
ABSTRACT
Background
Perianal fistula (PF), a complication of Crohn’s disease (CD), affects health-related quality of life (QOL).
Objective
To elucidate QOL of health states corresponding to different stages of PF associated with CD in Japan.
Method
This cross-sectional, observational, web-based questionnaire survey assessed eight different health states in patients with CD and PF and individuals without CD (non-patients) from the Medilead Healthcare Panel (MHP) and determined the utility values (QOL scores) in each health state by the time trade-off method. In patients, we determined also the utility value of the current health state associated with CD and the PF. The analysis excluded respondents with logical inconsistencies.
Results
The analysis included 82 patients and 576 non-patients with the same sex and age distribution as the Japanese population. In both groups, mean utility values were higher in remission (patients, 0.78; non-patients, 0.51) than in non-remission states, with lowest values for poor prognosis after proctectomy (patients, 0.13; non-patients, −0.10) and highest values for the state with mild symptoms (patients, 0.60; non-patients, 0.30). In patients, the mean utility value of the current health state was 0.71.
Conclusion
QOL decreases with increasing severity of PF and is lower for good prognosis after proctostomy than for remission.
Introduction
Perianal fistula is a complication of Crohn’s disease and occurs in 20% to 50% of patients with the disease [Citation1,Citation2]. It is usually the result of an infection near the anus that causes pus to accumulate in nearby tissues and leads to formation of a small tunnel between the end of the intestine and the skin near the anus. Physical symptoms, such as anal pain and fecal excretion, have been reported to be the most serious for patients [Citation3]. Consequences vary and include fecal incontinence [Citation4] caused by the disease itself or a complication of surgery; recurrence of infection or sepsis [Citation5] psychological problems, such as anxiety and depression [Citation6,Citation7] restriction of sexual activity [Citation3] reduction of pregnancy [Citation8] and restrictions in social interaction and employment [Citation5]. Several studies have evaluated the effects on health-related quality of life (HRQOL, hereafter QOL), and recent overseas studies found that the QOL of patients with Crohn’s disease and a fistula was significantly lower than that of patients with Crohn’s disease without a fistula [Citation9].
The numerical value of people’s health condition (hereinafter referred to as utility value) can be used to quantitatively assess QOL. Utility values are generally defined as values standardized from 0 (death) to 1 (perfect health) and can be acquired by several methods [Citation10,Citation11]. In addition to the profile-type scale used in the above-mentioned study [Citation9], common approaches include indirect methods, such as EuroQOL 5 dimensions (EQ-5D) and Health Utilities Index, and direct methods, such as the standard gamble (SG) and time trade-off (TTO) methods [Citation12–15]. In addition to the utility value in patients, the utility value in participants from the general population (non-patients) is also used in economic evaluations of healthcare technology. In this approach, non-patients are asked to imagine each health state, and their utility value is measured by a direct method. Institutions of health technology assessment in different countries are known to use different methods for economic evaluations [Citation16,Citation17], and it is important to select an appropriate method depending on the country-specific policy.
These methods can be used also to quantitatively evaluate QOL in each health state associated with the various severities of perianal fistula. A study performed in the USA by Arseneau et al. used an SG method to evaluate QOL in patients with Crohn’s disease (including patients with fistula) and healthy individuals [Citation14]. However, it is difficult to confirm the validity of the group’s findings and apply them to studies in Japan because detailed information on the evaluated health states and SG method is not provided. On the other hand, in a study in the UK, Longworth et al. used the TTO method in patients with Crohn’s disease and people from the general population; the group showed participants a description of multiple health states of perianal fistula associated with Crohn’s disease and asked them to imagine each health state and evaluate QOL [Citation15]. To the best of our knowledge, the two studies mentioned above [Citation14,Citation15] are the only ones that have quantitatively evaluated the QOL of different health conditions of perianal fistula associated with Crohn’s disease, and no such study has been performed in Japan. These two studies investigated the utility values in both patients and non-patients. We thought it would be meaningful to clarify the burden of Crohn’s disease in Japan because the development of treatments for perianal fistula associated with Crohn’s disease has been progressing in Japan and the disease burden might vary depending on race or nationality.
