
ABSTRACT
Home testing is an emerging innovation that can enable nations and health care systems to safely and efficiently test large numbers of patients to manage COVID-19 and other viral outbreaks. In this position paper, we explore the process of moving home testing across the translational continuum from labs to households, and ultimately into practice and communities for optimal public health impact. We focus on the four translational science drivers to accelerate the implementation of systems-wide home testing programmes 1) collaboration and team science, 2) technology, 3) multilevel interventions, and 4) knowledge integration. We use the Socio Ecological Model (SEM) as a framework to illustrate our vision for the ideal future state of a comprehensive system of stakeholders utilising tech-enabled home testing for COVID-19 and other virus outbreaks, and we suggest SEM as a tool to address key translational readiness and response questions.
1. Introduction to COVID-19 Diagnostic Testing
Accessing testing supplies, protecting health care providers and patients, administering tests efficiently to large numbers of individuals, and communicating results to all levels of stakeholders are imperative to a successful testing programme. The COVID-19 pandemic (we use the common nomenclature, COVID-19 for infection with SARS-CoV-2 going forward) has illuminated the need for innovative ways to test for infectious diseases. Traditionally, diagnostic testing relied on health care professionals to collect samples from patients and process them in clinic-based or central laboratories. However, the pressures of the pandemic have demonstrated that this workflow is unsustainable. Testing patients for COVID-19 by clinicians in health care facilities exposes both providers and other patients to infection and is limited by clinic capacity and competing clinical demands. Drive-through testing has mitigated some exposure risks and improved the efficiency of testing, but is limited by a paucity of sites in rural areas, and the need for private transport from friends or family members to participate, given that many such sites do not allow taxis or rideshare services (e.g., Uber, Lyft) (Araz et al., Citation2020; Groover, Citation2020; Kelliher, Citation2020; Washington State Department of Health, Citation2020). Some places have instituted walk-up sites, but this is not pervasive, and walking to a test site may not be realistic for people who have limitations or who feel unwell (Craighead, Citation2020). Over the course of the pandemic, many drive-through and walk-up sites have experienced long wait times for scheduling testing appointments and have been faced with long lines of cars and people waiting to be tested. A further challenge with drive-through and walk-up testing is that healthcare workers performing these tests outside may be exposed to inclement weather; some testing sites have had to curtail testing due to weather conditions (Kliff, Citation2020; Leins, Citation2020).
Thus, there is an opportunity for other forms of COVID-19 testing to address issues that have been identified using a system-wide lens. Many in-vitro diagnostic companies are developing at-home diagnostic tests for SARS-CoV-2, influenza, and other infectious diseases (U.S. Food and Drug Administration, Citation2020a). Most initial studies of such tests primarily focus on their accuracy and safety to achieve approval or emergency use authorisation from the U.S. Food and Drug Administration (FDA). For these innovative tests to be impactful in outbreak management, research is needed to create guidelines for utilising home-based diagnostics (referred to as home testing) in communities and integrating home testing with clinical workflows and public health programmes.
However, the path to impact community health with home testing is not easy as it involves moving across the translational continuum from labs into households. Khoury et al. developed a translational research framework to illustrate the interconnectedness of research involving multiple phases (T0–T4), beginning with scientific discoveries (T0) and ending with population health impacts (T4) (Khoury et al., Citation2011). Population health impacts may include policy development. Lam et al. further enhanced the translational research framework by introducing four influential drivers (collaboration, technology, multilevel analysis and interventions and knowledge integration) that are thought to accelerate the translation of scientific discoveries into health care and population health benefits (Lam et al., Citation2013). Of these drivers, the term “multilevel analysis and interventions” is arguably the most ambiguous. In presenting the concept of multilevel analysis and interventions, Lam and colleagues focused on the normal course of interactions among various stakeholders (e.g., provider, community) and conditions in a patient’s environment and the implications they would have on the success of an intervention (e.g., new cancer development). While the multilevel analysis and intervention driver presented in the Lam model acknowledged that we should look beyond the patient’s immediate environment to have a population level impact, the Taplin et. al., depiction of “multilevel intervention” and discussion of associated concepts seem to best capture the nature of the specific actions carried out by multi-level stakeholders as part of a population health initiative, which is most pertinent for our focus of translation into communities (Taplin et al., Citation2012). In this commentary, we apply the translation research framework derived from this lineage of studies from a public health perspective; specifically, we discuss how the drivers influence the impact and practice of home testing. The translational research framework presented in depicts the continuum of the transfer of evidence-to-practice and the drivers that can accelerate translational epidemiology that we use in this study.
Figure 1. Translational research framework adapted from the collective works of Khoury and colleagues (Lam et al., Citation2013) and Taplin and colleagues (Taplin et al., Citation2012)
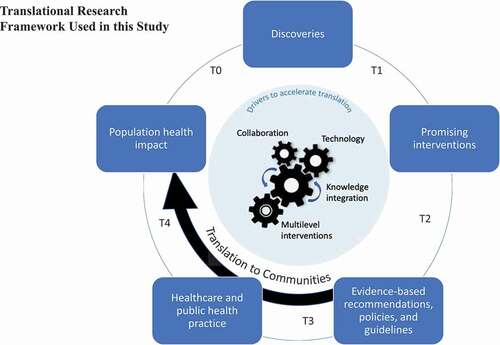
Emerging technologies such as home tests must be translated from the research environment into practice (translational level T3) and communities (T4). However, translation research on medical innovation does not typically delve into the dynamics of moving from T3 to T4 specifically for home testing (Vukotich & Charles, Citation2016). Furthermore, the role of information and communication technology in the translational process is generally not considered (Catalyst & (Producer), Citation2020; Fernandez-Moure, Citation2016).
This commentary explores the processes, adoption, and diffusion of home testing related to T3 and T4 phases, focusing on COVID-19. Our underlying position is that if a unified system is established involving multiple levels of stakeholders, home testing has the potential to tackle the demand for COVID-19 testing as the pandemic response continues. In addition, we maintain that leveraging home testing is a viable course of action for similar pandemics.
We first identify challenges in moving interventions to communities (see ) experienced historically with other forms of home testing that should be considered in the context of home testing for pandemics. We then support leveraging the Social Ecological Model (SEM) as the basis for a unified systems approach. In the remainder of the paper, using the SEM, we illustrate our vision for the end result of the translation continuum, namely, the ideal future state where multilevel stakeholders are engaged in a system to support utilisation and diffusion of technology-enabled home testing for COVID-19 and other viral outbreaks. As part of our vision, we provide “Key Translational Readiness and Response Questions” that can be used to help strategize moving home testing to communities.
This vision is informed by an interdisciplinary team of authors representing medicine, public health informatics, consumer health informatics, information systems, and health services. The authors also draw insights from two research programmes that have occurred over the past two years: an ongoing research programme in home-based smartphone-associated diagnostic testing for influenza (National Library of Medicine [NLM, Citation2020], NCT04245800; Stocks & Chilver, Citation2019), and a COVID-19 home-collection “swab and send” study (Chu et al., Citation2020; Doughton, Citation2020).
2. Learning from previous implementations of moving home testing into communities
To effectively implement home testing for COVID-19 as a unified system, we first briefly review the experience with other home tests and then examine the challenges they faced when being translated into communities. Testing at home is not unique to COVID-19 and exists in two primary forms. We refer to the first form as a “rapid home test”, which entails sampling and rapidly interpreting a test result (usually available within minutes). These rapid home tests include urine pregnancy tests (U.S. Food & Drug Administration, Citation2019b), oral HIV tests (U.S. Food and Drug Administration, Citation2020b) as well as capillary blood glucose monitoring for diabetes (U.S. Food & Drug Administration, Citation2019a). The second form of home testing is more aptly described as home collection kits; individuals collect a sample (nasal, oral, vaginal, blood prick, hair, etc.) and then mail it to a laboratory for processing and interpretation (Terrie, Citation2009). Home collection test kits are available for testing various health conditions, including genetic information (e.g., 23andMe), or sexually transmitted infections. Home tests can be approved by the FDA to be sold over the counter (OTC) directly to consumers. Alternatively, home tests can also be approved with a health care provider authorisation requirement (RxOTC). For RxOTC tests, a patient must have an initial provider consultation, at which point the provider authorises a test to be used by the patient at home. Blood glucose monitoring for diabetes is a common form of RxOTC diagnostic testing.
Some home tests, such as pregnancy tests, are not only assimilated into mainstream practice, but are a medical norm. Others, such as home HIV testing, are moving towards an mainstream assimilation path. Implementing home testing requires overcoming general medical innovation challenges such as getting buy-in from various stakeholders (such as providers and patients). In addition, there will be additional challenges unique to home testing. Getting individuals to conduct the right diagnostic test at the right time is often dependent on a complex, multilevel system where the levels and stakeholders are not connected seamlessly. We can anticipate some of the challenges to executing widespread COVID-19 home testing by considering issues identified from previous implementations of diagnostic tests at the community level. Here, we will review some previous challenges of translating home testing to communities. outlines the challenges that have threatened the adoption of some common types of home tests: pregnancy testing, HIV testing, blood glucose testing, and tests for drugs of abuse.
Table.1 Challenges of previous efforts to translate home tests to communities
A synthesis of the challenges noted in uncovers some inherent challenges specific to home testing. Meaning regardless of the technology itself or the health condition being tested, we can anticipate similar challenges with translating any home test to communities.
The first intrinsic challenge is related to the inability to ensure correct sample collection procedures – a challenge aligning with the emerging technology driver in the Translational Research Framework underpinning this commentary (see ). Many diagnostic tests feature a control function to indicate that the test has been run correctly, such as a control line on a pregnancy test (Koczula et al., Citation2016). Control mechanisms help confirm whether the test was run successfully or not; however, they may not provide information about why errors occurred or how an individual should conduct the test differently. In addition to the presence or absence of a control line, the only other way to ensure proper sample collection is to incorporate direct observation of the individual while testing. While direct observation could occur as part of telemedicine video calls, this may not be feasible within such consultations, and not all home test users will have access to telemedicine services or may want the privacy of testing without an observer.
