes into account the classification error (i.e. when some participants do not fit perfectly into a single profile). To account for the high number of comparisons, we selected alpha value of p < .01 to indicate a significant predictor. The predictors included two continuous (participants’ age, child adversities) and five binary variables (relationship status, employment status, time taken to contact CS, CMD, hazardous drinking), coded as specified in the Measures section.
3. Results
3.1. Descriptive statistics
In total, 403 participants returned completed questionnaires. Of these, 386 were males and were included in the current study. The mean age of the effective sample was 50.9 years (SD = 12.7). A total of 347/403 (86.1%) had served in the Army (6.7% naval services, 7.2% RAF). A majority of participants reported being in a relationship (in a relationship; 267/386: 69.2% versus single; 119/386: 30.8%) and not currently being in employment (not working; 263/386: 68.1% versus working; 123/386: 31.9%). Just over half (200/386; 51.8%) of participants reported that their first contact with CS was within five years of leaving the military compared to 186/386 (48.2%) who reported taking longer than five years. The scores on PCL-5 ranged from 0 to 80, with a mean score of 52.75 (SD = 16.89). A total of 334/386 (86.5%) of participants scored at or above the 34-point cut-off, indicating probable diagnosis of PTSD (Murphy et al., Citation2017b).
3.2. Latent profile analysis
The results of the LPA are presented in . Models consisting of between one and seven profiles were estimated. The seven-profile model contained a profile consisting of only 3.6% of the sample, which was deemed too small for generalizations. Models with higher number of profiles were therefore not estimated. The AIC, BIC and SSABIC values kept decreasing from the one- to the six-profile model, although the differences in BIC values were no longer substantial past the five-profile model. The LMRA pointed to the three-profile model and the BLRT statistic was significant for all models. All models had good entropy values. Taken together, the fit statistics did not point to a single model as superior. However, (1) as both the AIC and SSABIC suggested that the six-profile model fit the data better than the five-profile model, and (2) that the seven-profile model fit the data better than the six-profile model, but (3) the seven-profile contained a very small profile, and (4) additionally, the BIC suggested that the seven-profile model did not fit significantly better than the six-profile model, we selected the six-profile model as optimal.
Table 1. Fit indices of the latent profile models of PTSD symptom clusters.
The individual profiles are depicted in . The first profile (n = 27, 7.00% based on most likely latent profile membership) was characterized by low overall PTSD symptomatology and was named the Low symptom profile. The mean PCL-5 score in this group was 13.74 (SD = 7.46). There were four profiles characterized by moderate PTSD symptomatology: Profile 2 – Moderate with low avoidance (n = 31, 8.03%) with a mean PCL-5 score of 35.55 (SD = 6.10); Profile 3 – Moderate with high avoidance (n = 86, 22.28%) with a mean PCL-5 score of 52.31 (SD = 5.61); Profile 4 – Moderate with lower NACM and AAR (n = 41, 10.62%) with a mean PCL-5 score of 36.68 (SD = 5.89); and Profile 5 – Moderate with higher NACM and AAR (n = 56, 14.51%) with a mean PCL-5 score of 53.04 (SD = 6.73). The final profile – the Severe symptom profile (n = 145, 37.57%) was characterized by severe overall PTSD symptomatology. The mean PCL-5 score in this group was 68.38 (SD = 5.53).
3.3. Analyses of variance
One-way between-groups ANOVA with Bonferroni-adjusted post-hoc tests was conducted to compare the PCL-5 scores across the latent profiles. In order to do so, the most likely profile membership for each individual was exported to SPSS. With the exception of two comparisons (1) Moderate with low avoidance with Moderate with lower NACM/AAR; (2) Moderate with high avoidance with Moderate with higher NACM/AAR), all profiles differed significantly from each other (ps < .001) on the PCL-5 scores.
