
ABSTRACT
Background: Nightmares are a widespread phenomenon. In comparison to the general population, they occur in mentally ill and especially in traumatized individuals with an increased frequency. Despite the high prevalence, there is no short questionnaire in the German language that is able to characterize nightmares, to differentiate between different nightmare types and to assess their impact on daytime functioning.
Objective: The Hamburg Nightmare Questionnaire (HNQ) has been developed as a short self-rating instrument to fill this gap.
Method: Psychometric characteristics of the HNQ were evaluated in a sample of 707 German soldiers passing through the standard diagnostics of the Center for Mental Health at the German Armed Forces Hospital Hamburg.
Results: The results of this study show satisfactory psychometric characteristics as a sound factorial structure and adequate internal consistency for the HNQ as well as initial indications of the construct validity of its subscales.
Conclusions: The HNQ is a reliable and economic tool for the assessment of posttraumatic nightmares in clinical as well as research settings.
HIGHLIGHTS
• The Hamburg Nightmare Questionnaire (HAFB) is a new and short assessment tool for nightmares in clinical and research settings.• HAFB assesses frequency and duration of nightmare occurrence.• HAFB subscales cover the areas of emotional (e.g. fear) and psychophysiological (e.g. heart racing) reactions, dream content, reorientation after awakening and clarity of dream recall.• HAFB measures impairment in areas of everyday functioning such as family life or physical performance resulting from nightmares.
Antecedentes: Las pesadillas son un fenómeno ampliamente generalizado. En comparación con la población general, las pesadillas ocurren con una mayor frecuencia en personas con enfermedad mental y, especialmente, en personas traumatizadas. A pesar de su alta prevalencia, no existe ningún cuestionario breve en idioma alemán que sea capaz de caracterizar las pesadillas, diferenciarlas en tipos, y evaluar su impacto sobre la funcionalidad durante el periodo de vigilia.
Objetivo: Se desarrolló el Cuestionario de Pesadillas de Hamburgo (HNQ, por sus siglas en inglés) como un instrumento de valoración breve auto-aplicado para subsanar esta brecha.
Método: Se evaluaron las características psicométricas del HNQ a partir de una muestra de 707 soldados alemanes que eran sometidos a los diagnósticos estándar del Centro para la Salud Mental del Hospital de Hamburgo de las Fuerzas Armadas Alemanas.
Resultados: Los resultados de este estudio mostraron características psicométricas satisfactorias, tales como una firme estructura factorial y una adecuada consistencia interna para el HNQ, así como indicadores iniciales de la validez del constructo de sus subescalas.
Conclusiones: El HNQ es una herramienta confiable y económica para la evaluación de pesadillas postraumáticas tanto en el ámbito clínico como en el de investigación.
背景:噩梦是一种普遍存在的现象。与一般人群相比,在精神病患者身上,特别是在受创伤的人群中噩梦出现更频繁。尽管噩梦的发生率很高,但在德语中还没有简短的问卷调查表能够描述噩梦、区分不同的噩梦类型,并评估它们对日间功能的影响。
目标:以填补这一空白,我们开发了汉堡噩梦问卷(HNQ)作为一个简短的自我评估工具。
方法:经过德国汉堡武装部队医院的心理健康中心的标准诊断后,在707名德国士兵样本中进行了HNQ的心理测量特征评估。
结果:结果显示出令人满意的心理测量特征:HNQ的因子结构合理,并且内部一致性较好。并且有初始指标显示了其分量表的结构效度。
结论:HNQ是一种可在临床和研究环境中评估创伤后噩梦的可靠而经济的工具。
关键词:
1. Introduction
Dreams whose negative effects cause an awakening are called nightmares (Schredl, Citation2018). Representative epidemiological studies (e.g. Schredl, Citation2010) describe that up to 5% of the general population suffer from nightmares. This prevalence is strongly elevated in patients in psychiatric treatment (27.7% in patients without a PTSD diagnosis; Swart, van Schagen, Lancee, & van Den Bout, Citation2013). The prevalence of nightmares in posttraumatic stress disorder (PTSD) is 50–70% in several studies (see review by Wittmann, Schredl, & Kramer, Citation2007). Several studies document an association of PTSD severity and nightmare frequency (Blank, Kelly, Bootzin, & Haynes, Citation2009; Gerhart, Russ, Hall, & Canetti, Citation2014). Posttraumatic nightmares are a diagnostic criterion of PTSD according to ICD-10 (WHO, Citation2004) and DSM-5 (APA, Citation2013) and are considered to be emotionally the most intense type of dreaming (Levin & Nielsen, Citation2007). Accordingly, reliving of traumatic experiences in nightmares is associated with higher subjective distress in PTSD patients (Freese et al., Citation2018). Schreuder and Kleijn (Citation2001) distinguish between replicative nightmares (exact replication of a traumatic event) and non-replicative (symbolic) nightmares (dream content does not repeat the traumatic event, but refers to it by means of the associations of the dreamer). As an intermediate category that depicts elements of the traumatic event as well as deviations, these authors introduced the category of mixed-replicative nightmares.