A second inherent challenge to the assimilation of home testing is that it places the onus on the individual to determine when (or whether) to test and appropriate actions to take after testing – a knowledge integration challenge (see ). Timing of testing within an episode of illness can be critical to test accuracy. False negative test results can occur specifically when tests are taken too early, due to insufficient quantity of the target material available in the test sample. False negative and false positive results produce inaccurate data that impacts data integration. Examples include insufficient viral material at early stages of influenza or COVID-19 infection, low levels of urine beta HCG in the first few weeks after conception for pregnancy tests, and insufficient time for antibodies to develop following HIV exposure (Hayward, Citation2020; Pebody, Citation2019; Walker, Citation2019). Product labelling in approved home tests is required to guide consumers on when (i.e., how long after symptom onset or exposure to the pathogen) to conduct a home test, and when repeat testing is appropriate. However, for OTC tests, it is not possible to ensure compliance with such guidelines, potentially leading to consumer errors in testing and test interpretation and could lead to potential harms. For RxOTC tests this is less of a concern, given the need for connection with a health care provider. While acting on false negative results can have several consequences, actions following a positive test result can also pose challenges for home testing. Some individuals may seek advice or care from a provider to discuss appropriate next steps after a positive test, while others may avoid or delay needed care, potentially leading to complications from untreated illness (to the individual and to others). Individuals may also not understand that tests do not have perfect discrimination, and that false positive and false negative tests are inevitable. The implications of false results may be difficult for lay consumers to understand, whereas healthcare providers have a greater appreciation of this concept.
A third challenge to home testing is the financial burden placed on individuals to purchase them, particularly when they are not prescribed and/or not covered by insurance (i.e., if the testing is done in the U.S.) or other payment mechanism- a multilevel intervention challenge (See ) with specific attention to individual capacity, organisational benefits, and public health policy levels. Reimbursement and coverage policies require interactions at all levels (e.g., person, provider, family and social support, local community environment, and national environment) (Taplin et al., Citation2012). Cost is less of an issue for low-cost tests that are sold direct-to-consumer such as pregnancy tests – the consumer burden of purchasing multiple tests is relatively low, and most individuals can repeat testing as needed. In contrast, costs can be prohibitive for health conditions that require recurring testing, such as self-monitoring of blood glucose for individuals with diabetes (Cameron et al., Citation2010; Fleshler, Citation2019; WebMD, Citation2019), or for tests that are new on the market such as COVID-19 testing (Berger, Citation2020). Government and private payor health plans that covers the cost of home tests may be an option, particularly for tests that are used under the direction of an individual’s health care provider (RxOTC tests). Coverage for COVID-19 testing is currently highly variable, and likely to change further as the pandemic continues and emergency funding for testing evolves.
A fourth challenge is that home testing may not be appropriate or tailored to all subpopulations – which poses a multidisciplinary collaboration challenge (see ) on reaching certain subpopulations in research and targeted distribution efforts. As an aspect of multidisciplinary collaboration in translational science, Hall et. al indicates that team science “draws on diverse disciplinary perspectives to better understand and enhance the processes and outcomes of scientific collaboration” (Hall et al., Citation2008 p. 243). We need multidisciplinary teams comprised of and interested in diverse perspectives and diverse needs if home testing is to achieve population impact. In the context of home-based diagnostic testing, the concept of collaboration and moreover, team science, as a driver both acknowledges the collaboration driver situation of subpopulations in the laboratory (e.g., biological nuances) and also uses team science to better understand and enhance the processes on how innovations are presented to the public (essentially a more generalised “team science approach”). There are multiple examples of how a breakdown in this perspective of collaboration can occur with notable impact. For example, instructions for conducting and interpreting home tests may not be available in all languages, which could introduce disparities in access (Morga, Citation2020). In addition, home testing programmes may be inaccessible to individuals in low socioeconomic groups or people with cognitive or physical impairments (from existing conditions or brought on by current illness). Further, instructions may be too complex for individuals with low health literacy or diminishing cognition abilities. Alternatively, tests may require technology that is inaccessible or unaffordable such as requiring Bluetooth technology to obtain a result, or mobile apps for managing test results that are only supported on recent phone models. Furthermore, some home tests may not be appropriate for certain individuals. For example, home testing for children may be constrained by an inability of the testing company to verify who is conducting the test and with whose permission or assent (Branch, Citation2020; Everlywell, Citation2020).
Many, if not all, of the inherent challenges mentioned above could apply to home testing for COVID-19. While some problems may be resolved over time, in the case of viral outbreaks, a rapid and thorough response is critical. Time delays to “iron out the kinks” can severely impact individual health and public health outcomes during outbreaks, which has been experienced with the devastating impact of the COVID-19 pandemic due in part to lack of access to diagnostic testing.
3. Unified systems approach to challenges
The past home testing challenges discussed in the prior section illustrate the need for a process that can promote collaboration, identify best uses of technology, integrate knowledge and share multi-stakeholder perspectives for home testing to have an important life-saving impact. Vukotich and Charles (Citation2016 p. 1) indicated that “translational research is incomplete at any level unless appropriate steps are taken to communicate the results to relevant stakeholders”. Unlike some earlier forms of home testing focused on a single targeted group, in a pandemic situation, “relevant stakeholders”, who can benefit from home testing include the entire population. This broad coverage further calls for a unified systems-approach to overcome challenges and identify opportunities that can impact population health during a pandemic. A unified systems approach can help maximise the influence of the four acceleration drivers in the translational research framework to provide insights and overcome the challenges through open communication, identifying knowledge gaps, multi-layer stakeholder buy-in on policy and procedures, and employing appropriate technology.
Essentially, using a unified systems approach allows us to systematically see breakdowns and opportunities involving policy, organisational, community, interpersonal, and individual levels. Theoretical models can assist in understanding the complex dynamics in moving to T3 and T4 stages in implementing a comprehensive system of home testing. “By using theory, these frameworks increase the chances that localized research and communication interventions can effectively change desired behaviours and their behavioural determinants” (Figueroa, Citation2017, p. 1). To provide direction for cohesively addressing what we know about stakeholders, challenges and lessons from existing home testing as well as nuances associated with new forms of diagnostic testing, we need a framework that recognises the importance of an interconnected system to navigate the complexities of moving to T4.
4. Systems perspective towards translating to communities
Translational research typically encompasses a range of comparative effectiveness research, clinical outcomes research, and population-level research to determine whether the diffusion of an innovation will lead to measurable change. The translational research approach helps researchers assess how to best enable diffusion of an innovation throughout communities. We take a “whole system” approach of translation to communities that recognises the various factors and facets in the healthcare landscape. The underpinning philosophy of this approach is that “health and healthcare systems are characterised by complexity and interconnectedness, where ‘everything affects everything else’. Thus, problems in healthcare need to be viewed holistically as an integrated system of multiple components (people, organisations, technology and resources) and perspectives (Brailsford et al., Citation2012 p. 6)”.
While seminal adoption and diffusion models are valuable in providing insight related to the diffusion of home testing, in many cases, individual models do not recognise the various layers of the translational process. highlights three seminal models and issues from a home testing translational research perspective – particularly translating to communities (T4).
Table 2. Seminal adoption and diffusion models in relation to translating home testing to communities
As can be derived from , seminal adoption and diffusion models generally do not independently address the four translational science drivers identified to accelerate the diffusion 1) collaboration and team science, 2) technology, 3) multilevel interventions, and 4) knowledge integration from basic, clinical and populations sciences. (Lam et al., Citation2013). Models such as those presented in zoom in to focus on individual or organisational constructs. They do not provide appropriate level of zooming out to emphasise the interconnectedness of the multiple levels of stakeholders needed for operationalising a successful system of home testing or speak to the implications of interconnectedness of stakeholders. Collaboration among interconnected supply chain vendors, providers, patients, and public health organisations is vital to home testing because test results are most meaningful if individuals test early and take appropriate action in response to positive test results. Home testing becomes a powerful tool when it facilitates individual behaviour change, as well as early diagnosis, contact tracing, surveillance, and clinical management of their illness. Of course, there is a risk that the individual may not change their behaviour even if they test positive for a virus, but the hope is that individuals will by and large take advantage of the convenience of home testing and appropriately act in response to a positive test.
To address the societal needs that virus outbreaks impose, we need to augment mono-focused models with frameworks that recognise the implications of a collaborative, interconnected system to support various aspects of necessary mobilisation for adoption and diffusion. When it comes to healthcare, particularly at a public health level, the networks of entangled stakeholders cannot be ignored. Technology has the potential to connect stakeholders to manage an outbreak, but it requires the system to be clearly defined. The omission of key stakeholders, lack of clarity of stakeholder roles, and unfulfilled tasks in a workflow can hinder such technology’s utility. When such a system is well-developed, technology can facilitate strategy development, risk assessment, knowledge integration and effective use of communication channels. Systems-level models capture the aspect of interconnectedness of multilevel stakeholders that is missing from the frameworks mentioned previously. System-level models have been used effectively to guide research as well as the design and implementation of communication activities and strategies in practice to effectively impact the determinants of an effective response system (Figueroa, Citation2017).
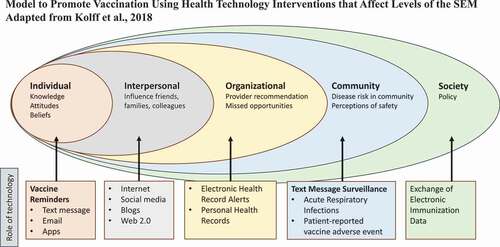
The Social Ecological Model (SEM) framework recognises that behaviour is shaped by factors at multiple levels – policy, community, organisational, interpersonal, and individual (McLeroy et al., Citation1988). The SEM has been used to provide insight on approaches to addressing a wide range of health issues, including preventing deaths in high school sports (Scarneo et al., Citation2019), managing end of life choices (Huang, Citation2014), facilitating suicide assessment and prevention efforts (Cramer & Kapusta, Citation2017), treating asthma (H. J. H. J. Nuss et al., Citation2016), screening and managing cancer (H. H. Nuss et al., Citation2012), and promoting influenza vaccination (Kolff et al., Citation2018; Kumar et al., Citation2012; McClarty et al., Citation2015; Nyambe, Van Hal et al., Citation2016). Kolff et al. advocated that the SEM “can be a useful analytical platform to address vaccine coverage across all populations, specific barriers at each level, and how interaction occurs between levels, which may help improve the impact of interventions (Kolff et al., Citation2018)”. They further recognised the use of the use of technology across each SEM level to promote vaccination (see ).