The purpose of this study was to evaluate in Japanese patients and non-patients the QOL corresponding to multiple health states defined by the severity of perianal fistula associated with Crohn’s disease and the clinical course after proctostomy, using the same methods as Longworth et al [Citation15].
Materials and methods
Study design
This was a cross-sectional, observational, web-based questionnaire survey of Japanese patients with Crohn’s disease and people from the general population without Crohn’s disease (non-patients). Surveyed participants were people registered in the Medilead Healthcare Panel (MHP) [Citation18–20], which is owned by Medilead, Inc. (Tokyo, Japan). The MHP comprises people in the Japanese general population who have agreed to cooperate in surveys such as questionnaires and interviews. About 4.2 million people are registered in the MHP. When this study was conducted, the MHP included 419 people who reported that they had visited a medical institution for Crohn’s disease in the past. The study endpoints were the utility values for eight types of health state related to perianal fistula associated with Crohn’s disease and, in the patient group, for the current health state.
In the study, we presented respondents with descriptions of multiple health states of perianal fistulae associated with Crohn’s disease and recorded their QOL assessments. The descriptions were Japanese translations of the descriptions of eight health states used in the above-mentioned study performed in the UK [Citation15]. The descriptions were translated by two independent translators, and the translated versions were compared; any inconsistencies between the translations were discussed by an expert in Crohn’s disease (MM) and one in QOL assessment (AI), and the experts chose the version that they considered to be the most appropriate. In addition, bilingual clinical experts in Crohn’s disease and bilingual experts in QOL evaluated the consistency of the Japanese descriptions with the original English text and whether the Japanese expressions correctly described the health states. presents the descriptions of health states used in this study.
Table 1. Descriptions of health states of perianal fistula associated with Crohn’s disease used in the survey.
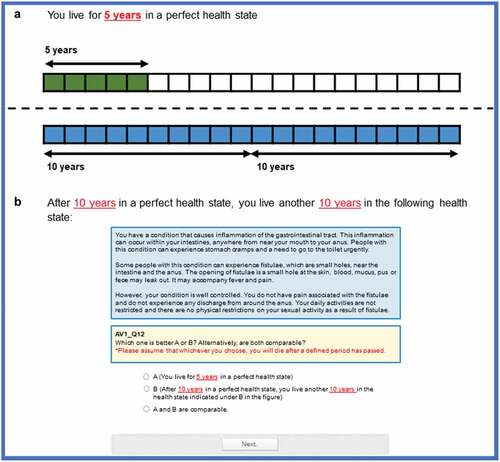
Like the UK study [Citation15], we obtained utility values corresponding to the descriptions of each health state by a composite TTO that combined a conventional TTO and a lead-time TTO. In TTO, a selection-based evaluation method, respondents are presented with a pair of states, one matching perfect health and the other matching disability, and are asked which state they prefer. At that time, respondents are asked to assume that they will stay in each health state for the specified period without receiving relief or treatment, that they have no health problem other than the presented health state, and that death will follow this period. First, we compared 10 years of perfect health state and 10 years of disability state, then 0 years of perfect health state (death) and 10 years of disability state. If respondents answered that the disability state was better than 0 years (death) of the perfect health state, they continued with the conventional TTO, in which they compared several years of the perfect health state, which fluctuated in the range of 0 to 10 years, with 10 years of the disability state (). On the other hand, if they answered that the disability state was worse than 0 years of the perfect health state, they continued with the lead-time TTO, in which they compared several years of the perfect health state, which fluctuated in the range of 0 to 10 years, with 10 years of the disability state after 10 years of the perfect health state (). The number of years of the perfect health state changed on a yearly basis, and the questionnaire continued until a respondent changed their response from the one chosen in the previous question or responded that the perfect health state was the same as the disability state. The resulting utility value ranged from −1.0 to +1.0 in increments of 0.05.
