

ABSTRACT
Background: There are large gender differences in PTSD prevalence. Gender differences in a wide range of trauma symptoms including disturbances in self-organization have not been extensively researched.
Objective: To explore gender differences in a wide range of trauma symptoms by comparing victimization trauma (VT) with accidental trauma (AT).
Method: A cross-sectional study of 110 traumatized patients attending a mental health outpatient clinic in Oslo, Norway (38.2% men, Mage = 40.4, 40% ethnic Norwegians). The trauma was categorized as VT or AT based on the Life Events Checklist. The Structured Clinical Interview for DSM-IV-PTSD-module and Structured Interview for Disorders of Extreme Stress Not-Otherwise-Specified (DESNOS) assessed a wide range of trauma symptoms. First, we examined gender differences within the trauma categories, then MANCOVA for an adjusted two-by-two between-groups analysis.
Results: Among VT patients, men reported more symptoms of alteration of negative self-perception (p = .02, ES = 0.50) and alteration in systems of meaning (p < .01, ES = 1.04). Within the AT group, women reported more symptoms of affect and impulses (p = .01, ES = 0.94). The VT-AT difference was significantly higher in men in intrusion (p < .01, η2 = 0.04), affect and impulses (p < .01, η2 = 0.12), negative self-perception (p < .01, η2 = 0.11), difficulty in relations (p = .01, η2 = 0.10) and alterations in systems of meaning (p = .01, η2 = 0.14). Conclusion: Comparing the VT-AT differences between the genders, men with VT had relatively more symptoms of intrusion, self-organization, identity, ideology/meaning, cognition, and relations difficulties. Effect sizes were moderate to large. Men may be relatively more vulnerable to VT than AT, while women may be more equally affected by VT and AT. Acknowledging possible gender differences in a wider range of trauma symptoms depending on trauma category may have clinical benefits
HIGHLIGHTS
Are men relatively more affected by victimization trauma and women by accidental trauma?.
A study on 110 trauma patients in Norway found large gender differences between these two trauma types.
The largest differences were in symptoms of disturbances in self-organization.
Antecedentes: Existen grandes diferencias de género en la prevalencia del trastorno de estrés postraumático. Las posibles diferencias de género en una amplia gama de síntomas de trauma, incluidas las alteraciones en la autoorganización, no se han investigado exhaustivamente.
Objetivo: Explorar las diferencias de género en una amplia gama de síntomas de trauma comparando el trauma de victimización (TV) con los traumas accidentales (TA).
Método: Un estudio transversal de 110 pacientes traumatizados que asistían a una clínica ambulatoria de salud mental en Oslo, Noruega (38,2% hombres, edad promedio = 40,4, 40% de etnia noruega). El trauma primario se clasificó como TV o TA según la Lista de verificación de eventos vitales. La Entrevista clínica estructurada para el módulo DSM-IV-TEPT y la Entrevista estructurada para trastornos de estrés extremo no especificado (DESNOS en su sigla en inglés) evaluaron una amplia gama de síntomas de trauma, principalmente analizando puntuaciones brutas de síntomas. Primero, examinamos las diferencias de género dentro de las categorías de trauma. Luego usamos MANCOVA para un análisis ajustado de dos por dos entre grupos.
Resultados: Entre los afectados por TV, los hombres reportaron más síntomas de alteración de la autopercepción negativa (p = .02, ES = 0.50) y alteración en los sistemas de significado (p < .01, ES = 1.04). Dentro del grupo TA, las mujeres informaron más síntomas de afecto e impulsos (p = 0.01, ES = 0,94). La diferencia TV-TA fue significativamente mayor en los hombres en uno de los tres grupos de síntomas de TEPT, intrusión (p < .01, η2 = 0.04), y cuatro de seis dominios de DESNOS, afecto e impulsos (p < .01, η2 = 0.12), autopercepción negativa (p < .01, η2 = 0.11), dificultad en las relaciones con los demás (p = .01, η2 = 0.10) y alteraciones en los sistemas de significado (p = .01, η2 = 0.14).
Conclusión: Al comparar las diferencias de TV y TA entre los géneros, los hombres con TV tenían relativamente más síntomas de intrusión, autoorganización, identidad, ideología/significado, cognición y dificultades en las relaciones. Los tamaños del efecto fueron de moderados a grandes. Los hombres pueden ser relativamente más vulnerables al TV que al TA, mientras que las mujeres pueden verse más igualmente afectadas por el TV y el TA. Reconocer las posibles diferencias de género en una gama más amplia de síntomas de trauma según la categoría del trauma puede tener beneficios clínicos.
背景: PTSD 的流行率存在很大的性别差异。包括自组织障碍在内的各种创伤症状中可能存在的性别差异尚未得到广泛研究。
目的: 通过比较侵害创伤 (VT) 和意外创伤 (AT), 探讨多种创伤症状的性别差异。
方法: 一项对 110 名在挪威奥斯陆心理健康门诊就诊的创伤患者进行的横断面研究 (38.2% 男性, 平均年龄为40.4, 40% 为挪威人) 。根据生活事件清单, 原发性创伤被分类为 VT 或 AT。 DSM-IV-PTSD 模块结构化临床访谈和未特定的极端应激障碍 (DESNOS) 的结构化访谈评估了广泛的创伤症状, 主要分析原始症状评分。首先, 我们考查了创伤类别中的性别差异。然后我们使用 MANCOVA 进行校正后的两两组间分析。
结果: 在受 VT 影响的人群中, 男性报告了更多的负面自我认知改变症状 (p= .02, ES = 0.50) 和意义系统改变 (p< .01, ES = 1.04) 。在 AT 组中, 女性报告了更多的情感和冲动症状 (p= .01, ES = 0.94) 。在三个 PTSD 症状簇之一的闯入 (p< .01, η2 = 0.04) 和 DESNOS, 情感和冲动六个域中的四个域中, 男性的 VT-AT 差异显著更高 (p< .01, η2 = 0.12), 消极的自我认知 (p< .01, η2 = 0.11), 与他人相处的困难 (p= .01, η2 = 0.10) 和意义系统的改变 (p= .01, η2 = 0.14)。
结论: 比较两性间VT-AT的差异, VT男性在入侵, 自组织, 身份, 意识形态/意义, 认知和人际关系困难方面的症状相对较多。效应量从中等到大。男性对VT比AT 更易感, 而女性对VT 和 AT同等易感。承认依据创伤类别的各种广泛创伤症状中可能的性别差异也许具有临床益处。
1. Introduction
1.1. Gender differences after trauma
Traumatic events are common and there seem to be comparable rates between the genders in a normal civilian setting (Kilpatrick et al., Citation2013). There is, however, a striking difference in the prevalence of trauma disorders. Rates of PTSD are estimated to be 1.5 to 5 times higher in women than in men, with the average risk of PTSD being about 2 times higher for women (Farhood, Fares, Sabbagh, & Hamady, Citation2016; Heir et al., Citation2019; Silove et al., Citation2017).
