
ABSTRACT
Background
With the development of positive psychology, posttraumatic growth research on cancer patients has attracted increasing attention from researchers. It is immensely important to effectively increase the posttraumatic growth level of cancer patients and improve their quality of life.
Objectives
To investigate the effectiveness of a nurse-led mindfulness-based Tai Chi Chuan (MTCC) programme for increasing posttraumatic growth (PTG) and decreasing the perceived stress and anxiety of breast cancer survivors.
Methods
A RCT was conducted. Participants were randomly assigned to either the MTCC group or the control group. The programme included 59 women with stage I–III breast cancer. Participants in the intervention group participated in a nurse-led 8-week, twice a week, one-hour per day mindfulness-based exercise programme. The effectiveness of the intervention was measured three times (T1 – before intervention; T2 – after intervention; T3 – one year after intervention) using validated scales, including the PTG inventory (PTGI), Perceived Stress Scale (PSS), and Self-rating Anxiety Scale (SAS). A repeated-measure analysis of variance model was used to analyse the data.
Results
Compared with the wait-list control group, the PTG level in the MTCC group was much higher after the 8-week intervention and the follow-up (F = 374.98, P < .000). The results showed that MTCC increased the level of PTG, and the effect persisted 1 year after intervention. In addition, PSS (F = 55.22, P < .000) and SAS (F = 148.92, P < .000) scores were significantly decreased at T2 and T3.
Conclusion
The research preliminarily revealed that the MTCC programme was simple, effective, and more suitable to clinical nurses which should be recommended to cancer survivors to promote their recovery.
HIGHLIGHTS
The posttraumatic growth level of breast cancer survivors may decrease as time goes on.
A nurse-led MTCC programme facilitates significant improvements in the posttraumatic growth level of breast cancer survivors.
Antecedentes: Con el desarrollo de la psicología positiva, la investigación de crecimiento postraumático en pacientes con cáncer ha atraído cada vez más la atención de los investigadores. Es sumamente importante aumentar de manera eficaz el nivel de crecimiento postraumático de los pacientes con cáncer y mejorar su calidad de vida.
Objetivos: Investigar la efectividad de un programa de Tai Chi Chuan basado en mindfulness (MTCC en sus siglas en inglés) dirigido por enfermeras para aumentar el crecimiento postraumático (PTG en sus siglas en inglés) y disminuir la percepción de estrés y ansiedad de las sobrevivientes de cáncer de mama.
Métodos: Se condujo un ECA. Las participantes fueron asignadas al azar al grupo MTCC o al grupo control. El programa incluyó a cincuenta y nueve mujeres con cáncer de mama en estadio I-III. Las participantes en el grupo de intervención participaron en un programa de ejercicios basados en mindfulness dirigido por enfermeras, de 8 semanas, dos veces por semana, de una hora diaria. La efectividad de la intervención se midió tres veces (T1 – antes de la intervención; T2 – después de la intervención; T3 – un año después de la intervención) usando escalas validadas, incluidas el inventario de PTG (PTGI), la Escala de Estrés Percibida (PSS) y la Escala de Ansiedad Auto-reportada (SAS). Para analizar los datos se utilizó un modelo de análisis de varianza de medidas repetidas.
Resultados: En comparación con el grupo control de la lista de espera, el nivel de PTG en el grupo MTCC fue mucho más alto después de intervención de 8 semanas y al seguimiento (F = 374.98, P< 0.000). Los resultados mostraron que la MTCC aumentó los niveles de PTG y el efecto persistió un año después de la intervención. Además, las puntuaciones de PSS (F = 55.22, P< 0.000) y SAS (F = 148.92, P< 0.000) disminuyeron significativamente en T2 y T3.
Conclusiones: Las investigaciones preliminares revelaron que el programa de MTCC era simple, efectivo y más adecuado para las enfermeras clínicas, lo que debería recomendarse a las sobrevivientes de cáncer para promover su recuperación.
