
ABSTRACT
Background: Empathy is essential for interpersonal relationships, yet remains difficult to measure. Some evidence suggests that early traumatic experiences leads to alterations in empathic responding.
Objective: This study sought to differentiate connections between subtypes of childhood maltreatment, a pictorial test of affective empathy (PET), and self-reported empathy (Interpersonal Reactivity Index; IRI) by using network analysis approach to investigate the structure of relationships between childhood maltreatment and later empathic responding.
Method: 301 participants completed the PET, the Early Trauma Inventory Self Report-Short Form (ETISR-SF), the IRI, and questionnaires assessing current mood and perceived stress levels.
Results: The PET showed a strong positive association with the IRI subscale empathic concern (EC), after conditioning on all other nodes in the network. EC proved to be a highly central node and was positively related to severity of childhood sexual abuse (CSA), yet not to childhood physical abuse or emotional maltreatment. Pathways between emotional maltreatment and physical abuse and the PET were indirect, passing through self-reported EC and CSA.
Conclusions: Our study suggests that CSA more so than other childhood maltreatment experiences is associated with increased self-reported affective empathy, but is not captured directly through a pictorial test of affective empathy.
Antecedentes: La empatía es esencial para las relaciones interpersonales, pero sigue siendo difícil de medir. Alguna evidencia sugiere que las experiencias traumáticas tempranas conducen a alteraciones en la respuesta empática.
Objetivo: Este estudio buscó diferenciar las conexiones entre los subtipos de maltrato infantil, una prueba pictórica de empatía afectiva (PET) y la empatía auto-reportada (Índice de reactividad interpersonal; IRI) mediante el uso de un enfoque de análisis de red para investigar la estructura de las relaciones entre el maltrato infantil y la respuesta empática posterior.
Método: 301 participantes completaron el PET, el Formulario abreviado del inventario de trauma temprano auto-reportado (ETISR-SF), el IRI y cuestionarios para evaluar el estado de ánimo actual y los niveles de estrés percibidos.
Resultados: Después del acondicionamiento en todos los demás nodos de la red, el PET mostró una fuerte asociación positiva con la preocupación empática (CE) de la sub-escala IRI. La CE demostró ser un nodo altamente central y se relacionó positivamente con la gravedad del abuso sexual infantil (CSA), pero no con el abuso físico infantil o el maltrato emocional. Las conexiones entre el maltrato emocional y el abuso físico con la PET fueron indirectas, pasando a través de CE y CSA auto-reportados.
Conclusiones: Nuestro estudio sugiere que el Abuso Sexual Infantil, más que otras experiencias de maltrato infantil, se asocia con una mayor empatía afectiva auto-reportada, pero no se observa directamente a través de una prueba pictórica de empatía afectiva.
目的: 本研究旨在通过网络分析方法探究童年期虐待与之后共情反应之间的关系结构, 以区分童年期虐待亚型, 情感共情图画测验 (PET) 和自我报告共情 (人际反应指数: IRI) 之间的联系。
方法: 301名参与者完成了PET, 早期创伤问卷自评简表 (ETISR-SF), IRI和评估当前情绪与感知应激水平的问卷。
结果: 在控制网络中所有其他结点之后, PET表现出与IRI中共情关注 (EC) 分量表很强的正相关。EC被证明是一个高度中心结点, 与童年期性虐待 (CSA) 的严重程度呈正相关, 但与童年期身体虐待或情感虐待无关。情感虐待, 身体虐待与PET之间的路径是间接通过自我报告的EC和CSA连接的。
结论: 我们的研究表明, 与童年期其他虐待经历相比, CSA与自我报告的情感共情增强有关, 但这一点不能通过情感移情图画测试直接捕捉到。
1. Introduction
Although it has been hypothesized that childhood maltreatment (CM) may lead to long-term alterations in interpersonal functioning (Briere & Jordan, Citation2009) including empathy, findings are presently mixed. For instance, whereas some studies suggest reduced empathy in maltreated children (Ometto et al., Citation2016), others found no deficits in empathic responding (McCloskey & Lichter, Citation2003). Similarly, whereas in some adult women with CM experience perspective-taking abilities and empathic concern are reduced, but personal distress is increased (Parlar et al., Citation2014), others documented higher empathic concern but lower personal distress (Hudson et al., Citation2020). Supporting the latter, Vollhardt and Staub (Citation2011) found that victims of adverse life events showed more empathy and felt more responsibility to help victims of a natural disaster.
