
Abstract
The overall aim was to examine participants’ perceptions of a communication course as held for parents of children with profound intellectual and multiple disabilities. The course curriculum included responsive strategies and augmentative and alternative communication. The research questions addressed the favourability, changes in parents’ or children’s communication and appreciated or unappreciated course features. Twenty-two written course evaluations were analysed. The mean scores for ratings were compared with ratings in a previous study, including those of parents of children with generally milder disabilities. Comments and answers to open-ended questions were analysed using thematic analysis. Participants were slightly more satisfied with the course as compared with parents who had children with milder disabilities. The thematic analysis suggested increased parental responsiveness after the course. Perceptions of augmentative and alternative communication varied. It was unclear whether the course altered the children’s communication or not. The supportive social milieu offered by the course was highly appreciated. Although generalisation beyond this course and setting is to be determined, the results suggest that parents of children with profound intellectual and multiple disabilities can appreciate a communication course and find it useful. An individual approach within the group setting and practical learning opportunities seem important.
Introduction
Profound intellectual and multiple disabilities (PIMD) is a term used to describe the combination of profound neuro-motor dysfunction and such profound intellectual disabilities that the exact level of intellectual function is hard to assess with standardized tests (Nakken and Vlaskamp Citation2007). The prevalence of sensory impairments among this group is high, with visual impairments being most common. Additional medical conditions, such as gastrointestinal problems and seizure disorders, are also common (Nakken and Vlaskamp Citation2007, Van der Heide et al. Citation2009). Individuals with PIMD constitute a heterogeneous group in terms of aetiology and diagnosis. Indeed, Nakken and Vlaskamp (Citation2007) suggest that PIMD is best viewed as a continuum. Acknowledging that the boundaries distinguishing PIMD from other conditions are somewhat indistinct, the prevalence of PIMD is suggested to be around 0.025% (Ylvén Citation2015).
Children with PIMD are highly dependent on the support of others when it comes to participating in any routines or activities, including communication. They have a very limited independent ability to use language or symbols in any form and communicate in personal and often inconsistent ways (Wilder Citation2014). Also, the level of awareness of their own (communicative) intentions is expected to be either low or difficult to determine (Grove et al. Citation1999) and they rarely initiate communication (Van Keer et al. Citation2017). For a child with PIMD to successfully interact with another person, that person must know the child’s personality, preferences, behavioural style and every day context (Grove et al. Citation1999, Wilder and Granlund Citation2003, Hostyn and Maes Citation2009). Also, different communicative behaviours from the child with PIMD may be elicited depending on the behaviour of the communication partner. In a study by Nijs et al. (2015) it was found that when children with PIMD interacted with their (typically developing) siblings, the complexity of the communicative behaviour directed towards the (typically developing) sibling increased when the (typically developing) sibling combined both verbal and non-verbal signals to attract their attention. Moreover, the quality of communication may vary for individuals with PIMD based on their health and bodily function, which often change from one day to the next. Their ability to communicate may be negatively affected when their health is unstable (Wilder Citation2014).
Parental responsivity refers to a parent’s sensitivity to their child’s focus of interest and to their giving contingent, prompt responses to his/her signals, activities and focus (Spiker et al. Citation2002). Parental responsivity is considered crucial in the early stages of communication development in typically-developing children (Topping et al. Citation2013) and in the cases of “at risk infants” (Landry et al. Citation2006) and children with diagnosed disabilities (Warren and Brady Citation2007, Van Keer et al. Citation2017). Hostyn and Maes (Citation2009) use the corresponding term sensitive responsiveness when referring to all possible communication partners (not just parents) and considers it to be one of the core principles of successful communication when engaging an individual with PIMD, regardless of their age. Nevertheless, children with disabilities may behave in ways that disrupt responsivity. Behaviours that are commonly observed in children with PIMD and that are reported to have a negative effect on parental responsivity include low initiation rates, slow response time, hypersensitivity to sensory input, atypical eye gaze and stereotypical behaviour (Warren and Brady Citation2007). Van Keer et al. (Citation2017) propose that responsivity should be the primary focus of intervention programmes targeting children with significant cognitive and motor delays.
Research into communication intervention for children with specified PIMD is limited, (Wilder Citation2014) and intervention research that focuses on naturally occurring parent-child communication even more so (Van Keer and Maes Citation2018). Although limited research has been done on the subject, several authors (Branson and Demchak Citation2009, Cress and Marvin Citation2003) suggest that Augmentative and Alternative Communication (AAC) (such as manual signs, tactile symbols, pictures, or speech generating devices) can be used effectively with children with disabilities who are early communicators (i.e. the developmental levels of infants and toddlers). Moreover, AAC intervention has been found to have a positive effect on parental perceptions of language development among toddlers with disabilities (Romski et al. Citation2011). Conversely, Stephenson and Dowrick (Citation2005) suggest that parents of children with severe disabilities may find it especially difficult to functionally apply AAC in everyday communication with a pre-verbal child. Hence, any proposed interventions would need to address this difficulty.
