
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Waiting time in healthcare is a significant problem that occurs across the world and often has catastrophic effects. There are various terms used for waiting time (“sojourn”, “throughput” etc.) and there is no consensus on how these terms are defined. Ambiguous definitions of waiting time make it difficult to compare and measure the problems related to waiting times and delays in healthcare. We present a systematic search and review of the Operations Research and Management Science (ORMS) literature on delays in healthcare services. We search for articles from 2004 to 2019 and base our search strategy on a well-known healthcare planning and control decision taxonomy. An important step towards reducing the ambiguity in the definitions is to distinguish between access time and waiting time. We provide clear definitions and examples of access time and waiting time, and we classify our search results according to three categories: article type, healthcare service investigated and ORMS technique used to solve the delay problem. We find that half of the ORMS research on the waiting and access time problem is done on Ambulatory Care services. We provide tables for each healthcare service that highlight key definitions, the techniques that are used most often and the healthcare environment where the research is done. This research highlights the significant ORMS research that is done on access and waiting time in healthcare as well as the remaining research opportunities. Moreover, it provides a common language for the ORMS community to solve critical waiting time issues in healthcare.
1. Introduction
Waiting time is a common problem that occurs in the delivery of healthcare services across the world. Although there is a growing body of the literature on how to improve waiting time problems in healthcare, the term “waiting time” is ambiguous in this literature. For instance, waiting time is sometimes reported as the time lapsed from when a patient arrives until the patient is seen by a healthcare professional, whereas in other contexts, waiting time is defined as the time that lapses from when a patient requires a medical intervention (such as after a cancer diagnosis) until the patient is given an appointment to see a healthcare professional or is admitted to hospital. Moreover, “access time”, “queueing”, “throughput” and “sojourn time” are some of the other terms that are also often used to describe time delay concepts in healthcare.
The aim of this article is primarily to eliminate ambiguity on waiting time definitions in the literature of OR/MS applied to healthcare. This is done by providing definitions of waiting times and related terms, whereafter we provide a taxonomic classification of waiting time in healthcare for different healthcare services.
This taxonomy is derived from the body of the literature pertaining to capacity planning and control decisions in the domain of Operations Research and Management Sciences (ORMS) applied to healthcare. Resource capacity planning and control decisions in healthcare have proven to result in significant efficiency improvements in healthcare delivery (Hulshof et al., Citation2012). Since capacity planning and control decisions are directly related to access to resources, we argue that waiting time is a function of resource capacity planning and control decisions.
Our research clarifies the aforementioned terms for future work on improving waiting and access times in healthcare. This article also provides a systematic overview of the scientific principles used by the ORMS community to solve the waiting time problem in healthcare.
This article is structured as follows: We explain our systematic literature search method that is based on the taxonomy of Hulshof et al. (Citation2012) in Section 2. In Section 3 we explain the categorisation of the literature and provide waiting time and access time definitions and examples. In Section 4 we illustrate the results of the literature categorisation. We elaborate on what was found on waiting and access time in the literature in Section 5 and discuss the main findings in Section 6. Finally, Section 7 presents future research.
2. Search method
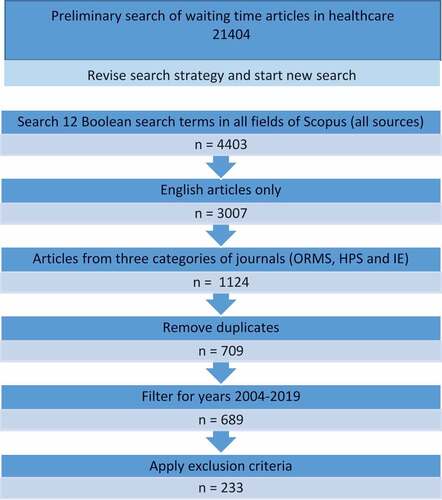
In this section, we explain the reasoning behind our search strategy. The exclusion criteria are also motivated, and we conclude the section with an article tree that shows how we obtained the 233 articles that were analysed.
We conducted a systematic search and review, which combines the strengths of critical review with a comprehensive search process (Grant & Booth, Citation2009). In order to determine how the literature describes waiting time and access time in healthcare, we conducted a preliminary journal article search by combining waiting time and healthcare search terms in Scopus, as follows:
“Wait* time*” AND (“healthcare” OR “health care”)
We focus on the years from 2004 to 2019 to ensure that we include the most recent research as well as research over a substantial time horizon of 15 years.
The result of this broad preliminary search was more than 20,000 articles. We subsequently developed a more refined search strategy and conducted a new search. In the remainder of this section, we describe how we scoped down the search in two steps: (1) by only including literature from specific sources, (2) and by deriving more effective keyword combinations for search terms from the taxonomy of resource capacity planning and control decisions by Hulshof et al. (Citation2012).
Since our aim is to provide a framework and taxonomic classification of waiting time in healthcare for the ORMS community, we scope our search on journal articles from three categories in the InCites Journal Citation Report (JCR) from Clarivate Analytics list
Operations Research and Management Science (ORMS) – this category includes journal topics on stochastic and mathematical modelling, decision theory and systems, and optimisation theory, amongst others. Examples of journals in this category are Operations Research and the Journal of Operations Management
Health Policy and Services (HPS) – resources in this category are journals pertaining to healthcare provision and management and health policy (e.g., Health Care Management Science, Health Care Management Review).
Industrial Engineering (IE) – journals in this category cover topics, such as operations research, process engineering, and productivity engineering. Many journals in this category are similar to the journals in the ORMS category. Examples of journals exclusive to this category are Computer and Industrial Engineering and the International Journal of Lean Six Sigma.
Other journals – two other journals (Health Systems and Operations Research for Health Care) are not part of the ORMS, HPS, or IE categories in Clarivate Analytics but frequently publish research by the ORMS community. Therefore, they are also included in the search.
As mentioned, our search strategy is further scoped down based on the taxonomy by Hulshof et al. (Citation2012). Hulshof et al. (Citation2012) developed a taxonomic classification of planning decisions in healthcare based on the extensive body of the literature on the subject in the field of ORMS in healthcare. This taxonomy is a comprehensive overview of the typical capacity planning and control decisions that are taken in healthcare at hierarchical levels (vertical axis) and in care services (horizontal axis). shows the elements of the taxonomy.
Figure 1. The taxonomy of resource capacity planning and control decisions (From Hulshof et al., Citation2012).
The horizontal axis represents various services in healthcare classified by Hulshof et al. (Citation2012), as follows:
Ambulatory Care services – a care service that is either free-standing or part of a hospital and provides care to patients without offering a bed and board. E.g., primary care services, radiology.
Emergency Care services – a service concerned with treatment and evaluation of urgent medical problems such as trauma patients, which can either be provided in a hospital or outside a hospital by means of for example, an ambulance.
Surgical Care services – a care service that provides surgical interventions to patients. This type of care takes place in a hospital’s operating room or surgical day care centres.
Inpatient Care services – these services provide care to patients in a hospital environment and include a bed and boarding.
Home Care services – community-based services provided at a patient’s home. The service is often a combination of multiple health and nursing services.
Residential Care services – these services provide assistance with daily living activities with nursing/medical services provided only as required.
The resource capacity planning and control decision taxonomy divides the vertical axis into four hierarchical planning stages that are associated with both the time horizon of the decisions to be made as well as the granularity of these decisions (Hans et al., Citation2012).
The hierarchical planning stages on the vertical axis are as follows:
Strategic planning – decisions pertaining to the design and development of the healthcare process. These decisions have a long planning horizon and are informed on an aggregate level such as demand forecasts.
Tactical planning – tactical planning decisions are made to facilitate the organisation of necessary resources required for operational implementation of strategic guidelines. The result of tactical planning decisions is a blueprint for resource allocation to tasks, patient groups, and specialities at an operational level.
Operational planning – short-term decision making to execute the delivery of healthcare. Contrary to higher planning levels, resource capacities are fixed. Operational planning can be further divided into offline and online operational planning. Offline operational planning is concerned with decisions made regarding advance coordination of activities that will serve current elective demand of healthcare services. Online operational planning can be considered as control decisions made based on the monitoring of actual performance of healthcare services and reacting to unforeseen events.
In our study, we leave strategic planning and control decisions out of our scope. Since these decisions are forecast-based and concern structural capacity decisions (e.g., hiring/firing, education, capacity expansion, layout), they only indirectly affect waiting or access time. We thus focus our literature search to tactical and operational decision-making processes, which (may) directly affect waiting. Concerning the taxonomy’s services, we scope our study to include all six healthcare services.
