
ABSTRACT
Background: Previous research has demonstrated heterogeneous patterns of posttraumatic stress disorder (PTSD) among children following disasters. However, no clear consensus has been reached regarding the postdisaster trajectories of PTSD among children.
Objective: The current study examined the trajectories of PTSD among children after exposure to the Wenchuan earthquake and explored potential predictors of distinct PTSD trajectories.
Methods: A four-year longitudinal study was conducted to follow 301 children who were evaluated for PTSD symptoms following the Wenchuan earthquake. Trauma exposure and some pre-existing characteristics were measured at four months after the disaster, and PTSD symptoms were measured at 4, 16, 29, 40 and 52 months after the disaster. The trajectories were identified with Latent Growth Mixture Modelling, and the predictors were explored with multinomial logistic regression.
Results: The following three latent PTSD trajectories were found among children: resilient (74.9%), relapsing (17.7%) and recovery (7.5%). Trauma exposure was more likely to be related to a more severe trajectory of PTSD, having experienced prequake trauma was more likely to be related to the recovery trajectory and school 2 was more likely to be related to the relapsing trajectory.
Conclusion: These findings provide novel insights into children’s postdisaster response patterns. Individual heterogeneity existed in posttraumatic reactions. This longer-term longitudinal study captured more detailed and accurate information about the development of these trajectories. Trauma exposure and previous traumatic experience were linked to malignant development of PTSD.
HIGHLIGHTS
• Three latent PTSD trajectories were found among children: resilient (74.9%), relapsing (17.7%) and recovery (7.5%).• The study captured more detailed and accurate information of long-term PTSD trajectories.• Trauma exposure and having experienced prequake trauma were predictors of distinct PTSD trajectories. • This study provided important clinical implications for stepped care models of intervention postdisaster.
Antecedentes: Investigaciones previas han demostrado patrones heterogéneos de trastorno de estrés postraumático (TEPT) entre los niños después de desastres. Sin embargo, no se ha alcanzado un consenso claro con respecto a las trayectorias post-desastre del TEPT entre los niños.
Objetivo: El estudio actual examinó las trayectorias de trastorno de estrés postraumático entre los niños después de la exposición al terremoto de Wenchuan y exploró los posibles predictores de distintas trayectorias de TEPT.
Métodos: Se realizó un estudio longitudinal de cuatro años para observar a 301 niños que fueron evaluados para los síntomas de TEPT luego del terremoto de Wenchuan. La exposición al trauma y algunas características preexistentes se midieron a los 4 meses después del desastre, y los síntomas del TEPT se midieron a los 4 meses, 16 meses, 29 meses, 40 meses y 52 meses después del desastre. Las trayectorias se identificaron con el Modelo Mixto de Curvas Latentes de Crecimiento y los predictores se exploraron con regresión logística multinomial.
Resultados: Se encontraron las siguientes tres trayectorias de TEPT latentes entre los niños: resilientes (74.9%), recaída (17.7%) y recuperación (7.5%). La exposición al trauma tenía más probabilidades de estar relacionada con una trayectoria más severa del trastorno de estrés postraumático (TEPT), haber experimentado un trauma previo al terremoto tenía más probabilidades de estar relacionado con la trayectoria de recuperación y la escuela 2 tenía más probabilidades de estar relacionada con la trayectoria de recaída.
Conclusion: Estos hallazgos brindan nuevas perspectivas sobre los patrones de respuesta post-desastre de los niños. La heterogeneidad individual existió en las reacciones postraumáticas. Este estudio longitudinal a más largo plazo capturó información más detallada y precisa sobre el desarrollo de estas trayectorias. La exposición al trauma y la experiencia traumática previa se relacionaron con el desarrollo maligno del TEPT.
背景:已有的研究证实了灾后儿童创伤后应激障碍(PTSD)的异质性模式。然而,关于灾后儿童创伤后应激障碍的轨迹类型还没有达成明确的共识。
目的:本研究调查了汶川地震后儿童PTSD的轨迹,并探索了不同PTSD轨迹的潜在预测因素。
方法:本研究进行了为期四年的纵向调查,对301名儿童进行了跟踪,这些儿童在汶川地震后接受了PTSD症状的评估。在灾后4个月最初测量了创伤暴露和一些人口学特征,在灾后4个月、16个月、29个月、40个月和52个月均测量PTSD症状。发展轨迹由潜在增长混合模型确定,预测因子通过逻辑回归法检验。
结果:在这些儿童中发现了以下三种潜在的PTSD轨迹:弹性(74.9%)、复发(17.7%)和恢复(7.5%)。创伤暴露高的被试更可能出现在PTSD更严重的轨迹中,经历过地震前创伤的被试更可能出现在恢复轨迹中, 而学校2的学生更可能出现在故态复发的轨迹中。
结论:研究的发现为灾后儿童反应模式提供了新的见解。创伤后反应存在个体的异质性。这项长期的纵向研究提供了关于轨迹发展更详细和准确的信息。创伤暴露及以往的创伤经历与PTSD的恶性发展有关。
1. Introduction
Exposure to disasters might pose a direct threat to individuals’ mental health (Cheng, Liang, Fu, & Liu, Citation2018; Lai, Lewis, Livings, La Greca, & Esnard, Citation2017). Among psychopathologies, posttraumatic stress disorder (PTSD) is one of the highest-concern and commonly studied disorders that can develop following disasters because it is directly related to traumatic events (Lowell et al., Citation2018). Previous research has identified a range of distinct trajectories of PTSD following natural disasters, which indicates that the course of PTSD is heterogeneous among populations (Galatzer-Levy, Huang, & Bonanno, Citation2018; Weems & Graham, Citation2014).
Bonanno (Citation2004) proposed a prototypical model suggesting four types of trajectories of psychological adaptation over the course of two years after potentially traumatic events. These trajectories are (a) resilience (persistent low symptoms over time); (b) recovery (initially elevated symptoms followed by a decrease in symptoms over time); (c) chronic (persistent elevated symptoms over time) and (d) delayed (initially low level of symptoms followed by an increase in symptoms over time). Many studies of adult responses following traumatic events have documented these four trajectories (Galatzer-Levy et al., Citation2018; Johannesson, Arinell, & Arnberg, Citation2015), while the documentation among children has been inadequate.