A clear reason for this has evaded researchers, but several explanations have been proposed. One theory is that men and women are exposed to different types of traumas. Typically, girls and women more often experience different types of sexual assault. Men, on the other hand, are more often exposed to violent traumas, including from combat (Tolin & Foa, Citation2006). Certain trauma types could cause more PTSD symptoms, and this could explain some of the gender differences (Chung & Breslau, Citation2008; Silove et al., Citation2017). A large study combining 18 samples found similar PTSD-prevalence gender differences within all the trauma types (Ditlevsen & Elklit, Citation2012).
Researchers have therefore looked more closely on the possibility of symptom expression being different between the genders. The proposed theory has been that the PTSD diagnosis is more suited to the symptom profile that women express (Ainamani, Elbert, Olema, & Hecker, Citation2020; Peters, Issakidis, Slade, & Andrews, Citation2006; Tekin et al., Citation2016). It has been suggested, for instance, that girls/women may be more inclined to internalizing their pain, while boys/men have a tendency to externalize it (Maschi, Morgen, Bradley, & Hatcher, Citation2008).
Other studies have not been able to confirm this theory. A large study of war veterans found minimal gender differences within items/symptoms and total burden of PTSD symptoms (King, Street, Gradus, Vogt, & Resick, Citation2013). Another study did not find any significant gender differences in the network structure of PTSD symptoms, even when women reported higher levels of all symptoms after a specific terrorist attack in Norway (Birkeland, Blix, Solberg, & Heir, Citation2017).
Furthermore, culture seems to play an important role in gender differences in trauma symptoms. One study suggests that more patriarchal cultures, like Latinos, have higher rates among women after a common trauma (Norris, Perilla, Ibañez, & Murphy, Citation2001). A larger recent study, however, found the opposite when they adjusted for other risk factors. They found no gender differences among Latinos and Asians, while women in all the other ethnic groups had significantly more PTSD symptoms (Valentine et al., Citation2019).
A few studies have interestingly found no gender differences in PTSD prevalence, mental health, or substance abuse after trauma (Kelley, Braitman, White, & Ehlke, Citation2019; Vogt et al., Citation2011). These studies are on specific populations of traumatized military and police personnel, however. There might be a significant selection bias in the small proportion of women who chose to go into these professions (Lilly, Pole, Best, Metzler, & Marmar, Citation2009).
Psychosocial differences clearly play a role as well. An interesting study, on 9/11 attacks survivors ten years later, found that gender differences in PTSD symptoms were no longer present when adjusting for socioeconomic resources, trauma type, and other demographic factors (Bowler et al., Citation2017).
Some studies have also looked at possible biological explanations. It has, for example, been suggested that females have a more sensitive hypothalamus-pituitary-adrenal-axis. Conversely males may have a more active sympathetic-adrenal-medullary-axis system (Olff, Citation2017). These may be mediated through the sex hormones (Christiansen & Berke, Citation2020; Muñoz-Reyes et al., Citation2020; Olff, Citation2017).
1.2. Gender differences in complex trauma symptoms
In normal psychology gender differences in interpersonal relationships, relational threats, group adherence, and ideology/meaning have been observed (Ekehammar & Sidanius, Citation1982; McDonald, Navarrete, & Van Vugt, Citation2012; Navarrete, McDonald, Molina, & Sidanius, Citation2010). It could therefore be that long-term intentional and interpersonal trauma could cause different symptoms between the genders.
Long-term or repeated inter-human violence and other complex traumas have been related to other symptoms than those in ‘regular’ PTSD in clinical settings for decades (Herman, Citation1992). PTSD in the DSM-IV (American Psychiatric Association, Citation1994) included an ‘associated feature’ category named Disorders of Extreme Stress Not Otherwise Specified (DESNOS). It includes seven other symptom categories, most of them related to disturbances of self-organization. The newer DSM-5 also includes two related sub-specification of PTSD: negative cognitions and mood, and a dissociative subtype (American Psychiatric Association, Citation2013).
The ICD-11 has included a diagnosis of complex PTSD where disturbances in self-organization are seen through problems in affect regulation, guilt and negative cognitions, mood and self-perception, and relational difficulties (World Health Organization, Citation2018). It specifies that complex PTSD most commonly occurs after prolonged extreme events of intentional harm from others (such as repeated abuse and torture). There is also evidence in the literature that this kind of victimization trauma (VT) more often cause these wider ranges of trauma symptoms, than accidental traumas (AT) (Bromet et al., Citation2017; Giourou et al., Citation2018). Possible gender differences in these wider ranges of trauma symptoms after VT and AT have not been thoroughly studied previously and represent a knowledge gap.
