
ABSTRACT
Diabetic nephropathy (DN is a dreaded consequence of diabetes mellitus, accounting for about 40% of end-stage renal disease (ESRD). It is responsible for significant morbidity and mortality, both directly by causing ESRD and indirectly by increasing cardiovascular risk. Extensive research in this field has thrown light on multiple pathways that can be pharmacologically targeted, to control or reverse the process of DN. Glomerulocentric approach of DN still continues to produce favourable results as evidenced by the recent data on SGLT-2 (sodium glucose co-transporter type 2) inhibitors. Beyond the glomerular mechanisms, numerous novel pathways have been discovered in the last decade. Some of these pathways target inflammatory and oxidative damage, while the others target more specific mechanisms such as AGE-RAGE (advanced glycation end products-receptors for advanced glycation end products), ASK (apoptotic signal-regulating kinase), and endothelin-associated pathways. As a result of the research, a handful of clinically relevant drugs have made it to the human trials which have been elucidated in the following review, bearing in the mind that there are many more to come over the next few years. Ongoing research is expected to inform the clinicians regarding the use of the newer drugs in DN.
Abbreviations: USFDA: Unites States Food and Drug Administration; SGLT-2: Sodium glucose transporter type 2; GLP-1: Glucagon-like peptide-1; DDP-4: Dipeptidyl peptidase-4; UACR: urinary albumin creatinine ratio; eGFR: Estimated glomerular filtration rate; CKD: Chronic kidney disease; DN: Diabetic nephropathy; TGF: Tubuloglomerular feedback; RAAS: Renin angiotensin aldosterone system; T1DM: Type 1 diabetes mellitus; T2DM: Type 2 diabetes mellitus; RCT: Randomized controlled trial; AGE-RAGE: Advanced glycation end products-receptors for advanced glycation end products; ASK-1: Apoptotic signal-regulating kinase-1; Nrf-2: Nuclear 1 factor [erythroid derived-2]-related factor 2; ml/min/1.73m2: Millilitre/minute/1.73 square meters of body surface area; ~: Approximately.
1. Introduction
Diabetes mellitus is a major cause of morbidity and mortality around the entire world [Citation1]. Kidney disease secondary to diabetes mellitus, termed as diabetic nephropathy (DN), accounts for over 40% of end-stage renal disease (ESRD) [Citation2]. It is also a strong predictor of cardiovascular disease and associated mortality [Citation3]. Among the patients with type 1 diabetes, the prevalence of DN is about 40% [Citation4]. Ten years after the diagnosis of type 2 diabetes, about 25% patients have DN [Citation5]. Worldwide prevalence of diabetes is rapidly increasing, making it one of the most significant contributors to healthcare costs [Citation6].
Mogensen et al. described DN to progress through five stages based on the changes in glomerular filtration rate and urinary albumin excretion [Citation7]. It starts as glomerular hyperfiltration due to hyperglycaemia. Next is the silent stage. This stage is characterized by histological abnormalities without clinical disease. The third stage is the incipient nephropathy stage involving urinary albumin losses (30-300 mg/day) and the fourth stage is characterized by overt proteinuria (>300 mg/day). The fifth stage is end-stage kidney disease requiring renal replacement therapy ().
Table 1. Stages of diabetic nephropathy.
Table 2. Summary of newer and clinically relevant drugs for diabetic nephropathy.
Initial stages of DN are characterized by microalbuminuria, which progresses to overt proteinuria over time. Proteinuria appears to be both the cause and the effect of DN [Citation8]. For over two decades, RAAS (renin angiotensin aldosterone system) blockade has played an important role in delaying the progression of DN via anti-hypertensive and anti-proteinuric effects [Citation9,Citation10]. However, there is emerging evidence on newer drugs that could mitigate deleterious effects of diabetes on renal function. DN has been an extremely active area of pharmacological research in the last decade, and multiple drugs targeting various pathways have been studied with only a few encouraging results [Citation11-Citation13]. This review attempts to summarize some of the newer and clinically significant pharmacotherapy.
2. Pathogenesis of DN
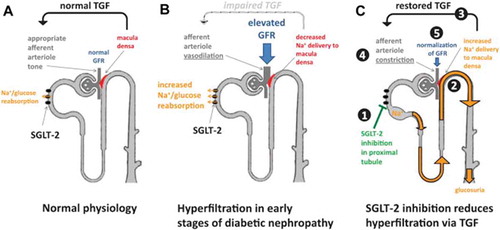
Pathogenesis of DN is a complex and multifactorial process that appears to be a combination of inflammation, oxidative stress, and epigenetic factors [Citation14,Citation15]. However, the role of glomerular hyperfiltration early in the course of diabetes lies at the heart of pathophysiology of DN. Vallon et al., through their single-nephron GFR studies, showed that the dysregulated tubuloglomerular feedback (TGF) in diabetic rats leads to a reduced tone in afferent arteriole which causes glomerular hypertension [Citation16]. Through these experiments, we currently understand that (a) juxta glomerular apparatus fine-tunes the glomerular filtration and is an important homeostatic mechanism that regulates glomerular pressures; (b) adenosine is an important mediator of TGF; and (c) in diabetes, the activity of sodium-glucose transporter (SGLT-2) is increased, leading to an enhanced absorption of sodium in the proximal convoluted tubule. This results in a decreased distal delivery of sodium, which in turn signals TGF mechanism to decrease the afferent arteriolar tone. Ultimately, this leads to glomerular hyperfiltration, thus beginning the pathologic changes of DN.