Children with specified PIMD have been found to be capable of learning to communicate choices and requests, reject unwanted objects/activities and attract the attention of others with the support of AAC (Wilder Citation2014, Roche et al. Citation2015, Roche Citation2017). Parents of children with severe disabilities who communicate pre-verbally have been found to adapt their communication with their children after having received parent-implemented communication intervention (de Carlos Isla and Baixauli Fortea Citation2016, Calculator Citation2016, Chen et al. Citation2007). The research of Chen et al. (Citation2007) could be of particular interest in this case, since the children in their study had PIMD. They found that a home-based curriculum that focused on caregiver-child communication within everyday routines could be successfully implemented despite diversity among the caregivers, children and interventionists. One result observed was that the parents reported becoming more responsive to their children’s signals and using more sensory cues in their interaction with their children. Wilder et al. (Citation2015) found that parents of children with severe disabilities felt empowered when given the opportunity to discuss and share their experiences related to communication and communication support with others in an organised manner in an online forum. Moreover, they also adjusted their communication with their children, according to self-reports.
Raising a child with PIMD is both difficult and demanding (Tadema and Vlaskamp Citation2010). Family-centred, professional support has been found to be important to parents of children with PIMD (Jansen et al. Citation2012) and can be valuable in strengthening parental resources and in promoting coping (Graungaard et al. Citation2011).
The ComAlong program is a course developed in Sweden and designed for parents of preschool children with communication disabilities. The course is typically offered within the public health care system’s child and youth habilitation services. These inter-professional services (Ylvén and Granlund Citation2015) potentially reach all families of children with intellectual disabilities, including PIMD, free of charge. The ComAlong course was developed within the AKKtiv project (www.akktiv.se [AKKtiv is a Swedish abbreviation for AAC Early Intervention]). This intervention is parent-mediated and aims to promote caregiver-child communication and AAC-supported communication within the context of everyday activities and routines (Broberg et al. Citation2012, Ferm et al. Citation2011, Jonsson et al. Citation2011). The AKKtiv program is based on 1) the definition of communication as a co-constructed and co-regulated process where meaning is created mutually/dialogically, dynamically and continuously (Bruner Citation1983, Fogel Citation1993) and 2) a theory that proposes children’s understanding of communicative intentionality as a cornerstone in their acquisition of language (Bruner Citation1974, Tomasello Citation2001). The course curriculum comprises responsive strategies, environmental-milieu teaching strategies and the use of multi-modal AAC (Broberg et al. Citation2012, Ferm et al. Citation2011, Jonsson et al. Citation2011).
The course is generally held for groups of 5-12 parents and is taught by two ComAlong course leaders, both of whom have attended an accredited training course. One of the course leaders is always a licensed speech-language pathologist. The other course leader might have another profession, such as special educator or clinical psychologist. The course consists of eight two-hour sessions and a coffee break with time for socialising. Each session has a theme (see ) and includes lectures, discussions and the collaborative analysis of video clips of parent-child interactions. Course leaders have access to ready-to-use PowerPoint presentations, video clips and suggested group exercises. In between sessions, the participants are given homework assignments to help enhance their learning and reflection and to support the application of the knowledge they have acquired in their communication with their child in the home environment (Broberg et al. Citation2012, Ferm et al. Citation2011, Jonsson et al. Citation2011).
Table 1. Overview of the ComAlong course’s eight sessions.
Ferm et al. (Citation2011) examined parents’ and course leaders’ experiences of the ComAlong course when held for a broad target group. The results showed that parents generally found the course to be a positive experience and that they also experienced positive changes in their own communication as well as that of their child (Ferm et al. Citation2011). Jonsson et al. (Citation2011) evaluated parents’ use of and experiences using the ComAlong boards (see ). They found that these experiences were positive overall, although parents of children who did not seem to understand pictures tended to find the boards less useful. As a result, a complementary set of simpler boards was designed, and course leaders were instructed to offer these to parents of children who did not yet communicate intentionally. The participants in the studies conducted by Ferm et al. (Citation2011) and Jonsson et al. (Citation2011) were parents of children with varying disabilities that affected their communication in different ways. While a few of these children may have had PIMD, this was not analysed specifically and the vast majority of the children in question had other, considerably milder disabilities than PIMD. Whether or not the conclusions drawn by Ferm et al. (Citation2011) are applicable to parents of children with PIMD is currently unknown. Both Gotthardsson (Citation2016) and Rensfeldt Flink (2014) have proposed a clinical need to adapt ComAlong to suit the PIMD group, given the special needs of this population. Jonsson et al. (Citation2011) recommended further research into the question of whether a child’s diagnosis and type of communication difficulty have an impact on their parents’ experiences and use of the ComAlong boards.
This current study focused on ComAlong as offered exclusively to parents of children with PIMD. The decision to offer exclusive courses with a PIMD focus was based on the clinical experience of parents of children with PIMD as being both more likely than others to drop out of the ComAlong course before it ended and more likely to express feeling uncomfortable (Rensfeldt Flink Citation2014). The resulting homogeneity among participants was assumed to allow course leaders leeway to focus primarily on the preverbal stages of communication development and to exemplify parental strategies, communication development and AAC use tailored to suit severely limited cognitive, motor and sensory functioning. It was also expected to enable the parents attending to both learn from and find validation in one another’s shared experiences, including how broader health issues affect communication. This is a factor that, at least informally, had been raised as a problematic issue by parents of children with PIMD who had previously attended ComAlong when a mixed and broader target group of children was predominant within the group (Rensfeldt Flink Citation2014).
Research questions
To the best of our knowledge, no group intervention targeting parents of children with PIMD has yet been studied scientifically, let alone any parental communication course. Consequently, no formal conclusions have been drawn as to which intervention features in a group-based communication course are either important or redundant in 1) helping parents of children with PIMD to experience the course as meaningful and motivating and 2) helping parents to effect positive change in their communication with their child. These knowledge gaps are what motivated this exploratory, mixed-method study that focuses on the ComAlong course as held exclusively for parents of children with PIMD within the context of child and youth habilitation services in Sweden.