Our hypothesis is that there are gender differences in PTSD and DESNOS symptoms after VT versus AT. Particularly, there may be gender differences in symptoms such as those in disturbances of self-organization, after VT and AT.
2. Method
2.1. Method selection
By selecting a group of severely traumatized patients attending an outpatient clinic, we believed that possible gender differences in a wide range of trauma symptoms could be explored. In the main analysis we included the full range of symptom severities, while diagnostic status is presented descriptively. The examination is based on the older DESNOS diagnosis that has been less researched, but many of the symptoms are still relevant in the context of complex trauma, and partly overlap with the current ICD-11 complex PTSD diagnosis.
2.2. Participants
In the SHOT-study (Study of Health Outcome after Trauma), 119 patients with trauma exposure (as defined by DSM-IV) between 18 and 60 years of age attending a secondary mental health outpatient clinic in Southern Oslo, Norway, between 2016 and 2018, gave their written consent for participation. Nine withdrew their consent, resulting in 110 participants in the analysis. There was no requirement of a trauma diagnosis for participation. In fact, 11% did not meet the criteria for any clinical diagnosis at the study’s assessment point. The study was approved by the Regional Ethical Committee in South-Eastern Norway in January 2016 (no. 2015/2081/REK-A).
Forty-four (40%) of the participants had ethnic Norwegian background, while the remaining had roots from many different parts of the world and had come to Norway for many different reasons (Søegaard, Kan, Koirala, Hauff, & Thapa, Citation2020). Most of the immigrants came from the Middle East (36%), Eastern Europe (18%) and South Asia (14%). Thirty-eight percent of the participants were male. The men were significantly older on average (43.6 vs. 38.5 years; p = .017).
2.3. Procedure and instruments
The study consisted of self-report questionnaires and in-depth interviews with structured and semi-structured, clinical, and para-clinical instruments. It also included a battery of questions on socio-demographic information, including self-reported gender. The interviews were conducted in Norwegian or English by one of two experienced psychiatrists with specialization in trauma patients.
2.3.1. Life Events Checklist – categorizing the primary trauma
The validated instrument Life Events Checklist (LEC) reviews all the traumatic events throughout their life and connects them to 17 different categories of trauma. It also evaluates each traumatic event’s impact and the participant selects the primary trauma which currently has the highest negative impact on their life, (Gray, Litz, Hsu, & Lombardo, Citation2004). The primary trauma was subcategorized as either victimization trauma (VT) or accidental trauma (AT). VT included different types of physical violence and sexual assault, war-related trauma, murder of a close relative, captivity, and torture. AT included all other types of traumas, accidental, coincidental, and non-intentional human traumas (for example, natural disasters or motor vehicle accidents).
2.3.2. Structured Clinical Interview for DSM-IV, PTSD-module
The Structured Clinical Interview for DSM-IV PTSD-module (SCID-1-PTSD) is frequently used to diagnose PTSD. The symptom section has 17 items subdivided in three groups: intrusion (5 items), avoidance (7 items), and hyperarousal (5 items). Each question has three categories evaluated by the clinician: (1) not present, (2) partially present and (3) criteria met. The degree of symptoms within each cluster was defined by counting the number of criteria met.
2.3.3. Structured interview for disorders of extreme stress
The Structured Interview for Disorders of Extreme Stress (SIDES) is a 48-item interview that assesses seven symptom-domains of the DSM-IV associated feature diagnosis DESNOS. They are symptoms of affect and impulse regulation (6 items), consciousness and attention (2 items), negative self-perception (6 items), alterations in perception of the abuser/perpetrator (3 items), difficulty in relations/relationships with others (3 items), somatization (5 items) and alterations in systems of meaning (2 items). The response format for each item is designed to measure the presence of specific symptoms and their severity. Each item is assessed on a Likert-like scale from 0 to 3; never, sometimes, often, and very often. Each item/severity has examples that help the interviewer assess severity. Since AT rarely involves an abuser/perpetrator, we removed this DESNOS cluster of symptoms from the VT-AT analysis.
2.4. Data analysis
The data were input in IBM SPSS version 25. Descriptive statistics with skewness and kurtosis values, Kolmogorov–Smirnov test of normality and histograms were used for assessing the normality of the distribution, linearity, and homoscedasticity for continues variables. The non-parametric Mann–Whitney U-test was used when normal distribution of continuous scores was not assumed. Otherwise, independent-sample t-test was conducted to compare significant differences between groups. Pearson’s Chi-square tests was used to explore relationship between categorical variables.
Finally, a 2 by 2 between-groups analysis of covariance was used to assess and compare the relative effect of VT and AT for men and women. The independent variables were primary VT and primary AT trauma types, and gender. The dependent variables were scores on the intrusion-, avoidance- and hypervigilance degree from SCID-1-PTSD, total DESNOS score and all seven DESNOS modules scores individually from SIDES. We used MANCOVA to adjust for age as the covariate and estimated the covariance. The main effects for the two primary trauma types, VT, and AT, and gender on symptoms scores were then calculated. Effect size (ES) was estimated by using Hedge’s g for t-tests, Cramer’s V for chi-square and partial eta squared (η2) for MANCOVA. The alpha level was set at 0.05.
3. Results
3.1. Background variables
The sociodemographic characteristics of the study subjects are summarized in .
Table 1. Background characteristics of the participants by gender
Men were significantly older, fewer received welfare benefits, and more of them were refugees.
There were no statistically significant differences between the gender groups on other variables, including specific country of origin.
3.2. Types of traumatic events
The types of trauma are summarized in . As expected, women were more often affected by sexual assaults (28% vs. 12%; p = .04). Men, conversely, reported combat or war-zone experiences more often as their primary trauma (26% vs. 3%; p = .04). Of the remaining primary trauma types from LEC there were no significant gender differences. Overall, there was no gender difference in the rates of VT. Eighty-three percent of men and 84% of women reported their index trauma as VT, the remaining as AT.
