
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Introduction: The coronavirus pandemic has swept across the United Kingdom (UK). Given the ever-evolving situation, little is known about the repercussions of coronavirus and the subsequent lockdowns for children diagnosed with Autism Spectrum Disorder (ASD). Therefore, this study explores the social-communicative impact of the first lockdown (March 2020 – July 2020) in the UK and the return to school period (September 2020 – October 2020), following prolonged disruption to routine, in children diagnosed with ASD. Methods: Parents of autistic children completed 2 separate online surveys following the first lockdown in the UK (n = 176) and also when children returned to school following the summer break (n = 54). Results: The results suggested that self-regulation skills (p < .05) and co-operation skills (p < .05) were most affected over the course of the lockdown. Children’s physical activity levels were perceived to significantly increase during the return to school (p < .0001), which was associated with better social-communication outcomes (p < .05). Conclusion: Future work is needed to confirm and explore the findings. Such work could be implemented to protect and improve the social-communicative outcomes of autistic children.
Introduction
Coronavirus
The current coronavirus (COVID-19) pandemic has spread rapidly across the world, causing much stress and uncertainty for all. Whilst medical doctors, researchers, epidemiologists, chemists, and many others work tirelessly to find an end to COVID-19, the short- and long-term impacts of the pandemic for certain populations, such as those living with physical or mental disabilities, seem somewhat overlooked (Crane et al. Citation2021). A saying that epitomises the current situation is – ‘We may all be in the same storm, but we do not all have the same boats’ (Barr, Citationn.d.).
On March 23rd the United Kingdom’s (UK) Government imposed a nationwide lockdown; requiring everyone to remain within the four walls of their home, unless for essential trips to the shops or pharmacy, essential work, and limited exercise. The introduction of social distancing, which is now referred to as ‘physical distancing’, caused families and friends to not see each other for months, hospital and social care visits to be cancelled, and restaurants, pubs, and clubs to close (Aminnejad and Alikhani Citation2020). Alongside the majority of public and hospitality sectors being forced to close, many schools closed their doors, only remaining open for vulnerable pupils, special education needs and disability (SEND) children, and those of key workers during the first nationwide lockdown. It is believed school closures have now affected over 80% of children worldwide (Lancker and Parolin Citation2020) and the school closures across the UK could have had detrimental educational and social consequences for children across the country (Dorn et al. Citation2020). For many children, these consequences are likely to be exacerbated when living in poverty or with a disability (Lancker and Parolin Citation2020).
Coronavirus and autistic children
Autism Spectrum Disorder (ASD) is the medical term used to describe common neurodevelopmental conditions characterised by chronic social communication challenges and restricted, repetitive, and inflexible patterns of behaviour, interests, and activities (Bell Citation1994, Lyall et al. Citation2017). Although we appreciate some individuals prefer the term Autism Spectrum Condition, we have decided to use the term ASD to fit in line with the National Health Service’s description (NHS Citation2019). Additionally, we have opted to use both the identity-first language and person-first language, for describing an autistic individual, interchangeably throughout the manuscript (Kenny et al. Citation2016).
Understandably, given the ever-evolving situation, little is known about the repercussions of COVID-19 and the subsequent lockdown for children diagnosed with ASD. However, the hallmark features of ASD put autistic children at greater risk of being negatively impacted by the COVID-19 pandemic (Bellomo et al. Citation2020). Already experiencing significant deficits in social-communicative behaviours, the resultant lockdown and change to routine may have imparted unique difficulties for autistic children.
It is currently estimated that one in every 100 children in the UK has an ASD diagnosis (Green et al. Citation2005). The recent COVID-19 pandemic has greatly altered how local communities and the wider global society operate, impacting many of these autistic children and their families, alongside clinical autism services and research progress (Amaral and de Vries Citation2020). Since the onset of the first lockdown in the UK, the required practical aid for the physical, social and educational needs of ASD children has not been reached, or at least not at the level it was pre-pandemic (Narzisi Citation2020). The very nature of social isolation during the lockdown made immersing autistic children in caring, supportive environments that gently challenged their social development near impossible to do with anyone other than their immediate family members (Bellomo et al. Citation2020). Therefore, the disruption to schools, minimised contact with peers, and reduced face-to-face support may have worsened the social communication challenges already experienced by a larger number of children living with ASD. In contrast, a recent study by Renzo et al. (Citation2020) indicated that despite behavioural problems worsening and symptomology intensifying in autistic children during the pandemic, parents reported improvements in their communicative relationships with their children. As a result, it is unclear what the actual impact of COVID-19 and the lockdowns may have been, and continue to be, for children diagnosed with ASD. Therefore, research priorities such as attempting to understand the impact of COVID-19, whether positive or negative, on the social development of autistic children are needed (Amaral and de Vries Citation2020).
Coronavirus, autistic children, and physical activity
Physical distancing and the ‘stay‐at‐home’ orders issued in cities across the globe reduced the opportunities for physical activity among children. Although the UK government allowed individuals to partake in one daily exercise routine outside during the height of the first lockdown, they placed a strong emphasis on walking, jogging, and running. It is recognised that most children are more likely to engage in physical activity through play; for example, chasing, climbing, or scooting, than they are through a linear activity like jogging (Russell and Stenning Citation2020). Therefore, engaging in exercise may have been difficult for many children during the height of the pandemic in the UK. In addition, sedentary activities and screen-time increased as a result of the viral outbreak, with the available evidence demonstrating that online video gaming usage in children soared due to the lockdown measures (Rundle et al. Citation2020).
Previous research indicates that low levels of physical activity and inactive behaviour can have particularly adverse effects on the quality of life, health, and well-being of children diagnosed with ASD (Ferreira et al., Citation2018, Jones et al. Citation2017). Further, increasing levels of physical activity has been linked with improving social development and enhancing communication skills in autistic children (Best Citation2010, Lang et al. Citation2010, Lee and Vargo Citation2017, Sam et al. Citation2015). The reported increase in sedentary activity and limited opportunity for play and physical activity may have had worse effects for children diagnosed with ASD, in comparison to their typically-developing peers (Jones et al. Citation2017). Therefore, it is important to understand whether levels of physical activity in autistic children have also changed since the outbreak of the pandemic.
Aims and hypotheses
The main aims of this study were to understand the impacts of the COVID-19 pandemic, the subsequent lockdown, and return to school period, on the social development and communication skills of autistic children in the UK from their parents' perspective and to examine if any associations exist between social-communicative behaviours and the variables affected by the lockdown or return to school period. Based on previous research and commentaries we have four main hypotheses:
Social development and communication skills will have worsened during the lockdown period (Amaral and de Vries Citation2020, Colizzi et al. Citation2020, Holt-Lunstad et al. Citation2010) and more parents will have noticed a worsening of social-communicative behaviours than an improvement or no change in social behaviours during the lockdown than during the return to school period (H1).
Based on parental ratings; social-communicative behaviours will have significantly improved since returning to school in comparison to the end of lockdown (H2).
Physical activity levels will have increased since returning to school, in comparison to the end of lockdown (H3).