Figure 1. Example of standard time trade-off internet survey screen.
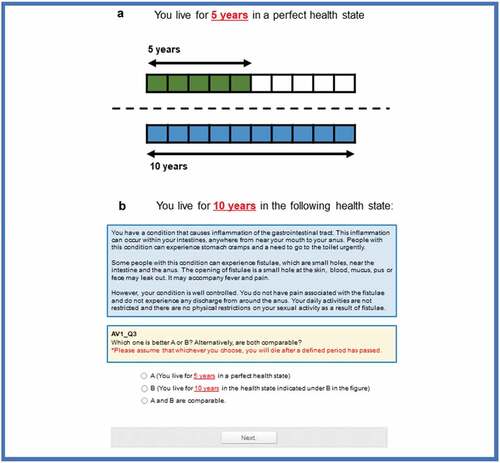
Figure 2. Example of lead-time time trade-off internet survey screen.
To minimize potential bias associated with the order in which the descriptions of health states were presented, respondents were presented the questions on health states #1 to #4 (health states without surgery) in random order, followed by the questions on health states #5 to #8 (health states after surgery) also in random order. In addition, before conducting the TTO survey, we confirmed that respondents properly understood the severity of each health state by first presenting the descriptions #1 to #4 and asking respondents to rank them in order of severity and then doing the same with descriptions #5 to #8.
In addition to the TTO, we also asked about demographic variables (sex, age), current illness, current health state, and the presence or absence of disability. In patients with Crohn’s disease, we asked the respondents whether they had experienced chronic perianal fistula, perianal abscess, or proctostomy. In non-patients, we asked whether they had a patient with Crohn’s disease among their close relatives, such as a family member.
This study was approved by the non-profit organization MINS Research Ethics Committee (MINS-REC-210223).
Study participants
An initial screening survey was conducted to select eligible persons for the composite TTO survey (hereinafter referred to as TTO survey). The screening survey was conducted among Japanese patients who were recorded in the MHP as having Crohn’s disease and Japanese non-patients from the general population; participants were men and women aged 20 years or older. The last part of the screening survey presented a patient information document asking for consent to participate in the study. After confirming that potential participants had fully understood the survey contents, electronic written informed consent was obtained.
In the non-patient group, the number of respondents in each age and sex group was calculated from the composition ratio [Citation21] of Japanese ages by sex. In both the patient and non-patient group, the inclusion criteria for enrollment in the TTO survey were as follows: age 20 years or older at the time of survey; born in Japan; completed the compulsory education in Japan; have lived mostly in Japan in the past 5 years; and provided electronic written informed consent. In the patient group, an additional inclusion criterion was a diagnosis of Crohn’s disease. In the patient group, ulcerative colitis was an exclusion criterion, but people from the general population with ulcerative colitis were not excluded from the non-patient group.
Data cleaning exclusion criteria were established on the basis of the above-mentioned study by Longworth et al [Citation15]. as follows: The assessed utility value was the same for all health states; remission was rated lower than the following health states abscess, defunctioning with negative outcome, or proctectomy with negative outcome; and the response time was less than 5 minutes. The data of respondents who did not meet any of these criteria were considered valid and included in the analysis set.
Statistical analysis
For the endpoints, the response data were summarized separately for the patient group and non-patient group. Summary statistics (mean, SD) were calculated for continuous variables, and ratios for categorical variables.
Furthermore, as an exploratory analysis, the effect of each respondent characteristic on the utility value was examined in a linear mixed model, with the utility value as the objective variable and each background factor and health state as the explanatory variables. At that time, a normal distribution was assumed for the objective variable, and the variability among respondents was considered as a variable intercept because each respondent repeatedly evaluated eight different health states. Results were considered statistically significant if the P-value was less than 0.05.
