
ABSTRACT
The growing demand for better quality of care, together with an increasing awareness of limited resources, is bringing attention to the need for design in healthcare. In mental health, considered the largest single cause of disability in the UK, the need is great. Existing services often fail to meet current levels of demand and do not consistently deliver good quality care for all service users. The design of better delivery systems has the potential to improve service user experience and care outcomes. This paper reports how through the interactive and participatory method of storytelling, the key components of a mental health delivery system were identified. We explain each of the ten components and discuss their implications for system understanding and service design. A model of a mental health delivery system has also been proposed.
1. Introduction
“ … of all the things that we try to measure in mental health services research, the most difficult and dangerous is describing the services”.
Mental health is gaining increasing and renewed attention globally (Vigo, Citation2021). It was estimated in 2009 that mental disorders affected 1 in 4 people around the world (WHO, Citation2009). The situation has been made worse by the COVID-19 pandemic over the past few years (WHO, Citation2022) and connections being made between issues such as climate change and mental health (The Lancet Regional Health – Europe, Citation2022). In most parts of the world, there are insufficient numbers of skilled policymakers, managers and clinicians, leading to delivery systems with inaccessible care and unacceptable quality of care (Minas & Cohen, Citation2007; WHO, Citation2021b). With mental health projected to be an increasing proportion of disability (WHO, Citation2021a), nations have been urged to support research aimed at filling the gaps in knowledge about mental health (WHO, Citation2021a). One area of knowledge gap in global mental health research which has been argued for decades is mental health systems research (Minas & Cohen, Citation2007). A focus on mental health systems opens a vast area for research. Minas and Cohen, for example, considered mental health systems to include policies, plans and programs; legislation, regulation, governance, organisation, and practice; financing and payment arrangements; information systems, monitoring and evaluation; health promotions and illness prevention, and arrangements that promote social participation (Minas & Cohen, Citation2007). In addition, Vigo has argued that shortage of skilled professionals and rising cost of mental health care delivery (especially since the COVID-19 pandemic) have been the “hill where most policy battles ended”, both in low and high income countries (Vigo, Citation2021). Vigo maintains that emerging innovations in task-shifting and “infinitely scalable” digital tools will play a major role in the dawn of a new era for mental health systems.
A number of important questions have received little attention in the mental health systems literature. These are: “how should we understand a mental health system in a way that supports improvements in care delivery?”, “what are the key components of a mental health delivery service from a systems perspective?” and “how do these components interact to impact on the experience of the service user?” These questions are inspired by the authors’ experience in the modelling and simulation of healthcare delivery systems together with their engineering background. In order to design better systems, it is essential to develop a better understanding of what the system is (Elliott & Deasley, Citation2007).
The aim of the research reported in this paper was to identify the key components of such a system and the potential value of understanding the relationships between them as part of the process to better understand mental health delivery systems. Within the time and resource constraints of the research, we focused on the perspectives of two system stakeholders – service users and staff (clinical staff and managers). We used the stories of these stakeholders as a window into the mental health delivery system.
2. Methods
2.1. Setting
This study was conducted prior to the COVID-19 global pandemic. It took place in a local mental health NHS Trust in the East of England. The Trust operates as a health and social care organisation with clinical teams providing a wide range of services in inpatient and community settings. The Trust supports a population of almost one million people and employs nearly 4,500 staff. The current study focused only on adult mental health services and was open to anyone between the ages of 16 and 65 who had accessed the services and all active clinical and management staff. All participants had capacity to consent. All focus group sessions took place in a facility owned by the NHS Trust. For all staff interviews, a researcher went to meet with staff in their workplaces. All sessions were between consented participants and researchers. Service users were allowed to bring a non-participant with them if that made them comfortable, but no one needed to do so.
2.2. Patient and public involvement
For this work a Service User Advisory Group (SUAG) was set up. This included one member who was a named Patient and Public Involvement (PPI) Advisor on the research protocol for the ethics application. The SUAG involved six members with a range of mental health challenges. All members had accessed services within the NHS Trust where the study was conducted. There were two men and four women. The SUAG provided significant input into the successful ethics application. The PPI Advisor co-authored publications, co-presented with researcher at events and co-facilitated all focus group sessions involving service users.
The SUAG had significant input to the development of the research ethics application, commented on the participant information sheets and lay summary for the study. At each SUAG meeting, the researcher kept records of all contributions made by the members and ensured that all perspectives were considered. This was often fed back to the members showing how each recommendation was applied and where it was not feasible, an explanation was given.
2.3. Ethical approval
Research and Development (R&D) approval for this work was given by the mental health Trust and ethical approval was received from the Health Research Authority’s (HRA) Cambridgeshire and Hertfordshire Research Ethics Committee (16/EE/0042).
2.4. Conceptual framework – Stories as methodology
Experiences of mental illness can be difficult for service users to retell. In conducting this study, it was desired to use an approach to data gathering that minimises emotional burden for service users. Stories were identified as a method that is ubiquitous in all cultures and almost natural to humans (Puckett, Citation2016). In a systematic review of the use of stories in health policymaking, Fadlallah and colleagues found that, in most cases, stories may have positive influence when used as inspiration and empowerment tools (Fadlallah et al., Citation2019). Storytelling then becomes an interactive and participatory process of exploring a complex problem situation (Klein et al., Citation2007).