Table 2. Primary trauma type of the participants by gender from the Life Events Checklist and recategorized as victimization (VT) or accidental trauma (AT)
There were no significant gender differences in the duration of the trauma, 67% men vs. 71% women reported their primary trauma as a repeated and/or longstanding (more than 3 days). Men reported on average a longer time since the trauma (16.5 vs. 9.5 years), but the finding was not statistically significant.
3.3. Gender differences in symptoms without trauma categorization
Before categorizing VT and AT, we did not find significant gender differences in the three PTSD symptom clusters. Of the seven DESNOS clusters, men had significantly higher scores in two: negative self-perception (p = .043, ES = 0.397) and alterations systems of meaning (p = .003, ES = 0.575).
Men trended to have higher rates of a current PTSD diagnosis (52.4% vs. 42.6%) and of current DESNOS diagnosis (19.0% vs. 11.8%), but neither was statistically significant. The average degrees of symptoms are shown in .
Table 3. PTSD and DESNOS symptom degree by gender, all trauma types included
3.4. Gender differences after victimization trauma and accidental trauma
When only examining the participants with VT (n = 92) men reported more symptoms negative self-perception (1.126 vs. 0.873, p = .022, ES = 0.498) and alteration in system of meaning (1.003 vs 0.606, p = .006, ES = 1.04). The remaining symptom clusters showed similar trends but were not statistically significant. The opposite was found when analysing the smaller group with AT (n = 18). Women in this group reported more symptoms of affect and impulses than men (0.253 vs. 0.157, ES = 0.943, p = .011). Women also tended to report more symptoms of most other symptom domains, but they were not statistically significant.
When we compared the VT-AT difference between the genders, we found that men with VT reported relatively more symptoms of intrusion, affect and impulse regulation, negative self-perception, difficulty in relations with others and alteration in systems of meaning. These VT-AT gender differences were statistically significant (p ≤ 0.01) after adjusting for age as a covariate. The effect sizes were moderate to large (0.040< η2 < 0.136).
As shown in , the other PTSD and DESNOS symptom clusters showed non-significant gender differences, but similar trends, with larger VT-AT differences in men. The only exception was hypervigilance symptoms, where women had a relatively higher VT-AT difference (p = .16). On the somatization symptoms module women with AT scored higher than those with VT, but this finding was not statistically significant either.
Table 4. Gender differences in PTSD and DESNOS symptom degree after victimization and accidental trauma
We also tested if refugee status, time since trauma or specific trauma type according to LEC (i.e., combat trauma) could explain some of these differences. We found they could not explain the gender differences, in neither adjusted or unadjusted analysis.
The specific DESNOS modules that showed significant VT-AT gender differences are explained in further detail below.
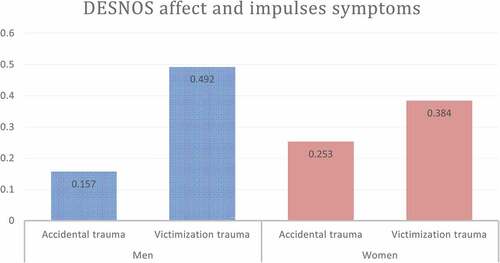
3.4.1. Affect and impulses symptoms
A higher score on this DESNOS symptoms module indicates reduction in ability to modulate anger and other affects. It includes excessive risk taking, increased sexual preoccupation, suicidal preoccupation, and self-destructiveness including suicidal ideation. Women with AT reported significantly higher scores than men with AT.
As shown in , the VT-AT difference was greater for men (0.335) than women (0.131). This relative difference between the genders was significant in the adjusted model (Δ = 0.204, p = .003, η2 = 0.122).
Figure 1. Disorder of extreme stress not otherwise specified, symptoms of affect and impulses. Gender differences between victimization and accidental traumas. (Δ = 0.204, p = .003, η2 = 0.122)
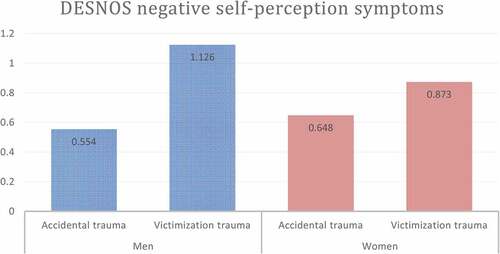
3.4.2. Negative self-perception
A higher score on the DESNOS module negative self-perception indicates more symptoms of shame, guilt, feelings of permanent damage and other related negative aspects of self-perception. Women with AT tended to have more symptoms than men with AT, while the opposite was true for VT. These findings were not statistically significant.
The VT-AT difference in men (0.572) was significantly higher than in women (0.225) when adjusting for age (Δ = 0.347, p = .007, η2 = 0.105), see .
Figure 2. Disorder of extreme stress not otherwise specified, negative self-perception. Gender differences between accidental and victimization traumas (Δ = 0.347, p = .007, η2 = 0.105)
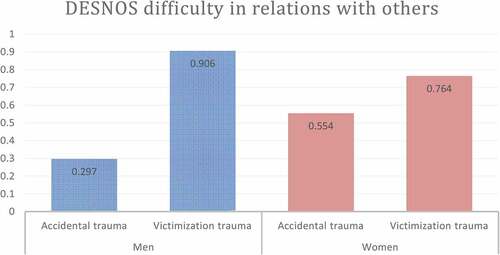
3.4.3. Difficulty in relations with others
The symptoms include inability to trust others, re-victimization, and victimizing/harming others. Within the trauma category AT women tended to report more of these symptoms than men with AT. The opposite was true for VT, but these findings were not statistically significant.
As shown in , the relative VT-AT difference was significantly higher in men (0.609) than women (0.210) when adjusting for age (Δ = 0.399, p = .013, η2 = 0.101).