Decreased levels of physical activity, not attending school regularly, not feeling supported by the school, and not seeing people outside of school/outside the household will be associated with detrimental changes in social-communicative scores during the lockdown and also during the return school period (H4). For example, more parents of children, who did not regularly attend school during the lockdown, will report a worsening of social-communicative behaviours during the lockdown, in comparison to parents of children who did regularly attend school.
Methods
Recruitment and participants
Ethical approval for the study was given by the Science and Health Ethics sub-committee at the University of Essex prior to starting the recruitment phase. During recruitment, a database of known autism charities, schools, and support groups within the UK was created. Organisations were then contacted via email, inviting them to distribute our questionnaire to parents of autistic children. Emails were addressed to the recipient and a brief description of the research project was given.
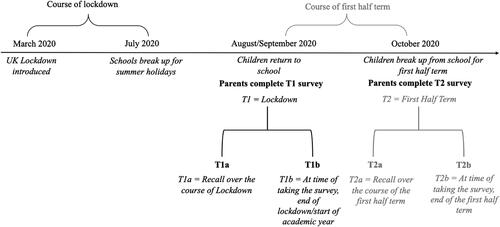
There were two rounds of data collection within the study. The first round of data collection, time-point 1 (T1), was concerned with social-communication scores of the child over the course of lockdown (T1a), and at the time the parent completed the questionnaire (T1b). The second round of data collection, time-point 2 (T2), was concerned with social-communication scores of the child during the course of the first half-term of the 2020/2021 academic year (T2a), and at the time the parent completed the questionnaire (T2b; see ). Data collection ran for 3 weeks in 2020 during the end of August/start of September for T1, and then for 2 weeks during the end of October 2020 for T2.
Figure 1. Schematic timeline of the two main time-points included in this study, including how data collection was split during the two time-points.
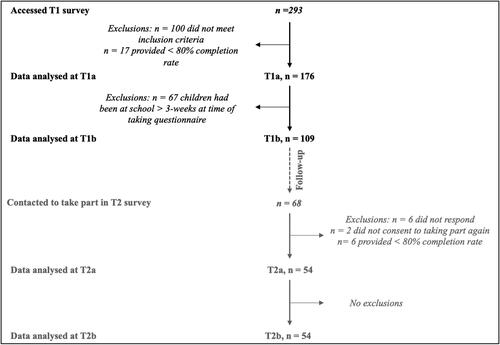
Before completing the questionnaires, all respondents were required to give their informed consent to participating online by answering a Yes/No checkbox. Over 293 participants accessed the questionnaire at T1 and of those, 193 met the inclusion criteria and provided some kind of response. Only those who consented, met the inclusion criteria, and provided at least an 80% partial response were included in the analysis (n = 176).
Participants who wished to take part in the study at T2 were contacted via an email they had given in the T1 questionnaire. Only sixty-eight respondents agreed to be contacted for the follow-up study; as a result, significantly fewer parents participated in the follow-up questionnaire, in comparison to the T1 questionnaire. Sixty-two parents from across the UK, who had previously taken part in the T1 questionnaire, accessed the follow-up questionnaire. Of these responses, 2 parents did not agree to participate in the questionnaire again and 6 responses did not reach the 80% completion threshold. Subsequently, 54 responses were used in the analysis of T2, providing a 31% retention rate. See for a flow diagram of participants.
Figure 2. Flow diagram for the number of responses used in the data analysis for T1 and T2.
Materials
Participants completed online questionnaires, which were created on the QualtricsTM platform (Qualtrics Citation2005, Provo, UT). Online questionnaires allow for enhanced access to geographically dispersed participants, increased participant safety, anonymity, and greater flexibility for scheduling, which were all important factors for our sample population (Drabble et al. Citation2016, Evans and Mathur Citation2005).
The questionnaires were split into 4 main sections. The first section asked simple socio-demographic questions before moving on to the second section, which explored five main factors that lockdown (T1) and the return to school (T2) may have affected. These included: 1) school attendance (yes/no), 2) support from school (yes/no), 3) access to family and friends (yes/no), 4) additional support (private therapy) (yes/no), and 5) change to levels of physical activity; as rated on 3-point Likert scale (1 – decreased, 2 – no change, and 3 – increased).
The third and fourth sections collected relevant information regarding how the social/communication skills of children diagnosed with ASD may have changed during the course of the lockdown, from March 24th (the start of lockdown) up until the ∼22nd of July (when most schools in the UK broke up for the summer holiday), and then how communication skills were at the time of taking the questionnaire. The follow-up questionnaire collected information on how social-communicative skills may have changed during the course first half term of the 20/21 academic year (∼1st September 2020 to ∼26th October 2020) and then how communication skills were at the time of taking the questionnaire.
The questions focused on three important subdomains of social development that are commonly observed to be affected in ASD, including: 1) communication skills (Chin and Bernard-Opitz Citation2000), 2) self-regulation skills (Loveland Citation2005), and 3) co-operation skills (Colombi et al. Citation2009, Jahr et al. Citation2000). Seven questions were formed for each subdomain, which were inspired by elements of already validated questionnaires that have been previously used to assess social-communication capabilities, including the Conversation Skills Rating Scale (Spitzberg Citation1995) for assessment of communication skills, Strengths and Difficulties Questionnaire (Goodman Citation1997) for assessment of self-regulation skills, and the Preschool and Kindergarten Behaviour Scale (Merrell Citation1994) for assessment of co-operation skills. All three standardised assessments were observed to have good internal consistency over and above 0.70 (Giannakopoulos et al. Citation2013, Shokri et al. Citation2013, Stone et al. Citation2015).
Parents were asked to rate whether they believed their child’s skills within each subdomain had: 1 – Got a lot worse, 2 – Got a little worse, 3 – Not changed, 4 – Got a little better, or 5 – Got a lot better, over the course of lockdown (T1a) and over the course of the first half-term (T2a). Then, parents were asked to score their child’s social skills currently at the time of taking both questionnaires (T1b and T2b), based on a 5-point Likert scale, where: 1 – Poor, 2 – Below average, 3 – Average, 4 – Good, and 5 – Excellent.
Data analysis
We initially calculated descriptive statistics of the socio-demographic data and social communication scores separately for each time-point using SPSS (IBM SPSS Statistics Citation2017). An average score was calculated for each child, in each social skill (communication, self-regulation and co-operation) for perceived change in social skill and perceived competence of social skill at the time of taking the questionnaire, at both time-points. To analyse the effect of lockdown and the return to school period on the change in autistic children’s social and communicative skills we performed a chi-squared test between each social-communication skill assessed and the two time-points of interest, separately. In addition, we performed a two-way, repeated-measures, mixed-model (due to missing values) ANOVA between the average parental rating scores for each social communication skill at the time of taking the questionnaire, with time-point as the between-group factor and social skill as the within-subject factor. Tukey posthoc was performed when ANOVA suggested significance (p < .05).