Nine studies on homogeneous patterns of postdisaster PTSD among children and adolescents had been published by August 2018 (Fan, Long, Zhou, Zheng, & Liu, Citation2015; Kronenberg et al., Citation2010; La Greca et al., Citation2013; Liu et al., Citation2011; McDermott, Cobham, Berry, & Kim, Citation2014; Osofsky, Osofsky, Weems, King, & Hansel, Citation2015; Self-Brown, Lai, Thompson, McGill, & Kelley, Citation2013; Weems & Graham, Citation2014; Zhou, Wu, Zhen, Wang, & Tian, Citation2018). Evidence regarding the PTSD trajectories in children was mixed in these studies. All these studies identified recovery and most identified the resilient and chronic trajectories (eight of nine studies). Seven studies identified the delayed trajectory, but three of them only found limited evidence showing that less than 5.0% of the participants studied displayed the delayed trajectory, which did not have a high degree of scalability. The relapsing/remitting trajectory was only found in one study (Fan et al., Citation2015); in the relapsing/remitting trajectory, PTSD symptoms increase again after recovering or display a cyclical course, and this trajectory was also found in a prior study among veterans (Koenen, Stellman, Stellman, & Sommer, Citation2003). Across these nine studies, there was no clear consensus regarding the postdisaster trajectories of PTSD among children.
Moreover, research also suggested that children’s PTSD trajectories following traumatic events were distinct from adults’ responses (Lai et al., Citation2017). Galatzer-Levy et al. (Citation2018) reviewed 54 studies related to the trajectories of PTSD following potential trauma among different populations and evaluated the findings. They found that the distribution of children among the different trajectories differed from that of adults; overall, children had lower probabilities of following the resilient and chronic trajectories but a higher probability of following the recovery trajectory. This difference may be due to the different psychological characteristics of children and adults. Children might be vulnerable because they lack effective coping strategies to assist in adaptation (Braun-Lewensohn, Citation2015) and are more easily exposed to ongoing vicarious trauma via TV or nonprofessional aid efforts (Yeung et al., Citation2016). Therefore, more children may be affected after disasters, and thus the proportion of resilient trajectories in children may be lower. Meanwhile, children also have a high degree of plasticity (Hochberg et al., Citation2011; Liang, Cheng, Ruzek, & Liu, Citation2019); therefore, they may recover faster after receiving psychological interventions and their PTSD symptoms may not last as long, which might be the reason for the higher proportion of children following the recovery trajectory and the lower proportion following the chronic trajectory. Due to the special psychological characteristics of children and insufficient evidence of PTSD trajectories among children, more research focusing on children is needed.
Studies on the trajectories of postdisaster PTSD among children have produced mixed results. Several potential reasons may account for these differences. First, the studies used different analytic approaches. Four of these studies used variable-centred approaches and chose trajectory categories according to a priori theoretical assumptions (Fan et al., Citation2015; Kronenberg et al., Citation2010; Liu et al., Citation2011; McDermott et al., Citation2014). Some limitations existed in these approaches, such as the inability to test potential trajectories and unstable classification results, which may change due to one measurement. Moreover, these methods may overfit the assumed categories. The theoretical assumptions and evidence were mostly based on research conducted with adults, although the patterns of children’s responses may not be similar to those of adults due to their different psychological characteristics. With the development of new analytical approaches, person-centred approaches gradually came to be widely used, and they are able to recognize heterogeneous patterns of responses according to person-level data. Five of the relevant studies used person-centred approaches, such as growth mixture modelling and group categorization (La Greca et al., Citation2013; Osofsky et al., Citation2015; Self-Brown et al., Citation2013; Weems & Graham, Citation2014; Zhou et al., Citation2018). In these studies, trajectory categories were chosen based on data-driven approaches and prior theory and evidence. Second, the study designs were different, including investigation duration and measurement intervals. Postdisaster responses vary greatly over time, so the different study designs might recognize different patterns of responses in different periods (Cheng et al., Citation2018; Osofsky et al., Citation2015). Four of the nine studies assessed the subjects at four time points, two assessed them at three time points and three assessed them at two time points. The investigation durations of these studies were mostly less than two years, and only one study had an investigation duration of three years postdisaster. Therefore, the results of most existing studies were the early PTSD trajectories among children following the disasters. These results might increase the proportion of children displaying the chronic trajectory and do not shed light on the long-term characteristics of PTSD trajectories. Third, the types and severities of disasters and the sample characteristics were different; these factors affect the level of symptoms and patterns of development (Galatzer-Levy et al., Citation2018; Lai et al., Citation2017). Meanwhile, person-centred approaches are data-driven, and the results determined by these approaches are largely influenced by the differences in disasters and sample characteristics. Consensus might only be developed by examining findings across multiple disasters and among multiple study populations.
Identifying potential predictors of PTSD trajectories postdisaster was another important consideration (Fan et al., Citation2015; Osofsky et al., Citation2015). Trauma exposure is an important risk factor for PTSD and has been demonstrated to be a potential determining factor for PTSD trajectories (Cheng et al., Citation2018; McDermott et al., Citation2014; Zhou et al., Citation2018). Low disaster trauma exposure was more likely to be related to the resilient PTSD trajectory than the other trajectories (Lai et al., Citation2017; McDermott et al., Citation2014). In addition, pre-existing characteristics of the children such as gender, age and experiencing previous trauma may be potential predictors of the postdisaster PTSD trajectory (Kronenberg et al., Citation2010; Osofsky et al., Citation2015). Female gender has been shown to be related to more severe trajectories in most studies (Fan et al., Citation2015; La Greca et al., Citation2013). However, research on the role of age has not yielded a consistent result (Kronenberg et al., Citation2010; Lai et al., Citation2017). The role of previous trauma has also been discussed; some scholars regarded previous trauma as leading to generalized vulnerability (Levy-Gigi, Richter-Levin, Okon-Singer, Keri, & Bonanno, Citation2016; Osofsky, Osofsky, & Hansel, Citation2011) to mental health problems, while others regarded it as inoculating against trauma and building resilience (Palgi, Gelkopf, Berger, Citation2015). Thus, the role of these potential predictors of PTSD trajectories needs to be further investigated.
