
ABSTRACT
Background
The hours immediately following a traumatic event may present a window of opportunity to interrupt the consolidation of memories of the traumatic event, and this may prevent PTSD development. This theory has been validated in a series of analogue studies, showing that a visuo-spatial task reduces intrusive memories, however clinical studies are scarce.
Objective
This pilot RCT examined the use of a semi-immersive Virtual Reality visuospatial task, as an intervention to interrupt memory consolidation, in the Emergency Department (ED) in the immediate hours following a traumatic event. We hypothesised that participants who had received the intervention would present with lower levels of PTSD symptoms than the control group who received no intervention.
Method
Seventy-seven adult survivors of traumatic events, meeting study criteria, were recruited in the ED of a Level III Trauma Centre. Survivors arrived at the ED less than one hour, on average, after the trauma. After signing informed consent, participants were randomized to the SnowWorld intervention or control group. Both groups completed self-report questionnaires, and the intervention group used SnowWorld for up to 10 minutes.
Results
No significant differences between the intervention and control groups were found regarding PTSD symptom levels two weeks and six months following the traumatic event.
Conclusions
These results add to the growing literature examining the use of a concurrent task to reduce intrusions following a traumatic event. In contrast to previous clinical studies, this study did not show significant group differences; however, it replicates an analogue study that used a specifically developed app. Further studies are needed to elucidate possible reasons for these conflicting results.
Antecedentes: Las horas que siguen inmediatamente a un evento traumático podrían presentar una ventana de oportunidad para interrumpir la consolidación de las memorias del evento traumático, y esto podría prevenir el desarrollo del TEPT. Esta teoría ha sido validada en una serie de estudios análogos, mostrando que una tarea viso-espacial reduce las memorias intrusivas; los estudios clínicos son escasos.
Objetivo: este ensayo controlado aleatorio (RCT en su sigla en inglés) piloto examinó el uso de una tarea viso-espacial de Realidad Virtual semi-inmersa como una intervención para interrumpir la memoria de consolidación en el Departamento de Emergencia, en las horas siguientes a un evento traumático. Hipotetizamos que al seguimiento aquellos que habían recibido la intervención presentarían niveles más bajos de los síntomas del TEPT que el grupo control.
Método: Fueron reclutados en el Departamento de Emergencia (ED en su sigla en inglés) de un Centro de Trauma de Nivel III, 77 sobrevivientes adultos de eventos traumáticos, cumpliendo los criterios del estudio; los sobrevivientes llegaron al ED en promedio menos de una hora luego del trauma. Luego de firmar el consentimiento informado, fueron aleatorizados a la intervención SnowWorld o al grupo control. Ambos grupos completaron cuestionarios de auto-reporte, y el primer grupo usó SnowWorld por un máximo de 10 minutos.
Resultados: No se encontraron diferencias significativas entre los grupos de estudio en los niveles de los síntomas de TEPT dos semanas y seis meses luego del evento traumático.
Conclusiones: Este estudio no replicó los estudios clínicos y análogos previos. Esto puede deberse a las diferencias metodológicas, y los estudios futuros deberían tomarlos en cuenta.
背景: 创伤事件发生后的头几个小时可能提供一个机会窗口以中断创伤事件的记忆巩固, 并组织PTSD的发展。一系列模拟实验研究证实了这一理论, 表明视觉空间任务减少了闯入性记忆。但相关临床研究很少。
目的: 该RCT试验研究了在创伤事件发生后数小时内, 使用半沉浸式虚拟现实视觉空间任务作为干预措施来中断急诊室 (ED) 的记忆巩固的情况。我们假设在随访阶段, 接受干预的病人的PTSD症状的水平要低于对照组。
方法: 在III级创伤中心急诊室招募了77名符合研究标准的成年创伤事件幸存者, 幸存者平均在受伤后不到一个小时到达急诊室。签署知情同意书后, 他们被随机分配到SnowWorld干预组或对照组。两组都填写了自我报告调查表, 干预组使用SnowWorld长达10分钟。
结果: 在创伤事件发生两周和六个月后, 在PTSD症状水平上没有发现组间差异。
结论: 该研究没有重复以前的类似研究和临床研究。这可能是由于不同的方法问题造成的, 未来的研究应将这些考虑在内。
PALABRAS CLAVE:
1. Introduction
Since PTSD develops following exposure to a discrete traumatic event, it has been possible to describe the developmental pathway, from trauma exposure to chronic PTSD. This insight has led to numerous studies examining whether it is possible to disrupt PTSD development, potentially preventing PTSD. Interventions to prevent PTSD have mostly taken place in the initial weeks post-trauma. Meta-analyses have demonstrated that cognitive behaviour therapy (CBT), performed on symptomatic survivors of a traumatic event, can successfully prevent PTSD development (Forneris, Gartlehner, & Brownley et al., Citation2013). However, other studies have shown that the longer term impact of CBT is limited (Kearns, Ressler, Zatzick, & Rothbaum, Citation2012; Shalev et al., Citation2016). Therefore better strategies to prevent PTSD development are needed.