We also performed an unpaired, nonparametric t-test (Mann–Whitney U test) to assess if levels of physical activity significantly differed between time-points. To examine the effect of physical activity on change in social communication scores over the course of lockdown and the course of the first half-term, we performed a correlation analysis and then simple linear regression analysis.
To establish how different variables of the lockdown or the first half-term were associated with an overall change in social-communicative behaviour over these time periods, we performed simple logistic regressions; where models were fitted to binary dependent variables coded as 1 s or 0 s and the perceived change in overall social-communication was the independent variable. For example, whether a child regularly attended school during the lockdown was answered as Yes or No, therefore ‘Yes’ became 1 and ‘No’ become 0, and was plotted on the Y-axis, where the change in overall social-communication score was plotted on the X-axis.
Results
Characteristics of respondents and their children
Data from the first questionnaire (T1) included 176 parents from across the UK, whose children all had a formal diagnosis of ASD. Most parents had known of their child’s diagnosis for 2 − 3 years. The majority of children were verbal and did not attend any kind of private therapy. The children were aged between 3 and 12 years old (see ).
Table 1. Characteristics of children whose parents took part in the time-point 1 (T1) questionnaire and time-point 2 (T2) questionnaire shown as frequency (n) and percentage (%).
Data from the second, follow-up questionnaire (T2) included responses from 54 parents from across the UK who had all previously taken part in the study. Again, all children had a formal diagnosis of ASD, were aged between 3 and 12 years old, most were verbal, did not attend private therapy, and the majority of parents had known about their child’s diagnosis for 2 years (see ). We also asked parents what type of local restrictions were in place in their area due to COVID-19 at the time of taking the questionnaire ().
There were no major differences in group demographics for participants at either T1 or T2 for age, being verbal/non-verbal, length of diagnosis, or attending private therapy (). Thus, indicating the demographics of those lost to follow-up and those followed-up were similar (Vandenbroucke et al. Citation2007). However, substantially more participants were from Scotland in T1 (40.9%), than they were in T2 (13.0%), albeit all respondents were still from the UK.
Factors affected by lockdown and the return to school
Outcomes of factors affected by the lockdown are detailed in . Results indicated that only 10.2% of children, whose parents answered the questionnaire, regularly attended school during the lockdown, suggesting that the school routine was disrupted for nearly 90% of children in the sample. Furthermore, over half (55.7%) of the parents felt they did not receive sufficient support from their child’s school over the course of the lockdown. Despite this, when asked what type of support was offered, many parents reported having online homework and activities set, regular phone calls home, interactions over Skype, Teams or Zoom, and email updates. However, some parents reported having no support at all, consequently struggling with the home learning and lack of help.
Table 2. Parental responses of factors affected during the lockdown (T1) and the return to school period (T2) represented as frequency (n) and percentage (%).
Outcomes from the T2 questionnaire are also shown in . In contrast to T1, 81.5% sample regularly attended school, indicating that most of the parents had sent their child back to school following the summer break. However, from the data collected it is unclear what percentage of children were already home-schooled prior to the outbreak of COVID-19 and therefore would not be ‘returning to school’ as such. Over half of the parents felt that they were supported by their child’s school during the return school period (64.8%), and reported that their child saw people outside of the home and school environment (66.7%).
Changes in physical activity
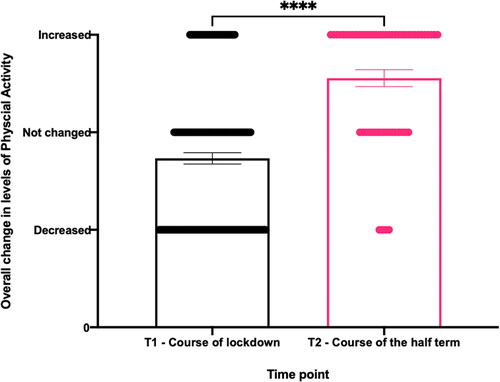
When asked how parents thought their child’s physical activity levels had changed over the course of lockdown and as rated on a three-point scale, 46.6% of parents reported a decrease in overall physical activity, whilst 33.5% of parents stated levels of physical activity stayed the same, and 19.9% reported that levels of physical activity had increased. In contrast to T1, during the return to school period only 7.4% of parents reported a decrease in physical activity levels, 29.6% reported physical activity levels staying the same, and 63% reported an increase in physical activity levels as rated on a three-point scale. An unpaired, nonparametric t-test (Mann-Whitney test) between overall means of change in physical activity levels between T1 and T2 suggested significantly more parents perceived their child’s level of physical activity to increase during the course of the first half-term, in comparison to the course of lockdown (p < .0001; ).
Figure 3. Mean (±SEM) on a three-point scale of parents' perceptions of their child’s change in overall physical activity levels during T1, the course of lockdown (n = 176), and T2, the course of the first half term (n = 54), represented as a bar chart. The scatter plot (horizontal lines) represents the individual values and proportion of parents who perceived their child’s activity levels to either increase, decrease or stay the same. Mann-Whitney test revealed a statistical difference between means of each time point (p <.0001; ****).
Changes in social-communicative behaviours
Changes in communication skills
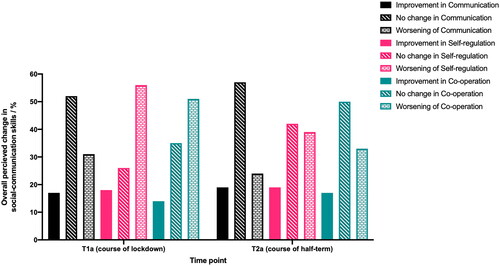
Descriptive statistics indicated that over half (51.7%) of the parents surveyed perceived their child’s communication skills to ‘not change’ during the lockdown (T1a; n = 176; no missing responses). 4.5% perceived their child’s communications skills to get ‘a lot worse’, 26.7% reported their skills to get ‘a bit worse’, whereas 13.6% perceived their child’s skills to get ‘little bit better’, and only 3.4% reported skills to get ‘a lot better’ throughout lockdown. Combining the percentage of parents who noted an improvement in communication skills and combining parents who reported a worsening of communication skills revealed that more parents saw an overall worsening of communication skills in comparison to an improvement of communication skills at T1a, but not compared to no change (). At T2a (n = 54, no missing responses), descriptive statistics revealed that most (57.4%) of the parents surveyed perceived their child’s communication skills to ‘not change’ during the first half term. 3.7% thought they had got ‘a lot worse’, 20.4% thought they had got ‘a little bit worse’, whereas, 16.7% believed them to get ‘a little bit better’, and only 1.9% perceived them to get a lot better’. Again, we combined the percentage of parents who noted an improvement and the percentage of parents who saw a worsening of communication skills, which revealed a slightly higher percentage of parents reporting a worsening of communication skills than an improvement at T2a, however most reported no change (). A chi-squared test revealed there was no significant relationship between parents' perception of change in communication skills and time-point (X2 = (2, N = 176) =1.025, p = .599).
