
ABSTRACT
Background: The estimated prevalence rate of comorbid posttraumatic stress disorder (PTSD) is high in trauma-exposed chronic pain patients. At the same time, self-report measures of PTSD tend to be over-inclusive within this specific population due to the high symptom overlap resulting in potential false positives. There is a need for an updated PTSD screening tools with a proper validation against clinical interviews according to the recently published 11th revision of the World Health Organization’s International Classification of Diseases (ICD-11).
Objective: The present study aimed to validate the Danish International Trauma Questionnaire (ITQ) PTSD part in a sample of trauma-exposed chronic pain patients.
Method: The ITQ was validated using a clinician-rated diagnostic interview of ICD-11 PTSD among chronic pain patients exposed to accident or work-related trauma (N = 40). Construct validity, concurrent and discriminant validity was investigated using confirmatory factor analyses (CFA) and correlation analysis, respectively. Three CFA models of ITQ PTSD part were tested in a sample of trauma-exposed chronic pain patients (N = 1,017) and a subsample of chronic pain patients exposed to accident or work-related trauma only (n = 367).
Results: Diagnostic consistency between the six ICD-11 PTSD symptoms derived from the ITQ and the clinical interview (κ = .59) and the overall accuracy of the scale (AUC = .90) were good. The Danish ITQ showed excellent construct, concurrent and discriminant validity. The ICD-11 three factor PTSD model had excellent fit in both the full sample and the subsample of traffic and work-related accidents.
Conclusions: The results indicate that the ITQ also has good psychometric properties in patients with chronic pain.
HIGHLIGHTS
• This study provides the first validation of the ITQ for PTSD using diagnostic interview in trauma-exposed chronic pain patients.
•Good diagnostic consistency and the overall accuracy as well as excellent construct, concurrent and discriminant validity were established.
Antecedentes: La prevalencia estimada del trastorno de estrés postraumático (TEPT) como comorbilidad es alta en los pacientes con dolor crónico expuestos a trauma. Asimismo, las mediciones por autorreporte del TEPT suelen ser en exceso incluyentes para este tipo de población debido a que existe una alta superposición de los síntomas, lo que resulta en potenciales resultados falsos positivos. Existe la necesidad de actualizar las herramientas de tamizaje del TEPT con una validación adecuada y acorde con las entrevistas clínicas basadas en la recientemente publicada 11° revisión de la Clasificación Internacional de Enfermedades de la Organización Mundial de la Salud (CIE-11).
Objetivo: El objetivo de este estudio fue el de validar la sección del TEPT del Cuestionario Internacional de Trauma danés (ITQ, por sus siglas en inglés) en una muestra de personas con dolor crónico expuestas a trauma.
Método: Se validó el ITQ empleando una entrevista diagnóstica para el TEPT según la CIE-11 calificada por un clínico en pacientes con dolor crónico expuestos a accidentes o a traumas relacionados con el trabajo (N = 40). Se investigaron la validez del constructo y la validez concurrente y discriminativa mediante el empleo de análisis confirmatorios de factor (ACF) y análisis de correlación, respectivamente. Los tres modelos realizados mediante ACF de la sección del TEPT del ITQ fueron luego evaluados en una muestra de pacientes con dolor crónico expuestos a trauma (N = 1.017) y en un grupo de esta muestra de pacientes con dolor crónico expuestos únicamente a accidentes o a traumas relacionados con el trabajo (N = 367).
Resultados: Tanto la consistencia diagnóstica entre seis síntomas del TEPT basados en la CIE-11 obtenidos mediante el ITQ y la entrevista diagnóstica (k = .59) como la precisión general de la escala (AUC = .90) fueron buenas. El ITQ danés mostró tanto una validez del constructo como una validez concurrente y discriminativa excelentes. El modelo de tres factores para el TEPT según la CIE-11 tiene una excelente adaptación tanto en la muestra completa como en el grupo tomado de la muestra para accidentes o traumas relacionados con el trabajo.
Conclusiones: Los resultados indican que el ITQ también posee propiedades psicométricas buenas en pacientes con dolor crónico.
背景: 在遭受创伤的慢性疼痛患者中, 并发的创伤后应激障碍 (PTSD) 的估计患病率很高。同时, 在此特定人群中, PTSD的自我报告测量倾向于纳入过多, 由于高度的症状重叠导致潜在的假阳性。根据世界卫生组织最近发布的第11版《国际疾病分类》 (ICD-11), 需要一种经过更新的PTSD筛查工具, 并对临床访谈进行适当验证。
目的: 本研究旨在验证创伤暴露的慢性疼痛患者样本中的丹麦国际创伤问卷 (ITQ) PTSD部分。
方法: 使用临床医师评定的ICD-11 PTSD诊断性访谈对暴露于事故或工作相关创伤的慢性疼痛患者进行了ITQ验证 (N = 40) 。分别使用验证性因子分析 (CFA) 和相关性分析研究了结构效度, 同时效度和区分效度。在创伤暴露的慢性疼痛患者的样本 (N = 1,017) 和仅暴露于事故或工作相关创伤的慢性疼痛患者的子样本 (n = 367) 中检验了三种ITFA PTSD部分的CFA模型。
结果: 从ITQ和临床访谈得出的六个ICD-11 PTSD症状之间的诊断一致性 (k = .59) 和量表的总体准确性 (AUC = .90) 良好。丹麦语ITQ表现出出色的构念, 同时性和区分性。 ICD-11三因素PTSD模型非常适合全部样本和交通事故和工作相关事故的子样本。
结论: 结果表明, ITQ在慢性疼痛患者中也具有良好的心理测量学特性。
1. Introduction
Posttraumatic stress disorder (PTSD) is common in chronic pain patients with estimated PTSD prevalence rates varying from 0% to 57% across 21 chronic pain samples with a pooled mean prevalence of 9.7% (Siqveland, Hussain, Lindstrøm, Ruud, & Hauff, Citation2017). However, the prevalence rates reported are highly varying across studies depending on the specific pain population and PTSD measure with the pooled mean prevalence rates found to be significantly higher when using a self-report measure (20.4%) compared to a diagnostic interview (4.5%, Siqveland et al., Citation2017). Due to the potential symptom overlap between pain and PTSD symptoms, it is not surprising that self-report measures result in false positives in this specific population. For example, a symptom of avoidance due to pain or sleep problems related to pain may be confused as a symptom of PTSD avoidance and re-experiencing. Thus, while there is a general need to validate PTSD screening tools against a clinical diagnostic interview, this is especially important and relevant within clinical samples of trauma-exposed chronic pain patients.