The profiles were further compared on their mean PTSD symptom cluster scores. One-way between-groups ANOVAs showed that all profiles were significantly different from each other: ps < .001 (Bonferroni-adjusted alpha level for the omnibus test = .05/4 = .013). With the exception of a few pairwise comparisons (see ), the majority of the PTSD symptom cluster scores were significantly different between the latent profiles (Bonferroni-adjusted post-hoc tests in SPSS), thus supporting the quantitative differences between the profiles.
Table 2. Mean PTSD symptom cluster scores by latent profile and differences between latent profiles.
3.4. Multinomial logistic regression analysis
Descriptive statistics on the covariates in the full sample and each latent profile are shown in . The full results of the multinomial logistic regression are presented in . Briefly, individuals in the Severe symptom profile relative to the Low symptom profile were more likely to have CMD problems and to have taken 5+ years to seek help. The Severe symptom profile also differed from two moderate symptom profiles: compared to the Moderate with low avoidance profile, those in the Severe symptom profile were more likely to have CMD problems and they were more likely to be unemployed; and compared to the Moderate with lower NACM and AAR symptom profile, they were more likely to have CMD problems, to be younger and to have experienced more childhood adversities. The Severe symptom profile did not differ from the Moderate with high avoidance and the Moderate with higher NACM and AAR symptom profiles on any of the covariates.
Table 3. Descriptive statistics for the covariates in the full sample and each latent profile.
Table 4. Odds ratios (99% confidence intervals) for the covariates predicting latent profile membership.
The Low symptom profile could be differentiated from two moderate symptom profiles: those in the Moderate with high avoidance profile were more likely to have CMD problems than those in the Low symptom profile; and those in the Moderate with higher NACM and AAR symptom profile were more likely to have CMD problems, but they were also more likely to have taken 5+ years to seek help for their problems than those in the Low symptom profile. The Low symptom profile could not be differentiated from the Moderate with low avoidance and the Moderate with lower NACM and AAR symptom profiles on any of the covariates.
Looking at the differences between the moderate symptom profiles, no covariates differentiated between the profiles consistently and there were only few significant findings (see ).
4. Discussion
This paper was the first to use LPA to explore the heterogeneity of PTSD presentations within a sample of UK veterans seeking treatment for mental health difficulties. Given the nature of the sample (i.e. treatment-seeking military veterans), the high prevalence of probable PTSD (86.5%) and the size of the Severe symptom profile (37.57% of the sample) were not surprising. A six-profile model was found to most accurately capture the heterogeneity in PTSD symptom presentation. The profiles were named the Low symptom profile (accounting for 7.00% of the sample), the Moderate with low avoidance symptom profile (8.03%), the Moderate with high avoidance symptom profile (22.28%), the Moderate with lower NACM and AAR symptom profile (10.62%), the Moderate with higher NACM and AAR symptom profile (14.51%) and the Severe symptom profile (37.57%).
There were primarily quantitative differences in PTSD symptom cluster scores between the individual profiles, with some qualitative differences identified between the four moderate symptom profiles. Specifically, the Moderate with low avoidance profile did not differ significantly on the total PCL-5 score from the Moderate with lower NACM/AAR profile, but the latter had markedly higher scores on avoidance symptoms (Cohen’s d = 2.67). Similarly, the Moderate with high avoidance profile did not differ significantly on the total PCL-5 score from the Moderate with higher NACM/AAR profile, but the latter had markedly lower scores on avoidance symptoms (Cohen’s d = 2.95).
The current study identified six latent profiles, whereas previous studies conducted with veterans found between two and four latent classes (Hebensteit et al., Citation2014; Maguen et al., Citation2013; Naifeh et al., Citation2010; Steenkamp et al., Citation2012). It is possible that this difference resulted from the different methodologies used; the previous studies used binary indicators in the LCA, whereas the current study used continuous indicators in the LPA, which naturally provide more information and possibly enabled the identification of additional profiles.
