
ABSTRACT
This letter provides an update on the activities of “The Global Collaboration on Traumatic Stress” (GC-TS) as first described by Schnyder et al. in 2017. It presents in further detail the projects of the first theme, in particular the development of and initial data on the Global Psychotrauma Screen (GPS), a brief instrument designed to screen for the wide range of potential outcomes of trauma. English language data and ongoing studies in several languages provide a first indication that the GPS is a feasible, reliable and valid tool, a tool that may be very useful in the current pandemic of the coronavirus disease 2019 (COVID-19). Further multi-language and cross-cultural validation is needed.
Since the start of the GC-TS, new themes have been introduced to focus on in the coming years: a) Forcibly displaced persons, b) Global prevalence of stress and trauma related disorders, c) Socio-emotional development across cultures, and d) Collaborating to make traumatic stress research data “FAIR”. The most recent theme added is that of Global crises, currently focusing on COVID-19-related projects.
1. The global collaboration on traumatic stress
The Global Collaboration on Traumatic Stress (GC-TS) started as a committee of the International Society for Traumatic Stress Studies (ISTSS) (Olff, Citation2014; Schnyder & Olff, Citation2013) Since 2019 it has grown into an independent body with a steering committee representing all major traumatic stress societies (see www.global-psychotrauma.net). The GC-TS recognizes that across the world, exposure to trauma is the norm rather than the exception (Kessler et al., Citation2017; Schnyder et al., Citation2017); that the great majority of the global burden of disease arising from mental health conditions occurs in low and middle income countries (Schnyder et al., Citation2017); that traumatic experiences, trauma-related symptoms, as well as treatment approaches differ across cultures, and, finally, that trauma does not stop at borders. It therefore aims ‘To identify objectives, facilitate development, and coordinate activities of global importance …. the community of traumatic stress researchers and practitioners should develop collaborations, and ultimately structures, that enable them to optimally respond to those tasks that are best addressed by means of international collaboration’ (Schnyder et al., Citation2017). The GC-TS began with representatives from eight traumatic stress related professional societies while others joined later. For more details see www.global-psychotrauma.net.
The GC-TS has recognized as one of its first priorities a focus on the wide range of potential outcomes of trauma, especially childhood trauma, and considering cross-cultural differences in trauma-related outcomes. With traumatic events happening all over the world (Kessler et al., Citation2017), one of the key questions to address is how to efficiently identify those at risk of developing adverse mental health outcomes, in particular how to specifically address the long-term impact of childhood trauma, and how to easily provide individuals worldwide with evidence-based information on the potential consequences of traumatic stress and effective and safe interventions. The recent pandemic of COVID-19 emphasizes again the need to collaborate around the world to prevent and treat the mental health impact of this crisis in all sectors of society, including health-care workers.
In this letter we aim to provide a brief update on the progress of these first activities of the GC-TS: (1) The development of a synthesized core guide on childhood maltreatment, ‘Internet information on Childhood Abuse and Neglect’ (iCAN e-pamphlets), (2) The testing of the Computerized Childhood Attachment and Relational Trauma Screen (CARTS), and (3) The development of, and first data on, the Global Psychotrauma Screen (GPS), an instrument to screen for a wide range of potential outcomes of trauma.
2. Internet information on childhood abuse and neglect – iCAN e-pamphlets
As its first undertaking, the GC-TS created easily accessible evidence-based information in several languages for adults, around the world, who have experienced childhood maltreatment. The materials we developed were intended to serve as a psychoeducational resource that would provide affected individuals with greater knowledge of the consequences of childhood abuse as well as potential interventions. This information was shared as an e-pamphlet called Internet information on Childhood Abuse and Neglect (iCAN, see ).
Figure 1. The iCAN brochure, see also https://www.global-psychotrauma.net/copy-of-ican
The group collected guidelines (TENTS, NATO, NICE, ISTSS guidelines, local, e.g. Bisson et al., Citation2019, Citation2010; Lewis, Roberts, Andrew, Starling, & Bisson, Citation2020; NICE, Citation2018; Roberts, Kitchiner, Kenardy, Lewis, & Bisson, Citation2019) that provided the basis for a synthesized evidence-based core guide that was customized for specific cultural contexts. For more information see Schnyder et al. (Citation2017).