So far, there is no specific questionnaire for the assessment and differentiation of nightmares as well as their effect on daytime functioning in German-speaking countries (Pietrowsky, Citation2011). In existing questionnaires on sleep quality such as the Pittsburgh Sleep Quality Index (PSQI; Backhaus & Riemann, Citation1999; Buysse, Reynolds, Monk, Berman, & Kupfer, Citation1989) or the sleep questionnaires by Görtelmeyer (Citation2011), indirect evidence for parasomnias can be found with singular items asking for nightmares without distinguishing their genesis or appearance.
A PSQI addendum for PTSD (Germain, Hall, Krakow, Katherine Shear, & Buysse, Citation2005) specifies the appearance of sleep disturbing events by means of two items. Item 1 assesses the frequency of hot flashes, general nervousness, memories or nightmares of a traumatic experience, bad dreams and panic attacks not related to a traumatic event, pavor nocturnus and acting out dreams during the last month. Individuals reporting posttraumatic memories/nightmares are requested to specify the intensity of anxiety and anger as well as the time of night of the sleep disturbance. The PSQI addendum does not consider the type of relation between dream content and traumatic event. To the best of our knowledge, a validated German version is not available.
Similarly, the Munich Parasomnia Screening (Fulda et al., Citation2008) contains two items on nightmares but does not allow for a distinction between replicative and non-replicative nightmares. This also applies to the Questionnaire for the Assessment of Nightmares (Pietrowsky, Citation2011). The Dream Rating Scale (Esposito, Benitez, Barza, & Mellman, Citation1999), which is applied by raters on previously collected dream reports, is designed to detect pathological trauma-associated dream content in soldiers with PTSD. However, this instrument requires considerable time and effort (rater training required; Davis, Citation2009). The Nightmare Effects Questionnaire (Schlarb, Zschoche, & Schredl, Citation2016) assesses by means of six items the frequency of different dream types in adolescents and adults. In a second section, 35 items elicit the effects of nightmares on the areas of emotion regulation, stress and aggression, depression, attention/concentration, anxiety and hyperactivity.
Donovan, Padin-Rivera, Chapman, Strauss, and Murray (Citation2005) developed the Nightmare Intervention & Treatment Evaluation Scale (NITE) with the goal of a detailed analysis of the effects of posttraumatic nightmares and the impact of interventions. Since the NITE scale was developed working with American veterans with a PTSD diagnosis and has been shown to be reliable in this patient group, it was translated into German in a preliminary study (Timmann, Citation2012) adding three items according to the nightmare criteria of the ICD-10 (WHO, Citation2004) and International Classification of Sleep Disorders 2 (ICSD-2; Happe & Walther, Citation2009; Mayer, Rodenbeck, Geisler, & Schulz, Citation2015). In the German translation, the NITE scale provided similar psychometric properties as the original version, but was not appropriate for a differentiation of nightmare types. Furthermore, there was a very low acceptance of the questionnaire within the population of German soldiers. Item formulations which were perceived as implying personal weakness and the six validity items of the NITE-scale (e.g. ‘There have been times I have dialled a phone number only to find the line was busy’) evoked strong levels of irritation in this sample resulting in elevated numbers of missing values (Timmann, Citation2012).