One potential direction lies in the role of memory, that has a well-established role in PTSD development. Specifically, PTSD is characterised by unwanted intrusive memories of the traumatic event. These are vivid and distressing, and therefore related to avoidance, concentration problems and heightened physiological reactivity (Iyadurai, Visser, & Lau-zhu et al., Citation2019). Intrusive memories are predictive of PTSD development (Bryant, O’Donnell, Creamer, McFarlane, & Silove, Citation2011). Memories are initially stored in short term memory, and over a 6–8 hour period they become consolidated in long term memory, before sleep (Brewin, Citation2014; Hu & Stylos-Allan, Citation2006). Memory consolidation can be interrupted, as demonstrated in both rats, with the use of anisomycin (Cohen, Kaplan, Matar, Loewenthal, & Kozlovsky, Citation2006), and in humans, with propranolol and morphine (Holbrook, Galarneau, Dye, Quinn, & Dougherty, Citation2010; Wood et al., Citation2015). This suggests that the first 6–8 hours following a traumatic event, before sleep (Cohen, Kaplan, Zohar, & Cohen, Citation2016), may be a window of opportunity to prevent the consolidation of intrusive memories into long term memory. It is now well established that memory has different components (Brewin, Citation2014): intrusive memories in PTSD are assumed to be non-verbal memories that have not been elaborated. Thus a tool that may be able to modify the consolidation of these non-declarative involuntary parts of a trauma memory is postulated as a strategy to prevent future intrusions. This would impact the subsequent development of PTSD (Visser, Lau-zhu, Henson, & Holmes, Citation2018).
This theory has been examined in a number of analogue studies, based on the precept that consolidation of memories can be enhanced or interrupted. Specifically, memories are likely to be more readily consolidated when performing a verbal task, but will be interrupted with a visuospatial task. This follows theories of memory – postulating that concurrent visuospatial tasks compete with visual images for resources, thus reducing their impact (Andrade, Kavanagh, & Baddeleyl, Citation1997; Lilley, Andrade, Turpin, Sabin-Farrell, & Holmes, Citation2009). These analogue studies have used healthy volunteer subjects, who first watched a traumatic film, and then used the Tetris computer game, immediately after the film (Deeprose, Zhang, Dejong, Dalgleish, & Holmes, Citation2012), after 30 minutes (Holmes, James, Coode-bate, & Deeprose, Citation2009; Holmes et al., Citation2009), and after four hours (Holmes, James, Kilford, & Deeprose, Citation2010). The analogue studies consistently reported significantly reduced intrusive memories at follow up (Brewin, Citation2014), and PTSD symptoms at one week (Holmes et al., Citation2009). Future studies should describe the features of the most effective visuospatial task. Although several studies have shown that Tetris appears to disrupt consolidation, another gaming app, showed no significant differences (Asselbergs et al., Citation2018). One analogue study compared Tetris on a computer versus VR Tetris, and showed that VR Tetris was more effective at reducing intrusions following the trauma film paradigm (Page & Coxon, Citation2017). Translating these findings to a clinical setting is in its infancy: two studies demonstrated that playing with Tetris immediately after a traumatic event resulted in lower reported intrusions in the first two weeks following the traumatic event, however this had no impact on PTSD symptoms at one month post trauma (Horsch et al., Citation2017; Iyadurai et al., Citation2018).
In recent years Virtual Reality (VR) has been increasingly utilized in different therapeutic domains, including rehabilitation, pain reduction, exposure therapy for anxiety disorders, eating disorders and psychosis assessment and treatment (Riva, Wiederhold, & Mantovani, Citation2018). Under the umbrella term of VR, studies have utilized fully immersive systems that use a head mounted display, and semi-immersive systems that use large, high resolution screens, as well as VR that is accessed via desktop computers (Tichon & Banks, Citation2006). Virtual Reality for PTSD has focused on exposure therapy, with VR specific environments for treating chronic PTSD related to combat and terrorist attacks using Virtual Reality Exposure Therapy (Carl, Stein, & Levihn-Coon et al., Citation2019). This utilizes traditional exposure therapy for PTSD (Prolonged Exposure (Hembree, Rauch, & Foa, Citation2003)), with patients carrying out the imaginal exposure in the VR environment (Reger et al., Citation2016).