The recently published International Trauma Questionnaire (ITQ) assesses PTSD according to the 11th revision of the World Health Organization’s international Classification of Diseases (ICD-11; Cloitre et al., Citation2018; WHO, Citation2018). The revisions were made based on an intention to conceptualize PTSD more narrowly and ‘simplify the diagnosis and direct clinicians’ attention to its core elements’ (Maercker et al., Citation2013, p. 1684). The ICD-11 describes PTSD as being comprised of three symptom clusters (1) re-experiencing of the trauma in the here and now (Re), (2) avoidance of traumatic reminders (Av), and (3) a persistent sense of current threat that is manifested by startle reactions and hypervigilance (Th) (WHO, Citation2018). The ITQ assesses the ICD-11 PTSD core symptoms using six items with two items reflecting each of the three PTSD symptom clusters.
The ITQ was originally developed in English and formally published in 2018 (Cloitre et al., Citation2018). Numerous studies have already investigated the latent structure of the ICD-11 PTSD diagnosis across various trauma populations and languages (e.g. Bondjers et al., Citation2019; Brewin et al., Citation2017; Glück, Knefel, Tran, & Lueger-Schuster, Citation2016; Hansen, Hyland, Armour, Shevlin, & Elklit, Citation2015; Hansen et al., Citation2017; Ho et al., Citation2019; Karatzias et al., Citation2016; Kazlauskas, Gegieckaite, Hyland, Zelviene, & Cloitre, Citation2018; Rocha et al., Citation2019; Sele, Hoffart, Bækkenlund, & Øktedalen, Citation2020; Somma, Maffei, Borroni, Gialdi, & Fossati, Citation2019; Vallieres et al., Citation2018). Studies investigating the latent structure of the ITQ PTSD subscale using confirmatory factor analysis (CFA) have generally compared three models (i.e. a one-factor model, a two-factor model and the ICD-11 PTSD three-factor model, please see for specifications) and found support for the ICD-11 PTSD three factor model (e.g. Hansen et al., Citation2017; Karatzias et al., Citation2016). Although the ICD-11 model has been examined using the International Trauma Interview (ITI; Bondjers et al., Citation2019), no validation studies to date have included diagnostic interviews in the validation of the ITQ.
Table 1. ITQ item mapping for the three tested ICD-11 PTSD factor models
Chronic pain patients report multiple symptom comorbidities and multiple traumatic exposures, however, the most common cause for comorbid PTSD is traffic or injury-related trauma (Andersen, Andersen, & Andersen, Citation2014; Andersen, Andersen, Vakkala, & Elklit, Citation2012). Both chronic pain symptoms and PTSD symptoms are therefore common after traffic accidents and injuries and the conditions are shown to be mutually maintaining (Ravn, Hartvigsen, Hansen, Sterling, & Andersen, Citation2018). Thus, the present study aims to validate the ITQ in trauma-exposed chronic pain patients with a special focus on traffic and injury-related trauma. Although the Danish translation of the ITQ has been used in prior CFA studies supporting the ICD-11 three-factor latent structure of PTSD (Hansen et al., Citation2017), the present study is the first study seeking to validate the ITQ in Danish (or any other languages) using clinical rated diagnostic interviews. First, we aimed to validate the ITQ in a sample of trauma-exposed chronic pain patients with an index trauma related to traffic or work injuries using clinical rated diagnostic interviews (N = 40). Secondly, we aimed to validate the ITQ investigating construct validity using CFA in a full sample of mixed trauma-exposed chronic pain patients (N = 1.017) and in a subsample with exposure to traffic or work injuries only (n = 367). Thirdly, we aim to investigate concurrent and discriminant validity of the ITQ by testing its correlations with related constructs (i.e. depression, anxiety, another PTSD screening tool, and fear of movement (kinesiophobia) in the full sample of trauma-exposed chronic pain patients (N = 1.017). Based on prior research and theoretical assumptions it was hypothesized that the ITQ would present good diagnostic consistency and overall accuracy, the three-factor ICD-11 PTSD model would provide the best fit, and ITQ scores would correlate positively with depression, anxiety, and another measurement of PTSD symptoms, but correlate weakly with fear of movement as fear of movement is related to pain avoidance and not PTSD related avoidance.
2. Materials and method
2.1. Patients (participants)
Data for the present study were collected from patients referred to assessment and treatment at the public interdisciplinary University Hospital Pain Centre Odense Denmark. The Pain Centre is an outpatient tertiary care hospital setting treating patients with chronic (>6 months) non-cancer pain conditions. Most patients present with widespread or musculoskeletal pain and report moderate to severe pain intensity, high disability, and psychological distress. The data for the present study were collected between January 2017 and September 2019. After referral to the clinic and before the initial consultation at the clinic all referred patients were asked to fill out an electronic questionnaire (Clinical Pain Registry, PainData) sent via personal link to the patients’ official inbox, e-Boks (the channel that the Danish State and municipalities use to send official documents to citizens). All necessary ethical and legal approval according to Danish legislation were obtained.
A total of 2,625 participants completed the questionnaires and 1,206 participants (45.9%) reported exposure to a traumatic event with an indication of an index trauma and consented to participate in the present research. From the 1,206 participants 107 participant had indicated ‘other’ as potential traumatic event and due to the lack of clarity surround the specific nature of the index trauma these participants were removed from the sample leaving a sample size of 1,099 (31.2% males, M age = 49.9 years, SD = 13.94, range: 17–98). The most frequently reported index traumas were traffic or work-related accident (36.7%, n = 403), life-threatening illness (24.8%, n = 273), sudden accidental death (23.7%, n = 261), assault (10.0%, n = 110), violence (4.4%, n = 48), and disaster (0.4%, n = 4). Patients reporting an index trauma related to traffic or work injury were consecutively invited to participate in the diagnostic interview (n = 40).
2.2. Assessment of traumatic events and PTSD
Traumatic exposure was assessed using seven fixed trauma categories (i.e. natural disaster, accident (work or traffic), sexual assault, physical or mental violence, life-threatening illness, sudden accidental death, and other). These fixed categories were selected based on prior research, research experiences, and datasets indicating that they are the most common types of traumatic exposure previously identified in pain patients (Andersen et al., Citation2014, Citation2012).
2.2.1. International trauma questionnaire
The ICD-11 PTSD symptoms were assessed in relation to the most distressing event (i.e. the index trauma) using the International Trauma Questionnaire (ITQ) for PTSD symptoms (Cloitre et al., Citation2018). The ITQ is a brief self-report simple-worded measurement of probable PTSD and complex PTSD (CPTSD, Cloitre et al., Citation2018). The present study is a validation study on the ITQ PTSD symptom subscale only. The PTSD ITQ consists of six items with; two items assessing each of the three PTSD core symptom clusters (Re, Av, and Th). Participants are asked how much they have been bothered by each of the six PTSD symptom items on a five-point Likert-type scale ranging from not at all (0) to extremely (4). A probable PTSD diagnosis is met if the participants endorse at least one symptom in each symptom cluster (Re, Av, and Th); indicated by a score ≥2 (‘moderately’). In the present study, the internal reliability (Cronbach’s α) was .89. The ITQ is freely available and translated into several languages (https://www.traumameasuresglobal.com/itq) – see Appendix for the Danish ITQ.