The mechanism of decreased distal sodium delivery leading to glomerular hyperfiltration was confirmed by the phenomenon called “salt paradox”. In this phenomenon, when rats in early phases of diabetes were salt restricted, they absorbed most of the sodium in the proximal convoluted tubule that lowered the delivery of sodium to the distal convoluted tubule. This decreased local adenosine levels resulting in the dilation of afferent arteriole. We refer readers to Vallon et al. for an excellent review on these mechanisms [Citation16].
3. Therapies
3.1. SGLT-2 inhibitors
Sodium glucose co-transporter-2 inhibitors are a unique class of diabetic agents that have beneficial effects on blood pressures, weight, and arterial stiffness [Citation17-Citation20]. Empagliflozin, dapagliflozin, and canagliflozin are the Unites States Food and Drug Administration-approved agents available in the United States. The renal significance of these drugs comes from their ability to restore a dysregulated TGF. Restoration of this mechanism results in reduced glomerular filtration and glomerulomegaly [Citation21]. explains how the enhanced absorption of sodium proximally leads to a decreased distal sodium delivery, which results in afferent arteriolar vasodilation and glomerulomegaly. When used in this scenario, SGLT-2 inhibitors restore TGF by blocking proximal sodium and glucose absorption. This in turn results in reduced glomerular filtration.
Figure 1. Tubuloglomerular and SGLT-2 inhibitors.
In EMPA-REG OUTCOME trial (empagliflozin cardiovascular event outcome event trial in type 2 diabetes mellitus (T2DM) patients) [Citation22,Citation23], the effect of empagliflozin was studied on cardiac outcomes in patients with T2DM. However, worsening renal end points (defined as progression to macroalbuminuria [UACR to 300mg/gm], doubling of serum creatinine, dialysis, or mortality from renal causes) was one of the secondary outcomes in this study. Out of 7020 subjects studied, 2250 (32%) had chronic kidney disease (CKD) (estimated GFR (eGFR) >60 ml/min and/or UACR >300 mg/gm). Patients were randomized to receive empagliflozin (10 or 25 mg) or placebo along with standard diabetes care. At the end of ~164 weeks, there was a reduction in cardiovascular death, all-cause mortality, and hospitalization in all the study subjects. The risk reduction was similar between patients with and without CKD. Even when the patients were stratified based on the severity of albuminuria (UACR: <30 mg/gm, 30–300 mg/gm and >300 mg/gm), the end-point reduction did not differ significantly.
More importantly, from a renal perspective, renal end points occurred in 12.7% in empagliflozin group versus 18.8% in placebo group. Worsening of albuminuria occurred in 11.2% in treatment group compared to 16.2% in the control group. Doubling of creatinine occurred in 1.5% in the treatment group compared to 2.6% in the control group. All these outcomes reached statistical significance. Despite a better renal outcome in this study, it must be noted that this study was not designed with renal outcomes as primary end point. A larger randomized controlled trial (RCT) targeting renal outcomes is still needed.
Canagliflozin, another SGLT-2, was investigated in an integrated study called CANVAS program. This program in turn consisted of two sister programs, CANVAS (canagliflozin cardiovascular) and CANVAS-R (CANVAS-renal) [Citation24,Citation25]. CANVAS involved 4330 participants and CANVAS-R involved 5812 participants. At the end of follow-up period, the two arms of the trial were jointly analysed to study the outcomes.
CANVAS was geared primarily towards studying cardiac outcomes, and the renal outcomes were secondary. One of the secondary outcomes was progression of albuminuria. The study subjects were followed for ~3.6 years. Primary outcomes (cardiac death, acute coronary, and stroke) were significantly less in the treatment group compared to the control group. Progression of albuminuria occurred less frequently in the treatment group with a hazard ratio of 0.64. Regression of albuminuria occurred more frequently in the treatment group compared to the control group with a corresponding hazard ratio of 1.7. The composite renal outcome (reduction in eGFR <40%, dialysis, death from kidney failure) occurred less frequently in the canagliflozin group.
