
ABSTRACT
The aim of this article is to present a research-based rationale for NETfacts, a newly developed integrated approach at the individual and the community level in order to mitigate the mental and social sequelae of war and crisis. To this end, we provide a selective review of relevant literature from neuroscience, clinical psychology, and social science. In psychotraumatology, individual avoidance describes the effort to prevent exposure to trauma reminders. Among patients with post-traumatic stress disorder (PTSD), this becomes pathological, exacerbating distress and preventing recovery. This silence resonates in traumatized communities and consequently taboo builds – ultimately to the advantage of the perpetrators. The resulting collective avoidance leads to a fragmented collective memory about trauma or human rights violations in the community so that a shared account of the group’s history becomes impossible. The deficient collective memory promotes ambiguous truths and anxiety, enabling a reactive construction of safety based on selective information that leads to an endorsement of extreme opinions. Ongoing insecurity, violence and crime lead to increasing anxiety and fear. The self-interest of the perpetrators and the abnormal behaviour of survivors leads to an escalation in stigma and social exclusion resulting in the prevention or limitation of community exposure to traumatic material, i.e., to reduce tension and protect the construction of safety. The exposure to and recognition of traumatic facts subject to avoidance is key to a coherent collective memory and sense of communion, and to prevent further cycles of violence. The NETfacts health system combines individual and community-based intervention to treat the structure of memory at both the individual and collective levels.
Abbreviations: NET: narrative exposure therapy; FORNET: narrative exposure therapy for forensic offender rehabilitation; NETfacts: facts derived from narrative exposure therapy
HIGHLIGHTS
The article provides selected neuroscientific, clinical, and social science research to introduce the theoretical rationale of NETfacts; a newly developed integrated approach at the individual and the community level to mitigate the mental and social sequelae of crisis.
El objetivo de este artículo es presentar una justificación basada en la investigación para NETfacts; un enfoque integrado recientemente desarrollado a nivel individual y comunitario para mitigar las secuelas mentales y sociales de la guerra y la crisis. Con este fin, proporcionamos una revisión selectiva de la literatura relevante de la neurociencia, la psicología clínica, y las ciencias sociales. En psicotraumatología, la evitación individual describe el esfuerzo para prevenir la exposición a recordatorios del trauma. Entre los pacientes con trastorno de estrés postraumático (TEPT), este se vuelve patológico, exacerbando la angustia e impidiendo la recuperación. Este silencio resuena en las comunidades traumatizadas y, en consecuencia, se construye como un tabú, en última instancia en beneficio de los perpetradores. La evasión colectiva resultante conduce a una memoria colectiva fragmentada sobre el trauma o las violaciones de los derechos humanos en la comunidad, por lo que un relato compartido de la historia del grupo se vuelve imposible. La memoria colectiva deficiente promueve verdades ambiguas y ansiedad, posibilitando una construcción reactiva de seguridad basada en información selectiva que conduce al respaldo de opiniones extremas. La inseguridad, la violencia y la delincuencia continuas provocan un aumento de la ansiedad y el miedo. El interés propio de los perpetradores y el comportamiento anormal de los sobrevivientes conduce a una escalada del estigma y la exclusión social que resulta en la prevención o limitación de la exposición de la comunidad al material traumático, es decir, reduce la tensión y protege la construcción de la seguridad. La exposición y el reconocimiento de los hechos traumáticos sujetos a evitación son claves para una memoria colectiva coherente y un sentido de comunión, y para prevenir nuevos ciclos de violencia. El sistema de salud NETfacts combina la intervención individual y comunitaria para tratar la estructura de la memoria tanto a nivel individual como colectivo.