2.2.2. Translation of ITQ
The ITQ was translated into Danish following international guidelines for translations of psychological tests (Hambleton, Merenda, & Spielberger, Citation2005; van Ommeren et al., Citation1999). This included independent back and forward translation, the committee approach, research expert group, focus group interviews, and approval of the backtranslation by two of the authors Marylene Cloitre and Chris Brewin.
2.2.3. Clinician-rated diagnostic interview
Currently, there does not exist a final validated diagnostic interview for ICD-11 PTSD and CPTSD. A clinical interview for ICD-11 PTSD and CPTSD, the International Trauma Interview (ITI), is currently under development (Roberts, Cloitre, Bisson, & Brewin, Citation2018), and one study has provided initial support regarding its validity in a Scandinavian sample (Bondjers et al., Citation2019). In the present study, ICD-11 PTSD was assessed by a clinical rated diagnostic interview with the four symptoms of Av and Th ICD-11 PTSD derived from the CAPS-5 (Weathers et al., Citation2013a) and two adjusted items for Re derived from the ITI test version 1.1. Participants are asked how much they have been bothered by each of the six PTSD symptom items on a five-point Likert-type scale (absent = 0, mild/subthreshold = 1, moderate/threshold = 2, severe/markedly elevated = 3, and extremely/incapacitating = 4). Of note, this means that although the ITI is still under development, the procedure and content used in the present study is highly identical with the ITI PTSD part validated in a Scandinavian sample and the latest versions of the ITI (Bondjers et al., Citation2019; Roberts et al., Citation2018). Following established guidelines (Roberts et al., Citation2018), an ICD-11 PTSD diagnosis was determined to be present when the participants endorse at least one symptom of Re, Av, and Th with a score ≥2.
The diagnostic interview was administered by doctoral-level psychology graduate students, who received initial training from the authors, and who participated in regular supervision. The ITQ was administrated first followed by the diagnostic interview the same day to ensure that both instruments referenced to the same time period and index trauma. The interviewers were blinded to the participants’ scores on the ITQ.
2.3. Measures to assess concurrent and discriminant validity
The following measurements were used in Danish to investigate concurrent and discriminant validity of the ITQ.
The total score for the Generalized Anxiety Disorder-7 scale was used as an indicator of anxiety (GAD-7: Spitzer, Kroenke, Williams, & Löwe, Citation2006). The scale is a seven items self-report questionnaire on which patients report the presence of general anxiety symptoms on a scale from 0 to 3 (0 = not at all to 3 = nearly every day). The GAD-7 is found to be a valid and reliable measurement across both general and psychiatric settings (Hinz et al., Citation2017; Rutter & Brown, Citation2017). In the present study, the internal reliability (Cronbach’s α) was .89 for the GAD-7 total score.
Symptoms of depression were assessed using the Patient Health Questionnaire (PHQ-9: Kroenke & Spitzer, Citation2002). The scale is a nine items self-report questionnaire on which patients report the presence of depressive symptoms on a scale from 0 to 3 (0 = not at all to 3 = nearly every day). The scale has been used in both epidemiological studies as well as in clinical populations (Kroenke, Spitzer, Williams, & Löwe, Citation2010). In the present study, the internal reliability (Cronbach’s α) was .82 for the PHQ-9 total score.
The PCL-5 was used as an alternative assessment of PTSD severity (Weathers et al., Citation2013b). The PCL-5 consists of 20 items measuring the four DSM-5 symptom clusters (American Psychiatric Association, Citation2013) rated on a five-point Likert-type scale identical to the ITQ. Although the PCL-5 is developed based on a different diagnostic system, the two descriptions of PTSD are expected to be positively related as they describe responses to traumatic events. The three identical items of the PCL-5 and the ITQ were removed (external avoidance, hypervigilance, and startle), and only the remaining 17 items were used in the present study. We included analyses with all 17 PCL-5 items for a general assessment of posttraumatic stress responses and for more direct comparability with the ICD-11 PTSD configuration, we also included analyses excluding the seven PCL-5 items assessing the fourth DSM-5 PTSD symptom cluster of negative alternations in cognitions and mood. Overall, the PCL-5 has shown acceptable validity and reliability (Bovin et al., Citation2016). In the present study, the internal reliability (Cronbach’s α) was .94 for the total score.
Fear of re-injury due to movement was measured with the Tampa Scale for Kinesiophobia (TSK: Kori, Miller, & Todd, Citation1990). The scale was used to test whether the ITQ captures PTSD related avoidance and not pain-related avoidance (i.e. fear of movement as measured by the TSK). For this reason, the TSK was expected to correlate positively but only weakly with the ITQ. The TSK is a 17-item self-report scale on which patients are asked to report their level of agreement with each item on a four-point Likert-type scale (1 = strongly disagree, 4 = strongly agree) with higher scores indicating higher levels of kinesiophobia. The scale is commonly used in diverse chronic pain samples and has good construct and predictive validity (Roelofs, Goubert, Peters, Vlaeyen, & Crombez, Citation2004). In the present study, the internal reliability (Cronbach’s α) was .86 for the TSK total score.
2.4. Statistical analyses
The analytical strategy for the present study included several steps. First, the diagnostic accuracy of the ITQ was assessed at different cut-off criteria by receiver operator characteristics (ROC) analysis in the subsample of patients with diagnostic interviews (N = 40). There were no missing data. The clinical rated diagnostic interview was used as the gold standard against which the ITQ was assessed. An area under the curve score ≥ .80 was considered satisfactory (Zhu, Zeng, & Wang, Citation2010). The optimal balance between sensitivity and specificity was calculated by Youden’s J ((J = (sensitivity + specificity) – 1). The optimal cut-off value is when J reaches its maximum. However, the balance between correct positives and false positives were also taken into consideration in deciding on an optimal cut-off. The sample size was calculated a priori by the software tool ‘easyROC’ with an expected AUC at .80 and an allocation ratio of 6. The allocation rate was a conservative estimate based on previous prevalence studies in pain centres (Andersen et al., Citation2014). A sample of 42 participants was calculated to be sufficient to obtain statistical power at the recommended .80 level. In the present study, the AUC was .90 and thus the statistical power was satisfactory with the 40 participants included in the present study.
The prevalence of PTSD for different cut-off values on the ITQ was assessed in terms of false positives and negatives, true positives and negatives, sensitivity, specificity, positive predictive value, negative predictive value, and overall performance at the different cut-off criteria. The diagnostic consistency across the ICD-11 PTSD interview and the ITQ was estimated using Cohen’s Kappa statistic where a value greater than .80 indicating almost perfect agreement, .61-.80, indicates substantial agreement, .41–.60 moderate, .21–.40, and fair; ≤.20 slight/poor (Landis & Koch, Citation1977).
