Abstract
There is a widespread lack of behavioral professionals available to support children and families affected by neurodevelopmental disabilities. As a result of limited availability, services that can be provided from a distance have developed. Telehealth is a modality that can increase access to services, lessen financial constraints, and support assessments of generalization. Using either synchronous or asynchronous components it can foster evaluation and coaching. Guidelines for usage have surfaced in North America and been integrated into the continent’s existing model of behavioral care. However, in Europe where all modalities of behavioral services are fighting to receive funding, frameworks are scarce. Understanding more about telehealth in behavioral care, its various applications throughout Europe, and the local context into which it can be applicable may promote system growth. To support this cause, a scoping review of recent behavioral telehealth practices for children and families impacted by neurodevelopmental disabilities in Europe was undertaken; looking specifically to assess types of studies, their targets and outcomes, telehealth modality components, barriers, and directions for future work. Although few studies surfaced, valuable conclusions can be drawn about the model’s empirical validation, creating a groundwork for sustainability, and the need for developing policy and standardized application.
A look at recent telehealth practices for children with neurodevelopmental disabilities in Europe
Children with neurodevelopmental disabilities can present with challenges in different areas (Ritzema et al. Citation2016). Areas of struggle may include socialization, communication, cognition, and self-care (Lollar et al. Citation2012). Resulting behavioral challenges can substantially decrease the child and family’s quality of life. Parents of children with neurodevelopmental disabilities may also face increased financial challenges, marital disharmony, social isolation, and reduced quality of life (Gardiner et al. Citation2018).
Strategies grounded in the science of applied behavior analysis (ABA) have been empirically demonstrated to increase skills by using systematic teaching methods, incremental instruction, and function-based approaches (e.g. Virués-Ortega Citation2010). ABA-based services can involve different tactics. Some of these include a verbal behavior approach (e.g. Barbera Citation2007), naturalistic teaching strategies (e.g. Schepis et al. Citation1998), functional communication training (e.g. Tiger et al. Citation2008), discrete trial training (e.g. Smith Citation2001), and self-management (Lee et al. Citation2007). Given the complex nature of the science of behavior, practicing competently requires specialized educational courses and training (Shook and Neisworth Citation2005). The specialized coursework must adhere to a certain number of hours of discretionary content. This content includes ethics, professional conduct, philosophical underpinnings and principles of behavior, measurement, analysis, experimental design, behavior assessment, and behavior change procedures (Association for Behavior Analysis International, Citation2018). Training requirements include the completion of supervised practicums across numerous competency areas which take, on average, over a year to complete (Behavior Analyst Certification Board, Citation2021b). The rigorous nature of working towards becoming a behavioral practitioner has contributed to the dearth of people available to provide ABA services.
As a result, many children and families affected by neurodevelopmental disability cannot access ABA services. While available in parts of North America and some metropolises in other countries, there is a lack of ABA services in areas of the world (Ferguson et al. Citation2019; Salomone et al. Citation2014). In Europe there are exceedingly fewer behavior practitioners than in North America (Keenan et al. Citation2015). At the time of writing this manuscript there were 1349 registered behavior analysts across the 49 European countries targeted in this review (Behavior Analyst Certification Board Citation2021a, March 2). This number is further put in perspective when considering that in the small US state of Florida there are over 5000 registered behavior analysts (Behavior Analyst Certification Board Citation2021a, March 2). Moreover, Keenan and colleagues (2015) reviewed behavior analysis in Europe, finding that unvalidated eclectic models of treatment are commonly used. In the Czech Republic for example, it was found that behavior analytic services were scarcely available for children with autism, and that current behavior analysts were spread very thin with many practitioners working without needed resources, social support, or mentorship opportunities (Kingsdorf and Pančocha Citation2020).
This lack of available behavioral professionals is widespread and ongoing. For example, rural communities in the United States have historically been left with fewer or lower quality ABA services (Mello et al. Citation2016). Other places across the Middle East (Eid et al. Citation2017), Africa (Ruparelia et al., Citation2016), Asia (Manohar et al. Citation2019), and Latin America (Montiel-Nava et al. Citation2020) are also facing this challenge. As a result of the limited access worldwide, services that can be provided from a distance have developed.
History of telehealth practices
Although not coined by the field of behavior analysis, delivering ABA services from a distance has been termed telehealth. Modern telehealth practices of providing behavioral services to children and families impacted by neurodevelopmental disabilities grew out of the field of telemedicine. In the field of ABA the terms telehealth and telemedicine are often used interchangeably. However, telemedicine, is a field broadly defined as providing medical information and services over a distance by telephone or other means of broadcasting or cable, and started in the 1960s (Bashshur and Shannon Citation2009), but began gaining popularity in the 1990s (Perednia and Allen Citation1995). It originated as sending still images between patients and doctors to allow for diagnosis of ailments such as skin conditions. Ordinary telephone communication was also used to allow for therapeutic consultations with medical professionals. Other early modalities and applications included medical education and case management using short video clips, sound, or voice. Over time, application became more complex with real-time one-way or two-way video sharing for services such as psychiatric evaluations. As bandwidth has become more available and digital technologies more accessible, the field has continued to grow. Despite issues in clinical expectations, legality, and economic factors, telemedicine has still allowed medical services to become available to individuals in rural and underserved areas (Perednia and Allen Citation1995). Some notable examples of positive telemedicine outcomes around the world include the 237,221,884 kilometers of patient travel avoided in 2012 in Ontario (Ontario Telehealth Network, Citation2013), and the $15.8 million USD saved in the central United States during a 5-year period when eEmergency services were used to avoid patient transfers (Kansas Health Institute Citation2014). With such successes, it is not surprising that the field has evolved to include service variations.
Telehealth is one such variation. Telehealth, also known as telepractice, is now often considered to encompass training, teaching, or coaching services provided using online delivery and two-way audio-visual communication (Rispoli and Machalicek Citation2020). Although at the most basic level telehealth involves the movement of images and data, advanced technologies have been utilized to improve the outcomes.
Telehealth technologies
A myriad of telehealth technologies can be identified throughout the literature. Two major categories of telehealth technology can be distinguished based on the temporal presence and mode of participation. Synchronous, or real-time support, may involve one-on-one parent and practitioner meetings or one-on-one service delivery between the behavior practitioner and the child done via videoconferencing or telephonically. Asynchronous support, where practitioner and client do not meet at the same time, may involve the sending of videos by parents to practitioners, the independent review of videos by practitioners, the review of electronic learning materials by parents, and monitoring the attribute of a client from afar (e.g. sleep patterns). When it comes to providing synchronous didactic instruction or coaching, some studies have demonstrated success using real-time video conferencing tools like Skype (e.g. Pantermuehl and Lechago Citation2015), FaceTime (Boutain et al. Citation2020) and the Google platform (e.g. Pennefather et al. Citation2018). In the case of asynchronous telehealth components, some studies have demonstrated success using common file storage applications like Dropbox for video sharing (e.g. Neely et al. Citation2020), store-and-forward technologies requiring low bandwidth where video recordings from live events and historical data are shared via a secured platform (e.g. Smith et al. Citation2017), and remote patient monitoring where a person’s physiological changes are tracked and shared with a professional (Taj-Eldin et al. Citation2018). E-learning platforms and Learning Management Systems (LMS) such as Moodle, Blackboard, and Adobe Authorware have been used for independent distance learning to provide information and training to families (Meadan and Daczewitz Citation2015).
Telehealth encompass both high-tech and low-tech formats. However, a minimum standard of connectivity, hardware, and software is usually needed to access any such technologies. This includes, but is not limited to, a minimum download and upload speed of 1Mpbs, a laptop or desktop computer with 4 GB of RAM, and anti-virus software (Lee et al. Citation2015).