The e-pamphlet that was created offers brief and relevant information to adults with childhood traumatic experiences. The content of the e-pamphlet is designed to support affected individuals to better understand what childhood trauma is, what its possible consequences are, what one can do to help oneself (e.g. ensuring safety, disclosure, healthy sleep and eating habits, self-care, writing), and how to get help from others (e.g. peer support and professional help).
The e-pamphlet is currently available in nine languages and can be accessed here: https://www.global-psychotrauma.net/copy-of-ican. The information is not meant to replace professional advice, but rather to encourage affected persons to seek help if needed.
3. Computerized childhood attachment and relational trauma screen (CARTS)
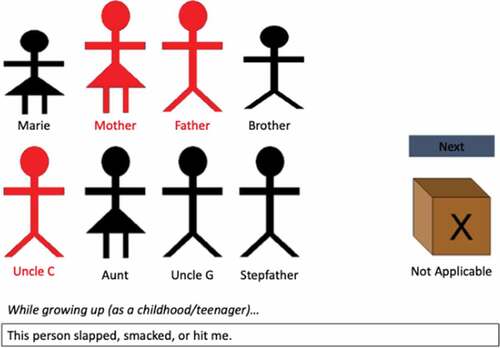
CARTS is a computerized survey of individuals’ recollections of the warmth, security and support of their relationships with their family members during childhood, and of relational traumatic experiences occurring during childhood (Frewen, Brown, De Pierro, D’Andrea, & Schore, Citation2015a; Frewen, Brown, Steuwe, & Lanius, Citation2015b; Frewen et al., Citation2013; Simonelli, Sacchi, Cantoni, Brown, & Frewen, Citation2017, see ). The currently available instruments for the assessment of childhood trauma experiences and their impact tend to overlook the socio-ecological and relational context of childhood trauma. For this reason, CARTS was developed as an innovative assessment tool to elucidate socio-ecological relational perspectives. This feature enables the evaluation of the subjective perception of the traumatic relational context, rather than only the frequency and severity of such experiences.
The CARTS survey can currently only be accessed and completed as part of a research project, but is expected to be made available through the Global Collaboration website, along with a summary of the study’s findings. Access to the survey can be found here: www.global-psychotrauma.net/carts.
Previous attest to the reliability and convergent validity of the CARTS item content when administered in English (Frewen et al., Citation2015a, Citation2015b, Citation2013). Moreover, due to the very high face validity of the survey items, the CARTS is expected to have high cross-cultural applicability, and one study has already compared responses in Italian versus Canadian undergraduates and found that the CARTS subscales were sensitive to differences between the cultures in childhood trauma exposure, whereby the Canadian group was overall more likely to report a lack of attachment security and more likely to report childhood emotional and physical abuse history, but less likely to report childhood sexual abuse history (Simonelli et al., Citation2017). Concerning specifically the evaluation of parents, the Canadian group also reported more positive and secure attachment descriptions of both their biological mothers and fathers (Simonelli et al., Citation2017). Therefore, one of the aims of the GC-TS is to investigate the use of CARTS in different languages and cultures to determine if further cultural differences can be identified among persons of other nationalities and languages. To this end, participants around the world are invited to take part in the CARTS-GPS study using several published translations (see https://www.global-psychotrauma.net/carts). Publication of further results collected among German, Spanish, and French speaking persons is expected soon, with data collected from persons of other languages also accumulating.
Figure 2. Example of CARTS items
4. The global psychotrauma screen (GPS)
Potential consequences of trauma are not limited to symptoms of posttraumatic stress disorder (PTSD) but include a wide variety of symptoms and disorders, including depression, anxiety, physical symptoms, self-harm and substance misuse. Moreover, symptoms frequently co-occur, especially after interpersonal trauma (e.g. Baekkelund, Frewen, Lanius, Ottesen Berg, & Arnevik, Citation2018; Cramer, Waldorp, van der Maas, & Borsboom, Citation2010; Kessler et al., Citation2017; McLaughlin et al., Citation2015; Olff et al., Citation2019; van der Kolk, Ford, & Spinazzola, Citation2019).