This study’s primary research question was How did parents of children with PIMD perceive the ComAlong parental course? More specifically, we outlined four sub-questions: 1) Did these parents’ perceptions differ from those of parents of children with varied and generally milder communication disabilities? 2) Did the parents perceive any change in either their own or their child’s communication as a result of taking the course? 3) What course features were experienced as particularly valuable or meaningful? 4) What course features were less appreciated?
Materials and methods
Participants
The study’s participants were parents of children with PIMD who took part in a ComAlong course organised by child and youth habilitation services of Region Västra Götaland, Sweden between 2011 and 2016 and who also filled out a course evaluation form. The four courses included in the study targeted parents of children with PIMD exclusively and were attended by 30 parents of 22 children. Twenty-two completed evaluation forms were collected, resulting in a response rate of 73%.
Seventeen of the participating parents were women (77%) and five were men (23%). Their ages ranged from 23 to 46 years, with a mean age of 36.0 years. Their levels of education were reported as follows: upper secondary school (4), vocational education (1) and university (16). One participant failed to answer the question about their level of education. Two of the participating parents stated that they were currently not working due to parental leave or in order to take care of their severely ill child, while the rest reported working at least part-time outside of the home. One of the participating parents required an interpreter to be able to participate in the course and to complete the evaluation form.
The courses targeted parents of children with combined and significant cognitive and motor impairments. Parents signed up for the course after consultation with a staff member at their local child and youth habilitation centre who had assessed their child’s communication level and who had met with the parents, typically the speech-language pathologist. The children of the participating parents were reported to be between 1.5 and 6.5 years of age at the start of the course. No mean age could be calculated due to the fact that some of the children may have generated more than one evaluation form, since parents attending the course as a couple usually filled out individual evaluation forms.
Material
The evaluation survey was part of the ComAlong course material. The participants completed the surveys anonymously. The results of the participants who consented to partake in research were sent to one of the researchers (the fourth author) by the course leaders. No personal data were kept once the evaluation surveys were collected.
The evaluation form was altered slightly in 2012. Some course leaders switched to the new format immediately, while others continued to use the older format for a couple of years. This means that during the period 2011-2016, two different versions of the evaluation form were in use. In this paper, the versions will be referred to as Survey 1 and Survey 2 and data from both formats are included in the study (see ).
Table 2. Overview of survey content and inclusion of data in the study.
The close-ended questions differed between Survey 1 and Survey 2 (Survey 2 has fewer, and somewhat rephrased, close-ended questions). The quantitative analysis could therefore only be conducted on one of the versions of the evaluation form. Since most of the participants (17 of 22) used Survey 1, it is this survey that was included in the quantitative analysis. The close-ended questions included in Survey 1 are listed in (in the results section). All 22 participants were however included in the quantitative analysis regarding the global rating scale that was included in both the forms. This procedure enabled us to compare the current results with the data reported in Ferm et al. (Citation2011) in order to find out whether the responses of the participants in this study (parents of children with PIMD) differed from those of the ComAlong course’s broader target group.
Table 3. Mean ratings for each question as answered by parents of children with PIMD.
All the subjected surveys included ratings as well as written comments and answers to open ended questions. The majority of the included, written statements were answers to open ended questions, but statements commenting or clarifying ratings were also present.
Ethics approval
This study formed part of the AKKtiv project that was submitted to the regional ethical review board for evaluation. According to the decision of the review board (Gothenburg Regional Ethic Review Board: 608-06), this research should be perceived as a clinical quality assurance measure and evaluation of standard practice. As such, the AKKtiv project was formally approved by the head of Habilitation Services in Region Västra Götaland, Sweden. The guidelines for research involving humans were followed, in keeping with the Helsinki Declaration (1964). Participation was based on the respondents’ informed consent concerning the inclusion of their anonymous course evaluation surveys in the research project.
Analysis
Parents’ ratings
Mann Whitney U tests were performed to compare the ratings in the current sample with those of Ferm et al. (Citation2011). The original data were provided by the authors of Ferm et al. (Citation2011) to facilitate the analysis. Two scores were included in the analyses: an average rating score for all 20 specific items (ranging from 1-5) and a global rating (ranging from 1-10). Descriptive data on parental ratings are included in order to provide an overall impression of the parents’ perceptions.
Written answers and comments on ratings
Thematic analysis with a semantic approach (Braun and Clarke Citation2006) was used to generate the key themes within the answers to open-ended questions and comments, in order to capture the voices and shared meanings of the participants. Thematic analysis was chosen because of its flexibility and potential ability to provide a rich and detailed, yet complex account of data (Braun and Clarke Citation2006). It has been used successfully in earlier research on parental perceptions where the data are quite limited, such as in connection with open-ended answers to questionnaires (e.g. Gore Langton and Frederickson Citation2016). The analysis’ approach was theoretical in the sense that it was closely linked to the research questions and semantic in the sense that it adhered closely to the explicit statements made by the participants (Braun and Clarke Citation2006). The choice of a theoretical, semantic approach was motivated by the fact that the research questions were specific, and that the included data were the result of a written survey without the possibility for follow up-questions potentially capturing more latent meanings.