One explanation for such mixed findings is that empathy as a construct remains difficult to measure. Evidence suggests that empathy is multidimensional, incorporating both cognitive (recognising others’ emotions and perspective-taking) and affective (sharing in another’s affective state) elements (Shamay-Tsoory, Aharon-Peretz, & Perry, Citation2009). Self-report measures have also been criticised as probing ability rather than propensity (Keysers & Gazzola, Citation2014) and reactions are not necessarily authentic (Lindeman, Koirikivi, & Lipsanen, Citation2018). Importantly, self-reported empathy and actual behavioural empathic responding may not correlate (Locher, Barenblatt, Fourie, Stein, & Gobodo-Madikizela, Citation2014).
To solve this problem, Lindeman et al. (Citation2018) developed the Pictorial Empathy Test (PET) to measure affective empathy and empathic responding. Participants rate how emotionally moving they find photographs of people in distress. Empathic feelings can thus be captured immediately, unlike questionnaires, which are retrospective. Compared to measures such as the Multifaceted Empathy Test (Dziobek et al., Citation2008), the PET is short and easy to complete, and therefore highly suitable for internet-based research with large samples (Lindeman et al., Citation2018). Furthermore, a photo-based measure has stronger ecological validity, leans closer to everyday situations compared to questionnaires, and may facilitate responding in clinical samples, who may have problems verbalizing their responses with questionnaires (Dziobek et al., Citation2008; Lindeman et al., Citation2018).
Recently, data-driven network analyses have become increasingly popular to analyse and visualise the complex relationship structure among constructs in psychopathology (Borsboom & Cramer, Citation2013). An advantage of network approaches over common approaches (e.g. mediation models) is that they are 1) less restrictive, 2) bottom-up data-driven, and 3) able to more realistically canvass the complex nature of the relationship among many different dimensions of symptoms and constructs. Because of these advantages, other’s have advocated the utility of such an approach for maltreatment and PTSD, especially in light of frequent comorbid psychopathology (McNally et al., Citation2015). Indeed, because research indicates strong associations between CM and later psychopathology (Jaffee, Citation2017) and links between affective disorders and interpersonal problems, a network approach may be ideal to explore their role.
Therefore, using the network approach, this study assessed 1) how individual subtypes of CM (while accounting for other CM types) may be connected to empathic responding, 2) whether such a connection may be better explained by the PET or standard questionnaires of empathy and 3) determine the contributing role of mood and anxiety symptoms.
2. Methods
2.1. Participants
315 participants were recruited through Prolific (https://prolific.ac/) for an online study titled ‘How emotionally moving do you find this photograph?’ and received £1.67 as compensation. Of the 310 completed the study, nine participants were excluded due to a post-experimental inclusion criterion of passing all ‘catch’ questions included to ensure participants were not answering at random. Thus, the final sample therefore comprised 301 participants (cf. , ). The study was programmed using Qualtrics (Provo, UT, USA) and allowed only single attempts from IP addresses to prevent multiple entry attempts. Pre-set eligibility requirements were fluency in English, being 18–50 years old, participation in ≤ 30 previous Prolific studies, and a Prolific approval rating of > 90% for previously-completed studies. The study was approved by the local ethical committee and all participants gave electronic informed consent before commencing.
Table 1. Sample characteristics.
Table 2. Summary of questionnaire data.