All analyses were performed with R version 4.1.0.
Results
Respondent characteristics
The flow chart of participant selection is shown in . Among the responses from the 1,227 people who completed the TTO survey, 658 responses from 82 patients and 576 non-patients were valid. The percentage of valid respondents was 74.5% in the patient group and 51.6% in the non-patient group, and non-patients were more likely than patients to be excluded because of data cleaning.
Figure 3. Flow chart of participants.* Total number of Medilead Healthcare Panel registrants. When registering for the panel, a total of 419 people reported that they had visited a medical institution for Crohn’s disease in the past. ** Comprises 419 people registered as having visited a medical institution for Crohn’s disease and 13,190 people randomly selected from the remaining non-Crohn’s disease patients. *** The allocation to the patient or non-patient group was based on the results of the screening survey, not on the information given by people when they registered with the panel. QOL, quality of life; TTO, time trade-off
The background information of the valid respondents in each group is presented in . Compared with the non-patient group, the patient group had a higher proportion of men, people in the age group 40 to 59 years, and people who rated their current health state as poor and answered ‘yes’ to the question whether they had a disability. In the patient group, 7.3% of patients were currently experiencing a chronic perianal fistula and 9.8% a perianal abscess, and 19.5% had undergone proctostomy. Compared with the age and sex of the Japanese general population as of 1 October 2019 [Citation21], the non-patient group had 4.0% fewer men and 4.0% more women and also showed a difference of −0.9% to +1.1% in each age group.
Table 2. Background information of valid responders.
Respondents’ understanding of the severity of each health state
Before conducting the TTO survey, we assessed respondents’ understanding of the severity of each health state by asking them to rank the health states in order of severity. The results are shown in Table S1. Most respondents ranked health state #1, #2, #5, or #7, each of which indicated a relatively good health state, first or second, and #3, #4, #6, or #8, each of which indicated a poor health state, third or fourth. The ranking of the responses tended to be similar in the patient and non-patient groups.
Utility values in each health state in patients and non-patients
The summary results of utility values based on descriptions of eight types of health state are shown in . In both groups, utility values for remission (#1) were higher than for any other state. As the severity increased from remission to abscess (#4), the corresponding utility values decreased. The utility values for defunctioning with positive outcome (#5) and proctectomy with positive outcome (#7) were between those of chronic symptomatic fistulae with mild symptoms (#2) and chronic symptomatic fistulae with severe symptoms (#3), but the values for defunctioning with negative outcome (#6) and proctectomy with negative outcome (#8) were the lowest. In all health states, the utility values of the patient group were higher than those of the non-patient group.
Table 3. Utility values in each health state.
The distributions of utility values were visualized by histograms (Figure S1). In most of the health states, the peaks at the extreme utility values, such as at −1.00, 0.00, +0.95, and +1.00, were observed in both the patient and non-patient groups. The utility values with a large standard deviation in each health state were considered to be mainly caused by these distributions. More respondents in the non-patient group than in the patient group tended to give extreme utility values of −1.00 and 0.00.
Utility values for the actual health state at the time of survey among patients with Crohn’s disease
The summary results of utility values by health state in the patient group at the time of survey are shown in . For chronic perianal fistula, perianal abscess, and proctostomy, the utility values were not markedly different, irrespective of the conditions experienced by patients. The utility value based on the health condition in the overall patient group at the time of survey (0.71 ± 0.48) and the utility value of the sub-population of patients currently experiencing chronic perianal fistula (0.63 ± 0.80) were between the values for remission (#1; 0.78 ± 0.33, see ) and chronic symptomatic fistulae with mild symptoms (#2; 0.60 ± 0.48, see ) and much higher than the value for chronic symptomatic fistulae with severe symptoms (#3; 0.23 ± 0.63, see ). Moreover, the utility value in the sub-population of patients currently experiencing perianal abscess (0.67 ± 0.68) was markedly different from the patient value for the hypothetical health condition abscess (#4; 0.21 ± 0.60, see ).