The current study was conducted after the Wenchuan earthquake, which occurred in Sichuan Province, China, in 2008 with a magnitude of 8.0 on the Richter scale. It was the most destructive earthquake since the founding of the People’s Republic of China and the deadliest since the 1976 Tangshan earthquake. The total death toll for this disaster reached 69,227. A total of 374,643 individuals were injured and 17,923 were recorded as missing. After the disaster, many children suffered long-lasting mental health problems, including PTSD (Guo, He, Qu, Wang, & Liu, Citation2017; Liang et al., Citation2019). To understand long-term PTSD trajectories among children, we conducted a four-year longitudinal investigation starting four months after the Wenchuan earthquake. The primary aim of this study was to identify distinct trajectories of PTSD in children after the earthquake. The second aim of this study was to explore the predictors of distinct PTSD trajectories.
2. Method
2.1. Procedures and participants
The Chinese Psychological Association stipulates the following ethical regulation for postdisaster psychological assistance: when the victims live in a fixed place, a collective questionnaire assessment can be carried out. Therefore, this study started four months after the Wenchuan earthquake when the children moved into the boarding facility. At this time, the children’s mental health was urgently in need of a large-scale assessment. The children surveyed were in grades four and six from two primary schools (Chinese Academy of Sciences Beichuan Hope Primary School and Bayi Tent School) located in Beichuan County, which was the most severely affected in the disaster. Both of these two schools were located in the worst hit areas of Beichuan County, and their facilities and environment were similar after the disaster. Participants were recruited using convenience sampling. The exclusion criteria for all participants were mental retardation, a history of clinically significant head injury including those that occurred during the earthquake and neurological disorders such as encephalitis or epilepsy.
Assessments were conducted at the following five time points: four (T1; September 2008), 16 (T2; September 2009), 29 (T3; October 2010), 40 (T4; September 2011) and 52 (T5; September 2012) months after the earthquake. At T1, 326 students were recruited using convenience sampling, and 301 children (92%) completed the checklists that measured their PTSD symptoms and demographic variables at baseline. In the subsequent assessments, 134, 276, 269 and 235 students participated in each survey, respectively. There were 301, 118, 263, 253 and 218 valid longitudinal samples at each time point, and the details of the longitudinal sample are shown in . The participants (n = 301) ranged in age from 9 to 14 years (M = 12.5, SD = 1.17) at T1, and 157 (52.2%) were male. Among these 301 participants, 129 were from Chinese Academy of Sciences Beichuan Hope Primary School and 172 were from Bayi Tent School.
Figure 1. Details of the longitudinal sample.
At T1 and T2, the participants were measured collectively using questionnaires in a group format during class by interviewers, and their teachers were present in the classrooms at the same time. The teachers and the children’s parents approved their participation in the investigation. In addition, we only surveyed participants from one primary school at T2 because the other school was holding exams and was unable to arrange a time. At T3, T4 and T5, data were collected using questionnaires at the children’s homes by the interviewers in the presence of their guardians because many students had transferred to another school and some had dropped out of school. The interviewers at each wave included a postgraduate and a volunteer, both of whom were uniformly trained by the same standardized instructions. Written informed consent was obtained from all participants and their parents/teachers (at home/school) after they were clearly informed that the participants were not required to respond to any of the questions and were free to withdraw from the survey at any time. After the questionnaire was completed at each time point, the participants were told that psychologists in our team were available to provide psychological/counselling services if needed. This study design and procedures were approved by the ethics review committee of the Institute of Psychology, Chinese Academy of Sciences.
2.2. Measures
2.2.1. Trauma exposure
Trauma exposure was assessed by the second part of the University of California at Los Angeles (UCLA) PTSD reaction index for DSM-IV, revision 1 (UCLA PTSD-RI; Steinberg, Brymer, Decker, & Pynoos, Citation2004). This part comprises 13 items that encompass objective (e.g. Were you hurt badly?) and subjective (e.g. Did you feel very scared, like this was one of your most scary experiences ever?) features of the traumatic exposure. These items are scored as being present (1) or absent (0). A total score for the 13 items was used to indicate the degree of trauma exposure in the current study. The mean value for the trauma exposure level of the participants was 8.66 (SD = 2.31) at T1. According to the total score for trauma exposure and the distribution of the scores of the participants, the participants were divided into the following three groups: low level exposure (total score ≤ 6; 17.94%), intermediate level exposure (7 ≤ total score ≤ 9; 42.19%) and high level exposure (total score ≥ 10; 39.87%).
2.2.2. PTSD
The third part of the UCLA PTSD reaction index for DSM-IV (Steinberg et al., Citation2004) was administered to assess PTSD at all time points. This part is a 20-item self-reported scale that assesses PTSD symptoms in children regarding the following three criteria of the DSM-IV: re-experiencing, avoidance and hyperarousal. The items are scored on a 5-point scale ranging from 0 (none of the time) to 4 (most of the time), and the children select the point according their situation during the past month. A cutoff for the total score equal to 38 or greater was considered to indicate PTSD (Rodriguez, Steinberg, Saltzman, & Pynoos, Citation2001a, Citation2001b). The reliability and validity of the Chinese version of the UCLA PTSD-RI have been demonstrated (Fu, Cheng, Wu, & Liu, Citation2018). In the present study, the scale exhibited good internal consistency (Cronbach’s α of 0.87, 0.88, 0.89, 0.92 and 0.92 at each time point, respectively).