Figure 4. Combined percentage of parents who reported their child’s social-communication skills, including communication, self-regulation and co-operation skills, to either improve (by a little bit and a lot), worsen (by a little bit and by a lot) or not change over the course of lockdown (T1a; n = 176) and over the course of the half-term (T2a; n = 54). Key to the right.
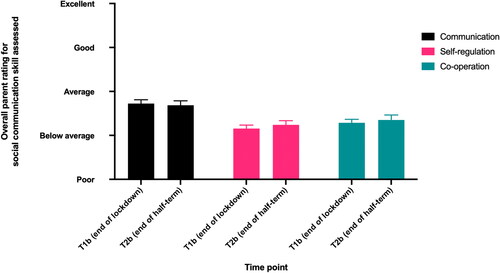
Only parents, whose children had been back at school for less than 3-weeks were asked to rate their child’s communication skills at the time of taking the questionnaire (n = 109; no missing response). At T1b, 8.3% of parents reported their child’s communication skills as ‘poor’, 31.2% reported them as ‘below average’, 42.2% perceived them as ‘average’, 16.5% saw them as ‘good’, and 1.8% rated them as ‘excellent’. At the end of the first half (T2b; n = 54, no missing responses) most parents rated their child’s communication skills as ‘average’ (51.9%). 3.7% rated them as ‘poor’ and 35.2% rated them as ‘below average’. In contrast, 7.4% of parents perceived their child’s communication skills as ‘good’, and again 1.9% rated them as ‘excellent’. When considering the overall parental rating for communication skills and taking into account those that perceived their child’s communication skills to be average, there was no notable difference in the overall means of perceived competence of communication skills between T1b and T2b () correspondingly a two-way, repeated-measures, mixed-model ANOVA revealed there was no statistically significant difference between T1b and T2b for communication skills (p = .989).
Figure 5. Mean (±SEM) of parental rating scores of their child’s social-communication skills; including communication, self-regulation, and co-operation, at the time of taking the first questionnaire following lockdown (T1b; n = 176) and at the time of taking the follow-up questionnaire at the end of the first half-term (T2b; n = 54). With parent rating scale on the Y-axis, time point on the X-axis and key to the right.
Changes in self-regulation skills
Descriptive statistics at T1a (n = 176; no missing responses) demonstrated that 19.9% of parents reported their child’s self-regulation skills to get ‘a lot worse’ during the lockdown and 36.6% of parents reported them to get ‘a little bit worse’. In contrast, 25.6% of parents reported their child’s self-regulation skills to ‘not change’ over lockdown and even 15.3% reported these skills getting ‘a little bit better’. However, only 2.3% of parents survey perceived their child’s self-regulation skills to get ‘a lot better’ during the lockdown. Combining the percentage of parents who reported an improvement in self-regulation skills and combining parents who noted a worsening of self-regulation skills clearly suggests that a large number of parents saw an overall worsening of self-regulation skills in comparison to parents who saw an improvement or reported no change (). Descriptive statistics at T2a (n = 54; no missing responses) indicated that the majority (42.6%) of parents surveyed perceived their child’s self-regulation skills to ‘not change’ during the course of the first half-term. 7.4% of parents believed their child’s self-regulation skills to get ‘a lot worse’, 31.5% perceived them to get ‘a little bit worse’, and 18.5% saw them to get ‘a little bit better’. However, no parents reported their child’s self-regulation skills to get ‘a lot better’. Combining the percentage of parents who saw an improvement and percentage of parents who saw a worsening of self-regulation skills during T2a, revealed that a larger percentage of parents saw an overall worsening of self-regulation skills during this time in comparison to an improvement, but not in comparison to no change. A chi-squared test suggested there was a significant relationship between parents' perception of self-regulation skills and time-point (X2 = (2, N = 176) =6.136, p = .047), given that more parents noted a worsening of self-regulation skills during the course of lockdown than during the course of the first half-term.
Only parents whose children had been back at school for less than 3 weeks were asked to rate their child’s self-regulation skills at the time of taking the first questionnaire (n = 109; no missing responses). At T1b, parents reported their child’s self-regulation skills as mostly ‘below average’ (51.4%), 19.3% rated them as ‘poor’, 24.8% rated them as ‘average’, 3.7% rated them as ‘good’, and less than 1% rated them as ‘excellent’. Descriptive analysis at T2b (n = 54; no missing responses) showed that a small number of parents surveyed rated their child’s self-regulation skills as ‘poor’ (11.1%) at the end of the first half-term, 57.4% rated them as ‘below average’, 27.8% rated them ‘average’, and 3.7% rated them as ‘good’. No parent rated their child’s self-regulation skills as ‘excellent’. When considering the overall means of parental rating for self-regulation skills and taking into account parents reporting their child self-regulation ability to be average, a small increase in the overall mean ratings of self-regulation skills was noted between T1b and T2b. However, a two-way, repeated-measures, mixed-model ANOVA revealed this was not statistically significant (p = .942; ).
Changes in co-operation
Descriptive statistics of the responses (n = 176; 3 missing responses) at T1a revealed 14.5% of parents surveyed perceived their child’s co-operation skills to get ‘a lot worse’ and 35.2% perceived them to get ‘a little bit worse’ over the lockdown. Similarly, 35.2% also reported their child’s co-operation and co-operative play skills to ‘not change’. However, 10.8% and 2.8% of parents perceived their child’s co-operation skills to get ‘a little bit better’ and ‘a lot better’, respectively. The combined percentage of parents who saw an improvement in co-operation skills or noted no change was substantially lower than the combined percentage of parents who reported a worsening of co-operation skills (). At T2a (n = 54; no missing responses) descriptive statistics showed that during the first half-term 5.6% of parents surveyed recalled their child’s co-operation skills to ‘get a lot worse’, 27.8% reported them to ‘get a little bit worse’, 50.0% said they did ‘not change’, 14.8% recalled them getting ‘a little bit better’, and only 1.9% report them to ‘get a lot better’. Again, the combined percentage of parents who noted an improvement of co-operation skills over the course of the first half-term was lower than the percentage of parents who reported a worsening over the course of the first half-term, but not lower than those that reported no change (). A chi-squared test revealed a significant association between co-operation skills and time-point (X2 = (2, N = 176) =6.179, p = .045), where more parents noted a worsening of co-operation skills during the lockdown than during the first half-term.
Only parents, whose children had been back at school for less than 3-weeks were asked to rate their child’s co-operation skills at the time of taking the first questionnaire (n = 109; 1 missing response). At the end of the lockdown, 13% of parents perceived their child’s co-operation skills as ‘poor’, 53.7% perceived them as ‘below average’, 25.9% rated them as ‘average’, 6.5% perceived them as ‘good’, and less than 1% perceived them as ‘excellent’. At the end of the half-term, 14.8% of parents rated their child’s co-operation skills as ‘poor’, 42.6% rated them as ‘below average’, 35.2% perceived them as ‘average’, and 7.4% rated them as ‘good’. A two-way, repeated-measures, mixed-model ANOVA revealed between the end of lockdown and the end of the half-term, there was no statistically significant difference in parents' scoring of their child’s co-operation skills (p = .968; ).