Table 4. Utility values based on actual health state at the time of the survey of patients with Crohn’s disease.
Factors affecting utility values
The results of the linear mixed model analysis of utility values are presented in . As shown in the table, the P-value for the partial regression coefficient was significant for the non-patient group compared with the patient group and for health states #2 to #8 compared with remission (#1). Thus, the variables ‘Differences between the patient group and the non-patient group’ and ‘Differences in descriptions about the health state’ appeared to affect utility values such that the variable ‘non-patient group’ and each health state from #2 to #8 significantly decreased the utility value compared with ‘patient group’ and health state #1, respectively. Furthermore, the higher the severity of the health state, the larger the decrease in the utility value. Other variables (i.e., sex, age, current health state, presence of own disability) were considered not to have an impact.
Table 5. Results of linear mixed model analysis of utility values.
Discussion
This study evaluated utility values corresponding with multiple health states that were based on the severity of perianal fistula associated with Crohn’s disease and the clinical course after proctostomy in Japan. To the best of our knowledge, it was the first study to perform a quantitative assessment of QOL associated with each state in Japanese patients with Crohn’s disease and the Japanese general population (non-patients). Among the eight health states evaluated in the study, both patients and non-patients rated remission as the state with the highest QOL. Moreover, utility values were lower for poorer health states. Specifically, as the severity increased from remission (#1), to chronic symptomatic fistulae with mild symptoms (#2), chronic symptomatic fistulae with severe symptoms (#3), and abscess (#4), the corresponding utility values decreased. Moreover, utility values for defunctioning with negative outcome (#6) and proctectomy with negative outcome (#8) were lower than those for defunctioning with positive outcome (#5) and proctectomy with positive outcome (#7). Before the assessment of QOL by TTO, we assessed respondents’ understanding of the severity of each health state. The results indicated that the respondents understood the order of severity represented by the descriptions of health states. Furthermore, the order of severity matched the order of mean utility values of each health state well. In addition, the ranking of severity showed that respondents’ understanding of the order of severity was similarly good in the patient and non-patient groups.
As mentioned above, the relative relationship between utility values and the eight types of health state was similar in patients and non-patients. On the other hand, in all eight health states the utility values were lower in non-patients than in patients. The results of the linear mixed model analysis of variables affecting utility values showed that being a non-patient and rating a description of a worse health state resulted in a lower utility value, indicating that these variables have a certain influence on QOL. The result also indicated that being in the non-patient group had a greater influence on QOL than being in the health state chronic symptomatic fistulae with mild symptoms (#2), defunctioning with positive outcome (#5), and proctectomy with positive outcome (#7).
The utility values obtained in this study in Japanese people were comparable to those of the similar study with a similar methodology performed in the UK [Citation15] in that both studies found lower utility values in non-patients and for descriptions of poorer health states. However, in the current study the utility values for any health state were lower in both patients and non-patients than the respective values in the UK study [Citation15], whereby they were markedly lower in non-patients. Overall, the utility values in our study were also lower in any corresponding health state and much lower in non-patients than the values in a US study that used an SG method to evaluate QOL for multiple health states in patients and non-patients [Citation14]. The utility values were similar in both international studies, one of which used TTO [Citation14] and one SG [Citation15]. The fact that the utility values in our study were lower than those in both international studies is considered a unique finding of this study in Japanese people. Moreover, among non-patients in our study who indicated very low utility values, negative mean values were reported for some health states, suggesting that these states were worse than death. In general, non-patients tend to rate QOL lower than patients do. A previous study that assessed QOL by TTO in a general Japanese population found that utility values were rarely negative [Citation22]. Accordingly, it is considered unusual to find such low utility values in Japanese non-patients. We hypothesize that the non-patients in our study might have perceived perianal fistula associated with Crohn’s disease as being more serious than it actually is and that the descriptions might not have accurately reflected the clinical picture. In addition, the proportion of respondents found to have invalid answers during data cleaning was particularly high in the non-patient group, suggesting that some selection bias may have occurred. One explanation may be that the non-patients could not fully understand the description of the health states, resulting in a relatively large number of inconsistencies in their responses. Furthermore, more respondents in the non-patient group than in the patient group tended to give extreme utility values of −1.00 and 0.00. The exclusion criterion for the exclusion of inconsistent answers defined by Longworth et al. might have been insufficient in the Japanese non-patient population, or the non-patient group might have rated the disease condition associated with perianal fistula more seriously than non-patients in the UK did. Even though a Japanese clinical expert confirmed the validity of our Japanese descriptions, the utility values may have been less reliable in the non-patient group than in the patient group. To overcome the limitations discussed above, future studies should perform a preliminary survey to verify respondents’ understanding. Because the utility values were much lower than in the UK study [Citation15], we suggest that further investigation and interpretation is necessary.