2.2.3. Demographic and predictor variables
Participants were required to report their gender, age and grade at each time point. Prequake trauma was also measured at T1. Participants were asked did you experience terrible events before the earthquake and their responses were scored as present (1) or absent (0). Then, the participants who indicated having experienced prequake trauma wrote down the time the event occurred and a simple description of the previous trauma. Fifty-three (17.61%) children reported that they had experienced prequake trauma. Of the prequake trauma that the participants reported, the largest proportion of the children (67%) had experienced accidents or injury (such as car accidents, near drowning), 11% had witnessed or heard trauma to a loved one, followed by the death of a relative (7%), natural disasters (7%), interpersonal violence (4%) and witnessing death (4%).
2.3. Data analyses
Mplus 7.0 software (Muthén & Muthén, Citation2012) was used to analyse our data. First, the Latent Growth Curve Model (LGCM) was used to estimate the mean development trajectory of PTSD over the course of the four years. The LGCM estimated the variations in two growth factors (the intercept and slope). Significant variations in the growth factors indicate that there were different PTSD development trajectories in the sample population in this study.
Then, Latent Growth Mixture Modelling (LGMM) was conducted to identify the PTSD trajectories over time. LGMM is a statistical approach to estimate change in individuals over time and is able to explore the existence of latent trajectories with the aim of identifying latent subpopulations. LGMM is robust at handling missing data. Moreover, Little’s Missing Completely at Random test was conducted to analyse the data missing from participants’ responses across the five measurements. The sample size and number of time points in the current study are appropriate for LGMM (Martin & Von Oertzen, Citation2015; Nylund, Asparouhov, & Muthén, Citation2007). The results revealed that the data were missing completely at random, χ2 (50) = 64.57, p = .081. Analyses conducted in Mplus 7.0 used the robust maximum likelihood (MLR) iteration procedure. Using the LGMM, we compared one to five class models that included random effects of slope and intercept. To determine the optimal number of latent classes, fit statistics, interpretability and theoretical considerations were considered and compared. The fit statistics were evaluated on the basis of lower Akaike information criteria (AIC), Bayesian information (BIC), sample size-adjusted Bayesian information criterion (a-BIC), higher entropy, a significant Vuong-Lo-Mendell-Rubin likelihood ratio test (VLMR-LRT) result and a significant bootstrap likelihood ratio test (BLRT; Lo, Mendell, & Rubin, Citation2001). Fit statistics meeting these criteria suggested that the categorization was credible, with a good fit. In addition, to increase the scalability of the research results, we also considered whether each trajectory category had a sufficient proportion of the total participants. Each category needed to have no less than 5% of the total number of participants.
To examine the relationship between the latent class variables and predictor variables, a multinomial logistic regression of the PTSD trajectories with the demographic and predictor variables was conducted. The predictors were selected based on both theoretical and statistical considerations. According to previous research, gender, grade, prequake trauma and earthquake exposure were considered potential predictors. Because of the differences in the management patterns and psychological services between the two schools, school (school 1 = Chinese Academy of Sciences Beichuan Hope Primary School; school 2 = Bayi Tent School) was also considered a potential predictor of the trajectories. Chi-square tests of these predictors among the trajectory categories were conducted, and the variables that reached significance were added into the following logistic regression analysis.
3. Results
3.1. PTSD trajectories
First, the LGCM was conducted to describe the average development of the trajectories of PTSD in children. The results showed that the PTSD slope in children was significant (β = − 0.63, p < .001). Moreover, the variance of the intercept and the variance of the slope were significant (ps < .01), which indicated that there were significant individual differences both in the initial level of PTSD and the changes in PTSD over time. This result suggested that there were different subgroups with various trajectories among the children with PTSD.
Then, the LGMM was conducted to explore the existence of latent trajectories. Five class models were tested and the fit indices of these models are presented in . The 2- to 4-class models showed relatively good fit to the data, as indicated by the lower AIC and BIC values and higher entropy values. However, the 4-class and 5-class models had some categories with small proportions of the total sample population that were less than 5%; thus, we did not consider the 4-class model. Comparing the 2-class and 3-class models, the fit indices of BIC, entropy and VLMR-LRT indicated that the 2-class model was a better fit to the data, while the fit indices of AIC, a-BIC and BLRT indicated that the 3-class model had a better fit. Based on current theory, the 3-class model identified a category that was not in the 2-class model, which accounted for 17.7% of the study population. This was a large proportion of the total population and should not be ignored. Thus, the 3-class model was determined to be the optimal model that characterized children’s PTSD trajectories over the four-year study period after an earthquake.
Table 1. Goodness of fit statistics for each class solution (n = 301).
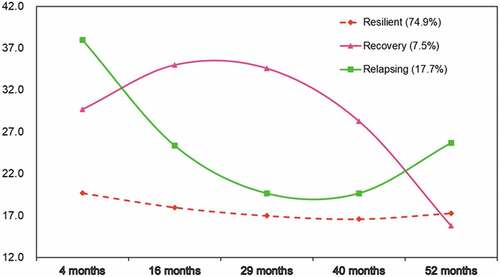
As shown in , the following three PTSD trajectories were identified: (1) the resilient trajectory (accounting for 74.9%), which was characterized by continuously low and stable PTSD scores over time; (2) the recovery trajectory (accounting for 7.5%), which was characterized by a high level of symptoms at the beginning that decreased to a normal level over time; (3) the relapsing trajectory (accounting for 17.7%), which was characterized by a high PTSD score at T1 that decreased to a low level until T3 but then increased again from T4 to T5.
Figure 2. PTSD trajectories in children.
3.2. Predictors of the trajectory class
The χ2 tests of demographic characteristics and predictors among the three types of trajectories are shown in . We included the variables that reached significance in the logistic regression analysis. Because some prior studies found that age was associated with risk of PTSD (Tang, Deng, Glik, Dong, & Zhang, Citation2017) and that students in different grades faced different degrees of academic pressure, we also added the variable of grade to the logistic regression, although the χ2 test of grade among the three types was not significant.
Table 2. Trajectories of PTSD according to demographics and predictors.