本文旨在 NETfacts, 一种新开发的用以减轻战争和危机的心理和社会后遗症的个人和团体水平的综合方法, 提供基于研究的理论依据。为此, 我们对神经科学, 临床心理学和社会科学的相关文献进行了选择性回顾。在心理创伤学中, 个体回避描述了防止暴露于创伤提示物的努力。在创伤后应激障碍 (PTSD) 患者中, 这会变成病理性的, 加剧痛苦并阻止康复。这种沉默在遭受创伤的团体中引起共鸣, 从而产生了禁忌——最终对施暴者有利。由此产生的集体回避导致关于团体创伤或侵犯人权的集体记忆破碎, 因此无法实现群体历史的共享解释。不足的集体记忆会促进模糊事实和焦虑, 使基于选择性信息的安全反应构建成为可能, 从而导致产生极端观点。持续的不安全感, 暴力和犯罪导致焦虑和恐惧加剧。肇事者的私利和幸存者的异常行为导致污名化和社会排斥升级, 从而防止或限制团体接触创伤材料, 即减少紧张感并保护安全感建立。以回避为准的暴露和识别创伤性事实是连贯集体记忆和共享感, 并防止进一步暴力循环的关键。 NETfacts 健康系统结合了个人和团体干预措施, 以在个人和集体层面处理记忆结构。
1. Trauma and the individual
When an individual is exposed to severe trauma or perpetrates violence, strong affective responses are triggered that enhance implicit details of the terrifying scene that are stored in memory (Belleau et al., Citation2020; Elbert & Schauer, Citation2002; Wilker & Kolassa, Citation2013). Over time, the mnesic consequences of cumulative victimization and perpetration may alter cognitive and affective processes fundamental to meaningful engagement in the social environment (Köbach, Schaal, & Elbert, Citation2015; Schauer & Robjant, Citation2018; Wilker et al., Citation2015). The bi-cycles of violence model describes how violence increases the likelihood of future violent behaviours as a result of complex automatic defence reactions and associative neural networks that also determine the mental sequelae of these events (Elbert, Schauer, & Moran, Citation2018; Schauer & Elbert, Citation2010). Whereas surviving trauma induces a negative valence (fear, horror, helplessness) and is linked to mental disorders like PTSD, depression, anxiety and reactive aggression (Anderson & Bushman, Citation2002; Crick & Dodge, Citation1996; Vitiello & Stoff, Citation1997), the perpetration of violence may carry an ambivalent or positive valence and facilitate antisocial personality traits, psychopathy and an ‘appetite’ or even addiction for aggression (Elbert, Weierstall, & Schauer, Citation2010; Golden, Jin, & Shaham, Citation2019). The opposite valence of the resulting associative networks for positive-perpetrated acts compared to negative-experienced events is theorized to prevent their fusion, facilitating the aforementioned bi-cyclic structure of trauma-related mental consequences (Elbert et al., Citation2018). With accumulating victimization and/or perpetration, the cohesive associative so-called trauma/fear and hunting networks (implicit/‘hot’) are detached from their spatio-temporal context and autobiographical (explicit/‘cold’) memory leading to a perceived omnipresence of threat. This also results in the re-experiencing of the trauma memory in the ‘here and now’ (intrusions/flashbacks), hyperarousal, heightened reactive/appetitive aggression and depression symptoms (Brewin, Citation2011; Elbert et al., Citation2018; Wilker & Kolassa, Citation2013). The threshold to behave violently is lowered in these individuals and leads to an increased collective aggression (see , ), and therefore higher levels of family (Catani, Citation2010; Webermann et al., Citation2020) and community violence (Nandi et al., Citation2017; Robjant, Schmitt, Chibashimba, et al., Citation2020), or crime (Aebi et al., Citation2017; Webb et al., Citation2017). At the same time, this specific memory structure impairs the verbal accessibility of its content (Brewin, Citation2011; Ehlers, Hackmann, & Michael, Citation2004; Foa, Molnar, & Cashman, Citation1995), especially when the victim dissociated during the traumatic experience (Bedard-Gilligan & Zoellner, Citation2012; Peltonen, Kangaslampi, Saranpää, Qouta, & Punamäki, Citation2017). Moreover, communication with others is inhibited through trauma-related social affect, avoidance, and transient mutism:
Figure 1. Theoretical model for the transfer of mental consequences of individual victimization and perpetration into an increasing fragmentation of the collective memory
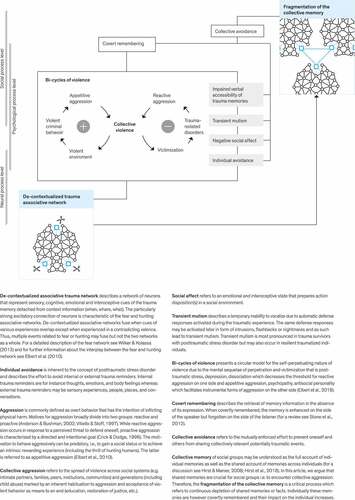
Figure 2. Social dynamics that escalate collective violence and mental health crises and how NETfacts aims to interrupt these processes by restoring individual and collective memory

1.1. De-contextualized and cohesive associative trauma networks impair verbal accessibility
Where there are several traumatic events linked together within the fear network, reminders of one event will trigger others to be re-experienced (Wilker & Kolassa, Citation2013). The de-contextualized, disorganized character of multiple fear-related memories (Brewin, Citation2011; Ehlers et al., Citation2004; Schauer, Neuner, & Elbert, Citation2011) potentially with amnesic gaps caused by peritraumatic dissociation (Schauer & Elbert, Citation2010) combined with the high negative emotional and physiological arousal during recall poses a major barrier to access trauma memories and to narrate this information during social interaction with family members or friends.
1.2. Social affects result in submission and withdrawal
Trauma-related social affects such as shame (Sznycer et al., Citation2018) and guilt (Kubany & Watson, Citation2003) further inhibit disclosure especially for events of perceived social transgression, for example sexual assaults or forced perpetration and lead to submission and withdrawal (Maercker & Horn, Citation2013) as well as altered cognitions (Ehlers & Clark, Citation2000; Stevens & Jovanovic, Citation2019). Bryant et al. (Citation2017) used a social network approach and found individuals with the highest risk of PTSD were at the margins of the network and had fewer social connections.