Figure 3. Disorder of extreme stress not otherwise specified, module difficulty in relation with others. Gender differences between accidental and victimization traumas. (Δ = 0.399, p = .013, η2 = 0.101)
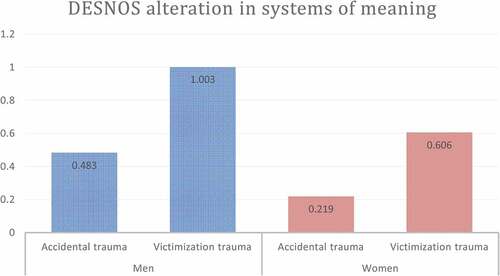
3.4.4. Alterations in systems of meaning
shows the DESNOS module alterations in systems of meaning. It includes symptoms of despair and hopelessness, and loss of previously sustaining beliefs. Men reported relatively more of these symptoms after both AT and VT than women. The VT-AT difference was also higher in men (0.520) than in women (0.387). This difference was statistically significant in the adjusted model (Δ = 0.134, p = .009, η2 = 0.136).
Figure 4. Disorder of extreme stress not otherwise specified, module alteration in systems of meaning. Gender differences between accidental and victimization traumas. (Δ = 0.134, p = .009, η2 = 0.136)
4. Discussion
The participants presented a diversity of different combinations of symptoms and symptom severity. Subtreshold symptoms were prevalent. We found significant symptom differences between the genders when we separated VT and AT trauma types. Among the participants affected by VT men reported significantly more symptoms of negative self-perception and alteration in system of meaning and trended to do so on the other symptom clusters. The opposite was true when looking at the AT group, where women reported significantly more symptoms of affect and impulses and tended to have higher scores on other symptom measures than men.
When examining the VT-AT difference within the genders men had higher differences on intrusion, affect and impulses, negative self-perception, difficulty in relations with others and alteration in systems of meaning.
The domain affect and impulses includes both aggression and risk taking, self-destruction and suicidal ideation, and sexual preoccupation. This VT-AT difference was significantly higher in men. Research has shown that boys and men have more tendencies to physical aggression and risk taking (Crocker, Haller, Norman, & Angkaw, Citation2016; Vandenberg & Marsh, Citation2009). When examining gender differences in suicidal ideation one large study that used machine learning on war veterans found that PTSD strongly predicted it in men (Gradus, King, Galatzer-Levy, & Street, Citation2017). A web-based population wide study found traumatic events were more strongly associated with suicidality in men, particularly after interpersonal trauma, childhood trauma and sexual trauma (Ásgeirsdóttir et al., Citation2018). This coincides well with our findings
The domain-negative self-perception showed similar gender differences. A recent large meta-analysis also finds clear evidence that shame plays an integral part in posttraumatic reactions (López-Castro, Saraiya, Zumberg-Smith, & Dambreville, Citation2019). Gender differences in overall negative self-perception after trauma has been less studied. One veteran study did not find gender differences in shame symptoms, but it predicted mental health symptoms and alcohol abuse (Kelley et al., Citation2019). Guilt and shame together with PTSD have been associated with more depression and functional impairment in men in two studies (Browne, Trim, Myers, & Norman, Citation2015; Bryan, Bryan, Roberge, Leifker, & Rozek, Citation2018).
The symptom domain difficulty in relations with others also showed a higher VT-AT difference in men. It includes lack of trust and propensity for re-victimization. A meta-analysis of PTSD and intimate relationship problems also found more issues in men (Taft, Watkins, Stafford, Street, & Monson, Citation2011). Two studies indicate that betrayal trauma may cause more trust issues in women, however, but the effect was small (Klest, Tamaian, & Boughner, Citation2019; Tang & Freyd, Citation2012).
Loss of meaning or negative change in existential/religious beliefs also showed gender differences in our study, where men with VT were most affected. Previous gender-specific studies on this topic found an effect both among traumatized women (Florez, Allbaugh, Harris, Schwartz, & Kaslow, Citation2018) and among mostly male war veterans (Mihaljević, Aukst-Margetić, Vuksan-Ćusa, Koić, & Milošević, Citation2012). A recent systematic review of 79 quantitative studies did not find that religiosity affected trauma reactions, however (Kucharska, Citation2020). We have not found other comparable studies that have shown gender differences in alterations of systems of meaning or religious beliefs after trauma.
When looking for possible explanations for gender differences in a wide range of trauma symptoms after the two trauma types, it may be constructive to look at gender as a biopsychosocial concept. One study suggests that women may be better at coping with VT because they seek more social support (Panknin, Citation2019). Another suggests that men may have more experiential avoidance (Leonard, Ellis, & Orcutt, Citation2020). It may also be that women are more affected by AT and have more symptoms (Udwin, Boyle, Yule, Bolton, & O’Ryan, Citation2000), and that this may explain the relative smaller VT-AT differences we found in women.
Furthermore, a recent review examining 19 studies since 2015 also found that having masculine ideals and experiencing gender role stress were associated with more PTSD symptoms (Christiansen & Berke, Citation2020). Similarly, another systematic review of both quantitative and qualitative studies of masculinity and PTSD found stronger traditional masculine ideals were related to more PTSD symptoms (Neilson, Singh, Harper, & Teng, Citation2020).
In the field of evolutionary psychology, the male-warrior hypothesis has gained support in the past decade (Van Vugt, Citation2011, pp. 233–248). Some studies have suggested that men inherently adhere more strongly to in-group/out-group categorizations as an adaptation to thousands of years inter-group conflict (McDonald et al., Citation2012; Navarrete et al., Citation2010). It could also be possible that gender differences in reactions to VT and AT have evolutionary sociobiological roots, where the stronger group attachment in men could be more affected by VT.