Three significant predictors of PTSD trajectories were found. The results of the multinomial logistic regression are shown in . Trauma exposure was significantly predictive of all three trajectories. Compared to the relapsing trajectory, the resilient trajectory was significantly more likely to be associated with a low level (low level vs. high level: B = 2.93, p < .01, OR = 18.66) and intermediate level (intermediate level vs. high level: B = 1.19, p < .01, OR = 3.28) of trauma exposure. Compared to the relapsing trajectory, the recovery trajectory was significantly more likely to be associated with a low level of trauma exposure (low level vs. high level: B = 2.52, p < .05, OR = 12.38). Compared to the recovery trajectory, the resilient trajectory was significantly more likely to be associated with an intermediate level of trauma exposure (intermediate level vs. high level: B = 1.25, p < .05, OR = 3.50). In general, the relapsing trajectory was associated with greater trauma severity, while the resilient trajectory was associated with lower trauma severity. Prequake trauma experience was significantly predictive of the resilient and recovery trajectories. Compared to the recovery trajectory, the resilient trajectory was significantly more likely to be associated with no prequake trauma experience (no prequake trauma vs. prequake trauma: B = 1.42, p < .05, OR = 4.13). School was also significantly predictive of all three trajectories. Compared to the relapsing trajectory, the resilient trajectory (school 1 vs. school 2, B = 1.02, p < .05, OR = 2.76) and recovery trajectory (school 1 vs. school 2, B = 1.61, p < .01, OR = 5.00) were significantly more likely to be associated with school 1 than school 2.
Table 3. Multinomial logistic regressions for predictors of PTSD trajectory.
4. Discussion
The results of the four-year longitudinal study advance our understanding of children’s postdisaster response patterns over the course of a relatively long period following a natural disaster. Following exposure to the Wenchuan earthquake, three different PTSD trajectories were identified among children. These results indicated that individual heterogeneity existed in posttraumatic reactions.
A large number of children (74.9%) demonstrated the resilient trajectory, exhibiting a stable low level of symptoms. Our study found a relatively higher proportion of children exhibiting the resilient trajectory than the proportions found in most other studies on PTSD in children (40–80%; Fan et al., Citation2015; La Greca et al., Citation2013). There were two main reasons for this finding. First, few deaths and injuries occurred in the two schools we surveyed. Second, the state and the public provided excellent support and attention to victims of the Wenchuan earthquake, which might have had positive psychological impacts on these individuals (Fan et al., Citation2015; Liang et al., Citation2019).
The recovery trajectory was observed in 7.5% of the present sample; this trajectory is characterized by an initial increase in symptoms over the first two years followed by a decrease in symptoms to a relatively low level. The proportion of the study population exhibiting this trajectory was smaller than those identified in previous studies (Lai et al., Citation2017; Self-Brown et al., Citation2013). The main reason for this finding was that the shape of the recovery trajectory in the present sample was not exactly the same as the shapes of the recovery trajectories in previous studies. In the first two years, this trajectory was characterized by an overall high and increasing symptom level. Meanwhile, the proportion of the study population exhibiting the recovery trajectory in the present sample was similar to proportion exhibiting the delayed trajectory in previous studies (Weems & Graham, Citation2014; Zhou et al., Citation2018). The similarity of shape in the early period and the proportion might reflect the fact that the recovery trajectory in the current study is the continuation of the delay trajectory in other short-term studies.
A third trajectory (17.7%) showed an initially high level of symptoms followed by a steep decrease in symptom and then a subsequent increase to an intermediate level of symptoms later in the period (relapsing). This relapsing class was rarely found in previous studies (Fan et al., Citation2015; Koenen et al., Citation2003). Both the study by Fan et al. and the study by Koenen et al. used variable-centred analytic approaches that were limited by unstable results, so there were certain methodological limitations to generalizing regarding the existence of this trajectory. The present study using person-centred approaches more strongly confirmed the existence of this response pattern. Including our study, all the research that identified relapsing class was conducted over a long duration. School was found to be an important distinguishing factor in the current study. Specifically, students in school 2 were more likely to develop the relapsing trajectory (7.75% students in school 1 and 20.93% students in school 2 belonged to the relapsing trajectory). To understand whether there were differences in important variables between the students in the two schools at the beginning of the survey, we conducted further analyses. The results showed that there were no significant differences in gender, age and trauma exposure at T1 between the students from the two schools (ps < .08) but the students in school 2 had higher PTSD symptoms (PTSS) at T1 (Mschool 1 = 22.54, SD = 10.55; Mschool 2 = 26.59, SD = 11.83; t = – 3.08, p = .002). All of these students were in the worst hit areas of Beichuan County and experienced similar levels of earthquake exposure (Mschool 1 = 8.48, SD = 2.32; Mschool 2 = 8.81, SD = 2.30; t = −1.33, p = .186). One potential reason for the difference in PTSD symptoms at four months is because the classes and teachers in school 1 were almost the same as before the earthquake, whereas the students and teachers in school 2 were integrated from several different schools (due to severe earthquake damage, the local government could not be responsible for the reconstruction of all schools. School 2 was a construction aid project and was supervised by the relevant department from other places). Therefore, compared to the students from school 1, the students from school 2 were relocated to a new school and received lower peer social support, which might have led to their higher PTSD symptoms (Hansel, Osofsky, Osofsky, & Friedrich, Citation2013; Ma et al., Citation2011). To understand whether the initial PTSS affected the relapsing trajectory, we included PTSS-T1 as a control variable in the regression model (for results, see Supplementary Table 2). Several changes were found in the new model. PTSS was significantly predictive of three PTSD trajectories and trauma exposure no longer predicted three PTSD trajectories, which indicated that the influence of traumatic exposure on PTSD trajectories is through the initial PTSS. More importantly, school no longer distinguished relapsing and resilient trajectories. These changes indicated that the reason more students in school 2 belonged to the relapsing rather than the resilient trajectory was because of initial higher PTSS, which is the prerequisite for the relapsing trajectory. Meanwhile, school still distinguished the relapsing and recovery trajectories. This may be because school 1 had more positive support, such as peer social support and psychological services. After the earthquake, school 1 received relatively sufficient psychological services, while the department that managed school 2 was relatively weak in terms of the psychological services it provided, which might explain why the students in school 1 showed better psychological recovery than those in school 2.