SnowWorld is a VR environment that contains a frozen world, populated by animals and snowmen, and it was specifically designed for treating burn patients receiving analgesia medication (Carrougher et al., Citation2009)The participant listens to music while throwing snowballs at virtual snowmen using a mouse or joystick. This involves both visual and spatial skills in a non-threatening environment. SnowWorld has been shown to effectively decrease acute procedural pain during wound debridement, severe burn wound care and physical therapy (Maani et al., Citation2008).
VR is being used in the ED for pain distraction in children (Knight, McClenaghan, & Singh, Citation2019), and has been used to assess and improve visuospatial skills (Maggio et al., Citation2018). As far as we aware, VR has not been previously used in a clinical setting as a method to interrupt memory consolidation. Taking these studies together, VR may be an ideal candidate for a visuospatial task in the ED.
The present study is a pilot randomized controlled trial, examining the effect of a visuospatial task presented in a semi-immersive virtual reality environment, on the development of PTSD. We hypothesized that participants who carried out the semi-immersive visuospatial task would develop fewer intrusion symptoms and fewer PTSD symptoms at follow up, compared to the control group participants.
2. Method
This randomized controlled trial was performed in the ED of a Level III Trauma Medical Centre. The study received IRB approval (HMO 0033–10) and was registered: clinical trials.gov, NCT01162044. Participants signed informed consent. The CONSORT statement was adhered to for the study performance and manuscript preparation.
2.1. Participants and recruitment
Adult participants were recruited following presentation to the ED following a potentially traumatic event. No data was kept regarding the total number of participants approached, however in order to determine whether these participants were representative of the general ED population, the recruited participants were compared with 5374 consecutive participants recruited in the same ED as part of another research study (Shalev, Ankri, Peleg, Israeli-Shalev, & Freedman, Citation2011). There were no significant differences in terms of age (current study, 34.5 (12.5), cf. 36.4 (12.0), F (1,5372) = 2.2, ns), or trauma type (current study 84.12% Motor vehicle accidents, cf. 75.4%, X2 = 3.6, ns). There was a significant difference in terms of gender (current study 75% men, cf. 60.9%, X2 = 7.3, p <0.05).
2.2. Recruitment took place in the ED
The research worker approached adults in the ED, enquired whether or not they had experienced a traumatic event as defined in DSM IV (objective danger and subjective feeling of fear), and if so, explained the purpose of the study. The research worker was also alerted to potential participants by the medical team in the ED. Participants arrived at the ED on average within an hour of the traumatic event (85.5% arrived, and were recruited within one hour). All but one participant arrived within five hours, and one participant arrived eight hours after the traumatic event. The research worker confirmed that the participants had not slept since the event. Participants were recruited if they were aged between 18 and 65, had Hebrew as a first language, were able to understand study procedures and give informed consent. Participants with loss of consciousness or head injuries were not included. The hospital’s ED divides patients after triage into surgical care, ambulatory care and an intervention ward. Participants in this study were recruited from ambulatory care.
2.3. Randomization and blinding
Subject numbers were randomized in advance to one of the two study groups; sealed envelopes were prepared in advance, containing group allocation. The research worker who recruited the participant obtained informed consent. Following signing informed consent, the research worker opened the sealed envelope to reveal group allocation. Follow up assessments were carried out by a different research worker who was blinded to treatment condition.
3. Procedure
After signing informed consent, all participants filled in self-report questionnaires outlined below. SnowWorld participants completed the post-task questionnaires after they had finished using SnowWorld. Control group participants completed the post-task questionnaires 10 minutes after they had completed the self-report questionnaires. All participants received usual medical care in the ED. Follow up assessments, at two weeks and six months, were performed by a second research worker, blinded to treatment allocation.
4. Interventions
The SnowWorld semi-immersive VR was set up in a small treatment room situated in a quiet corridor away from the main ambulatory care waiting area. The SnowWorld was housed in a desktop Asus computer, and participants were seated, wearing headphones, facing an Apple 30- inch Cinema Display screen, 2560 × 1600 resolution, 170/170 viewing angle. The screen was placed within a large housing unit that effectively blocked the participant’s view of the room. SnowWorld was activated using a wireless mouse, and participants moved through the virtual scene of snow, snowmen and animals, using the mouse to throw and explode snowballs. The scene moves constantly, thus participants may passively progress through the observed scene.