In another pooled analysis of 11-phase 3 RCTs involving patients with type 2 diabetes, effects of dapagliflozin was analysed on changes in eGFR and UACRs [Citation26]. In this analysis, there were 220 patients with eGFR between 12 and 45 ml/min/1.73m2. At the end 102 weeks of the study period, dapagliflozin 5mg and 10 mg daily reduced UACR by 47.1% and 38.4 %, respectively. No changes in eGFR were noted at the end of study between the two groups.
All the above RCTs established the role of potential nephroprotective ability of SGLT-2 inhibitors even though none of them were designed to study renal outcomes as primary end points. A dedicated RCT to study the effects of SGLT-2 inhibitors on renal outcomes named CREDENCE trial (canagliflozin and renal events in diabetes with established nephropathy clinical evaluation) is currently in process (NCT02065791).
3.2. Incretin-related therapies
Incretin-related therapies include GLP-1 (glucagon-like peptide type 1) analogues and DPP-4 (dipeptidyl peptidase type 4) inhibitors. GLP-1 is a gastrointestinal hormone that enhances insulin secretion and has a pleotropic effect on glucose metabolism. GLP-1 is metabolized and degraded by DPP-4 at proximal convoluted tubules and podocytes [Citation27]. Experiments have shown that insulin resistance in diabetes results from a combination of lower levels of GLP-1 and increased expression of DPP-4.
3.3. GLP-1 agonists
Exenatide, liraglutide, dulaglutide, and albiglutide are the currently available GLP-1 analogues in the drug market. Some of the uncontrolled studies in type 2 diabetes patients with GLP-1 agonists suggested a trend towards improvement in albuminuria which provided the impetus to study the effects of GLP-1 analogues in DN [Citation28,Citation29].
SCALE diabetes trial, an RCT designed to study the benefit of liraglutide on weight reduction, noted that the drug caused a dose-dependent reduction in albuminuria [Citation30].
In another integrated analysis that included nine clinical trials, dulaglutide caused reduction of albuminuria compared to placebo, long-acting glargine insulin, and other diabetic medications. In this study, dulaglutide lowered UACR by 17% compared to placebo which reduced UACR by only 10%. Similarly, dulaglutide reduced UACR by 16.7% compared to glargine, which reduced UACR by only 3.7%. Reduction of albuminuria was statistically significant in both cases. However, there were no significant changes in eGFR over the follow-up period (26–104 weeks) [Citation31].
In another small RCT involving 42 patients, exenatide showed a statistically significant reduction in 24-h urine albumin, urinary TGF-beta1 (transforming growth factor), and type 4 collagen compared to glimepiride [Citation32].
Two RCTs, LEADER [Citation33] and SUSTAIN-6 [Citation34], were designed to study liraglutide and semaglutide, respectively, on cardiac end points in type 2 diabetes. They also included pre-specified composite microvascular outcomes such as worsening of new-onset proteinuria, doubling of serum creatinine, or need for dialysis. However, renal outcomes were secondary again. Lower rate of renal outcomes were noted in both LEADER trial and SUSTAIN-6 trial.
In conclusion, most studies involving GLP-1 analogues show a favourable effect on albuminuria, although none of these trials studied renal end points as primary outcomes. Large RCTs targeting GLP-1 effects on pre-specified primary renal outcomes are required to enhance our understanding regarding the effects of this drug class on DN.
3.4. DPP-4 inhibitors
Among the available DPP-4 inhibitors (linagliptin, saxagliptin, alogliptin, and sitagliptin), linagliptin has been extensively analysed with regard to DN.
LIRA-RENAL RCT was primarily designed to study the effect of liraglutide in lowering glycohaemoglobin in patients with moderate renal impairment (eGFR 30–59 ml/min/1.73m2). At the end of 26 weeks, albuminuria in linaliptin group was 17% lower, although it did not attain statistical significance [Citation35].
MARLINA-T2D trial was designed to investigate linagliptin in patients with T2DM and CKD [Citation36]. This study, which involved 360 participants who were followed over 24 weeks, was also designed to test superiority of linagliptin over placebo in terms of albuminuria. Despite a trend towards reduction in albuminuria, the differences between the study groups were not statistically significant.
In a pooled analysis of 13 phase 2 or 3 RCTs, the effect of linagliptin was studied on renal end points [Citation37]. Primary end points in this study were new onset of moderate albuminuria (UACR > 30−300 mg/gm), new onset of severe elevation in albuminuria (UACR increased to >300 mg/gm from lower values), reduction in kidney function from a baseline value, and halving of eGFR and acute kidney injury (AKI) incidence. Out of 5466 participants, 3505 received linagliptin and the rest received placebo. In this analysis, linagliptin significantly reduced the hazard of the first occurrence of primary event by 16% (HR: 0.84, P=0.02). New-onset moderate elevation in albuminuria was reduced by 18% (HR: 0.82, P=0.03). No difference in decline in eGFR was noted between the two groups.