The thematic analysis was conducted in accordance with the procedure described by Braun and Clarke (Citation2006) by the first author, with co-authors being consulted in key steps of the analysis. The first author was a PhD student and a speech-language pathologist with extensive clinical experience from children with PIMD and their parents as well as the ComAlong course. In Step 1, familiarisation with data, the responses provided by the participants were collected in one document to generate an overview. The initial analysis that followed was guided by the research questions. All participating parents (i.e. all included surveys) provided data for the thematic analysis. In Step 2, generating initial codes, each interesting piece of text was assigned an initial code. 172 statements were coded in relation to the research questions. In Step 3, searching for themes, the codes were collected into groups related to the research questions. A number of initial themes were determined for each research question. These were created to reflect commonly reported experiences, but also to reflect less commonly reported experiences that were nonetheless judged to be valuable in connection with intervention goals and the study’s research questions. Four preliminary thematic maps were created, one for each research question. In Step 4, reviewing themes, more general, final and bridging themes were generated that were deemed to tell the most important stories of the data. This was a back-and-forth procedure from the detailed level of the coded extracts to the level of specified research questions and initial themes and on to the level of broader patterns and narratives. Eight themes were generated and collected in a final, thematic map without hierarchies. Quotes were then selected to illustrate the thematic framework.
Results
Parents’ ratings
First, the mean ratings for the questions addressing specific aspects of the course (answered on a 1-5 Likert scale) were calculated for the current sample (parents of children with PIMD), see , as well as for the participants in the ComAlong course studied by Ferm et al. (Citation2011). In general, ratings were very high in both groups (indicating favourable evaluations of the courses). Mean scores across all items were 4.58 (SD = 0.43) and 4.41 (SD = 0.42) for the current sample and sample of Ferm et al. (Citation2011), respectively. The difference between the groups only just fell short of statistical significance according to a Mann Whitney U test (z = - 1.95, p = 0.051). Second, the mean of the participants’ global ratings for the course (on a 1-10 Likert scale) were calculated (see ) and compared with the corresponding results from the participants in the study by Ferm et al. (Citation2011). Again, ratings were high for both the PIMD focused course (M = 9.22, SD = 1.1) and the general ComAlong course (M = 8.46, SD = 1.09), indicating highly favourable perceptions. A Mann Whitney U test revealed that parents in the current sample scored significantly higher (z = -2.84, p = 0.005, r = -0.29). Looking at individual items in the current sample, item 16 (‘There was enough room for me with regard to questions and discussion’) received the highest mean score (M = 4.94) and item 13 (‘I have got useful hints/strategies with regard to communication’) received the lowest mean score (M = 3.76) (see ).
Written answers and comments on ratings
The thematic analysis resulted in eight themes. provides an overview of the themes. The themes are subsequently accounted for in written text using illustrative extracts from parental statements.
Figure 1. Thematic map.
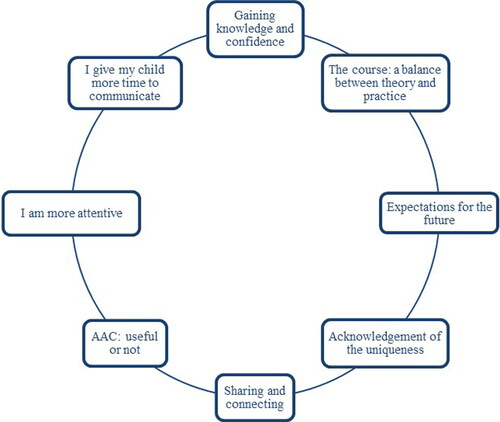
Gaining knowledge and confidence
Learning about communication seemed to be one of the most valued aspects of the course, as in this example: ‘That we have really broadened our understanding regarding communication’ (Participant 13). It was described in various ways how participants increased and deepened their knowledge and awareness of communication, not just the child’s communication but also one’s own: ‘A new world has opened up. Íve learned so much about my own way of communicating’ (participant 18). Some reported that their newfound awareness made them more confident in their child as a more capable communication partner: ‘Yes, I am more aware of communication and see that my child does, in fact, communicate’ (Participant 3). It was also commonly stated that the course leaders were skilled in providing the knowledge, e.g.: ‘Knowledgeable teachers with pedagogical skills’ (Participant 1). The statement below is an example of how one participants’ increased reflections on communication and actual communication with their child seem to be closely intertwined: ‘[I] think more about what I do and how I do it’ (Participant 7).
I give my child more time to communicate
The core concept of this theme is parents’ act of mindfully waiting for their children’s communicative initiatives and responses. It was one of the most reoccurring themes relating to changed, communicative behaviour. The course teaches expectant waiting together with responding and confirming as a three-step responsive communication strategy. In their written statements however, parents generally described waiting (“giving the child time”) as an independent strategy, e.g.: ‘Not to be in such a rush and to give her time to answer” (Participant 20).
I am more attentive
This theme collects various experiences of an increased sensitivity to any instance where the child’s behaviour could be interpreted as a communicative initiative or response and an increase in the use of strategies to confirm these signals, e.g.: ‘I have become better at (…) picking up and running with whatever catches his interest instead of focusing on ‘pushing ahead with practising’. I imitate my child more often” (Participant 8).