As Drummond et al [Citation23]. wrote, it is a topic of discussion whether utility values used for economic assessments of healthcare technology should be obtained from non-patients or patients. Specifically, one study reported that patients who described a state with a stoma as pleasant indicated that the state would be miserable after removal of the stoma [Citation24]. Thus, although obtaining reliable values is necessary for decision-making, it is challenging for health states that are not experienced. Consequently, investigators should decide on a case-by-case basis whether to use patient or non-patient results [Citation23]. Because the reliability of the non-patient utility values in this study is unclear, as discussed above, before using non-patient utility values for economic assessment it may be necessary to evaluate the appropriateness for non-patients of the descriptions of each health state.
In this study, we used two approaches to assess QOL in Japanese patients with Crohn’s disease, i.e., by asking patients to rate the health states after reading descriptions of them and by asking them about their own experience of fistulae and abscesses, and we found differences between the two approaches. Interestingly, in the UK study, similar differences were not seen, and the two utility values were close to each other [Citation15]. The reason for this discrepancy may be that the current health state of the subgroup of patients who answered that they had experienced fistulae or abscesses might not be as serious as the health states in the corresponding descriptions (#3 and #4). However, the study result should be interpreted with caution because of the relatively small number of cases in the subgroup currently experiencing chronic perianal fistula or perianal abscess. Another reason for this discrepancy may be that the descriptions of health states used in this study did not fully reflect the situation of Japanese patients; however, a Japanese clinical expert confirmed the validity of the descriptions of the health states. An additional survey would be needed to determine the validity of each description in Japanese patients and evaluate whether any change in descriptions and methods could improve the accuracy of the results.
In this study, we focused on perianal fistula, one of the complications of Crohn’s disease, and evaluated QOL from both patient and non-patient perspectives. Proctostomy is performed when a fistula is severe and medication or other procedures are not expected to be sufficiently effective. However, compared with the state of remission, this study suggested that QOL after proctostomy is low, even if the postoperative clinical course is good. This finding indicates that a highly effective treatment method is needed that makes it easier to achieve and maintain long-term remission without surgery.
The study has some limitations. We did not conduct an experiment to verify whether the descriptions of health states used by Longworth et al [Citation11]. were valid in the Japanese population. Therefore, the Japanese version of the descriptions of health states used in our study may not have fully reflected the situation of Japanese patients with perianal fistula associated with Crohn’s disease. To ensure comparability of the results, we used the same criteria as Longworth et al. to exclude dishonest or inaccurate respondents from the dataset; however, we did not examine whether the criteria should be modified when applying them to the Japanese population.
Because the questionnaire survey was conducted via the internet, only individuals were selected who had access to a computer or smartphone. As such, there may have been some selection bias.