Figure 2. Model to promote vaccination using health technology interventions that affect levels of the SEM adapted from (Kolff et al., Citation2018)
Basic tenants of the SEM align with general perspectives of moving to public practice and policy in translational research. In fact, multiple translation science researchers have acknowledged that public practice and policy changes are often necessary along with interventions at the individual, interpersonal and organisational levels to improve health outcomes (Dougherty & Conway, Citation2008; Khoury et al., Citation2010; Szilagyi, Citation2009). Overall, SEM as applied to public health matters is about translating promising health interventions into impactful use in the community (T4). SEM is essentially an integrated multilevel analysis approach to highlighting and considering the complex interplay between individual, relationship, community, and societal factors. SEM can be used to assess and strategize how interactions between stakeholders and levels can be deployed concurrently for maximal impact. The SEM perspective combined with the four translational science drivers can serve as an exploratory and explanatory tool to accelerate the diffusion (see ) of innovations into communities. This integrated multilevel analysis approach includes, but also extends the concept of a multilevel intervention driver focused on the influence of environmental interactions described by Lam et al. to a deeper and broader analysis of connecting relationships, potential for change and influence, and the system acting as a whole, coherent assemble. Such an assemble is sometimes more and more complex than just a summation of parts. For example, regarding relationships, the overlapping rings in the SEM model (see ) are meant to illustrate how factors at one level influence factors at another level. Furthermore, in recognising the system lens, SEM supports it may be necessary to act across multiple levels of the model at the same time to move things forward, particularly in the case of population impact (The social-ecological model: a framework for violence prevention, Citation2015).
In a pandemic situation, early adoption of systems frameworks can help stakeholders move expeditiously towards a clearly defined behavioural outcome, and specifically move from T3 clinical practice to T4 public assimilation (see ). In this context, the target outcome is diagnostic testing that is readily available and used by organisations and individuals to perform home testing and inform individual actions, surveillance, and clinical care. A promising study that supports this approach is an epidemiological model developed by Specht et al., which found that COVID-19 testing programs that are “altruistic” and community-focused (meaning organisations offer testing to community members outside their institutions) yield fewer COVID-positive cases compared to siloed efforts (where each institution only offers testing services to their own members) (Specht et al., Citation2021). A systems perspective that recognises the collaborative interconnectedness of multilevel stakeholders can be used to identify possible leverage points to maximise opportunities to impact decision making and behaviour change. To illustrate, a study by Kumar et al. (Citation2012) that examined influenza vaccine uptake during the “swine flu” (2009 H1N1) pandemic, found that variables at every level of the SEM impact on vaccine uptake. The authors used a binary logistic regression model to determine how interventions targeting each SEM level impacted vaccine uptake. They found the variables at the intrapersonal level explained the most variance at 53%, followed by the interpersonal level (at 47%), the institutional level (at 34%), and the policy and community levels each explained 8% of the variance associated with vaccine uptake. Most notably, the levels together explained 65% of the variance, “suggesting that interventions targeting multiple levels of the framework would be more effective than interventions aimed at a single level” (Kumar et al., Citation2012, p. 1). This finding echoes the need for a “coherent ensemble” approach to interventions that considers the potential interconnectedness of components within the SEM. An integrated multilevel analysis can help reveal the possible arrangements, procedures, or acknowledgements that could bridge the complex network of stakeholders, and that would be more effective than a more insular approach.
In addition to efforts to increase influenza vaccination, the value of the SEM has also been recognised in interventions including screening for communicable (e.g., HIV) and noncommunicable (e.g., cancer) diseases, as well as to increase participation in HIV vaccine research (De Bruin et al., Citation2020; Frew et al., Citation2011; Kumar et al., Citation2012; Nyambe, Hal et al., Citation2016). However, few studies have extended the use of this model to other aspects of epidemic and pandemic management. A study where SEM was applied to communication management of the Ebola epidemic in Liberia is a notable exception (Figueroa, Citation2017). The current COVID-19 pandemic has illuminated several efforts in addition to communication management that could benefit from assessment using an SEM approach – namely, efforts to reduce spread (driving behaviour change), supply chain management of critical goods (e.g., health supplies, food) and establishing best practices for test and vaccine distribution. Without such assessment, missed opportunities may exist such as the opportunity to leverage communication pathways among multilevel stakeholders in the SEM to drive behaviour change to promote the use of face masks. Without the development and implementation of consistent policies and communication regarding the use of face masks, many communities and individuals resisted adoption of face masks. Conflicting messages were received from stakeholders including public health departments, political figures and religious leaders within and between SEM levels. A more collaborative and cohesive messaging campaign around masking could have been deployed if an SEM approach had been used for stakeholder identification, knowledge integration, and dissemination of existing knowledge regarding masking.
While the previously discussed research helps ground our model and contextual application, we know of no existing paper that explores the SEM as a framework to understand home testing in managing pandemic response efforts, and the role of information and communication technology in providing linkages among the SEM levels. We also do not know of any paper that uses SEM as a tool for prospective scenario analysis to explore structures, roles, and actions to fuelling translational drivers.
Therefore, in addition to providing a unique contribution to outbreak management, we next demonstrate how SEM can be leveraged to facilitate scenario analysis regarding how home testing can achieve the benefits of the translational science continuum. “A scenario can be defined as a description of a possible future situation, including the path of development leading to that situation. Scenarios are not intended to represent a full description of the future, but rather to highlight central elements of a possible future and to draw attention to the key factors that will drive future developments”. (Kosow & Gaßner, Citation2008 p. 133) Scenario analysis can help to analyse plausible future events by considering the outcomes that can result from iterations of the actions, interactions, and even inactions of various multilevel stakeholders to potential developments and turning points (Spaniol & Rowland, Citation2019). SEM can support a multilevel, qualitative narrative scenario technique (see Kosow & Gaßner for discussion of qualitative narrative scenario technique). By identifying and exploring actors, their roles, and the tools that can help actors fulfill their roles, SEM can help to project and discern the various pathways associated with desired scenario outcomes.
5. Using the SEM to explore translating technology supported home testing into communities
5.1. Recognising the socio-tech
Creating an effective home testing system in modern times is a socio-technical challenge in which social and technical systems must work synergistically. Technological systems have become vital to pandemic management for communications on outbreaks, identifying and sequencing viruses, and clinical management of infected patients (Deng et al., Citation2020; Verhagen et al., Citation2020; Ye et al., Citation2020). Various forms of technology can act as the line of connection to facilitate the effectiveness and efficiency of stakeholders’ roles with respect to home testing. For example, consumer-based technology has already played a role in research studies to understand COVID-19 through the use of mobile apps and wearables to conduct screening, track symptoms, support contact tracing and predict COVID-19 infection (“COVIDENTIFY – A Duke University Study, Citation2020; Pifer, Citation2020; “UCSF TemPredict Study, Citation2020).
We use SEM as a tool for scenario analysis to assess key stakeholders, identify challenges and risks, and discern communication channels and opportunities for technology to support the complex system of home testing. We situate our application of SEM in a comprehensive system of home testing that includes smartphone components. In November 2020, Lucira Health was awarded the first EUA for a home test for COVID-19 with a provider prescription (RxOTC), while in December 2020, Ellume Health received the first authorisation for a home test directly over-the-counter (OTC) without a prescription requirement (“FDA Authorizes Ellume COVID-19 Home Test as First Over-the-Counter Fully At-Home Diagnostic Test”, 2020; “US FDA issues EUA to Lucira COVID-19 All-In-One Test Kit for COVID-19 self-testing at home”, Citation2020). These tests (and many others in development) enable individuals to not only take their own samples, but also obtain test results at home. Smartphone and website capabilities coupled with the diagnostic test are now available to further facilitate the testing process (through instructions and providing result interpretation) and impact (with the potential for telemedicine connection or to share results for public health surveillance) (Abbott, Citation2020; “MobileDetect Bio”,; Park et al., Citation2020). Incorporating smartphone technology into home testing will be valuable for enabling stakeholders at all levels to utilise test result data. Our discussion is contextualised primarily to the environment in the United States. However, the key SEM decision points and challenges we discuss are relevant to multiple settings globally.
5.2. Mobilisation process for technology-supported home testing for COVID-19
Core to SEM is identifying stakeholders at various levels through an integrated multilevel analysis. We have already seen in the COVID-19 pandemic how important it is for various stakeholders to fulfil their respective interconnected roles and collaborate to facilitate system-wide success for COVID-19 testing. For instance, policymakers have a critical role to support rapid development and deployment of diagnostics, and manufacturers must have robust supply chains to procure and deliver necessary supplies (including diagnostic tests) during an outbreak. Furthermore, our earlier discussion of challenges faced in implementing previous home testing into communities (e.g., pregnancy tests, glucose tests) revealed several inherent and test specific challenges historically experienced, e.g., cost, distribution, process, test interpretation, provider support and buy-in (e.g., trust test results, would recommend to patients), and workplace requirements.
Indeed, we believe it requires a complex network of stakeholders representing distinct SEM levels to address the challenges of bringing technology-supported home testing to the community. Additionally, the network of stakeholders that has to come together for population reach (T4) in pandemic situation (and moreover, a pandemic of the magnitude of COVID-19) may be even more complex. provides an SEM conceptualisation of the stakeholders who need to engage in a comprehensive COVID-19 home-based testing effort. We visualised the SEM level rings in an overlapping manner to convey the importance of stakeholder integration across levels.
Figure 3. SEM mapping of key stakeholders for home testing implementation
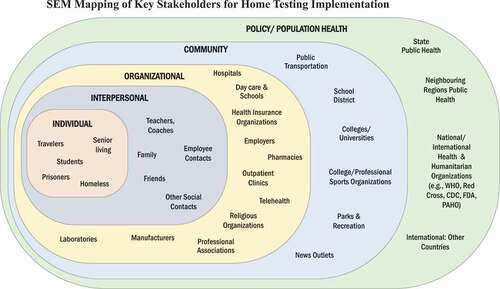
Stakeholders should collectively perform an integrated set of actions to act as a cohesive network to optimise the translation of home testing to communities. In , we capture our ideal vision of the stakeholders (mapped across SEM levels) who need to act as a coherent ensemble to enable individual home test results to contribute to public health management of the COVID-19 pandemic.