2.2. Materials
2.2.1. Pictorial Empathy Test
The Pictorial Empathy Test (PET; Lindeman et al., Citation2018) comprises seven photographs of individuals in physical and/or emotional distress (Supplementary Figure 1) and is thought to measure affective empathy. For each photograph, participants are asked ‘How emotionally moving do you find the photograph?’ using a 5-point Likert scale from ‘not at all’ to ‘very much’. The PET is scored by calculating the average score. Participants may spend as much time as needed viewing each photograph. None of the pictures contains a direct gaze at the observer. Internal validity of the 7 items was good (Cronbach’s α = .87) and replicated that of the developers (α = .90).
2.2.2. Questionnaires
IRI. The Interpersonal Reactivity Index (IRI; Davis, Citation1983) measures self-reported empathy using 28 items rated on 5-point Likert scales. The questionnaire assesses both cognitive (perspective-taking, Cronbach’s αpresent = .82; fantasy, αpresent = .82) and affective (empathic concern, αpresent = .87; personal distress, αpresent = .85) empathy.
ETISR-SF. The Early Trauma Inventory-Self Report short form (ETISR-SF; Bremner, Bolus, & Mayer, Citation2007) assesses traumatic exposure by simply answering yes/no to each item. One section (11 items) assesses general traumas (αpresent = .70), whereas three sections assess CM: physical punishment (5 items, αpresent = .77), emotional maltreatment (5 items, αpresent = .85), and sexual events (6 items, αpresent = .82).
MASQ-30. The Mood and Anxiety Symptoms Questionnaire 30-item short adaptation (MASQ-30; Wardenaar et al., Citation2010) comprises 10 items assessing anxious arousal (αpresent = .90), 10 items assessing anhedonic depression (αpresent = .92), and 10 items assessing general distress (αpresent = .92). Respondents rate each item on 5-point Likert scales for how much they have experienced it within the past week.
PSS. The Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, Citation1983) assesses respondents’ stress levels in the preceding month using 14 items answered on 5-point Likert scales (αpresent = .87).
2.3. Procedure
Participants performed the study online from their personal computer (Mtime = 13.25 minutes, SD = 5.94 minutes), first completing the PET, followed by the questionnaires in randomised order. PET items were presented individually and in randomised order; questionnaires were presented on individual pages, with items randomised. In the IRI, MASQ-30, and PSS, ‘catch’ questions (e.g. ‘answer this question with “extremely”’) were included to ensure participants were not answering at random. ‘Catch’ questions were not included in the PET or ETI due to their sensitive nature. Lastly, participants completed demographics questions. Finally, participants read a short explanation of the study aims and a reiteration of confidentiality/anonymity.
2.4. Network analyses
A regularised conditional independence network was constructed using state-of-the-art standard methodologyFootnote1 comprising scores on: IRI affective empathy subscales (empathic concern [EC] and personal distress [PD]), IRI cognitive empathy subscales (perspective-taking [PT] and fantasy [FS]), PET, ETI-SF subscales for child physical abuse (CPA; physical punishment), child sexual abuse (CSA; sexual events), child emotional maltreatment (CEM; emotional abuse), general trauma (general traumas), and MASQ-30 subscales, and PSS.
Edges represent regularised partial correlations between two nodes and indicate an association between two items or variables after controlling for all other nodes in the network. To reduce the likelihood of spurious connections (see Costantini et al., Citation2015), a graphical least absolute shrinkage and selection operator (gLASSO; Friedman, Hastie, & Tibshirani, Citation2008) was applied with an Extended Bayesian Information Criterion (EBIC) tuning parameter of γ = .5 (Foygel & Drton, Citation2010). For ease of visualisation, a minimum absolute value of 0.03 was set for edge weights (Isvoranu et al., Citation2017).
Nodes were then investigated for importance in the resultant network. Network stability was assessed by use of bootstrapped centrality-stability (CS) coefficients and 95% confidence intervals (CIs) around edge weights. CS-coefficients indicate the proportion of data that can be dropped and still retain a correlation of >.7 with the original centrality indices, and should be preferably above .5 and not below .25 (Epskamp & Fried, Citation2018).