1.3. Individual avoidance of internal and external trauma reminders
Individual avoidance is a symptom of PTSD and includes avoidance of people, places, activities, thoughts or other reminders of traumatic events (American Psychiatric Association, Citation2013). However, in the aftermath of trauma, resilient coping involves both the confrontation of emotional details of the traumatic events in the internal or external world as well as the private and social realm, but conversely its suppression when this is not appropriate (Pennebaker & Harber, Citation1993). Excessive avoidance prevents habituation to the memory and the reappraisal of meaning (Foa, Steketee, & Rothbaum, Citation1989) and therefore becomes maladaptive and contributes to the development of PTSD when intrinsic dynamics of the fear network are uncontrollably triggered outside of the spatio-temporal context in which they occurred. Stone, Coman, Brown, Koppel, and Hirst (Citation2012) describe various experiments showing a facilitation of memory when events are covertly remembered (see ). Thus, intrusive memories – typically subject to covert remembering – would be more frequently recalled by the victim. Accordingly, individuals with high levels of avoidance presented with lower post-trauma remission rates in a sample of survivors of sexual violence (Müller et al., Citation2018).
1.4. Transient mutism due to automatic defence reactions
Biological mechanisms that are automatically activated during the traumatic experience suppress verbal expression during the attack and enforce the expression of submissive behaviour in the victim in order to avoid further aggression from the perpetrators and ensure the best possible chance of survival (Moskowitz, Citation2004; Schauer & Elbert, Citation2010). Victims in the peritraumatic fright or shut down/flag state are physiologically unable to shout out, scream or cry or express certain emotions (here referred to as transient mutism). When remembering the experience(s) these automatic responses are again activated together with other peritraumatic physiological reactions.
2. Trauma and the community
How does this resonate at the social process level? The interplay of these complex factors of the trauma associative network that imposes an impaired verbal accessibility, social affect/cognition, transient mutism and avoidance at the individual level contribute to the development and maintenance of a traumatized community, whose ability to cope with their personal trauma and care for the traumatized individuals within the family and community is compromised. Traumatic events are increasingly covertly remembered (Stone et al., Citation2012). Furthermore, with increasing trauma exposure, and with it the increasing loss of contextual integration of one’s trauma memories, more rigorous and systematic avoidance is perceived to be required and may actually be adaptive to maintain psychological integrity and stability (Mary et al., Citation2020). The assumedly necessary and adaptive avoidance practiced by the majority of individuals in trauma-exposed communities together with the extreme (pathological) efforts to avoid reminders in individuals with PTSD together with the inhibition to talk about the trauma due to the impaired memory, transient mutism, shame and guilt, all combine to result in a collective avoidance. Traumatic events are not disclosed, and where they are, the listener is protected from the full horror of the events. As a result, details about the most severe human rights abuses remain unknown, and therefore there is no challenge of existing incomplete and biased narratives or perspective taking. Consequently, the complete ‘facts’ that also include the survivor’s complete internal experience of the events fail to enter the shared account of the collective memory of community members (Hirst & Echterhoff, Citation2012; Hirst, Yamashiro, & Coman, Citation2018) and lead to a continuous fragmentation of the collective memory (see ).
2.1. Adding insult to injury: the institutionalization of ‘othering’
This vicious cycle is doomed to escalate in the absence of a functioning justice system and in contexts of continuous violence and crime. The collective adaptation to violent behaviours and resulting learned helplessness increases the perceived need to restore safety/control and regulate anxiety to maintain psychological integrity. In an attempt to resolve this cognitive dissonance (Festinger, Citation1957) subjects tend to exaggerate individual characteristics or behaviour as the primary reasons for victimhood (attitude change; McGrath, Citation2017), especially when defending their assumption of a just world or safety (Dawtry, Callan, Harvey, & Gheorghiu, Citation2020; Lerner, Citation1980; Pinciotti & Orcutt, Citation2019; Walster, Citation1966). In a meta-analysis with 55 experimental studies, Dawtry et al. (Citation2020) confirmed that victims were rated less favourable when presenting with greater and more authentic suffering, or when harm went unpunished. The emotional impact of the situation was associated with a stronger effect (Dawtry et al., Citation2020; Lerner, Citation2003) suggesting that there would be a higher likelihood of victim blaming/derogation in the real and post-conflict world compared to Western laboratory experiments. As multiple individuals in a community are targeted, confirmation bias (Nickerson, Citation1998) and social influence (Cialdini & Goldstein, Citation2004) mechanisms render the characteristics that are congruent with victim blaming/derogation more salient. This allows counterfactual narratives to emerge. Social inclusiveness is therefore broken down as conformity increases. At the same time, the reality of the indiscriminate, unpredictable and extreme violence is too frightening to confront since it is uncontrollable, and therefore remains subject to avoidance. In the absence of authentic, complete and detailed narratives about interpersonal assaults and crime, optimal narratives are adopted to create a coherent ‘explanation’ of these events – enhancing perceived safety but ignoring the unspoken details (Callan, Kay, Davidenko, & Ellard, Citation2009; Hirst & Coman, Citation2018; Stone, Barnier, Sutton, & Hirst, Citation2010). With a critical mass adopting this coping strategy, the ‘othering’ is institutionalized and discriminatory practices embedded within cultural norms and local customs and laws (Edwards, Turchik, Dardis, Reynolds, & Gidycz, Citation2011). A reciprocal conspiracy of avoidance, silence, shame, and othering, prevents the sharing of the testimony of trauma survivors and consequently leads to a fragmentation of the collective past. This results in victim marginalization (which in turn increases mental illness; Bryant et al., Citation2017), the acquittal of perpetrators from responsibility (Edwards et al., Citation2011), lack of trust and ultimately the continuation of violence alongside discriminatory narratives and norms.