Validated telehealth practices
Telehealth practices can allow for increased access to services, reduced travel time for overworked professionals and overstressed families, more cost-effective services, and provide professionals with information about how teaching has extended to the natural environment (LeBlanc et al. Citation2020). As a result, the use of telehealth practices for delivering services to children with neurodevelopmental disabilities and their families has increased (Tsami et al. Citation2019). A literature search conducted by the Behavior Change Institute revealed over 80 telehealth studies that were published since 1997 (Behavior Change Institute, Citation2020). A comprehensive review conducted by McLay et al. (Citation2020) found that some early empirical support exists for using telehealth services to deliver interventions to children and adolescents with sleep difficulties. Additional article reviews were conducted by Akemoglu et al. (Citation2020) and Unholz-Bowden et al. (Citation2020) which found over 30 studies looking at using telehealth practices to train parents. Further empirical validation for behavioral telehealth exists for practices focused on training direct care staff (e.g. Rios et al. Citation2020) and supporting and coaching educators (e.g. Rosenberg et al. Citation2020). In a recent randomized controlled trial conducted by Lindgren and colleagues (Citation2020), it was demonstrated that parents who received telehealth services teaching them to use functional communication training with their children saw much greater improvements than their control group counterparts who received treatment as usual. The value of telehealth services has been demonstrated outside the field of ABA, too. Speech-language pathology services (Molini-Avejonas et al. Citation2015) and occupational therapy services (Cason Citation2014) have been successfully provided via teleheath. Overall, evidence-based practices have been made more accessible to parents and schools because of telehealth (Chung et al. Citation2020). Moreover, as discussed by Unholz‐Bowden et al. (Citation2020), research shows that parents receiving telehealth services provide high ratings of treatment acceptability. Most recently, considering the COVID-19 pandemic, the focus on medical care has shifted to the telehealth model prompting extensive publications and reviews which discuss ongoing research and development of this service delivery modality (e.g. Rodriguez Citation2020). The pandemic has also resulted in funding for ABA services via a distance model, which was previously unpermitted in many places (Council of Autism Service Providers Citation2020).
However, when it comes to telehealth practices in Europe, movement forward has been slower. Raposo (Citation2016) discussed the challenges with establishing telemedical practices in Europe being the result of a missing comprehensive legal framework around services. Some steps have been taken to support telepractice in the region, though. For example, training courses on telemedicine have been incorporated into the health practitioner education in Switzerland (Brockes et al. Citation2017) and professionals have pushed for the use and regulation of telemedicine apps across Europe (Crico et al. Citation2018). Moreover, it was recently presented that some of the European nations which are part of the Organisation for Economic Co-operation and Development (OECD), such as Belgium, Denmark, and Poland, are working towards building public funding and legislation around telehealth (Hashiguchi Citation2020). With another review being generated because of COVID-19 showing the European nations of Italy and Spain taking increased steps towards telehealth transitions (Bhaskar et al., Citation2020).
Europe and behavioral services
Despite the small steps being taken in some European nations towards telehealth applications, there appears to be little formal alignment between this modality and behavioral services. To understand this lag, it is necessary to consider the context of behavior analysis in the region. In most European countries behavior analysis is not a recognized, or resultantly publicly funded, profession (Kelly et al. Citation2019). Moreover, in places across the continent, like Germany for example, there has been funding for only eclectic approaches as opposed to ABA-based services (Dillenburger Citation2011). Europe has not seen legislation surrounding behavior analysis services and their integration into the healthcare system (Keenan et al. Citation2010). In European nations, like Italy, where ABA appears to be offered as a service for individuals with autism, its prevalence of usage is less than one third and there are not mandates surrounding its application (Borgi et al. Citation2019). In the Czech Republic, for example, behavioral services have never been widely accessible due to the lack of skilled professionals and financial constraints for the families (Kingsdorf and Pančocha Citation2020). In another recent study of southeastern European nations less than one half of the survey respondents were presently receiving behavioral services for their children with autism with less than 10% accessing these services from a behaviorist (Daniels et al. Citation2017). This aligns with the previous work of Salomone et al. Citation2016 who surveyed 18 European countries to find that behavior analytic services for children with autism were not the norm. This minimal use of behavioral services in Europe is likely the result of missing legislation, funding guidelines, availability of professionals, and misinformation (Gillen and Keenan Citation2018). These concerns have been historically echoed when discussing the plight of children and families impacted by neurodevelopmental disabilities on the continent (e.g. Hughes and Shook Citation2007; Keenan et al. Citation2015; Roll-Pettersson et al. Citation2020).
Given the overwhelming research which supports that evidence-based practices for children with autism are based on the science of ABA (Grigorenko et al. Citation2018), it is not surprising that in the United States these treatments have become the standard of practice. In accordance with the recommendations of the American Academy of Pediatrics (Myers and Johnson Citation2007), U.S. Surgeon General (U.S. Surgeon General, Citation2001), and others, the accessibility of services has increased throughout the nation. As a result, funding for ABA services has steadily grown over the past decades, to include access via insurance, state or federal funds, public education, and voucher or scholarship programs (Harvey et al. Citation2010). While there is a recognized challenge, even in the U.S., with placing the funding responsibility for ABA services on the shoulders of education or medicine (Pollak Citation2016), guidelines have still been developed to help provide access to care. These regulations have helped to later establish a framework for increasing the availability of services to those in more rural or underserved regions. The process of evaluating the context of need and the development of, or transition to, telehealth has been made explicit by several governmental agencies like the Center for Disease Control (CDC) (National Center for Immunization and Respiratory Diseases (NCIRD) and Division of Viral Diseases Citation2020), telehealth task forces like the Council of Autism Service Providers (CASP) (e.g. Council of Autism Service Providers Citation2020), and professional journals (e.g. Rodriguez Citation2020).
As made evident earlier, more needs to be done in Europe to support the needs of families impacted by neurodevelopmental disabilities. There are projects underway to drive the allocation of funding and development of practitioner training to support behavioral services in the region (Roll-Pettersson et al. Citation2020). However, to date, little has been done to integrate telehealth services into any European model of care for behavioral services. Perhaps better understanding the telehealth system in behavioral care, its various applications throughout Europe, and the local context into which it can be applicable will support system growth and better serve families in need.
Research aim
Countless telehealth studies have been conducted looking at the efficacy of delivering intervention services to children and training staff and parents via this methodology. However, it appears that there is less empirical support for the practice in European countries, which may be responsible for its slow growth. To inform the development of better practices and guidelines for integrated models of care for telehealth services in Europe, a review of telehealth practices for providing services to children and families impacted by neurodevelopmental disabilities in Europe was undertaken. Looking at the literature aimed to answer these questions:
What type of studies on providing telehealth services to families of children with neurodevelopmental disabilities in Europe have been conducted in the last five years?
What were the main behaviors targeted for change and intervention strategies used?
What were the main telehealth components?
What barriers were faced?
What future work needs to be done to support children and families impacted by neurodevelopmental disabilities in Europe looking to access behavioral services via a telehealth model?
Method
Numerous literature reviews of telehealth have been conducted in recent years (e.g. Ferguson et al. Citation2019; Meadan and Daczewitz Citation2015; Neely et al. Citation2021; Tomlinson et al. Citation2018). As a result, this literature search was targeted. A scoping review of the literature was conducted. This method was chosen given the relatively limited nature of the topic. It was anticipated that too few studies would be found to enable a quantitative analysis. As a result, this more rapid method for summary was selected.
Eligibility criteria
Studies were included in the review if they reported on the use of a telehealth modality to deliver behavior-analytic interventions to support families impacted by neurodevelopmental disabilities in Europe. Only recent studies, those published since 2015, were included. Given the novelty of telehealth practices and behavior analytic services in the region, it was anticipated that searching prior to 2015 would not result in more studies. This decision was additionally supported by the reported mandate for widespread telemedicine services in Europe which was presented in 2014 (eHealth Stakeholder Group Citation2014). As well, studies needed to be published in the English language and involve caregivers in the telehealth model. There were no restrictions on the specific telehealth modality used or the age of the participants. However, studies were excluded in the review if they were review articles themselves, “how-to” guides that did not evaluate the use of an intervention, used strategies that were not grounded in the science of behavior (e.g. music therapy, psychiatry), focused on only using telehealth to facilitate a diagnosis or follow-up care, or reported on survey data in the absence of intervention.