4.1. Conclusion
While women in the general population seem to get more PTSD symptoms and diagnoses, we found that in a sample of multi-traumatized patients seeking a mental health clinic, men with VT had relatively more symptoms of intrusion, affect and impulses, negative self-perception, difficulty in relations with others and alterations in systems of meaning. Conversely, the VT-AT difference was much smaller in women, and they seemed to be more affected by AT than men. Assessing trauma type may be relevant in a clinical setting, particularly in men. More precise assessment of patients could lead to more individually tailored treatments, especially in the context of disturbances of self-organization.
4.2. Limitations, strengths, and further research
The cross-sectional design and relatively low number of participants pose clear limitations on the generalizability of the findings. Furthermore, all the participants had been referred to the second line mental health centre, suggesting that trauma load and mental health issues were greater than what the individual could handle his/her own or through support from primary care and existing network. The findings could therefore be less applicable to the general population. Also, the group with AT was relatively small compared to those with VT in both genders.
It is well documented that men in the general population have higher threshold for seeking help for mental health symptoms (Sagar-Ouriaghli, Godfrey, Bridge, Meade, & Brown, Citation2019). Even though the men in our sample overall scored significantly higher on negative self-perception and alteration in systems of meaning symptoms, we did not find indications that they generally had more risk factors for PTSD. The differences we found held true when we tested the effect of specific trauma type, total trauma load, older age, and worse psychosocial situation (including refugee status). Men tended to have longer time since the trauma, though. This could indicate more severe symptoms or higher threshold for seeking help.
The MANCOVA analyses excludes the possibility of adjusting for non-continuous covariates. Even though we did not find statistically significant differences in refugee status within the genders, the slight non-significant difference in men with VT could contribute to their worse outcomes. Similarly, there were slightly more participants with war/combat trauma in the men with VT group. This has been found to be significant risk factors for developing a wide range of trauma symptoms (Silove, Citation1999).
Since we were primarily interested in a difference between VT and AT within each gender, and then compare the VT-AT differences between the genders, many of the above-mentioned possible bias should not pose major limitations. Age is known to affect PTSD prevalence and it interacts with gender (Ditlevsen & Elklit, Citation2010). Since we adjusted for age in the analysis, we also reduced this possible bias.
The strengths of this study were that the clinical interviews were thorough, and the statistical findings were clear, even with relatively few participants. A larger study with newer instruments assessing gender differences in ICD-11 complex PTSD symptoms after victimization and accidental traumas is recommended.
Open scholarship
 This article has earned the Center for Open Science badge for Open Data. The data are openly accessible at https://doi.org/10.17605/OSF.IO/TPA6U.
This article has earned the Center for Open Science badge for Open Data. The data are openly accessible at https://doi.org/10.17605/OSF.IO/TPA6U.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data described in this article are openly available in the Open Science Framework at https://doi.org/10.17605/OSF.IO/TPA6U.
Additional information
Funding
References
- Ainamani, H. E., Elbert, T., Olema, D. K., & Hecker, T. (2020). Gender differences in response to war-related trauma and posttraumatic stress disorder – A study among the Congolese refugees in Uganda. BMC Psychiatry, 20(1), 17. doi:10.1186/s12888-019-2420-0
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). doi:10.1176/appi.books.9780890425596
- Ásgeirsdóttir, H. G., Valdimarsdóttir, U. A., Þorsteinsdóttir, Þ. K., Lund, S. H., Tomasson, G., Nyberg, U., … Hauksdóttir, A. (2018). The association between different traumatic life events and suicidality. European Journal of Psychotraumatology, 9(1), 1510279–1510279. doi:10.1080/20008198.2018.1510279
- Birkeland, M. S., Blix, I., Solberg, Ø., & Heir, T. (2017). Gender differences in posttraumatic stress symptoms after a terrorist attack: A network approach [Original Research]. Frontiers in Psychology, 8(2091). doi:10.3389/fpsyg.2017.02091
- Bowler, R. M., Adams, S. W., Gocheva, V. V., Li, J., Mergler, D., Brackbill, R., & Cone, J. E. (2017, December). Posttraumatic stress disorder, gender, and risk factors: World trade center tower survivors 10 to 11 years after the September 11, 2001 Attacks. Journal of Traumatic Stress, 30(6), 564–12. doi:10.1002/jts.22232
- Bromet, E. J., Atwoli, L., Kawakami, N., Navarro-Mateu, F., Piotrowski, P., King, A. J., … Kessler, R. C. (2017). Post-traumatic stress disorder associated with natural and human-made disasters in the World Mental Health Surveys. Psychological Medicine, 47(2), 227–241. doi:10.1017/S0033291716002026
- Browne, K. C., Trim, R. S., Myers, U. S., & Norman, S. B. (2015). Trauma-related guilt: Conceptual development and relationship with posttraumatic stress and depressive symptoms. Journal of Traumatic Stress, 28(2), 134–141. doi:10.1002/jts.21999