In SAVOR-TIMI trial, a large RCT with 16,492 participants, the effect of saxagliptin was studied on cardiovascular outcomes with patients of type 2 diabetes. In this study, saxagliptin did not improve cardiovascular outcomes at the end of follow-up period (2.1 years). However, the data was re-analysed for albuminuria. It was noted that irrespective of baseline UACR, treatment with saxagliptin was associated with improvement of albuminuria with P values of 0.021, <0.001, and 0.049 for normo-albuminuria, microalbuminuria, and macroalbuminuria, respectively [Citation38].
DPP-4 inhibitors, like GLP1 agonists, do appear to have a beneficial effect on albuminuria but none of the RCTs above were designed or powered to detect renal outcomes as primary.
At this point, the RCT called CARMELINA trial (composite and renal microvascular outcome study with linagliptin) has recruited 7003 participants to study composite renal end points over 54 months (NCT01897532). The results are much awaited.
3.5. Endothelin receptor antagonists
Data from both human and animal studies suggest that albuminuria is not only a marker of renal disease but also contributes to the progression of kidney disease. There is emerging evidence of role of endothelin in the pathogenesis of proteinuria [Citation39,Citation40]. In addition to this, endothelin also plays a role in the upregulation of inflammation and fibrosis in renal parenchyma [Citation41]. Therefore, endothelin antagonists were hypothesized to improve albuminuria in addition to causing anti-inflammatory and anti-fibrotic effects.
ASCEND, a multicentre RCT, was designed to study the effects of avosentan, an endothelin antagonist, on composite renal outcomes including albuminuria [Citation11]. 1392 subjects were randomized to receive placebo and avosentan 25 mg or 50 mg. The subjects were already on RAAS blockade for the management of DN. Unfortunately, this study had to be terminated prematurely after 4 months due to excessive number of cardiovascular deaths in the avosentan group. However, the treatment group did experience significant reduction of albuminuria. Median reduction of albuminuria was 44.3, 49.3, and 9.7%, respectively, in 25 mg, 50 mg, and placebo groups. Congestive heart failure and fluid retention were the notable adverse effects.
Atrasentan, a highly selective ET-A antagonist, was studied next. Fluid retention was thought to be mediated mainly via ET-B receptor and atrasentan showed less of these side effects in animal models [Citation42,Citation43]. 211 participants were randomized to receive atrasentan 0.75 mg/day, 1.25 mg/day, or placebo and followed for 12 weeks. Compared to placebo, both doses of atrasentan caused at least 35% reduction in UACR. Estimated GFR changes between the groups were not significant. Fluid retention was not noted in the low-dose group, but atrasentan 1.25 mg/day significantly increased the body weight compared to placebo.
Encouraged by this trial, a larger trial was planned. SONAR (NCT01858532), an RCT, had intended to study the effectiveness of atrasentan in DN with primary renal end points. However, the study ended in December 2017 due to futility reasons, as the frequency of end points was occurring at a very low rate, limiting its ability to test the primary hypothesis.
3.6. Mineralocorticoid receptor antagonists (MRA)
Apart from regulating sodium absorption and potassium excretion in the kidney, mineralocorticoid receptor activation is associated with activation of pro-inflammatory, oxidative, and pro-fibrotic pathways in various organ systems [Citation44]. Therefore, the antagonism of mineralocorticoid receptors results in anti-inflammatory, antioxidative, and anti-fibrotic effects. However, steroidal MRAs such as eplerenone and spironolactone, when added to ACE-I or ARB, often result in severe hyperkalemia [Citation45,Citation46]. Finerenone, a novel nonsteroidal MRA, despite having more selectivity towards mineralocorticoid receptors, caused lower incidence of hyperkalemia in earlier trials [Citation47,Citation48]. Lower incidence of hyperkalemia by finerenone is due to its characteristic tissue distribution. Older MRAs cause more hyperkalemia by accumulating three- to sixfold higher in kidney when compared to newer drugs such as finerenone [Citation49].
ARTS-DN was a randomized trial designed to test the efficacy and safety of finerenone in patients with DN and persistent albuminuria. Participants in this study received oral finerenone 1.25, 2.5, 5, 7.5, 10, 15, and 25 mg/day or placebo. Eight hundred and twenty one patients were randomized and followed for 90 days. Primary outcome was the ratio of UACR at 90 days versus baseline. At the end of the study, the finerenone group had dose-dependent reduction in UACR from the dose of 7.5 mg/day and above. Hyperkalemia was noted in 1.8% of the intervention group and 0% in placebo group. However, eGFR changes did not reach statistical significance in the treatment compared to placebo group [Citation50]. Although this trial determined the effective dose of finerenone, head-to-head comparison with other MRA is needed to study its superiority with respect to changes in albuminuria and hyperkalemia.