1.1. Development of the Hamburg Nightmare Questionnaire (HNQ)
The instruments reviewed above consider nightmares and especially posttraumatic ones either with a few items only or they selectively focus on specific aspects of nightmares (e.g. as effects on daytime functioning). It was thus the aim for the development of the HNQ (German abbreviation: HAFB) to design a short self-rating scale allowing for the reliable assessment of dream characteristics, subjective experience and resulting impairment associated with the occurrence of nightmares. Furthermore, the HNQ should allow for differentiation of various nightmare types. The items were constructed based on the criteria of the second and third edition of the International Classification of Sleep Disorders (Happe & Walther, Citation2009; Mayer et al., Citation2015). At the same time, the aim was to differentiate between replicative and non-replicative nightmares. Furthermore, self-phrased items on psychophysiological and emotional involvement, on reorientation after awakening and on clarity of dream recall were constructed. In addition to these items depicting the dream content or the immediate response to it, an additional subscale was developed capturing the impairment on the functional level in different areas during the days following a nightmare occurrence.
An initial review of the content validity was carried out by presenting the test version with 61 items to a panel of experts, consisting of experienced psychiatrists and clinical psychologists at the Center for Mental Health at the Federal Armed Forces Hospital Hamburg, who are specialists in the diagnosis and treatment of PTSD. This test version was presented to volunteer soldiers (n = 200) to check for acceptance. Eight items were eliminated due to missing data and a 53-item version was submitted to a sample of patients from the Center for Mental Health at the German Armed Forces Hospital Hamburg who presented themselves for diagnosis and therapy (n = 129). Principal component analysis was conducted and all items not loading clearly on a factor were eliminated. After these steps, the HNQ with a total of 30 items was considerably shorter as compared to its initial version (Timmann, Citation2012).
The aim of the present study is to investigate the psychometric properties of the HNQ and to obtain first indications of its construct validity. In order to test the construct validity of the HNQ subscales, the following hypotheses were generated: It is expected that elevated values in the replicativity subscale are specifically related to a PTSD diagnosis, but not to other psychiatric diagnoses (Wittmann & de Dassel, Citation2015). A substantial positive correlation between the reorientation and dream recall subscales is predicted as both aspects differentiate between nightmares (clear dream memory, rapid reorientation; Schredl, Citation1999) and the phenomenon of pavor nocturnus (hardly any dream memory, difficult reorientation; Schredl, Citation1999). Positive correlations are expected for the emotional involvement subscale and the personality dimension of neuroticism (Köthe & Pietrowsky, Citation2001; Spoormaker, Citation2008) and with the nightmare impairment subscale. For the psychophysiological involvement subscale a substantial correlation is expected with the personality dimension of neuroticism (Spoormaker, Citation2008). It is also predicted that subjects with posttraumatic stress disorder will show more psychophysiological involvement as psychophysiological responsiveness is a criterion for PTSD diagnosis (APA, Citation2013).
2. Methodology
The present study was approved by the Institutional Review Board of the International Psychoanalytic University Berlin.
2.1. Sample
The psychometric evaluation of the questionnaire was based on anonymized data of all soldiers who passed through the standard diagnostics of the Center for Mental Health at the German Armed Forces Hospital Hamburg from March 2014 to December 2016. Of 1427 eligible subjects, 781 (54.7%) reported having had nightmares. Seventy-four (9.5%) of these were excluded due to missing data within the HNQ. Statistical calculations were performed on sub-samples (March–December 2014 [n = 234] and January–December 2016 [n = 473]) as well as on the total sample (n = 707). Splitting into subsamples allowed for independent exploratory and confirmatory factor analysis (see below).
2.2. Procedure
The standard diagnostic was performed immediately after admission to the Center for Mental Health at the German Armed Forces Hospital Hamburg by completing a partially computer-based set of questionnaires. Subsequent clinical interviews were conducted by the treating psychiatrists of the department. Diagnostic decisions on ICD-10 diagnoses (WHO, Citation2004) were made by taking into account the results of standard diagnostics, interview information and observations of psychiatrists, psychologists, physiotherapists and occupational therapists involved in the case.
2.3. Instruments
2.3.1 Socio-demographic information
In the context of standard diagnostics, patients’ age, sex and educational status were recorded.