Information sources and search strategy
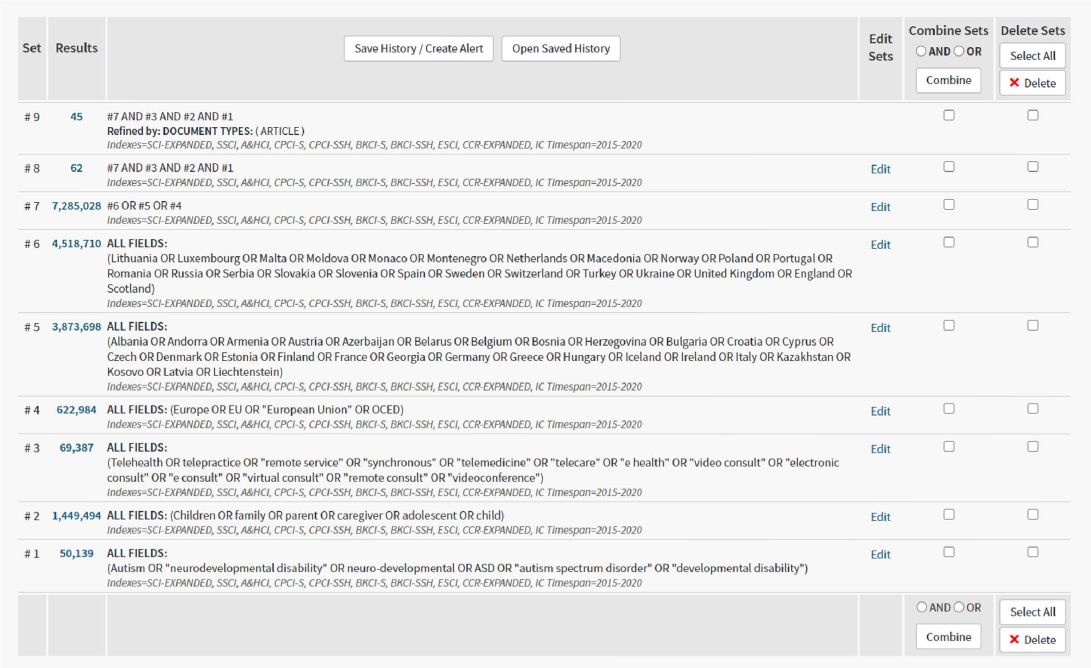
The Web of Science, Scopus, and PsycInfo databases were searched. Since the focus of this review was on intervention-based telehealth services provided to families impacted by neurodevelopmental disabilities in Europe a combination of terms and keywords relevant to the diagnosis (neurodevelopmental disability), participants, mode of delivery (telehealth), and location (Europe) were used (see for the lists of keywords). Appendix 1 provides one of the detailed searches. Google Scholar was additionally used to search for titles from reference lists and previously conducted review studies. However, no new articles surfaced.
Table 1 Search terms.
Selections of sources of evidence
Search results, after being filtered for the language and journal article requirements, if needed, then underwent title review. After title review the remaining articles were combined and duplicates were removed. After the subsequent abstract screening, very few articles remained. During the title review and abstract screenings, the authors looked for the key words as well as indications that the articles involved training caregivers and using behavior analysis. Those left underwent full-text review. Permanent products were generated by the first author of all searches and screenings at each level and for each database. The permanent products were shared with the second author for review and confirmation.
Data extraction and synthesis
A form for data extraction was created based on the summary of characteristics charts provided in published telehealth literature reviews (e.g. Ferguson et al. Citation2019; Unholz-Bowden et al. Citation2020), and the form used by the authors in a previous literature review study (Pančocha and Kingsdorf Citation2021). Data extracted included first author and year of publication, and then the 15 targeted components of: (1) location, (2) strategies used via telehealth, (3) child dependent variables (behaviors targeted for change), (4) caregiver dependent variables (behaviors targeted for change), (5) study design, (6) participant characteristics of children, (7) participant characteristics of caregivers, (8) asynchronous telehealth components used, (9) synchronous telehealth components used, (10) technology components used, (11) use of an in situ (in-person) component, (12) whether or not cultural competence was demonstrated (i.e. the intervention was driven by local norms or values), (13) children’s outcomes, (14) caregivers’ outcomes, and (15) social validity outcomes. The data extraction was conducted by the first author and checked by the second author for 33% of the studies, a total of 30 targeted components. The agreement percentage for the coding of data extraction was compared for each targeted component and was calculated by dividing agreements by agreements plus disagreements and multiplying by 100. The intercoder agreement was 100%.
Three tables were created to summarize the components. displays the technical components of the studies including the location, dependent variables, design, and participant characteristics. displays the training strategies and telehealth components. displays the various outcomes for the participants, the assessment of cultural competence, and social validity. All the components are also discussed qualitatively below.
Table 2 Technical components of the studies.
Table 3 Training and telehealth components of the studies.
Table 4 Outcome components of the studies.
Results
Selection of sources of evidence
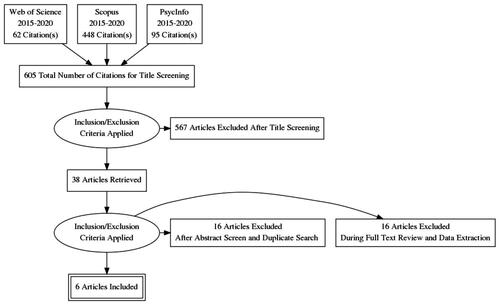
A total of six publications were included in the review. The decision was ultimately made to include the one relevant thesis found, given the very limited amount of research on this topic. A PRISMA flow diagram was created using the PRISMA Flow Diagram Generator tool (http://prisma.thetacollaborative.ca/). The diagram in shows the screening and retrieval process throughout the literature search.
Figure 1. Screening and retrieval process.
Characteristics of Sources of Evidence
Study location and design
The goal of this study was to evaluate research that was conducted in Europe. Despite aiming to inclusively search all countries in Europe, the only European countries with results were Iceland (Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019), Greece, Turkey, Russia, Ukraine (Tsami et al. Citation2019), Albania (Dai et al. Citation2018; Griffiths Citation2020), and Italy (Marino et al. Citation2020). Four of the studies (67%) used single subject experimental designs, all versions of a multiple baseline design (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). Two of the studies (33%) used group designs: randomized controlled trial and a group comparison (Dai et al. Citation2018; Marino et al. Citation2020).
Participants
A total of 72 children completed participation across the six studies. Despite making the search criteria inclusive of all neurodevelopmental disabilities, all the children in the studies had diagnoses of autism. The children ranged in age from 18 months to 13 years old. A total of 95 parents completed participation in the studies. Of those 95 participants, 23 identified as male (22 fathers and one brother) and 72 identified as female (all mothers). The Tsami et al. (Citation2019) study had two male participants, one father and one brother. However, the father and the brother in that study only participated in one generalization probe and were therefore not trained in the intervention. Two fathers participated in the Guðmundsdóttir et al. (Citation2017) study, but only for the assessment and goal setting process, not the training. The remaining male participants were part of the Marino et al. (Citation2020) study; and were fathers that participated fully in the intervention. Therefore, in five out of the six studies (83%) the main parental participants were mothers.