In previous studies, the qualitative differences between the profiles were identified primarily on the emotional numbing symptoms (Hebensteit et al., Citation2014; Maguen et al., Citation2013). In the current study, the four moderate symptom profiles did differ significantly on the NACM symptom cluster scores, however, the differences in avoidance symptoms were more pronounced. This discrepancy could possibly be explained by the different PTSD symptoms assessed in the current study and the two previous ones. The current study utilized a DSM-5 (as opposed to DSM-IV) measure of PTSD, which included two additional symptoms of emotional numbing: ‘D3: distorted cognitions and blame’ and ‘D4: negative emotional state’. It is possible that the inclusion of these two symptoms lessened the differences between the profiles.
In relation to the avoidance symptoms, one previous LPA study conducted with treatment-seeking older adults identified two classes that differed in the severity of avoidance symptoms (Böttche, Pietrzak, Kuwert, & Knaevelsrud, Citation2015). The authors reasoned that the high avoidance class possibly consisted of participants with delayed onset PTSD, as avoidance symptoms have been found to develop at a later stage post-trauma in some trauma survivors (Yehuda et al., Citation2009). Unfortunately, we did not assess the onset of PTSD symptoms in our study.
The current study also found that membership in some of the profiles could be differentially predicted by certain external variables; most consistently the CMD. Specifically, individuals with CMD were more likely to be categorized into the more severe profiles (i.e. in the Moderate with high avoidance, the Moderate with higher NACM/AAR and Severe symptom profile relative to the Low symptom profile; and in the Severe symptom profile relative to the Moderate with low avoidance and the Moderate with lower NACM/AAR profiles). This association of CMD with the higher severity profiles is not surprising and concurs with previous research (Momartin, Silove, Manicavasagar, & Steel, Citation2004; Owens, Steger, Whitesell, & Herrera, Citation2009). Greater severity of PTSD may therefore be an indication that comorbidities are likely.
The majority of our participants had probable PTSD (86.5%) and all profiles except for the Low symptom profile had a mean PCL-5 score above the cut-off of 34, indicating probable PTSD (Murphy et al., Citation2017b) and warranting further assessment and possibly treatment. Despite this, not all of the profiles were equally likely to be associated with CMD. Research has shown that individuals with PTSD and comorbid depression and/or anxiety may have worse outcomes when it comes to treatments (Richardson et al., Citation2014). It is therefore important that clinicians assess for the comorbid anxiety and depression, especially with severe PTSD cases, as it may be necessary to address these comorbidities prior to delivering standardized PTSD interventions.
In the current study, none of the external variables differentiated consistently between the four moderate symptom profiles. This could imply that the profiles are not meaningfully different from each other. However, the profiles were significantly different on the majority of PTSD symptom cluster scores and some were different in relation to the age of participants, history of childhood adversities and CMD. It is possible that other variables, not examined in the current study, would reliably and consistently differentiate between the profiles. For example, Böttche et al. (Citation2015) found that individuals with lower PTSD avoidance symptoms had achieved higher education compared to those with higher PTSD avoidance symptoms. It is also possible that more clinically relevant variables, such as different types of traumatic experiences, would differentially predict membership in the profiles.
4.1. Implications
The current study has important implications for clinicians and researchers working within this field. Firstly, we reported evidence to show the applicability of a six-profile model to explain the heterogeneity of PTSD symptoms within UK veterans seeking support for mental health difficulties. Five of these profiles reported a burden of symptoms suggesting the presence of probable PTSD. The profiles differed from each other primarily in the severity of PTSD symptoms; however, there were also some qualitative differences, particularly in relation to the PTSD avoidance symptoms. Additionally, membership in the profiles with greater PTSD severity was predicted by CMD. This provides further evidence to support a move away from a ‘one-size fits all’ approach to interventions (Steenkamp, Citation2016). It may be advantageous to develop interventions that are informed not only by the diagnosis of PTSD, but also by the profile of PTSD symptoms and co-morbidities. For example, individuals in the Moderate with high avoidance symptom profile may derive greater benefits from interventions that include trauma memory processing techniques that target the avoidance symptoms (such as Prolonged Exposure, Cognitive Processing Therapy, Trauma-Focused or EMDR). Those with the highest levels of avoidance could potentially find therapies that include elements of behavioural exposure or interpersonal therapies (such as IPT-T, BEPP and STAIR-NA) valuable to increase adaptive behaviours outside of sessions. Whilst individuals with low avoidance and higher levels of negative cognition and arousal symptoms may profit from therapies that focus on cognitive restricting (such as TF-CBT or CPT) and affect regulation (such as STAIR or relaxation training). Individuals who fit in the Severe symptom profile may benefit from interventions that provide additional support to overcome difficulties associated with CMD (such as STAIR).