研究背景: 随着积极心理学的发展, 关于癌症患者创伤后生长的研究越来越受到研究者的关注。有效提高癌症患者创伤后生长水平, 提高其生活质量具有重要意义
研究目的: 探讨护士主导的正念太极 (MTCC) 计划对乳腺癌幸存者创伤后成长 (PTG)、感知压力和焦虑的有效性
研究方法: 本研究进行了RCT设计。参与者被随机分配到MTCC组或对照组。59名患有I -III期乳腺癌的妇女参加了项目。干预组接受护士指导的8周, 每周2次, 每次1小时的正念训练计划。采用经验证的PTG量表 (PTGI)、感知压力量表 (PSS) 和焦虑自评量表(SAS), 分干预前 (T1)、干预后 (T2) 和干预1年后 (T3) 三次测量干预效果。采用重复测量方差分析模型对数据进行分析
研究结果: MTCC组干预8周及随访后PTG水平明显高于对照组 (F= 374.98, P< .000)。MTCC可提高PTG水平, 且干预1年后效果持续。此外, PSS (F = 55.22, P< .000) 和SAS (F = 148.92, P< .000) 评分在T2和T3时显著降低
1. Introduction
Breast cancer is the most common type of cancer in women. In 2019, a national cancer statistics report showed that breast cancer, continuing to threaten the health and quality of life of women across the world, remains the leading cause of death in women. It is estimated that by 2030, the number of cases of and deaths from breast cancer worldwide will reach 26.4 million and 1.7 million, respectively (Siegel, Miller, Jemal, et al., Citation2017). In China, the incidence rate of breast cancer increases, on average, 3% per year, with 12.2% of new cases and 9.6% of deaths per year (Fan, Strasser-Weippl, Li, et al., Citation2014). In recent years, with early-stage diagnosis and the extensive use of comprehensive treatment methods, breast cancer death rates have decreased dramatically (Azria, Belkacemi, Romieu, et al., Citation2010). Throughout the course of the disease, serious psychological symptoms may result from the patients’ experiences of stress related to the cancer itself, treatment and social issues. Research has suggested that approximately 7%–46% of breast cancer patients are distressed in the early stage of the disease and suffer psychological problems such as stress, anxiety, fear and grief, which affects their quality of life (Hoffman, Ersser, Hopkinson, et al., Citation2012).
With the positive psychology research perspective and in-depth study of an effective psychological intervention method for breast cancer, scholars found that individuals will, as a result of an individual’s struggle after a traumatic event, also produce positive psychology changes, which is defined by Tedeschi and Calhoun (Tedeschi, Calhoun, Citation1996) as posttraumatic growth (PTG). PTG can help cancer patients pay closer attention to positive emotions, the value of human life, and improving their mental health conditions and quality of life, while also strengthening patients’ confidence in fighting the disease and increasing their compliance to improving the treatment and rehabilitation of diseases. Breast cancer is a malignant disease among women that has the highest risk of psychological stress. Exploring the potential of positive psychology and providing effective intervention is important to improving the quality of life of breast cancer survivors.
Since 1970, an increasing number of psychologists and practitioners have begun to pay attention to the practice of mindfulness, a method of mind regulation that originated in Buddhist meditation (Crane, Brewer, Feldman, et al, Citation2017). The practice of mindfulness awakens the internal mindfulness of the body through meditation and escorts it into a state of awareness of the physical and mental experience that occurs without any subjective comments (Kenne Sarenmalm, Martensson, Andersson, Karlsson, & Bergh, Citation2017). Mindfulness training plays an active role in reducing stress and anxiety and enhancing subjective well-being. With the in-depth study of mindfulness training, an increasing number of treatment methods, known as ‘third-generation cognitive behavioral therapy’, have been applied (Kabat-Zinn, Citation1982). The effects of mindfulness training have been researched in breast cancer patients, showing improvements to negative emotions after intervention (Huang, Shi, Citation2016). However, some qualitative studies on mindfulness interventions in cancer patients have shown that the traditional mindfulness project has difficulty grasping core intervention components and, therefore, requires a long time to integrate into the world of mindfulness (Schellekens, Jansen, Willemse, et al., Citation2016; Zainal, Booth, & Huppert, Citation2013). Due to limited physical condition or difficulty grasping the core skills, many people suspend or quit psychological treatment in the final period. The best way to implement a psychological intervention to improve psychological health is to allow the individual to gradually apply and integrate techniques into their life. Therefore, a mindfulness programme that is feasible for breast cancer survivors and suitable for clinical nurses is needed to promote their psychological health.