In , we show the integrated set of actions that can occur at each SEM level to maximise the utility of data from home tests. We further inform by discussing and expanding upon the stakeholder actions and the role technology plays in connecting the various levels and stakeholders within and across levels. The ideal state of home testing entails fully capitalising on knowledge integration to make the most impactful decisions. This knowledge integration is possibly by applying state-of-the-art science and technology methods to manage data, synthesise into knowledge, and translate knowledge to influence policy, practice, and research. This process aligns with the goals Lam et al. proposed to move along the continuum (Lam et al., Citation2013).
Figure 4. Actions to occur across SEM levels to reach ideal future state of home testing for COVID-19
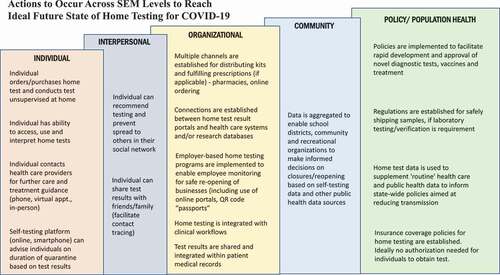
5.2.1. Individual level actions
Acting on home test data across all SEM levels is only feasible if individuals conduct home tests. In , the “Individual” bar captures the actions individuals should do to initiate the home testing system. At the Individual level, people should be willing to conduct a self-test (e.g., nasal swab or saliva collection) and trust their results are accurate. Many individuals may prefer the privacy of home testing over testing in other settings. For tests with technology that supports immediate provision of test results, individuals should be able to easily locate, interpret, and report results. For tests that require laboratory testing and/or provider consultation, individuals should be able and willing to send their sample to a laboratory for testing and easily access the results. Home testing should be accessible to most, if not all, individuals regardless of language, socioeconomic background, urban/rural locale. In recognising the socioeconomic challenges, the technology will be developed so that out-of-pocket expenses are minimal, or reimbursement from third-party payers or government subsidies is available. Individuals should be able to easily access home testing, ideally involving some form of convenient purchase location (e.g., pharmacies or online) or telemedicine ordering with home delivery to mitigate exposure and to provide some degree of “home-based comfort” to a person feeling unwell and to offer privacy while testing. As therapies emerge for COVID-19 that are suitable for home use, the ability to test rapidly with self-tests could become a critical step to appropriate use of these therapies.
highlights categorisations of individuals who live in dense communities or shared living spaces, such as college dormitories, homeless shelters, prisons, or senior living communities, who can benefit significantly from using home tests. Home tests can empower individuals to quickly act upon a test result to reduce rapid spread in their environment. Other priority groups include those who work closely with the public, e.g., transport workers, teachers, store clerks. Individuals may be more likely to complete COVID-19 home testing prior to travel including migrant workers, or those travelling for leisure, especially if they are unable to access their healthcare providers.
5.2.2. Leveraging technology to fulfil the individual level actions
At the Individual Level, a home test combined with mobile app and website capabilities could allow individuals to monitor their illness and may help individuals better manage their condition (such as seeking health care for complications treatment, self-isolating, or determining when to re-test). This may be particularly valuable for individuals who have poor access to existing health care services due to lack of health insurance, language or other barriers. For individuals with limited resources, SMS-based technology could be implemented for accessing test results and seeking clinical care. Creating a system that does not require a mobile app, Wi-Fi or internet access will enable home testing to be deployed in communities with limited resources. Wearables could also potentially help individuals determine when it is appropriate or necessary to seek testing, as markers such as heart rate, sleep, body temperature, and physical activity “may enable providers and patients to be alerted of a potential COVID-19 infection before symptoms become severe” (Konty et al., Citation2019; Seshadri et al., Citation2020).
5.2.3. Interpersonal level actions
On the Interpersonal level, individuals who test positive have a choice in their actions regarding spread and contact tracing. This includes actions within their home, as well as determining if and how they notify others (see , “Interpersonal” bar). Ideally, they could select appropriate channels to notify their social and work contacts, as well as choose to share their results with public health bodies for surveillance purposes. Social networks could also include schools and sports teams, meaning that teachers and coaches are critical stakeholders at this level (represented in ).
5.2.4. Leveraging technology to fulfil the interpersonal level actions
Regarding leveraging technology at the Interpersonal Level, individuals could choose to notify their network of their test result using texting (SMS), telephone calls, mobile apps, or social media sites, thus facilitating some degree of contact tracing. Individuals may need to use multiple channels to connect with their communities as there may not be one universal system (e.g., seniors may prefer telephone and Gen Z may opt for social media notification). For the most part, current information and communications technology (ICT) solutions could be used for notification, but new channels of communication may be needed. To help individuals discover if they have been exposed to someone who has tested positive for COVID-19, some states have already developed mobile apps (“Washington Exposure Notifications – WA Notify, Citation2020) that leverage Bluetooth technology to exchange random, anonymous codes with the phones of people near the infected user who have also enabled the app. Individuals using the app who have been in close contact with another user testing positive COVID-19, receive anonymous notifications of possible exposure. A critical mass of users is needed to maximise the effectiveness of this technology. An easy installation process, combined with endorsement of community and organisational leaders can create an elevated level of stakeholder buy-in. Additionally, technology organisations can be transparent about how home testing data is used to minimise consumers’ privacy concerns (Sheldon, Citation2020). These novel forms of surveillance and contact notification need not replace traditional efforts led by public health bodies, but rather can be a useful supplement.
5.2.5. Organisational level actions
highlights many actions that should occur at the organisational level to maximise the utility and impact of home tests. At the Organizational level, adopting home testing could relieve some pressure on constrained health care services. Self-swabbing and rapid home testing can become the recommended testing method for asymptomatic individuals seeking testing for reasons such as returning to work/school, or prior to travelling which are likely to involve repeated testing at frequent intervals. This would alleviate clinical workload to allow providers to focus on higher risk groups and symptomatic individuals, especially those needing urgent medical attention.
emphasises many organisations that play critical roles in the system-wide success of home testing programs. Diagnostic manufacturers and laboratories are key stakeholders in test development, production, and distribution. Professional associations (such as the American Association for Clinical Chemistry) can play a critical role in creating cultural norms over diagnostic testing (American Association for Clinical Chemistry, Citation2020). Press releases and endorsements of home testing are critical for adoption because “community-based practitioners do not have the time, inclination, or resources to monitor this peer-reviewed literature. Community and government leaders do not read the medical literature, and they are not colleagues of those doing the investigations”. (Vukotich & Charles, Citation2016). Telehealth companies play a vital role, as many home collection COVID-19 kits have received EUA only if associated with a telemedicine encounter (RxOTC tests). Additionally, telehealth follow-up consultations after home testing may have additional value for providing clinical care and follow up recommendations, while minimising risk of spread of the virus. Pharmacies and outpatient clinics may be appropriate outlets to sell or distribute home tests. In times of pandemic, day care centres, schools, and employers may require individuals to be tested before resuming activities in shared workspaces and classrooms. Hospitals may require visitors to complete a home test before entering facilities.
Organizational level players have a crucial role in establishing and maintaining channels for providing test kits that enable rapid delivery and high compliance. Organizations in the transportation chain also have a key role in the safe delivery of patient-collected self-swab samples to a laboratory if test interpretation cannot be completed at home. Shipping carriers play an important role in ensuring such samples are appropriately classified and labelled as infectious or biological substances to ensure both the safety of handling during shipping to the laboratory, as well as maintaining privacy and security (United Parcel Service of America (UPS), Citation2020). If test kits are limited, organisations must have policies and infrastructure in place to determine who should be priority tested and to mitigate the risks of hoarding or selling tests. Health insurance organisations also play a critical role in creating coverage policies for home testing.
5.2.6. Leveraging technology to fulfil the organizational level actions
At the Organization level, home test results could be aggregated to facilitate real-time, comprehensive tracking and contribute to minimising the spread of infection. One technology that has been developed to help organisations manage reopening after closures due to the COVID-19 pandemic is a mobile app that stores test results; for negative test results, the app displays a temporary encrypted digital pass (like an airline boarding pass) with a QR code. Organizations can scan these QR codes to view test results to allow entry into facilities (“Abbott’s New NAVICA App: What You Need to Know”, Abbott’s New NAVICA App: What You Need to Know, Citation2020). This technology may be helpful for stakeholders such as employers and schools. However, for this technology to be deployed effectively, organisation procedures and guidelines need be developed to protect individual privacy around personal health information. Moreover, for successful implementation there needs to be appropriate support for individuals who test positive, in terms of their rights as employees. Organizations can instil a culture where health and safety of employees are valued, and employees feel confident seeking testing to protect themselves and their colleagues from spreading COVID-19.
5.2.7. Community level actions
At the Community level, communities need ample tests available and a critical mass of health consumers willing to share their test results to provide sufficient data for accurate surveillance (see ). This surveillance is essential to provide multiple different types of organisations (e.g., schools, colleges/universities, workplaces, sports organisations, public transportation) with data that is sufficiently accurate and timely to inform appropriate levels of restrictions. News outlets are another essential stakeholder at the community level that can provide information about testing, treatment options (if available), and quarantine restrictions. Ideally, they send a unified, clear message on the home testing process.
5.2.8. Leveraging technology to fulfil the community level actions
At the Community level, home testing data should be also be shared to contribute to public health surveillance. ICT needs to be designed to ensure appropriate levels of data privacy and security. Dashboards that provide key indicators of status should be available and effectively designed to enable providers and public health officials to quickly digest and act upon results. Many people have demonstrated their interest and willingness to share data for public health surveillance; this is evident due to the existence and high compliance with voluntary crowdsourced surveillance systems based on symptoms that have already been implemented in several countries (e.g., GrippeNet.fr and fluNearYou.org) (Guerrisi et al., Citation2018; HealthMap, Citation2020). Data from home testing should be integrated with test data gathered from many other settings (e.g., health care facilities) to be of most value to inform public health efforts. Home testing companies can aggregate results from their users and share anonymised test results with local public health officials to provide data on test positivity rates, geographic “hot spots” etc. With this rapid scale-up augmenting clinic-based surveillance systems, communities have the potential to make more informed decisions based on more accurate, more granular, or more rapid information.