Dependent variables
A mix of direct and indirect assessments of intervention effectiveness was used across the six studies. Four of the studies (67%) included measures of both the caregiver and the child behaviors (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). All four studies (67%) measured the children’s communication responses (e.g. requests or mands). Tsami et al. (Citation2019) additionally measured the challenging behaviors of the children (e.g. aggression). Five of the studies (83%) collected direct assessment data on the behaviors of the caregivers (Dai et al. Citation2018; Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). A fidelity checklist was used to assess the caregivers’ applications of the mand protocol in the Griffiths study (2020). Treatment fidelity data were also collected in the Tsami et al. (Citation2019) study on the caregivers’ procedural fidelity when implementing the functional assessment (FA) and functional communication training (FCT) procedures. The Guðmundsdóttir et al., studies (2017; 2019) collected caregiver data on the number of teaching episodes that they delivered to their children. In the Dai et al. (Citation2018) study, caregiver data were collected on pretest and posttest knowledge assessments. That study additionally collected indirect data on the caregiver-completed assessment tool of the Early Intervention Parenting Self-Efficacy Scale. Similar self-assessment scales were used in the Marino et al., (Citation2020) study: The Home Situation Questionnaire (HSQ-ASD) and the Parental Stress Index (PSI/SF).
Strategies used during telehealth
This article review centered on assessing family-focused behavioral interventions which involved a component delivered via a telehealth modality. Therefore, telehealth was not the intervention in these studies, but rather, a mode for delivering at least a portion of education, training, or intervention to families. The telehealth components used several different strategies. In four of the studies (67%) it was made clear that the parents were taught specific intervention strategies/teaching protocols such as the use of naturalistic teaching methods (Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019), FA and FCT procedures (Tsami et al. Citation2019), and mand (request) training procedures (Griffiths Citation2020). In these studies, ABA-based training techniques were used to train the caregivers. In the Guðmundsdóttir et al., studies (2017; 2019) a specific methodology for training the parents was not stated. However, they appeared to use components of behavioral skills training by incorporating explanation, modelling, positive and corrective feedback, and a written summary of teaching procedures. The Guðmundsdóttir et al., studies (2017; 2019) also included a data review component with the parents during the video conferences including a self-monitoring video review of the parent behaviors in the 2019 study. The Griffiths study (2020) explicitly stated the usage of behavioral skills training, outlining the use of all four steps of instructions, modelling, rehearsal, and feedback. The Tsami et al., study (2019) provided procedural explanations to the parents and then relied on coaching with prompting and prompt fading. In the Marino et al., study (Citation2020) the telehealth component involved coaching parents during individual ABA therapy sessions with their child. The targets or procedures were not made clear but were said to involve assisting parents in interactive play activities with their children. The study by Dai and colleagues (Citation2018) used telehealth to deliver only parent education. The education procedures included the independent learning activities of watching videos, completing activities, vignettes, manuals, and tests.
Telehealth modality and technology
All the studies used a telehealth modality in some way. However, four of the studies (67%) did some in-situ initial assessment or follow-up (Dai et al. Citation2018; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Marino et al. Citation2020). Regardless, telehealth was the main method of intervention delivery.
Five of the six studies (83%) used both asynchronous and synchronous modalities (Dai et al. Citation2018; Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). All the studies used synchronous modalities. These included combinations of real-time video conferencing and telephone calls; with most of the studies using real-time video conferencing (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Marino et al. Citation2020; Tsami et al. Citation2019). The most used asynchronous modality was the use of video recordings, specifically videos sent by the caregivers for the clinicians to review and vice versa (Dai et al. Citation2018; Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). In the Guðmundsdóttir et al. (Citation2017; Citation2019) and the Tsami et al. (Citation2019) studies, though, the teleconference sessions were recorded, and the videos were later watched and scored by the clinicians. Several different hardware components were utilized. Combinations of laptops, desktop computers, smartphones, tablets, and webcams were needed for family participation in five out of the six studies (83%) (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Marino et al. Citation2020; Tsami et al. Citation2019). The one exception was the Dai et al. (Citation2018) study that provided DVDs for the parents to review and conducted audio-only interviews. Video-conferencing software included commonly known tools like Skype, Zoom, Vidyo, and Google platforms. Asynchronous file-sharing was done using Dropbox, the Google platform, and proprietary encrypted systems.
Cultural competence
Since a goal of research, especially research which involves working with families, should be respecting the cultural values and norms of research participants (Bal and Trainor Citation2016), the decision was made to do a cursory assessment of the cultural competence displayed in the studies. Based on previous evaluations of cultural competence in parent training research (Pančocha and Kingsdorf Citation2021), the following components were combined to assess this variable: match between participant native language and information delivery, the development of the intervention with input from the participants and using interventionists that were part of the local community. These components were selected based on the limited cultural information provided in most of the studies. Only the Dai et al. (Citation2018) study explicitly appeared to meet all these criteria. The Guðmundsdóttir et al. (Citation2017; Citation2019) studies appeared to teach in the local language, develop intervention goals with the input of the families and possibly use an interventionist from the local community. However, the last component, the location of the interventionist in relation to the study participants, was not made clear in either article. It should also be noted, that the Guðmundsdóttir et al. (Citation2017) study stated that one of the parental participants was not trained in her native language, but still fluent in the language of instruction. The Tsami et al. (Citation2019) study either provided training in the native language or used translators, and incorporated families into the intervention development. However, it did not appear that the interventionists were currently part of the local community. The Griffiths study (2020) appeared to provide the intervention in the local language and did translate needed materials. The interventionist did not appear to currently be part of the local community. However, it appeared that the items to target for mand training for each child were selected by the parents. The Marino et al. (Citation2020) study did not provide any information regarding these criteria.
Outcomes
All the studies reported favorable outcome measures. Both Guðmundsdóttir et al. (Citation2017; Citation2019) studies demonstrated that parents’ skills of using a naturalistic teaching intervention and their children's communication skills increased as assessed via either visual analysis or percentage of nonoverlapping data (PND). The Tsami et al. (Citation2019) study demonstrated high treatment integrity data (90% or higher). Child problem behaviors (e.g. aggression) decreased and mands (requests) also increased as assessed via visual analysis. The Marino et al. (Citation2020) study conducted numerous statistical tests comparing the telehealth and control groups. Overall, there was a statistically significant positive effect of the telehealth intervention in terms of parents’ stress levels, perception of the disruptive and noncompliant behavior of their children, coping with their children in cases of inadequate behaviors, as well as in the influence on their children’s behavior. The Griffiths (Citation2020) study demonstrated via visual analysis increased fidelity in parents’ use of mand (request) teaching procedures and increases in child mands from baseline to intervention for all dyads. The Dai et al. (Citation2018) study had the least favorable outcomes with the repeated measures ANOVA comparing the telehealth and control groups and showing only minimal differences.
In addition to the above measures, specific social validity or caregiver rating scales of intervention effectiveness and acceptability were targeted in three of the six studies (50%) (Dai et al. Citation2018; Griffiths Citation2020; Tsami et al. Citation2019). The Dai et al. (Citation2018) and Griffiths (Citation2020) studies both used a 5-point Likert-scale questionnaire to assess parent agreement with statements regarding the intervention and had average agreement ratings over 4. The Tsami et al. (Citation2019) study used a similar tool, a 7-point Likert scale where higher scores also indicated a higher level of acceptability and had over 80% of the statements receive average agreement ratings of 5 of higher. The Guðmundsdóttir et al., studies (2017; 2019) did not describe social validity assessment procedures. However, the 2019 study did mention that there were positive anecdotal social validity reports. This was like the Marino et al. Citation2020 study, which did not appear to collect social validity data but did mention anecdotal reports from parents on the value of the training.