2.3.2 HNQ
In the first section, patient’s name, age and sex as well as the date of the assessment are recorded (see appendix in supplementary material also). The second section of the HNQ (six items) collects general information on nightmares (screening question for the occurrence of nightmares, duration and frequency of occurrence, reliving of a real experienced event in the dream). Subsequently, the subject is asked to estimate the percentage of replicative, mixed and non-replicative nightmares with the total of these three percentages summing up to 100%. At the end of the second section, the subjects are asked to outline topics or contents of their nightmares. In the third part, 17 items on nightmare characteristics reflecting the five aspects of Emotional Involvement, Psychophysiological Involvement, Replicativity of dream content, Reorientation after awakening and Dream Recall clarity) are presented applying a 5-step Likert scale (1 = strongly disagree to 5 = strongly agree; see appendix in supplementary material). Two items of the replicativity subscale (items 13 and 16) as well as all items of dream recall subscale (items 5 and 10) need to be reversed for calculation of mean values. Thus, higher mean values represent more emotional or psychophysiological involvement, higher replicativity of dream content, impeded reorientation after awakening and a lower clarity of dream recall. In the fourth section of the HNQ, seven items evaluate the severity of the impairment in the areas of social environment, work (‘service’), family life, physical and mental performance, mood and everyday impairment overall. A 5-level Likert scale (1 = not at all to 5 = very strong) is used to measure this facet. Due to the content of sections 3 and 4 (nightmare content vs. everyday function level) and differences in response format, these seven items are presented in a separate section of the questionnaire.
2.3.3 NEO Five-Factor-Inventory
(NEO-FFI; Borkenau & Ostendorf, Citation2008): Costa and McCrae’s NEO-FFI is a multi-dimensional personality inventory that captures key areas of individual differences. The NEO-FFI captures these dimensions with its 60 items on five scales: neuroticism, extraversion, openness to experience, agreeableness and conscientiousness. The internal consistencies of the scales are between r = .72 and r = .87 (Borkenau & Ostendorf, Citation2008). In this study, only the neuroticism scale (12 items) was considered.
2.4. Data analysis
Descriptive and inferential statistics and psychometric analysis were performed using IBM SPSS Statistics version 25. Confirmatory factor analyses were calculated with IBM SPSS AMOS version 23. Based on the 2014 sample, the factorial validity of the questionnaire was examined (exploratory factor analysis [EFA], principal component analysis with Kaiser normalization and subsequent varimax rotation). The suitability of the data, i.e. the correlation matrix, for performing factor analysis was established based on the Kaiser-Meyer-Olkin (KMO) measure (KMO = 0.873) and Bartlett’s Test of Sphericity (Chi-Quadrat = 2213,6, p ≤ .001). The number of factors was determined applying the Kaiser-Guttmann-criterion (Eigenvalue > 1). Factor loadings ≥ 0.30 were considered for interpretation. Based on the sample of 2015 and 2016 patients, the replicability of the factorial structure was tested (confirmatory factor analysis [CFA]). Due to differences regarding content and response format (see section 2.3. Instruments), only the five subscales of HNQ section 3 were included into factor analyses, whereas the nightmare impairment subscale of HNQ section 4 was not. To assess the extent to which the subscale values are related to socio-demographic and psychopathological variables, a multiple regression analysis (method: enter) was performed for each subscale with the predictors age, gender, education, frequency of nightmares and presence of a PTSD diagnosis. Due to missing values among predictor variables, 43 individuals (6.1%) were excluded from these analyses. The evaluation of psychometric characteristics and construct validity of the questionnaire were based on the total sample.
3. Results
3.1. Sample characteristics
Sociodemographic characteristics of total and subsamples are reported in . There were no significant differences between the two sub-samples with regard to age or education. As for sex, there was a statistical trend (p = .07) towards a larger proportion of females in the 2014 sample. Most soldiers (95.8%) received at least one ICD-10 F-diagnosis. Mean number of ICD-10 F-diagnoses was 1.6 (SD = 0.9, Range = 0–6). Most frequently, diagnoses from clusters F1 (14.0%), F3 (43.6%), F4 (66.1%) and F6 (9.3%) were present (numbers refer to cases with at least one diagnoses from the respective cluster). In 50 cases (7.1%) a tentative or a differential diagnosis had been recorded. Soldiers of the 2014 sample obtained a mean of 1.5 (SD = 0.9) F-diagnoses, soldiers of the 2015–2016 sample a mean of 1.6 (SD = 1.0) F-diagnoses (T = −1.61, df = 500.8, p = .11, unequal variances). As for diagnoses of PTSD, the following picture was obtained: 53 (22.6%) soldiers of the 2014 sample were diagnosed to suffer from PTSD. For the 2015–2016 sample this number was significantly elevated (147 [31.1%] soldiers; Chi2 = 5.5, p < .05). There was a statistical trend (p = .06) towards a higher frequency of nightmare occurrence in the 2014 sample (). No significant group differences (p > .4) were found in regard to the neuroticism scale of the NEO-FFI (Borkenau & Ostendorf, Citation2008; M [total sample] = 60.8 [SD = 10.6]).