Our scoping process has led us to focus on 12 planning and control decision themes on tactical and operational levels, deduced from the capacity taxonomy of Hulshof et al. (Citation2012). shows the result of the first scoped literature search, using the search terms concerning the theme, along with the following Boolean terms to specifically look for articles that address waiting issues:
Table 1. Number of articles found per theme and search term.
This first scoped search resulted in a total of 4403 articles. We filtered these articles and only kept English language articles published between 2004 and 2019 in journals that belong to the InCites JCR categories of ORMS, HPS, and IE as well as the journals Health Systems and Operations Research for Health Care. All 689 abstracts were read. We omitted articles without any aim to solve a waiting time/access time/throughput/queueing problem in one of the healthcare services under investigation. Then, we applied the following general exclusion criteria:
Exclude articles with the primary objective to reduce cost or increase resource utilisation.
Exclude articles that investigate/evaluate the clinical outcomes as a result of waiting time/access time/throughput problems/queueing.
Exclude articles that analyse of duration of healthcare services without addressing waiting time/accesstime/throughput/queueing problem.
Exclude articles that analyse/predict no-show probability without addressing waiting time/access time/throughput/queueing problem.
After completing the screening phase, 233 articles remained. The article tree in details the search process.
Figure 2. Article tree.
3. Categorisation approach
Section 3 explains our categorisation approach of the 233 articles based on three attributes, namely waiting time vs. access time, healthcare service, and Operations Research and Operations Management (OR/OM) techniques. We provide important definitions of waiting time and access time classification based on whether a patient has entered the healthcare habitat to be served.
shows the 233 articles per theme that remained after the screening process.
Table 2. Results per theme.
A first impression after reading the articles confirmed that there are no generally accepted or unambiguous definitions for waiting time, access time, queueing time, and throughput. We also found that there are roughly two types of articles in our results: 1) the ones addressing waiting to for getting access to a care provider; 2) the ones addressing waiting for service while being inside the care provider’s organisation. We therefore propose to distinguish between a waiting time type article when the aim is to solve a delay problem inside the healthcare habitat where the patient gets serviced, and an access time type article where the article addresses waiting before the patient is allowed to enter the healthcare habitat. Patients are considered to be allowed to enter the healthcare habitat, i.e., have been granted access, when they have an appointment, or are allowed to walk-in, or have been admitted to a bed (ward, ICU, etc.). We further motivate that the term “access time” (to a service) is less ambiguous than “waiting time” since “access” is arguably immediately associated with the process of accessing a service, whilst “waiting” is used more commonly for any delay. This brings us to the following definitions:
Definition 1. Access time is the time that a patient waits before being allowed to enter the healthcare habitat to receive service.
Definition 2. Waiting time is the time that a patient waits for service while having been granted access to the healthcare habitat.
To illustrate how these definitions work, we provide four examples:
Example 1: If a patient is allowed to walk-in anytime, the access time is zero by definition, and hence there can only be waiting time. If, however, the allowed time window for walk-in is in the future, the time until walk-in is access time. When the patient walks in, within the allowed time window, waiting time commences.
Example 2: Assume that a patient has two outpatient appointments on 1 day, say at 9:00–10:00 and at 15:00–15:30. There are two possible situations: (1) The appointments do not require a specific sequence. The access time for each appointment is the time from when the appointment was made until the planned appointment time. Any delay after 9:00 is waiting time for appointment 1, and delay after 15:00 is waiting time for appointment 2. (2) Now say that appointment 2 has to take place any time after appointment 1. Then, the time from 10:00 (planned end time of appointment 1) to 15:00 is access time to appointment 2. Note that in this example the patient is not required to stay in the habitat between the appointments, although in practice in many cases would do so.
Example 3: If a patient receives a surgery date and is admitted (by protocol) the day before, then the access time is the time from when the surgery was planned until hospital admission. We do not consider the time from admission to the planned surgery start time as waiting time, as it is part of the surgical pathway/protocol. However, if the surgery takes place later than the planned start time, this delay is waiting time.
Example 4: If a patient is collected by an ambulance and taken to hospital, the time from when an ambulance is requested until the ambulance arrives at the patient is seen as waiting time. While the patient is in the ambulance, he or she receives emergency medical care and there is no waiting time. When the ambulance arrives at the hospital and there is a delay in offloading the patient due to congestion in the Emergency Department (ED), this is seen as access time. In other words, if there is a delay in giving the patient access to a new healthcare habitat that is different from the location where the patient is, this is seen as access time. If a patient is waiting at the hospital to be transferred to a residential care facility, we also classify this delay as access time.
Example 5: In a remote consult setting (e.g., a video call with a hospital physician), we would consider the time to the scheduled appointment time as access time. Although our access time definition speaks of a patient entering the healthcare habitat, the habitat in this case would be virtual.
We acknowledge that access time may not always be involuntary. A patient may, for example, choose to have (non-urgent) elective surgery scheduled at a more convenient future date, such as after their vacation. The same holds for waiting time. A patient may voluntarily arrive early for an appointment, expecting to have to wait, but hoping to be served earlier. These are cases of voluntary access and waiting time. Involuntary access and waiting time, on the other hand, is a delay in getting access to the healthcare habitat or being serviced in the healthcare habitat when a patient desire service as soon as possible or at a specific appointment time. Whether this “desire” is a personal preference or a clinical urgency may lead to a further distinction of involuntary waiting time. According to Harding et al. (Citation2011), “triage processes are often used by EDs according to the urgency or type of service required” (p. 371). The implication is that some patients may wait longer for services in an ED than others based on their condition. As such ED-practices differ world-wide, and there are various triage systems, we leave the clinical urgency of patients related to waiting and access time outside the scope of our research.
This leads us to provide three attributes according to which articles are categorised:
Attribute 1: Waiting time versus access time
We assigned the attribute of either “waiting time” or “access time” to each article irrespective of which terms the article uses to describe the healthcare delay problem that it aims to solve.
Attribute 2: Healthcare service
All 233 articles were classified according to the healthcare service area on which the research was done, as described by Hulshof et al. (Citation2012).
Attribute 3: Operations Research and Operations Management (OR/OM) techniques
The main OR/OM technique that is used to solve the waiting time/delay problem in each article was recorded. These techniques were grouped by similarity into 10 groups. The technique is the third attribute that was assigned to each article.In addition to the three attributes, relevant quotes, and explanations of waiting and/or access time and similar definitions were captured, which we elaborate on in the next section.
4. Results
We present the results obtained from analysing the 233 articles per attribute as discussed in the categorisation approach section. Results are graphically presented. We also indicate in which journals the most of the articles in our results are published along with the Journal Citation Report (JCR) category that the journals belong to.
The first article categorisation attribute is waiting time versus access time. There are 233 articles in total, of which 8 are literature reviews. Six of the literature review articles can be classified as waiting time type article and one article as an access time type article. This access time type article provides a literature review on simulation techniques that can be used to solve the various outpatient clinic problems (Hong et al., Citation2013). The eighth literature review article is an overview of OR in healthcare (Brailsford & Vissers, Citation2011) and is therefore not classified as a waiting or access time article.
presents the article classification of all articles according to the first categorisation attribute.
Table 3. Article classification according to the attributes “waiting time” and “access time”.
shows the classification of the articles according to the healthcare service attribute. Two of the eight literature review articles (Brailsford & Vissers, Citation2011; Kujala et al., Citation2006) are not assigned to any healthcare service. One of the eight articles (Brailsford & Vissers, Citation2011) is neither assigned to a healthcare service nor classified as either a waiting time or access time type article because it presents an analysis of all the papers presented at the Operations Research Applied to Health Services (ORAHS) annual conference from 1975 to 2009.
The other one (Kujala et al., Citation2006) presents a conceptual framework of a patient’s journey through the entire healthcare system and not one specific healthcare service. The two mentioned articles are placed in the “Other” category.
Figure 3. Article classification according to the healthcare service attribute.
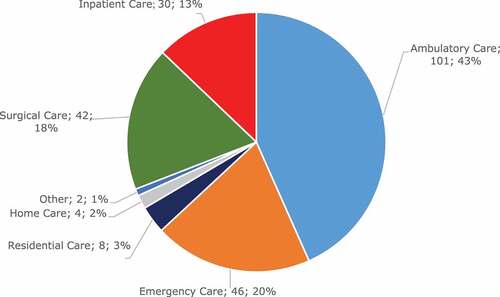
Evidently, most articles belong to Ambulatory Care services. One of the reasons for this is that studies on waiting and access times are often done on outpatient facilities and outpatient access to radiology (Bikker et al., Citation2015; Castro & Petrovic, Citation2012; Conforti et al., Citation2010, Citation2011; Crop et al., Citation2015; Geng et al., Citation2017; Sauré et al., Citation2020; Van Sambeek et al., Citation2011; Vieira et al., Citation2018; Zhou et al., Citation2017). Emergency Care, Surgical Care and Inpatient Care healthcare services have approximately an equal number of articles, whereas significantly fewer articles are on Home Care and Residential Care healthcare services.