Overall evaluation
Specific steps were not taken to evaluate the quality of the studies included in this review, or the overall effectiveness of telehealth interventions for families impacted with autism in Europe. These decisions were made given the small amount of research on this topic. However, certain conclusions can be drawn from looking at this small battery of research. Only one of the studies (17%) used the gold standard of research design: a randomized controlled trial (Marino et al. Citation2020). All the studies had relatively small sample sizes. The single subject experimental design studies did use control measures to demonstrate experimental control by using iterations of the multiple baseline design (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019; Tsami et al. Citation2019). However, again, the limited number of participants in those studies as well as the Dai et al. (Citation2018) study makes the generalizability of the research questionable. While interobserver agreement data were collected in all the studies which used single subject designs, the amount and quality of data collected were not enough for validation in some cases (Griffiths Citation2020; Guðmundsdóttir et al. Citation2017; Guðmundsdóttir et al. Citation2019). Also, while most of the articles were peer-reviewed, the inclusion of a thesis (Griffiths Citation2020) should be considered when evaluating research quality.
Barriers in application of telehealth
Several barriers were noted in the research reviewed. In the Guðmundsdóttir et al. (Citation2017; Citation2019), Tsami et al. (Citation2019), and Dai et al. (Citation2018) studies, high-speed internet access was a challenge for participants. Therefore, the technology usage was kept simple. As a result, in the Dai et al. (Citation2018) study the decision was made to use DVD recordings that were mailed to the families and telephone calls occurred without video. The level of telehealth utilized in the study could be questioned, though. The impact of connectivity was specifically assessed after each video-conferencing session in the Tsami et al. (Citation2019) study, but still impacted several of the families’ abilities to remain in the study. Attrition was a pervasive barrier across all studies. The Dai et al. (Citation2018), Marino et al. (Citation2020), and Tsami et al. (Citation2019) studies all specifically discussed large losses of participants during their research. Another issue was that most of the studies seemingly struggled with recruiting male caregivers, specifically fathers, to actively participate. This could be a barrier to providing the most generalizable outcomes in the home setting. Lastly, most of the studies noted that there was collaboration with professionals based in North America to support their work. While collaboration is valuable, its persistent need throughout the studies highlights Europe’s barrier of access to high quality information and services grounded in the science of behavior and its telehealth modality.
Discussion
Research questions
The goal of this research was to assess the current literature base on behavioral telehealth services for children with neurodevelopmental disabilities in Europe. This review of studies found that a limited number of current works exist in this area. However, of the studies available, Iceland and Albania were the most targeted locations. Children with autism and their mothers were typically the participants. The intervention strategies for training caregivers to implement procedures more often, or with fidelity, frequently used components of behavioral skills training or coaching, to increase their children’s communication responses. Single-subject methodology was used most to assess increases in these measurable behaviors. Video conferencing was the most used telehealth component and had a high level of acceptability. Overall, outcome data, when collected on children and caregiver behaviors were positive. However, several barriers and opportunities for future research exist.
Limitations
A few key limitations exist in this review. One of the main considerations is that only studies in the English language were targeted. However, in most of the countries targeted within Europe the main language spoken is not English. Therefore, studies published in local-language journals were likely missed. While it is important that research is made available in local languages to local communities, also having research available in the global language of English supports the goals of widespread healthcare access for diverse populations throughout the European Union (EU) region (Ledoux et al. Citation2018). With European citizens generally being covered for a broad range of healthcare services within and between countries in the EU, it stands to reason that similar services should be available (Busse et al. Citation2011). Efforts to build a more unified system of telehealth care in the region are likely to be influenced by research conducted within the area and accessible to everyone via a common language.
An additional limitation of this review may be the narrow date range used for the search. With only very recent publications targeted for this review important outcomes of previous studies may have been overlooked. However, this decision was made based on the influx of recent reviews on the broader topic of telehealth as well as the constantly evolving world of technology. This is to say, that older studies may have already been discussed in review articles and may no longer hold relevance in the face of the rapidly changing digital world.
Future research
As discussed by Rispoli and Machalicek (Citation2020), there is a body of quality single-subject research looking at the use of telehealth practices in the behavioral sciences. However, the field is only emerging, needs more empirical validation, and should support ongoing evaluation of constantly advancing technology. In the case of Europe specifically, there appears to be even less research in this arena. While active telepractice programs have roots in Europe, such as the University of Tromso in Norway’s teleconsultation department (Perednia and Allen Citation1995), Italy’s history of experimental telemedicine (Pisanelli et al. Citation1995), and the Balkans’ 18-year-old telemedicine center (Latifi Citation2012), the use of a remote model for behavioral services appears scarce. Only six studies were found during a search of the relevant recent literature. Therefore, there is plenty of room for future research.
When it comes to addressing some of the reoccurring barriers found here, future work might consider looking at creating incentive programs to sustain families’ participation in telehealth services. Research suggests that incentives can increase the participation of individuals in studies even when commitment requirements are difficult (Guyll et al. Citation2003). However, another route to consider when addressing this same barrier is doing an initial assessment of how much time and effort families can contribute and having plans in place to shape parent participation throughout the study (e.g. systematically increase the amount of time committed each week). Shaping procedures have been used to increase the participation behaviors of individuals in different contexts (e.g. Athens et al. Citation2007). The specific issue of male caregiver involvement in parent training interventions is something that persists across the literature (Fabiano Citation2007). Some strategies that should be incorporated into future intervention-based telehealth research are treating fathers as co-parents, increasing fathers’ knowledge and awareness of the intervention participation possibility, training researchers/clinicians to facilitate father-inclusive practices, and upholding high expectations of fathers at the start of the intervention (Lechowicz et al. Citation2019). Digital inequality, as lack of access to reliable high-speed internet, needed hardware, and resultantly information, is an issue that has historically hindered more rural and disadvantaged populations (McLaren and Zappala Citation2002). Future work in behavioral interventions that are delivered to families via telehealth should continue to take into consideration the bandwidth needed to access certain technological modalities, alternative ways to access information in the case of internet malfunctions, and even technology confidence prior to intervention (Salomone and Maurizio Arduino Citation2017).
In addition to the barriers that were noted, other areas of concern were raised that could be addressed in the future. For one, the study quality needs to be more rigorous to build a solid foundation of behavioral telehealth in Europe. Future work should consider increasing the number of study participants, increasing data collection methods to include more outcome measures focusing on direct data collection, extended methods to provide data validation, and increased assessments of social validity to see the impact of the intervention on not just perceived effectiveness but later applications of skills after training. Similar recommendations were echoed in previous reviews (e.g. Akemoglu et al. Citation2020). The area of cultural competence, although looked at only minimally here, is another area for future consideration. Upcoming telehealth interventions should work to form partnerships with their study participants and community; including them in the planning to support intervention buy-in and recruiting local interventionists to support sustainability of the outcomes. Increased reports of these dimensions (i.e. richer descriptions of participant and clinician characteristics, settings, and intervention development) in the research will also help support the external validity.
Lastly, an area that was not looked at in any of these studies, but might be valuable to explore in the future, is the impact of the telehealth model on clinicians. With the noted issues of access to qualified behavior analysts in large parts of Europe, such as in the Czech Republic (e.g. Kingsdorf and Pančocha Citation2020), those currently working in the field are often spread thin and at increased risk of burnout (Plantiveau et al. Citation2018). Creating more widespread and validated models of behavioral telehealth can help ease some of the burden. Research could investigate changes in the number of clients seen over a period, the number of cases held, the differences in intensity of services (e.g. visits/sessions per week) across models, and perhaps even an evaluation of cost-effectiveness.
Conclusions
Overall, the impact of future telehealth research in Europe might not only facilitate the growth of the modality, but also bolster support for the science of behavior analysis. As discussed earlier, in Europe behavior analysis is fighting a war against misinformation and unvalidated treatment practices. Embracing a telehealth model could increase access to care, improve family outcomes, and foster dissemination. The modality multiplies the reach of the few qualified practitioners who are working on the ground providing traditional in-person services. If created systematically and sustainably their impact can be spread across greater distances. Establishing research-driven behavioral telehealth guidelines on the continent could be the catalyst for future legislation surrounding comprehensive access to ABA-based services.