Table 1. Sociodemographic information and nightmare frequency.
3.2. Item characteristics and factorial validity
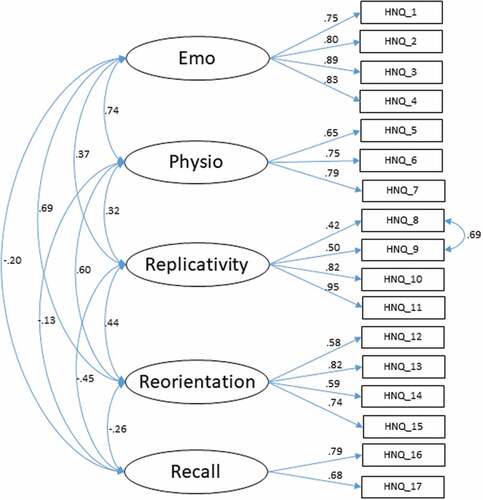
Factor loadings and item communalities are depicted in . Items are distributed on five subscales without substantial cross loadings. Variance explained by the five factors was 73.1% (emotional participation [4 items]: 18.1%, psychophysiological participation [3 items]: 12.9%, replicativity [4 items]: 16.9%, reorientation [4 items]: 15.1%, dream recall [2 items]: 10.1%). Applying CFA, this factor structure was tested using the data of the 2014–2015 sample (). Factor loads were high for all variables (Range = .42–.95), model fit indices are in the good and adequate range (Chi2 = 239.3, df = 108, Chi2/df = 2.2, GFI = .95, NFI = .94, CFI = .97, RMSEA = .05, AIC = 329.3; Schermelleh-Engel, Moosbrugger, & Müller, Citation2003). The intercorrelations of the five HNQ subscales are shown in . The emotional involvement subscale has strong correlations with the psychophysiological involvement (r = .59) and reorientation (r = .60) subscales. All other coefficients are small or moderate. The reliability (internal consistency: Cronbach’s alpha coefficient) of the individual subscales of the HNQ was in the range .70–.95, whereby values below .80 for both sub-samples are found in the psychophysiological involvement and recall subscales. No substantial differences were found between the two subsamples (). depicts means, standard deviations and corrected item-scale-correlation of the Hamburg Nightmare Questionnaire items in the study sample.
Table 2. Factor loadings and communalities of the Hamburg Nightmare Questionnaire items after principal component analysis with Kaiser-normalization with Varimax-rotation (sample 2014, n = 234).
Table 3. Inter-correlations of the Hamburg Nightmare Questionnaire subscales (total sample, n = 707).
Table 4. Internal consistency of the Hamburg Nightmare Questionnaire subscales.
Table 5. Means, standard deviations and corrected item-scale-correlation of the Hamburg Nightmare Questionnaire items in the study sample (n = 707).
Figure 1. Confirmatory factor analysis (see section 3.2 for model fit indices).
3.3. Correlates of the HNQ subscales
Depending on the subscale, the five predictors entered into the regression analyses yielded a variance explanation of 2–32% (). The frequency of nightmare occurrence and the presence of a PTSD diagnosis were the two strongest predictors in almost all regression models. Higher age was significantly associated with higher emotional and psychophysiological involvement, more replicative nightmares and greater impairment. The nightmares of male soldiers were associated with greater impairment. Education was not significantly associated with any of the HNQ subscales. More frequent nightmares predicted more involvement, more replicativity, a worse reorientation as well as more impairment. The presence of a PTSD diagnosis predicted more involvement, more replicativity, a worse reorientation after awakening, a clearer dream memory and a greater impairment.