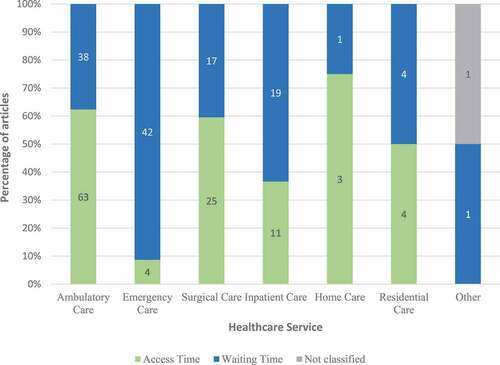
A classification of the articles by both attribute 1 (access versus waiting time) and attribute 2 (healthcare service) is depicted in . Most articles on Ambulatory Care services are access time type of articles (63 articles), which constitutes almost a third (27%) of all articles. Emergency Care services have significantly more waiting time type articles than access time type articles. Emergency Care services are generally available 24/7 and according to our definition in Section 3, access time is only applicable in this context when there is ambulance offload delay. Home Care services have more access time than waiting time type articles, while Inpatient Care and Residential Care services have approximately the same amount of waiting time and access time type of articles.
Figure 4. Article analysis by healthcare service and access time versus waiting time.
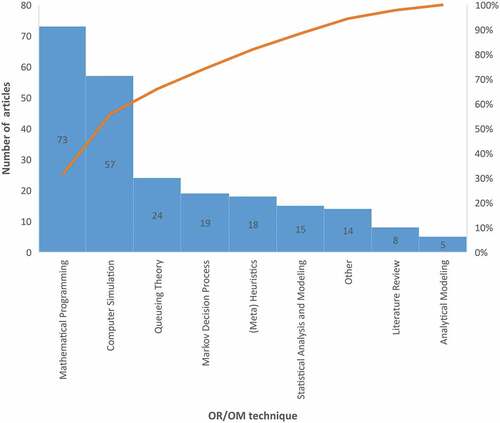
shows the categorisation of articles according to the third attribute (OR/OM technique). Computer Simulation and Mathematical Programming are the most used techniques in these articles. The category “Other” noticeably contains an equal amount of articles as “Statistical Analysis and Modelling” and more articles than the “Literature Review” and “Analytical Modelling” categories. Articles in the “Other” category make use of specific tools such as Fishbone diagrams, Process Design and Answer Set Programming rather than of an OR/OM technique.
Figure 5. Pareto chart of number of articles per OR/OM technique.
A total of 55 journals are represented in the search results, and 54% of the articles occur in six of the 55 journals presented in .
Table 4. List of journals that contain over 50% of the articles analysed.
The most articles occur in Health Care Management Science (39). Other journals with more than five articles are Computers and Industrial Engineering (8), Health Systems (8), IIE Transactions on Healthcare Systems Engineering (8), International Journal of Production Research (6), Omega – International Journal of Management Science (6).
5. Discussion of the found articles
In this section, we discuss the 233 articles that are a result of our search from a delay in healthcare point of view. After a brief discussion on what was found in the articles of each healthcare service, a table is presented for each service that includes key terms and definitions, the OR/OM techniques used most frequently as well as the healthcare environment where most of the research for the particular healthcare service is done.
5.1. Ambulatory care services
5.1.1. Access time type articles
As discussed in Section 4, most articles (101) were found in Ambulatory Care services, of which 63 were classified as access time type articles. This implies that research on delay time in ambulatory care is mostly done on providing access to the healthcare habitat. The healthcare habitat investigated in access time type articles in Ambulatory Care is predominantly outpatient clinics and diagnostic services.
We now present some of the key terms and definitions that were found in the access time type articles in Ambulatory Care. Studies on appointment scheduling for outpatient clinics tend to refer to access times as the delay the patient experiences to access the healthcare system, whereas the waiting time is seen as the patients’ duration of wait while in outpatient facility. This is similar to our definition of access time.
Ma et al. (Citation2016) use the term “waiting time” for patients to get access to oncology treatment. Wait time in this article is the time from when triage is complete until new patient consultancy, which we refer to as access time. Bikker et al. (Citation2015) define access time as the number of calendar days from referral to treatment. This access time includes the time that patients spend attending consultations before treatment. Other articles that elaborate on access times for diagnostic services such as radiotherapy facilities include Geng et al. (Citation2017), Saure et al. (Citation2012) and Zhou et al. (Citation2017).
Other terms used to describe access time as we have defined it include “patients waiting to be scheduled” (Saure et al., Citation2015, p. 586) as well as “waiting time until day of service” (Sauré et al., Citation2020, p. 254). Moreover, the terms “direct waiting time” and “indirect waiting time” occur in articles (Chen & Robinson, Citation2014; Deglise-Hawkinson et al., Citation2018; Geng et al., Citation2017; Patrick, Citation2012; Schacht, Citation2018; Wiesche et al., Citation2017), while Patrick (Citation2012) uses “appointment lead time” to describe the time duration from the date that a patient requests an appointment up to the date of the appointment. Wiesche et al. (Citation2017) define direct waiting time as “the difference between patient arrival time and the time the patient is served by the Primary Care Physician” (p. 404). Therefore, a patient who arrives early for an appointment but is seen on time would experience direct waiting time. Indirect waiting time is defined as “the time between a patient requesting an appointment and the time of that appointment” (Wiesche et al., Citation2017, p. 404). Dogru and Melouk (Citation2019) provide similar definitions “We define indirect waiting time as the difference between the requested appointment time of a patient and the actual scheduled appointment time for that patient. Direct (clinical) waiting time, on the other hand, captures the amount of time between the arrival time of a patient for a scheduled appointment and the actual start time of service” (p. 166).
Some other key terms in the access time type articles in Ambulatory Care are appointment time and open access. Appointment time is the time that a patient waits at the clinic plus the consultation time (Leeftink et al., Citation2019). Open access refers to the scenario in an outpatient facility where there are no advanced appointments but only same day appointments (Huang & Zuniga, Citation2012; Robinson & Chen, Citation2010).
5.1.2. Waiting time type articles
There are 38 Ambulatory Care articles that can be classified as waiting time type articles. Most of these articles (22) investigate appointment scheduling at outpatient facilities. One article (Palmer et al., Citation2018), is a systematic literature review on the use of operational research to model and improve flow in community healthcare and other settings.
White et al. (Citation2011) refer to waiting time as the time a patient spends in the waiting room as well as the time a patient spends waiting for the physician in the consultation room. Wu et al. (Citation2019) divide waiting time for outpatient appointment patients into two parts namely the time from booking the appointment until arrival at the facility and the time from arrival at the facility until receiving the service.
Montecinos et al. (Citation2018) use the term “waiting time” to denote the time from when a walk-in patient arrives at an outpatient clinic until a physician is seen. This is similar to our definition of waiting time but different from the definition of Morikawa and Takahashi (Citation2017) who consider patient waiting time as the time from arrival of a walk-in patient without an appointment at the outpatient clinic until the appointment time allocated to the walk-in patient upon arrival. Research by Anderson et al. (Citation2015) use “wait time” interchangeably for access time to care and waiting time for service.
Idle time and turnaround time are also some of the key terms we found in waiting time type articles in Ambulatory Care. De Vuyst et al. (Citation2014) explain that if the physician arrives later than the scheduled appointment time, it is seen as patient waiting time. If the patient appointment starts at the scheduled time while the physician completed the previous patient consultation earlier, De Vuyst et al. (Citation2014) regard the time that the physician waits for the patient as idle time of the physician. The term idle time is also used with reference to patients by Jiang et al. (Citation2012), who refer to patient idle time as the time from when a patient arrives early for an appointment until the patient is served where the service occurs on the time originally agreed upon. Kong et al. (Citation2013) define turnaround time as “the time from the moment the patient walks into the clinic to the moment the patient leaves the clinic” (p. 712). Turnaround time in this context is therefore a synonym for appointment time according to Leeftink et al. (Citation2019) and can include administrative activities after the clinical appointment.
A summary of the results from literature on waiting and access times (as we have defined it) in Ambulatory Care services is shown in :
Table 5. Summary of Ambulatory Care services articles.