Second, the construct validity of the ITQ was investigated using CFA tested in Mplus 7.4 (Muthén & Muthén, Citation2013) using the mean and variance adjusted weighted least squares (WLSMV estimator), which provides more accurate standard errors for ordinal level indicators (Flora & Curran, Citation2004). Three different competing models of the ICD-11 PTSD symptoms operationalized as six symptoms in the ITQ (see ) were estimated using CFA across the two samples (i.e. the full sample of mixed traumatic exposure and the subsample of victims of traffic and work-related injury). The three models were a one-factor model (Forbes et al., Citation2015), a two-factor model (i.e. Re-Av and Th, Forbes et al., Citation2015), and the ICD-11 PTSD three-factor model (WHO, Citation2018). Model fit were assessed using traditional approaches: Good model fit was indicated by a non-significant chi-square result; Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) values greater than .90 indicate adequate fit and values greater than .95 indicate excellent fit. Furthermore, Root-Mean-Square Error of Approximation (RMSEA) values ≤ .08 indicated acceptable fit and values ≤ .05 indicate excellent fit. Changes in the RMSEA results were used to compare alternative models as the RMSEA index includes penalty for model complexity, and changes ≥.015 indicate significant changes in the respective models (Chen, Curran, Bollen, Kirby, & Paxton, Citation2008). Missing data were handled in the following way for the CFA analyses. Only participants with complete information on the ITQ were used leaving the following final sample sizes for the analyses at 1,017 participants (92.5%) in the full sample and the 367 participants (91.1%) in the accident and injury subsample.
Third, concurrent and discriminant validity were tested using a series of Spearman’s rho correlation analyses in the full mixed sample only. Missing data were handled in the following way for the analyses of concurrent and discriminant validity. In the full eligible sample of 1,099 participants, a total of 67 (6.1%) had more than 20% missing data on the selected combination of variables and were excluded from the analyses and leaving an eligible sample size of 1,032. Afterwards, there were only a few missing data (0.0– 6.7%), which were missing completely at random (Little’s MCAR test Chi2(9493) = 9,671.71, p = .098). Of note, due to changes in the data-collection the PCL-5 was not collected in the full sample, but it was only collected across 767 participants (69.7% of the 1,099 participants with an index trauma). From the 767 a total of 16 participants had more than 20% missing data and were therefore excluded from the analyses leaving an eligible sample size of 751. Afterwards, there were only a few missing data (0.9–4.8%), which were also missing completely at random (Little’s MCAR test Chi2(9741) = 9,850.70, p = .215).
3. Results
3.1. Clinician-rated diagnostic interviews
In total 40 patients participated in the diagnostic interview (52.5% males, M age = 44.55 years, SD = 10.90, range: 22–63). According to the diagnostic interview, 17.5% of the patients (n = 7) met the ICD-11 diagnostic criteria for PTSD and according to the established cluster cut-off criteria on the ITQ 20% of the patients (n = 8) qualified for possible PTSD. The performance of the ITQ compared to the diagnostic interview and the estimated prevalence of PTSD based on the different ITQ cut-off criteria is presented in . The prevalence rates ranged from 12.5% (cut-off score 18) to 50% (cut-off score 6).
Table 2. Prevalence of PTSD for different cut-off values
Table 3. Sensitivity, specificity, positive predictive value and negative predictive value for different cut-off values
The diagnostic consistency across the ICD-11 PTSD interview and the ITQ was κ = .59 indicating substantial agreement (κ ranged from .37 to 61 for the different cut-off scores in ). Furthermore, as illustrated by showing the ROC curve of the ITQ validated against the diagnostic interview, a satisfactory overall accuracy of the ITQ was found AUC = .90.
Figure 1. Receiving operator characteristics curve for ITQ relative to ICD-11 interview
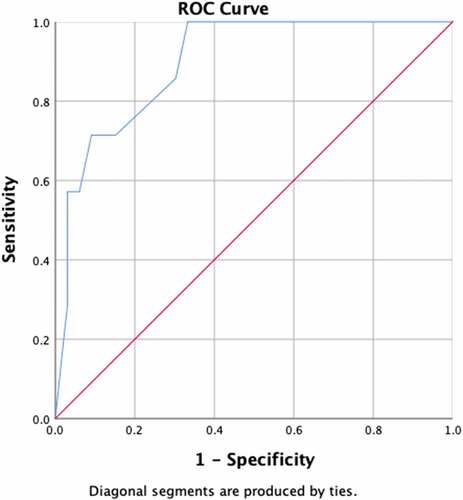
Youden’s J was highest at a cut-off of seven followed by the ITQ cluster criteria or a cut-off of 13 on the ITQ. However, the cut-off of seven produced too many false positives and thus the ITQ algorithm using cluster criteria or the cut-off of 13 is considered optimal. Both of these cut-off criteria estimated the PTSD prevalence rate to be 20%, which is close to the ‘true prevalence’ (estimated prevalence from the clinical interview) of 17.5%. Using these cut-off criteria, the negative likelihood ratio was 3.14 (the likelihood that a negative result is to be found in a person without, as opposed to with the diagnosis). The positive likelihood ratio was 7.89 (the likelihood that a positive result is to be found in a person with the diagnosis, as opposed to without the diagnosis).
3.2. Estimated PTSD prevalence rate and construct validity
The estimated PTSD prevalence rate according to the ITQ in the full sample was 17.4% (N = 180) and 12.9% in the accident subsample (N = 48). Results of the CFA are presented in . shows the model fit statistics of the three tested models of the ITQ PTSD subscale across the subsample of victims of accidents and the full sample. All models provided excellent or close to excellent fit of the data with the changes in RMSEA ≥.015 indicating that the three-factor models provided a significantly better fit than the remaining models across both samples. Of note, the chi-square statistics was statistically significant for all models in the large overall sample (N = 1,017), however, this should not lead to model rejection as the chi-square test is affected by large sample size (Tanaka, Citation1987). The standardized factor loadings for all the factors across the 2 three-factor models were all positive and strong ranging between .80-.94 (p < .001). Factor correlations were also all positive and strong ranging from .78-.95 (p < .001).
Table 4. Model fit statistics for the alternative models of ITQ ICD-11 PTSD symptoms in the accident sample and the mixed remaining sample
3.3. Concurrent and discriminant validity
The descriptive statistics of the measurements in the full samples were the following: the ITQ PTSD total score (M= 5.87, SD = 6.00, range = 0–24), the total scores of PCL-5 (M = 23.51, SD = 17.94, range = 0–80), the GAD7 (M= 6.17, SD = 5.03 range = 0–21), the PHQ-9 (M= 10.43, SD = 5.66, range = 0–27), and the TSK (M= 40.74, SD = 7.79, range = 19–66). The ITQ total score correlated strongly and positively with the 17 PCL-5 items (Spearman’s rho = .84 p < .001) and the 10 PCL-5 items (excluding the seven items assessing the DSM-5 PTSD symptom cluster of negative alternations in cognition and mood) (Spearman’s rho = .84 p < .001), and the GAD-7 (Spearman´s rho = .53 p < .001) and moderately and positively with the PHQ-9 (Spearman’s rho = .41 p < .001). Finally, the ITQ total correlated positively and weakly with the TSK (Spearman’s rho = .22 p < .001).