5.2.9. Policy level actions
Regarding the Policy level, translation of home testing to communities will be best achieved if home testing insurance coverage policies are consistent payors and if regulatory guidance supports expansion of safe home testing (see ). The FDA continues to refine its regulatory guidance based on the ever-growing body of COVID-19 research and new diagnostic technology developments for COVID-19 fuelled by federal and industry funding. For example, researchers have established that tests can be conducted by swabbing more easily accessible body parts (such as the lowest part of the nose in contrast to the upper nasal cavity) while maintain test accuracy (Patriquin et al., Citation2020). Additionally, the accuracy of swabbing by lay individuals has been deemed equivalent to swabbing by health care professionals (Tu et al., Citation2020). Policies already exist and will continue to evolve to ensure samples can safely be stored in public-facing collection bins (e.g., at pharmacies) and can be mailed to laboratories in which samples remain stable and postal workers are not exposed to pathogens. The rapid evolution of policies has been highly challenging for test developers, particularly as they try to balance the need for return on investment with the commercial viability of developing test kits beyond the current pandemic. However, this challenge will subside as our understanding of COVID-19 levels out.
5.2.10. Leveraging technology to fulfil the policy level actions
Regarding the use of technology that supports the policy level, for home collection kits that require authorisation from a provider (RxOTC tests), individuals could complete an online screening to determine their eligibility for home testing. Additionally, some home test companies require a telemedicine visit as part of this process to help ensure proper sample collection and to support patients’ clinical care, which creates a need for connection with health organisations (Organizational level) providing such services. Aggregation of data from home testing (albeit with the caveats we noted above) has the potential to inform policies regarding shutdown/reopening.
6. Reaching the ideal future state: key translational questions
Kolff et al. (see ) used SEM retrospectively to identify missed opportunities for the intended behaviour change to manage an epidemic (increased vaccination). While reflective applications are beneficial to learning, in “facing growing complexity and uncertainty of social and environmental contexts, […] it is more important than ever to reflect todays decisions prospectively and to adjust them in a future-oriented and sustainable way”. (Kosow & Robert, Citation2008 p. 133) Working with scenarios provides a central tool to proactively navigate this complexity and uncertainty. We used SEM prospectively to illuminate key stakeholder decisions, actions, and resources needed to achieve a desired scenario outcome (increased home testing for COVID-19). In alignment with scenario analysis, our narrative description of an ideal future state needs to be plausible and therefore we must recognise risks associated with key turning points, if we are to mitigate missed opportunities and avoid missteps. Key stakeholders and modern technologies need to be ready and responsive to key risks and pinnacle decision points.
Through the lens of a socio-technical SEM, we can assimilate past experiences with home testing, the role of stakeholders, and the possibilities of current technologies to generate questions that explore areas of risk at each SEM level. Indeed, we can derive key questions from our SEM analysis to identify risks associated with actions within and across various levels that may impede the acceleration of the four translational drivers. Questions emerge from the review of potential challenges, risks, and hindrances to the key actions (as presented in ) required of the various SEM roles to achieve the desired outcome. The ultimate goal is that the narrative of the ideal scenario and the questions it generates become a tool to analyse and improve efforts to move home testing into communities.
We provide a model of representative Key Translational Readiness and Response Questions for each SEM level in . The list of questions included in is not exhaustive; however, this list does present illustratively some critical readiness challenges that need to be addressed to achieve system-wide use of home tests in the greater community. By addressing these questions early with risk response planning and other strategies, we can be more proactive in our efforts to expedite widespread diffusion and maximise the impact of home testing.
Figure 5. Key translational readiness and response questions across SEM levels
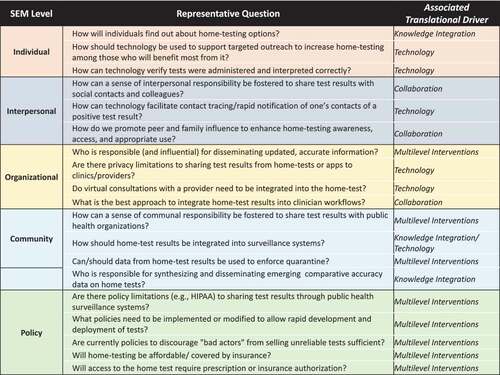
For example, we can leverage the history conveyed in the retrospective Kloff model (see ) towards future situations of promoting vaccination. By asking questions such as, “Who is responsible (and influential) for disseminating updated, accurate information?” (organisation level), we are able to uncover several likely challenges. There are some prevailing stigmas with vaccination that may, in part, be traced to the dissemination of flawed research studies associating vaccination with autism and other adverse outcomes (Pluviano et al., Citation2017; Wolfe & Sharp, Citation2002). When studies were published, these findings caught the attention of the press and were publicly disseminated planting roots of hesitancy and fear towards vaccination by some. Although the journals retracted the articles due to lack of evidence and inconclusive findings, the updated findings were not as widely disseminated, and many people continue to trust the original (outdated) published information (Bordon, Citation2020; Jarrett et al., Citation2015) Even with efforts towards updating misconceptions, “people’s inability to update their memories in light of corrective information may have important public health consequences, as in the case of vaccination choice (Pluviano et al., Citation2017 p. 1)”. While one may think that public health messaging correcting the misinformation would move belief patterns, this has not been the case; and, in fact, such messaging may even enhance rooted misconceptions due to illusory truth resulting from repetition. Therefore, in addressing this readiness and response question, we must look across other SEM levels (e.g., policy, community, interpersonal, organisational) to try to facilitate understanding and appreciation of correct, updated information. Government entities, coalitions, and scientific journals are responsible for (and should continue) disseminating updated and accurate scientific information in ways the public can understand. Furthermore, important that technologies such as social media are leveraged more to ensure important scientific findings reach the general public in spaces where targeted individuals seek information.
Kumar and colleagues found it was the impact of concurrent, multilevel interventions that drove vaccination behaviour during the 2009 H1N1 flu pandemic. Similarly, future home testing interventions must act upon all SEM levels concurrently. In order for effective interventions at each level to occur (and for the ideal future state to be realised), it is important that the translational drivers are in motion. The Key Translational Questions provide platform to do this. The responses to each of these questions has impact on one or more of the translational drivers to accelerate the translation movement. We tag each question (highlighted in green) with possible associated translational driver impact to facilitate the connection of how risks and strategies identified in exploring these questions can impact accelerate movement into communities. We further explain these associations in ensuing paragraphs. While we present these drivers separately, there is a strong interdependent symbiosis among the drivers and in the actions taken to accelerate the drivers.
6.1. Multilevel interventions driver
The multilevel interventions driver is manifested in the Translational Readiness and Response Questions at the Organizational, Community, and Policy levels. In looking across the questions associated with the this driver, it is apparent that determining and assigning responsibilities to stakeholders may be a challenge. Addressing communication and policy challenges will require stakeholders to have direct contact and frequent opportunities to interact to ensure actions at all SEM levels are occurring in tandem. Healthcare leaders must proactively identify those most at risk or most likely to benefit from home testing and determine effective communication channels and responsible stakeholders to notify these individuals about the availability of this testing. Communication efforts could include various types of social media, organisational websites, email, flyers and other common communication mechanisms. Many of these communication channels leverage the technology driver, demonstrating an example of symbiosis between the translational drivers.
6.2. Collaboration driver
We provide representative Translational Readiness and Response Questions related to collaboration among the Interpersonal and Organizational levels in . These collective questions point to fostering a sense of communal responsibility to ensure home tests (and the data they generate) are being widely used and acted upon. Integrating home test data into clinical workflows may be one of the most challenging collaboration tasks and will require committed engagement from testing companies and healthcare organisations. Collaborations will be required to establish best practices and guidelines. For example, at the organisational level, healthcare organisations that support home testing will need to provide guidance to the patient populations they serve on how much contact or guidance home test users should have (or need to have) with the health care system, through routine clinics, or telemedicine services, and ways to integrate or share test results with health care providers, such as existing patient portals or similar. This is particularly true for infectious diseases such as COVID-19, where there have been very few home tests approved for use in the U.S. (with the exception of the over-the-counter HIV test), and thus are breaking new ground.
6.3. Technology driver
Technology is used across levels and responses to risks associated with key questions may point to technological intervention. We specifically call out technology questions from the Individual to Organizational levels, where primary users and most technology developers reside. As COVID-19 home tests continue to be released with increasingly sophisticated technology (including mobile apps), questions about how the technology should be used for various purposes will emerge. At the community level, leveraging technology to support data-sharing and aggregation systems must be developed for COVID-19 test results, regardless of source (e.g., home, clinic); this is essential to provide accurate and timely disease surveillance efforts and knowledge integration to public health bodies and local government. The availability of home tests has multiple policy implications and going forward there needs to be far clearer policies to support test research and development efforts that will lead to accurate and sustainable tests, as well as polices to protect users from tests that may be available for online purchase, but which lack regulatory approval. As home tests become more widely available, policies will be needed to not only protect individual’s rights to their health information, but also to help support safe return to work or school policies. As the numbers of COVID-19 infections reduces (partly from vaccination efforts), and we return to normal activity and usual seasonal viral outbreaks (e.g., influenza, common colds, as well as COVID-19), policies for employers and schools/workplaces informed by the COVID-19 experience will need to be developed on how to deal with respiratory tract symptoms in individuals over the coming years.
6.4. Knowledge integration driver
This driver is often coupled with the other translational drivers, particularly the technology driver. Questions associated with knowledge integration generally revolve around disseminating lessons learned from past experiences and accommodating updates as an epidemic or pandemic situation plays out. Knowledge integration is supported through communication efforts accomplished via technology tools to drive awareness for home testing and integrating home test data into surveillance efforts and other forms of data collection. In addition to supporting technology tools to deliver the knowledge, widespread integration requires collaboration among stakeholders for data sharing and enhancing collective insights. The world’s understanding of the COVID-19 virus continues to evolve at a staggering pace. Deliberate efforts towards knowledge integration will continue to be vital to spawn additional knowledge and ensure all stakeholders are acting upon the latest, most accurate information.