Tai Chi Chuan is a traditional, globally practiced, conditioning exercise that integrates breath movement into body movement. It enhances muscle strength through a series of gentle movements, improves fatigue and psychological sleep problems, and has a significant effect on the postoperative recovery of breast cancer patients (Reid-Amdt, Matsuda, & Cox, Citation2012). At present, the latest guidelines and standards for the diagnosis and treatment of breast cancer in China have recommended Tai Chi Chuan as one of the aerobic exercises that can continue long term after surgery (Fong et al., Citation2013). At present, the latest guidelines and standards for the diagnosis and treatment of breast cancer in China have recommended Tai Chi Chuan as one of the aerobic exercises that can be practiced for a long time after the operation on breast cancer patients (Lan, Chen, Lai, & Wong, Citation2013).
The core mechanism of mindfulness therapy is consistent with the principle of Tai Chi, which emphasizes the unity of mind and body and the core position of mind in both.
To the best of our knowledge, no researchers have combined mindfulness skills with Tai Chi Chuan to establish a mixed programme to apply to clinical cancer patients. Therefore, this study aimed to combine psychology (mindfulness) and exercise (Tai Chi Chuan) interventions and designed an RCT comprising a nurse-led mindfulness-based Tai Chi (MTCC) programme to evaluate its effects on the psychological health of breast cancer survivors, including anxiety and depression, and the PTG level. We hypothesized that the participants in the intervention group would experience long term and significantly increased levels of PTG. In addition, the MTCC programme reduced the perceived stress and anxiety of breast cancer survivors.
2. Methods
This study was a randomized controlled trial. We recruited patients by putting up posters in hospitals. Participants who met the criteria completed baseline assessments to gather demographic and health history information, as well as various other measures; they were then randomized to an eight-week, twice-per-week mindfulness-based Tai Chi Chuan (MTCC) group or a wait-list control group. When the study was completed, the waitlist control group participated in the same programme. Randomization was computer-generated and kept in sequentially numbered opaque sealed envelopes to prevent bias in intervention group allocation. To minimize potential bias, we solicited the help of a trained assistant who was blinded to the entire study process to help collect anonymous data.
2.1. Sample and setting
Breast cancer survivors diagnosed with stage I–III breast cancer who had completed chemotherapy and/or radiation therapy less than one year prior were eligible to participate in this study. All participants were recruited from the breast surgery department at the fifth hospital affiliated with Harbin Medical University from January 2018 to June 2018. The sample size was calculated using the G*POWER version 3.1 program. From related data (Zainal et al., Citation2013), we set a power (1-β) of 0.80 in the t-test, a significance level of 0.05, an effect size (d) of 0.796 and a total sample size of 52. Finally, we recruited 59 patients with a 15% possibility of dropping out rate.
The study coordinator screened potential participants via telephone for eligibility criteria, which were as follows:
Older than 18 at the time of diagnosis
Female breast cancer under recovery
Willing to travel to the study site 2 days per week
Without other major physical illness or mental disorder
Not currently doing the similar intervention such as yoga or meditation.
Able to do moderate intensity exercise
Agree to join and get informed consent.
2.2. Ethical considerations
All procedures performed in this study were in accordance with the ethical standards of Harbin Medical University for the protection of human participants. Each participant was informed the aims and details of the research and written consent was completed by all participants. The clinical registered number: ChiCTR-IOR-16007713.
2.3. Intervention
Participants assigned to the MTCC groups received 8 weeks of mindfulness-based Tai Chi Chuan programmes twice per week. The MTCC programme combined mindfulness skills with 24 simplified Tai Chi Chuan short forms (shown in attachment) by a qualified psychological expert who has been engaged in MBSR treatment for 7 years and a national sports expert who taught Tai Chi Chuan for 12 years. Based on traditional mindfulness skills, the programme was designed according to the characteristics of breast cancer survivors, which emphasized instruction on applying formal techniques such as meditation to Tai Chi Chuan exercise. The core of the programme is to maintain the attitude of ‘mindfulness’ while exercising.
We selected clinical nurses who has the psychological consultant qualification and willing to participate in the research. Oncology nurses from the wards were excluded to avoid contamination. Finally, two clinical nurses who are not bedside nurses were trained by the psychologist who is skilled at mindfulness skills for 10 years and conducted the intervention for participants. Moreover, the nurses should complete the Tai Chi Chuan training to grasp the core skills. In order to avoid the bias, two nurses received the same training by the psychologist and the PE teacher.