Table 6. Multiple regression analyses of the Hamburg Nightmare Questionnaire subscales (total sample, N = 664).
Soldiers with PTSD diagnosis had significantly higher scores in the replicativity subscale relative to those without such a diagnosis (M = 3.8 (SD = 0.9, n = 188) vs. M = 2.9 (SD = 1.2, n = 506), T = −11.1, df = 420.3, p < .001, unequal variances). This finding also persists in the multivariate context as demonstrated by the respective regression analysis. In contrast, soldiers with diagnosis of agoraphobia (n = 26; t = 1.2, df = 692, p = .24) or social phobia (n = 19; t = 0.8, df = 692, p = .42) did not differ significantly in relation to the replicativity of their nightmares as compared to soldiers without these diagnoses. Thirteen soldiers with comorbidity (at least two of these three diagnoses) were excluded from these comparisons. The reorientation and dream recall subscales correlated negatively and significantly, but with a small effect size (r = −.24, p < .001, n = 707). The emotional involvement subscale correlated substantially with the personality dimension of neuroticism (r = .43, p < .001, n = 707) and strongly with the impairment resulting from nightmares (r = .69, p < .001, n = 707). The psychophysiological involvement subscale correlated significantly with the personality dimension of neuroticism (r = .32, p < .001, n = 707). Subjects with PTSD diagnosis had higher psychophysiological involvement scores compared to subjects without such a diagnosis (M = 3.4 (SD = 1.0, n = 200) vs. M = 2.7 (SD = 1.1, n = 507), T = −7.7, df = 404.0, p < .001, unequal variances). This finding also persists in the multivariate context as demonstrated by the respective regression analysis.
4. Discussion
The aim of the present study was to test the psychometric properties of the Hamburg Nightmare Questionnaire and to obtain first indications of its construct validity. Exploratory factor analysis showed a clear pattern of main factor loadings without substantial cross loadings. The replication of this five-factor solution using an independent sample showed a satisfying model fit. The internal consistencies of the subscales mostly reached from an acceptable to an excellent range. Both subscales with coefficients below .8 in both sub-samples (Psychophysiological Involvement and Dream Recall) comprise less items as compared to the other subscales which probably explains their slightly reduced reliability. The item-subscale-correlations of the 17 items in the third part of the questionnaire are consistently high.
The values in all HNQ subscales are not influenced by the educational level of the subjects. The finding that nightmares were associated with greater impairment in male as compared to female soldiers could be explained by a greater traumatization severity of male soldiers. Future studies should determine whether the association of higher age and elevated values in four of the six HNQ subscales could be explained by a higher probability of traumatic events due to more service years. The finding that presence of a PTSD diagnosis significantly and strongly predicted scores on all six subscales demonstrates the potential of the questionnaire to differentiate posttraumatic and non-traumatic nightmares in terms of the dominant nightmare type. In this context, it is interesting that, based on a previous version of the HNQ individuals with different dominant nightmare types (replicative vs. non-replicative vs. mixed) could reliably be distinguished from each other (Freese et al., Citation2018). Frequency of nightmares was the strongest predictor of impairment in different everyday areas resulting from nightmares. Further research should provide a deeper understanding of the relationship between nightmare frequency and other variables. For example, the association of nightmare frequency and replicativity could be due to the fact that subjects with PTSD diagnosis experience both more frequent and more replicative nightmares.
The hypotheses established to test the construct validity of the subscales were largely supported by the empirical evidence. As expected based on previous research (Wittmann & de Dassel, Citation2015), soldiers diagnosed with PTSD have a more replicative dream content than those without this diagnosis, while diagnoses of social or agoraphobia are unrelated to the replicativity of nightmares. This can be interpreted as a direct consequence of the occurrence of replicative nightmares in individuals with a PTSD diagnosis. Instead of the expected substantial positive correlation between the reorientation after awakening and clarity of dream recall subscales, a weak negative correlation (r = −.24) was found. The underlying hypothesis was based on the assumption that persons with pavor nocturnus achieve low values in both dimensions. For the present sample, however, it is unclear whether or to what extent subjects suffered from this disorder. In order to check whether persons suffering from pavor nocturnus actually achieve lower values on these HNQ subscales, a sleep laboratory study including patients with and without this condition is necessary. As predicted, the emotional and psychophysiological involvement subscales correlate substantially with the personality dimension of neuroticism. In accordance with our expectation, greater emotional involvement was associated with more severe impairment in the days after a nightmare. Soldiers with a PTSD diagnosis experience as predicted stronger psychophysiological responses to their nightmares, which is consistent with the diagnostic criterion of psychophysiological hyperarousal (APA, Citation2013) and underlying psychobiological dysregulations (Germain & Nielsen, Citation2003; Jones & Moller, Citation2011).