Associations between the overall change in social-communicative skills and lockdown variables
Spearman’s r correlation analysis revealed there was no significant correlation between change in overall social-communicative behaviours of autistic children as rated by their parents and the overall change of their physical activity levels over the course of lockdown (r = 0.1034; p = .172). As a result, a simple linear regression analysis was not warranted.
Simple logistic regressions were used to test the effects of, 1) having a sibling (yes/no) as a proxy for greater social interaction at home throughout the lockdown period, 2) regularly attending school (yes/no) during the period of interest, 3) parent feeling sufficiently supported by the school (yes/no) throughout the lockdown period, and 4) seeing friends/family outside the household and outside of school (yes/no) during the lockdown (). Only sufficient support from school during the lockdown period, and seeing friends and family during the lockdown period were positively associated with an improvement in overall social-communicative behaviours during the lockdown. Suggesting, children whose parents felt supported by their schools were reported to, on average, show an improvement in their social communication skills (i.e. social-communicative skills got a little bit better, or got a lot better) over the course of the lockdown (p = .007; ). Similarly, children who continued to see friends and family outside of school and outside of the household over the course of lockdown were perceived to also show a slight improvement in their overall social-communicative behaviours in comparison to those who did not (p = .002; ). The model proposes that children in the sample analysed (n = 176) were 1.824 times more likely to see friends or family outside the household/outside of school during the lockdown period for every increment on the Likert scale provided (1 − 5; communication skills got a lot worse – communication skills got a lot better). For example, a child whose overall score was 5 – social-communication skills got a lot better, was 1.824 times more likely to have seen friends or family during the lockdown than a child who scored 4 – social-communication skills got a little bit better overall.
Table 3. Predictors of change in overall social-communication skills of autistic children as perceived by their parents (n = 176) during the lockdown (S.E; standard error, OR; odds ratio, CI; confidence interval; p < .01; **).
Associations between overall change in social-communicative skills and first half-term variables
Spearman’s r correlation revealed there was a small, but significant, positive correlation between change in overall social-communicative behaviour and overall change in physical activity levels during the course of the first half-term (r = 0.285; p = .037). Simple linear regression suggested the change in overall communication score could be anticipated from the overall change in physical activity levels, such that an increase in overall physical activity level may have foreshadowed an improvement in social communication skills in autistic children, as perceived by their parents (R2 = 0.085; p = .033).
Further simple logistic regressions were used to test the effects of 1) having a sibling (yes/no) as a proxy for greater social interaction at home throughout the first half-term, 2) regularly attending school (yes/no) during the first half-term, 3) parent feeling sufficiently supported by the school (yes/no) throughout the period of interest, and 4) seeing friends/family outside the household and outside of school (yes/no) during the first half-term (). Again, having a sibling was not associated with the overall change of social-communication skills in autistic children as perceived by their parents. However, regularly attending school throughout the first half term (p = .004; ) and parents feeling sufficiently supported by the school over the course of the first half term (p = .003; ) were positively associated with a change in overall communication scores. Parents of children who regularly attended school throughout the first half-term were more likely to report an increase in their child’s overall social-communication score in comparison to children that did not attend school regularly during the first half-term. The likelihood of regularly attending school during the first half-term increased by 4.254 with every increment on the Likert scale (i.e. 1 − 5; communication skills got a lot worse – communication skills got a lot better). Seeing family and friends outside of the household and outside of school also showed a positive association with changing social skills, however this association did not reach significance.
Table 4. Predictors of change in overall social-communication skills of autistic children as perceived by their parents (n = 54) during the first half-term (S.E; standard error, OR; odds ratio, CI; confidence interval; p < .01; **).
Discussion
To our knowledge, this is the first study that explored the social-communicative impacts of lockdown as a result of the COVID-19 outbreak, and the return to school period following prolonged disruption to routine, in children diagnosed with ASD living in the UK. Results from the surveys indicated that the majority of parents believed that their child’s self-regulation and co-operation skills, but not their communication skills, had worsened during the course of lockdown. As a result, our first hypothesis (HFootnote1) can only be partially accepted. During the return to school period, the majority of parents believed their child’s communication, self-regulation or co-operation skills did not change and there was no significant difference observed between the group means for the overall change in the competence of social-communication skills between T1b and T2b. Therefore our second hypothesis (H2Footnote2) cannot be accepted as social-communication skills did not significantly improve upon returning to school. Physical activity levels were reported to significantly increase during the return to school period; suggesting, our third hypothesis (H3Footnote3) can confidently be accepted. In addition, our fourth hypothesis (H4Footnote4) can be partially accepted as positive changes in overall social-communication skills during the lockdown were significantly associated with parents feeling supported by their child’s school and still seeing friends and family despite the lockdown rules, but were not associated with the other factors explored in this study.
Implications for practice and future directions
Despite our previous hypothesis that all social-communication skills would worsen in children diagnosed with ASDs due to the lockdown implemented in the UK, the majority of parents reported that the subdomain of social development – communication skills, did not change in their children. This may seem somewhat counterintuitive due to not being at school and socially isolating during the lockdown. However, Renzo et al. (Citation2020) reported that several parents, who completed their survey, noted an improvement in their child’s verbal and non-verbal communication skills during the first month of lockdown in Italy. Our results indicated that over 90% of autistic children were not in school during the UK’s first lockdown and many parents were often required to work from home or were furloughed during this lockdown period (Barker and Russell Citation2020, Burchell et al. Citation2020, ONS Citation2020, Reuschke and Felstead Citation2020). Therefore, the results from our work and the aforementioned study may reflect parents spending more time with their autistic child and subsequently developing more successful communicative relationships with their child. Previous research has demonstrated that child-parent relations are more successful at producing desirable outcomes, such as improving communication skills, than child-teacher-based relationships (Duch et al. Citation2019, Pianta et al. Citation1997, Zivan and Horowitz-Kraus Citation2020). Therefore, increased child-parent interactions may have prevented communication skills from worsening during the lockdown period.
Interestingly, only support from school and seeing friends and family were significantly associated with social-communicative changes over the course of lockdown. Our preliminary findings suggested that parents, who felt supported by the school, were more likely to report an improvement in their child’s social-communicative skills. Similarly, continuing to see friends and family outside of school and outside the household was associated with better social-communicative skills as rated by parents. Social exposure, social interactions, and larger social networks are all believed to improve social development and communication skills (Lev-Ari Citation2018, Lev-Ari and Sebanz Citation2020, Rost and McMurray Citation2009). As a result, it is not surprising that children who continued to see their friends and family, despite the lockdown restrictions, were, overall, more likely to be protected against worsening social-communication skills. Furthermore, social support from friends and spending spare time with friends have both been established as strong protective factors against mental disorders in young people; therefore, exemplifying the importance of social support for not only social-communication skills but also for well-being. Future work may wish to investigate if the benefits of social support are still maintained through virtual environments, such as video-calling, for children diagnosed with ASD. The findings from such work could be implemented to protect and improve the social-communicative outcomes of autistic children if we were to ever face another period of prolonged social isolation and help prevent the deterioration of self-regulation and co-operation skills.