The nurses who completed the programme intervention and were able to teach easily conducted the programme at the demonstration classroom of the breast cancer department. The participants in the MTCC group were divided into four groups with seven or eight people in each group. Each group participated in 8 weeks, twice a week, one hour per day training sessions. The programme consisted of two elements: theoretical direction and practice training. More details of each session were as follows ():
Table 1. A detailed intervention scheme
In the follow-up period, due to participants having grasped the intervention, nurses recorded and guided the participants to continue personalized training. If they met any problems, they could contact the nurses freely.
Wait-list control group
Participants in this group only received relevant health information about the recovery of breast cancer. After completion of the study, participants in the wait-list control group participated in the same MTCC programme.
2.4. Assessment of outcomes
Demographic and clinical information
The demographic and clinical data included age, educational level, residence, employment, monthly household income, marital status, religion, TNM stage, type of treatment and time since completion of treatment.
2.4.1 Posttraumatic growth (PTG) level
The PTG level was measured using the Posttraumatic Growth Inventory-Chinese version (PTGI). The PTGI is a 21-item self-report measure yielding a total score of 0–105, with higher scores indicating better PTG levels. The questionnaire consists of new possibilities, personal strength, relating to others, appreciation of life and spiritual change subscales. Dong et al. translated the Chinese version of the PTGI, and it has been proven to have high reliability and validity (Dong, Yan, Guohui, & Jialing, Citation2013). The scale has a Cronbach’s α of 0.927 (total PTGI).
2.4.2. Perceived stress level
The Perceived Stress Scale (PSS) has been commonly used to assess individuals’ perceived stress levels in China. It contained 14 items, each of which was rated on a 5-point Likert scale ranging from 0 to 4, and the total score ranged from 0 to 56 (Yang, Wu, Zhang, Cottrell, & Rockett, Citation2012). Higher scores indicated a high level of perceived stress. The scale has been proven to have good reliability and validity (Cohen, Kamarack, & Mermelstein, Citation1983).
2.4.3. Anxiety level
The Self-rating Anxiety Scale (SAS) was designed by Zung and used in this study to measure degree of anxiety and its changes during treatment. The scale has become one of the most used psychological measurement tools in the clinic. The SAS has 20 items, and each item is rated on a 4-point Likert scale ranging from 1 to 4, with higher scores reflecting higher levels of anxiety. In our study, we set a revised Chinese version of the scale as a rating standard, that is, a score of 50 represents normal, 50–59 represents mild anxiety, 60–69 represents moderate anxiety and ≥70 represents severe anxiety. The scale has a Cronbach’s α of .931 (Wu, Citation1999).
2.5. Data collection procedures
All participants need to accomplish their questionnaires at three times (T1 – the initial baseline orientation the day before the modified MTCC programme started, T2 – the day after the 8-week programme completed, T3 – follow up period that one year after T2).
2.6. Statistical analyses
All collecting data was analysed using IBM SPSS 24.0 (IBM Corp, Armonk, NY). Baseline comparisons between the MTCC group and wait-list control group were performed using independent samples t tests or chi-square analyses. Continuous variables such as age was presented as mean ± standard deviation. Repeated-measures analysis of variance was conducted to compare changes in PTG, stress and anxiety between two groups at postintervention, controlling for the baseline value of the specific outcome. Statistical significance was set at p < .05.
3. Results
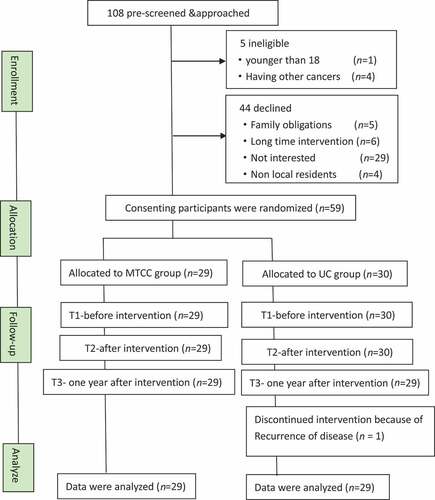
The baseline demographics and medical characteristics of all 59 participants who enrolled in the study and those randomized to the MTCC intervention group or wait-list control group are displayed in . All participants had completed active treatment (surgery, radiation therapy, chemotherapy). One participant in the MTCC group was eliminated prior to follow-up at T3 because of the recurrence of disease (see ).
Table 2. Comparison of demographic and clinical characteristics of two groups (n = 58)
Figure 1. Study flow diagram: enrolment to analysis.