AAC: useful or not
AAC was a reoccurring topic in the statements of the participants, but the analysis generated two conflicting, shared meanings: AAC as useful and not useful. Half of the participants made positive remarks about the course’s AAC related content and/or described various ways in which they included AAC in communication with their child as a result of taking the course: ‘I (…) use communication boards and manual signs regularly’ (Participant 4). The AAC material included in the curriculum was considered as being valuable, together with receiving support in producing individually tailored AAC materials: ‘Getting concrete material and an introduction to how to make [communication] boards and what other aids are available’ (Participant 8). However, AAC was also repeatedly mentioned as difficult to apply with the child or that it was “too soon” to use AAC with the child. The majority of the reoccurring, critical remarks on AAC came from four participants. One participant considered that AAC, as he/she perceived it, simply was not useful to their family: ‘AAC not really meaningful’ (Participant 19), the others that either they or their children were not yet ready for AAC: ‘Too difficult with pictures yet’ (participant 12). It was also expressed that AAC assignments could have been more flexible and that the course’s standard AAC exercises were hard to apply: ‘The last assignments focused a lot on the ComAlong boards. Possible to add new exercises with alternatives to the boards?” (Participant 5).
Sharing and connecting
The opportunity to meet and connect with the others in the group was one of the aspects of the course that was most frequently mentioned as valuable. Fifteen of the twenty-two participants mentioned this experience, e.g.: ‘made a wonderful connection with the parents and [learned] what their everyday lives are like!” (Participant 5). Various participants mentioned the importance of meeting with parents of children with disabilities resembling those of their own child: ‘That you selected course participants based on the similarity of the difficulties experienced by their children, which helped me feel at home, comfortable” (Participant 4). Participants also connected with the course leaders’, whose knowledgeable empathy and respect were mentioned with appreciation as well as their willingness to allow the participants’ spontaneous discussions to arise: ‘To get to speak freely and share experiences with everybody’ (Participant 3).
Acknowledgement of the uniqueness
It seemed important to several of the parents that the course leaders understood and acknowledged that their children had a complex combination of disabilities and/or a slow development: ‘Perhaps clarify that the result is likely to come with time: not in a week’ (Participant 17). The receiving of personal attention from the course leaders, even though the intervention was group-based, was highly valued. Those who mentioned this point seemed confident that the course leaders had understood the individual needs of the child and had sufficient knowledge about each child and parent to be able to provide individually-tailored advice and feedback: ‘All the info and special attention given to each child in the group, the [course] leader really thought out solutions for each child” (Participant 18). On the other hand, not all parents found that they got this individually-tailored advice that acknowledged the uniqueness of the child: ‘How to practise communicating with someone who is blind, severely cognitively disabled and probably autistic’ (Participant 19).
Expectations for the future
Based on the analysed statements, no clear patterns could be seen related to perceived child development during the course. Many parents seemed aware of their children’s slow development and did not anticipate any change during the course period. However, several of the participants shared the experience that they assumed that results would indeed come with time. ‘Not yet’, was a reoccurring answer to the question whether the parents perceived any changes in the communication of the child: ‘It will get better, but he needs more time” (Participant 21).
The course: a balance between theory and practice
A lot of theory leaving too little time for practical, “hands-on” activities was a point of criticism regarding the course: ‘A bit less theory. This doesn’t have to be a course about academic theory’ (Participant 14). Some participants forwarded ideas on how to strengthen the practical aspect of the course. These ideas often concerned ways to expand the course and did not necessarily include a request to reduce its theoretical content: ‘Perhaps more group-based exercises, or more videos of examples to imitate?’ (Participant 18) or ‘To have one course meeting where the children could be present’ (Participant 16).
Discussion
This study aimed to define participants’ experiences of a communication course, with a focus on parental responsivity and AAC. The course participants were parents of children with PIMD. Raising a child with PIMD is demanding and very time consuming (Luijkx et al. Citation2017). Notwithstanding, professional support has been shown to relieve the strain on parents and can according to parents themselves play a very important role in their lives (Tadema and Vlaskamp Citation2010). It is consequently very important that parental experiences, needs and wishes are taken into account when structuring and offering services to the families of children with PIMD (Luijkx et al. Citation2017). To this end, we analysed parental perceptions as expressed in the evaluation forms submitted after the ComAlong course as offered to parents of children with PIMD.
The results of parents’ overall evaluation of the course showed that the parents were generally very positive about the course. These course participants were at least as positive, or even more so, than those surveyed in the study by Ferm et al. (Citation2011). This implies that the ComAlong intervention is as well suited to children with very severe disabilities as it is to the broader target group, at least when offered as a dedicated PIMD course. Ferm et al. (Citation2011) found that ComAlong course participants appreciated having a diverse range of fellow participants as concerned the nature of their respective children’s disabilities. Nevertheless, in the current case, the clinicians involved chose to offer ComAlong groups exclusively for parents of children with PIMD, based on their clinical experience (Rensfeldt Flink Citation2014). The overall positive evaluations provide clinical implications to keep offering designated communication groups for parents of children with PIMD. Moreover, in the qualitative analysis, participants commonly mentioned the opportunity to openly share their own experiences and connect with parents who have children with similar disabilities as a greatly appreciated feature of the intervention. This corresponds with the findings of Wilder et al. (Citation2015), who found that learning about communication and AAC in an online network of parents and professionals all focusing on children with severe disabilities was an overwhelmingly positive and empowering experience. In this current study, course participants commented on the trained course leaders by remarking on their warmth and empathy as well as knowledge and skills. In this respect, it can be assumed that they played a role in creating a relaxed and open environment that allowed participants to feel free to share their experiences and trust that they could get useful feedback from co-participants as well as course leaders. Moreover, participants also developed an affective bond with their course leaders comparable with the parent-professional alliance that has been found to be associated with improved clinical outcomes and stronger treatment engagement in various child, parent and family interventions (de Greef et al. Citation2017).