It appears that telehealth is a viable option for delivering behavior analytic support to families impacted by neurodevelopmental disabilities in Europe. While there is limited research in this region, what is available seems to align with what has been found in North America. Our conclusions here echo that there is a high level of parental acceptability for behavioral telehealth (Unholz‐Bowden et al., 2020), that providing services even in the face of low-speed internet conditions is possible with the right practices (Oberleitner et al. Citation2004), and that behavioral improvements are possible for both caregivers and children (Akemoglu et al. Citation2020). The match between the conclusions of our study and the works of others in North America, as well as additional work that has demonstrated the ability of telehealth applications to be culturally adapted to the broader world context (Sivaraman and Fahmie Citation2020), bodes well for the future of behavioral telehealth in Europe. The need, empirical validation, and groundwork for sustainability already seem to exist- so now the work on policy, procedures, and future research needs to happen.
Disclosure statement
The authors have no conflict of interest or disclosures to declare.
Additional information
Funding
References
- Akemoglu, Y., Muharib, R. and Meadan, H. 2020. A systematic and quality review of parent-implemented language and communication interventions conducted via telepractice. Journal of Behavioral Education, 29, 282–316. doi: 10.1007/s10864-019-09356-3.
- Association for Behavior Analysis International. 2018. Verified course sequence handbook. Retrieved September 23, 2019, from Abainternational.org website: https://www.abainternational.org/media/155079/abai_vcs_handbook_2018.pdf
- Athens, E. S., Vollmer, T. R. and Pipkin, C. C. S. P. 2007. Shaping academic task engagement with percentile schedules. Journal of Applied Behavior Analysis, 40, 475–488.
- Bal, A. and Trainor, A. A. 2016. Culturally responsive experimental intervention studies: The development of a rubric for paradigm expansion. Review of Educational Research, 86, 319–359.
- Barbera, M. L. 2007. The verbal behavior approach: How to teach children with autism and related disorders. London: Jessica Kingsley Publishers.
- Bashshur, R. L. and Shannon, C. W. 2009. History of telemedicine: Evolution, context, and transformation. New Rochelle: Mary Ann Liebert, Inc.
- Behavior Analyst Certification Board. 2021a. BACB certificant registry. https://www.bacb.com/services/o.php?page=101135&s=1
- Behavior Analyst Certification Board. 2021b. Board certified behavior analyst handbook. Littleton, CO: Author
- Behavior Change Institute. 2020. Telehealth research summaries. https://casproviders.org/wp-content/uploads/2020/03/Behavior-Change-Institute-Telehealth-Research-Summaries.pdf
- Borgi, M., Ambrosio, V., Cordella, D., Chiarotti, F. and Venerosi, A. 2019. Nationwide survey of healthcare services for autism spectrum disorders (ASD) in Italy. Advances in Neurodevelopmental Disorders, 3, 306–318.
- Boutain, A. R., Sheldon, J. B. and Sherman, J. A. 2020. Evaluation of a telehealth parent training program in teaching self-care skills to children with autism. Journal of Applied Behavior Analysis, 53, 1259–1275.
- Bhaskar, S., Bradley, S., Chattu, V. K., Adisesh, A., Nurtazina, A., Kyrykbayeva, S., Sakhamuri, S., Yaya, S., Sunil, T., Thomas, P., Mucci, V., Moguilner, S., Israel-Korn, S., Alacapa, J., Mishra, A., Pandya, S., Schroeder, S., Atreja, A., Banach, M. and Ray, D. 2020. Telemedicine across the globe-position paper from the COVID-19 pandemic health system resilience PROGRAM (REPROGRAM) international consortium (Part 1). Frontiers in Public Health, 8, 556720. doi: 10.3389/fpubh.2020.556720
- Brockes, C., Grischott, T., Dutkiewicz, M. and Schmidt-Weitmann, S. 2017. Evaluation of the education “Clinical Telemedicine/e-Health” in the curriculum of medical students at the University of Zurich. Telemedicine and e-Health, 23, 899–904.
- Busse, R., van Ginneken, E. and Wörz, M. 2011. Crossborder healthcare in the European Union: Mapping and analyzing practices and policies. M. Wismar, W. Palm, J. Figueras, K. Ernst, E. van Ginneken, Eds. Regional Office for Europe: World Health Organization. https://apps.who.int/iris/handle/10665/327961
- Cason, J. 2014. Telehealth: A rapidly developing service delivery model for occupational therapy. International Journal of Telerehabilitation, 6, 29–35.
- Chung, M. Y., Meadan, H., Snodgrass, M. R., Hacker, R. E., Sands, M. M., Adams, N. B. and Johnston, S. S. 2020. Assessing the social validity of a telepractice training and coaching intervention. Journal of Behavioral Education, 29, 327–382.
- Council of Autism Service Providers 2020. Practice parameters for telehealth-implementation of applied behavior analysis: Continuity of care during COVID-19 pandemic. Wakefield, MA: Author.
- Crico, C., Renzi, C., Graf, N., Buyx, A., Kondylakis, H., Koumakis, L. and Pravettoni, G. 2018. mHealth and telemedicine apps: In search of a common regulation. ecancermedicalscience, 12, 853. doi: 10.3332/ecancer.2018.853
- Dai, Y. G., Brennan, L., Como, A., Hughes-Lika, J., Dumont-Mathieu, T., Rathwell, I. C., Minxhozi, O., Aliaj, B. and Fein, D. A. 2018. A video parent-training program for families of children with autism spectrum disorder in Albania. Research in Autism Spectrum Disorders, 56, 36–49.
- Daniels, A. M., Como, A., Hergüner, S., Kostadinova, K., Stosic, J. and Shih, A. 2017. Autism in Southeast Europe: A survey of caregivers of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 47, 2314–2325.
- Dillenburger, K. 2011. The Emperor's new clothes: Eclecticism in autism treatment. Research in Autism Spectrum Disorders, 5, 1119–1128.
- Eid, A. M., Aljaser, S. M., AlSaud, A. N., Asfahani, S. M., Alhaqbani, O. A., Mohtasib, R. S., Aldhalaan, H. M. and Fryling, M. 2017. Training parents in Saudi Arabia to implement discrete trial teaching with their children with autism spectrum disorder. Behavior Analysis in Practice, 10, 402–406.
- eHealth Stakeholder Group. 2014. Widespread deployment of telemedicine services in Europe. European Commission. https://ec.europa.eu/information_society/newsroom/cf/dae/document.cfm? doc_id=5167
- Fabiano, G. A. 2007. Father participation in behavioral parent training for ADHD: Review and recommendations for increasing inclusion and engagement. Journal of Family Psychology : JFP : Journal of the Division of Family Psychology of the American Psychological Association (Division 43), 21, 683–693.
- Ferguson, J., Craig, E. A. and Dounavi, K. 2019. Telehealth as a model for providing behaviour analytic interventions to individuals with Autism Spectrum Disorder: A systematic review. Journal of Autism and Developmental Disorders, 49, 582–616.
- Gardiner, E., Miller, A. R. and Lach, L. M. 2018. Family impact of childhood neurodevelopmental disability: Considering adaptive and maladaptive behaviour. Journal of Intellectual Disability Research : JIDR, 62, 888–899.
- Gillen, E. and Keenan, M. 2018. When policy decisions for autism treatment in Europe are hijacked by a category mistake. Psichologija, 56, 72–78.
- Griffiths, F. 2020. The effects of telehealth training on parents of children with autism in Albania. Unpublished Thesis. Brigham Young University, Utah.
- Grigorenko, E., Torres, S., Lebedeva, E. I. and Bondar, Y. A. 2018. Evidence-based interventions for ASD: A focus on applied behavior analysis (ABA) interventions. Psychology. Journal of Higher School of Economics, 15, 711–727.