3.1. Posttraumatic growth (PTG), perceived stress and anxiety
The changes in PTG, stress and anxiety between the two groups over time are shown in . For PTGI, the results revealed a significant group and time interaction effect (F = 374.98, p < .01, η2 = 0.11). Over time, the PTG level improved significantly in the MTCC group at T2 and T3, while the PTGI scores in the waitlist group decreased at T3. In addition, the interaction effect of PSS (F = 155.22, p < .01, η2 = 0.03) and SAS (F = 148.92, p < .01, η2 = 0.05) was also obvious. There were no statistically significant changes in stress or anxiety in the wait-list control group.
Table 3. Comparison of two groups on PSS, SAS and PTG
4. Discussion
This study design is the first RCT to apply an MTCC programme to PTG levels and negative emotions in breast cancer survivors to evaluate the effects on their psychological health over one year. The effects of the MTCC programme on participants have shown an increase in PTG levels and a decrease in stress and anxiety levels. Although researchers have been studying mindfulness training for decades, modifications and tailored interventions for different populations are noncontinuous, especially in cancer survivors. Mindfulness-based psychological interventions, such as mindfulness-based stress reduction and mindfulness-based cognitive therapy, warrants specialized skills that clinical nurses have difficulty understanding in a short time. Therefore, this study was designed to integrate a mindfulness core component into local exercise (Tai Chi Chuan) to improve feasibility and compliance. The results revealed that a programme implemented by nurses has a positive effect on the compliance of patients. A total of 96.55% of participants in the MTCC group completed the 16 session programme, and only one participant discontinued because of the recurrence of disease.
Breast cancer survivors suffer from side effects, physiological, psychological, and social pressures, such as shoulder joint dysfunction, upper limb lymphoedema and changes in body image, during their disease trajectory and recovery state (Sprod et al., Citation2012). Influenced by Chinese cultural values, most people who suffer psychological distress experience a decrease in their quality of life because they refuse to receive help from counselling or clinical psychotherapy. Studies have shown that breast cancer survivors with higher PTG could, with a positive illness perception, face the disease directly and effectively cope with stress and produce active emotions throughout the trajectory. These active changes could not only give more hope to overcome illness but could also alter the perception of cancer and encourage patients to undergo relevant treatment (Chen et al., Citation2019). PTG often occurred shortly after a stressful event. Romeo (Romeo et al., Citation2017) found that, as with the results of Groarke (Groarke et al., Citation2017), the PTG of patients with breast cancer occurred within 2 months of diagnosis. As treatment progresses, the PTG level of patients with breast cancer increases, and effective interventions can significantly increase the level of PTG in breast cancer survivors. The results showed that the efficacy of the MTCC programme on the PTG level of breast cancer survivors lasted for 1 year, while the PTG level of participants in the waitlist control group decreased in the follow-up period. In line with most studies (Schell, Monsef, Weckel, & Skoetz, Citation2019; Henderson et al., Citation2012) that suggest that mindfulness is beneficial to the psychological health of breast cancer survivors, the results also revealed the positive impacts of a modified mindfulness programme on negative emotions.
Mindfulness skills have been commonly used in the psychotherapy field, and associated formal systems and guidelines have been gradually established and recommended for promoting health for different worldwide populations (Fletcher, Citation2010; Siegel, Citation2007). For patients with breast cancer in recovery, this methodical and skilled method was difficult to grasp in a short time, and they could terminate their participation in the intervention due to time constraints and trafficking. In our research, a nurse-led eight-week MTCC programme, according to breast cancer characteristics, was designed to be applied to breast cancer survivors. In our study, the results showed that the level of PTG in the MTCC group increased with a mean of 59.94 ± 3.19 points at T2 and a mean of 68.45 ± 5.00 points at T3. The effects were significant and lasted for 1 year. Compared with traditional mindfulness interventions, the MTCC programme combined mindfulness skills with Tai Chi Chuan, which was easily accepted by participants and for mindfulness cultivation. Previous studies reported that when participants underwent a 2-hour or 2.5-hour mindfulness training, it was difficult for them to be clear and focused, and that they were always met with problems such as sleepiness, tiredness or disturbances (Yu & Zhang, Citation2013). In our study, we reduced the training time and modified the content to establish a psychology-exercise intervention to ensure feasibility. Through mindful exercise, participants could peacefully deal with emotions and keep a mild attitude towards stress, respecting things or events without judgement or feelings. We aim to let participants gradually grasp the basic forms of mindfulness skills through practice to cultivate mindfulness in life.