3. Results
3.1. Network analyses
n the regularised partial correlation network (), PET responses were strongly positively associated with self-reported EC when controlling for CM exposure, general traumatic exposure, and psychopathology. However, no associations emerged with other IRI subscales or CM. EC showed positive associations with all IRI subscales.
Figure 1. Network depicting conditional relationships between childhood maltreatment history, self-reported empathy, behavioural empathic responding, and psychopathology. Domains are differentiated by colour. Thicker edges represent stronger relative connections (solid dark cyan lines indicate a positive association, dashed red lines indicate negative). Edges with a minimum absolute value below .03 are not depicted. EBIC tuning parameter set at γ = .5 to maximise specificity and minimise the risk of spurious connections.
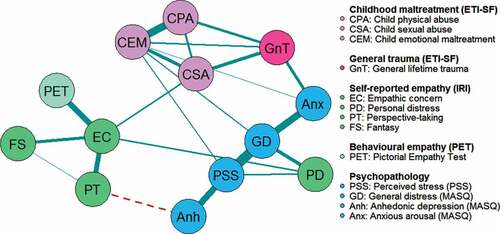
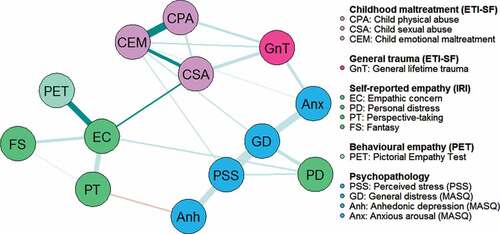
Severity of CSA was positively related to EC when conditioned on all other nodes, yet no other IRI subscales. Neither CEM nor CPA were related to any IRI subscale; CM subtypes were moderately-to-strongly positively interrelated, as well as positively related to general traumatic exposure. Pathways to self-reported empathic responding from CPA and CEM lay through CSA – i.e. severity of CSA exposure acted as a bridge between CPA/CEM and EC ().
Regarding psychopathology, neither CSA nor CPA showed any direct associations but CEM showed modest associations with general distress and perceived stress. General trauma was moderately positively associated with self-reported anxious arousal. In sum, pathways to psychopathology from CSA and CPA lay through general traumatic exposure and CEM. A secondary pathway through self-reported empathy (EC and PT) also linked CSA and feelings of anhedonia. When gender was additionally taken into consideration, an indirect, second, path between CSA and EC was created, indicating a positive association between EC and CSA for women (Supplementary Figure 2).
Figure 2. Shortest paths from childhood maltreatment to Pictorial Empathy Test scores.
3.2. Centrality
EC was a particularly central node, facilitating the most links between other nodes (betweenness) and most relevantly, links between other IRI subscales and CM exposure (). Self-reported general distress was also a central node, with the highest closeness and strength centrality indices in the network, facilitating connections with other psychopathology nodes. PET score was the second-least central node, after fantasy abilities.
Figure 3. Node centrality. ‘Betweenness’ measures the number of times a node lies on the shortest path between two other nodes. ‘Closeness’ refers to the average distance to other nodes. ‘Strength’ measures the number and strength of connections with other nodes in the network. Note: z-scores are shown on the x-axis rather than raw centrality indices. For each measure, a higher score indicates a more central node.
3.3. Network accuracy and stability
The case-dropping bootstrap revealed that strength centrality was the most stable of the centrality indices (Supplementary Figure 3), which parallels previous literature (Epskamp, Borsboom, & Fried, Citation2018). CS-coefficients were .74 for node strength and .31 for node closeness, indicating stability, yet .17 for node betweenness indicating this should be interpreted cautiously. Bootstrapped CIs around estimated edge-weights are shown in Supplementary Figure 4.