In line with previous research (Colizzi et al. Citation2020), our results signified the importance of parents feeling supported by their children’s schools, as both changes in social skills over the course of the lockdown and over the course of the first half-term were associated with this variable. Families of individuals diagnosed with ASD are reported to experience greater levels of stress than families of children affected by other disabilities (Drogomyretska et al. Citation2020, Seltzer and Krauss Citation2001). Therefore, it is key for schools and educational support (if the child is home-schooled) to continue supporting parents during periods of disruption, and even when the child is still attending school, in order to minimise stress and increase the likelihood of positive social-communication outcomes. Future research may wish to investigate how schools and educational provisions can more effectively support parents and children whilst at school, and during periods when attending school may not be possible. Additionally, support packages for enhancing the specific sub-domains of social development; communication and importantly, self-regulation, and co-operation, could be developed to help children improve these skills during periods of lockdown and social isolation.
Consistent with our hypothesis (H3), physical activity levels were reported to decrease during the lockdown and increase during the return to school. The significant increase in the level of physical activity during the return to school was significantly associated with better social-communicative outcomes in our sample of autistic children, thus suggesting the importance of physical activity for enhancing or maintaining social development. Although this association is only preliminary, our results are in line with previous research that highlights the benefits of physical activity for developing communications skills and improving social development in the autistic population (Morris et al. Citation2020, Sam et al. Citation2015). As a result, future research may wish to build on current research (Yarımkaya and Esentürk Citation2020) and investigate how physical activity levels can be maintained if there is a possibility of returning to a lockdown, or for those who do not readily have access to ‘green-space’ for physical activities. Similarly, research may wish to explore how physical activity levels can be increased within the home environment, with a specific focus on also improving social-communication skills. For example, tailored exergames (online/virtual exercise games) in the home environment have shown to reduce stereotyped and repetitive movements in autistic individuals (Anderson-Hanley et al. Citation2011). Thus, it may be worth investigating if these exergames can also be used as a vehicle to improve social-communication skills, whilst maintaining or increasing levels of physical activity in the home environment.
Many individuals diagnosed with ASD are male. It is expected that males are 5 times more likely to be diagnosed with ASDs than females, as the current ratio is approximately 5:1 (Werling and Geschwind Citation2013). Furthermore, it is common that individuals diagnosed with ASD experience co-morbid disorders; such as emotional difficulties, depression, stress, obsessive compulsion disorder (OCD) and anxiety (Salazar et al. Citation2015). However, during the present study, we did not collect data on the participant’s sex or whether they had any existing co-morbidities. From the data, it is difficult to understand whether social-communication changes differed between boys and girls, or those with additional diagnoses. Therefore, future work may wish to investigate whether social skill changes are associated with sex or with pre-existing co-morbidities. This may help to further tailor actions and interventions for specific sub-populations of autistic individuals.
Limitations
Surveys conducted during former Public Health Emergencies of International Concern have afforded timely data collection to inform best practices in reacting to different emergencies (Abir et al., Citation2016). Similarly, the online survey employed here has shown to be a useful data collection tool, benefiting from the strengths that have been associated with this type of instrument, such as increased sample sizes, access to geographically dispersed respondents, and low running costs. However, the findings and assumptions generated from this work must be made whilst recognising some of the study’s limitations.
Due to the nature of this project, we relied on parents to recall their child’s social skills prior to the UK lockdown (March 24th) and reflect on how their child’s social skills may have changed up until the 22nd of July (when most schools broke up for the summer holiday). The study relied on parents’ perception of social-communication skills and behaviours associated with a stressful and unprecedented experience; as such, the potential for recall bias is concerning, and responses may be flawed by social desirability (Renzo et al. Citation2020). Nevertheless, research suggests that blinding participants to the study’s hypothesis and the specific factors being studied may help to reduce recall bias (Hassan Citation2005). Therefore, parents were not made aware of the study’s hypothesis prior to providing their responses in order to minimise the potential for recall bias and social desirability.
Although questions of our survey were inspired by already validated parental questionnaires and rating scales with good internal consistency (Loveland Citation2005, Chin and Bernard-Opitz Citation2000, Colombi et al. Citation2009, Jahr et al. Citation2000), we had to adapt the available answers to all reflect a 5-point Likert Scale. Further, we only asked 7 questions from each of the standardised instruments to ensure the survey was not too long, so as not to deter potential respondents. Therefore, the study suffered from the lack of a standardised outcome measure to assess the change in social-communication skills over the course of the lockdown and the first half-term. As a result, comparisons with different studies may prove difficult. Future work may wish to carry out a confirmatory factor analysis to corroborate our questionnaire’s validity using larger datasets and respondents from different demographics, for example, different geographical locations.
We ideally would have liked to perform within-subject comparisons between T1 and T2 for children whose parents completed both surveys (n = 54). However, the survey was anonymous and a large number of parents forgot their memorable word/phrase, which made coupling children from T1 and T2 not possible. Furthermore, the retention rate for the second survey was only 31%. Although we appreciate longitudinal studies often suffer from loss of participants due to follow up, especially during particularly challenging times, we believe a higher retention rate would improve the study’s validity (Dettori Citation2011). Future work may wish to investigate how lockdowns and social isolation affect children’s social-communication skills by performing within-subject comparisons across two or more time-points with a larger sample size.
Whilst the results provide potential answers to some interesting questions, they do not provide causality (Noar Citation2018). The data suggests that some social skills of autistic children worsened during the lockdown, but the data does not confidently indicate that lockdown caused this. From the data, we are able to preliminary suggest that no support from school and not seeing friends and family were associated with worse social-communication outcomes during the lockdown, and not regularly attending school, no support from the school, and limited physical activity were preliminary associated with worse social-communication outcomes during the return to school period. However, we cannot confirm these factors caused a decline in social development and communication skills.
Conclusion
In conclusion, the results from this study bring to our attention the stark variability in parents' perceptions of change in social-communication skills of autistic children during the UK’s lockdown and the return to school period. Many parents observed a worsening of their child’s social-communication skills; however, some parents noted an improvement and some noted no change at all. Although the majority of parents noted a worsening of self-regulation skills and co-operation skills over the course of the lockdown there was, surprisingly, no overall difference in the means of perceived competence in social-communication skills between the end of the first lockdown and the end of the first half-term. However, children’s physical activity levels were perceived to significantly increase during the return to school, and this was positively associated with better social-communication outcomes. The results suggested the importance of school support, maintaining contact with friends and family during the lockdown period, and then attending school regularly during the return to school period for protecting against social skills worsening during these times. Although the COVID-19 pandemic continues to cause much disruption to our lives in the UK, it could very well be the much-needed catalyst for change and reform to the educational provisions and support available for the autistic community, leading to better outcomes and quality of life for children diagnosed with ASD.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Science and Health Ethics sub-committee at the University of Essex prior to starting the recruitment phase (ETH2021-0016).