Although there are several brief instruments that screen for specific types of traumatic stress reactions such as posttraumatic stress reactions (e.g. Trauma Screening Questionnaire, Impact of Event Scale (-Revised), SPAN, (DSM-IV based), or Posttraumatic Stress Disorder Checklist for DSM-5; Blevins, Weathers, Davis, Witte, & Domino, Citation2015; Brewin et al., Citation2002; Mouthaan, Sijbrandij, Reitsma, Gersons, & Olff, Citation2014; Prins et al., Citation2016; Sijbrandij, Olff, Opmeer, Carlier, & Gersons, Citation2008; Weiss & Marmar, Citation1997), for complex PTSD (International Trauma Questionnaire, Bondjers et al., Citation2019; Cloitre et al., Citation2018; Shevlin et al., Citation2018); or acute reactions (Peritraumatic Dissociative Experiences Questionnaire, Peritraumatic Distress inventory; Brunet et al., Citation2001), or for psychological resilience (Van der Meer et al., Citation2018) the GC-TS is not aware of brief screening instruments including these various reactions simultaneously, while also including assessment of important well-established risk and protective factors.
Screening for a wide range of potential outcomes of trauma, as well as for risk and protective factors, was expected to fill a gap in rapid assessment of trauma-related symptoms, especially if the measure could be simple, cross-culturally valid, and easy to administer in a variety of circumstances, e.g. shortly after mass trauma, but would also tap potential consequences up to decades after chronic childhood abuse or combat experience. Moreover, in line with Open Science, we were keen to develop a measure that was free-of-charge and available to everyone with no copyright issues. This formed the basis of the development of the Global Psychotrauma Screen (GPS) by the GC-TS international group of psychotrauma experts from different cultural backgrounds.
For item selection, the GC-TS first reached consensus on the domains that would cover the wide range of reactions to trauma, as well as risk and protective factors. The domains identified with regard to symptoms were: PTSD, complex PTSD, anxiety, depression, sleep problems, self-injurious behaviour, dissociation, substance abuse, other physical, emotional or social problems. Risk factors and protective factors identified included: other stressful events, childhood trauma, history of mental illness, social support and psychological resilience. Substance abuse can be perceived as a symptom, but also as a measure of palliative coping, which would make it a risk factor in this case (Olff, Langeland, & Gersons, Citation2005). Risk and protective factors are believed to be of particular importance for assessing the future course of symptoms when the screener will be used over time to monitor and predict outcome.
In the next phase, GPS items were selected (as much as possible) from existing valid and reliable measures that were already available for the specific domains and where there were no barriers to access. We could thus build on previous validation studies for the subdomains.
The result was a short screener consisting of 22 items, each to be answered using a simple yes/no format, format to ensure ease of administration cross-culturally. The yes/no response format was chosen to make sure that the GPS is a true screener in the sense that it can be filled out within several minutes, while at the same time is sensitive to picking up potential symptoms or problems. A ‘GPS total’ score can be calculated, including all GPS items, with the resilience item 22 being reversely scored. ‘GPS symptoms’, i.e. the sum score of all symptom items, as well as subdomain scores, can also be calculated. SPSS syntax files can be provided.
The GPS is currently available in more than 20 languages: Afrikaans, Arabic, Armenian, Chinese, Croatian, Dutch, English, Persian-Farsi, French, Georgian, German, Greek, Hebrew, Indonesian, Italian, Japanese, Norwegian, Portuguese (European and Brazilian), Russian, Spanish, Turkish, and Xhosa. Translations into various African languages are being prepared (check here for currently available translations: www.global-psychotrauma.net/gps). Following Sousa and Rojjanasrirat (Citation2011), translations required at least one translation into the target language by one translator and one back-translation into English by a second independent translator who was blind to the original material. The back-translation had to be checked with the primary author of the GPS. In case of discrepancies, more rounds would be necessary. Translations were piloted in 5–20 traumatized subjects which in some cases led to small adaptations. In general, it was found to be a quick and easy to administer tool.
A GPS web-app has been built for individuals to easily fill out the GPS in several languages (https://gps.global-psychotrauma.net). The app additionally includes questions on the type and time of the event experienced (COVID-19 has currently been added) as well as an item on global functioning. It provides – at this time – conservative feedback on the scores with advice on seeking further help if needed, using international websites that provide contact information for mental health crisis hotlines internationally. Norm scores are currently being collected in various languages and ongoing validation research will allow for more detailed feedback in the future. For researchers (or clinicians) there is a ‘scientist portal’ to collect data for specific groups of participants/patients.
