
In response to the Letter to the Editor by Drs. Ong, Swift and Ong [Citation1], we appreciate your feedback on our case report titled ‘Rare cause of gastric outlet obstruction’ [Citation2].
We went over your suggestions and we would like to highlight our reply as outlined below:
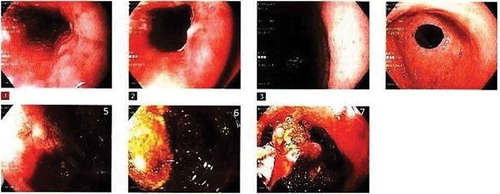
The endoscopic images that are included in our case report shows the stone in the duodenal lumen in . It is an image of the forceps lifting the stone in the duodenal lumen.
Figure 1. CT Abdomen and pelvis on presentation. (a) Marked distention of the stomach with fluid. (b) Pneumobilia involvingleft lobe of liver (pointed with thin arrow). Stone in the duodenal lumen as shown in the image (pointed with thick arrow).

Figure 2. Initial EGD: 1,2 - Reveal LA Grade D esophagitis. 6,7 - Reveal large malignant ulcerated mass with stigmata of bleeding in secondpart of duodenum. 7- Reveal image of forceps lifting the stone in Duodenal lumen.
Similarly, the CT scan in , shows the stone in the duodenal lumen as shown in the attached image (pointed with an arrow.)
Regarding the pathogenesis of Bouveret’s syndrome, we mentioned in our case report that it is caused by the cholecysto-enteric fistula. We agree with your description of dividing the passage of the stone from either cholecysto-gastric, cholecysto-duodenal and choledocho-duodenal. We were unable to visualize the fistula because of the degree of ulceration that was seen on the initial EGD.
The diagnostic approach for our patient was multi modal. The patient underwent CT scan of the abdomen, ERCP, EGD, EUS and PET CT for the diagnostic process. EGD was one modality but initial diagnostic workup was started with imaging. Initial CT scan revealed marked distention of stomach, pneumobilia and poor gall bladder visualization. This was followed by EGD and EUS. PET CT was performed subsequently as suspicion for malignancy was high based on the initial EGD.
We mentioned in our case report that MRCP aids in diagnosis in cases where CT scan is inconclusive (15–25% iso-attenuating stones). We mentioned EGD as a gold standard as it can both be diagnostic (providing direct visualization) and therapeutic but the initial work up will begin with an imaging study.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Ong J, Swift C, Ong S. Bouveret’s syndrome: sense and sensitivity. J Commun Hosp Intern Med Perspect. 2018;8(3):170–171.
- Gandhi S, Jani N. Rare cause of gastric outlet obstruction. J Commun Hosp Intern Med Perspect. 2018;8(2):84–86.