In the aftermath of violence or conflict, it is therefore necessary not only to ensure that individuals are treated for both PTSD and aggression but also that the community is ‘treated’ for the collective avoidance that mirrors the individual avoidance and that otherwise leads to or maintains a ‘pathological’ response within the community. For recovery, traumatized individuals must be able to share their experiences with other community members, who must reciprocally be able to bear the testimonies and integrate these events into the community narrative.
3. The NETfacts health system: building up on evidence based trauma therapy
The core element of evidence-based trauma treatments for individuals is the reprocessing of traumatic memories in a safe environment and, together with the therapist, verbalizing and re-structuring the most terrifying moments (Schnyder et al., Citation2015). This is realized in Narrative Exposure Therapy (NET; Schauer et al., Citation2011) in which the client reports and relives the most arousing events from birth to present while the therapist writes down the narrative. Due to the level of detail acquired during therapeutic exposure, these narratives or testimonies contain a great deal of authenticity and truth. Effectiveness of NET has been demonstrated in multiple trials and meta-analyses with largest effects found in long-term follow-ups (Siehl, Robjant, & Crombach, Citation2020). Another strength of NET is that the majority of studies were conducted in humanitarian and emergency settings (e.g. Koebach, Carleial, Elbert, Schmitt, & Robjant, Citation2021; Neuner, Schauer, Klaschik, Karunakara, & Elbert, Citation2004; Orang et al., Citation2018; Schaal, Elbert, & Neuner, Citation2009). Biological studies have revealed impacts on the immune system (Morath, Gola, et al., Citation2014; Morath, Moreno-Villanueva, et al., Citation2014) and DNA methylation in genes relevant to memory processes (Carleial et al., Citation2021). As described above, symptoms of PTSD may drive violence, especially when fear is triggered by cues from the past (reactive aggression). Perpetrating violence in turn leads to ‘appetitive aggression’, which may acquire addictive properties (Golden et al., Citation2019). Therefore, unless the aggression is treated alongside the trauma, peace-building efforts will always be sabotaged by those with appetitive aggression from high exposure to perpetration. To address this dual problem, NET has been adapted for traumatized offenders (NET for forensic offender rehabilitation, FORNET; Elbert, Hermenau, Hecker, Weierstall, & Schauer, Citation2012). In two recent randomized controlled trials, we have demonstrated that the latest version of FORNET significantly reduces aggressive and antisocial behaviour alongside symptoms of posttraumatic stress (Koebach et al., Citation2021; Robjant et al., Citation2019).
Testimonies derived from NET and FORNET treatments reveal trauma-related dynamics in communities subject to suppression due to collective avoidance and provide the missing facts that when integrated can re-compose the fragmented collective memory. To this end, the NETfacts health system combines individual and community-based treatment to enable a stepped care model in which clinical cases receive individual treatment for their symptoms of PTSD and/or aggression (NET or FORNET) and (traumatized) resilient individuals receive a low-intensity community-based intervention to share facts derived from NET (NETfacts). To enable avoided information of the trauma narratives to re-emerge in the community and create collective memory, NETfacts adopts forms of information sharing that are already socially accepted. Therefore, narrative storytelling, theatre, fine art, dance and other local and specific culturally relevant practices can be utilized. Additionally, NETfacts involves discussions about the collective past and future to facilitate a more peaceful future path from within the community. Essential elements of NETfacts are the community lifeline and composite narratives. The community lifeline is developed jointly by the community members to represent their collective past and presents the basis for the selection of information fed back to the community. Analogue to the individual lifeline exercise in NET, the community lifeline uses flowers, stones and sticks for positive and negative events and active involvement in violent perpetration. NETfacts composite narratives are anonymized versions of repetitive features of traumatic events in a community derived from narratives recorded during NET and FORNET. A composite narrative describes a single traumatic event including essential sensory, cognitive, emotional and interoceptive details of the same type that are inherent and familiar to the community members who have also experienced these types of events.For instance, the perception of danger automatically results in a thought “I’m in danger” (cognition), triggering fear (emotion), and associated physiological responses (e.g. fast heartbeat and respiration). Composite narratives aim to reveal and emphasize the deliberate action of the perpetrator and the arbitrariness of the selection of the person as victim and thus break biases induced by beliefs in a just world and false claims. The process of vicarious remembering of traumatic events is an essential therapeutic mechanism of NETfacts but requires special attention to individuals whose trauma memories may be triggered. To this end, access to NET and FORNET is essential and trauma counsellors should accompany community exposure meetings and provide support. The implementation of the NETfacts system is limited to settings where individuals who report their experiences are safe and carry no risk of being punished by an armed force for that reason. Implementation should only be realized by an organization that can ensure no potential conflict of interest regarding the facts that may emerge.