In order for the GPS to be a reliable and valid screening instrument, research on its psychometric properties is needed in a variety of trauma-exposed samples from different countries. In we present preliminary data from the different samples, partly presented at the ISTSS conference in November 2019. For all projects, IRB approval was obtained to include the GPS or it was exempted from formal approval by the local ethical authority. The data show that means vary per type of sample and country/culture, and by sex. Cronbach’s alpha for all projects were fairly high (>0.8). The GPS in all projects showed a moderate correlation with PTSD symptoms, which is to be expected with the GPS partly assessing PTSD symptoms.
Table 1. Psychometric properties of the GPS in a variety of samples – ongoing research
In summary, pilot testing and initial study data showed that the GPS is easy to administer, it showed good internal consistency, as well as convergent validity with measures of PTSD symptoms. More psychometric properties, normative responses, domain scores, and clinical cut-off points of the GPS will be presented when rigorous testing is completed. Further GPS research is currently starting up or taking place in Indonesia (I. Primasari, representative population study), Liberia (J Pinto, mixed sample), Netherlands (A. Bakker, Representative population sample; B. Winter, student sample), US (E. Grace, mixed sample), Italy (R. Rossi, General population and health-care professionals). Thus, we will carry on with data collection in several languages in order to ultimately document the wider cross-cultural validity.
5. Conclusion
Reflecting on the work of the Global Collaboration on Traumatic Stress (GC-TS), we have shown that with a diverse group of international experts, we are able to effectively work together on topics of global importance as a diverse group of international experts from traumatic stress societies worldwide. We were able to create evidence-based information pamphlets on childhood trauma (iCAN) adapted to different cultures. We conducted a study on individuals’ recollections of the quality of their relationships with their family members during childhood and of relational traumatic experiences occurring during childhood (CARTS), using a computerized survey. And we created a brief screening instrument to tap into the wide range of potential outcomes of any type of trauma, available in over 20 languages (GPS) with initial results providing the first indications that the GPS may be a reliable and valid instrument to capture posttraumatic stress reactions.
In addition, a website was created bringing together all activities of the GC-TS: www.global-psychotrauma.net.
We hope that the efforts of the GC-TS will facilitate the use of the tools in practice, especially in times like these where there is a huge need for freely accessible quick screening tools, shortly after trauma and for monitoring the course of the range of posttraumatic reactions.
The success of the Global Collaboration on Traumatic Stress is reflected in four new themes adopted (presented in greater detail on the https://gps.global-psychotrauma.net/).
With over 70 million forcibly displaced persons worldwide, Theme 2 ‘Forcibly displaced persons’ (led by Angela Nickerson) was the topic all traumatic stress societies agreed on as the next most important global issue to address. The project ‘Post-Displacement Stressors and mental health of refugees and asylum-seekers’ (D-STRESS) proposes to advance knowledge regarding the conceptualization, measurement and impact of ongoing stressors experienced by individuals from refugee backgrounds.
ICD-11 represents the primary diagnostic manual used worldwide, and includes a new and distinct model of stress-related psychopathology. Therefore, Theme 3 ‘Global prevalence of stress and trauma related disorders’ (led by Philip Hyland) with the main project ‘Global assessment of the ICD-11 stress-related disorders (G-Stress)’ aims to determine the global prevalence rates of these disorders.
Theme 4 ‘Socio-emotional development across cultures’ (led by Monique Pfaltz), with the main project ‘Cross-cultural Emotion Recognition in traumatized individuals across the life span’ (CROSS-ER) will inform us on emotional, cognitive, behavioural and physiological developmental processes across the lifespan in individuals with and without childhood maltreatment across different cultures.
Theme 5, ‘Collaborating to make traumatic stress research data “FAIR”’ (led by Nancy Kassam-Adams), is based on the Open Science FAIR Guiding Principles, i.e. to make data Findable, Accessible, Inter-operable, and Re-usable (FAIR). Today we often cannot even find available traumatic stress data. Making traumatic stress research data more FAIR can promote better science and enhance understanding of trauma impact and recovery.
Finally, we recently launched a Theme 6, Global crises, currently focusing on the COVID-19 pandemic (see https://www.global-psychotrauma.net/corona).