We recognise that that are many stakeholders already working to respond to these challenges. There have been many calls for collaboration, and many partnerships that have formed for pandemic response efforts (Abenoza et al., Citation2020; Bump et al., Citation2021; Vervoort et al., Citation2020). Addressing the questions and resolving the foreseen challenges means working across various levels.
7. Conclusion
Readily available home testing stands as a cornerstone of hope in pandemic management. Migrating home testing innovations from research to communities is critical to reaping the benefits of these innovations. Despite unprecedented investment in test development efforts, there is a void in translational research focused on the translation to practice (T3) and communities (T4). In particular, there has been limited attention to how translational science drivers (collaboration, technology, multilevel interventions and knowledge integration) can lead to improved and more comprehensive implementation of home testing for COVID-19. We have attempted to illustrate this progress through the lens of diffusing home testing to communities.
We propose a broader use of SEM to support narrative scenario analysis that leverages past experiences, present circumstances, and projected realities to proactively address this void. Until now, few studies have extended the use of this model to aspects of epidemic and pandemic management beyond retrospective analyses of efforts to improve vaccination. As a specific demonstration, we proactively applied SEM to create a narrative scenario including “Translational Readiness and Response Questions” to maximise the impact of home testing as part of the COVID-19 pandemic response. SEM provided a pathway for the scenario to depict how to connect scientific products, people, information, processes, and policies in a more accurate, timely, and complete way of translating these tests to communities. Through our SEM analysis, we found that successful implementation of home testing requires (1) identifying ways to continually improve processes and policies to better support evolving pandemic management goals and conditions of spread, (2) establishing interconnectedness among stakeholders, and (3) leveraging various technology and communication platforms. Overall, the SEM “lens” promoted a more comprehensive understanding of the stakeholders involved and the roles they play in the success of home testing efforts for COVID-19 and the interconnected challenges they face. The effective translation of home testing into communities requires the interconnectedness of the whole diagnostic testing system to accelerate the four translation science drivers.
Our resulting position is that SEM can be used to provide a holistic, socio-technical perspective towards narrative scenario analysis that can help prospectively identify (1) stakeholders and the roles they need to fulfil (2) how technology can be leveraged as the line of connection among stakeholders and can enable integrated multilevel responses, and 3) barriers and risks (through exploring key readiness and response questions) to minimise missed opportunities and maximise the clinical, community, policy, economic benefits of home testing.
A robust SEM supported narrative could be a key component to guide federal efforts to disseminate home based testing, including as part of the NIH Rapid Acceleration of Diagnostics (RADx) Initiative, which aims to accelerate the development and commercialisation of diagnostic tests for COVID-19 (Tromberg et al., Citation2020). For diagnostic test developers, our proposed approach could be valuable in itself for helping them understand the multiple components that will be needed for successful deployment of home tests. For public health organisations, we believe our approach could help to support efforts to use results of home testing for innovative pandemic surveillance efforts, and to guide decision making around test regulatory approval and deployment. Using SEM as a multilevel, scenario analysis tool empowers key decision makers to proactively design interventions that facilitate actions across SEM levels. This can potentially fuel a robust risk analysis and also minimise missed opportunities where collaboration and support can have great impact. In sum, without this perspective, we miss risks that should be addressed, transient windows of opportunities, and possible actors that can play a role in the coherent assembly of a functional system.
Acknowledgments
The authors report no conflict of interest.
Efforts that helped to shape this paper were partly supported by the following:
National Institute of General Medical Sciences, U54 GM115458, which funds the Great Plains IDeA-CTR Network.
The greater Seattle Coronavirus Assessment Network (SCAN). SCAN is a partnership between the team behind the Seattle Flu Study and Public Health — Seattle & King County. It is executed by the Brotman Baty Institute, a collaboration between UW Medicine, Fred Hutchinson Cancer Research Center, and Seattle Children’s. SCAN is funded by Gates Ventures (the private office of Bill Gates) and receives technical guidance from the Bill & Melinda Gates Foundation and the Centers for Disease Control and Prevention.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, the Great Plains IDeA-CTR Network, Gates Ventures, or the other collaborators in SCAN, listed above.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abbott. (2020). Abbott’s Fast, $5, 15-minute, Easy-to-use COVID-19 Antigen Test Receives FDA Emergency Use Authorization; Mobile App Displays Test Results to Help Our Return to Daily Life; Ramping Production to 50 Million Tests a Month [Press release]. Retrieved from https://abbott.mediaroom.com/2020-08-26-Abbotts-Fast-5-15-Minute-Easy-to-Use-COVID-19-Antigen-Test-Receives-FDA-Emergency-Use-Authorization-Mobile-App-Displays-Test-Results-to-Help-Our-Return-to-Daily-Life-Ramping-Production-to-50-Million-Tests-a-Month
- Abbott’s New NAVICA App: What You Need to Know. (2020). [Press release]. Retrieved from https://www.abbott.com/corpnewsroom/diagnostics-testing/abbotts-new-NAVICA-app-what-you-need-to-know.html
- Abenoza, N., Hernandez, C., Martinez, E., Mora, J., & Siker, M. (2020). ‘Knowing what’s best’: Community partnerships against COVID-19. Wisconsin Medical Journal (Madison, Wis.), 119(2), 76-76. https://pubmed.ncbi.nlm.nih.gov/32659055
- Alcorn, T. (2019, January 14). The strange marketplace for diabetes test strips. TheNew York Times. Retrieved from https://www.nytimes.com/2019/01/14/health/diabetes-test-strips-resale.html
- American Association for Clinical Chemistry. (2020). The Nation Needs More Evidence Before Relying on Home Test Collection Kits for COVID-19 [Press release]. Retrieved from https://www.aacc.org/media/press-release-archive/2020/04-apr/more-evidence-needed-on-home-test-collection-kits-for-covid19
- Araz, O. M., Ramirez-Nafarrate, A., Jehn, M., & Wilson, F. A. (2020). The importance of widespread testing for COVID-19 pandemic: Systems thinking for drive-through testing sites. Health Systems, 9(2), 119–123. https://doi.org/https://doi.org/10.1080/20476965.2020.1758000
- Berger, K. (2020, July 30). COVID-19 at-home test kits: What we know. SingleCare. Retrieved from https://www.singlecare.com/blog/news/at-home-coronavirus-tests/
- Bordon, Y. (2020). Public trust in vaccines. Nature Reviews. Immunology. Retrieved from https://www.nature.com/articles/d42859-020-00024-5
- Brailsford, S., Harper, P., Lerouge, C., & Payton, F. C. (2012). Editorial. Health Systems, 1(1), 1. https://doi.org/https://doi.org/10.1057/hs.2012.9
- Branch, J. (2020, January 20). Should you trust a rapid diagnostic test? Consumer Reports. Retrieved from https://www.consumerreports.org/medical-tests/rapid-diagnostic-test-should-you-trust/
- Buirse, L. E. (2020, March 6). What you need to know about pre-employment drug tests. Concentra. Retrieved from https://www.concentra.com/resource-center/articles/what-do-you-need-to-know-about-pre-employment-drug-tests/
- Bump, J. B., Friberg, P., & Harper, D. R. (2021). International collaboration and covid-19: What are we doing and where are we going? BMJ (Online), 372, n180–n180. doi:https://doi.org/https://doi.org/10.1136/bmj.n180
- Cameron, C., Coyle, D., Ur, E., & Klarenbach, S. (2010). Cost-effectiveness of self-monitoring of blood glucose in patients with type 2 diabetes mellitus managed without insulin. Canadian Medical Association Journal, 182(1), 28–34. https://doi.org/https://doi.org/10.1503/cmaj.090765
- Catalyst, H. (Producer). (2020). Pathfinder: Clinical and translational research spectrum. Harvard Catalyst. Retrieved from https://catalyst.harvard.edu/pathfinder/
- Centers for Disease Control and Prevention. (2019, May 12). HIV and STD criminal laws. HIV. Retrieved from https://www.cdc.gov/hiv/policies/law/states/exposure.html
- Centers for Disease Control and Prevention. (2020, July 20). HIV self-testing (home testing), can I get an HIV test to use at home or in a private location? HIV. Retrieved from https://www.cdc.gov/hiv/basics/hiv-testing/hiv-self-tests.html
- Chu, H., Boeckh, M., Englund, J., Famulare, M., Lutz, B., Nickerson, D., … Bedford, T. (2020). The seattle flu study: A multi-arm community-based prospective study protocol for assessing influenza prevalence, transmission, and genomic epidemiology. BMJ Open 2020;10:e037295. doi:https://doi.org/10.1136/bmjopen-2020-037295
- Cleveland Clinic. (2017, June 21). Your guide to pregnancy tests. Retrieved from https://my.clevelandclinic.org/health/articles/9703-your-guide-to-pregnancy-tests
- COVIDENTIFY - A Duke University Study. (2020). Retrieved from https://covidentify.covid19.duke.edu/
- Craighead, C. (2020). Two new self-collected, walk-up COVID-19 testing sites open in Seattle to expand testing options. Seattle PI. Retrieved fromhttps://www.seattlepi.com/coronavirus/article/seattle-covid-testing-northgate-central-district-15781721.php
- Cramer, R. J., & Kapusta, N. D. (2017). A social-ecological framework of theory, assessment, and prevention of suicide. Frontiers in Psychology, 8, 1756. https://doi.org/https://doi.org/10.3389/fpsyg.2017.01756
- De Bruin, B., Galesic, W., Parker, A. M., M., & Vardavas, R. (2020). The role of social circle perceptions in “False consensus” about population statistics: evidence from a national flu survey. Medical Decision Making, 40(2), 235–241. https://doi.org/https://doi.org/10.1177/0272989X20904960
- Deng, X., Gu, W., Federman, S., Du Plessis, L., Pybus, O. G., Faria, N. R., … Chiu, C. Y. (2020). Genomic surveillance reveals multiple introductions of SARS-CoV-2 into Northern California. Science (American Association for the Advancement of Science), 369(6503), 582–587. https://doi.org/https://doi.org/10.1126/science.abb9263
- Dougherty, D., & Conway, P. H. (2008). The “3T’s” Road map to transform US health care: The “How” of high-quality care. JAMA: The Journal of the American Medical Association, 299(19), 2319–2321. https://doi.org/https://doi.org/10.1001/jama.299.19.2319