3.7. Phosphodiesterase inhibitors
Inflammation is believed to play a key role in progression on DN. Pentoxifylline, a nonspecific phosphodiesterase inhibitor, is known for its anti-inflammatory and anti-fibrotic properties in experimental models [Citation51,Citation52].
PREDIAN trial was designed to test if pentoxifylline would benefit patients with DN. In this study, 169 patients with eGFR < 60 ml/min/1.73m2 were optimized on RAAS blockers and randomized to receive pentoxifylline or placebo. Study subjects were followed for a duration of ~1 year [Citation53]. At the end of the study period, eGFR in the treatment group decreased by 2 ml/min/1.73m2 compared to 6.5 ml/min/1.73m2 in the control group (P<0.001). Percent change in UACR in treatment group was −14.9% in the treatment group compared to +5.7% in the control group (P=0.001). This study therefore concluded by saying that pentoxifylline could slow the progression of DN in advanced CKD. However, there were two major drawbacks limiting the generalizability of this trial. All the study participants were Caucasian, and the follow-up duration was short.
3.8. Xanthine oxidase inhibitors
Prospective data are available to implicate uric acid levels as a risk factor in rapid decline of eGFR and development of macroalbuminuria in type 2 diabetes. Multiple cohort studies suggest that elevated uric acid levels are associated with faster progression of diabetic kidney disease [Citation54,Citation55]. It was therefore hypothesized that lowering serum uric acid levels can slow the progression of DN. In fact, a smaller randomized trial involving 113 participants showed that allopurinol use may slow the decline in eGFR in DN [Citation56]. Encouraged by the literature and smaller trials, a large RCT, is currently testing allopurinol type 1 diabetic patients to see if this drug slows the progression of renal disease (PERL trial [Citation57]).
3.9. Drugs targeting AGE-RAGE axis
Diabetes mellitus leads to glycosylation and oxidation of proteins, lipids, and various cell surface receptors, leading to the formation of advanced glycosylation end products (AGEs). Several receptors for AGE have been identified which are named RAGE (receptors for AGE). These receptors initiate maladaptive changes by initiating certain intracellular pathways, which disrupt cellular function. Advanced glycation end products-receptors for advanced glycation end products (AGE-RAGE) axis is now recognized to be an important pathway through which diabetes contributes to vascular damage [Citation58].
Pyridoxamine dihydrochloride, a derivative of vitamin B6, is known to inhibit a broad range of mechanisms that are responsible for the formation of AGEs [Citation59]. In a pilot trial (PYR-210), pyridoxamine showed a trend towards improved creatinine in a cohort of patients with DN [Citation60]. Proteinuria differences did not reach statistical significance. However, the pilot was not powered to detect changes in proteinuria.
A larger RCT, PIONEER-CSG-17, is currently in process. This study is designed to study pyridoxamine in DN and plans to study composite renal end points as primary outcomes.
3.10. Antioxidants
Oxidative stress has been proposed as an important mechanism in progression of renal disease. There is emerging evidence to support that reactive oxygen species cause impaired activity of the transcription factor call Nrf-2 (nuclear 1 factor-related factor 2) [Citation61]. A synthetic triterpenoid derivative, bardoxolone methyl, is a potent activator of Nrf-2 that was shown to reduce oxidative stress in rat models [Citation62,Citation63].
BEAM study, a RCT, was designed to study the effect of bardoxolone on CKD patients. In this RCT, 227 patients with CKD (eGFR 20–45 ml/min/1.73m2) were assigned to receive 25,75, or 150 mg of bardoxolone daily versus placebo. At the end of study that lasted 52 weeks, eGFR in the treatment group was significantly higher compared to the placebo group [Citation64]. Encouraged by the results, another larger RCT, BEACON, was designed to test bardoxolone in 2185 patients with type 2 diabetes and stage 4 CKD [Citation65]. Unfortunately, the study was prematurely terminated after 9 months due to higher rate of cardiovascular deaths.
Another oxidative stress pathway mediated by activation of apoptotic signal-regulating kinase-1 (ASK-1) has received attention recently. ASK-1 pathway activation results in downstream activation of terminal kinases, leading to the production of inflammatory chemokines [Citation66,Citation67]. A novel molecule GS-4997 was shown to reduce inflammation in rat models by inhibiting ASK-1 pathway. Currently, an RCT is in process to test this drug in DN with stage 3 and 4 CKD. The primary outcome being studied is change in eGFR and the secondary outcome is change in albuminuria [Citation68]. summarizes the newer and clinically relevant drugs that have been tested for diabetic nephropathy.