Each of these themes will in the end help us to better understand trauma survivors worldwide, and to better prevent and treat the wide range of consequences of traumatic experiences. These collective endeavours can ultimately benefit trauma-exposed individuals and communities around the world. We are looking forward to collaborating with colleagues around the world on these global issues.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Baekkelund, H., Frewen, P., Lanius, R., Ottesen Berg, A., & Arnevik, E. A. (2018). Trauma-related altered states of consciousness in post-traumatic stress disorder patients with or without comorbid dissociative disorders. European Journal of Psychotraumatology, 9(1), doi:10.1080/20008198.2018.1544025.
- Bisson, J. I., Berliner, L., Cloitre, M., Forbes, D., Jensen, T. K., Lewis, C., … Shapiro, F. (2019). The international society for traumatic stress studies. New guidelines for the prevention and treatment of PTSD: Methodology and development process. Journal of Traumatic Stress, 32(4), 471–8.
- Bisson, J. I., Tavakoly, B., Witteveen, A. B., Ajdukovic, D., Jehel, L., Johansen, V., … Olff, M. (2010). TENTS guidelines: Development of post-disaster psychosocial care guidelines through a Delphi process. British Journal of Psychiatry, 196(1), 69–74.
- Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., & Domino, J. L. (2015, December). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress, 28(6), 489–498.
- Bondjers, K., Hyland, P., Roberts, N. P., Bisson, J. I., Willebrand, M., & Arnberg, F. K. (2019). Validation of a clinician-administered diagnostic measure of ICD-11 PTSD and complex PTSD: The international trauma interview in a Swedish sample. European Journal of Psychotraumatology, 10(1), doi:10.1080/20008198.2019.1665617.
- Brewin, C. R., Rose, S., Andrews, B., Green, J., Tata, P., McEvedy, C., & Foa, E. B. (2002). Brief screening instrument for post-traumatic stress disorder. British Journal of Psychiatry, 181(2), 158–162.
- Brunet, A., Weiss, D. S., Metzler, T. J., Best, S. R., Neylan, T. C., Rogers, C., & Marmar, C. R. (2001). The peritraumatic distress inventory: A proposed measure of PTSD criterion A2. American Journal of Psychiatry, 158(9), 1480–1485.38.
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., … Hyland, P. (2018). The international trauma questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546.
- Cramer, A. O., Waldorp, L. J., van der Maas, H. L., & Borsboom, D. (2010). Comorbidity: A network perspective. Behavioral and Brain Sciences, 33(2–3), 137–150.
- Frewen, P. A., Brown, M. F. D., De Pierro, J., D’Andrea, W., & Schore, A. (2015a). Assessing the family dynamics of childhood maltreatment history with the childhood attachment and relational trauma screen (CARTS). European Journal of Psychotraumatology, 6(1), 27792.
- Frewen, P. A., Brown, M. F. D., Steuwe, C., & Lanius, R. A. (2015b). Latent profile analysis and principal axis factoring of the DSM-5 dissociative subtype. European Journal of Psychotraumatology, 6(1), 1.
- Frewen, P. A., Evans, B., Goodman, J., Halliday, A., Boylan, J., Moran, G., … Lanius, R. A. (2013). Development of a childhood attachment and relational trauma screen (CARTS): A relational-socioecological framework for surveying attachment security and childhood trauma history. European Journal of Psychotraumatology, 4, 1–17.
- Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., … Survey, W. W. M. H. (2017). Trauma and PTSD in the WHO world mental health surveys. European Journal of Psychotraumatology, 8(1), doi:10.1080/20008198.2017.1353383.
- Lewis, C., Roberts, N., Andrew, M., Starling, E., & Bisson, J. (2020). Psychological therapies for post-traumatic stress disorder in adults: Systematic review and meta-analysis. European Journal of Psychotraumatology, 11 (1). doi: 10.1080/20008198.2019.1709709.
- McLaughlin, K. A., Koenen, K. C., Friedman, M. J., Ruscio, A. M., Karam, E. G., Shahly, V., … Kessler, R. C. (2015). Subthreshold posttraumatic stress disorder in the world health organization world mental health surveys. Biological Psychiatry, 77(4), 375–384.
