
ABSTRACT
A 63-year-old male with a past medical history of stage 3 chronic kidney disease, type 2 diabetes mellitus, hypertension, and coronary artery disease presented with recurrent symptomatic pleural effusions, low back pain and unintentional weight loss. Labs revealed elevated serum calcium and parathyroid hormone-related peptide, but normal parathyroid hormone, vitamin D, and angiotensin-converting enzyme levels. Malignancy workup was revealing for salt-and-pepper appearance of the bone marrow on MRI of the lumbar spine consistent with multiple myeloma. CT of chest, abdomen, and pelvis was negative for neoplastic process but showed a pleural effusion and calcified granulomas in hilar lymph nodes. Bone marrow biopsy of the lumbar region was subsequently conducted and revealed granulomas confirming the diagnosis of sarcoidosis. Treatment of sarcoidosis resulted in complete resolution of his symptoms and pleural effusion. This case highlights the variable presentation of sarcoidosis and its ability to mimic malignancy. Prompt recognition and treatment is essential in avoiding unnecessary costs and harm to the patient.
1. Introduction
Sarcoidosis is a multisystem disease that is characterized by the formation of epithelioid and giant cell granulomas without caseous necrosis [Citation1]. The diagnosis of sarcoidosis requires compatible clinical and radiological findings, exclusion of other diseases with similar presentations such as infections or malignancy, and pathological evidence of non-caseating granulomas [Citation1].
We present a case of sarcoidosis that presented with recurrent pleural effusions, unintentional weight loss, low back pain and elevated parathyroid hormone-related peptide.
2. Case Presentation
A 63-year-old male with a past medical history of stage 3 chronic kidney disease, type 2 diabetes mellitus, hypertension, hyperlipidemia, coronary artery disease presented with recurrent symptomatic pleural effusions, low back pain and unintentional weight loss. His lab work revealed serum calcium: 12.7 mg/dL (8.3–10.6 mg/dL), parathyroid hormone (PTH): 6.5 pg/mL (14.0 − 72.0 pg/mL), PTHrP: 4.2 pmol/L (0.0–2.3 pmol/L), 1,25-vitamin D level: 43.8 pg/mL (19.9–79.3 pg/mL) and angiotensin converting enzyme: 60 U/L (9–67 U/L). His erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were 92 mm/Hr (0–20 mm/Hr) and 14.0 mg/L (0.0–5.1 mg/L) respectively.
Given his back pain, unintentional weight loss and hypercalcemia a malignancy workup was undertaken. An MRI lumbar spine showed salt-and-pepper appearance of the bone marrow. The serum kappa to lambda light chain ratio was 1.9 (0.26–1.65), the serum protein electrophoresis showed polyclonal gammopathy and, urine protein electrophoresis was negative for monoclonal bands. Further oncology workup included CT chest, abdomen and pelvis which showed scattered calcified granulomas in the hilar and mediastinal lymph nodes, large left-sided pleural effusion and no evidence of neoplastic process ().
Figure 1. Calcified hilar lymph nodes and a large left-sided pleural effusion seen on CT chest without contrast
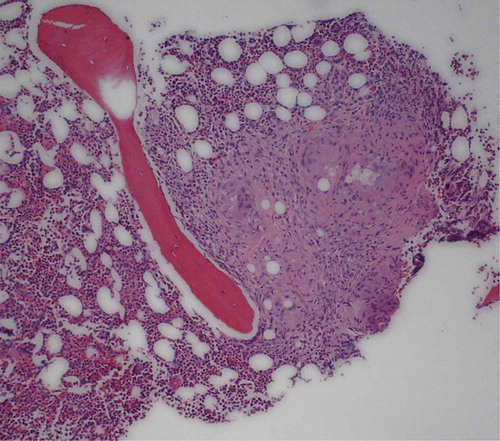
Given the recurrent, large pleural effusions, patient underwent a therapeutic and diagnostic thoracentesis, which was only remarkable for lymphocytic exudate and a significant amount of blood, without any malignant cells on cytology. Recurrence of the pleural effusion prompted a video-assisted thoracoscopic surgery (VATS) procedure with PleurX catheter placement. Finally, he underwent a bone marrow biopsy of his lumbar region which revealed granulomas suggestive of sarcoidosis ().
Figure 2. Bone marrow biopsy of the lumbar spine showing non-caseating granuloma suggestive of sarcoidosis
Patient was started on prednisone 60 mg daily which resulted in a complete resolution of his symptoms and decreased drainage from the PleurX catheter at a 2-week follow up visit.
3. Discussion
Hypercalcemia in sarcoidosis is due to the uncontrolled synthesis of 1,25-dihydroxyvitamin D3 by macrophages [Citation2]. Our patient presented with hypercalcemia and recurrent large pleural effusions. Interestingly, 1,25-dihydroxyvitamin D3 level was normal. Elevated PTHrP and an abnormal MRI prompted a search for a malignancy. Sarcoid involvement of the bone marrow mimicking malignancy and multiple myeloma on MRI has previously been described [Citation3]. Zeimer et al. outlined two cases of sarcoidosis where PTHrP was detected on immunohistochemistry in the granulomas suggesting PTHrP production in small amounts only detectable in the local inflammatory tissue [Citation4]. Multiple inflammatory mediators may stimulate PTHrP expression. However, PTHrP-associated hypercalcemia in sarcoidosis is rare [Citation4,Citation5]. Another unique aspect of our case was the recurrent pleural effusions. Pleural effusions are a rare complication of sarcoidosis. In a study of 181 outpatients with sarcoidosis, 2.8% had pleural effusions, and only 1.1% had sarcoid pleural involvement [Citation6]. A lymphocytic, often blood-stained effusion is highly characteristic of sarcoidosis [Citation7,Citation8], as in our patient. Both hypercalcemia and pleural effusions responded well to steroids.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153–2165.
- Falk S, Kratzsch J, Paschke R, et al. Hypercalcemia as a result of sarcoidosis with normal serum concentrations of vitamin D. Med Sci Monit. 2007 Nov;13(11):CS133–136.
- Mehrotra P, Muller M, Higgins B, et al. An unusual cause of widespread lytic bone lesions caused by sarcoidosis.. Journal of Radiology Case reports. 2011;5(9):1–7.
- Zeimer HJ, Greenaway TM, Slavin J, et al. Parathyroid-hormone-related protein in sarcoidosis.. Am J Pathol. 1998 Jan;152(1):17–21.
- van Raalte DH, Goorden SM, Kemper EA, et al. Sarcoidosis-related hypercalcaemia due to production of parathyroid hormone-related peptide. BMJ Case Rep. 2015 Jul(2015):bcr2015210189
- Huggins JT, Doelken P, Sahn SA, et al. Pleural effusions in a series of 181 outpatients with sarcoidosis. Chest. 2006 Jun;129(6):1599–1604.
- Nicholls AJ, Friend JAR, Legge JS. Sarcoid pleural effusion: three cases and review of the literature.. Thorax. 1980;35(4):277–281.
- Sharma D, Rubenfeld J. Pleural Effusion: an Unusual Complication of Sarcoidosis. Chest. 2014;145(3):269A.