5.1.3. Aggregate overview: ambulatory care
The primary focus of the research we reviewed in the ambulatory care domain focuses on providing non-acute patient access to services, such as primary healthcare and radiology. Outpatient facilities and staff are most often a constrained resource and not accessible 24 hours a day. The focus is therefore to ensure there is a consistent flow of patients throughout ambulatory facilities where capacity is often constrained, especially in terms of healthcare workers. The aim is further not to add additional capacity in the form of healthcare worker overtime to address the demand for outpatient services.
There is an ambiguous use of the terms “waiting time”, “indirect waiting time”, “direct waiting time” and “access” to refer to the duration of time from when a patient requires an ambulatory service until the patient receives the service.
Although long patient queues are associated with ambulatory care services, queueing theory is not one of the tools used most frequently to solve the waiting time problem in ambulatory care. Instead, computer simulation and mathematical programming are the operational research methods that are used most frequently.
5.2. Emergency care services
5.2.1. Access time type articles
As we have discussed in Example 1 of Section 3, access time for a walk-in healthcare service such as the Emergency Department (ED) will only occur if a patient is denied access to enter the facility. Our results have shown that not much research has been done on a scenario where a patient is denied access for some reason to the Emergency Department. Only 4 articles are classified as access time type articles in Emergency Care Services (Almehdawe et al., Citation2013, Citation2016; Laan et al., Citation2016; Nezamoddini & Khasawneh, Citation2016).
Three articles (Almehdawe et al., Citation2013, Citation2016; Laan et al., Citation2016) investigate ambulance offload delays at an ED due to no bed being available in the ED. Although the patient is technically speaking under medical care, he or she does not have access to the right healthcare habitat (the ED). Almehdawe et al. (Citation2016) mention that the scenario where an ambulance has to wait to offload a patient due to bed availability in ED is known as waiting time in North America and access block in Australia. The authors also refer to this scenario as ambulance offload delay. Almehdawe et al. (Citation2013) also define waiting time of a walk-in patient as the time from when a patient arrives until he or she gets a bed (or medical care by implication).
The fourth access time type article in Emergency Care investigates the transfer of non-emergency patients to an alternative hospital if the ED that they walk-in to are under capacity pressure (Nezamoddini & Khasawneh, Citation2016).
5.2.2. Waiting time type articles
The majority of articles on Emergency Care are classified as waiting time type articles. Most research is done on improving the throughput of patients through the ED.
Niyirora et al. (Citation2017) describe waiting time in the ED as a delay in medical intervention where the cause of this delay is long queues. The research of Leo et al. (Citation2016) directly associates patient waiting time with ED workload. Yang et al. (Citation2016) argue that waiting time in the ED is often as a result of delays in ancillary services such as diagnostics.
According to example 4 in Section 3, the time from when a patient requests an ambulance until the ambulance arrives at the patient is waiting time. Many articles such as Lee (Citation2017), Jagtenberg et al. (Citation2017), and Rajagopalan and Saydam (Citation2009) focus on the logistics of ambulance placing and dispatching in order to reach the patient as soon as possible. Another aspect that researched in emergency care, is the decision-making of which hospital to route ambulances to Lee (Citation2014) and Leo et al. (Citation2016).
The term throughput is also associated with the flow of patients through the ED. Oh et al. (Citation2016) mention that throughput has an impact on both economic feasibility and patient satisfaction. Throughput differs from waiting time since it is the time from patient arrival until patient departure and therefore includes service time.
Uriarte et al. (Citation2017) mention three types of waiting time in ED. The first is waiting time to triage, the second waiting time to see a physician and the third the patient’s length of stay. Although Uriarte et al. (Citation2017) do not clearly indicate what the length of stay entails, it presumably is the entire time that a patient spends in the ED, which would include the time waiting for triage and for a physician. The third type of “waiting time” in this instance is therefore similar to throughput and not what we classify as waiting time.
provides a summary of all the Emergency Care services articles.
Table 6. Summary of Emergency Care services articles.
5.2.3. Aggregate overview: emergency care
It is evident that the only access time type articles in Emergency care services are the ones that are concerned with ambulance offload-delays for reasons such as upstream bed-blocking. Waiting time type articles in Emergency care can be divided into articles on delays that occur in the ED and the articles that focus on ambulance logistics such as where to place ambulances (Ramirez-Nafarrate et al., Citation2014). Due to the wide variety of ORMS research subjects that are covered in Emergency care services, our systemised literature review shows that it is the second most researched healthcare service in ORMS applied to healthcare (20% of the articles). We have found that delays in emergency care services are most often due to the unpredictable nature of patient arrivals which makes planning and control decisions, specifically related to resource allocation, challenging. Upstream bed blocking, waiting for laboratory test results (Salmon et al., Citation2018) and delays in ambulance offload are some of the other reasons for delays in emergency care.
5.3. Surgical care services
5.3.1. Access time type articles
4The 20 access type articles in Surgical Care services mainly refer to the time that patients who require surgery spend on a waiting list to be admitted to a healthcare facility. Most of the 20 access time type articles predominantly address operating room scheduling to improve patient access to surgery. An article that is often cited in explaining access time to surgery, is the work of Gupta and Denton (Citation2008). Similar to articles on Ambulatory Care Services, Gupta and Denton (Citation2008) refer to direct and indirect waiting time. Indirect waiting time is also referred to as virtual waiting time which is the time from when a patient requests and appointment (for surgery, for example) until the appointment occurs. Gul et al. (Citation2015) uses indirect waiting time in the same context.
A few authors use the term waiting time to denote the duration from when a patient requires surgery until surgery takes place. Aringhieri et al. (Citation2015) see waiting time as the time from referral to surgery. Other authors who refer to surgery waiting time in this way include Briggs et al. (Citation2011) and Creemers et al. (Citation2012). It is not clear from these definitions whether the waiting time includes the time between the start of hospitalisation and surgery. It is clear that the term “waiting time” in these articles are generally used to refer to access time as we have defined it.
A key term that often occur in access time type articles in Surgical Care is waiting list. A waiting list is defined by (Creemers et al., Citation2012) as a queue of patients who are waiting for their appointed date to receive treatment. This implies that the waiting time here includes the delay from admission to hospital until actual surgery.
5.3.2. Waiting time type articles
In Surgical Care services 10 articles are classified as waiting time type articles. The research environment includes elective and emergency surgery scheduling.
One definition that occurs in these articles is direct waiting time which is also called captive waiting time and is “ … the difference between a patient’s appointment time (or his/her arrival time if he/she is tardy) and the time when he/she is actually served by the service provider” (Gupta & Denton, Citation2008, p. 801).
Jung et al. (Citation2019) distinguish between emergency patients waiting for surgery and elective patients waiting for surgery as follows: “Arrival of emergency patients could lead to delay in elective surgeries” (p. 1408).
A summary of the results from literature on waiting and access times (as we have defined it) in Surgical Care services is shown in :
Table 7. Summary of Surgical Care services articles.
5.3.3. Aggregate overview: surgical care services
The access time type of articles categorised under surgical care services predominantly focus on reducing the waiting list of patients to have surgery scheduled. Such articles are therefore very similar to access time type articles in the ambulatory care services category. Definitions of access time in surgical care are similar to the access time definitions in ambulatory care services and access time buckets are denoted in calendar days.
We find that many articles on surgical care services focus on improving theatre utilisation. The improvement of waiting time for surgery, once a patient is in the healthcare habitat, is a secondary objective. On the contrary, the emphasis of articles related to emergency surgery scheduling is on ensuring that critical patients receive surgical care timeously whilst resource utilisation is often a secondary objective.
5.4. Inpatient care services
5.4.1. Access time type articles
There are 11 articles that can be categorised as access time type articles for Inpatient Care services. Hulshof et al. (Citation2013) present a care pathway that may involve an outpatient clinic visit followed by surgery at a later stage and a return visit to the outpatient clinic days or weeks after surgery. They argue that patients may experience varying access times between each stage of the care pathway. Access time in this research is defined as “ … the time a patient spends on the waiting list before being served” (Hulshof et al., Citation2013, p. 152). This access time definition does not distinguish between delays in the hospital environment and outside the hospital environment.
Vissers et al. (Citation2007) use the term waiting time in referral to patient access to Inpatient Care by mentioning that “ … patients nowadays do not accept long waiting times for hospital admission … ” They use waiting time to refer to access time for Inpatient Care as we have defined it.
An interesting concept, namely, “Access Time Target” (ATT) is illustrated in the research by Zhou et al. (Citation2018) who define ATT as “the tolerance threshold on waiting time based on both the patients’ payment and clinical acceptable time” (p. 221). The term “waiting time” is what we refer to as access time and the payment in this instance refers to patients with private healthcare insurance. There is therefore an extra dimension to patients waiting for access to Inpatient Care.