4. Discussion
The present study is the first to validate and examine the diagnostic accuracy of the ITQ PTSD subscale using a clinician-rated diagnostic interview. The validation of the ITQ PTSD subscale was based on trauma-exposed clinical chronic pain patients, which is a particularly important trauma population to validate PTSD screening tools within due to the overlap between symptoms of PTSD and pain. The overall findings suggest that the diagnostic consistency between the ITQ and the clinician-rated interview (κ = .59) as well as the overall accuracy of the scale (AUC = .90) were good. Furthermore, the Danish ITQ has shown excellent construct validity in both the full sample and the subsample of traffic and work-related accidents as well as excellent concurrent and discriminant validity in the full sample.
The optimal balance between sensitivity and specificity was found using the cluster criteria algorithm or a cut-off score of 13 on the ITQ. Applying the cut-off score of 13 and the ITQ algorithm also resulted in similar prevalence rates of PTSD between the ITQ (20%) and the diagnostic interview (17.5%). This finding is satisfactory since previous pain studies have tended to show self-report questionnaires to be over-inclusive (Siqveland et al., Citation2017). In particularly comorbid PTSD and pain poses a challenge, since several symptoms are potentially overlapping or being shared (for instance, sleep problems, and avoidance behaviours). Thus, self-report questionnaires can potentially result in false positives (i.e. over-diagnosing PTSD) or false negatives (i.e. under-diagnosing PTSD). Both are problematic, since the purpose of screening is to identify those in need of a targeted intervention for PTSD.
The CFA findings indicated that the three-factor model in accordance with the diagnostic criteria best represented the latent structure of the Danish ITQ PTSD subscale as indicated by overall best model fit statistics including reductions of RMSEA of at least .015 across both samples. Similar results were found in prior studies using the Danish ITQ, which may indicate that the results of the Danish ITQ can generalize across different trauma populations (Hansen et al., Citation2017). At the same time, consistent with previous studies on the ITQ or other measurements of ICD-11 PTSD the ICD-11 three-factor model as well as the additional proposed two factor-model also showed acceptable and even excellent fit (e.g. Forbes et al., Citation2015; Hansen et al., Citation2017). Furthermore, the concurrent and discriminant validity analyses indicate that the ITQ performs satisfactorily. Indeed, the ITQ PTSD total score correlated moderately to strongly with symptoms of anxiety and depression as in previous research (e.g. Andersen et al., Citation2018; Ho et al., Citation2019) and symptoms of PTSD assessed by another PTSD measurement. At the same time, the correlation between the ITQ total score and fear of movement was weak (kinesiophobia), which indicates that avoidance associated with pain is not related with the avoidance associated with PTSD measured by the ITQ and thus does not result in false positives (i.e. over-diagnosing). Of note, discriminant and concurrent validity were further supported by the finding that the correlation between the ITQ PTSD total score and the other PTSD measurement (i.e. the PCL-5, Spearman’s rho = .84) were stronger than the correlations between the ITQ PTSD total score and symptoms of anxiety and depression (i.e. the GAD-7 and the PHQ-9, Spearman’s rho = .53 and .41, respectively).
The results of the study have several implications for clinical practice. Combined the results of the present study support the ITQ and suggest that the ITQ is a potentially valuable screening tool in the context of pain rehabilitation, where brief and up to date population-specific validated screening tools are needed not to overburden the patients. Furthermore, the results indicate that the use of a cut-off score of 13 and the ITQ scoring algorithm may result in the same estimation of PTSD. However, as it is in theory possible to meet the cut-off score of 13 on the ITQ without meeting the diagnostic criteria for each symptom cluster (i.e. obtaining a total score of ≥13 based on items belonging solely to two symptom clusters and scoring zero on the third remaining symptom cluster), we recommend the use of the ITQ scoring algorithm and not the cut-off scores. This is also in accordance with the original scoring key of the ITQ. In general, the ITQ has shown excellent psychometric properties across a wide range of trauma populations and languages (e.g. Hansen et al., Citation2017; Ho et al., Citation2019; Karatzias et al., Citation2016; Kazlauskas et al., Citation2018; Rocha et al., Citation2019; Sele et al., Citation2020; Somma et al., Citation2019). However, as the present study is the first study to validate the ITQ using diagnostic interviews and thus assess the optimal diagnostic threshold, future studies are needed to replicate the results following a wider range of traumatic exposure including more complex traumas.
Although the results of the present study are promising, several limitations need to be considered. First, although our clinical rated interview is highly similar to the latest version of the ITI, further validation is needed of the ITQ using the final version of the ITI. Secondly, the sample for the present study was a clinical sample of trauma-exposed chronic pain patients with a mean age of nearly 50 years, which is expected within this context and population. Although the construct validity has also been established in other Danish trauma populations of younger ages, cross-validation of our results across a wider range of populations would be beneficial. This includes distinguishing between traumatic exposure in childhood and adulthood, which was not possible in the present study. In addition, future studies are needed to validate the ITQ using diagnostic interviews following complex traumas and thus also validate the ITQ CPTSD subscale using diagnostic interviews. Thirdly, due to the nature of the sample (i.e. being a treatment-seeking chronic pain sample), it was not possible to assess functional impairment as all participants were severely disabled or functionally limited by their comorbid pain making it difficult to separate it from functional impairment solely associated with PTSD. Fourthly, although sufficient statistical power was achieved in the present study for calculating diagnostic accuracy, the sample size was still modest. Future studies should therefore include larger sample sizes to further strengthen the results.
Despite its limitations the present study has provided the first validation of the ITQ using a diagnostic interview in a trauma-exposed clinical chronic pain sample. In general, it is important that PTSD screening tools are validated against a clinical diagnostic interview to ensure diagnostic precision. This is especially evident within trauma-exposed chronic pain patients due to the high potential risk of inclusion of false positives caused by elevated distress related to pain such as depressive symptoms or fear-avoidance behaviours. This could potentially lead to the risk of concluding that comorbid PTSD does not have an impact on the effect of pain rehabilitation, since rehabilitation reduces general distress. Hence, a valid screening tool in the context of chronic pain rehabilitation is important and very much needed. The ITQ has proven valid in terms of identifying patients with clinical rated diagnosis of PTSD as indicated by its overall performance. At the same time, the present study is also the first study seeking to explicitly validate the ITQ in Danish. In conclusion, the overall findings suggest that the diagnostic consistency between the clinical rated diagnostic interview and the ITQ as well as the overall accuracy of the scale were good. Furthermore, the Danish ITQ has excellent construct validity as well as concurrent and discriminant validity.