- Mouthaan, J., Sijbrandij, E. M., Reitsma, J. B., Gersons, B. P. R., & Olff, M. (2014). Comparing screening instruments to predict posttraumatic stress disorder. Plos One, 9(5), e97183.
- NICE. (2018). Guidelines for post-traumatic stress disorder. NICE guideline (NG116). Retrieved from https://www.nice.org.uk/guidance/ng116
- Olff, M. (2014). From iSTSS to ISTSS - Traumatic stress around the globe. ISTSS StressPonts. Retrieved from http://www.istss.org/education-research/traumatic-stresspoints/2014-december/president%E2%80%99s-message-from-istss-to-istss-traumatic.aspx
- Olff, M., Amstadter, A., Armour, C., Birkeland, M. S., Bui, E., Cloitre, M., … Thoresen, S. (2019). A decennial review of psychotraumatology: What did we learn and where are we going? European Journal of Psychotraumatology, 10(1), doi:10.1080/20008198.2019.1672948.
- Olff, M., Langeland, W., & Gersons, B. P. R. (2005). Effects of appraisal and coping on the neuroendocrine response to extreme stress. Neuroscience and Biobehavioral Reviews, 29(3), 457–467.
- Prins, A., Bovin, M. J., Smolenski, D. J., Marx, B. P., Kimerling, R., Jenkins-Guarnieri, M. A., … Tiet, Q. Q. (2016). The primary care PTSD screen for DSM-5 (PC-PTSD-5): Development and evaluation within a veteran primary care sample. Journal of General Internal Medicine, 31(10), 1206–1211.
- Roberts, N. P., Kitchiner, N. J., Kenardy, J., Lewis, C. E., & Bisson, J. I. (2019). Early psychological intervention following recent trauma: A systematic review and meta-analysis. European Journal of Psychotraumatology, 10(1), doi:10.1080/20008198.2019.1695486.
- Schnyder, U., & Olff, M. (2013). The global initiative, ISTSS StressPoints. Retrieved from http://www.istss.org/education-research/traumatic-stresspoints/2013-march/the-global-initiative.aspx
- Schnyder, U., Schafer, I., Aakvaag, H. F., Ajdukovic, D., Bakker, A., Bisson, J. I., … Olff, M. (2017). The global collaboration on traumatic stress. European Journal of Psychotraumatology, 8(S7), doi:10.1080/20008198.2017.1403257.
- Shevlin, M., Hyland, P., Roberts, N. P., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2018). A psychometric assessment of disturbances in self-organization symptom indicators for ICD-11 complex PTSD using the international trauma questionnaire. European Journal of Psychotraumatology, 9(1), doi:10.1080/20008198.2017.1419749.
- Sijbrandij, M., Olff, M., Opmeer, B. C., Carlier, I. V., & Gersons, B. P. (2008). Early prognostic screening for posttraumatic stress disorder with the Davidson trauma scale and the SPAN. Depress Anxiety, 25, 1038–1045.
- Simonelli, A., Sacchi, C., Cantoni, L., Brown, M., & Frewen, P. A. (2017). Italian translation and cross-cultural comparison with the Childhood Attachment and Relational Trauma Screen (CARTS). European Journal of Psychotraumatology, 8(1), doi:10.1080/20008198.2017.1375839.
- Sousa, V. D., & Rojjanasrirat, W. (2011). Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. Journal of Evaluation in Clinical Practice, 17, 268–274.
- van der Kolk, B., Ford, J. D., & Spinazzola, J. (2019). Comorbidity of developmental trauma disorder (DTD) and post-traumatic stress disorder: Findings from the DTD field trial. European Journal of Psychotraumatology, 10(1), doi:10.1080/20008198.2018.1562841.
- Van der Meer, C. A. I., Te Brake, H., Van der Aa, N., Dashtgard, P., Bakker, A., & Olff, M. (2018). Assessing psychological resilience: Development and psychometric properties of the English and Dutch version of the Resilience Evaluation Scale (RES). Frontiers in Psychiatry, 9. doi:10.3389/fpsyt.2018.00169
- Weiss, D. S., & Marmar, C. R. (1997). The impact of event scale-revised. In J. P. Wilson & T. M. Keane (Eds.), Assessing psychological trauma and PTSD (pp. 399–411). New York: Guilford Press.