Secondly, data from a range of PTSD treatment outcome studies from different countries suggest that whilst the majority of veterans respond well, a sizeable minority have less favourable treatment outcomes (Creamer, Morris, Biddle, & Elliot, Citation1999; Johnson et al., Citation1996; Richardson et al., Citation2014). Further, studies using latent class models that have explored treatment trajectories with Australian, American and UK veterans have demonstrated the presence of different treatment trajectories (Currier et al., Citation2014; Murphy & Smith, Citation2018; Phelps et al., Citation2018). Exploring whether different pre-treatment LPA profiles predict treatment response could provide evidence for how best to triage individuals to different treatment pathways that are specific to their presentations.
4.2. Strengths and limitations
The current study was the first examination of the latent structure of PTSD conducted with UK military veterans. Replicating studies across different countries is important, as cultural factors may potentially influence the results, which can then lead to different conclusions and possibly different interventions. In relation to the military, there are marked differences between the US and the UK that could potentially impact upon the results. These include the different conflicts that the two countries have been involved in, the different levels of stigma associated with mental health difficulties or the differences in healthcare provision. Future comparative studies examining these and other factors could help to examine whether findings from veteran studies can be generalized across cultures.
The study also profited from recruiting a clinical sample of treatment seeking veterans that were randomly selected from a nationwide population in the UK. However, data was provided only from one time point. It would be advantageous to collect data longitudinally to examine the emerging profiles at different time points and to potentially explore participants’ transition across different profiles as well as the variables (e.g. demographics and other co-morbid difficulties) affecting this transition. For example, Steenkamp et al. (Citation2015) showed that there is great variability in PTSD symptom presentations immediately following return from deployment and screening too soon may therefore reflect transient, rather than more long-lasting, post-traumatic reactions. In the current study, participants had been out of service for an average of 18.8 years, so we can assume that their responses reflect more long-lasting reactions.
Another limitation concerns the use of the PCL-5. This is a self-report measure of PTSD that indicates probable PTSD rather than a clinical diagnosis. This may be mitigated as use of self-report measures is standard within this area and the PCL-5 has been validated against the CAPS-5 within this population (Murphy et al., Citation2017b). Finally, there may have been a number of other factors associated with profile membership that were not included in the study. For example, dissociation has been observed to predict membership in classes with a higher burden of PTSD symptoms (Armour, Karstoft, & Richardson, Citation2014; Nugent, Koenen, & Bradley, Citation2012), which warrants future research.
4.3. Conclusions
The current study was the first to use LPA to explore the heterogeneity of PTSD symptom presentations within a sample of treatment-seeking UK veterans. Whilst limitations exist, a six-profile model was found to best account for the heterogeneity in PTSD symptom cluster scores. Profiles differed primarily in the severity of PTSD symptom clusters, but some qualitative differences were also observed, primarily in relation to avoidance symptoms. CMD were associated with a greater burden of PTSD symptoms. The presence of different PTSD symptom and co-morbidity profiles implies the importance of ensuring interventions can address the diversity of presentations.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Armour, C., Karstoft, K., & Richardson, D. (2014). The co-occurrence of PTSD and dissociation: Differentiating severe PTSD from dissociative-PTSD. Social Psychiatry and Psychiatric Epidemiology, 8(1297), 1306.
- Asparouhov, T., & Muthén, B. O. (2014). Auxiliary variables in mixture modelling: 3-step approaches using Mplus. In Mplus web notes (No. 15, Version 8). Retrieved from https://www.statmodel.com/download/webnotes/webnote15.pdf
- Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). AUDIT. The alcohol use disorders identification test. Geneva: Department of Mental Health and Substance Dependence, World Health Organization.