In the Eastern DR Congo, we implemented the NETfacts health system through the following components: (1) scale up of NET and FORNET for trauma survivors and perpetrators with clinically relevant symptoms; (2) provision of singular exposure sessions for community members with subclinical symptom severities to (a) enhance resilience in survivors with subclinical symptoms, (b) increase ownership of the archive of narratives; (3) re-creation of a collective memory through a community lifeline to enhance understanding of the shared history and multi-faceted nature of collective trauma; (4) sharing of composite narratives incorporating the facts about recurrent trauma and violence of collective relevance to reduce collective avoidance (community exposure); (5) promotion of adaptive trauma communication and support by encouraging discussions about ‘collectively relevant trauma’, (6) discussing a future in which needs of trauma survivors and the social realm are harmonized by collecting identified needs and practical steps to achieve them (Robjant, Schmitt, Koebach, Chibashimba, & Elbert, Citation2020). Results of our feasibility trial show an increase in reconciliation with former combatants and willingness to care for family members who experience sexual violence, a wide spread problem in the region (Schmitt et al., Citationsubmitted). In a randomized controlled trial (RCT), we found a greater reduction of rape myth acceptance and less scepticism to reconstruct with former combatants in community members who presented with war-related PTSD in the NETfacts condition compared to the individual component only (CitationRobjant, Schmitt, Chibashimba, Elbert, & Koebach, in prep). We further found a significant decrease in PTSD and depression symptom severity after the NETfacts community meetings in PTSD clients (CitationRobjant etal., in prep).
4. Summary
Collective avoidance of trauma-related facts is an inherent strategy to cope with anxiety that collectively escalates when safety cannot be guaranteed. However, it also allows violence and trauma to spread through facilitating silence around the ‘facts’ of the trauma experienced and the emergence of a fragmented collective memory. The NETfacts health system combines individual and community-based interventions to restore individual autobiography (‘This is me, I am’; Schauer et al., Citation2011) and collective memory (‘This is us, we are’) and with it, facilitates a trauma informed, peaceful future for the next generation.
Ethics statement
Not applicable.
Acknowledgments
We would like to dedicate special acknowledgement to Prof. Thomas Elbert who co-developed NET and initiated NETfacts and continuously emphasized the importance of the human rights perspective in the approach. Moreover, we would also like to express great appreciation to Dr. Sabine Schmitt who coordinated the implementation of a pilot and randomized controlled study in NETfacts. We thank Amani Chibashimba, Dr. Harald Hinkel, Pia Peeter, Patricia Fernandes, and the NGO vivo international e.V for their continuous support.
Data availability statement
Not applicable.
Disclosure statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors aim to disseminate NETfacts to those in need. They have worked as trainers in the DR Congo and are ready to support training in other contexts.
Additional information
Funding
References
- Aebi, M., Mohler-Kuo, M., Barra, S., Schnyder, U., Maier, T., & Landolt, M. (2017). Posttraumatic stress and youth violence perpetration: A population-based cross-sectional study. European Psychiatry, 40, 88–10. doi:10.1016/j.eurpsy.2016.08.007
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). 5th ed . Arlington: American Psychiatric Pub https://doi.org/10.1176/appi.books.9780890425596.
- Anderson, C. A., & Bushman, B. J. (2002). Human aggression. Annual Review of Psychology, 53(1), 27–51. doi:10.1146/annurev.psych.53.100901.135231
- Bedard-Gilligan, M., & Zoellner, L. A. (2012). Dissociation and memory fragmentation in post-traumatic stress disorder: An evaluation of the dissociative encoding hypothesis. Memory, 20(3), 277–299. doi:10.1080/09658211.2012.655747
- Belleau, E. L., Ehret, L. E., Hanson, J. L., Brasel, K. J., Larson, C. L., & Cassini, T. A. (2020). Amygdala functional connectivity in the acute aftermath of trauma prospectively predicts severity of posttraumatic stress symptoms. Neurobiology of Stress, 100217. doi:10.1016/j.ynstr.2020.100217
- Brewin, C. R. (2011). The nature and significance of memory disturbance in posttraumatic stress disorder. Annual Review of Clinical Psychology, 7(1), 203–227. doi:10.1146/annurev-clinpsy-032210-104544
- Bryant, R. A., Gallagher, H. C., Gibbs, L., Pattison, P., MacDougall, C., Harms, L., … Ireton, G. (2017). Mental health and social networks after disaster. American Journal of Psychiatry, 174(3), 277–285. doi:10.1176/appi.ajp.2016.15111403