We did not verify whether the web-based questionnaire survey is applicable as a method for collecting TTO responses in the Japanese population and therefore cannot rule out the possibility that the results contained more bias than those obtained by the face-to-face survey performed by Longworth et al. Furthermore, the chance that some respondents did not fully understand the TTO method may have been higher in the online survey than in the face-to face one, in which an investigator was available to explain every questionnaire item. Response results reflect respondents’ subjective opinions after reading descriptions of a particular health condition and these descriptions may have differed from the physician’s judgment or medical evidence. In addition, recall bias may have affected results.
Because the MHP contained a limited number of patients with Crohn’s disease, we prioritized maximizing the sample size over ensuring the representativeness of the sample and did not match patient demographic distributions with those of the actual population with Crohn’s disease in Japan. Therefore, the representativeness of the patient population is not guaranteed. Non-patients were individuals without Crohn’s disease, but we did not consider the presence or absence of other diseases such as ulcerative colitis in participants. Therefore, people with serious diseases might have been included, although the distribution of answers about the current health state indicated that the overall health condition of the study group was good.
This study performed an exploratory analysis of factors that may influence utility values but some background variables that were not investigated in this study may have influenced the results.
Conclusions
This study quantitatively measured the QOL of eight health conditions based on the severity and postoperative clinical course on perianal fistula associated with Crohn’s disease from the viewpoints of patients with Crohn’s disease and people from the general population in Japan. The results indicate that the higher the severity of the perianal fistula, the lower the corresponding utility value. In addition, the utility value of patients who have undergone proctostomy is lower than that of patients in remission, even if the postoperative clinical course was good.
Supplemental Material
Download Zip (158.5 KB)Acknowledgements
We thank Hisato Deguchi, Akina Takami, and Annabelle Yoon from Takeda Pharmaceutical Company Limited and Tatsuhiro Uenishi and Ayako Shoji from Medilead, Inc. for valuable advice on the planning and execution of the study and the writing of the manuscript.
Disclosure statement
Masafumi Kato is an employee of Takeda Pharmaceutical Company Limited. Mariko Yoneyama-Hirozane was an employee of Takeda Pharmaceutical Company Limited at the time the work was conducted. Katsuhiko Iwasaki was outsourced from Takeda Pharmaceutical Company Limited and is employed by Medilead, Inc. Mao Matsubayashi has received advisory fees from Takeda Pharmaceutical Company Limited. Ataru Igarashi belongs to a department that is sponsored by Takeda Pharmaceutical Company Limited and has received lecture fees. Ataru Igarashi is an advisor to Medilead, Inc. and has received advisory fees from Medilead. The authors report that there are no other conflicts of interest to declare.
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/20016689.2023.2166374
Data availability statement
We have not acquired an agreement from participants of this study for data to be shared publicly, so supporting data are not available.
Additional information
Funding
References
- Bell SJ, Williams AB, Wiesel P, et al. The clinical course of fistulating Crohn’s disease. Aliment Pharmacol Ther. 2003;17(9):1145–11.
- Sciaudone G, Di Stazio C, Limongelli P, et al. Treatment of complex perianal fistulas in Crohn disease: infliximab, surgery or combined approach. Can J Surg. 2010;53(5):299–304.
- Marzo M, Felice C, Pugliese D, et al. Management of perianal fistulas in Crohn’s disease: an up-to-date review. World J Gastroenterol. 2015;21(5):1394–1403. DOI:10.3748/wjg.v21.i5.1394
- de Zoeten EF, Pasternak BA, Mattei P, et al. Diagnosis and treatment of perianal Crohn disease: nASPGHAN clinical report and consensus statement. J Pediatr Gastroenterol Nutr. 2013;57(3):401–412.
- Falconi M, Pederzoli P. The relevance of gastrointestinal fistulae in clinical practice: a review. Gut. 2001;49(Suppl 4):iv2–10.