In the thematic analysis it was found that several parents experienced a heightened awareness concerning communication and applied responsive strategies on their part as well as an increase in their use of AAC. The true extent of the parents’ application of the communication strategies and aids in their communication with their children was never examined in the study. Hence, whether or not these reported changes can be observed by an independent observer are questions for future research. However, parents learning about communication and, as a result, coming to view themselves as instrumental in the communication development of their children in a positive sense should not be understated as a desirable outcome of the intervention, regardless of any changes in child outcomes. Graungaard et al. (Citation2011) suggested that a sense of “taking action” and “maintaining hope” are two out of nine important factors in the creation of personal, emotional resources for parents of children with severe disabilities. The parents’ reappraisal of themselves as instrumental in the positive communicative development of their children could potentially help protect the parents of children with severe disabilities against succumbing to negative emotional states. Graungaard et al. (Citation2011) also stated that the creation of personal resources should be considered crucial for this group of parents in all clinical encounters. At the same time, supporting parents in developing realistic expectations of future development seems equally important. How clinicians balance this issue when interacting with families would be an important topic for future research.
No clear patterns could be identified in the parents’ perceptions regarding changes in their children’s communication as a result of the course, though many participants who reported no change also mentioned that their child’s development was slow. They had not expected a noticeable change to occur over an eight-week period. This is obviously relevant in the case of children with such severe disabilities and implies that further research aimed at tracking changes in children’s communication would need to be both highly detailed and preferably longitudinal in order to measure subtle change. Moreover, evaluating the communication of the child and their parent as separate “units” in the communicative exchange might prove to be problematic, given the theoretical view of communication as a dynamic and co-created process (Bruner Citation1983, Fogel Citation1993). The questions in the surveys were expressed in a way that clearly separated the communication of the parent from the communication of the child, which hindered a dialogical approach in the analysis. Hostyn et al. (Citation2010) argue that a dialogical approach is especially appropriate when studying interactions involving individuals with PIMD, as it takes into account the natural asymmetry between communication partners and the reliance on contextual factors in the communication process. In terms of research implications, further studies on parent-child interaction and communication and the possible effects of ComAlong might benefit from applying research methods that are clearly in line with a dialogical, theoretical framework.
The results regarding the participants’ perceptions of AAC as useful were mixed. Several participants mentioned their increased use of AAC. The chance to acquire a practical knowledge of AAC was also regarded as a valuable aspect of the course. A few others described AAC as a less-relevant part of the course curriculum and/or as an aspect that was difficult to apply. The item addressing the course specific AAC boards (item 9, see ) held one of the lowest mean scores (but still fairly high) and with a relatively high standard deviation (M = 4.06, SD = 1.34). This result may also support the notion of a division among participants regarding their experiences of AAC. Parental ambivalence towards using AAC with children with severe disabilities has been previously noted by Stephenson and Dowrick (Citation2005), who suggest that interventions should include a greater focus on parental knowledge of pre-verbal communication development, the possible benefits of AAC and the role the parents can play in the child’s communicative development. Indeed, although this is the ComAlong intervention’s core, the participating parents still drew somewhat different conclusions about the possible benefits of AAC. These results seem to be in line with previous findings by Jonsson et al. (Citation2011). They raise questions about the variation’s possible correlation with 1) parental conceptions of AAC and 2) the individual characteristics of the child (i.e. degree of intellectual or physical disability, alertness, sensory comorbidity and age), or other factors.
Although beyond the scope of this study, further research that provides a more in-depth understanding of how different factors affect parents’ use of AAC with children with PIMD would be very welcome. Such knowledge would potentially facilitate a more personalised application of interventions such as the ComAlong course. Indeed, according to the results, receiving individual support that take into account the uniqueness of the child was one of the more highly-valued features of the course. Consequently, in terms of clinical applications, these results support the introduction of an even more highly individualised approach within the course setting and with regard to AAC, in particular.
In the thematic analysis, the course’s balance between theory and practice was found to be important. Some parents even found the course to be too theoretical in nature and suggested that its practical content should be given greater emphasis. This notion is perhaps strengthened by the fact that the item addressing “hints and strategies” received the lowest mean score of all (see ). Parents of children with PIMD are experts on communicating with their respective children (Wilder and Granlund Citation2003). To be able to make the most of this role, however, parents require suitable information about the available options concerning aids, activities and adjustments in everyday life that will help them in making decisions about how best to support their child (De Geeter et al. Citation2002). The current results suggest an eagerness on the part of parents to acquire and make practical use of such information. It seems that important theoretical knowledge acquired by parents about communication, interaction and AAC (Stephenson and Dowrick Citation2005) needs to be clearly paired with hands-on tips and tools that are easy to apply without delay. One clinical application of these results is the need for the connection between theory and practice to be presented in a balanced way that is perceived as meaningful by all participating parents. Also, that the ComAlong course benefits from practical instructional approaches.
Concerning the balance between theory and practice, it should be emphasised that, in this instance, the participants’ educational levels were relatively high; 73% described themselves as having a university education. This can be compared with official statistics (Statistics Sweden 2016), which reveal that 48% of the Swedish population in a comparable age span (35-44 years) has some kind of post-upper secondary school education. It seems particularly interesting that, despite an unusually high number of the parents having tertiary training, they still preferred more practical, “hands-on” exercises. We cannot deduce the reason for the over-representation of university-educated parents in this course. To the best of our knowledge, this does not reflect the norm in the target group as such. Although not explored further in this study (nor in any previous research, as far as we are aware), the fact that parents with university degrees are over-represented in this sample should be of significant interest to Sweden’s child and youth habilitation services, since it might indicate unequal access to communication interventions for children with PIMD based on the educational level of their parents.