- Callan, M. J., Kay, A. C., Davidenko, N., & Ellard, J. H. (2009). The effects of justice motivation on memory for self- and other-relevant events. Journal of Experimental Social Psychology, 45(4), 614–623. doi:10.1016/j.jesp.2009.02.013
- Carleial, S., Nätt, D., Unternaehrer, E., Elbert, T., Robjant, K., Zeller, A., … Koebach, A. (2021). DNA methylation changes following Narrative Exposure Therapy in a randomised controlled trial with former female child soldiers. Scientific Reports, 11. doi:10.1038/s41598-021-98067-9
- Catani, C. (2010). War at home–a review of the relationship between war trauma and family violence. Verhaltenstherapie, 20(1), 19–27. doi:10.1159/000261994
- Cialdini, R. B., & Goldstein, N. J. (2004). Social influence: Compliance and conformity. Annual Review of Psychology, 55(1), 591–621. doi:10.1146/annurev.psych.55.090902.142015
- Crick, N. R., & Dodge, K. A. (1996). Social information‐processing mechanisms in reactive and proactive aggression. Child Development, 67(3), 993–1002. doi:10.2307/1131875
- Dawtry, R. J., Callan, M. J., Harvey, A. J., & Gheorghiu, A. I. (2020). Victims, vignettes, and videos: Meta-analytic and experimental evidence that emotional impact enhances the derogation of innocent victims. Personality and Social Psychology Review, 24(3), 233–259. doi:10.1177/1088868320914208
- Edwards, K. M., Turchik, J. A., Dardis, C. M., Reynolds, N., & Gidycz, C. A. (2011). Rape myths: History, individual and institutional-level presence, and implications for change. Sex Roles, 65(11–12), 761–773. doi:10.1007/s11199-011-9943-2
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345. doi:10.1016/S0005-7967(99)00123-0
- Ehlers, A., Hackmann, A., & Michael, T. (2004). Intrusive re‐experiencing in post‐traumatic stress disorder: Phenomenology, theory, and therapy. Memory, 12(4), 403–415. doi:10.1080/09658210444000025
- Elbert, T., Hermenau, K., Hecker, T., Weierstall, R., & Schauer, M. (2012). FORNET: Behandlung von traumatisierten und nicht-traumatisierten Gewalttätern mittels Narrativer Expositionstherapie. In J. Endrass, and A. Rossegger (Eds.), Interventionen bei Gewalt- und Sexualstraftätern: Risk-Management, Methoden und Konzepte der forensischen Therapie (pp. 255–276). Berlin: Medizinisch Wissenschaftliche Verlagsgesellschaft.
- Elbert, T., Schauer, M., & Moran, J. K. (2018). Two pedals drive the bi-cycle of violence: Reactive and appetitive aggression. Current Opinion in Psychology, 19, 135–138. doi:10.1016/j.copsyc.2017.03.016
- Elbert, T., & Schauer, M. (2002). Psychological trauma: Burnt into memory. Nature, 419(6910), 883–883. doi:10.1038/419883a
- Elbert, T., Weierstall, R., & Schauer, M. (2010). Fascination violence: On mind and brain of man hunters. European Archives of Psychiatry and Clinical Neuroscience, 260(2), 100–105. doi:10.1007/s00406-010-0144-8
- Festinger, L. (1957). A theory of cognitive dissonance (Vol. 2). Stanford, Californien: Stanford university press.
- Foa, E. B., Molnar, C., & Cashman, L. (1995). Change in rape narratives during exposure therapy for posttraumatic stress disorder. Journal of Traumatic Stress, 8(4), 675–690. doi:10.1002/jts.2490080409
- Foa, E. B., Steketee, G., & Rothbaum, B. O. (1989). Behavioral/cognitive conceptualizations of post-traumatic stress disorder. Behavior Therapy, 20(2), 155–176. doi:10.1016/S0005-7894(89)80067-X
- Golden, S. A., Jin, M., & Shaham, Y. (2019). Animal models of (or for) aggression reward, addiction, and relapse: Behavior and circuits. Journal of Neuroscience, 39(21), 3996–4008. doi:10.1523/JNEUROSCI.0151-19.2019
- Hirst, W., & Coman, A. (2018). Building a collective memory: The case for collective forgetting. Current Opinion in Psychology, 23, 88–92. doi:10.1016/j.copsyc.2018.02.002
- Hirst, W., & Echterhoff, G. (2012). Remembering in conversations: The social sharing and reshaping of memories. Annual Review of Psychology, 63, 55–79. doi:10.1146/annurev-psych-120710-100340
- Hirst, W., Yamashiro, J. K., & Coman, A. (2018). Collective memory from a psychological perspective. Trends in Cognitive Sciences, 22(5), 438–451. doi:10.1016/j.tics.2018.02.010
- Köbach, A., Schaal, S., & Elbert, T. (2015). Combat high or traumatic stress: Violent offending is associated with appetitive aggression but not with symptoms of traumatic stress. Frontiers in Psychology, 5, 1518 https://doi.org/10.3389/fpsyg.2014.01518.
- Koebach, A., Carleial, S., Elbert, T., Schmitt, S., & Robjant, K. (2021). Treating trauma and aggression with Narrative Exposure Therapy in former child and adult soldiers: A randomised controlled trial in Eastern DR Congo Journal of Consulting and Clinical Psychology, 89(3), 143–155. https://doi.org/10.1037/ccp0000632 .
- Kubany, E. S., & Watson, S. B. (2003). Guilt: Elaboration of a multidimensional model. Psychological Record, 53(1), 51–90.