The research worker recorded the duration of playing time, and the post-intervention questionnaires regarding the semi-immersive VR experience were completed (outlined below).
5. Measures
5.1. ED
Event Questionnaire – this 15-item questionnaire assesses objective aspects of the traumatic event (e.g. type of traumatic event, need for stitches) and subjective aspects (e.g. fear, feeling of being in danger of dying). These latter were assessed on a 10-point scale, with 1 indicating not experiencing this, to 10 indicating experiencing this strongly. This scale has been used in numerous studies with this population (Freedman & Shalev, Citation2016). Medications administered in the ED were noted, and this was later checked against the medical file. A senior physician (CFW) manually determined the medication group classification, according to opioid or not.
PTSD symptoms (pertaining to previous events) was assessed using the Posttraumatic Symptom Scale (PSS, (Foa, Riggs, Dancu, & Rothbaum, Citation1993)). This scale was also used at the two follow ups. Total scores over 14 were considered to be probable PTSD (Coffey, Gudmundsdottir, Beck, Palyo, & Miller, Citation2006).
Participants in the SnowWorld condition were asked to evaluate their levels of nausea, presence and realism.
Nausea: To what extent (if at all) did you feel nausea (sick to your stomach) as a result of experiencing the virtual world during the most recent VR session? (from 0: “no nausea at all,” 1 – 4: mild nausea, 5: moderate nausea, 7–9: severe nausea, 10: vomit).
Presence: While experiencing the virtual world, to what extent did you feel like you WENT INSIDE the virtual world? (10-cm line with numeric and verbal descriptors: 0: I did not feel like I went inside at all; 1–4 mild sense of going inside; 5–6 moderate sense of going inside; 7–9 strong sense of going inside; 10 I went completely inside the virtual world).
Realism: How REAL did the virtual objects seem to you during virtual reality? 0: completely fake, 1–4: somewhat real, 5: moderately real, 6–9: very real, 10: indistinguishable from a real object (Atzori et al., Citation2018).
5.2. Primary outcomes
Primary outcome was PTSD symptom levels at follow up (two weeks and six months), assessed using the PSS. This questionnaire was administered during a telephone call by a research worker who was blinded to treatment group.
5.3. Sample size
At the time of study planning, no comparable clinical studies had been published, and analogue studies had demonstrated significant differences, with sample sizes smaller than the subject numbers in this study (Holmes et al., Citation2010). Based on the same analogue study, a similar clinical trial estimated that using an estimated effect size of d = 0.7, 80% at alpha = 0.05, a sample size of 66 would be adequate (Iyadurai et al., Citation2018).
5.4. Statistical analysis
Data were analysed using SPSS 23.0 (SPSS Inc). Probable PTSD was measured by the PSS, using DSM IV criteria, giving dichotomous scoring for PTSD presence. Normality was tested using Kolomgorov-Smirnov tests. Differences between study groups (SnowWorld and Control) in baseline and follow-up variables were examined using t, Mann-Whitney, Chi square and Fisher’s exact tests, according to the variables scales and distribution normality. Spearman correlations were used to clarify the relationships between baseline and follow-up variables. All analyses were performed with p < 0.05 indicating statistical significance.
6. Results
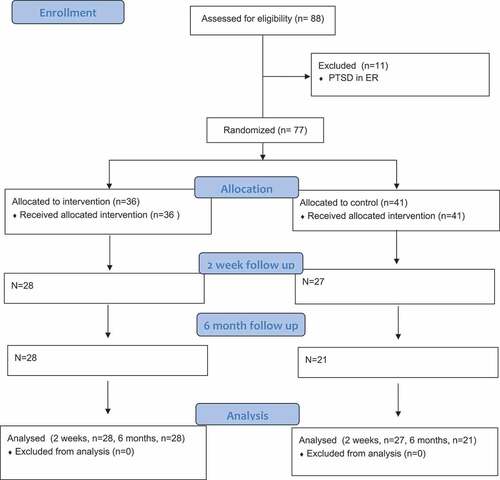
We recruited 88 patients. shows participant flow through the study; 61 subjects (79.2%) attended the ED following a motor vehicle accident (MVA), 16 (20.8%) following another incident. Participants in the control and SnowWorld groups were compared regarding reactions and interventions in the ED; no significant differences were found on any variable (). The dropout rate did not differ between groups. No significant differences were found between the participants that dropped out and those who did not. The distributions of all the study variables except heart rate were not normal, thus, non-parametric tests were used when needed.