Limitations and future directions
Besides the limitations already discussed above, the study’s qualitative data is somewhat limited in as much as that the statements made by the participants were generally brief and that, for obvious reasons, the data does not include any responses to follow-up questions. Overall, the total dataset can therefore be viewed as painting a rather basic picture of the reality. On a related note, the evaluation questions were not specifically composed for this particular sub-group of children (children with PIMD). Moreover, they focus directly on the course itself and do not explicitly address indirect effects on parenting or parents’ feelings of adequacy/inadequacy when communicating with their child. Hence, future research would benefit from richer data, such as interview data, which would enable qualitative analysis beyond the more descriptive level provided in this study. Also, objectively studying intervention outcomes on naturally occurring communication between parents and children would be much warranted. Notwithstanding, we believe that despite this study’s limitations, this study does provide important foundational information for future research in the field. For instance, the results undeniably shed light on the fact that far more knowledge is needed about barriers to and facilitators of parents’ application of AAC in communicating with children with PIMD. Moreover, research focusing on child outcomes is sorely needed.
Declaration of interest statement
The authors report no conflict of interest.
Acknowledgements
The authors wish to thank the participating parents for their time and willingness to contribute to the study. The study was financed by grants from the Swedish state under the agreement between the Swedish government and the city councils, the ALF-agreement.
Additional information
Funding
Related Research Data
References
- Branson, D. and Demchak, M. 2009. The use of augmentative and alternative communication methods with infants and toddlers with disabilities: A research review. Augmentative and Alternative Communication, 25, 274–286.
- Braun, V. and Clarke, V. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77–101.
- Broberg, M., Ferm, U. and Thunberg, G. 2012. Measuring responsive style in parents who use AAC with their children: Development and evaluation of a new instrument. Augmentative and Alternative Communication, 28, 243–253.
- Bruner, J. 1974. From communication to language—A psychological perspective. Cognition, 3, 255–287.
- Bruner, J. 1983. Child’s talk: Learning to use language. Oxford: Oxford University Press.
- Calculator, S. N. 2016. Description and evaluation of a home-based, parent-administered program for teaching enhanced natural gestures to individuals with Angelman syndrome. American Journal of Speech-Language Pathology, 25, 1–13.
- Chen, D., Klein, M. D. and Haney, M. 2007. Promoting Interactions with Infants Who Have Complex Multiple Disabilities: Development and Field‐testing of the PLAI Curriculum. Infants & Young Children, 20, 149–162.
- Cress, C. J. and Marvin, C. A. 2003. Common questions about AAC services in early intervention. Augmentative and Alternative Communication, 19, 254–272.
- de Carlos Isla, M. and Baixauli Fortea, I. 2016. Parent-implemented Hanen program more than Words in Angelman syndrome: A case study. Child Language Teaching and Therapy, 32, 35–51.
- De Geeter, K. I., Poppes, P. and Vlaskamp, C. 2002. Parents as experts: The position of parents of children with profound multiple disabilities. Child: Care, Health and Development, 28, 443–453.
- de Greef, M., Pijnenburg, H. M., van Hattum, M. J., McLeod, B. D. and Scholte, R. H. 2017. Parent-professional alliance and outcomes of child, parent, and family treatment: A systematic review. Journal of Child and Family Studies, 26, 961–976.
- Ferm, U., Andersson, M., Broberg, M., Liljegren, T. and Thunberg, G. 2011. Parents’ and course leaders’ experiences of the ComAlong augmentative and alternative communication early-intervention course. Disability Studies Quarterly, [e-journal] 31(4). Available through: Open Journal Systems [Accessed 1 June 2018]
- Fogel, A. 1993. Two principles of communication: Co-regulation and framing. In: J. Nadel and L. Camaioni, eds. New perspectives in early communication development. London: Routledge. pp.9–22.
- Gore Langton, E. and Frederickson, N. 2016. Parents’ experiences of professionals’ involvement for children with extreme demand avoidance. International Journal of Developmental Disabilities, 64, 16–24.
- Gotthardsson, E. 2016. Utbildning i kommunikation för föräldrar till barn som är blinda och på tidig utvecklingsnivå. Kristianstad: Region Skåne.
- Graungaard, A. H., Andersen, J. S. and Skov, L. 2011. When resources get sparse: A longitudinal, qualitative study of emotions, coping and resource-creation when parenting a young child with severe disabilities. Health: An Interdisciplinary Journal for the Social Study of Health, Illness and Medicine, 15, 115–136.
- Grove, N., Bunning, K., Porter, J. and Olsson, C. 1999. See what I mean: Interpreting the meaning of communication by people with severe and profound intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 12, 190–203.
- Hostyn, I., Daelman, M., Janssen, M. J. and Maes, B. 2010. Describing dialogue between persons with profound intellectual and multiple disabilities and direct support staff using the Scale for Dialogical Meaning Making. Journal of Intellectual Disability Research, 54, 679–690.
- Hostyn, I. and Maes, B. 2009. Interaction between persons with profound intellectual and multiple disabilities and their partners: A literature review. Journal of Intellectual & Developmental Disability, 34, 296–312.
- Jansen, S., Van den Putten, A. and Vlaskamp, C. 2012. What parents find important in the support of a child with profound intellectual and multiple disabilities. Child: Care, Health and Development, 39, 432–441.