This study reinforces the findings of previous studies that mindfulness is an effective method for decreasing stress and anxiety (Henderson et al., Citation2012). The results showed that the MTCC group participants significantly alleviated stress and anxiety compared with the waitlist group. The practice of mindfulness helps patients develop a natural, nonjudgmental state, leads them to receive mental activities peacefully and without discrimination and encourages them to live in harmony with the flow of mental activities. Farb N.A. indicated that mindfulness practice can strengthen the prefrontal cortex in the rhesus brain region, which is positively related to mood and emotion regulation (Nakamura, Tawatsuji, Fang, & Matsui, Citation2021). Participants in the intervention group were provided with effective mindfulness skills in daily life to maintain a positive attitude. Through continuous mindfulness training, participants grasp the core concepts of training to integrate into their lives and gradually establish positive attitudes on stressful events. At the same time, Tai Chi Chuan (TCC) is an aerobic exercise that emphasizes the organic combination of mind and body training and is a perfect long-term exercise for breast cancer survivors after surgery (Pan et al., Citation2015). Previous studies showed that TCC had obvious advantages in comparison with traditional rehabilitation methods (Luo et al., Citation2020; Galantino, Callens, Cardena, Piela, & Mao, Citation2013;. Yao, Ge, & Yu et al., Citation2021). First, TCC can utilize a flexible choice of exercise site and does not need any special equipment. Participants can exercise at anytime and anywhere to objectively ensure the continuity of intervention. Second, TCC is a low-cost, low-tech, low-intensity exercise that is easy to learn and practical in the clinic. Third, conducive to the postoperative recovery of breast cancer, participants can adjust the amount of exercise according to their own conditions. Given the limited limb mobility of breast cancer survivors, we adapted mild upper movement to our study. TCC is an entirely dynamic exercise, and when combined with mindfulness skills, the effects of the MTCC programme last for 1 year and promote the psychological health of breast cancer survivors.
4.1. Strengths and limitations
The strengths were the combination of psychology and exercise to form a practical, effectiveness programme that clinic nurses could grasp to apply to breast cancer survivors. The results proved that the MTCC programme was suitable for breast cancer survivors, promoted their PTG level and decreased their stress and anxiety. To the current authors’ knowledge, this is the first RCT implemented to see improvement of MTCC in both PTG and the negative emotions of breast cancer survivors.
Given the advantages of PTG in physical and psychological health for breast cancer patients, health care professionals should address issues related to PTG in breast cancer survivors during transitional survivorship and investigate more effective interventions to support PTG. Overall, the findings from this study will improve nurses’ intervention methods for psychological improvements that may result for breast cancer survivors. The results revealed that the nurse-led MTCC programme significantly improved PTG and decreased negative emotions such as stress and anxiety for one year, and can be used by nurses in clinical or community environments. Hence, further studies could investigate more modified mindfulness programmes according to specific characteristics for different populations. For example, if we aim to apply the mindfulness intervention to children, then the design of the programme should emphasize enjoyment and simpleness.
This study was not without limitations. Due to staffing availability and financial constraints, this study was administered in one hospital. Future studies should recruit more participants from different settings to confirm the effectiveness. In addition, the observation indicators were subjective questionnaires, and future studies should incorporate validated, objective measures to prove its effectiveness. In our study, we only recruit Chinese breast cancer women who are more likely to accept the traditional TCC exercise, and future studies should examine the cultural adaptation for other counties. Moreover, we did not measure the mindfulness level of participants, not measuring the purported mechanisms makes it difficult to illustrate the role of mindfulness on psychological health.
5. Conclusion
Findings from this study provide preliminary data and strengthen the findings from tailored mindfulness-based approaches as an effective modality to promote the psychological health of breast cancer survivors. The results from this randomized controlled trial showed that mindfulness-based Tai Chi Chuan was effective in cultivating PTG levels and reducing the stress and anxiety of breast cancer survivors for 1 year. It is a feasible, operable and easily acceptable intervention for clinic nurses to promote the psychological health of breast cancer patients during recovery.
Data statement
All data generated or used during the study are available from the corresponding author by request. The data are not publicly available due to privacy restrictions.