Ethics statement
Institutional review board approval information: As treatment was not affected by participation in the study, under Danish law, this study did not need ethics approval (Act on Research Ethics Review of Health Research Projects, October 2013, Section 14.2) (REF: Danish National Committee on Biomedical Research Ethics. Act on research ethics review of health research projects. 2000. Available at: www.cvk.sum.dk/English/actonabiomedicalresearch.aspx).
Informed consent: Written informed consent (electronic signature) was obtained from all patients included in this study.
Acknowledgments
The authors would like to thank all the participants for participating and The Council of The Danish Victims’ Fund (Offerfonden) for funding research into PTSD in pain patients. The authors would also like to thank Chris Brewin for his advice and recommendation to capture ICD-11 PTSD.
Data availability statement
The data used in the present study cannot be shared due to the EU general Data Protection Regulation.
Disclosure statement
MC was part of the WHO ICD-11 PTSD workgroup and one of the original authors of the International Trauma Questionnaire.
Additional information
Funding
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
- Andersen, T. E., Andersen, L.-A. C., & Andersen, P. G. (2014). Chronic pain patients with possible co-morbid post-traumatic stress disorder admitted to multidisciplinary pain rehabilitation – A 1-year cohort study. European Journal of Psychotraumatology, 5(1), 23235. doi:10.3402/ejpt.v5.23235
- Andersen, T. E., Andersen, P. G., Vakkala, M. A., & Elklit, A. (2012). The traumatized chronic pain patient—Prevalence of posttraumatic stress disorder - PTSD and pain sensitization in two Scandinavian samples referred for pain rehabilitation. Scandinavian Journal of Pain, 3(1), 39–13. doi:10.1016/j.sjpain.2011.10.001
- Andersen, T. E., Hansen, M., Ravn, S. L., Seehuus, R., Nielsen, M., & Vaegter, H. B. (2018). Validation of the PTSD-8 scale in chronic pain patients. Pain Medicine, 19(7), 1365–1372.
- Bondjers, K., Hyland, P., Roberts, N. P., Bisson, J. I., Willebrand, M., & Arnberg, F. K. (2019). Validation of a clinician-administered diagnostic measure of ICD-11 PTSD and Complex PTSD: The International Trauma Interview in a Swedish sample. European Journal of Psychotraumatology, 10(1), 1665617.
- Bovin, M. J., Marx, B. P., Weathers, F. W., Gallagher, M. W., Rodriguez, P., Schnurr, P. P., & Keane, T. M. (2016). Psychometric properties of the PTSD checklist for diagnostic and statistical manual of mental disorders–Fifth Edition (PCL-5) in Veterans. Psychological Assessment, 28(11), 1379–1391. doi:10.1037/pas0000254
- Brewin, C. R., Cloitre, M., Hyland, P., Shevlin, M., Maercker, A., Bryant, R. A., & Reed, G. M. (2017). A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clinical Psychology Review, 58, 1–15.
- Chen, F., Curran, P. J., Bollen, K. A., Kirby, J., & Paxton, P. (2008). An empirical evaluation of the use of fixed cutoff points in RMSEA test statistic in structural equation models. Sociological Methods & Research, 36(4), 462–494.
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Robert, N. P., Maercker, A., & Hyland, P. (2018). The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546. doi:10.1111/acps.12956
- Flora, D. B., & Curran, P. J. (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9(4), 466.
- Forbes, D., Lockwood, E., Creamer, M., Bryant, R. A., McFarlane, A. C., Silove, D., & O’Donnell, M. (2015). Latent structure of the proposed ICD-11 post-traumatic stress disorder symptoms: Implications for the diagnostic algorithm. British Journal of Clinical Psychiatry, 206(3), 1–7. doi:10.1192/bjp.bp.114.150078
- Glück, T. M., Knefel, M., Tran, U. S., & Lueger-Schuster, B. (2016). PTSD in ICD-10 and proposed ICD-11 in elderly with childhood trauma: Prevalence, factor structure, and symptom profiles. European Journal of Psychotraumatology, 7(1), 1–9.
- Hambleton, R. K., Merenda, P. F., & Spielberger, C. (2005). Adapting educational and psychological tests for cross-cultural assessment. Mahwah, NJ: Lawrence Erlbaum Associates. ISBN: 1410611752.
- Hansen, M., Hyland, P., Armour, C., Shevlin, M., & Elklit, A. (2015). Less is more? Assessing the validity of the ICD-11 model of PTSD across multiple trauma samples. European Journal of Psychotraumatology, 6(1), 1–11. doi:10.3402/ejpt.v6.28766
- Hansen, M., Hyland, P., Karstoft, K.-I., Vaegter, H. B., Bramsen, R. H., Nielsen, A. B. S., … Andersen, T. E. (2017). Does size really matter? A multisite study assessing the latent structure of the proposed ICD-11 and DSM-5 diagnostic criteria for PTSD. European Journal of Psychotraumatology, 8(2), 1398002. doi:10.1080/20008198.2017.1398002
- Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., & Hilbert, A. (2017). Psychometric evaluation of the generalized anxiety disorder screener GAD-7, based on a large German general population sample. . Journal of Affective Disorders, 210, 338–344. doi:10.1016/j.jad.2016.12.012
- Ho, G., Karatzias, T., Cloitre, M., Chan, A. C. Y., Bressington, D., Chien, W. T., … Shevlin, M. (2019). Translation and validation of the Chinese ICD-11 International Trauma Questionnaire (ITQ) for the Assessment of Posttraumatic Stress Disorder (PTSD) and Complex PTSD (CPTSD). European Journal of Psychotraumatology, 10(1), 1608718. doi:10.1080/20008198.2019.1608718
- Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D., … Cloitre, M. (2016). An initial psychometric assessment of an ICD-11 based measure of PTSD and complex PTSD (ICD-TQ): Evidence of construct validity. Journal of Anxiety Disorders, 44, 73–79. doi:10.1016/j.janxdis.2016.10.009
- Kazlauskas, E., Gegieckaite, G., Hyland, P., Zelviene, P., & Cloitre, M. (2018). The structure of ICD-11 PTSD and complex PTSD in Lithuanian mental health services. European Journal of Psychotraumatology, 9(1), 1414559. doi:10.1080/20008198.2017.1414559
- Kori, H. S., Miller, R. P., & Todd, D. D. (1990). Kinesiophobia: A new view of chronic pain behavior. Pain Management, 3, 35–43.
- Kroenke, K., & Spitzer, R. L. (2002). The PHQ-9: A new depression diagnostic and severity measure. Psychiatric Annals, 32(9), 509–515. doi:10.3928/0048-5713-20020901-06
- Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2010). The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. General Hospital Psychiatry, 32(4), 345–359.
- Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), 159–174.
- Maercker, A., Brewin, C. R., Bryant, R. A., Cloitre, M., Reed, G. M., van Ommeren, M., … Saxena, S. (2013). Proposals for mental disorders specifically associated with stress in the International Classification of Diseases-11. Lancet, 381(9878), 1683–1685. doi:10.1016/S0140-6736
- Muthén, L. K., & Muthén, B. O. (2013). Mplus user’s guide (7th ed.). Los Angeles: Muthén.
- Ravn, S. L., Hartvigsen, J., Hansen, M., Sterling, M., & Andersen, T. E. (2018). Do post-traumatic pain and post-traumatic stress symptomatology mutually maintain each other? A systematic review of cross-lagged studies. Pain, 159(11), 2159–2169. doi:10.1097/j.pain.0000000000001331
- Roberts, N., Cloitre, M., Bisson, J. I., & Brewin, C. (2018). PTSD & complex PTSD diagnostic interview schedule for ICD-11 (unpublished interview).
- Rocha, J., Rodrigues, V., Santos, E., Azevedo, I., Machado, S., Almeida, V., … Cloitre, M. (2019). The first instrument for complex PTSD assessment: Psychometric properties of the ICD-11 Trauma Questionnaire. Brazilian Journal of Psychiatry, 42(2), 185–189. doi:10.1590/1516-4446-2018-0272
- Roelofs, J., Goubert, L., Peters, M. L., Vlaeyen, J. W. S., & Crombez, G. (2004). The Tampa scale for kinesiophobia: Further examination of psychometric properties in patients with chronic low back pain and fibromyalgia. European Journal of Pain, 8(5), 495–502.
- Rutter, L. A., & Brown, T. A. (2017). Psychometric properties of the generalized anxiety disorder scale-7 (GAD-7) in outpatients with anxiety and mood disorders. Journal of Psychopathology and Behavioral Assessment, 39(1), 140–146. doi:10.1007/s10862-016-9571-9
- Sele, P., Hoffart, A., Bækkenlund, H., & Øktedalen, T. (2020). Psychometric properties of the International Trauma Questionnaire (ITQ) examined in a Norwegian trauma-exposed clinical sample. European Journal of Psychotraumatology, 11(1), 1796187. doi:10.1080/20008198.2020.1796187
- Siqveland, J., Hussain, A., Lindstrøm, J. C., Ruud, T., & Hauff, E. (2017). Prevalence of posttraumatic stress disorder in persons with chronic pain: A meta-analysis. Frontiers in Psychiatry, 8, 164. doi:10.3389/fpsyt.2017.00164
- Somma, A., Maffei, C., Borroni, S., Gialdi, G., & Fossati, A. (2019). Post traumatic reactions as individual differences: Latent structure analysis of the International Trauma Questionnaire in Italian trauma-exposed ad non-trauma exposed adults. Mediterranean Journal of Clinical Psychology, 7. doi:10.6092/2282-1619/2019.7.2058
- Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder the GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. doi:10.1001/archinte.166.10.1092
- Tanaka, J. S. (1987). How big is big enough?”: Sample size and goodness of fit in structural equation models with latent variables. Child Development, 58(1), 134–146.
- Vallieres, F., Ceannt, R., Daccache, F., Daher, A., Sleiman, J., Gilmore, B., … Hyland, P. (2018). ICD-11 PTSD and complex PTSD amongst Syruan refugees in Lebanon: The factor structure and the clinical utility of the International Trauma Questionnaire. Acta Psychiatrica Scandinavica, 138(6), 547–557. doi:10.11111/acps.12973
- van Ommeren, M., Sharma, B., Thapa, S., Makaju, R., Prasain, D., & de Jong, J. (1999). Preparing instruments for transcultural research: Use of the translation monitoring form with Nepali-speaking Bhutanese refugees. Transcultural Psychiatry, 36(3), 285–301.
- Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., & Keane, T. M. (2013a). The clinician-administered PTSD scale for DSM-5 (CAPS-5). Retrieved from Interview available from the National Center for PTSD: www.ptsd.va.gov
- Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013b). The PTSD Checklist for DSM-5 (PCL-5). Retrieved from Scale available from the National Center for PTSD: www.ptsd.va.gov
- World Health Organization. (2018, December). ICD-11 for mortality and morbidity statistics [Diagnostic Criteria for post-traumatic stress disorder]. Retrieved from https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f2070699808
- Zhu, W., Zeng, N., & Wang, N. (2010). Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS. Implementations. NESUG Health Care and Life Sciences, 67, 1–9.
Appendix.
The Danish International Trauma Questionnaire (ITQ)
OVERSIGT:
Det vedhæftede spørgeskema er et kort, simpelt formuleret måleredskab, som udelukkende fokuserer på kerneelementerne i posttraumatisk stress forstyrrelse (PTSD) og kompleks PTSD (KPTSD) og som anvender ukomplicerede diagnostiske regler. ITQ blev udviklet til at være i overensstemmelse med de organiserende principper for ICD-11 fastlagt af Verdenssundhedsorganisationen (World Health Organization, WHO), som skal maksimere klinisk relevans og sikre international anvendelighed gennem fokus på kernesymptomerne af en given lidelse. ITQ er offentligt frit tilgængelig for alle interesserede. Evaluering af spørgeskemaet er ikke afsluttet og fortsætter især i forhold til definitionen af funktionsnedsættelse for både PTSD og KPTSD samt muligvis indholdet i spørgsmålene, eftersom de kan være prædiktive for forskellige behandlingsudfald.
DE DIAGNOSTISKE ALGORITMER er følgende:
PTSD. En PTSD-diagnose kræver tilstedeværelsen af et af to symptomer fra symptomklyngerne: (1) genoplevelse her og nu, (2) undgåelse, og (3) fornemmelse/oplevelse af aktuel trussel (sense of current threat), samt tilstedeværelsen af mindst en indikator for funktionsnedsættelse forbundet med disse symptomer. Tilstedeværelsen af et symptom eller et funktionsnedsættelsesspørgsmål er defineret som en score ≥ 2.
KPTSD. En KPTSD-diagnose kræver tilstedeværelsen af et af to symptomer fra hver af de tre PTSD symptomklynger (genoplevelse her og nu, undgåelse og fornemmelse/oplevelse af aktuel trussel (sense of current threat) og et af to af symptomer fra hver af de tre forstyrrelser i selvorganisering (DSO) klynger: (1) affektiv dysregulering, (2) negativt selvbillede, og (3) forstyrrelser i relationer til andre. Funktionsnedsættelse skal identificeres med tilstedeværelsen af mindst en indikator for funktionsnedsættelse relateret til PTSD-symptomerne og tilstedeværelsen af en indikator for funktionsnedsættelse relateret til DSO-symptomerne. Tilstedeværelsen af et symptom eller funktionsnedsættelsesspørgsmål er defineret som en score ≥2
Et individ kan møde kriterierne for enten en PTSD-diagnose eller en KPTSD-diagnose ikke begge. Hvis en person møder kriterierne for KPTSD, får denne person ikke også en PTSD-diagnose.