- Lerner, M. J. (1980). The belief in a just world: A fundamental delusion. New York: Plenum Press.
- Lerner, M. J. (2003). The justice motive: Where social psychologists found it, how they lost it, and why they may not find it again. Personality and Social Psychology Review, 7(4), 388–399. doi:10.1207/S15327957PSPR0704_10
- Maercker, A., & Horn, A. B. (2013). A socio‐interpersonal perspective on PTSD: The case for environments and interpersonal processes. Clinical Psychology & Psychotherapy, 20(6), 465–481. doi:10.1002/cpp.1805
- Mary, A., Dayan, J., Leone, G., Postel, C., Fraisse, F., Malle, C., … De la Sayette, V. (2020). Resilience after trauma: The role of memory suppression. Science, 367(6479). doi:10.1126/science.aay8477
- McGrath, A. (2017). Dealing with dissonance: A review of cognitive dissonance reduction. Social and Personality Psychology Compass, 11(12), e12362. doi:10.1111/spc3.12362
- Morath, J., Gola, H., Sommershof, A., Hamuni, G., Kolassa, S., Catani, C., … Elbert, T. (2014). The effect of trauma-focused therapy on the altered T cell distribution in individuals with PTSD: Evidence from a randomized controlled trial. Journal of Psychiatric Research, 54, 1–10. doi:10.1016/j.jpsychires.2014.03.016
- Morath, J., Moreno-Villanueva, M., Hamuni, G., Kolassa, S., Ruf-Leuschner, M., Schauer, M., … Kolassa, I.-T. (2014). Effects of psychotherapy on DNA strand break accumulation originating from traumatic stress. Psychotherapy and Psychosomatics, 83(5), 289–297. doi:10.1159/000362739
- Moskowitz, A. K. (2004). Scared stiff”: Catatonia as an evolutionary-based fear response. Psychological Review, 111(4), 984. doi:10.1037/0033-295X.111.4.984
- Müller, M., Ajdacic-Gross, V., Rodgers, S., Kleim, B., Seifritz, E., Vetter, S., … Preisig, M. (2018). Predictors of remission from PTSD symptoms after sexual and non-sexual trauma in the community: A mediated survival-analytic approach. Psychiatry Research, 260, 262–271. doi:10.1016/j.psychres.2017.11.068
- Nandi, C., Elbert, T., Bambonye, M., Weierstall, R., Reichert, M., Zeller, A., & Crombach, A. (2017). Predicting domestic and community violence by soldiers living in a conflict region. Psychological Trauma: Theory, Research, Practice, and Policy, 9(6), 663. doi:10.1037/tra0000262
- Neuner, F., Schauer, M., Klaschik, C., Karunakara, U., & Elbert, T. (2004). A comparison of narrative exposure therapy, supportive counseling, and psychoeducation for treating posttraumatic stress disorder in an African refugee settlement. Journal of Consulting and Clinical Psychology, 72(4), 579. doi:10.1037/0022-006X.72.4.579
- Nickerson, R. S. (1998). Confirmation bias: A ubiquitous phenomenon in many guises. Review of General Psychology, 2(2), 175–220. doi:10.1037/1089-2680.2.2.175
- Orang, T., Ayoughi, S., Moran, J. K., Ghaffari, H., Mostafavi, S., Rasoulian, M., & Elbert, T. (2018). The efficacy of narrative exposure therapy in a sample of Iranian women exposed to ongoing intimate partner violence—a randomized controlled trial. Clinical Psychology & Psychotherapy, 25(6), 827–841. doi:10.1002/cpp.2318
- Peltonen, K., Kangaslampi, S., Saranpää, J., Qouta, S., & Punamäki, R.-L. (2017). Peritraumatic dissociation predicts posttraumatic stress disorder symptoms via dysfunctional trauma-related memory among war-affected children. European Journal of Psychotraumatology, 8(1), 1375828. doi:10.1080/20008198.2017.1375828
- Pennebaker, J. W., & Harber, K. D. (1993). A social stage model of collective coping: The Loma Prieta earthquake and the Persian Gulf War. Journal of Social Issues, 49(4), 125–145. doi:10.1111/j.1540-4560.1993.tb01184.x
- Pinciotti, C. M., & Orcutt, H. K. (2019). It won’t happen to me: An examination of the effectiveness of defensive attribution in rape victim blaming. Violence against Women, 26(10) , 1059–1079. doi:10.1177/1077801219853367.
- Robjant, K., Elbert, T, Schmitt, S., Chibashimba, A., & Koebach, A. (2020 The NETfacts health system: An integrative approach to counter the mental sequelae of trauma and violence at the individual and community level. Maltrattamento e Abuso All'Infanzia: Rivista Interdisciplinare, 22(3), 63–72 https://doi.org/10.3280/MAL2020-003006).