- Bryan, C. J., Bryan, A. O., Roberge, E., Leifker, F. R., & Rozek, D. C. (2018). Moral injury, posttraumatic stress disorder, and suicidal behavior among National Guard personnel. Psychological Trauma: Theory, Research, Practice, and Policy, 10(1), 36–45. doi:10.1037/tra0000290
- Christiansen, D. M., & Berke, E. T. (2020). Gender- and sex-based contributors to sex differences in PTSD. Current Psychiatry Reports, 22(4), 19. doi:10.1007/s11920-020-1140-y
- Chung, H., & Breslau, N. (2008). The latent structure of post-traumatic stress disorder: Tests of invariance by gender and trauma type. Psychological Medicine, 38(4), 563–573. doi:10.1017/s0033291707002589
- Crocker, L. D., Haller, M., Norman, S. B., & Angkaw, A. C. (2016). Shame versus trauma-related guilt as mediators of the relationship between PTSD symptoms and aggression among returning veterans. Psychological Trauma: Theory, Research, Practice, and Policy, 8(4), 520–527. doi:10.1037/tra0000151
- Ditlevsen, D. N., & Elklit, A. (2010, July 21). The combined effect of gender and age on post traumatic stress disorder: Do men and women show differences in the lifespan distribution of the disorder? Annals of General Psychiatry, 9, 32. doi:10.1186/1744-859x-9-32
- Ditlevsen, D. N., & Elklit, A. (2012). Gender, trauma type, and PTSD prevalence: A re-analysis of 18 nordic convenience samples. Annals of General Psychiatry, 11(1), 26–26. doi:10.1186/1744-859X-11-26
- Ekehammar, B., & Sidanius, J. (1982). Sex differences in sociopolitical attitudes: A replication and extension. British Journal of Social Psychology, 21(3), 249–257. doi:10.1111/j.2044-8309.1982.tb00546.x
- Farhood, L. F., Fares, S., Sabbagh, R., & Hamady, C. (2016). PTSD and depression construct: Prevalence and predictors of co-occurrence in a South Lebanese civilian sample. European Journal of Psychotraumatology, 7(1), 31509. doi:10.3402/ejpt.v7.31509
- Florez, I. A., Allbaugh, L. J., Harris, C. E., Schwartz, A. C., & Kaslow, N. J. (2018). Suicidal ideation and hopelessness in PTSD: Spiritual well-being mediates outcomes over time. Anxiety, Stress, and Coping, 31(1), 46–58. doi:10.1080/10615806.2017.1369260
- Giourou, E., Skokou, M., Andrew, S. P., Alexopoulou, K., Gourzis, P., & Jelastopulu, E. (2018). Complex posttraumatic stress disorder: The need to consolidate a distinct clinical syndrome or to reevaluate features of psychiatric disorders following interpersonal trauma? World Journal of Psychiatry, 8(1), 12–19. doi:10.5498/wjp.v8.i1.12
- Gradus, J. L., King, M. W., Galatzer-Levy, I., & Street, A. E. (2017). Gender differences in machine learning models of trauma and suicidal ideation in veterans of the Iraq and Afghanistan Wars. Journal of Traumatic Stress, 30(4), 362–371. doi:10.1002/jts.22210
- Gray, M. J., Litz, B. T., Hsu, J. L., & Lombardo, T. W. (2004). Psychometric properties of the Life Events Checklist. Assessment, 11(4), 330–341. doi:10.1177/1073191104269954
- Heir, T., Bonsaksen, T., Grimholt, T., Ekeberg, Ø., Skogstad, L., Lerdal, A., & Schou-Bredal, I. (2019). Serious life events and post-traumatic stress disorder in the Norwegian population. BJPsych Open, 5(5), e82. doi:10.1192/bjo.2019.62
- Herman, J. L. (1992). Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress, 5(3), 377–391. doi:10.1002/jts.2490050305
- Kelley, M. L., Braitman, A. L., White, T. D., & Ehlke, S. J. (2019). Sex differences in mental health symptoms and substance use and their association with moral injury in veterans. Psychological Trauma: Theory, Research, Practice, and Policy, 11(3), 337–344. doi:10.1037/tra0000407
- Kilpatrick, D. G., Resnick, H. S., Milanak, M. E., Miller, M. W., Keyes, K. M., & Friedman, M. J. (2013). National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress, 26(5), 537–547. doi:10.1002/jts.21848
- King, M. W., Street, A. E., Gradus, J. L., Vogt, D. S., & Resick, P. A. (2013). Gender differences in posttraumatic stress symptoms among OEF/OIF veterans: An item response theory analysis. Journal of Traumatic Stress, 26(2), 175–183. doi:10.1002/jts.21802
- Klest, B., Tamaian, A., & Boughner, E. (2019). A model exploring the relationship between betrayal trauma and health: The roles of mental health, attachment, trust in healthcare systems, and nonadherence to treatment. Psychological Trauma: Theory, Research, Practice, and Policy, 11, 656–662. doi:10.1037/tra0000453
- Kucharska, J. (2020). Religiosity and the psychological outcomes of trauma: A systematic review of quantitative studies. Journal of Clinical Psychology, 76(1), 40–58. doi:10.1002/jclp.22867
- Leonard, K. A., Ellis, R. A., & Orcutt, H. K. (2020). Experiential avoidance as a mediator in the relationship between shame and posttraumatic stress disorder: The effect of gender. Psychological Trauma: Theory, Research, Practice, and Policy, 12, 651–658. doi:10.1037/tra0000601
- Lilly, M., Pole, N., Best, S., Metzler, T., & Marmar, C. (2009). Gender and PTSD: What can we learn from female police officers? Journal of Anxiety Disorders, 23, 767–774. doi:10.1016/j.janxdis.2009.02.015
- López-Castro, T., Saraiya, T., Zumberg-Smith, K., & Dambreville, N. (2019). Association between shame and posttraumatic stress disorder: A meta-analysis. Journal of Traumatic Stress, 32(4), 484–495. doi:10.1002/jts.22411
- Maschi, T., Morgen, K., Bradley, C., & Hatcher, S. S. (2008). Exploring gender differences on internalizing and externalizing behavior among maltreated youth: Implications for social work action. Child and Adolescent Social Work Journal, 25(6), 531–547. doi:10.1007/s10560-008-0139-8