Table 1. Study characteristics.
Figure 1. CONSORT flow diagram.
7. Treatment adherence
All 36 subjects randomized to use the SnowWorld intervention completed the programme in the ED. The mean duration of SnowWorld use was 8.06 (SD = 2.02) minutes. Subjects reported low levels of nausea (M = 2.42, SD = 2.56), and relatively high levels of realism (M = 6.94, SD = 3.14) and presence in VR (M = 5.31, SD = 2.84). No participant spontaneously reported any other adverse effects or requested to stop. All subjects in the control group completed questionnaires in the ED.
8. Outcome measures
PTSD measures (intrusions, avoidance, arousal, total PTSD score) were completed twice, two weeks and six months after the first measure. No significant differences were found between the SnowWorld and control group ( & ).
Table 2. PTSD symptoms- follow up.
Table 3. Spearman correlations between ER measures and intrusions and PTSD in follow-up.
9. Discussion
This pilot RCT aimed to test whether interrupting memory consolidation in the first 6–8 hours following a traumatic event reduced the level of intrusions and PTSD symptoms at follow up.
The results indicate that a short ten-minute semi-immersive VR intervention can be administered to participants within a few hours of a traumatic event, in the setting of a busy ED. All participants who received the intervention completed the task, with no dropouts; and no adverse effects, such as nausea, were reported.
The intervention used in the current study had no significant effects on PTSD symptoms at two weeks or six month follow up compared to the control group. These results differ from the two previously published clinical studies (Horsch et al., Citation2017; Iyadurai et al., Citation2018), and various methodological factors may account for this. First, the authors of previous studies using Tetris have assumed that any generic visuospatial task would have similar efficacious results (Iyadurai et al., Citation2018). However the results of one analogue study using a task that was not Tetris, together with the current study, suggest this may not be accurate. It is possible that Tetris requires a greater level of working memory visuospatial skills (Asselbergs et al., Citation2018); insufficient studies have been performed to discriminate between specific types of visuospatial task. Therefore future clinical studies should take into account the visuospatial task being used, for example comparing Tetris to other tasks.
Secondly, unlike the previous study in the ED (Iyadurai et al., Citation2018), participants in the current study were not asked to bring up a trauma memory before completing the intervention, since it was assumed that being in the ED was a sufficient trigger to be thinking about the traumatic event (Horsch et al., Citation2017). This assumption may be overly simplified, and needs to be tested empirically in order to better understand the importance of memory focus while completing the task.
Thirdly, participants in the current study were not requested to complete a diary of their intrusions, rather to complete a questionnaire at follow up interviews about intrusions. This contrasts to participants in the two previous Tetris clinical studies (Iyadurai et al., Citation2018; James, Lau-Zhu, Tickle, Horsch, & Holmes, Citation2016), where significant differences were found in levels of intrusions according to diaries. Keeping a diary may be a more reliable strategy for accurate reporting, however is not the current gold standard. Future investigations should consider the optimum strategy for reporting intrusions, as this may influence the results.
One analogue study examining memory consolidation has shown that changing the meaning of the event can effect PTSD levels (Pile, Barnhofer, & Wild, Citation2015), and this has important implications. In the current study, as with previous studies, meaning-making in the ED was not assessed, and therefore its potential effects on the results are unknown. For instance, a conversation with the doctor, where the patient is reassured that the event was not so bad, and there are no life-threatening injuries, may be another way to interrupt trauma memory consolidation, thus potentially reducing PTSD. Future studies should include this type of interruption as a comparison intervention.
No differences were found between the study groups regarding the amount of opioids administered in the ED; however previous studies have shown confounding results regarding the effects of opioids on PTSD development (Mouthaan et al., Citation2015; Usuki et al., Citation2012), and future studies should consider opioid use in the ED as an exclusion criteria or a co-variant.
The current study had several important limitations. Firstly, the small sample size means that the study was underpowered, and therefore any significant differences will not have been detected (Cohen, Citation1988).