Consent to participate and publish
Informed consent was obtained from all individual participants included in the study. No identifying information was used during the study and participants were made aware that their answers to the surveys could be used in published data before consenting to take part.
Author’s contributions
Author contributions were as follows: Conceptualization: PM, JPM; Methodology: PM, JPM; Formal analysis and investigation: PM, TF; Writing – original draft preparation: PM; Writing – review and editing: PM, JPM, EH, TF; Supervision: JPM, ED, TF. All authors read and approved the final manuscript.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
Notes
1 H = Social development and communication skills will have worsened during the lockdown period, and more parents will have noticed a worsening of social-communicative behaviours during the lockdown than during the return to school.
2 H2 = Social-communicative behaviours will have significantly improved, based on parental rating, since returning to school in comparison to the end of lockdown.
3 H3 = Physical activity levels will have increased since returning to school in comparison to the end of lockdown.
4 H4 = Decreased levels of physical activity, not attending school regularly, not feeling supported by the school and not seeing people outside of school/outside the household will be associated with detrimental changes in social-communicative scores during lockdown when compared to the return to school (H4).
References
- Abir, M., Moore, M., Chamberlin, M., Koenig, K. L., Hirshon, J. M., Singh, C., Schneider, S. and Cantrill, S. 2016. Using timely survey-based information networks to collect data on best practices for public health emergency preparedness and response: Illustrative case from the American College of Emergency Physicians’ Ebola Surveys. Disaster Medicine and Public Health Preparedness, 10, 681–690.
- Amaral, D. G. and de Vries, P. J. 2020. COVID-19 and autism research: perspectives from around the globe. Autism Research, 13, 844–869.
- Aminnejad, R. and Alikhani, R. 2020. Physical distancing or social distancing: That is the question. Canadian Journal of Anaesthesia, 1–2..
- Anderson-Hanley, C., Tureck, K. and Schneiderman, R. L. 2011. Autism and exergaming: Effects on repetitive behaviors and cognition. Psychology Research and Behavior Management, 4, 129–137..
- Barker, M. and Russell, J. 2020. Feeding the food insecure in Britain: Learning from the 2020 COVID-19 crisis. Food Security, 12, 865–870.
- Barr, D. (n.d.). We are not all in the same boat. We are all in the same storm.—Latest news from Damian Barr. Damian Barr. Available at: https://www.damianbarr.com/latest/tag/We+are+not+all+in+the+same+ boat.+We+are+all+in+the+same+storm [Accessed Retrieved 2 March 2021].
- Bell, C. C. 1994. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. JAMA, 272, 828–829.
- Bellomo, T. R., Prasad, S., Munzer, T. and Laventhal, N. 2020. The impact of the COVID-19 pandemic on children with autism spectrum disorders. Journal of Pediatric Rehabilitation Medicine, 13, 349–354.
- Best, J. R. 2010. Effects of physical activity on children's executive function: Contributions of experimental research on aerobic exercise. Developmental Review, 30, 331–351.
- Burchell, B., Wang, S., Kamerāde, D., Bessa, I. and Rubery, J. 2020. Cut hours, not people: No work, furlough, short hours and mental health during COVID-19 pandemic in the UK [Monograph]. University of Cambridge Judge Business School. https://www.cbr.cam.ac.uk/research/research-projects/the-employment-dosage-how-much-work-is-needed-for-health-and-wellbeing/#item-1
- Chin, H. Y. and Bernard-Opitz, V. 2000. Teaching conversational skills to children with autism: Effect on the development of a theory of mind. Journal of Autism and Developmental Disorders, 30, 569–583.
- Colizzi, M., Sironi, E., Antonini, F., Ciceri, M. L., Bovo, C. and Zoccante, L. 2020. Psychosocial and behavioral impact of COVID-19 in autism spectrum disorder: An online parent survey. Brain Sciences, 10, 341.
- Colombi, C., Liebal, K., Tomasello, M., Young, G., Warneken, F. and Rogers, S. J. 2009. Examining correlates of cooperation in autism: Imitation, joint attention, and understanding intentions. Autism, 13, 143–163.
- Crane, L., Adu, F., Arocas, F., Carli, R., Eccles, S., Harris, S., Jardine, J., Phillips, C., Piper, S., Santi, L., Sartin, M., Shepherd, C., Sternstein, K., Taylor, G. and Wright, A. 2021. Vulnerable and forgotten: The impact of the COVID-19 pandemic on autism special schools in England. Frontiers in Education, 6, 175.
- Dettori, J. R. 2011. Loss to follow-up. Evidence-Based Spine-Care Journal, 2, 7–10.
- Dorn, E., Hancock, B., Sarakatsannis, J. and Viruleg, E. 2020. COVID-19 and student learning in the United States: The hurt could last a lifetime. McKinsey & Company, Public Sector Practice, 9, 2–4.
- Drabble, L., Trocki, K. F., Salcedo, B., Walker, P. C. and Korcha, R. A. 2016. Conducting qualitative interviews by telephone: Lessons learned from a study of alcohol use among sexual minority and heterosexual women. Qualitative Social Work, 15, 118–133.
- Drogomyretska, K., Fox, R. and Colbert, D. 2020. Brief report: Stress and perceived social support in parents of children with ASD. Journal of Autism and Developmental Disorders, 50, 4176–4182.
- Duch, H., Marti, M., Wu, W., Snow, R. and Garcia, V. 2019. CARING: The impact of a parent-child, play-based intervention to promote Latino Head Start children's social-emotional development. The Journal of Primary Prevention, 40, 171–188.
- Evans, J. R. and Mathur, A. 2005. The value of online surveys. Internet Research, 15, 195–219.
- Ferreira, J. P., Andrade Toscano, C. V., Rodrigues, A. M., Furtado, G. E., Barros, M. G., Wanderley, R. S. and Carvalho, H. M. 2018. Effects of a Physical Exercise Program (PEP-Aut) on autistic children's stereotyped behavior, metabolic and physical activity profiles, physical fitness, and health-related quality of life: A study protocol. Frontiers in Public Health, 6, 47.
- Giannakopoulos, G., Dimitrakaki, C., Papadopoulou, K., Tzavara, C., Kolaitis, G., Ravens-Sieberer, U. and Tountas, Y. 2013. Reliability and validity of the Strengths and Difficulties Questionnaire in Greek adolescents and their parents. Health, 05, 1774–1783.
- Goodman, R. 1997. The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 38, 581–586.
- Green, H., McGinnity, A., Meltzer, H., Ford, T. and Goodman, R. 2005. Mental health of children and young people in Great Britain, 2004. H. Green (Ed.). Basingstoke: Palgrave Macmillan. p. 2005.
- Hassan, E. 2005. Recall bias can be a threat to retrospective and prospective research designs. The Internet Journal of Epidemiology, 3. https://ispub.com/IJE/3/2/13060
- Holt-Lunstad, J., Smith, T. B. and Layton, J. B. 2010. Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7, e1000316.
- IBM SPSS Statistics. 2017. (Version 25.0 Armonk for Macintosh) [Computer software]. NY: IBM Corp.