The healthcare environment where the research is done is mainly the inpatient areas of a hospital such as wards and ICU but there is also an article (Helm et al., Citation2011) that investigates the phenomenon of patients who use the emergency department as a gateway to gain access to inpatient care instead of waiting on a waiting list.
5.4.2. Waiting time type articles
There are 13 waiting time type articles in Inpatient Care services. Geng et al. (Citation2013) use the term waiting time and access time interchangeably to denote the time from when a call is made for an MRI appointment for an inpatient until the patient’s MRI time slot.
The term blocking is mentioned in 3 of the Inpatient Care waiting time type articles (Bai et al., Citation2018; Bretthauer et al., Citation2011; Yang et al., Citation2015). Bretthauer et al. (Citation2011) define blocking as “ … the inability to move patients who have completed service at a given stage to the subsequent stage because of lack of capacity at that stage” (p. 375). Blocking is therefore a term that can be used for inpatient waiting time when there is a lack of capacity to service the patient. According to Bai et al. (Citation2018) “Blocking in ICU may lead to increased waiting times in upstream units such as operating rooms which leads to an overall reduction in patient throughput” (p. 3).
Yang et al. (Citation2015) argue that ICU often becomes the bottleneck in patient flow which results in the cancellation or postponement of surgeries. This will ultimately lead to patients waiting longer to receive surgery. Long et al. (Citation2018) define boarding time as “when patients wait to exit the ICU” (p. 2122). Shi et al. (Citation2016) expand on boarding time and contend that the admission from the Emergency Department (ED) to the inpatient ward is known as ED boarding time which results in overcrowding of ED departments if delays occur. They specifically define the waiting time of an ED-GW (Emergency Department to General Ward) patient as “ … duration between her bed request time and actual admission time” (Shi et al., Citation2016, p. 2). The articles by Yang et al. (Citation2015), Long et al. (2018) and Shi et al. (Citation2016) are waiting time type articles since it describes the delay in the same healthcare habitat.
Finally, Dellaert et al. (Citation2016) investigates the impact of hospital capacity planning and control on waiting time. They argue that there is a trade-off between hospital efficiency and patient waiting time which is a measure of patient satisfaction.
is a summary of the Inpatient Care services articles.
Table 8. Summary of Inpatient Care services articles.
5.4.3. Aggregate overview: inpatient care services
The general aim of articles categorised under inpatient care services is to improve flow of acute patients in a hospital setting. It is therefore not surprising that the most common technical method for inpatient care services type of articles are computer simulation. Although articles in ambulatory and emergency care services sometimes focus on patient length of stay, this is not the case for in an inpatient setting since patient length of stay is often influenced by clinical outcomes in this setting. Although we have found some articles on access times to inpatient services, there are very few articles that focus on the duration from patient referral at an outpatient facility to admission to hospital, which we define as access time.
The articles in this category do not provide many definitions of waiting and access time but reference is made to the term “blocking” in some articles to refer to waiting time between stages in the inpatient environment.
5.5. Home care and residential care services
Articles on Home Care and Residential Care services are grouped together for the purposes of this discussion.
5.5.1. Access time type articles
Our results contain 3 access time type articles each for Home Care services and 4 for Residential Care services.
The results show no specific definitions for access time in terms of Home Care services although Zhang et al. (Citation2012) use the term waiting time to refer to the time it takes for resources to be allocated to a patient at his/her home and for Home Care services to start on a long-term basis. According to our definitions, this would be classified as access time.
Some authors mention other terms related to access time for Home Care services. Mohammadi Bidhandi et al. (Citation2019) note that blocking occurs when there is inefficient planning for Home Care services in a community. Rodriguez et al. (Citation2015) argue that patients do not get timely access to Home Care services if staff planning is not done efficiently at tactical level.
An access time definition for Residential Care services is found in an article by Patrick et al. (Citation2015) who use the term waiting time to refer to the duration from when a patient in the community requests to be placed in a long-term care facility until the patient can be accommodated. Konrad et al. (Citation2017) clearly state that improved access to a patient centred medical home can be obtained by achieving a higher throughput rate of patients through the facility.
5.5.2. Waiting time type articles
There is 1 waiting time type article for Home Care services and 3 for Residential Care services.
The waiting time type article for Home Care services by Bard et al. (Citation2014) does not provide a specific definition for waiting time but emphasise that it is important for patients to be seen by healthcare workers at home during their specified time window.
Some terms that are used for waiting time in Residential Care include earliness and tardiness (Lieder et al., Citation2015) where both terms indicate times of the day that are not preferable for patients in a long-term care facility to receive care. Van Eeden et al. (Citation2016) use the term “care on demand” (p. 228). They measure the time from when a patient presses the call button in a nursing home until the patient is assisted by a care worker. The term waiting time is not specifically used. Instead, the authors use the term “80/10 service level” (p. 230) which means that 80% of patients need to receive assistance within 10 minutes from pressing the call button. From our definition this would mean that waiting time needs to be 10 minutes or less for 80 percent of patients.
shows a summary of Home Care and Residential Care articles.
Table 9. Summary of Home Care and Residential Care services articles.
5.5.3. Aggregate overview: inpatient care services
The context of waiting and access time is quite different in home and residential care than it is in ambulatory, emergency, surgical and inpatient care. The reason for this is that patients are permanently in the health habitat of home care and/or residential care. This does not, however, imply that delays in home and residential care are not important. In fact, providing patients with timeous care at their permanent place of residence alleviates the pressure on and potentially decreases the utilisation of ambulatory, emergency, surgical and inpatient care services. The ultimate result of this is shorter delays for other patients in the healthcare habitat who do not necessarily require home and residential care. Since most of the waiting and access time literature we found focus on resource allocation in home and residential care, there is a significant opportunity for OR/OM research on access and waiting time in residential and home care services. Aspects such as behavioural OR and how patients’ experience and behaviour are affected (and subsequently modelled) whilst waiting for service in their permanent environment are examples of potential OR/OM research areas.
5.6. Other articles
Two articles in our results are not classified according to any healthcare service (Brailsford & Vissers, Citation2011; Kujala et al., Citation2006). The article by Kujala et al. (Citation2006) is classified as a waiting time type article since it addresses a patient’s journey through healthcare services as a production process with the main focus on waiting time in the healthcare habitat. They divide a patient’s journey into three major parts, namely, diagnostic and care time, administration time and lastly waiting time. They use the term waiting time to refer to all the time a patient waits for a medical procedure that is recommended as an official care process. It is not clear whether this waiting time includes the time a patient waits for a procedure in the healthcare habitat that is not part of the official care process recommendation. Kujala et al. (Citation2006) further divide waiting time into positive, passive, and negative waiting time. Positive waiting time denotes the time during which a patient’s condition is likely to improve, passive waiting time is the time when a patient is stable and negative waiting time is waiting time that is not desirable for a positive clinical outcome.
The second article that is not classified according to a specific healthcare service is a literature review by Brailsford and Vissers (Citation2011). As discussed in Section 4, the review is an analysis of papers presented at ORAHS over 35 years (from 1975 to 2009). This analysis shows that any delay is synonymous with poor quality of service from a patient perspective. The paper refers to this delay as waiting time, but the delay can in fact be any delay inside or outside the healthcare habitat. The delay (or waiting time as they describe it) is seen as a criterion for measuring healthcare performance. Access time in Brailsford and Vissers (Citation2011) is described as the waiting list for care. This access time definition is, however, part of waiting time as they describe it.
6. Conclusion
The contribution of this paper is twofold. First, we provide clear definitions with illustrative examples of access and waiting times in healthcare. Second, we provide an overview on how waiting time in healthcare is perceived and described in ORMS healthcare literature by means of a systematic search.
We found that there are many terms that are used to describe the delay of delivering healthcare services. There is, however, no unambiguous definition in the ORMS literature for waiting time in healthcare. The need for a uniform definition is evident from the many authors who attempt to provide definitions for the delay of providing healthcare services to patients. Reference is often made to direct and indirect waiting times which is also called captive and virtual waiting times. Although these definitions are useful, it is not always clear when indirect waiting time stops, and direct waiting time starts.
By using our definitions of waiting time and access time in healthcare, we could classify the literature by means of three attributes. First, we classified articles as either solving the waiting time or access time problem. Second, we classified the articles according to the healthcare service that the research focuses on. Finally, we identified which OR/OM tools and techniques were used to solve the waiting time/access time problem in the research.