4. Conclusion
DN remains a very active field of research with multiple drugs in the research pipeline in both human and animal studies. SGLT-2 inhibitors currently offer more promise than most other drugs under active investigation. This class of drugs is followed by incretin-related therapies which might prove beneficial in management of DN. However, more research and RCTs are needed to support their use in delaying the progression of DN. Strict blood pressure and glycaemic control along with RAAS blockade still remain the standard of care to delay the progression to ESRD. Ongoing research is expected to inform the clinicians regarding the use of the newer drugs in DN.
Disclosure statement
No potential conflict of interest was reported by the author.
Additional information
Funding
References
- Roglic G, Unwin N, Bennett PH, et al. The burden of mortality attributable to diabetes: realistic estimates for the year 2000. Diabetes Care. 2005;28(9):2130–2135.
- Center for Disease Control and Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States. Atlanta (GA): US Department of Health and Human Services, Center for Disease Control and Prevention; 2011. p. 1–12.
- Orchard TJ, Secrest AM, Miller RG, et al. In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetologia. 2010;53(11):2312–2319.
- Andersen AR, Christiansen JS, Deckert T, et al. Diabetic nephropathy in Type 1 (insulin-dependent) diabetes: an epidemiological study. Diabetologia. 1983;25(6):496–501.
- Adler AI, Stevens RJ, Manley SE, et al. Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003;63(1):225–232.
- Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes mellitus–present and future perspectives. Nat Rev Endocrinol. 2011;8(4):228–236.
- Mogensen CE, Christensen CK, Vittinghus E. The stages in diabetic renal disease. With emphasis on the stage of incipient diabetic nephropathy. Diabetes. 1983;32(Suppl 2):64–78.
- Tabaei BP, Al-Kassab AS, Ilag LL, et al. Does microalbuminuria predict diabetic nephropathy? Diabetes Care. 2001;24(9):1560–1566.
- Mann JF, Schmieder RE, McQueen M, et al. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet. 2008;372(9638):547–553.
- Rahman M, Pressel S, Davis BR, et al. Renal outcomes in high-risk hypertensive patients treated with an angiotensin-converting enzyme inhibitor or a calcium channel blocker vs a diuretic: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern Med. 2005;165(8):936–946. 7.
- Mann JF, Green D, Jamerson K, et al. Group AS: avosentan for overt diabetic nephropathy. J Am Soc Nephrol. 2010;21(3):527–535.
- Parving HH, Brenner BM, McMurray JJ, et al. Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med. 2012;367(23):2204–2213.
- Pfeffer MA, Burdmann EA, Chen CY, et al. A trial of darbepoetin alfa in type 2 diabetes and chronic kidney disease. N Engl J Med. 2009;361(21):2019–2032.
- Nguyen DV, Shaw LC. Grant MB: inflammation in the pathogenesis of microvascular complications in diabetes. Front Endocrinol (Lausanne). 2012;3:170.
- Sharma D, Bhattacharya P, Kalia K, et al. Diabetic nephropathy: New insights into established therapeutic paradigms and novel molecular targets. Diabetes Res Clin Pract. 2017;128:91–108.
- Vallon V. Tubuloglomerular feedback and the control of glomerular filtration rate. News Physiol Sci. 2003;18:169–174.
- Cherney DZ, Perkins BA. Sodium-glucose cotransporter 2 inhibition in type 1 diabetes: simultaneous glucose lowering and renal protection? Can J Diabetes. 2014;38(5):356–363.
- Cherney DZ, Perkins BA, Soleymanlou N, et al. The effect of empagliflozin on arterial stiffness and heart rate variability in subjects with uncomplicated type 1 diabetes mellitus. Cardiovasc Diabetol. 2014;13:28.
- Perkins BA, Cherney DZ, Partridge H, et al. Sodium-glucose cotransporter 2 inhibition and glycemic control in type 1 diabetes: results of an 8-week open-label proof-of-concept trial. Diabetes Care. 2014;37(5):1480–1483.
- Stanton RC. Sodium glucose transport 2 (SGLT2) inhibition decreases glomerular hyperfiltration: is there a role for SGLT2 inhibitors in diabetic kidney disease? Circulation. 2014;129(5):542–544.
- Cherney DZ, Perkins BA, Soleymanlou N, et al. Renal hemodynamic effect of sodium-glucose cotransporter 2 inhibition in patients with type 1 diabetes mellitus. Circulation. 2014;129(5):587–597.
- Wanner C, Lachin JM, Inzucchi SE, et al. Empagliflozin and Clinical Outcomes in Patients With Type 2 Diabetes Mellitus, Established Cardiovascular Disease, and Chronic Kidney Disease. Circulation. 2018;137(2):119–129.
- Wanner C, Inzucchi SE, Zinman B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med. 2016;375(18):1801–1802.
- Neal B, Perkovic V, Matthews DR, et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017;377(21):2099.