- Doughton, S. (2020). New coronavirus monitoring program launched in Seattle based on home-test kits. The Seattle Times. Retrieved from https://www.seattletimes.com/seattle-news/health/new-coronavirus-surveillance-program-launched-in-seattle-based-on-home-test-kits/
- Everlywell. (2020). At-home lab testing made easy. Retrieved fromhttps://www.everlywell.com/
- FDA Authorizes Ellume COVID-19 Home Test as First Over-the-Counter Fully At-Home Diagnostic Test. (2020). Globenewswire. https://www.globenewswire.com/news-release/2020/12/15/2145612/0/en/FDA-Authorizes-Ellume-COVID-19-Home-Test-as-First-Over-the-Counter-Fully-At-Home-Diagnostic-Test.html
- Fernandez-Moure, J. S. (2016). Lost in Translation: The Gap in Scientific Advancements and Clinical Application. Frontiers in Bioengineering and Biotechnology, 4, 43. https://doi.org/https://doi.org/10.3389/fbioe.2016.00043
- Figueroa, M. E. (2017). A theory-based socioecological model of communication and behavior for the containment of the ebola epidemic in liberia. Journal of Health Communication, 22(sup1), 5–9. https://doi.org/https://doi.org/10.1080/10810730.2016.1231725
- Fleshler, D. (2019, November 19). Glucose test strips for diabetes: Uses, accuracy, and costs explained. Healthline. Retrieved from https://www.healthline.com/diabetesmine/glucose-test-strips-diabetes-uses-accuracy-costs#1
- Frew, P. M., Archibald, M., Hixson, B., & Del Rio, C. (2011). Socioecological influences on community involvement in HIV vaccine research. Vaccine, 29(36), 6136–6143. https://doi.org/https://doi.org/10.1016/j.vaccine.2011.06.082
- Gabriel, M. (1987, June 21). Doctors warn women: Don’t rely on home pregnancy test. Los Angeles Times. Retrieved from https://www.latimes.com/archives/la-xpm-1987-06-21-mn-8979-story.html
- Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A’Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), 21. https://doi.org/https://doi.org/10.2196/jmir.8775
- Groover, H. (2020, April 8). How to get tested for coronavirus in Seattle if you don’t have a car. The Seattle Times. Retrieved from https://www.seattletimes.com/seattle-news/transportation/coronavirus-drive-thru-testing-brings-extra-challenges-for-people-who-dont-drive/
- Guerrisi, C., Turbelin, C., Souty, C., Poletto, C., Blanchon, T., Hanslik, T., Bonmarin, I., Levy-Bruhl, D., & Colizza, V. (2018). The potential value of crowdsourced surveillance systems in supplementing sentinel influenza networks: The case of France. Eurosurveillance, 23(25), 1. doi:https://doi.org/https://doi.org/10.2807/1560-7917.ES.2018.23.25.1700337
- Hall, K. L., Feng, A. X., Moser, R. P., Stokols, D., & Taylor, B. K. (2008). Moving the science of team science forward: Collaboration and creativity. American Journal of Preventive Medicine, 35(2 Suppl), S243–S249. https://doi.org/https://doi.org/10.1016/j.amepre.2008.05.007
- Hayward, M. (2020, May 26). State official: False positive COVID-19 tests very rare; not so with false negatives. New Hampshire Union Leader. Retrieved from https://www.unionleader.com/news/health/coronavirus/state-official-false-positive-covid-19-tests-very-rare-not-so-with-false-negatives/article_369216dc-3a09-5139-8a29-0520bc3c9d63.html
- HealthMap. (2020). Flu Near You. Retrieved from https://flunearyou.org/#!/
- Hopkins, R., Shaver, K., & Weinstock, R. S. (2016). Management of adults with diabetes and cognitive problems. Diabetes Spectrum, 29(4), 224–237. doi:https://doi.org/https://doi.org/10.2337/ds16-0035
- Huang, Y. L. (2014). Social ecological influences on preferences for care provided at the end of life amongst Taiwanese city-dwelling Adults. Queensland University of Technology.
- Ibitoye, M., Frasca, T., Giguere, R., & Carballo-Diéguez, A. (2014). Home testing past, present and future: Lessons learned and implications for HIV home tests (A review). AIDS and Behavior, 18(5), 933–949. doi:https://doi.org/https://doi.org/10.1007/s10461-013-0668-9
- Jarrett, C., Wilson, R., O’Leary, M., Eckersberger, E., & Larson, H. J. (2015). Strategies for addressing vaccine hesitancy – A systematic review. Vaccine, 33(34), 4180–4190. https://doi.org/https://doi.org/10.1016/j.vaccine.2015.04.040
- Kelliher, F. (2020, March 16). Kaiser opens drive-thru COVID-19 testing, but members only. The Mercury News. Retrieved from https://www.mercurynews.com/2020/03/16/kaiser-opens-drive-thru-covid-19-testing-but-members-only/
- Khoury, M. J., Clauser, S. B., Freedman, A. N., Gillanders, E. M., Glasgow, R. E., Klein, W. M. P., & Schully, S. D. (2011). Population Sciences, Translational Research, and the Opportunities and Challenges for Genomics to Reduce the Burden of Cancer in the 21st Century. Cancer epidemiology, biomarkers & prevention,20(10), 2105–2114. https://doi.org/https://doi.org/10.1158/1055–9965
- Khoury, M. J., Gwinn, M., & Ioannidis, J. P. A. (2010). Khoury et al. Respond to “The epicenter of translational science”: Crossing All the T’s. American Journal of Epidemiology, 172(5), 528–529. doi:https://doi.org/https://doi.org/10.1093/aje/kwq214
- Kliff, S. (2020, June 25). Arizona ‘Overwhelmed’ with demand for tests as U.S. system shows strain. The New York Times. Retrieved from https://www.nytimes.com/2020/06/25/upshot/virus-testing-shortfall-arizona.html
- Koczula, K. M., Gallotta, A., & Estrela, P. (2016). Lateral flow assays. Essays in Biochemistry, 60(1), 111–120. https://doi.org/https://doi.org/10.1042/EBC20150012
- Kolff, C. A., Scott, V. P., & Stockwell, M. S. (2018). The use of technology to promote vaccination: A social ecological model based framework. Human Vaccines & Immunotherapeutics, 14(7), 1636–1646. https://doi.org/https://doi.org/10.1080/21645515.2018.1477458
- Konty, K. J., Bradshaw, B., Ramirez, E., Lee, W.-N., Signorini, A., & Foschini, L. (2019). Influenza surveillance using wearable mobile health devices. Online Journal of Public Health Informatics, 11(1). https://journals.uic.edu/ojs/index.php/ojphi/article/view/9758
- Kosow, H., & Gaßner, R. (2008). Methods of future and scenario analysis. Overview, assessment, and selection criteria (Vol. 39). German Development Institute.
- Kosow, H., & Robert, G. (2008). Methods of future and scenario analysis. Overview, assessment, and selection criteria (Vol. 39). German Development Institute.
- Kumar, S., Quinn, S. C., Kim, K. H., Musa, D., Hilyard, K. M., & Freimuth, V. S. (2012). The social ecological model as a framework for determinants of 2009 H1N1 influenza vaccine uptake in the United States. Health Education & Behavior, 39(2), 229–243. https://doi.org/https://doi.org/10.1177/1090198111415105
- Lam, T. K., Spitz, M., Schully, S. D., & Khoury, M. J. (2013). “Drivers” of translational cancer epidemiology in the 21st century: Needs and opportunities. Cancer Epidemiology, Biomarkers & Prevention, 22(2), 181–188. https://doi.org/https://doi.org/10.1158/1055-9965.EPI-12-1262
- Leavitt, S. (2006). “A private little Revolution”: The home pregnancy test in American Culture. Bulletin of the History of Medicine, 80(2), 317–345. https://doi.org/https://doi.org/10.1353/bhm.2006.0064
- Leins, C. (2020). Colorado speeds up coronavirus testing with drive-thru option. US News & World Report. Retrieved from March 13,2020 https://www.usnews.com/news/national-news/articles/2020-03-13/colorados-drive-thru-coronavirus-testing-faces-early-challenges
- McClarty, L. M., Lorway, R. R., Ramanaik, S., Wylie, J., & Becker, M. L. (2015). Factors influencing frontline health service providers’ likelihood to recommend a future, preventive HIV vaccine to key populations in Karnataka, south India. Vaccine, 33(5), 656–663. https://doi.org/https://doi.org/10.1016/j.vaccine.2014.12.009
- McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion programs. Health Education & Behavior, 15(4), 351–377. https://doi.org/https://doi.org/10.1177/109019818801500401
- Morga, A. (2020, July 21). When a 10-year-old translated for her parents on live radio, thousands recognized themselves. KQED. Retrieved from https://www.kqed.org/news/11829745/when-a-10-year-old-translated-for-her-parents-on-live-radio-thousands-recognized-themselves
- National Library of Medicine (U.S). (2020, January 29-2020, July 22). Home testing of respiratory illness. Identifier NCT04245800. https://clinicaltrials.gov/ct2/show/NCT04245800
- Nuss, H., Williams, D., Hayden, J., & Huard, C. (2012). Applying the social ecological model to evaluate a demonstration colorectal cancer screening program in Louisiana. Journal of Health Care for the Poor and Underserved, 23(3), 1026–1035. https://doi.org/https://doi.org/10.1353/hpu.2012.0120
- Nuss, H. J., Hester, L. L., Perry, M. A., Stewart‐Briley, C., Reagon, V. M., & Collins, P. (2016). Applying the social ecological model to creating asthma‐friendly schools in Louisiana. Journal of School Health, 86(3), 225–232. https://doi.org/https://doi.org/10.1111/josh.12369
- Nyambe, A., Hal, V. G., & Kampen, J. K. (2016). Screening and vaccination as determined by the social ecological model and the theory of triadic influence: A systematic review. BMC Public Health, 16(1), 1166-1166. https://doi.org/https://doi.org/10.1186/s12889-016-3802-6
- Nyambe, A., Van Hal, G., & Kampen, J. K. (2016). Screening and vaccination as determined by the social ecological model and the theory of triadic influence: A systematic review. BMC Public Health, 16(1), 1166. https://doi.org/https://doi.org/10.1186/s12889-016-3802-6
- Park, C., Mariakakis, A., Yang, J., Lassala, D., Djiguiba, Y., Keita, Y., … Patel, S. (2020). Supporting smartphone-based image capture of rapid diagnostic tests in low-resource settings. Paper presented at the Proceedings of the 2020 International Conference on Information and Communication Technologies and Development, Guayaquil, Ecuador. https://doi.org/https://doi.org/10.1145/3392561.3394630
- Patriquin, G., Davis, I., Heinstein, C., MacDonald, J., Hatchette, T. F., & LeBlanc, J. J. (2020). Exploring alternative swabs for use in SARS-CoV-2 detection from the oropharynx and anterior nares. Journal of Virological Methods, 285, 113948-113948. https://doi.org/https://doi.org/10.1016/j.jviromet.2020.113948
- Pebody, R. (2019, June). False negative results on HIV tests. aidsmap. Retrieved from https://www.aidsmap.com/about-hiv/false-negative-results-hiv-tests#:~:text=False%20negative%20results%20most%20often,being%20accurate%20is%20over%2099.9%25
- Pifer, R. (2020, May 15). UnitedHealth, Microsoft launch COVID-19 screening app for employers. Healthcare Dive. Retrieved from. https://www.healthcaredive.com/news/unitedhealth-microsoft-covid-19-screening-app-employers-work/578068/
- Pluviano, S., Watt, C., Della Sala, S., & Moore, A. C. (2017). Misinformation lingers in memory: Failure of three pro-vaccination strategies. PloS One, 12(7), e0181640. doi:https://doi.org/https://doi.org/10.1371/journal.pone.0181640
- Puckrein, G. A., Nunlee-Bland, G., Zangeneh, F., Davidson, J. A., Vigersky, R. A., Xu, L., Parkin, C. G., & Marrero, D. G. (2016). Impact of CMS competitive bidding program on medicare beneficiary safety and access to diabetes testing supplies: A retrospective, longitudinal analysis. Diabetes Care, 39(4), 563–571. https://doi.org/https://doi.org/10.2337/dc15-1264
- Rogers, E. M. (2003). Diffusion of Innovations (5th ed.). Free Press.