According to our analysis of the literature, more than half of the articles (52%) are research done on the access time problem. Most articles focus on research in Ambulatory Care (43%). The articles in Ambulatory Care services mostly focus on outpatient clinics or radiology services with the aim to provide prompt access to these services (in other words, reduce both access time and waiting time) while minimising staff idle time and clinic/facility overtime. The OR techniques that are used most often are Computer Simulation and Mathematical Programming where Mathematical Programming is often used to optimise patient waiting time, staff idle time and facility overtime. We observe that 54% of the articles appear in 6 of the 54 journals represented in the search results (Health Care Management Science, European Journal of Operational Research, Operations Research for Health Care, Productions and Operations Management, Flexible Services and Manufacturing Journal, and Operations Research). There is a significant gap in research on decreasing both the access time and waiting time of patients in Home Care and Residential Care.
A consistent point of view in the literature is that any delay in providing healthcare services to patients is perceived by patients as reduced quality of care whether this delay in service has an impact on their clinical outcome or not. The quality of healthcare can be improved by reducing both access and waiting time to healthcare services. We believe that our clear definitions of access time and waiting time provides an unambiguous starting point for research and comparison of delays in healthcare across healthcare services.
7. Future research directions
Our literature study has shown that waiting and access issues form the motivation for many healthcare OR/MS studies. We do not expect this to change in the coming decades, however the focus may shift as a result of various developments that are reshaping the healthcare landscape. In the remainder of this section, we discuss some of these developments and their foreseen impact. We note that these developments are necessitated by the increased pressure on the healthcare system due to the ageing societies and are spurred on by technological and medical advances.
The first development is the shift from hospital care towards primary care and community. This reform ensures a more coordinated, less fragmented, less costly, and more prevention (rather than intervention) focused health management. Examples are low complexity interventions or medicine administrations for chronically ill. This development is supported and spurred on by ICT innovations like technologies for sensing, remote/tele monitoring, e-coaching for health, etc. Remote consultation technologies have been around for quite long time but really have taken off as a result of the COVID-19 crisis. This is likely to remain after the crisis and will reduce the number of hospital visits. This will have major impact on healthcare capacity planning and scheduling. Accordingly, delays in healthcare would take on a different form than before. More virtual than physical delays to access the healthcare habitat will occur and subsequently we envisage a larger focus in future research on access time than waiting time.
Example 5 in Section 3 articulates access time in a virtual setting according to our definition.
The second development is the increasingly better informed and articulated patient. Patients will become even more demanding as a result of increasingly accessible information regarding performance of healthcare providers (both quality and efficiency-wise), alternative medicines and treatments, etc. We also expect that self-diagnosis and self-referrals will increase as a result of wearable sensing technologies. These trends will impact the patient’s perception of waiting/access time. Primary clinical indicators such as heart rate, body temperature and oxygen saturation levels can be measured by the patient using wearable devices. The patient’s perception is therefore that the first step in a primary care pathway can be completed by patients themselves. This is likely to raise the expectation of the patient to have quicker access to the healthcare habitat and clinical decision-making since they collect information related to their condition themselves prior to a medical consultation (Min and Jake, Citationn.d.)
Another development is that of the quality and efficiency driven concentration of care. As a result, we observe the emergence of diagnostic centres, specialised intervention centres, after-care centres, etc. This necessitates more collaboration between healthcare providers to ensure seamless transfer of patients within their care pathways. There needs to be more focus on integrated care pathway planning to optimise care pathway lead-time and to minimise blocking. Since such transfers used to take place within hospitals, the waiting times is now classified as access times.
Finally, we point out the emerging field of behavioural operational research applied to healthcare. Behavioural operational research (BOR) examines the human behaviours and emotions in operational research modelling, problem solving and complex decision-making processes (Hämäläinen et al., Citation2013). Furthermore, BOR investigates the outcomes of OR models in the form of behaviour in models, behaviour with models and behaviour beyond models. It has been shown that perceived waiting time has a significant effect on customer satisfaction and behaviour (Kim et al., Citation2020), which has to be accounted for in OR/MS models (Kunc et al., Citation2020). Furthermore, machine learning techniques can be used in combination with OR models (such as simulation) to understand and influence patients’ behaviour to under-, correctly and overestimate waiting times (Gartner & Padman, Citation2020). Future research on the use of OR/OM models that consider patient behaviour in terms of perceived waiting and access times will encourage the use of OR/OM models for planning and control decision-making within healthcare organisations. Research by Fux-Noy et al. (Citation2019) found that providing a multisensory waiting environment reduce patients’ anxiety level and perception of waiting. Research into the psychology of waiting will give insights into what aspects affect the patient’s perception of waiting (Kim et al., Citation2020). This knowledge can be used in the context of behavioural OR in healthcare.
In order to achieve the above future directions of research, a clear understanding and common language of patient waiting and access times in different healthcare services have to be in place. Our definitions serve this purpose and provide an unequivocal starting point for research on delays in healthcare.
Availability of data and material
All review articles and classification information are available in a Mendeley data repository
Supplemental Material
Download Zip (102.7 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
Related Research Data
References
- Almehdawe, E., Jewkes, B., & He, Q.-M. (2013). A Markovian queueing model for ambulance offload delays. European Journal of Operational Research, 226(3), 602–614. https://doi.org/10.1016/j.ejor.2012.11.030
- Almehdawe, E., Jewkes, B., & He, Q.-M. (2016). Analysis and optimization of an ambulance offload delay and allocation problem. Omega (United Kingdom), 65, 148–158. https://doi.org/10.1016/j.omega.2016.01.006
- Anderson, K., Zheng, B., Yoon, S. W., & Khasawneh, M. T. (2015). An analysis of overlapping appointment scheduling model in an outpatient clinic. Operations Research for Health Care, 4, 5–14. https://doi.org/10.1016/j.orhc.2014.12.001
- Aringhieri, R., Landa, P., Soriano, P., Tànfani, E., & Testi, A. (2015). A two level metaheuristic for the operating room scheduling and assignment problem. Computers and Operations Research, 54, 21–34. https://doi.org/10.1016/j.cor.2014.08.014
- Bai, J., Fügener, A., Schoenfelder, J., & Brunner, J. O. (2018). Operations research in intensive care unit management: A literature review. Health Care Management Science, 21(1), 1–24. https://doi.org/10.1007/s10729-016-9375-1
- Bard, J. F., Shao, Y., & Jarrah, A. I. (2014). A sequential GRASP for the therapist routing and scheduling problem. Journal of Scheduling, 17(2), 109–133. https://doi.org/10.1007/s10951-013-0345-x
- Bikker, I. A., Kortbeek, N., van Os, R. M., & Boucherie, R. J. (2015). Reducing access times for radiation treatment by aligning the doctor’s schemes. Operations Research for Health Care, 7, 111–121. https://doi.org/10.1016/j.orhc.2015.06.005
- Brailsford, S., & Vissers, J. (2011). OR in healthcare: A European perspective. European Journal of Operational Research, 212(2), 223–234. https://doi.org/10.1016/j.ejor.2010.10.026