- Maconi G, Gridavilla D, Vigano C, et al. Perianal disease is associated with psychiatric co-morbidity in Crohn’s disease in remission. Int J Colorectal Dis. 2014;29(10):1285–1290. DOI:10.1007/s00384-014-1935-6
- Mahadev S, Young JM, Selby W, et al. Quality of life in perianal Crohn’s disease: what do patients consider important? Dis Colon Rectum. 2011;54(5):579–585.
- Grouin A, Brochard C, Siproudhis L, et al. Perianal Crohn’s disease results in fewer pregnancies but is not exacerbated by vaginal delivery. Dig Liver Dis. 2015;47(12):1021–1026. DOI:10.1016/j.dld.2015.08.001
- Vollebregt PF, van Bodegraven AA, Markus-DeKwaadsteniet TML, et al. Impacts of perianal disease and faecal incontinence on quality of life and employment in 1092 patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2018;47(9):1253–1260.
- Tosh JC, Longworth LJ, George E. Utility values in National Institute for Health and Clinical Excellence (NICE) technology appraisals. Value Health. 2011;14(1):102–109.
- Longworth L, Rowen D. Mapping to obtain EQ-5D utility values for use in NICE health technology assessments. Value Health. 2013;16(1):202–210.
- Rabin R, de Charro F. EQ-SD: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–343.
- Horsman J, Furlong W, Feeny D, et al. The Health Utilities Index (HUI): concepts, measurement properties and applications. Health Qual Life Outcomes. 2003;1(1):54.
- Arseneau KO, Cohn SM, Cominelli F, et al. Cost-utility of initial medical management for Crohn’s disease perianal fistulae. Gastroenterol. 2001;120(7):1640–1656.
- Longworth L, Fountain D, Singh J, et al. Elicitation of health-related utility in perianal fistula in Crohn’s disease. Patient. 2019 Jun;12(3):339–348. 10.1007/s40271-018-0352-2.
- TLV. Tandvårds- och läkemedelsförmånsverkets allmänna råd. 2017. Accessed 11 Nov 2021. https://www.tlv.se/download/18.467926b615d084471ac3230c/1510316374332/TLVAR_2017_1.pdf.
- NICE. Guide to the methods of technology appraisal. 2013. Accessed 11 Nov 2021. https://www.nice.org.uk/process/pmg9/resources/guide-to-the-methods-of-technology-appraisal-2013-pdf-2007975843781.
- Medilead, Inc. Research panel MHP (Medilead Healthcare Panel). Accessed 11 Nov 2022. https://www.medi-l.com/.
- Yamaguchi H, Iwasaki K, Shoji A, et al. Health‒related Quality of Life (QoL) in Japanese patients with cancer: a large‒scale questionnaire survey using EQ‒5D‒5L. Ther Res. 2020;41(12):949–955.
- Masaki H, Ishizaki S, Uenishi T, et al. A survey of theimpact of COVID‒19 on the visiting frequency of Japanese Patients with gastrointestinal diseases. Jpn Pharmacol Ther. 2021;49(1):17–39.
- Statistics Bureau, Ministry of Internal Affairs and Communications. Population Estimates as of October 1, 2019. Population by Age (Single Years), Sex and Sex ratio – Total population, Japanese population, Table 1: Population by Age (Single Years) and Sex. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00200524&tstat=000000090001&cycle=7&year=20190&month=0&tclass1=000001011679. Accessed 13 Sept 2021.
- Ikeda S, Shiroiwa T, Igarashi A, et al. Developing a Japanese version of the EQ-5D-5L value set. J Natl Inst Public Health. 2015;64:47–55.
- Drummond MF, Sculpher MJ, Claxton K, et al. Methods for the economic evaluation of health care programmes. Oxford, United Kingdom: Oxford University Press; 2015.
- Smith DM, Sherriff RL, Damschroder L, et al. Misremembering colostomies? former patients give lower utility ratings than do current patients. Health Psychol. 2006;25(6):688–695.