- Jonsson, A., Kristoffersson, L., Ferm, U. and Thunberg, G. 2011. The ComAlong communication boards: Parents’ use and experiences of aided language stimulation. Augmentative and Alternative Communication, 27, 103–116.
- Landry, S. H., Smith, K. E. and Swank, P. R. 2006. Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42, 627–642.
- Luijkx, J., van der Putten, A. and Vlaskamp, C. 2017. Time use of parents raising children with severe or profound intellectual and multiple disabilities. Child: care, Health and Development, 43, 518–526.
- Nakken, H. and Vlaskamp, C. 2007. A need for a taxonomy for profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, 4, 83–87.
- Nijs, S., Vlaskamp, C. and Maes, B. 2016. Children with PIMD in interaction with peers with PIMD or siblings. Journal of Intellectual Disability Research, 60, 28–42.
- Rensfeldt Flink, A. 2014. KomIgång – erfarenheter från kurser med föräldrar till barn med flerfunktionsnedsättning. In: The Swedish Family Care Competence Center, 1st national conference about individuals with multiple disability: Livets Möjligheter. Stockholm, Sweden, 10-11 March 2014, Kalmar: Nationellt Kompetenscentrum Anhöriga (NKA).
- Roche, L. 2017. Evaluating and enhancing communication skills in four adolescents with profound and multiple disabilities. PhD thesis and dissertations. Victoria University of Wellington, New Zeeland. https://www.tandf.co.uk//journals/authors/style/reference/ref_YJDD.pdf.
- Roche, L., Sigafoos, J., Lancioni, G. E., O’Reilly, M. F. and Green, V. A. 2015. Microswitch technology for enabling self-determined responding in children with profound and multiple disabilities: A systematic review. Augmentative and Alternative Communication, 31, 246–258.
- Romski, M., Sevcik, R. A., Adamson, L. B., Smith, A., Cheslock, M. and Bakeman, R. 2011. Parent perceptions of the language development of toddlers with developmental delays before and after participation in parent-coached language interventions. American Journal of Speech-Language Pathology, 20, 111–118.
- Statistics Sweden. 2016. Befolkningens utbildning 2016 (UF37). [pdf] Stockholm: Statistics Sweden. Available at: http://www.scb.se/hitta-statistik/statistik-efter-amne/utbildning-ochforskning/befolkningens-utbildning/befolkningens-utbildning/pong/publikationer/befolkningens-utbildning-2016/ [Accessed 17 May 2018].
- Stephenson, J. and Dowrick, M. 2005. Parents’ perspectives on the communication skills of their children with severe disabilities. Journal of Intellectual & Developmental Disability, 30, 75–85.
- Spiker, D., Boyce, G. C., Boyce, L. K., et al. 2002. Parent-child interactions when young children have disabilities. In: P. Davidson, M. Guralnick, and L. Hickson, eds. International review of research in mental retardation, vol. 25. Cambridge, MA: Academic Press, pp.35–70.
- Tadema, A. C. and Vlaskamp, C. 2010. The time and effort in taking care for children with profound intellectual and multiple disabilities: A study on care load and support. British Journal of Learning Disabilities, 38, 41–48.
- Tomasello, M. 2001. Perceiving intentions and learning words in the second year of life. In: M. Bowerman and S. Levinson, eds. Language acquisition and conceptual development. Cambridge: Cambridge University Press, pp.132–158.
- Topping, K., Dekhinet, R. and Zeedyk, S. 2013. Parent-infant interaction and children’s language development. Educational Psychology, 33, 391–426.
- Van der Heide, D., Van Der Putten, A., Van Den Berg, P., Taxis, K. and Vlaskamp, C. 2009. The documentation of health problems in relation to prescribed medication in people with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, 53, 161–168.
- Van Keer, I., Colla, S., Van Leeuwen, K., Vlaskamp, C., Ceulemans, E., Hoppenbrouwers, K., Desoete, A. and Maes, B. 2017. Exploring parental behavior and child interactive engagement: A study on children with a significant cognitive and motor developmental delay. Research in Developmental Disabilities, 64, 131–142.
- Van Keer, I. and Maes, B. 2018. Contextual factors influencing the developmental characteristics of young children with severe to profound intellectual disability: A critical review. Journal of Intellectual & Developmental Disability, 43, 183–201.
- Warren, S. F. and Brady, N. C. 2007. The role of maternal responsivity in the development of children with intellectual disabilities. Mental Retardation and Developmental Disabilities Research Reviews, 3, 330–338.
- Wilder, J. 2014. Kommunikation hos och med barn och ungdomar med flerfunktionsnedsättningar: En systematisk kunskapsöversikt. Kalmar: Nationellt Kompetenscentrum Anhöriga (NKA).
- Wilder, J. and Granlund, M. 2003. Behaviour style and interaction between seven children with multiple disabilities and their caregivers. Child: Care, Health and Development, 29, 559–567.
- Wilder, J., Magnusson, L. and Hanson, E. 2015. Professionals’ and parents’ shared learning in blended learning networks related to communication and augmentative and alternative communication for people with severe disabilities. European Journal of Special Needs Education, 30, 367–383.
- Ylvén, R. 2015. Samordning av stöd för barn och ungdomar med flerfunktionsnedsättning och deras familjer. Kalmar: Nationellt Kompetenscentrum Anhöriga (NKA).
- Ylvén, R. and Granlund, M. 2015. Collaborative problem solving in the context of early childhood intervention – the link between problems and goals. Scandinavian Journal of Disability Research, 17, 221–239.