The sample was 75% male, which might impact PTSD development rates, although previous studies from this ED population have consistently found no gender differences for PTSD development (Freedman et al., Citation2002; Shalev & Freedman, Citation2005). Additionally, no data were kept regarding the number of potential participants who refused to take part; thus potentially this sample may not represent the total population. The study used a desktop computer, with an extremely large high-resolution screen. Although participants reported feeling as if the environment was real, it is possible that the use of a VR helmet would better replicate the results found with Tetris. A direct comparison between Tetris and VR is also important. Additionally, the costs of VR hardware and software may mean that it is less cost-effective than an easily purchased game such as Tetris. Related to this, it is possible that 10 minutes is an insufficient dose, and that a longer duration exposure to the semi-immersive visuospatial task may be more effective at preventing memory consolidation. Given the high rates of natural recovery following exposure to a traumatic event, the use of a control group, without an intervention in the ED, is essential; however, a control condition that is given a neutral task may be more appropriate. This study was carried out before DSM5 was published and should be replicated with more up-to-date measures (e.g. PCL5 (Blevins, Weathers, Davis, Witte, & Domino, Citation2015)). The exclusion of participants with past and current PTSD is important in prevention studies but may exclude those likely to require treatment.
This pilot RCT shows that interrupting memory consolidation in the ED in the first few hours following a traumatic event is an acceptable and achievable aim, and adds to the small literature of RCTs carried out in this timeframe. The results presented here do not indicate successful secondary prevention of PTSD, however given the theoretical and analogue studies on which this trial was based, it is important to replicate. Future studies should explore the impact of the differences in methodology, including the dose of the visuospatial task, type of task (e.g. Tetris vs VR), type of VR (semi-immersive vs. fully immersive) and the activation of a traumatic memory.
Data access and responsibility
The PI, Dr Sara Freedman, has full access to all the study data and takes responsibility for the integrity of the data and accuracy of the analysis.
Disclosure statement
The authors report no potential conflict of interest
Additional information
Funding
References
- Andrade, J. , Kavanagh, D., & Baddeleyl, A. (1997). Eye-movements and visual imagery: A working memory approach to the treatment of post-traumatic stress disorder. British Journal of Clinical Psychology, 36, 209–223.
- Asselbergs, J. , Sijbrandij, M. , Hoogendoorn, E. , Cuijpers, P. , Olie, L. , Oved, K. , & Riper, H. (2018). Development and testing of TraumaGameplay: An iterative experimental approach using the trauma film paradigm. European Journal of Psychotraumatology , 9(1), 1–10.
- Atzori, B. , Grotto, R. L. , Giugni, A. , Calabrò, M. , Alhalabi, W. , & Hoffman, H. G. (2018). Virtual reality analgesia for pediatric dental patients. Frontiers in Psychology , 9(November), 1–6.
- Blevins, C. A. , Weathers, F. W. , Davis, M. T. , Witte, T. K. , & Domino, J. L. (2015). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress , 28(6), 489–498.
- Brewin, C. R. (2014). Episodic memory, perceptual memory, and their interaction: Foundations for a theory of posttraumatic stress disorder. Psychological Bulletin , 140(1), 69–97.
- Bryant, R. A. , O’Donnell, M. L. , Creamer, M. , McFarlane, A. C. , & Silove, D. (2011). Posttraumatic intrusive symptoms across psychiatric disorders. Journal of Psychiatric Research , 45(6), 842–847.
- Carl, E. , Stein, A. T. , Levihn-Coon, A. , Pogue, J. R., Rothbaum, B., Emmelkamp, P., Asmundson, G. J. G., Carlbring, P., & Powers, M. B. (2019). Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials. Journal of Anxiety Disorders , 61, 27–36. doi:10.1016/j.janxdis.2018.08.003
- Carrougher, G. J. , Hoffman, H. G. , Nakamura, D. , Lezotte, D. , Soltani, M. , Leahy, L. , & Engrav, L. H. P. D. (2009). The effect of virtual reality on pain and range of motion in adults with burn injuries. Journal of Burn Care & Research , 30(5), 785–791.
- Coffey, S. R. , Gudmundsdottir, B. , Beck, J. G. , Palyo, S. A. , & Miller, L. (2006). Screening for PTSD in motor vehicle accident survivors using the PSS-SR and IES. Journal of Traumatic Stress , 19(1), 119–128.
- Cohen, H. , Kaplan, Z. , Matar, M. A. , Loewenthal, U. , & Kozlovsky, N. Z. J. (2006). Anisomycin, a protein synthesis inhibitor, disrupts traumatic memory consolidation and attenuates posttraumatic stress response in rats. Biological Psychiatry , 60(7), 767–776.
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Statistical Power Analysis for the Behavioral Sciences , 2nd, 567.
- Cohen, S. , Kaplan, Z. , Zohar, J. , & Cohen, H. (2016). Preventing sleep on the first resting phase following a traumatic event attenuates anxiety-related responses. Behavioural Brain Research , 320, 450–456.