The relapsing trajectory in the present sample showed a recovery trend for the first two years and a symptom recurrence starting three years after the earthquake. The most potential reason triggering the relapsing of PTSD symptoms is major life stressors. Prior studies have suggested that the recurrence of PTSD symptoms is largely related to the presence of secondary stressors following traumatic events (Fan et al., Citation2015; Neria, DiGrande, & Adams, Citation2011). The students were in grade 7 and 9 at T4, which are two grades characterized by higher stress. Students in grade 7 need to adapt to a new school environment, and students in grade 9 face high academic stress because they need to undergo senior high school entrance examinations. Further data analysis found that a larger proportion of grade 9 students belonged to the relapsing trajectory than those in grade 7 (19.46% in grade 9 and 9.48% in grade 7). These results might indicate that students with a higher level of stressors are more likely to experience PTSD symptom recurrence, which supports our hypothesis to a certain extent. Another potential reason was that the government and public provided excellent support for reconstruction in the early years after the earthquake, while the amount of help provided gradually decreased thereafter (Liu, Citation2012). The available resources and social support in the early period might slow the development of symptoms in children. After the help was no longer available, some children felt the loss and changes in life brought about by the earthquake, which led to a recurrence of PTSD symptoms. Thus, the relapsing trajectory suggests that major life events postquake are important, and concern and support need to be provided to victims in the disaster area over the long term.
Overall, the types of trajectories found in the present study were not completely consistent with those identified in previous studies PTSD trajectories in children (La Greca et al., Citation2013; Self-Brown et al., Citation2013). One important reason was that most of the prior studies investigating PTSD trajectories were conducted within one to two years after the disasters, while we conducted the study for a longer period. Over the course of the four-year investigation, we found more complex and accurate trajectory patterns. If the study had only been conducted in the two years immediately following the earthquake, the relapsing trajectory might be identified as the recovery trajectory, and the recovery trajectory might be identified as the delayed or chronic trajectory; in addition, the proportion of the total study population exhibiting each trajectory might have been different. Therefore, longer-term longitudinal observations captured more detailed and accurate trajectory development information and better characterized the development trends of PTSD, which could have important implications for clinical work.
In addition, this study examined the predictors of trajectories. Gender and grade had no predictive effects in this study, which was not consistent with the results of some prior studies (e.g. Kronenberg et al., Citation2010; Lai et al., Citation2017). The two grades surveyed in this study were close to each other (4th and 6th grades), and the children were also young, which might have contributed to these results. Trauma exposure was significantly predictive of three PTSD trajectories in the present sample. The results indicated that higher levels of trauma exposure were more likely to be related to more severe trajectories, which supported the dose–response model between trauma exposure and childhood PTSD; more stressful traumatic events could lead to the more severe posttraumatic reactions (Furr, Comer, Edmunds, & Kendall, Citation2010). The Wenchuan earthquake caused destructive damage and tremendous losses due to its high magnitude. More exposure to trauma might indicate a greater risk to an individual’s life, which causes a direct threat and results in fear, thereby increasing the severity of PTSD (Liang et al., Citation2019). In addition, having experienced prequake trauma was significantly predictive of the recovery and resilient trajectories. Compared to the resilient trajectory, the recovery trajectory was more likely to be associated with having experienced prequake trauma. This result supports the generalized vulnerability hypothesis (Daskalakis, Bagot, Parker, Vinkers, & de Kloet, Citation2013; Levy-Gigi et al., Citation2016). Previous traumatic experiences could impair individuals’ mental health and functioning, which might lead to generalized vulnerability (Berntsen et al., Citation2012; Olff, Polak, Witteveen, & Denys, Citation2014). Furthermore, some prior research indicated that the premise of early trauma promoting resilience was based on experiencing similar challenges in later life (Daskalakis et al., Citation2013; Levy-Gigi et al., Citation2016). As the children surveyed in the present study had not experienced an earthquake before, their previous traumatic experiences could not build resilience in recovering from this disaster.
Several limitations of our study need to be acknowledged. First, no data were collected before the earthquake, and the prequake trauma was also measured through the children’s recollections, which were limited in their ability to facilitate a pre- and postquake comparison of the children’s’ mental health statuses. Second, all measures relied on self-reporting questionnaires rather than clinical interviews, which were dependent on individuals’ subjective reports and had potential reporting bias. Third, although our observations lasted for a relatively long period of time, longer-term studies are still needed. We found that a recurrence of symptoms in the later stages of the relapsing trajectory, and the continued development of this trajectory needs to be studied. Fourth, postquake traumatic experience is an important risk factor for PTSD (Guo et al., Citation2017) but was not measured in the present study. A prior study investigating children’s PTSD trajectories during a relative long period (from 12 months to 48 months after hurricane exposure) found different trajectories to those reported in the current study: resilient (52%), recovery (21%), delayed (18%) and chronic (9%) (Osofsky et al., Citation2015). The major difference between Osofsky et al.’s study and our study is that another technological disaster, the Gulf Oil Spill, occurred (April 2010) before the second survey time (September 2010) in the Osofsky et al. study. Multiple traumas could explain the greater proportion of malignant trajectories in the Osofsky et al. study. Furthermore, Osofsky et al. found that both oil spill stress and hurricane exposure had an effect on PTSD symptom levels and trajectories, suggesting a dose effect. Therefore, traumatic experience following a disaster needs to be considered in further studies. Last, in the current study, we found that the students in the school with better psychological intervention and peer social support networks had lower PTSD symptoms, which might indicate that positive support has protective effects on PTSD. Psychological interventions play a crucial role in PTSD remission and recovery (Liang et al., Citation2019; Zhu et al., Citation2014). Some indigenous activity has also been able to improve victims’ mental health through the role of social support (Zhu, Wu, Wang, Shi, & Zhang, Citation2009). Thus, the impact of these supporting activities on PTSD trajectories should be examined more definitively using more accurate measurements in the future.