Acknowledgments
All authors were grateful for all the participants in this study for their corporation.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Azria, D., Belkacemi, Y., Romieu, G., Gourgou, S., Gutowski, M., Zaman, K., … Ozsahin, M. (2010). Concurrent or sequential adjuvant letrozole and radiotherapy after conservative surgery for early-stage breast cancer(CO-HO-RT):a phase 2 randomized trial. The Lancet Oncology, 11(3), 258–10. doi:10.1016/S1470-2045(10)70013-9.
- Chen, H. M., Chen, V. C., Hsiao, H. P., Weng, Y.-P., Hsu, Y.-T., Weng, J.-C., & Chen, Y.-L. (2019). Correlations and correlates of post-traumatic growth and post-traumatic stress symptoms in patients with breast cancer. Neuropsychiatric Disease and Treatment, 15, 3051–3060. doi:10.2147/NDT.S218450.
- Cohen, S., Kamarack, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. doi:10.2307/2136404.
- Crane, R. S., Brewer, J., Feldman, C., Kabat-Zinn, J., Santorelli, S., Williams, J. M. G., & Kuyken, W. (2017). What defines mindfulness-based programs? The warp and the weft. Psychological Medicine, 47(6), 990–999. doi:10.1017/S0033291716003317.
- Dong, L., Yan, H., Guohui, X., & Jialing, H. (2013). Reliability and validity of the Chinese version of post-traumatic growth inventory scale in breast cancer survivors. Journal of Nursing Sciences, 28(22), 21–23 doi:10.3870/hlxzz.2013.22.021.
- Fan, L., Strasser-Weippl, K., Li, J. J., St Louis, J., Finkelstein, D. M., Yu, K.-D., & Goss, P. E. (2014). Breast cancer in China. The Lancet Oncology, 15(7), e279–289. doi:10.1016/S1470-2045(13)70567-9.
- Fletcher, L. B. (2010). Searching for mindfulness in the brain: A process-oriented approach to examining the neural correlates of mindfulness. Mindfulness, l(1), 41–63. doi:10.1007/s12671-010-0006-5.
- Fong, S. S., Ng, S. S., Luk, W. S., Chung, J. W. Y., Chung, L. M. Y., Tsang, W. W. N., & Chow, L. P. Y. (2013). Shoulder mobility, muscular strength, and quality of life in breast cancer survivors with and without Tai Chi Qigong training. Evidence-Based Complementary and Alternative Medicine, 2013, 787169. doi:10.1155/2013/787169.
- Galantino, M. L., Callens, M. L., Cardena, G. J., Piela, N. L., & Mao, J. J. (2013). Tai chi for well-being of breast cancer survivors with aromatase inhibitor-associated arthralgias: A feasibility study. Alternative Therapies in Health and Medicine, 19(6), 38–44.
- Groarke, A., Curtis, R., Groarke, J. M., Hogan, M. J., Gibbons, A., & Kerin, M. (2017). Post-traumatic growth in breast cancer: How and when do distress and stress contribute?Psychooncology. Psycho-oncology, 26(7), 967–974. doi:10.1002/pon.4243.
- Henderson, V. P., Clemow, L., Massion, A., Hurley, T. G., Druker, S., & Hebert, J. R. (2012). The effects of mindfulness-based stress reduction of psychosocial outcomes and quality of life in early-stage breast cancer patients: A randomized trial. Breast Cancer Research and Treatment, 13l(1), 99–109. doi:10.1007/s10549-011-1738-1.
- Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington, J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-based stress reduction in mood, breast- and endocrine-related quality of life, and well-being in stage 0 to III breast cancer: A randomized, controlled trial. Journal of Clinical Oncology, 30(12), 1335. doi:10.1200/JCO.2010.34.0331.
- Huang, J., & Shi, L. (2016). The effectiveness of mindfulness-based stress reduction(MBSR) for survivors of breast cancer: Study protocol for a randomized controlled trial. Trials, 17(1), 209. doi:10.1186/s13063-016-1335-z.
- Kabat-Zinn, J. (1982). An our patient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical consideration and preliminary results. General Hospital Psychiatry, 4(1), 33–47. doi:10.1016/0163-8343(82)90026-3.
- Kenne Sarenmalm, E., Martensson, L. B., Andersson, B. A., Karlsson, P., & Bergh, I. (2017). Mindfulness and its efficacy for psychological and biological responses in women with breast cancer. Cancer Medicine, 6(5), 1108–1122. doi:10.1002/cam4.1052.