The present study is not free of methodological shortcomings, which need to be taken into account for any interpretation of our results. Our study is based on the retrospective analysis of cross-sectional data collected as part of standard clinical diagnostics at the German Armed Forces Hospital Hamburg. The HNQ was developed and reviewed in a military context on the basis of a predominantly male sample. It is left to a study of a civilian sample with a balanced gender ratio to test the generalizability of our results. Since no complete dream reports were collected (for example through the accompanying use of dream diaries or interviews on awakening from a nightmare), the subjective descriptions of the dream content of our sample cannot be independently verified. The indirect access to the object of investigation is, however, a general methodological problem of dream research (Schredl, Citation1999) not unique for our study. Objective data on event-related psychophysiological reactions or on the presence of parasomnias such as the pavor nocturnus can only be obtained by the use of polysomnographic procedures, ideally in the habitual sleep environment of the subjects (Germain, Hall, Katherine Shear, Nofzinger, & Buysse, Citation2006).
Notwithstanding these methodological limitations, the development of the HNQ can be described as successful. The questionnaire has convincing psychometric properties and the construct validity hypotheses were mostly in line with the data. Thus, a short tool is available for the assessment of different aspects of both form and content, as well as for the differentiation of dominant types of nightmare in the German language. In our clinical experience, the HNQ proved to be an important and well accepted instrument supplementing trauma diagnostics, which can be used both for therapy planning and evaluation of therapy outcome. Open tasks for future research are the in-depth examination of the validity of the questionnaire, calculation of reliable cut-off values for the recognition of specific psychopathological aspects in nightmares, as well as translations into other languages.
Supplemental Material
Download Zip (82.5 KB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
References
- APA. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington DC: APA.
- Backhaus, J., & Riemann, D. (1999). Schlafstörungen. Göttingen: Hogrefe.
- Blank, Y., Kelly, M., Bootzin, R. R., & Haynes, P. L. (2009). Does sleep mediate the relationship between nightmares and symptom severity in patients with PTSD and depression? Sleep, 32(Abstract Supplement), A358.
- Borkenau, P., & Ostendorf, F. (2008). NEO-Fünf-Faktoren-Inventar nach Costa und McCrae. Bern: Hogrefe.
- Buysse, D. J., Reynolds, C. F., 3rd, Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–9.
- Davis, J. L. (2009). Treating Post-Trauma nightmares: A cognitive behavioral approach. New York: Springer.
- Donovan, B. S., Padin-Rivera, E., Chapman, H., Strauss, M., & Murray, M. (2005). Development of the Nightmare Intervention and Treatment Evaluation (NITE) scale. Journal of Trauma Practice, 3(4), 47–68.
- Esposito, K., Benitez, A., Barza, L., & Mellman, T. (1999). Evaluation of dream content in combat-related PTSD. Journal of Traumatic Stress: Official Publication of The International Society for Traumatic Stress Studies, 12(4), 681–687.
- Freese, F., Wiese, M., Knaust, T., Schredl, M., Schulz, H., De Dassel, T., … Wittmann, L. (2018). Comparison of dominant nightmare types in patients with different mental disorders. International Journal of Dream Research, 11, 1–5.
- Fulda, S., Hornyak, M., Müller, K., Cerny, L., Beitinger, P. A., & Wetter, T. C. (2008). Development and validation of the Munich Parasomnia Screening (MUPS). Somnologie, 12(1), 56.
- Gerhart, J. I., Russ, E. U., Hall, B. J., & Canetti, D. (2014). Sleep disturbances predict later trauma-related distress: Cross-panel investigation amidst violent turmoil. Health Psychology, 33(4), 365–372.