- Bretthauer, K. M., Heese, H. S., Pun, H., & Coe, E. (2011). Blocking in healthcare operations: A new heuristic and an application. Production and Operations Management, 20(3), 375–391. https://doi.org/10.1111/j.1937-5956.2011.01230.x
- Briggs, R. J., Smith, K. M., Dejager, E. M., Callahan, J. T., Abernethy, J. A., Dunn, E. J., & Hunter-Smith, D. J. (2011). The active management of surgical waiting lists: A urological surgery case study. Australian Health Review, 35(4), 399–403. https://doi.org/10.1071/AH10923
- Castro, E., & Petrovic, S. (2012). Combined mathematical programming and heuristics for a radiotherapy pre-treatment scheduling problem. Journal of Scheduling, 15(3), 333–346. https://doi.org/10.1007/s10951-011-0239-8
- Chen, R. R., & Robinson, L. W. (2014). Sequencing and scheduling appointments with potential call-in patients. Production and Operations Management, 23(9), 1522–1538. https://doi.org/10.1111/poms.12168
- Conforti, D., Guerriero, F., Guido, R., & Veltri, M. (2011). An optimal decision-making approach for the management of radiotherapy patients. OR Spectrum, 33(1), 123–148. https://doi.org/10.1007/s00291-009-0170-y
- Conforti, D., Guerriero, F., & Guido, R. (2010). Non-block scheduling with priority for radiotherapy treatments. European Journal of Operational Research, 201(1), 289–296. https://doi.org/10.1016/j.ejor.2009.02.016
- Creemers, S., Beliën, J., & Lambrecht, M. (2012). The optimal allocation of server time slots over different classes of patients. European Journal of Operational Research, 219(3), 508–521. https://doi.org/10.1016/j.ejor.2011.10.045
- Crop, F., Lacornerie, T., Mirabel, X., & Lartigau, E. (2015). Workflow optimization for robotic stereotactic radiotherapy treatments: Application of constant work in progress workflow. Operations Research for Health Care, 6, 18–22. https://doi.org/10.1016/j.orhc.2015.05.002
- De Vuyst, S., Bruneel, H., & Fiems, D. (2014). Computationally efficient evaluation of appointment schedules in health care. European Journal of Operational Research, 237(3), 1142–1154. https://doi.org/10.1016/j.ejor.2014.02.058
- Deglise-Hawkinson, J., Helm, J. E., Huschka, T., Kaufman, D. L., & Van Oyen, M. P. (2018). A capacity allocation planning model for integrated care and access management. Production and Operations Management, 27(12), 2270–2290. https://doi.org/10.1111/poms.12941
- Dellaert, N., Cayiroglu, E., & Jeunet, J. (2016). Assessing and controlling the impact of hospital capacity planning on the waiting time. International Journal of Production Research, 54(8), 2203–2214. https://doi.org/10.1080/00207543.2015.1051668
- Dogru, A. K., & Melouk, S. H. (2019). Adaptive appointment scheduling for patient-centered medical homes. Omega (United Kingdom), 85, 166–181. https://doi.org/10.1016/j.omega.2018.06.009
- Fux-Noy, A., Zohar, M., Herzog, K., Shmueli, A., Halperson, E., Moskovitz, M., & Ram, D. (2019). The effect of the waiting room’s environment on level of anxiety experienced by children prior to dental treatment: A case control study. BMC Oral Health, 19(1). https://doi.org/10.1186/s12903-019-0995-y
- Gartner, D., & Padman, R. (2020). Machine learning for healthcare behavioural OR: Addressing waiting time perceptions in emergency care. Journal of the Operational Research Society, 71(7), 1087–1101. https://doi.org/10.1080/01605682.2019.1571005
- Geng, N., Chen, L., Liu, R., & Zhu, Y. (2017). Optimal patient assignment for W queueing network in a diagnostic facility setting. International Journal of Production Research, 55(19), 5609–5631. https://doi.org/10.1080/00207543.2017.1324650
- Geng, N., Xie, X., & Jiang, Z. (2013). Implementation strategies of a contract-based MRI examination reservation process for stroke patients. European Journal of Operational Research, 231(2), 371–380. https://doi.org/10.1016/j.ejor.2013.05.043
- Grant, M. J., & Booth, A. (2009). A typology of reviews: An analysis of 14 review types and associated methodologies. Health Information and Libraries Journal, 26(2), 91–108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
- Gul, S., Denton, B. T., & Fowler, J. W. (2015). A progressive hedging approach for surgery planning under uncertainty. INFORMS Journal on Computing, 27(4), 755–772. https://doi.org/10.1287/ijoc.2015.0658
- Gupta, D., & Denton, B. (2008). Appointment scheduling in health care: Challenges and opportunities. IIE Transactions (Institute of Industrial Engineers), 40(9), 800–819. https://doi.org/10.1080/07408170802165880
- Hämäläinen, R. P., Luoma, J., and Saarinen, E. (2013): On the importance of behavioral
- Hans, E. W., Van Houdenhoven, M., & Hulshof, P. J. H. (2012). . In International series in operations research and management science, 168, 303–320. https://doi.org/10.1007/978-1-4614-1734-7_12.
- Harding, K. E., Taylor, N. F., & Leggat, S. G. (2011). Do triage systems in healthcare improve patient flow? A systematic review of the literature. Australian Health Review, 35(3), 371–383. Retrieved from https://doi.org/10.1071/AH10927
- Helm, J. E., Ahmadbeygi, S., & Van Oyen, M. P. (2011). Design and analysis of hospital admission control for operational effectiveness. Production and Operations Management, 20(3), 359–374. https://doi.org/10.1111/j.1937-5956.2011.01231.x
- Hong, T. S., Shang, P. P., Arumugam, M., & Yusuff, R. M. (2013). Use of simulation to solve outpatient clinic problems: A review of the literature. South African Journal of Industrial Engineering, 24(3), 27–42. https://doi.org/10.7166/24-3-551
- Huang, Y., & Zuniga, P. (2012). Dynamic overbooking scheduling system to improve patient access. Journal of the Operational Research Society, 63(6), 810–820. https://doi.org/10.1057/jors.2011.83
- Hulshof, P. J. H., Boucherie, R. J., Hans, E. W., & Hurink, J. L. (2013). Tactical resource allocation and elective patient admission planning in care processes. Health Care Management Science, 16(2), 152–166. https://doi.org/10.1007/s10729-012-9219-6
- Hulshof, P. J. H., Kortbeek, N., Boucherie, R. J., Hans, E. W., & Bakker, P. J. M. (2012). Taxonomic classification of planning decisions in health care: A structured review of the state of the art in OR/MS. Health Systems, 1(2), 129–175. https://doi.org/10.1057/hs.2012.18
- Jagtenberg, C. J., Bhulai, S., & van der Mei, R. D. (2017). Dynamic ambulance dispatching: Is the closest-idle policy always optimal? Health Care Management Science, 20(4), 517–531. https://doi.org/10.1007/s10729-016-9368-0
- Jiang, H., Pang, Z., & Savin, S. (2012). Performance-based contracts for outpatient medical services. Manufacturing and Service Operations Management, 14(4), 654–669. https://doi.org/10.1287/msom.1120.0402
- Jung, K. S., Pinedo, M., Sriskandarajah, C., & Tiwari, V. (2019). Scheduling elective surgeries with emergency patients at shared operating rooms. Production and Operations Management, 28(6), 1407–1430. https://doi.org/10.1111/poms.12993
- Kim, M. H., Park, J.-W., & Choi, Y.-J. (2020). A study on the effects of waiting time for airport security screening service on passengers’ emotional responses and airport image. Sustainability (Switzerland), 12(24), 1–16. https://doi.org/10.3390/su122410634
- Kong, Q., Lee, C.-Y., Teo, C.-P., & Zheng, Z. (2013). Scheduling arrivals to a stochastic service delivery system using copositive cones. Operations Research, 61(3), 711–726. https://doi.org/10.1287/opre.2013.1158
- Konrad, R., Ficarra, S., Danko, C., Wallace, R., & Archambeault, C. (2017). A decision-support approach for provider scheduling in a patient-centered medical home. Journal of Healthcare Management, 62(1), 46–59. https://doi.org/10.1097/00115514-201701000-00009
- Kujala, J., Lillrank, P., Kronström, V., & Peltokorpi, A. (2006). Time-based management of patient processes. Journal of Health, Organisation and Management, 20(6), 512–524. https://doi.org/10.1108/14777260610702262
- Kunc, M., Harper, P., & Katsikopoulos, K. (2020). A review of implementation of behavioural aspects in the application of OR in healthcare. Journal of the Operational Research Society, 71(7), 1055–1072. https://doi.org/10.1080/01605682.2018.1489355
- Laan, C. M., Vanberkel, P. T., Boucherie, R. J., & Carter, A. J. E. (2016). Offload zone patient selection criteria to reduce ambulance offload delay. Operations Research for Health Care, 11, 13–19. https://doi.org/10.1016/j.orhc.2016.09.001
- Lee, S. (2014). The role of hospital selection in ambulance logistics. IIE Transactions on Healthcare Systems Engineering, 4(2), 105–117. https://doi.org/10.1080/19488300.2014.914608
- Lee, S. (2017). A new preparedness policy for EMS logistics. Health Care Management Science, 20(1), 105–114. https://doi.org/10.1007/s10729-015-9340-4
- Leeftink, A. G., Vliegen, I. M. H., & Hans, E. W. (2019). Stochastic integer programming for multi-disciplinary outpatient clinic planning. Health Care Management Science, 22(1), 53–67. https://doi.org/10.1007/s10729-017-9422-6