- Jahr, E., Eldevik, S. and Eikeseth, S. 2000. Teaching children with autism to initiate and sustain cooperative play11Parts of this manuscript are based on the first and second author’s thesis for the cand. Psychol. Degree, submitted to the Department of Psychology, University of Oslo. Research in Developmental Disabilities, 21, 151–169.
- Jones, R. A., Downing, K., Rinehart, N. J., Barnett, L. M., May, T., McGillivray, J. A., Papadopoulos, N. V., Skouteris, H., Timperio, A. and Hinkley, T. 2017. Physical activity, sedentary behavior and their correlates in children with autism spectrum disorder: A systematic review. PLoS One, 12, e0172482.
- Kenny, L., Hattersley, C., Molins, B., Buckley, C., Povey, C. and Pellicano, E. 2016. Which terms should be used to describe autism? Perspectives from the UK autism community. Autism, 20, 442–462.
- Lancker, W. V. and Parolin, Z. 2020. COVID-19, school closures, and child poverty: A social crisis in the making. The Lancet Public Health, 5, e243–e244..
- Lang, R., Koegel, L. K., Ashbaugh, K., Regester, A., Ence, W. and Smith, W. 2010. Physical exercise and individuals with autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, 4, 565–576.
- Lee, J. and Vargo, K. K. 2017. Physical activity into socialization: A movement-based social skills program for children with autism spectrum disorder. Journal of Physical Education, Recreation & Dance, 88, 7–13.
- Lev-Ari, S. 2018. The influence of social network size on speech perception. Quarterly Journal of Experimental Psychology, 71, 2249–2260.
- Lev-Ari, S. and Sebanz, N. 2020. Interacting with multiple partners improves communication skills. Cognitive Science, 44, e12836.
- Loveland, K. A. 2005. Social-emotional impairment and self-regulation in autism spectrum disorders. In Emotional development: Recent research advances. New York: Oxford University Press, pp.365–382.
- Lyall, K., Croen, L., Daniels, J., Fallin, M. D., Ladd-Acosta, C., Lee, B. K., Park, B. Y., Snyder, N. W., Schendel, D., Volk, H., Windham, G. C. and Newschaffer, C. 2017. The Changing epidemiology of autism spectrum disorders. Annual Review of Public Health, 38, 81–102.
- Merrell, K. W. 1994. Preschool and kindergarten behavior scales: Test manual. Brandon: Clinical Psychology Publishing Inc.
- Morris, P., Hope, E., Foulsham, T. and Mills, J. P. 2020. Dancing out for a voice; a narrative review of the literature exploring autism. Physical Activity and Dance, SportRxiv. Pre-print.
- Narzisi, A. 2020. Handle the autism spectrum condition during coronavirus (COVID-19) stay at home period: Ten tips for helping parents and caregivers of young children. Brain Sciences, 10, 207.
- NHS. 2019, May 2. What is autism? Nhs.Uk. https://www.nhs.uk/conditions/autism/what-is-autism/
- Noar, S. 2018. What do survey data really mean? Considering issues of casualty and temporality in survey | Grant Programs | National Institute of Dental and Craniofacial Research. https://www.nidcr.nih.gov/grants-funding/grant-programs/behavioral-social-sciences-research-program/what-do-survey-data-really-mean-considering-issues-of-casualty-and-temporality-in-survey
- ONS. 2020. Coronavirus and the social impacts on Great Britain—Office for National Statistics. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandwellbeing/datasets/coronavirusandthesocialimpactsongreatbritaindata
- Pianta, R. C., Nimetz, S. L. and Bennett, E. 1997. Mother-child relationships, teacher-child relationships, and school outcomes in preschool and kindergarten. Early Childhood Research Quarterly, 12, 263–280.
- Qualtrics. 2005 (September 2020). [Computer software]. Qualtrics. https://www.qualtrics.com
- Renzo, M. D., Castelbianco, F. B. D., Vanadia, E., Petrillo, M., D’Errico, S., Racinaro, L. and Rea, M. 2020. Parent-reported behavioural changes in children with autism spectrum disorder during the COVID-19 lockdown in Italy. Continuity in Education, 1, 117–125.
- Reuschke, D. and Felstead, A. 2020. The effect of the great lockdown on homeworking in the United Kingdom. Wales Institute of Social & Economic Research, Data & Methods, 1, 12.
- Rost, G. C. and McMurray, B. 2009. Speaker variability augments phonological processing in early word learning. Developmental Science, 12, 339–349.
- Rundle, A. G., Park, Y., Herbstman, J. B., Kinsey, E. W. and Wang, Y. C. 2020. COVID-19-related school closings and risk of weight gain among children. Obesity, 28, 1008–1009.
- Russell, W. and Stenning, A. 2020. Beyond active travel: Children, play and community on streets during and after the coronavirus lockdown. Cities & Health, 1–4.
- Salazar, F., Baird, G., Chandler, S., Tseng, E., O'sullivan, T., Howlin, P., Pickles, A. and Simonoff, E. 2015. Co-occurring psychiatric disorders in preschool and elementary school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2283–2294.
- Sam, K.-L., Chow, B.-C. and Tong, K.-K. 2015. Effectiveness of exercise-based interventions for children with autism: A systematic review and meta-analysis. International Journal of Learning and Teaching, 1, 98–103.
- Seltzer, M. M. and Krauss, M. W. 2001. Quality of life of adults with mental retardation/developmental disabilities who live with family. Mental Retardation and Developmental Disabilities Research Reviews, 7, 105–114..
- Shokri, A., Khosravi, A. A. and Hooman, H. A. 2013. Basic psychometric properties of the preschool and kindergarten behavior scales in a sample of İranian children. Procedia - Social and Behavioral Sciences, 84, 479–485.
- Spitzberg, B. H. 1995. CSRS The Conversational Skills Rating Scale. San Diego State University: NCA Diagnostic Series, San Antonio 61.
- Stone, L. L., Janssens, J. M. A. M., Vermulst, A. A., Van Der Maten, M., Engels, R. C. M. E. and Otten, R. 2015. The Strengths and Difficulties Questionnaire: Psychometric properties of the parent and teacher version in children aged 4-7. BMC Psychology, 3, 4.
- Vandenbroucke, J. P., von Elm, E., Altman, D. G., Gøtzsche, P. C., Mulrow, C. D., Pocock, S. J., Poole, C., Schlesselman, J. J. and Egger, M. 2007. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Medicine, 4, e297.
- Werling, D. M. and Geschwind, D. H. 2013. Sex differences in autism spectrum disorders. Current Opinion in Neurology, 26, 146–153..
- Yarımkaya, E. and Esentürk, O. K. 2020. Promoting physical activity for children with autism spectrum disorders during coronavirus outbreak: Benefits, strategies, and examples. International Journal of Developmental Disabilities, 0, 1–6..
- Zivan, M. and Horowitz-Kraus, T. 2020. Parent-child joint reading is related to an increased fixation time on print during storytelling among preschool children. Brain and Cognition, 143, 105596