- Bisson, J., Ehlers, A., Matthews, R., Pilling, S., Richards, D., & Turner, S. (2007). Psychological treatments for chronic post-traumatic stress disorder: Systematic review and meta-analysis. British Journal of Psychiatry, 190, 97–11.
- Bisson, J., Roberts, N., Andrew, M., Cooper, R., & Lewis, C. Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database of Systemic Reviews. 2013;(12). doi: 10.1002/14651858.CD003388.pub4.
- Böttche, M., Pietrzak, R., Kuwert, P., & Knaevelsrud, C. (2015). Typologies of posttraumatic stress disorder in treatment-seeking older adults. International Psychogeriatric, 27, 3–501.
- Brunello, N., Davidson, J., Deahl, M. P., Kessler, R. C., Mendlewicz., J., Racagni, G., … Zohar, J. (2017). Posttraumatic stress disorder: Diagnosis and epidemiology, co-morbidity and social consequences, biology and treatment. Neuropsychobiology, 43, 150–163.
- Creamer, M., Morris, P., Biddle, D., & Elliot, P. (1999). Treatment outcome in Australian veterans with combat-related posttraumatic stress disorder: A cause for cautious optimism? Journal of Traumatic Stress, 22(1), 545–558.
- Currier, J., Holland, J., Drescher, K., Elhai, J., & Elhai, J. D. (2014). Residential treatment for combat-related posttraumatic stress disorder: Identifying trajectories of change and predictors of treatment response. PLoS ONE, 9(7), e101741.
- Defence Analytical Services Agency. (2017). DASA outflow statistics. Retrieved from: https://www.gov.uk/government/statistics/uk-armed-forces-monthly-service-personnel-statistics-2017
- Goldberg, D., & William, P. (1998). A users’ guide to the general health questionnaire. Windsor: NFER-Nelson.
- Hebensteit, C., Madden, E., & Maguen., S. (2014). Latent classes of PTSD symptoms in Iraq and Afghnistan female veterans. Journal of Affective Disorders, 166, 132–138.
- Iversen, A., Dyson, C., Smith, N., Greenberg, N., Walwyn, R., Unwin, C., … Wessely, S. (2005). ‘Goodbye and good luck’: The mental health needs and treatment experiences of British ex-service personnel. British Journal of Psychiatry, 186(June), 480–486.
- Iversen, A., Fear, N., Simonoff, E., Hull, L., Horn, O., Greenberg, N., … Wessely, S. (2007). Influence of childhood adversity on health among male UK military personnel. British Journal of Psychiatry, 191, 506–511.
- Iversen, A. C., van Staden, S. L., Hughes, J. H., Greenberg, N., Hotopf, M., Rona, R. J., … Fear, N. T. (2011). The stigma of mental health problems and other barriers to care in the UK armed forces. BMC Health Services Research, 11, 31.
- Johnson, D., Rosenheck, R., Fontana, A., Lubin, H., Charney, D., & Southwick, S. M. (1996). Outcome of intensive inpatient treatment for combat-related posttraumatic stress disorder. American Journal of Psychiatry, 153, 771–777.
- Maguen, S., Madden, E., Bosch, J., Galatzer-Levy, I., Knight, S., Litz, B., … McCaslin, S. E. (2013). Killing and latent classes of PTSD symptoms in Iraq and Afghanistan veterans. Journal of Affective Disorders, 145, 344–348.
- Momartin, S., Silove, D., Manicavasagar, V., & Steel, Z. (2004). Comorbidity of PTSD and depression: Associations with trauma exposure, symptom severity and functional impairment in Bosnian refugees resettled in Australia. Journal of Affective Disorders, 80, 231–238.