- McDonald, M. M., Navarrete, C. D., & Van Vugt, M. (2012). Evolution and the psychology of intergroup conflict: The male warrior hypothesis. Philosophical Transactions of the Royal Society B: Biological Sciences, 367(1589), 670–679. doi:10.1098/rstb.2011.0301
- Mihaljević, S., Aukst-Margetić, B., Vuksan-Ćusa, B., Koić, E., & Milošević, M. (2012). Hopelessness, suicidality and religious coping in Croatian war veterans with PTSD. Psychiatria Danubina, 24(3), 292–297. http://www.psychiatria-danubina.com/UserDocsImages/pdf/dnb_vol24_no3/dnb_vol24_no3_292.pdf
- Muñoz-Reyes, J. A., Polo, P., Valenzuela, N., Pavez, P., Ramírez-Herrera, O., Figueroa, O., … Pita, M. (2020). The male warrior hypothesis: Testosterone-related cooperation and aggression in the context of intergroup conflict. Scientific Reports, 10(1), 375. doi:10.1038/s41598-019-57259-0
- Navarrete, C. D., McDonald, M. M., Molina, L. E., & Sidanius, J. (2010). Prejudice at the nexus of race and gender: An outgroup male target hypothesis. Journal of Personality and Social Psychology, 98(6), 933. doi:10.1037/a0017931
- Neilson, E. C., Singh, R. S., Harper, K. L., & Teng, E. J. (2020). Traditional masculinity ideology, posttraumatic stress disorder (PTSD) symptom severity, and treatment in service members and veterans: A systematic review. Psychology of Men & Masculinities, 21(4), 578–592. doi:10.1037/men0000257
- Norris, F. H., Perilla, J. L., Ibañez, G. E., & Murphy, A. D. (2001). Sex differences in symptoms of posttraumatic stress: Does culture play a role? Journal of Traumatic Stress, 14(1), 7–28. doi:10.1023/A:1007851413867
- Olff, M. (2017). Sex and gender differences in post-traumatic stress disorder: An update. European Journal of Psychotraumatology, 8(sup4), 1351204. doi:10.1080/20008198.2017.1351204
- Panknin, J. (2019). Man-up when down—gender-specific coping with life stressors (Master thesis). Lund, Sweden: Lund University. Retrieved from https://lup.lub.lu.se/student-papers/search/publication/8984489
- Peters, L., Issakidis, C., Slade, T., & Andrews, G. (2006). Gender differences in the prevalence of DSM-IV and ICD-10 PTSD. Psychological Medicine, 36(1), 81–89. doi:10.1017/s003329170500591x
- Sagar-Ouriaghli, I., Godfrey, E., Bridge, L., Meade, L., & Brown, J. S. L. (2019). Improving mental health service utilization among men: A systematic review and synthesis of behavior change techniques within interventions targeting help-seeking. American Journal of Men’s Health, 13(3), 155798831985700. doi:10.1177/1557988319857009
- Silove, D. (1999). The psychosocial effects of torture, mass human rights violations, and refugee trauma: Toward an integrated conceptual framework. The Journal of Nervous & Mental Disease, 187(4), 200–207. doi:10.1097/00005053-199904000-00002
- Silove, D., Baker, J. R., Mohsin, M., Teesson, M., Creamer, M., O’Donnell, M., … Rees, S. (2017). The contribution of gender-based violence and network trauma to gender differences in Post-Traumatic Stress Disorder. PloS One, 12(2), e0171879–e0171879. doi:10.1371/journal.pone.0171879
- Søegaard, E. G. I., Kan, Z., Koirala, R., Hauff, E., & Thapa, S. B. (2020). Variations in psychiatric morbidity between traumatized Norwegian, refugees and other immigrant patients in Oslo. Nordic Journal of Psychiatry, 74(6), 390–399. doi:10.1080/08039488.2020.1714724
- Taft, C. T., Watkins, L. E., Stafford, J., Street, A. E., & Monson, C. M. (2011). Posttraumatic stress disorder and intimate relationship problems: A meta-analysis. Journal of Consulting and Clinical Psychology, 79(1), 22–33. doi:10.1037/a0022196
- Tang, S. S. S., & Freyd, J. J. (2012). Betrayal trauma and gender differences in posttraumatic stress. Psychological Trauma: Theory, Research, Practice, and Policy, 4, 469–478. doi:10.1037/a0025765
- Tekin, A., Karadağ, H., Süleymanoğlu, M., Tekin, M., Kayran, Y., Alpak, G., & Şar, V. (2016). Prevalence and gender differences in symptomatology of posttraumatic stress disorder and depression among Iraqi Yazidis displaced into Turkey. European Journal of Psychotraumatology, 7, 28556–28556. doi:10.3402/ejpt.v7.28556
- Tolin, D. F., & Foa, E. B. (2006, November). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132(6), 959–992. doi:10.1037/0033-2909.132.6.959
- Udwin, O., Boyle, S., Yule, W., Bolton, D., & O’Ryan, D. (2000, November). Risk factors for long-term psychological effects of a disaster experienced in adolescence: Predictors of post traumatic stress disorder. Journal of Child Psychology and Psychiatry, 41(8), 969–979. doi:10.1111/1469-7610.00685
- Valentine, S. E., Marques, L., Wang, Y., Ahles, E. M., Dixon De Silva, L., & Alegría, M. (2019). Gender differences in exposure to potentially traumatic events and diagnosis of posttraumatic stress disorder (PTSD) by racial and ethnic group. General Hospital Psychiatry, 61, 60–68. doi:10.1016/j.genhosppsych.2019.10.008
- Van Vugt, M. (2011). The male warrior hypothesis. The psychology of social conflict and aggression. Psychology Press. https://psycnet.apa.org/record/2011-07931-015
- Vandenberg, B., & Marsh, U. (2009). Aggression in youths: Child abuse, gender and SES. North American Journal of Psychology, 11(3), 437–442. http://najp.us/wp-content/uploads/2014/11/Vol.-11-Issue-3.pdf
- Vogt, D., Vaughn, R., Glickman, M. E., Schultz, M., Drainoni, M. L., Elwy, R., & Eisen, S. (2011). Gender differences in combat-related stressors and their association with postdeployment mental health in a nationally representative sample of U.S. OEF/OIF veterans. Journal of Abnormal Psychology, 120(4), 797–806. doi:10.1037/a0023452
- World Health Organization. (2018). International statistical classification of diseases and related health problems (ICD-11). Retrieved from https://icd.who.int/