Scoringsinstruktionerne er tilgængelige i slutningen af dette dokument.
REFERENCER for den engelske version er:
Cloitre, M., Shevlin M., Brewin, C.R., Bisson, J.I., Roberts, N.P., Maercker, A., Karatzias, T., Hyland, P. (2018). The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and Complex PTSD. Acta Psychiatrica Scandinavica. DOI: 10.1111/acps.12956
Referencen for denne validerede danske oversættelse:
Hansen, M., Vægter, H. B., Cloitre, M., & Andersen, T. E. (2021). Validation of the Danish International Trauma Questionnaire for posttraumatic stress disorder in chronic patients pain. European Journal of Psychotraumatology.
BAGGRUNDSARTIKLER:
Brewin, C. R., Cloitre, M., Hyland, P., Shevlin, M., Maercker, A., Bryant, R. A., … Reed, G. M. (2017). A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clinical Psychology Review, 58, 1–15. doi: 10.1016/j.cpr.2017.09.001.
Karatzias T., Shevlin M., Fyvie C., Hyland P., Efthymiadou E., Wilson D., … Cloitre M. (2017). Evidence of distinct profiles of posttraumatic stress disorder (PTSD) and complex posttraumatic stress disorder (CPTSD) based on the new ICD-11 trauma questionnaire (ICD-TQ). Journal of Affective Disorders, 207, 181–187. http://dx.doi.org/10.1016/j.jad.2016.09.032
Hyland, P., Shevlin M., Brewin C.R., Cloitre M., Downes A.J., Jumbe, S., … Roberts, N.P. (2017). Validation of post‐ traumatic stress disorder (PTSD) and complex PTSD using the International Trauma Questionnaire. Acta Psychiatrica Scandinavica. 136, 313–322. doi: 10.1111/acps.12771.
Hansen, M., Hyland, P., Karstoft, K-I., Vaegter, H. B., Bramsen, R. H., Nielsen, A. B. S., Armour, C., Andersen, S. B., Høybye, M. T., Larsen, S. K., & Andersen, T. E. (2017). Does size really matter? A multisite study assessing the latent structure of the proposed ICD-11 and DSM-5 diagnostic criteria for PTSD. European Journal of Psychotraumatology. doi:10.1080/20008198.2017.1398002
Shevlin, M., Hyland, P., Roberts, N. P., Bisson, J. I., Brewin C.R. & Cloitre M. (2018). A psychometric assessment of Disturbances in Self-Organization symptom indicators for ICD-11 Complex PTSD using the International Trauma Questionnaire, European Journal of Psychotraumatology, 9:1, DOI: 10.1080/20008198.2017.1419749
International Trauma Questionnaire
Instruktioner: Angiv venligst den begivenhed, som generer dig mest og besvar de efterfølgende spørgsmål ud fra denne begivenhed.
Kort beskrivelse af begivenheden_____________________
Hvornår skete begivenheden? (Sæt cirkel om én)
Mindre end 6 måneder siden
6–12 måneder siden
1–5 år siden
5–10 år siden
10–20 år siden
Mere end 20 år siden
Nedenfor er der en liste med problemer, som mennesker kan have som reaktion på traumatiske eller stressende livsbegivenheder. Læs venligst hvert spørgsmål omhyggeligt og sæt derefter en cirkel om dét tal til højre, der bedst beskriver, hvor meget du har været generet af det problem indenfor den sidste måned.
Nedenfor er der en liste med problemer, som mennesker, der har været udsat for stressende eller traumatiske oplevelser sommetider oplever. Spørgsmålene refererer til, hvordan du typisk har det, hvordan du typisk tænker om dig selv, og hvordan du typisk relaterer dig til andre mennesker. Besvar følgende ud fra, hvor sand hver enkelt påstand er for dig.
1. Diagnostisk scoring for PTSD og KPTSD
PTSD
Hvis P1 eller P2 ≥ 2 er kriteriet for Genoplevelse her og nu (Re_dx) opfyldt
Hvis P3 or P4 ≥ 2 er kriteriet for Undgåelse (Av_dx) opfyldt
Hvis P5 or P6 ≥ 2 er kriteriet for Fornemmelse/Oplevelse af aktuel trussel (Sense of current threat) (Th_dx) opfyldt
OG
Hvis mindst et af P7, P8, eller P9 ≥ 2 er kriteriet for funktionsnedsættelse mødt (PTSDFI)
Hvis kriterierne for ‘Re_dx’ OG ‘Av_dx’ OG ‘Th_dx’ OG ‘PTSDFI’ er mødt, er kriterierne for PTSD mødt.
CPTSD
Hvis C1 or C2 ≥ 2 er kriteriet for Affektiv Dysregulering (AD_dx) opfyldt
Hvis C3 or C4 > ≥ 2 er kriteriet for Negativt selvbillede (NSC_dx) opfyldt
Hvis C5 or C6 ≥ 2 er kriteriet for Forstyrrelser i relationer til andre (DR_dx) opfyldt
OG
Hvis mindst et af C7, C8, eller C9 ≥ 2 mødes DSO kriteriet for funktionsnedsættelse (DSOFI).
Hvis kriteriet for ‘AD_dx’ OG ‘NSC_dx’ OG ‘DR_dx’, OG ‘DSOFI’ er opfyldte, er kriterierne for DSO opfyldt.
PTSD diagnosticeres, hvis kriterierne for PTSD er opfyldt men IKKE for DSO.
KPTSD diagnosticeres, hvis kriterierne for PTSD er opfyldt OG kriterierne for DSO.
Hvis kriterierne for PTSD ikke er opfyldt eller det udelukkende er kriterierne for DSO, som opfyldes, stilles ingen diagnose.
2. Dimensional scoring for PTSD og KPTSD.
Der kan beregnes scores for hver PTSD og DSO symptomklynge, som kan lægges sammen til PTSD og DSO total scores.
PTSD
Summen af P1 og P2 = Genoplevelse her og nu (Re)
Summen af P3 and P4 = Undgåelse (Av)
Summen af P5 and P6 = Fornemmelse/Oplevelse af aktuel trussel (Sense of current threat)(Th).
PTSD score = Summen af Re, Av, og Th
DSO
Sum af C1 og C2 = Affektivt dysregulering (AD)
Sum af C3 og C4 = Negativt selvbillede (NSC)
Sum af C5 og C6 = Forstyrrelser i relationer til andre (DR)
DSO score = Sum af AD, NSC, and DR