Despite these limitations, the current study has significant theoretical and practical implications. The most significant contribution of this study was the relatively long postquake period over which it detailed the PTSD, which complemented the previous short-term models of PTSD trajectories. The results suggested that the shape of long-term PTSD trajectories might be more complicated and that the proportion of the study population exhibiting each trajectory could differ from the conclusions drawn on short-term studies. This study also provided important clinical implications for stepped care models of intervention postdisaster. Overall, 82% of children exhibiting the resilient and recovery trajectories reached low levels of PTSD symptoms at the last time point, which indicated that most children may have good mental health statuses four years after an earthquake. It is worth noting that the children exhibiting the recovery trajectory reported high levels of PTSD symptoms in the first two years, and the children exhibiting the relapsing trajectory experienced a recurrence of symptoms at three years postquake, which might suggest the importance of our early psychological intervention and the influence of major stressors postquake. Overall, these results suggest that intensive interventions need to be conducted in the early stages following a disaster, and mental health screening should also be conducted to find high-risk populations in the later stages to provide necessary psychological assistance.
5. Conclusion
The following three latent PTSD trajectories were found among children in a four-year longitudinal investigation following the Wenchuan earthquake: resilient (74.9%), relapsing (17.7%) and recovery (7.5%). Additionally, trauma exposure, having experienced prequake trauma and the school were predictors of distinct PTSD trajectories. Through this long-term investigation, we captured more detailed and accurate information of long-term PTSD trajectories and provided novel insights into children’s postdisaster response patterns.
Supplemental Material
Download MS Word (19.4 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
References
- Berntsen, D., Johannessen, K. B., Thomsen, Y. D., Bertelsen, M., Hoyle, R. H., & Rubin, D. C. (2012). Peace and war: Trajectories of posttraumatic stress disorder symptoms before, during, and after military deployment in Afghanistan. Psychological Science, 23, 1557–11.
- Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist, 59, 20–28.
- Braun-Lewensohn, O. (2015). Coping and social support in children exposed to mass trauma. Current Psychiatry Reports, 17, 1–10.
- Cheng, J., Liang, Y., Fu, L., & Liu, Z. (2018). Posttraumatic stress and depressive symptoms in children after the Wenchuan earthquake. European Journal of Psychotraumatology, 9, 1472992.
- Daskalakis, N. P., Bagot, R. C., Parker, K. J., Vinkers, C. H., & de Kloet, E. R. (2013). The three-hit concept of vulnerability and resilience: Towards understanding adaptation to early-life adversity outcome. Psychoneuroendocrinology, 38, 1858–1873.
- Fan, F., Long, K., Zhou, Y., Zheng, Y., & Liu, X. (2015). Longitudinal trajectories of post-traumatic stress disorder symptoms among adolescents after the Wenchuan earthquake in China. Psychological Medicine, 45, 2885–2896.
- Fu, L., Cheng, J., Wu, S. M., & Liu, Z. K. (2018). Validity and reliability of Chinese version of the university of California at Los Angeles posttraumatic stress disorder reaction index for DSM-IV. Chinese Mental Health Journal, 32, 160–165.
- Furr, J. M., Comer, J. S., Edmunds, J. M., & Kendall, P. C. (2010). Disasters and youth: A meta-analytic examination of posttraumatic stress. Journal of Consulting & Clinical Psychology, 78, 765–780.
- Galatzer-Levy, I. R., Huang, S. H., & Bonanno, G. A. (2018). Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clinical Psychology Review, 63, 41–55.
- Guo, J., He, H., Qu, Z., Wang, X., & Liu, C. (2017). Post-traumatic stress disorder and depression among adult survivors 8 years after the 2008 Wenchuan earthquake in China. Journal of Affective Disorders, 210, 27–34.
- Hansel, T. C., Osofsky, J. D., Osofsky, H. J., & Friedrich, P. (2013). The effect of long‐term relocation on child and adolescent survivors of hurricane Katrina. Journal of Traumatic Stress, 26, 613–620.
- Hochberg, Z. E., Feil, R., Constancia, M., Fraga, M., Junien, C., Carel, J. C., ... Albertsson-Wikland, K. (2011). Child health, developmental plasticity, and epigenetic programming. Endocrine Reviews, 32, 159–224.
- Johannesson, K. B., Arinell, H., & Arnberg, F. K. (2015). Six years after the wave. Trajectories of posttraumatic stress following a natural disaster. Journal of Anxiety Disorders, 36, 15–24.
- Koenen, K. C., Stellman, J. M., Stellman, S. D., & Sommer, J. F. (2003). Risk factors for course of posttraumatic stress disorder among vietnam veterans: A 14-year follow-up of american legionnaires. Journal of Consulting & Clinical Psychology, 71, 980–986.
- Kronenberg, M. E., Hansel, T. C., Brennan, A. M., Osofsky, H. J., Osofsky, J. D., & Lawrason, B. (2010). Children of Katrina: Lessons learned about postdisaster symptoms and recovery patterns. Child Development, 81, 1241–1259.
- La Greca, A. M., Lai, B. S., Llabre, M. M., Silverman, W. K., Vernberg, E. M., & Prinstein, M. J. (2013). Children’s postdisaster trajectories of PTS symptoms: Predicting chronic distress. Child and Youth Care Forum, 42, 351–369.
- Lai, B. S., Lewis, R., Livings, M. S., La Greca, A. M., & Esnard, A. M. (2017). Posttraumatic stress symptom trajectories among children after disaster exposure: A review. Journal of Traumatic Stress, 30, 571–582.
- Levy-Gigi, E., Richter-Levin, G., Okon-Singer, H., Keri, S., & Bonanno, G. A. (2016). The hidden price and possible benefit of repeated traumatic exposure. Stress-The International Journal on the Biology of Stress, 19, 1–7.