- Leo, G., Lodi, A., Tubertini, P., & Di Martino, M. (2016). Emergency department management in Lazio, Italy. Omega (United Kingdom), 58, 128–138. https://doi.org/10.1016/j.omega.2015.05.007
- Lieder, A., Moeke, D., Koole, G., & Stolletz, R. (2015). Task scheduling in long-term care facilities: A client-centered approach. Operations Research for Health Care, 6, 11–17. 10.1016/j.orhc.2015.06.001
- Long, E. F., & Mathews, K. S. (2018). The Boarding Patient: Effects of ICU and Hospital Occupancy Surges on Patient Flow. Production and Operations Management, 27(12), 2122–2143. https://doi.org/10.1111/poms.12808
- Ma, X., Sauré, A., Puterman, M. L., Taylor, M., & Tyldesley, S. (2016). Capacity planning and appointment scheduling for new patient oncology consults. Health Care Management Science, 19(4), 347–361. https://doi.org/10.1007/s10729-015-9331-5
- Min, W., & Jake, L. (n.d.). Wearable Technology Applications in Healthcare: A Literature Review | HIMSS. Online Journal of Nursing Informatics Contributors. Retrieved May 17, 2021, from https://www.himss.org/resources/wearable-technology-applications-healthcare-literature-review
- Mohammadi Bidhandi, H., Patrick, J., Noghani, P., & Varshoei, P. (2019). Capacity planning for a network of community health services. European Journal of Operational Research, 275(1), 266–279. https://doi.org/10.1016/j.ejor.2018.11.008
- Montecinos, J., Ouhimmou, M., & Chauhan, S. (2018). Waiting-time estimation in walk-in clinics. International Transactions in Operational Research, 25(1), 51–74. https://doi.org/10.1111/itor.12353
- Morikawa, K., & Takahashi, K. (2017). Scheduling appointments for walk-ins. International Journal of Production Economics, 190, 60–66. https://doi.org/10.1016/j.ijpe.2016.10.010
- Nezamoddini, N., & Khasawneh, M. T. (2016). Modeling and optimization of resources in multi-emergency department settings with patient transfer. Operations Research for Health Care, 10, 23–34. https://doi.org/10.1016/j.orhc.2016.06.001
- Niyirora, J., & Zhuang, J. (2017). Fluid approximations and control of queues in emergency departments. European Journal of Operational Research, 261(3), 1110–1124. https://doi.org/10.1016/j.ejor.2017.03.013
- Oh, C., Novotny, A. M., Carter, P. L., Ready, R. K., Campbell, D. D., & Leckie, M. C. (2016). Use of a simulation-based decision support tool to improve emergency department throughput. Operations Research for Health Care, 9, 29–39. https://doi.org/10.1016/j.orhc.2016.03.002
- Palmer, R., Fulop, N. J., & Utley, M. (2018). A systematic literature review of operational research methods for modelling patient flow and outcomes within community healthcare and other settings. Health Systems, 7(1), 29–50. https://doi.org/10.1057/s41306-017-0024-9
- Patrick, J., Nelson, K., & Lane, D. (2015). A simulation model for capacity planning in community care. Journal of Simulation, 9(2), 111–120. https://doi.org/10.1057/jos.2014.23
- Patrick, J. (2012). A Markov decision model for determining optimal outpatient scheduling. Health Care Management Science, 15(2), 91–102. https://doi.org/10.1007/s10729-011-9185-4
- Rajagopalan, H. K., & Saydam, C. (2009). A minimum expected response model: Formulation, heuristic solution, and application. Socio-Economic Planning Sciences, 43(4), 253–262. https://doi.org/10.1016/j.seps.2008.12.003
- Ramirez-Nafarrate, A., Baykal Hafizoglu, A., Gel, E. S., & Fowler, J. W. (2014). Optimal control policies for ambulance diversion. European Journal of Operational Research, 236(1), 298–312. https://doi.org/10.1016/j.ejor.2013.11.018
- Robinson, L. W., & Chen, R. R. (2010). A comparison of traditional and open-access policies for appointment scheduling. Manufacturing and Service Operations Management, 12(2), 330–346. https://doi.org/10.1287/msom.1090.0270
- Rodriguez, C., Garaix, T., Xie, X., & Augusto, V. (2015). Staff dimensioning in homecare services with uncertain demands. International Journal of Production Research, 53(24), 7396–7410. https://doi.org/10.1080/00207543.2015.1081427
- Salmon, A., Rachuba, S., Briscoe, S., & Pitt, M. (2018). A structured literature review of simulation modelling applied to emergency departments: Current patterns and emerging trends. Operations Research for Health Care, 19, 1–13. https://doi.org/10.1016/j.orhc.2018.01.001
- Samorani, M., & Laganga, L. R. (2015). Outpatient appointment scheduling given individual day-dependent no-show predictions. European Journal of Operational Research, 240(1), 245–257. https://doi.org/10.1016/j.ejor.2014.06.034
- Sauré, A., Begen, M. A., & Patrick, J. (2020). Dynamic multi-priority, multi-class patient scheduling with stochastic service times. European Journal of Operational Research, 280(1), 254–265. https://doi.org/10.1016/j.ejor.2019.06.040
- Saure, A., Patrick, J., & Puterman, M. L. (2015). Simulation-based approximate policy iteration with generalized logistic functions. INFORMS Journal on Computing, 27(3), 579–595. https://doi.org/10.1287/ijoc.2015.0645
- Sauré, A., Patrick, J., Tyldesley, S., & Puterman, M. L. (2012). Dynamic multi-appointment patient scheduling for radiation therapy. European Journal of Operational Research, 223(2), 573–584. https://doi.org/10.1016/j.ejor.2012.06.046
- Schacht, M. (2018). Improving same-day access in primary care: Optimal reconfiguration of appointment system setups. Operations Research for Health Care, 18, 119–134. https://doi.org/10.1016/j.orhc.2017.09.003
- Shi, P., Chou, M. C., Dai, J. G., Ding, D., & Sim, J. (2016). Models and insights for hospital inpatient operations: Time-dependent ED boarding time. Management Science, 62(1), 1–28. https://doi.org/10.1287/mnsc.2014.2112
- Uriarte, A., Ruiz Zúñiga, E., Urenda Moris, M., & Ng, A. H. C. (2017). How can decision makers be supported in the improvement of an emergency department? A simulation, optimization and data mining approach. Operations Research for Health Care, 15, 102–122. https://doi.org/10.1016/j.orhc.2017.10.003
- Van Eeden, K., Moeke, D., & Bekker, R. (2016). Care on demand in nursing homes: a queueing theoretic approach. Health Care Management Science, 19(3), 227–240. https://doi.org/10.1007/s10729-014-9314-y
- Van Sambeek, J. R. C., Joustra, P. E., Das, S. F., Bakker, P. J., & Maas, M. (2011). Reducing MRI access times by tackling the appointment-scheduling strategy. BMJ Quality and Safety, 20(12), 1075–1080. https://doi.org/10.1136/bmjqs.2010.049643
- Vieira, B., Demirtas, D., van de Kamer, J. B., Hans, E. W., & van Harten, W. (2018). A mathematical programming model for optimizing the staff allocation in radiotherapy under uncertain demand. European Journal of Operational Research, 270(2), 709–722. https://doi.org/10.1016/j.ejor.2018.03.040
- Vissers, J. M. H., Adan, I. J. B. F., & Dellaert, N. P. (2007). Developing a platform for comparison of hospital admission systems: An illustration. European Journal of Operational Research, 180(3), 1290–1301. https://doi.org/10.1016/j.ejor.2006.04.034
- White, D. L., Froehle, C. M., & Klassen, K. J. (2011). The effect of integrated scheduling and capacity policies on clinical efficiency. Production and Operations Management, 20(3), 442–455. https://doi.org/10.1111/j.1937-5956.2011.01220.x
- Wiesche, L., Schacht, M., & Werners, B. (2017). Strategies for interday appointment scheduling in primary care. Health Care Management Science, 20(3), 403–418. https://doi.org/10.1007/s10729-016-9361-7
- Wu, X., Li, J., & Khasawneh, M. T. (2019). Rule-based task assignment and scheduling of medical examinations for heterogeneous MRI machines. Journal of Simulation,14 (3) https://doi.org/10.1080/17477778.2019.1623988
- Yang, K. K., Lam, S. S. W., Low, J. M. W., & Ong, M. E. H. (2016). Managing emergency department crowding through improved triaging and resource allocation. Operations Research for Health Care, 10, 13–22. https://doi.org/10.1016/j.orhc.2016.05.001
- Yang, M., Fry, M. J., & Scurlock, C. (2015). The ICU will see you now: Efficient-equitable admission control policies for a surgical ICU with batch arrivals. IIE Transactions (Institute of Industrial Engineers), 47(6), 586–599. https://doi.org/10.1080/0740817X.2014.955151
- Zhang, Y., Puterman, M. L., Nelson, M., & Atkins, D. (2012). A simulation optimization approach to long-term care capacity planning. Operations Research, 60(2), 249–261. https://doi.org/10.1287/opre.1110.1026
- Zhou, L., Geng, N., Jiang, Z., & Wang, X. (2017). Combining revenue and equity in capacity allocation of imaging facilities. European Journal of Operational Research, 256(2), 619–628. https://doi.org/10.1016/j.ejor.2016.06.046
- Zhou, L., Geng, N., Jiang, Z., & Wang, X. (2018). Multi-objective capacity allocation of hospital wards combining revenue and equity. Omega (United Kingdom), 81, 220–233. https://doi.org/10.1016/j.omega.2017.11.005