4. Discussion
Using a network approach, this study aimed to unravel the complex relationship among maltreatment subtypes and empathy, as well as examining the utility of the PET in relation to standard questionnaires of empathy. With regards to the first hypothesis of maltreatment type and empathic responding, the first main finding was that CSA, but not CEM or CPA, was independently and directly associated with increased self-reported empathic concern. Moreover, CSA was only indirectly related to increased empathic responding on the PET (via the EC node). A positive association between maltreatment and empathic concern thus replicates prior work (Hudson et al., Citation2020; Vollhardt & Staub, Citation2011). Moreover, it suggests that despite criticisms against self-report (Keysers & Gazzola, Citation2014; Lindeman et al., Citation2018), the strong centrality of the IRI’s empathic concern node in the data appears to support its validity.
Indeed, the second main finding was that the PET score was not directly related to the CM node thus suggesting limited suitability of this measure in maltreatment samples. Lack of such a connection might indicate that while someone with more severe CSA exposure is more likely to self-report higher EC, they are no more (or less) likely to be emotionally moved by photographs of people in distress. Along this line, Locher et al. (Citation2014) also discovered discrepancies between self-reported and experimenter-assessed empathy in maltreated adults, with participants scoring themselves as higher on empathy than independent assessors did.
Alternatively, some evidence suggests that severity itself may play a role. Parlar’s (Citation2014) study focused on differences between healthy controls and women with maltreatment-related PTSD, whereas our study focused on a representative community sample and only had few people reporting PTSD diagnoses (5.3%). In Mrug, Madan, Cook, and Wright (Citation2015) empathy was highest amongst college students who had medium levels of violence exposure, but were diminished for low/severe exposure. Relative to Bremner’s (Citation2007) original investigation of the ETISR-SF’s psychometric properties, our sample’s average CM exposure lies in-between his average exposure for healthy controls and known CM survivors without psychiatric disorder. This may be related to the study sample.
Despite prolific academic’s reputation for the quality and representativeness of a general population sample, trauma and psychopathology (MASQ) scores were slightly on the higher end relative to a normative group (Tully, Wardenaar, & Penninx, Citation2015) and thus confirm elevated scores in internet samples relative to samples recruited in labs. Importantly, when gender was included in the network, a second path between CSA and EC emerged. This is not unexpected as women tend to score higher on empathic responsiveness (Lindeman et al., Citation2018) and report more CSA (Stoltenborgh, van IJzendoorn, Euser, & Bakermans-Kranenburg, Citation2011), but it is crucial to note that a direct (but reduced) relationship remained despite this.
With regards to mental health, a third noteworthy finding was that a pathway from CSA to anhedonic depression lay through the empathic concern and perspective-taking nodes. Individuals with more severe CSA exposure showed increased EC, which was positively related to PT, which was negatively related to anhedonia. This finding poses important clinical implications as it might suggest a buffering effect of empathic responsiveness against depression, plausibly via improved interpersonal relationships (Sened et al., Citation2017) leading to increased social support (Fritz, de Graaff, Caisley, van Harmelen, & Wilkinson, Citation2018). Although the underlying mechanisms of this effect are yet unknown, a recent study documented that resting-state brain activity in theory of mind areas depended on severity and number of abuse types in maltreated women (Boccadoro et al., Citation2019). This begs for further inquiry on how social skills change in maltreated people. Simultaneously, another path between CSA and psychopathology lay through general traumatic exposure. Here, individuals with more severe CSA were likely to have experienced a greater degree of general trauma, including dysfunctional family life, which in turn was associated with more severe psychopathology. Thus, it appears that interventions targeting empathy are essential to guard against poor mental health in CM survivors. In a longitudinal study, Caputi, Lecce, Pagnin, and Banerjee (Citation2012) documented that early theory of mind mediated lower peer rejection (or higher peer acceptance) via prosocial behaviour. Thus, one question will be how negative trajectories of social development through maltreatment experience can be buffered and counteracted.