- Scarneo, S. E., Kerr, Z. Y., Kroshus, E., Register-Mihalik, J. K., Hosokawa, Y., Stearns, R. L., DiStefano, L. J., & Casa, D. J. (2019). The socioecological framework: A multifaceted approach to preventing sport-related deaths in high school sports. Journal of Athletic Training, 54(4), 356–360. https://doi.org/https://doi.org/10.4085/1062-6050-173-18
- Seshadri, D. R., Davies, E. V., Harlow, E. R., Hsu, J. J., Knighton, S. C., Walker, T. A., Voos, J. E., & Drummond, C. K. (2020). Wearable sensors for COVID-19: A call to action to harness our digital infrastructure for remote patient monitoring and virtual assessments. Frontiers in Digital Health, 2. https://doi.org/https://doi.org/10.3389/fdgth.2020.00008
- Sheldon, L. (2020, December 7, 2020). WA Notify reaches 1.2 million users, privacy and tech expert weighs in. Kiro 7 News. Retrieved from https://www.kiro7.com/news/local/wa-notify-reaches-12-million-users-privacy-tech-expert-weighs/4BQO7TDNZ5DLFAHLWHRVPOQQBA/
- Spaniol, M. J., & Rowland, N. J. (2019). Defining scenario. Futures & Foresight Science, 1(1), e3–n/a. doi:https://doi.org/https://doi.org/10.1002/ffo2.3
- Specht, I., Sani, K., Botti-Lodovico, Y., Hughes, M., Heumann, K., Bronson, A., … Sabeti, P. C. (2021). The Case for Altruism in Institutional Diagnostic Testing. medRxiv, 2021.2003.2016.21253669. https://doi.org/https://doi.org/10.1101/2021.03.16.21253669
- Stocks, N., & Chilver, M. (2019). Testing patients visiting a general practice suspected of having Influenza using an in-home test for influenza vs. PCR gold-standard test. Australian New Zealand Clinical Trials Registry [Internet] Retrieved May 31 2020 http://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=377981&isReview=true
- Szilagyi, P. G. M. D. M. P. H. (2009). Translational research and pediatrics. Academic Pediatrics, 9(2), 71–80. https://doi.org/https://doi.org/10.1016/j.acap.2008.11.002
- Taplin, S. H., Anhang Price, R., Edwards, H. M., Foster, M. K., Breslau, E. S., Chollette, V., Prabhu Das, I., Clauser, S. B., Fennell, M. L., & Zapka, J. (2012). Introduction: Understanding and influencing multilevel factors across the cancer care continuum. JNCI Monographs, 2012(44), 2–10. https://doi.org/https://doi.org/10.1093/jncimonographs/lgs008
- Terrie, Y. (2009). At-home diagnostic kits: A growing trend. Pharmacy Times. Retrieved from https://www.pharmacytimes.com/publications/issue/2009/2009-03/2009-03-10050
- The social-ecological model: a framework for violence prevention. (2015). Atlanta. National Center for Injury Prevention and Control, Centers for Disease Control.
- Tromberg, B. J., Schwetz, T. A., Pérez-Stable, E. J., Hodes, R. J., Woychik, R. P., Bright, R. A., Fleurence, R. L., & Collins, F. S. (2020). Rapid scaling up of Covid-19 diagnostic testing in the United States — The NIH RADx initiative. The New England Journal of Medicine, 383(11), 1071–1077. https://doi.org/https://doi.org/10.1056/NEJMsr2022263
- Tu, Y.-P., Cangelosi, G. A., Jennings, R., Wood, R. C., Verma, P., Wood, R. C., Verma, P., Vojta, D., & Berke, E. M. (2020). Swabs collected by patients or health care workers for SARS-CoV-2 testing. The New England Journal of Medicine, 383(5), 494–496. https://doi.org/https://doi.org/10.1056/NEJMc2016321
- U.S. Food & Drug Administration. (2019a). Home Use Tests. Retrieved from https://www.fda.gov/medical-devices/vitro-diagnostics/home-use-tests
- U.S. Food & Drug Administration. (2019b). Home Use Tests: Pregnancy. Retrieved from https://www.fda.gov/medical-devices/home-use-tests/pregnancy#:~:text=What%20does%20this%20test%20do,only%20when%20you%20are%20pregnant
- U.S. Food and Drug Administration. (2020a, May 29). Coronavirus (COVID-19) Update: FDA Takes Steps to Streamline Development of Tests With At-Home Sample Collection. Retrieved from https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-takes-steps-streamline-development-tests-home-sample-collection
- U.S. Food and Drug Administration. (2020b, June 3). Information regarding the OraQuick In-Home HIV Test. Retrieved from https://www.fda.gov/vaccines-blood-biologics/approved-blood-products/information-regarding-oraquick-home-hiv-test
- UCSF TemPredict Study. (2020). Retrieved from https://ouraring.com/ucsf-tempredict-study
- United Parcel Service of America (UPS). (2020). Infectious Substances. Retrieved from https://www.ups.com/us/en/help-center/packaging-and-supplies/special-care-shipments/hazardous-materials/responsibilities/diagnostic.page
- US FDA issues EUA to Lucira COVID-19 All-In-One Test Kit for COVID-19 self-testing at home. (2020). PharmaBiz. Retrieved from http://www.pharmabiz.com/NewsDetails.aspx?aid=133568&sid=2
- Venkatesh, V., Morris, M. G., Davis, G. B., & Davis, F. D. J. M. Q. (2003). User acceptance of information technology: Toward a unified view. MIS Quarterly, 27(3), 425-478. doi:https://doi.org/10.2307/30036540Copy
- Verhagen, L. M., de Groot, R., Lawrence, C. A., Taljaard, J., Cotton, M. F., & Rabie, H. (2020). COVID-19 response in low- and middle-income countries: Don’t overlook the role of mobile phone communication. International Journal of Infectious Diseases, 99, 334–337. https://doi.org/https://doi.org/10.1016/j.ijid.2020.07.069
- Vervoort, D., Ma, X., & Luc, J. G. Y. (2020). COVID-19 pandemic: A time for collaboration and a unified global health front. International Journal for Quality in Health Care 33(1). https://doi.org/https://doi.org/10.1093/intqhc/mzaa065
- Vukotich, J., & Charles, J. (2016). Challenges of T3 and T4 translational research. Journal of Research Practice, 12, 2. Retrieved from https://eric.ed.gov/?id=EJ1121185
- Walker, J. (2019, February 27). The truth about getting a false positive on your pregnancy test. Clearblue. Retrieved from https://www.clearblue.com/pregnancy-tests/false-positive-results#:~:text=Most%20home%20pregnancy%20tests%20are,false%20positive%20is%20extremely%20rare
- Washington Exposure Notifications - WA Notify. (2020). Retrieved from https://www.doh.wa.gov/Emergencies/COVID19/WANotify
- Washington State Department of Health. (2020). Guidance for rideshare and taxi drivers. Novel Coronavirus Outbreak 2020 (COVID-19). Retrieved from https://www.doh.wa.gov/Emergencies/NovelCoronavirusOutbreak2020COVID19/RideshareandTaxiDrivers
- WebMD. (2019, February 17). How much do glucose meters cost? Guidelines for Buying and Using Diabetes Supplies. Retrieved from https://www.webmd.com/diabetes/qa/how-much-do-glucose-meters-cost#:~:text=A%20glucose%20meter%20can%20vary,cost%20around%20%24100%20a%20month
- Wolfe, R. M., & Sharp, L. K. (2002). Anti-vaccinationists past and present. BMJ (Clinical Research Ed.), 325(7361), 430–432. https://doi.org/https://doi.org/10.1136/bmj.325.7361.430
- World Health Organization. (2017). Number of countries adopting HIV self-testing policies rises sharply [Press release]. Retrieved from https://www.who.int/hiv/mediacentre/news/hiv-self-testing-increases/en/
- Ye, Q., Zhou, J., & Wu, H. (2020). Using information technology to manage the COVID-19 pandemic: development of a technical framework based on practical experience in China. JMIR Medical Informatics, 8(6), e19515–e19515. https://doi.org/https://doi.org/10.2196/19515