- Neal B, Perkovic V, Matthews DR, et al. Rationale, design and baseline characteristics of the CANagliflozin cardioVascular Assessment Study-Renal (CANVAS-R): a randomized, placebo-controlled trial. Diabetes Obes Metab. 2017;19(3):387–393.
- Dekkers CCJ, Wheeler DC, Sjostrom CD, et al. Effects of the sodium-glucose co-transporter 2 inhibitor dapagliflozin in patients with type 2 diabetes and Stages 3b-4 chronic kidney disease. Nephrol Dial Transplant. 2018.
- Tonneijck L, Smits MM, van Raalte DH, et al. Incretin-based drugs and renoprotection-is hyperfiltration key? Kidney Int. 2015;87(3):660–661.
- Imamura S, Hirai K, Hirai A. The glucagon-like peptide-1 receptor agonist, liraglutide, attenuates the progression of overt diabetic nephropathy in type 2 diabetic patients. Tohoku J Exp Med. 2013;231(1):57–61.
- Zavattaro M, Caputo M, Sama MT, et al. One-year treatment with liraglutide improved renal function in patients with type 2 diabetes: a pilot prospective study. Endocrine. 2015;50(3):620–626.
- Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the SCALE Diabetes Randomized Clinical Trial. JAMA. 2015;314(7):687–699.
- Muskiet MHA, Tonneijck L, Smits MM, et al. GLP-1 and the kidney: from physiology to pharmacology and outcomes in diabetes. Nat Rev Nephrol. 2017;13(10):605–628.
- Zhang H, Zhang X, Hu C, et al. Exenatide reduces urinary transforming growth factor-beta1 and type IV collagen excretion in patients with type 2 diabetes and microalbuminuria. Kidney Blood Press Res. 2012;35(6):483–488.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016;375(4):311–322.
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844.
- Davies MJ, Bain SC, Atkin SL, et al. Umpierrez GE: efficacy and safety of liraglutide versus placebo as add-on to glucose-lowering therapy in patients with type 2 diabetes and moderate renal impairment (LIRA-RENAL): a randomized clinical trial. Diabetes Care. 2016;39(2):222–230.
- Groop PH, Cooper ME, Perkovic V, et al. Linagliptin and its effects on hyperglycaemia and albuminuria in patients with type 2 diabetes and renal dysfunction: the randomized MARLINA-T2D trial. Diabetes Obes Metab. 2017;19(11):1610–1619.
- Cooper ME, Perkovic V, von Eynatten M, et al. Kidney Disease End Points in a Pooled Analysis of Individual Patient-Level Data From a Large Clinical Trials Program of the Dipeptidyl Peptidase 4 Inhibitor Linagliptin in Type 2 Diabetes. Am J Kidney Dis. 2015;66(3):441–449.
- Mosenzon O, Leibowitz G, Bhatt DL, et al. Effect of saxagliptin on renal outcomes in the SAVOR-TIMI 53 Trial. Diabetes Care. 2017;40(1):69–76.
- Remuzzi G, Benigni A, Remuzzi A. Mechanisms of progression and regression of renal lesions of chronic nephropathies and diabetes. J Clin Invest. 2006;116(2):288–296.
- Hocher B, Schwarz A, Raschack M, et al. Effects of endothelin receptor antagonists on the progression of diabetic nephropathy. Nephron. 2001;87(2):161–169.
- Simonson MS, Ismail-Beigi F. Endothelin-1 increases collagen accumulation in renal mesangial cells by stimulating a chemokine and cytokine autocrine signaling loop. J Biol Chem. 2011;286(13):11003–11008.
- Opgenorth TJ, Adler AL, Calzadilla SV, et al. Pharmacological characterization of A-127722: an orally active and highly potent ETA-selective receptor antagonist. J Pharmacol Exp Ther. 1996;276(2):473–481.
- de Zeeuw D, Coll B, Andress D, et al. The endothelin antagonist atrasentan lowers residual albuminuria in patients with type 2 diabetic nephropathy. J Am Soc Nephrol. 2014;25(5):1083–1093.
- Haller H, Bertram A, Stahl K, et al. Finerenone: a new mineralocorticoid receptor antagonist without hyperkalemia: an opportunity in patients with CKD? Curr Hypertens Rep. 2016;18(5):41.
- Bomback AS, Kshirsagar AV, Amamoo MA, et al. Change in proteinuria after adding aldosterone blockers to ACE inhibitors or angiotensin receptor blockers in CKD: a systematic review. Am J Kidney Dis. 2008;51(2):199–211.
- Epstein M, Williams GH, Weinberger M, et al. Selective aldosterone blockade with eplerenone reduces albuminuria in patients with type 2 diabetes. Clin J Am Soc Nephrol. 2006;1(5):940–951.
- Barfacker L, Kuhl A, Hillisch A, et al. Discovery of BAY 94-8862: a nonsteroidal antagonist of the mineralocorticoid receptor for the treatment of cardiorenal diseases. Chem Med Chem. 2012;7(8):1385–1403.