- Deeprose, C. , Zhang, S. , Dejong, H. , Dalgleish, T. , & Holmes, E. A. (2012). Journal of Behavior Therapy and Imagery in the aftermath of viewing a traumatic film: Using cognitive tasks to modulate the development of involuntary memory. Journal of Behavior Therapy and Experimental Psychiatry , 43(2), 758–764.
- Foa, E. B. , Riggs, D. S. , Dancu, C. V. , & Rothbaum, B. O. (1993). Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress , 6(4), 459–473.
- Forneris, C. A., Gartlehner, G., Brownley, K. A., Gaynes, B. N., Sonis, J., Coker-Schwimmer, E., Jonas, D. E., Greenblatt, A., Wilkins, T. M., Woodell, C. L., & Lohr, K. N. (2013). Interventions to prevent post-traumatic stress disorder: A systematic review. American Journal of Preventive Medicine, 44(6), 635–650. https://doi.org/10.1016/j.amepre.2013.02.013
- Freedman, S. A. , Gluck, N. , Tuval-Mashiach, R. , Brandes, D. , Peri, T. , & Shalev, A. Y. (2002). Gender differences in responses to traumatic events: A prospective study. Journal of Traumatic Stress , 15(5), 407–413.
- Freedman, S. A. , & Shalev, A. Y. (2016). Immediate psychological reactions in the emergency department following exposure to potentially traumatic events. International Journal of Emergency Mental Health , 18(2), 742–744.
- Hembree, E. A. , Rauch, S. A. M. , & Foa, E. B. (2003). Beyond the manual: The insider’s guide to Prolonged Exposure therapy for PTSD. Cognitive and Behavioral Practice , 10(1), 22–30.
- Holbrook, T. L. , Galarneau, M. R. , Dye, J. L. , Quinn, K. , & Dougherty, A. L. (2010). Morphine use after combat injury in Iraq and post-traumatic stress disorder. New England Journal of Medicine , 362(2), 110–117.
- Holmes, E. A. , James, E. L. , Coode-bate, T. , & Deeprose, C. (2009). Can playing the computer game ‘“ tetris ”’ reduce the build-up of flashbacks for Trauma? A proposal from cognitive science. PloS One , 4(1), 1–6.
- Holmes, E. A. , James, E. L. , Kilford, E. J. , & Deeprose, C. (2010). Key steps in developing a cognitive vaccine against traumatic flashbacks: Visuospatial tetris versus verbal pub quiz. 5(11). doi:10.1371/journal.pone.0013706
- Horsch, A. , Vial, Y. , Favrod, C. , Harari, M. M. , Blackwell, S. E. , Watson, P. , & Holmes, E. A. (2017). Reducing intrusive traumatic memories after emergency caesarean section: A proof-of-principle randomized controlled study. Behaviour Research and Therapy , 94, 36–47.
- Hu, P. , & Stylos-Allan, M. W. M. (2006). Sleep facilitates consolidation of emotional declarative memory. Psychological Science , 17(10), 891–898.
- Iyadurai, L. , Blackwell, S. E. , Meiser-Stedman, R. , Watson, P. C. , Bonsall, M. B. , Geddes, J. R. , … Holmes, E. (2018). Preventing intrusive memories after trauma via a brief intervention involving Tetris computer game play in the emergency department: A proof-of-concept randomized controlled trial. Molecular Psychiatry , 23(3), 674–682.
- Iyadurai, L. , Visser, R. M. , Lau-zhu, A. , Porcheret, K., Horsch, A., Holmes, E. A., & James, E. L. (2019). Intrusive memories of trauma : A target for research bridging cognitive science and its clinical application. Clinical Psychology Review , 69, 67–82. doi:10.1016/j.cpr.2018.08.005
- James, E. L. , Lau-Zhu, A. , Tickle, H. , Horsch, A. , & Holmes, E. A. (2016). Playing the computer game Tetris prior to viewing traumatic film material and subsequent intrusive memories: Examining proactive interference. Journal of Behavior Therapy and Experimental Psychiatry , 53(2016), 25–33.
- Kearns, M. C. , Ressler, K. J. , Zatzick, D. , & Rothbaum, B. O. (2012). Early interventions for PTSD: A review. Depression and Anxiety , 29(10), 833–842.
- Knight, K. , McClenaghan, C. E. , & Singh, B. (2019). Virtual reality distraction from painful procedures in the paediatric emergency department. Archives of Disease in Childhood , 104(2), 204–205.