- Germain, A., Hall, M., Katherine Shear, M., Nofzinger, E. A., & Buysse, D. J. (2006). Ecological study of sleep disruption in PTSD: A pilot study. Annals of the New York Academy of Sciences, 1071, 438–441.
- Germain, A., Hall, M., Krakow, B., Katherine Shear, M., & Buysse, D. J. (2005). A brief sleep scale for posttraumatic stress disorder: Pittsburgh sleep quality index addendum for PTSD. Journal of anxiety disorders, 19(2), 233–244.
- Germain, A., & Nielsen, T. A. (2003). Sleep pathophysiology in posttraumatic stress disorder and idiopathic nightmare sufferers. Biological Psychiatry, 54(10), 1092–1098.
- Görtelmeyer, R. (2011). SF-A/R und SF-B/R: Schlaffragebogen A und B. Göttingen: Hogrefe.
- Happe, S., & Walther, B. W. (Eds.). (2009). Schlafmedizin in der Praxis. Die internationale Klassifikation von Schlafstörungen in Fallberichten. Heidelberg: ecomed MEDIZIN.
- Jones, T., & Moller, M. D. (2011). Implications of hypothalamic-pituitary-adrenal axis functioning in posttraumatic stress disorder. Journal of the American Psychiatric Nurses Association, 17(6), 393–403.
- Köthe, M., & Pietrowsky, R. (2001). Behavioral effects of nightmares and their correlations to personality patterns. Dreaming, 11, 43–52.
- Levin, R., & Nielsen, T. A. (2007). Disturbed dreaming, posttraumatic stress disorder, and affect distress: A review and neurocognitive model. Psychological Bulletin, 133(3), 482–528.
- Mayer, G., Rodenbeck, A., Geisler, P., & Schulz, H. (2015). Internationale Klassifikation der Schlafstörungen: Übersicht über die Änderungen in der ICSD-3. Somnologie, 19(2), 116–125.
- Pietrowsky, R. (2011). Alpträume. Gättingen: Hogrefe.
- Schermelleh-Engel, K., Moosbrugger, H., & Müller, H. (2003). Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods of Psychological Research Online, 8(2), 23–74.
- Schlarb, A. A., Zschoche, M., & Schredl, M. (2016). The Nightmare Effects Questionnaire (NEQ). Somnologie, 20(4), 251–257.
- Schredl, M. (1999). Die nächtliche Traumwelt. Eine Einführung in die psychologische Traumforschung. Stuttgart: Kohlhammer.
- Schredl, M. (2010). Nightmare frequency and nightmare topics in a representative German sample. European Archives of Psychiatry and Clinical Neuroscience, 260(8), 565–570.
- Schredl, M. (2018). Researching dreams. The fundamentals. Cham: Palgrave Macmillan.
- Schreuder, B. J., & Kleijn, W. C. (2001). Intrusive phenomena after psychotrauma. Italian Journal of Psychiatry and Behavioural Sciences, 11(1), 29–34.
- Spoormaker, V. I. (2008). A cognitive model of recurrent nightmares. International Journal of Dream Research, 1(1), 15–22.
- Swart, M. L., van Schagen, A. M., Lancee, J., & van Den Bout, J. (2013). Prevalence of nightmare disorder in psychiatric outpatients. Psychother Psychosom, 82(4), 267–268.
- Timmann, J. (2012). Die Erfassung von Alpträumen als ein Symptom der Posttraumatischen Belastungsstörung bei Soldaten der Bundeswehr nach Auslandseinsätzen an Hand einer modifizierten, deutschsprachigen Fassung der NITE-Scale (Diplomarbeit). Hamburg: Universität Hamburg.
- WHO. (2004). ICD-10: International statistical classification of diseases and related health problems. Geneva: World Health Organization.
- Wittmann, L., & de Dassel, T. (2015). Posttraumatic nightmares: From scientific evidence to clinical significance. In M. Kramer & M. L. Glucksman (Eds.), Dream research (pp. 135–148).Contributions to clinical practice. New York: Routledge.
- Wittmann, L., Schredl, M., & Kramer, M. (2007). Dreaming in posttraumatic stress disorder: A critical review of phenomenology, psychophysiology and treatment. Psychotherapy and Psychosomatics, 76(1), 25–39.