Despite these important clinical implications, some limitations warrant discussion. Firstly, the ETISR-SF asks respondents if they have ever experienced particular events, but does not ask about their frequency. Thus, our measurement of CM severity is only approximate. Moreover, we did neither measure nor select for PTSD symptoms and cannot assess its potential mediating role. Yet, the ETISR-SF is able to discriminate known CM survivors from controls and furthermore a simple sum of experienced events is often sufficient for assessing severity (Bremner et al., Citation2007). Secondly, the PET can only be used to assess an individual’s initial reaction to a distressing image and not their tendency to act on those feelings. Moreover, since a) we wanted participants to be naïve when encountering the PET without priming people about the topic and b) because it was very short and a non-verbal task, it was always presented first. However, this may have resulted in potential bias effects on the subsequent questionnaires that could not be assessed.
In summary, future research could investigate network associations between maltreatment exposure and develop behavioural empathy tasks (e.g. in virtual reality), that might specifically assess the propensity to act empathically.
Supplemental Material
Download MS Word (1.8 MB)Supplemental Material
Download MS Word (1.8 MB)Disclosure statement
No potential conflict of interest was reported by the authors.
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
Notes
1. For full details, see supplementary information.
References
- Boccadoro, S., Siugzdaite, R., Hudson, A. R., Maeyens, L., Van Hamme, C., & Mueller, S. C. (2019). Women with early maltreatment experience show increased resting-state functional connectivity in the theory of mind (ToM) network. European Journal of Psychotraumatology, 10(1), 1,1647044.
- Borsboom, D., & Cramer, A. O. J. (2013). Network analysis: An integrative approach to the structure of psychopathology. Annual Review of Clinical Psychology, 9(1), 91–7.
- Bremner, J. D., Bolus, R., & Mayer, E. A. (2007). Psychometric properties of the early trauma inventory? Self report. The Journal of Nervous and Mental Disease, 195(3), 211–218.
- Briere, J., & Jordan, C. E. (2009). Childhood maltreatment, intervening variables, and adult psychological difficulties in women. Trauma, Violence, & Abuse, 10(4), 375–388.
- Caputi, M., Lecce, S., Pagnin, A., & Banerjee, R. (2012). Longitudinal effects of theory of mind on later peer relations: The role of prosocial behavior. Developmental Psychology, 48(1), 257–270.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396.
- Costantini, G., Epskamp, S., Borsboom, D., Perugini, M., Mõttus, R., Waldorp, L. J., & Cramer, A. O. J. (2015). State of the aRt personality research: A tutorial on network analysis of personality data in R. Journal of Research in Personality, 54, 13–29.
- Davis, M. H. (1983). Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of Personality and Social Psychology, 44(1), 113–126.
- Dziobek, I., Rogers, K., Fleck, S., Bahnemann, M., Heekeren, H. R., Wolf, O. T., & Convit, A. (2008). Dissociation of cognitive and emotional empathy in adults with Asperger syndrome using the Multifaceted Empathy Test (MET). Journal of Autism and Developmental Disorders, 38(3), 464–473.
- Epskamp, S., Borsboom, D., & Fried, E. I. (2018). Estimating psychological networks and their accuracy: A tutorial paper. Behavior Research Methods, 50(1), 195–212.
- Epskamp, S., & Fried, E. I. (2018). A tutorial on regularized partial correlation networks. Psychological Methods, 23(4), 617–634.
- Foygel, R., & Drton, M. (2010). Extended Bayesian information criteria for Gaussian graphical models. Advances in Neural Information Processing Systems, 23, 2020–2028.
- Friedman, J. H., Hastie, T., & Tibshirani, R. (2008). Sparse inverse covariance estimation with the graphical lasso. Biostatistics, 9(3), 432–441.
- Fritz, J., de Graaff, A. M., Caisley, H., van Harmelen, A.-L., & Wilkinson, P. O. (2018). A systematic review of amenable resilience factors that moderate and/or mediate the relationship between childhood adversity and mental health in young people. Frontiers in Psychiatry, 9, 230.