- Lilley, S. A. , Andrade, J. , Turpin, G. , Sabin-Farrell, R. , & Holmes, E. A. (2009). Visuospatial working memory interference with recollections of trauma. British Journal of Clinical Psychology , 48(Pt 3), 309–321.
- Maani, C. , Hoffman, H. G. , DeSocio, P. A. , Morrow, M. , Galin, C. , Magula, J. M. A. , & Gaylord, K. (2008). Pain control during wound care for combat-related burn injuries using custom articulated arm mounted virtual reality goggles. The Journal of Cybertherapy and Rehabilitation , 1, 193–198.
- Maggio, M. G. , De Cola, M. C. , Latella, D. , Maresca, G. , Finocchiaro, C. , La Rosa, G. , & Calabrò, R. S. (2018). What about the role of virtual reality in parkinson disease’s cognitive rehabilitation? Preliminary findings from a randomized clinical trial. Journal of Geriatric Psychiatry and Neurology , 31(6), 312–318.
- Mouthaan, J. , Sijbrandij, M. , Reitsma, J. B. , Luitse, J. S. K. , Goslings, J. , Gersons, B. P. R. , & Olff, M. (2015). The role of early pharmacotherapy in the development of posttraumatic stress disorder symptoms after traumatic injury: An observational cohort study in consecutive patients. General Hospital Psychiatry , 37(3), 230–235.
- Page, S. , & Coxon, M. (2017). Preventing post-traumatic intrusions using virtual reality. The Annual Review of CyberTherapy and Telemedicine , 15, 129–134.
- Pile, V. , Barnhofer, T. , & Wild, J. (2015). Updating versus exposure to prevent consolidation of conditioned fear. PloS One , 10(4), 1–21.
- Reger, G. M. , Koenen-woods, P. , Zetocha, K. , Smolenski, D. J. , Holloway, K. M. , Rothbaum, B. O. , & Gahm, G. A. (2016). Randomized controlled trial of prolonged exposure using imaginal exposure vs. virtual reality exposure in active stress disorder (PTSD) randomized controlled trial of prolonged exposure using imaginal expos. Journal of Consulting and Clinical Psychology , 84(11), 946–959.
- Riva, G. , Wiederhold, B. K. , & Mantovani, F. (2018). Neuroscience of virtual reality: From virtual exposure to embodied medicine. Cyberpsychology, Behavior, and Social Networking , cyber.2017.29099.gri. doi:10.1089/cyber.2017.29099.gri
- Shalev, A. Y. , Ankri, Y. , Gilad, M. , Israeli-Shalev, Y. , Adessky, R. , Qian, M. , & Freedman, S. (2016). Long-Term outcome of early interventions to prevent posttraumatic stress disorder. The Journal of Clinical Psychiatry , 77(5), e580–e587.
- Shalev, A. Y. , Ankri, Y. L. E. , Peleg, T. , Israeli-Shalev, Y. , & Freedman, S. (2011). Barriers to receiving early care for PTSD: Results from the Jerusalem trauma outreach and prevention study. Psychiatric Services , 62(7), 765–773.
- Shalev, A. Y. , & Freedman, S. (2005). PTSD following terrorist attacks: A prospective evaluation. American Journal of Psychiatry , 162(6), 1188–1191.
- Tichon, J. , & Banks, J. (2006). Virtual reality exposure therapy: 150-degree screen to desktop PC. CyberPsychology & Behavior, 9(4), 480–489.
- Usuki, M. , Matsuoka, Y. , Nishi, D. , Yonemoto, N. , Matsumura, K. , Otomo, Y. , & Kim, Y. K. S. (2012). Potential impact of propofol immediately after motor vehicle accident on later symptoms of posttraumatic stress disorder at 6-month follow up: A retrospective cohort study. Critical Care , 16(5), R196.
- Visser, M. , Lau-zhu, A. , Henson, R. N. , & Holmes, E. A. (2018). Multiple memory systems, multiple time points: How science can inform treatment to control the expression of unwanted emotional memories. Philosophical Transactions of the Royal Society B , 373(1742), 20170209.
- Wood, N. E. , Rosasco, M. L. , Suris, A. M. , Spring, J. D. , Marin, M. F. , Lasko, N. B. , … Orr, S. P. P. R. (2015). Pharmacological blockade of memory reconsolidation in posttraumatic stress disorder: Three negative psychophysiological studies. Psychiatry Research , 225(1–2), 31–39.