- Murphy, D., Ashwick, R., Palmer, E., & Busuttil, W. (2017a). Describing the profile of a population of UK veterans seeking support for mental health difficulties. Journal of Mental Health. doi:10.1080/09638237.2017.1385739
- Murphy, D., Ross, J., Ashwick, R., Armour, C., & Busuttil, W. (2017b). Exploring optimum cut-off scores to screen for probable posttraumatic stress disorder within a sample of UK treatment-seeking veterans. European Journal of Psychotraumatology, 8(1), 1398001.
- Murphy, D., & Smith, K. (2018). Treatment efficacy for UK veterans with posttraumatic stress disorder: Latent class trajectories of treatment response and their predictors. Journal of Traumatic Stress, 22(1), 11–19.
- Murphy, D., Spencer-Harper, L., Carson, C., Palmer, E., Hill, K., Sorfleet, N., … Busuttil, W. (2016). Long-term responses to treatment in UK veterans with military-related PTSD: An observational study. BMJ Open, 6(e011667). doi:10.1136/bmjopen-2016-011667
- Muthén, L. K., & Muthén, B. O. (2007). MPlus. Mplus, Version 3.
- Naifeh, J. A., Richardson, D., Del Ben, K. S., & Elhai, J. (2010). Heterogeneity in the latent structure of PTSD symptoms among Canadian veterans. Psychological Assessment, 23(3), 666–674.
- Nugent, N., Koenen, K., & Bradley, B. (2012). Heterogeneity of postraumatic stress symptoms in a highly traumatized low income, urban, African American sample. Journal of Psychiatric Research, 46(12), 1576–1583.
- Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14(4), 535–569.
- Nylund, K. L., Bellmore, A., Nishina, A., & Graham, S. (2007). Subtypes, severity, and structural stability of peer victimization: What does latent class analysis say? Child Development, 78, 1706–1722.
- Owens, G. P., Steger, M. F., Whitesell, A. A., & Herrera, C. J. (2009). Posttraumatic stress disorder, guilt, depression and meaning in life among military veterans. Journal of Traumatic Stress, 22(6), 654–657.
- Phelps, A., Steel, Z., Metcalf, O., Alkemade, N., Kerr, K., O’Donnell, M., … Forbes, D. (2018). Key patterns and predictors of response to treatment for military veterans with post-traumatic stress disorder: A growth mixture modelling approach. Psychological Medicine, 48(1), 95–103.
- Pinder, R., Murphy, D., Iversen, A., Wessely, S., & Fear, N. (2011). Social exclusion amongst UK ex-service personnel based on measures of employment. Occupational & Environmental Medicine, 68(Supplement 1), A50.
- Richardson, D., Contractor, A., Armour, C., St Cyr, K., Elhai, J., & Sareen, J. (2014). Predictors of long-term treatment outcome in combat and peacekeeping veterans with military-related PTSD. The Journal of Clinical Psychiatry, 75(11), 1299–1305.
- Steenkamp, M. (2016). True evidence-based care for posttraumatic stress disorder in military personnel and veterans. JAMA, 73(5), 431–432.
- Steenkamp, M., Boasso, A., Nash, W., Larson, J., Lubin, R., & Litz, B. (2015). PTSD symptom presentation across the deployment cycle. Journal of Affective Disorders, 176, 87-94. doi:10.1016/j.jad.2015.01.043
- Steenkamp, M., Nickerson, A., Maguen, S., Dickstein, B., Nash, W., & Litz, B. (2012). Latent classes of PTSD symptoms in Vietnam veterans. Behavior Modification, 36(6), 857–874.
- Weathers, F., Litz, B., Keane, T., Palmieri, T., Marx, B., & Schnurr, P. (2013). The PTSD checklist for DSM-5 (PCL-5). In Scale available from the national center for PTSD. Retrieved from www.ptsd.va.gov
- Yehuda, R., Bierer, L., Andrew, R., Schmeidler, J., & Seckl, J. (2009). Enduring effects of severe developmental adversity, including nutritional deprivation, on cortisol metabolism in aging holocaust survivors. Journal of Psychiatric Research, 43, 877–883. doi:10.1016/j.jpsychires.2008.12.003