- Guðmundsdóttir, K., Ala’i-Rosales, S. and Sigurðardóttir, Z. G. 2019. Extending caregiver training via telecommunication for rural Icelandic children with autism. Rural Special Education Quarterly, 38, 26–42.
- Guðmundsdóttir, K., Sigurðardóttir, Z. G. and Ala'i-Rosales, S. 2017. Evaluation of caregiver training via telecommunication for rural Icelandic children with autism. Behavioral Development Bulletin, 22, 215–229.
- Guyll, M., Spoth, R. and Redmond, C. 2003. The effects of incentives and research requirements on participation rates for a community-based preventive intervention research study. The Journal of Primary Prevention, 24, 25–41.
- Harvey, A. C., Harvey, M. T., Kenkel, M. B. and Russo, D. C. 2010. Funding of applied behavior analysis services: Current status and growing opportunities. Psychological Services, 7, 202–212.
- Hashiguchi, T. O. 2020. Bringing health care to the patient: An overview of the use of telemedicine in OECD countries. OECD Health Working Papers, 116. OECD Publishing, Paris, https://doi.org/10.1787/8e56ede7-en.
- Hughes, C. J. and Shook, G. L. 2007. Training and certification of behaviour analysts in Europe: Past, present, and future challenges. European Journal of Behavior Analysis, 8, 239–249.
- Kansas Health Institute 2014. Specialists in South Dakota use telehealth system to give ER care in Kansas. https://www.khi.org/news/article/specialists-south-dakota-use-telehealth-system-giv
- Keenan, M., Dillenburger, K., Moderato, P. and Röttgers, H. R. 2010. Science for sale in a free market economy: But at what price? ABA and the treatment of autism in Europe. Behavior and Social Issues, 19, 126–143.
- Keenan, M., Dillenburger, K., Röttgers, H. R., Dounavi, K., Jónsdóttir, S. L., Moderato, P., Schenk, J. J. A. M., Virués-Ortega, J., Roll-Pettersson, L. and Martin, N. 2015. Autism and ABA: The gulf between North America and Europe. Review Journal of Autism and Developmental Disorders, 2, 167–183.
- Kelly, M., Martin, N., Dillenburger, K., Kelly, A. and Miller, M. M. 2019. Spreading the news: History, successes, challenges and the ethics of effective dissemination. Behavior Analysis in Practice, 12, 440–451.
- Kingsdorf, S. and Pančocha, K. 2020. A survey of the use of applied behaviour analysis for children with autism in the Czech Republic. European Journal of Special Needs Education, 35, 1–12.doi: 10.1080/08856257.2020.1726092
- Latifi, R. 2012. Using telemedicine to strengthen medical systems in limited-resource countries. Bulletin of the American College of Surgeons, 97, 15–21.
- LeBlanc, L. A., Lerman, D. C. and Normand, M. P. 2020. Behavior analytic contributions to public health and telehealth. Journal of Applied Behavior Analysis, 53, 1208–1218.
- Lechowicz, M. E., Jiang, Y., Tully, L. A., Burn, M. T., Collins, D. A. J., Hawes, D. J., Lenroot, R. K., Anderson, V., Doyle, F. L., Piotrowska, P. J., Frick, P. J., Moul, C., Kimonis, E. R. and Dadds, M. R. 2019. Enhancing father engagement in parenting programs: Translating research into practice recommendations. Australian Psychologist, 54, 83–89.
- Ledoux, C., Pilot, E., Diaz, E. and Krafft, T. 2018. Migrants' access to healthcare services within the European Union: a content analysis of policy documents in Ireland, Portugal and Spain. Globalization and Health, 14, 57.
- Lee, J. F., Schieltz, K. M., Suess, A. N., Wacker, D. P., Romani, P. W., Lindgren, S. D., Kopelman, T. G. and Dalmau, Y. C. P. 2015. Guidelines for developing telehealth services and troubleshooting problems with telehealth technology when coaching parents to conduct functional analyses and functional communication training in their homes. Behavior Analysis in Practice, 8, 190–200.
- Lee, S. H., Simpson, R. L. and Shogren, K. A. 2007. Effects and implications of self-management for students with autism: A meta-analysis. Focus on Autism and Other Developmental Disabilities, 22, 2–13.
- Lindgren, S., Wacker, D., Schieltz, K., Suess, A., Pelzel, K., Kopelman, T., Lee, J., Romani, P. and O'Brien, M. 2020. A randomized controlled trial of functional communication training via Telehealth for Young Children with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders, 50, 4449–4462.
- Lollar, D. J., Hartzell, M. S. and Evans, M. A. 2012. Functional difficulties and health conditions among children with special health needs. Pediatrics, 129, e714–e722.
- Manohar, H., Kandasamy, P., Chandrasekaran, V. and Rajkumar, R. P. 2019. Brief parent-mediated intervention for children with autism spectrum disorder: A feasibility study from South India. Journal of Autism and Developmental Disorders, 49, 3146–3158.
- Marino, F., Chilà, P., Failla, C., Crimi, I., Minutoli, R., Puglisi, A., Arnao, A. A., Tartarisco, G., Ruta, L., Vagni, D. and Pioggia, G. 2020. Tele-assisted behavioral intervention for families with children with autism spectrum disorders: A randomized control trial. Brain Sciences, 10, 649. doi: 10.3390/brainsci10090649
- McLaren, J. and Zappala, G. 2002. The digital divide among financially disadvantaged families in Australia. First Monday, 7. http://firstmonday.org/issues/issue7_11/mclaren/index.html
- McLay, L., Sutherland, D., Machalicek, W. and Sigafoos, J. 2020. Systematic review of telehealth interventions for the treatment of sleep problems in children and adolescents. Journal of Behavioral Education, 29, 222–245.
- Meadan, H. and Daczewitz, M. E. 2015. Internet-based intervention training for parents of young children with disabilities: A promising service-delivery model. Early Child Development and Care, 185, 155–169.
- Mello, M. P., Goldman, S. E., Urbano, R. C. and Hodapp, R. M. 2016. Services for children with autism spectrum disorder: Comparing rural and non-rural communities. Education and Training in Autism and Developmental Disabilities, 51, 355–365.
- Molini-Avejonas, D. R., Rondon-Melo, S., de La Higuera Amato, C. A. and Samelli, A. G. 2015. A systematic review of the use of telehealth in speech, language and hearing sciences. Journal of Telemedicine and Telecare, 21, 367–376.
- Montiel-Nava, C., Cukier, S., Garrido, G., Valdez, D., Paula, C. S., García, R., Rosoli, A., Irarrázaval, M. and Rattazzi, A. 2020. Service encounters across the lifespan in individuals with autism spectrum disorders: Results from a multisite study in Latin America. Research in Autism Spectrum Disorders, 79, 101670.
- Myers, S. M., and Johnson, C. P. 2007. Management of children with autism spectrum disorders. Pediatrics, 120, 1162–1182.
- National Center for Immunization and Respiratory Diseases (NCIRD), Division of Viral Diseases. (2020, June 10). Using telehealth to expand access to essential health services during the COVID-19 pandemic. https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html
- Neely, L., Hong, E. R., Kawamini, S., Umana, I. and Kurz, I. 2020. Intercontinental telehealth to train Japanese interventionists in incidental teaching for children with autism. Journal of Behavioral Education, 29, 1–16.doi: 10.1007/s10864-020-09377-3
- Neely, L., MacNaul, H., Gregori, E. and Cantrell, K. 2021. Effects of telehealth‐mediated behavioral assessments and interventions on client outcomes: A quality review. Journal of Applied Behavior Analysis, 54, 484–510.