- Pitt B, Kober L, Ponikowski P, et al. Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: a randomized, double-blind trial. Eur Heart J. 2013;34(31):2453–2463.
- Kolkhof P, Borden SA. Molecular pharmacology of the mineralocorticoid receptor: prospects for novel therapeutics. Mol Cell Endocrinol. 2012;350(2):310–317.
- Bakris GL, Agarwal R, Chan JC, et al. Effect of Finerenone on Albuminuria in Patients With Diabetic Nephropathy: a Randomized Clinical Trial. JAMA. 2015;314(9):884–894.
- Doherty GM, Jensen JC, Alexander HR, et al. Pentoxifylline suppression of tumor necrosis factor gene transcription. Surgery. 1991;110(2):192–198.
- Strutz F, Heeg M, Kochsiek T, et al. Effects of pentoxifylline, pentifylline and gamma-interferon on proliferation, differentiation, and matrix synthesis of human renal fibroblasts. Nephrol Dial Transplant. 2000;15(10):1535–1546.
- Navarro-Gonzalez JF, Mora-Fernandez C, Muros de Fuentes M, et al. Effect of pentoxifylline on renal function and urinary albumin excretion in patients with diabetic kidney disease: the PREDIAN trial. J Am Soc Nephrol. 2015;26(1):220–229.
- Jalal DI, Rivard CJ, Johnson RJ, et al. Serum uric acid levels predict the development of albuminuria over 6 years in patients with type 1 diabetes: findings from the Coronary Artery Calcification in Type 1 Diabetes study. Nephrol Dial Transplant. 2010;25(6):1865–1869.
- Zoppini G, Targher G, Chonchol M, et al. Serum uric acid levels and incident chronic kidney disease in patients with type 2 diabetes and preserved kidney function. Diabetes Care. 2012;35(1):99–104.
- Goicoechea M, de Vinuesa SG, Verdalles U, et al. Effect of allopurinol in chronic kidney disease progression and cardiovascular risk. Clin J Am Soc Nephrol. 2010;5(8):1388–1393.
- Maahs DM, Caramori L, Cherney DZ, et al. Uric acid lowering to prevent kidney function loss in diabetes: the preventing early renal function loss (PERL) allopurinol study. Curr Diab Rep. 2013;13(4):550–559.
- Goldin A, Beckman JA, Schmidt AM, et al. Advanced glycation end products: sparking the development of diabetic vascular injury. Circulation. 2006;114(6):597–605.
- Chetyrkin SV, Zhang W, Hudson BG, et al. Pyridoxamine protects proteins from functional damage by 3-deoxyglucosone: mechanism of action of pyridoxamine. Biochem. 2008;47(3):997–1006.
- Dwyer JP, Greco BA, Umanath K, et al. Pyridoxamine dihydrochloride in diabetic nephropathy (PIONEER-CSG-17): lessons learned from a pilot study. Nephron. 2015;129(1):22–28.
- Ruiz S, Pergola PE, Zager RA, et al. Targeting the transcription factor Nrf2 to ameliorate oxidative stress and inflammation in chronic kidney disease. Kidney Int. 2013;83(6):1029–1041.
- Dinkova-Kostova AT, Liby KT, Stephenson KK, et al. Extremely potent triterpenoid inducers of the phase 2 response: correlations of protection against oxidant and inflammatory stress. Proc Natl Acad Sci U S A. 2005;102(12):4584–4589.
- Yates MS, Tauchi M, Katsuoka F, et al. Pharmacodynamic characterization of chemopreventive triterpenoids as exceptionally potent inducers of Nrf2-regulated genes. Mol Cancer Ther. 2007;6(1):154–162.
- Pergola PE, Raskin P, Toto RD, et al. Bardoxolone methyl and kidney function in CKD with type 2 diabetes. N Engl J Med. 2011;365(4):327–336.
- de Zeeuw D, Akizawa T, Audhya P, et al. Bardoxolone methyl in type 2 diabetes and stage 4 chronic kidney disease. N Engl J Med. 2013;369(26):2492–2503.
- Adhikary L, Chow F, Nikolic-Paterson DJ, et al. Abnormal p38 mitogen-activated protein kinase signalling in human and experimental diabetic nephropathy. Diabetologia. 2004;47(7):1210–1222.
- Nagai H, Noguchi T, Takeda K, et al. Pathophysiological roles of ASK1-MAP kinase signaling pathways. J Biochem Mol Biol. 2007;40(1):1–6.
- Lin JH, Zhang JJ, Lin SL, et al. Design of a phase 2 clinical trial of an ASK1 inhibitor, GS-4997, in patients with diabetic kidney disease. Nephron. 2015;129(1):29–33.