- Hudson, A. R., De Coster, L., Spoormans, H., Verbeke, S., Van der Jeught, K., Brass, M., Mueller, S.C. (2020). Childhood abuse and adult sociocognitive skills: Distinguishing between self and other following early trauma. Journal of Interpersonal Violence. doi:10.1177/0886260520906190
- Isvoranu, A.-M., van Borkulo, C. D., Boyette, -L.-L., Wigman, J. T. W., Vinkers, C. H., & Borsboom, D. (2017). A network approach to psychosis: Pathways between childhood trauma and psychotic symptoms. Schizophrenia Bulletin, 43(1), 187–196.
- Jaffee, S. R. (2017). Child maltreatment and risk for psychopathology in childhood and adulthood. Annual Review of Clinical Psychology, 13(1), 525–551.
- Keysers, C., & Gazzola, V. (2014). Dissociating the ability and propensity for empathy. Trends in Cognitive Sciences, 18(4), 163–166.
- Lindeman, M., Koirikivi, I., & Lipsanen, J. (2018). Pictorial Empathy Test (PET). European Journal of Psychological Assessment, 34(6), 421–431.
- Locher, S. C., Barenblatt, L., Fourie, M. M., Stein, D. J., & Gobodo-Madikizela, P. (2014). Empathy and childhood maltreatment: A mixed-methods investigation. Annals of Clinical Psychiatry : Official Journal of the American Academy of Clinical Psychiatrists, 26(2), 97–110.
- McCloskey, L. A., & Lichter, E. L. (2003). The contribution of marital violence to adolescent aggression across different relationships. Journal of Interpersonal Violence, 18(4), 390–412.
- McNally, R. J., Robinaugh, D. J., Wu, G. W. Y., Wang, L., Deserno, M. K., & Borsboom, D. (2015). Mental disorders as causal systems. Clinical Psychological Science, 3(6), 836–849.
- Mrug, S., Madan, A., Cook, E. W., & Wright, R. A. (2015). Emotional and physiological desensitization to real-life and movie violence. Journal of Youth and Adolescence, 44(5), 1092–1108.
- Ometto, M., de Oliveira, P. A., Milioni, A. L., Dos Santos, B., Scivoletto, S., Busatto, G. F., & Cunha, P. J. (2016). Social skills and psychopathic traits in maltreated adolescents. European Child & Adolescent Psychiatry, 25(4), 397–405.
- Parlar, M., Frewen, P., Nazarov, A., Oremus, C., MacQueen, G., Lanius, R., & McKinnon, M. C. (2014). Alterations in empathic responding among women with posttraumatic stress disorder associated with childhood trauma. Brain and Behavior, 4(3), 381–389.
- Sened, H., Lavidor, M., Lazarus, G., Bar-Kalifa, E., Rafaeli, E., & Ickes, W. (2017). Empathic accuracy and relationship satisfaction: A meta-analytic review. Journal of Family Psychology, 31(6), 742–752.
- Shamay-Tsoory, S. G., Aharon-Peretz, J., & Perry, D. (2009). Two systems for empathy: A double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain, 132(3), 617–627.
- Stoltenborgh, M., van IJzendoorn, M. H., Euser, E. M., & Bakermans-Kranenburg, M. J. (2011). A global perspective on child sexual abuse: Meta-analysis of prevalence around the world. Child Maltreatment, 16(2), 79–101.
- Tully, P. J., Wardenaar, K. J., & Penninx, B. W. J. H. (2015). Operating characteristics of depression and anxiety disorder phenotype dimensions and trait neuroticism: A theoretical examination of the fear and distress disorders from the Netherlands study of depression and anxiety. Journal of Affective Disorders, 174, 611–618.
- Vollhardt, J. R., & Staub, E. (2011). Inclusive altruism born of suffering: The relationship between adversity and prosocial attitudes and behavior toward disadvantaged outgroups. American Journal of Orthopsychiatry, 81(3), 307–315.
- Wardenaar, K. J., van Veen, T., Giltay, E. J., de Beurs, E., Penninx, B. W. J. H., & Zitman, F. G. (2010). Development and validation of a 30-item short adaptation of the Mood and Anxiety Symptoms Questionnaire (MASQ). Psychiatry Research, 179(1), 101–106.