- Oberleitner, R., Laxminarayan, S., Suri, J., Harrington, J. and Bradstreet, J. 2004. September). The potential of a store and forward tele-behavioral platform for effective treatment and research of autism. In The 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (Vol. 2, pp. 3294–3296. ). .Ieee
- Ontario Telehealth Network. 2013. Embarking on the journey for virtual care: 2012/13 annual report. https://support.otn.ca/sites/default/files/otn-annual-report-2012-13.pdf
- Pančocha, K. and Kingsdorf, S. 2021. A review of the components, outcomes, and cultural responsiveness of the pyramidal parent training literature. Child & Family Behavior Therapy.doi: 10.1080/07317107.2021.1895412.
- Pantermuehl, R. M. and Lechago, S. A. 2015. A comparison of feedback provided in vivo versus an online platform on the treatment integrity of staff working with children with autism. Behavior Analysis in Practice, 8, 219–222.
- Pennefather, J., Hieneman, M., Raulston, T. J. and Caraway, N. 2018. Evaluation of an online training program to improve family routines, parental well-being, and the behavior of children with autism. Research in Autism Spectrum Disorders, 54, 21–26.
- Perednia, D. A. and Allen, A. 1995. Telemedicine technology and clinical applications. JAMA, 273, 483–488.
- Pisanelli, D. M., Ricci, F. L. and Maceratini, R. 1995. A survey of telemedicine in Italy. Journal of Telemedicine and Telecare, 1, 125–130.
- Plantiveau, C., Dounavi, K. and Virués-Ortega, J. 2018. High levels of burnout among early-career board-certified behavior analysts with low collegial support in the work environment. European Journal of Behavior Analysis, 19, 195–207.
- Pollak, Y. 2016. Is applied behavior analysis education, medicine, or both: A study of the funding challenges that accompany an autism diagnosis. Seton Hall Law Review, 47, 267–296.
- Raposo, V. L. 2016. Telemedicine: The legal framework (or the lack of it) in Europe. GMS Health Technology Assessment, 12, Doc03. doi: 10.3205/hta000126.
- Rios, D., Schenk, Y. A., Eldridge, R. R. and Peterson, S. M. 2020. The effects of remote behavioral skills training on conducting functional analyses. Journal of Behavioral Education, 29, 449–468.
- Rispoli, M. and Machalicek, W. 2020. Advances in telehealth and behavioral assessment and intervention in education: Introduction to the special issue. Journal of Behavioral Education, 29, 189–194.
- Ritzema, A. M., Lach, L. M., Rosenbaum, P. and Nicholas, D. 2016. About my child: Measuring ‘complexity’ in neurodisability. Evidence of reliability and validity. Child: Care, Health and Development, 42, 402–409.
- Rodriguez, K. A. 2020. Maintaining treatment integrity in the face of crisis: A treatment selection model for transitioning direct ABA services to telehealth. Behavior Analysis in Practice, 13, 291–298.
- Roll-Pettersson, L., Gena, A., Eldevik, S., Moderato, P., Sigurdardottir, Z. G., Dillenburger, K., Keenan, M. and Ala’i-Rosales, S. 2020. Higher education and behavior analysis in Europe: Creating a unified approach for the training of autism professionals. European Journal of Behavior Analysis, 21, 158–184.
- Rosenberg, N. E., Artman-Meeker, K., Kelly, E. and Yang, X. 2020. The effects of bug-in-ear coaching package on implementation of incidental teaching by paraprofessionals in a K-12 school. Journal of Behavioral Education, 29, 409–432.
- Ruparelia, K., Abubakar, A., Badoe, E., Bakare, M., Visser, K., Chugani, D. C., Chugani, H. T., Donald, K. A., Wilmshurst, J. M., Shih, A., Skuse, D. and Newton, C. R. 2016. Autism spectrum disorders in Africa: Current challenges in identification, assessment, and treatment: A report on the International child neurology association meeting on ASD in Africa, Ghana, April 3-5, 2014. Journal of Child Neurology, 31, 1018–1026.
- Salomone, E., Beranová, Š., Bonnet-Brilhault, F., Briciet Lauritsen, M., Budisteanu, M., Buitelaar, J., Canal-Bedia, R., Felhosi, G., Fletcher-Watson, S., Freitag, C., Fuentes, J., Gallagher, L., Garcia Primo, P., Gliga, F., Gomot, M., Green, J., Heimann, M., Jónsdóttir, S. L., Kaale, A., Kawa, R., Kylliainen, A., Lemcke, S., Markovska-Simoska, S., Marschik, P. B., McConachie, H., Moilanen, I., Muratori, F., Narzisi, A., Noterdaeme, M., Oliveira, G., Oosterling, I., Pijl, M., Pop-Jordanova, N., Poustka, L., Roeyers, H., Rogé, B., Sinzig, J., Vicente, A., Warreyn, P. and Charman, T. 2016. Use of early intervention for young children with autism spectrum disorder across Europe. Autism : The International Journal of Research and Practice, 20, 233–249.
- Salomone, E., Kutlu, B., Derbyshire, K., McCloy, C., Hastings, R. P., Howlin, P. and Charman, T. 2014. Emotional and behavioural problems in children and young people with autism spectrum disorder in specialist autism schools. Research in Autism Spectrum Disorders, 8, 661–668.
- Salomone, E. and Maurizio Arduino, G. 2017. Parental attitudes to a telehealth parent coaching intervention for autism spectrum disorder. Journal of Telemedicine and Telecare, 23, 416–420.
- Schepis, M. M., Reid, D. H., Behrmann, M. M. and Sutton, K. A. 1998. Increasing communicative interactions of young children with autism using a voice output communication aid and naturalistic teaching. Journal of Applied Behavior Analysis, 31, 561–578.
- Shook, G. L. and Neisworth, J. T. 2005. Ensuring appropriate qualifications for applied behavior analyst professionals: The Behavior Analyst Certification Board. Exceptionality, 13, 3–10.
- Sivaraman, M. and Fahmie, T. A. 2020. A systematic review of cultural adaptations in the global application of ABA-based telehealth services. Journal of Applied Behavior Analysis, 53, 1838–1855.
- Smith, C. J., Rozga, A., Matthews, N., Oberleitner, R., Nazneen, N. and Abowd, G. 2017. Investigating the accuracy of a novel telehealth diagnostic approach for autism spectrum disorder. Psychological Assessment, 29, 245–252.
- Smith, T. 2001. Discrete trial training in the treatment of autism. Focus on Autism and Other Developmental Disabilities, 16, 86–92.
- Taj-Eldin, M., Ryan, C., O’Flynn, B. and Galvin, P. 2018. A review of wearable solutions for physiological and emotional monitoring for use by people with autism spectrum disorder and their caregivers. Sensors, 18, 4271.
- Tiger, J. H., Hanley, G. P. and Bruzek, J. 2008. Functional communication training: A review and practical guide. Behavior Analysis in Practice, 1, 16–23.
- Tomlinson, S. R., Gore, N. and McGill, P. 2018. Training individuals to implement applied behavior analytic procedures via telehealth: A systematic review of the literature. Journal of Behavioral Education, 27, 172–222.
- Tsami, L., Lerman, D., and Toper‐Korkmaz O. 2019. Effectiveness and acceptability of parent training via telehealth among families around the world. Journal of Applied Behavior Analysis, 52, 1113–1129.
- Unholz-Bowden, E., McComas, J. J., McMaster, K. L., Girtler, S. N., Kolb, R. L. and Shipchandler, A. 2020. Caregiver training via telehealth on behavioral procedures: A systematic review. Journal of Behavioral Education, 29, 246–281.
- U.S. Surgeon General. 2001. Mental health a report of the surgeon general. Department of Health and Human Services. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health, Retrieved from http://www.allianceforschoolchoice.org
- Virués-Ortega, J. 2010. Applied behavior analytic intervention for autism in early childhood: Meta-analysis, meta-regression and dose-response meta-analysis of multiple outcomes . Clinical Psychology Review, 30, 387–399.
Appendix 1.
The search strategy used in the web of science database