- Robjant, K., Koebach, A., Schmitt, S., Chibashimba, A., Carleial, S., & Elbert, T. (2019). The treatment of posttraumatic stress symptoms and aggression in female former child soldiers using adapted narrative exposure therapy–a RCT in Eastern Democratic Republic Of Congo. Behaviour Research and Therapy, 123, 103482. doi:10.1016/j.brat.2019.103482
- Robjant, K., Schmitt, S., Chibashimba, A., Carleial, S., Elbert, T., & Koebach, A. (2020). Trauma, aggression, and post conflict perpetration of community violence in female former child soldiers—A study in Eastern DR Congo. Frontiers in Psychiatry, 11, 885. doi:10.3389/fpsyt.2020.533357
- Robjant, K., Schmitt, S., Chibashimba, A., Elbert, T., & Koebach, A. (in prep.). Effectiveness of the NETfacts health system: A randomized controlled trial in the Eastern DR Congo.
- Schaal, S., Elbert, T., & Neuner, F. (2009). Narrative exposure therapy versus interpersonal psychotherapy. Psychotherapy and Psychosomatics, 78(5), 298–306. doi:10.1159/000229768
- Schauer, M., & Elbert, T. (2010). Dissociation following traumatic stress. Zeitschrift Für Psychologie/Journal of Psychology, 218, 109–127. doi:10.1027/0044-3409/a000018
- Schauer, M., Neuner, F., & Elbert, T. (2011). Narrative exposure therapy: A short-term treatment for traumatic stress disorders. Göttingen, Germany: Hogrefe Publishing.
- Schauer, M., & Robjant, K. (2018). Commentary on Scheidell et al.(2018): En‐counting adversities; the ‘building blocks’ of psychopathology. Addiction, 113, 57–58. doi:10.1111/add.14067
- Schmitt, S., Robjant, K., Elbert, T., Chibashimba, A., Hoeffler, A., Samuel, C., & Koebach, A. (submitted). Breaking the cycles of violence with narrative exposure: Development and feasibility of a community-based intervention for populations living under continuous threat.
- Schnyder, U., Ehlers, A., Elbert, T., Foa, E. B., Gersons, B. P., Resick, P. A., … Cloitre, M. (2015). Psychotherapies for PTSD: What do they have in common? European Journal of Psychotraumatology, 6(1), 28186. doi:10.3402/ejpt.v6.28186
- Siehl, S., Robjant, K., & Crombach, A. (2020). Systematic review and meta-analyses of the long-term efficacy of narrative exposure therapy for adults, children and perpetrators. Psychotherapy Research, 31(6) , 695–710. doi:10.1080/10503307.2020.1847345.
- Stevens, J. S., & Jovanovic, T. (2019). Role of social cognition in post-traumatic stress disorder: A review and meta-analysis. Genes, Brain and Behavior, 18(1), e12518. doi:10.1111/gbb.12518
- Stone, C. B., Barnier, A. J., Sutton, J., & Hirst, W. (2010). Building consensus about the past: Schema consistency and convergence in socially shared retrieval-induced forgetting. Memory, 18(2), 170–184. doi:10.1080/09658210903159003
- Stone, C. B., Coman, A., Brown, A. D., Koppel, J., & Hirst, W. (2012). Toward a science of silence: The consequences of leaving a memory unsaid. Perspectives on Psychological Science, 7(1), 39–53. doi:10.1177/1745691611427303
- Sznycer, D., Xygalatas, D., Agey, E., Alami, S., An, X.-F., Ananyeva, K. I., … Flores, C. (2018). Cross-cultural invariances in the architecture of shame. Proceedings of the National Academy of Sciences, 115(39), 9702–9707. doi:10.1073/pnas.1805016115
- Vitiello, B., & Stoff, D. M. (1997). Subtypes of aggression and their relevance to child psychiatry. Journal of the American Academy of Child & Adolescent Psychiatry, 36(3), 307–315. doi:10.1097/00004583-199703000-00008
- Walster, E. (1966). Assignment of responsibility for an accident. Journal of Personality and Social Psychology, 3(1), 73. doi:10.1037/h0022733
- Webb, R. T., Antonsen, S., Carr, M. J., Appleby, L., Pedersen, C. B., & Mok, P. L. (2017). Self-harm and violent criminality among young people who experienced trauma-related hospital admission during childhood: A Danish national cohort study. The Lancet Public Health, 2(7), e314–e322. doi:10.1016/S2468-2667(17)30094-4
- Webermann, A. R., Maldonado, A., Singh, R., Torres, S., Bushee, S., & Murphy, C. M. (2020). Centrality of traumatic events and men’s intimate partner violence perpetration. Psychological Trauma: Theory, Research, Practice, and Policy, 12(2), 200–206. doi:10.1037/tra0000497
- Wilker, S., & Kolassa, I.-T. (2013). The formation of a neural fear network in posttraumatic stress disorder: Insights from molecular genetics. Clinical Psychological Science, 1(4), 452–469. doi:10.1177/2167702613479583
- Wilker, S., Pfeiffer, A., Kolassa, S., Koslowski, D., Elbert, T., & Kolassa, I.-T. (2015). How to quantify exposure to traumatic stress? Reliability and predictive validity of measures for cumulative trauma exposure in a post-conflict population. European Journal of Psychotraumatology, 6(1), 28306. doi:10.3402/ejpt.v6.28306