- Liang, Y., Cheng, J., Ruzek, J., & Liu, Z. (2019). Posttraumatic stress disorder following the 2008 Wenchuan earthquake: A 10-year systematic review among highly exposed populations in China. Journal of Affective Disorder, 243, 327–339.
- Liu, M., Li, W., Shi, Z., Zhen, Z., Kan, Z., & Shen, J. (2011). Mental health problems among children one year after Sichuan earthquake in China: A follow-up study. PloS one, 6, e14706.
- Liu, Z. (2012). Time and space two-dimensional model of psychological assistance for major natural disasters. China Emergency Management, 2012, 41–45.
- Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of components in a normal mixture. Biometrika, 88, 767–778.
- Lowell, A., Suarezjimenez, B., Helpman, L., Zhu, X., Durosky, A., Hilburn, A., ... Neria, Y. (2018). 9/11-related PTSD among highly exposed populations: A systematic review 15 years after the attack. Psychological Medicine, 48, 537–553.
- Ma, X., Liu, X., Hu, X., Qiu, C., Wang, Y., Huang, Y., ... Li, T. (2011). Risk indicators for post-traumatic stress disorder in adolescents exposed to the 5.12 Wenchuan earthquake in China. Psychiatry Research, 189, 385–391.
- Martin, D. P., & Von Oertzen, T. (2015). Growth mixture models outperform simpler clustering algorithms when detecting longitudinal heterogeneity, even with small sample sizes. Structural Equation Modeling: A Multidisciplinary Journal, 22, 264–275.
- McDermott, B., Cobham, V., Berry, H., & Kim, B. (2014). Correlates of persisting posttraumatic symptoms in children and adolescents 18 months after a cyclone disaster. Australian and New Zealand Journal of Psychiatry, 48, 80–86.
- Muthén, L. K., & Muthén, B. O. (2012). Mplus statistical modeling software: Release 7.0. Los Angeles, CA: Muthén & Muthén.
- Neria, Y., DiGrande, L., & Adams, B. G. (2011). Posttraumatic stress disorder following the September 11, 2001, terrorist attacks: A review of the literature among highly exposed populations. American Psychologist, 66, 429–446.
- Nylund, K. L., Asparouhov, T., & Muthén, B. O. (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal, 14, 535–569.
- Olff, M., Polak, A. R., Witteveen, A. B., & Denys, D. (2014). Executive function in posttraumatic stress disorder (PTSD) and the influence of comorbid depression. Neurobiology of Learning & Memory, 112, 114–121.
- Osofsky, H. J., Osofsky, J. D., & Hansel, T. C. (2011). Deepwater Horizon oil spill: Mental health effects on residents in heavily affected areas. Disaster Medicine and Public Health Preparedness, 5, 280–286.
- Osofsky, J. D., Osofsky, H. J., Weems, C. F., King, L. S., & Hansel, T. C. (2015). Trajectories of post-traumatic stress disorder symptoms among youth exposed to both natural and technological disasters. Journal of Child Psychology and Psychiatry, 56, 1347–1355.
- Palgi, Y., Gelkopf, M., & Berger, R. (2015). The inoculating role of previous exposure to potentially traumatic life events on coping with prolonged exposure to rocket attacks: A lifespan perspective. Psychiatry Research, 227, 296–301.
- Rodriguez, N., Steinberg, A. M., Saltzman, W. S., & Pynoos, R. S. (2001b). Youth PTSD Assessment: Psychometric investigation of PTSD self-report instruments. In 17th Annual ISTSS Meeting, New Orleans.
- Rodriguez, N., Steinberg, A. S., Saltzman, W. S., & Pynoos, R. S. (2001a). PTSD Index: Psychometric analyses of the adolescent version. In Symposium conducted at the annual meeting of the International Society for Traumatic Stress Studies, New Orleans, LA.
- Self-Brown, S., Lai, B. S., Thompson, J. E., McGill, T., & Kelley, M. L. (2013). Posttraumatic stress disorder symptom trajectories in Hurricane Katrina affected youth. Journal of Affective Disorders, 147, 198–204.
- Steinberg, A. M., Brymer, M. J., Decker, K. B., & Pynoos, R. S. (2004). The University of California at Los Angeles post-traumatic stress disorder reaction index. Current Psychiatry Reports, 6, 96–100.
- Tang, B., Deng, Q., Glik, D., Dong, J., & Zhang, L. (2017). A meta-analysis of risk factors for post-traumatic stress disorder (PTSD) in adults and children after earthquakes. International Journal of Environmental Research and Public Health, 14, 1537.
- Weems, C. F., & Graham, R. A. (2014). Resilience and trajectories of posttraumatic stress among youth exposed to disaster. Journal of Child and Adolescent Psychopharmacology, 24, 2–8.
- Yeung, N. C. Y., Lau, J. T. F., Yu, N. X., Zhang, J., Xu, Z., Choi, K. C., et al. (2016). Media exposure related to the 2008 Sichuan earthquake predicted probable PTSD among Chinese adolescents in Kunming, china: A longitudinal study. Psychological Trauma Theory Research Practice & Policy, 10, 253–262.
- Zhou, X., Wu, X., Zhen, R., Wang, W., & Tian, Y. (2018). Trajectories of posttraumatic stress disorders among adolescents in the area worst-hit by the Wenchuan earthquake. Journal of Affective Disorders, 235, 303–307.
- Zhu, Z., Wang, R., Kao, H. S., Zong, Y., Liu, Z., Tang, S., ... Lam, S. (2014). Effect of calligraphy training on hyperarousal symptoms for childhood survivors of the 2008 China earthquakes. Neuropsychiatric Disease and Treatment, 10, 977–985.
- Zhu, Z. H., Wu, S. T., Wang, W. Z., Shi, Z. B., & Zhang, J. X. (2009). Mahjong play and cigarette/alcohol use affect mental health of people in Sichuan earthquake area. Advances in Psychological Science, 17, 551–555.