- Lan, C., Chen, S. Y., Lai, J. S., & Wong, A. M. K. (2013). Tai chi chuan in medicine and health promotion. Evidence-based Complementary and Alternative Medicine: eCAM, 2013, 502131. doi:10.1155/2013/502131.
- Luo, X. C., Liu, J., Fu, J., Yin, H.-Y., Shen, L., Liu, M.-L., … Tang, Y. (2020). Effect of Tai Chi Chuan in breast cancer patients: A systematic review and meta-analysis. Frontiers in Oncology, 10, 607. doi:10.3389/fonc.2020.00607.
- Nakamura, H., Tawatsuji, Y., Fang, S., & Matsui, T. (2021). Explanation of emotion regulation mechanism of mindfulness using a brain function model. Neural Networks, 138, 198–214. doi:10.1016/j.neunet.2021.01.029.
- Pan, Y., Yang, K., Shi, X., Liang, H., Zhang, F., & Lv, Q. (2015). Tai Chi Chuan exercise for patients with breast cancer: A systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine, 2015, 535237. doi:10.1155/2015/535237.
- Reid-Amdt, S. A., Matsuda, S., & Cox, C. R. (2012). Tai Chi effects on neuropsychological, emotional, and physical functioning following cancer treatment: A pilot study. Complementary Therapies in Clinical Practice, 18(1), 26–30. doi:10.1016/j.ctcp.2011.02.005.
- Romeo, A., Ghiggia, A., Tesio, V., Di Tella, M., Torta, R., & Castelli, L. (2017). Post-traumatic growth, distress and attachment style among women with breast cancer. Journal of Psychosocial Oncology, 35(3), 309–322. doi:10.1080/07347332.2017.1289291.
- Schell, L. K., Monsef, I., Weckel, A., & Skoetz, N. (2019). Mindfulness-based stress reduction for women diagnosed with breast cancer. The Cochrane Database of Systematic Reviews, 3, CD011518. doi:10.1002/14651858.CD011518.pub2.
- Schellekens, M. P., Jansen, E. T., Willemse, H. H., van Laarhoven, H. W. M., Prins, J. B., & Speckens, A. E. M. (2016). A qualitative study on mindfulness-based stress reduction for breast cancer patients: how women experience participating with fellow patients. Supportive Care in Cancer, 24(4), 1813–1820. doi:10.1007/s00520-015-2954-8.
- Siegel, D. J. (2007). The mindful brain: Reflection and attune. New York: Norton Press.
- Siegel, R. L., Miller, K. D., & Jemal, A. (2017). Cancer Statistics. CA: A Cancer Journal for Clinicians, 67(2), 7–30. doi:10.3322/caac.21387.
- Sprod, L. K., Janelsins, M. C., Palesh, O. G., Carroll, J. K., Heckler, C. E., Peppone, L. J., & Mustian, K. M. (2012). Health- related quality of life and biomarkers in breast cancer survivors participating in tai chi chuan. Journal of Cancer Survivorship, 6(2), 146–154. doi:10.1007/s11764-011-0205-7.
- Tedeschi, R. G., & Calhoun, L. G. (1996). The post traumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress, 9(3), 455–471. doi:10.1002/jts.2490090305.
- Wu, W. (1999). Self-rating anxiety scale. Chinese Mental Health Journal, (suppl), 235Y238.
- Yang, T., Wu, D., Zhang, W., Cottrell, R. R., & Rockett, I. R. (2012). Comparative stress levels among residents in three Chinese provincial capitals, 2001 and 2008. PLoS One, 7(11), e48971. doi:10.1371/journal.pone.0048971.
- Yao, Y., Ge, L., Yu, Q. et al. (2021). The effect of Tai Chi Chuan on emotional health: Potential mechanisms and prefrontal cortex hypothesis. Evidence-based Complementary and Alternative Medicine: eCAM, 5, 5549006 doi:10.1155/2021/5549006.
- Yu, Q. Y., & Zhang, H. Z. (2013). On analysis of the psychotherapy based on mindfulness meditation. Medicine and Philosophy, 31(2), 49–51 doi:10.12014/j.issn.1002-0772.2013.15.14. (Chinese).
- Zainal, N. Z., Booth, S., & Huppert, F. A. (2013). The efficacy of mindfulness-based stress reduction on mental health of breast cancer patients: A meta-analysis. Psycho-oncology, 22(7), 1457–1465. doi:10.1002/pon.3171.