It must be clarified that the use of stories in this study was only to enable participants to provide descriptions of their experiences of using the mental health system, that were as complete as possible. It was not intended to determine whether the experiences were meaningful or not. Thus, the researchers hypothesised that a rich story about a service user’s experience of the delivery system could provide a unique window into the system. In the focus groups and interviews, the focus was on getting participants to tell stories of their experiences of using the system. All the service user focus groups were co-facilitated by the PPI Advisor who had experience accessing mental health support from the Trust. She started each session with her own story to create a safe space for the participants to share their stories. Most of the questions used in the focus groups and interviews were only intended to enhance the stories, often by stimulating recall (Sinnott et al., Citation2017).
2.5. Study design
This study used a qualitative exploratory design using focus group (Kitzinger, Citation1994, Citation1995; Nyumba et al., Citation2018) and semi-structured interview (Britten, Citation1995) methodologies. The design involved four stages – categorisation (identification of components), syntactics (identification of relationships between components), semantics (representation of components and their relationships) and pragmatics (the understanding of the representation). The current paper focuses on the full analysis of the categorisation stage. Each stage had a focus group for service users with about six participants. The focus groups lasted 2.5 hours each whilst the interviews lasted about an hour. Staff had a focus group for the first stage but due to the difficulty in getting staff together at the same time, the research protocol was amended to include face-to-face interviews only for staff. Service user participants were identified through a patient involvement coordinator for the NHS Trust and study posters placed at various clinics in the Trust. The poster had an email address and dedicated mobile number that service users could call or text. Staff participants were recruited through email that was sent to staff by the Clinical Lead for the study.
3. Data analysis
All focus groups and interviews were audio recorded and transcribed verbatim. All the transcriptions were imported into the ATLAS.ti qualitative analysis software package (ATLAS.ti, Citation2019). The analysis was thematic (Taylor et al., Citation2018) and started with the initial assumption of nine components of the mental health delivery system based on the experience of the researchers in the modelling and simulation of healthcare delivery systems. An earlier study by Karni and Kaner also identified similar components of a service system (Karni & Kaner, Citation2007). These initial components included – Patients, Conditions, Goals, Interventions, Processes, Resources, Data/information, Staff, and the External environment. These were used as an initial framework to start coding the data.
3.1. Service user stories
We conducted a thematic analysis on the data (Braun & Clarke, Citation2006), starting with the identification of appropriate quotations in the transcript. A quotation contained at least one example of a system component. In most cases a quotation was limited to a few sentences that sufficiently capture an aspect of a user’s experience. The method of analysing the data was qualitative with coding for exploratory purposes only and not necessarily in a rigorous thematic manner. The general plan for coding the data is as follows:
Identify “quotations” which represent a meaningful portion of a participant’s narrative.
Identify, within each “quotation”, every element of the care delivery system that occur and
Assign to the element a code according to what kind of system component it may be referring to.
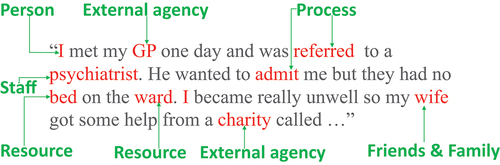
An example of a quotation and its associated codes are shown in below. The basic principle of this analysis is that the stories that service users tell of their experience of accessing care, together with the stories that staff tell of their experience providing care can give us a unique window into the care delivery system. This approach will also validate the original set of components that was based on the experience of the researchers in systems modelling and previous work by Karni & Kaner (Karni & Kaner, Citation2007) in the service industry.
Figure 1. Example of a quotation, identifiable system elements and related system components.
4. Results
4.1. Characteristics of participants
A total of ten service users (eight female and two male) and twelve staff participated in four service users focus groups, one staff focus group and seventeen staff interviews throughout the entire study.
The service users had experience of a wide range of mental health conditions including bipolar disorder, Post Traumatic Stress Disorder (PTSD), Borderline Personality Disorder (BPD), depression, self-harming behaviours, eating disorders, co-existing physical conditions like Multiple Sclerosis (MS) causing depression, and those without a clear diagnosis. All service user participants had been accessing the mental health services provided by the Trust for varying lengths of time up to a maximum of ten years. Service user participants also varied widely in the experience of the care they received, ranging from very positive to very negative, illustrated by the following quotes: “I think I’ve had one of the best psychiatrists in the world, literally, everybody knows her and when I first went to see her she said ‘You are unwell but I will get you better’, which is great because you think ‘I’m going to go back to normal’. I was seeing her for three years and she’s sort of leaving it to me now when to leave. Like I feel really well and I just want to go for a chat and a laugh and that’s not what it’s about, so I’ll say to her ‘I want to go now’, she’s just been really … I’m able to get an appointment if I ring up. … ‘Get in if you can’t cope’, and she’s just been there for everything really, my family, she’s a very well-known community psychiatrist here, so I’ve been lucky again. It’s luck.” (Service user participant)
“And that would be my concern because I think accessing mental health services in … , in my experience the service you get is based on luck and who answers the phone than it is on any sort of system. I don’t know if anybody else has had that experience, but certainly my experience of elderly care it’s very, very much driven by ‘Does this work, yes, does that work, yes, in all four chaps’ and it’s human beings we’re dealing with here”.
Staff participants had a variety of roles, including those working as Occupational Therapists (OTs), psychiatrists, and psychologists and those with managerial responsibilities. They were involved in different care pathways, such as Borderline Personality Disorders (BPD), Child and Adolescent Mental Health Services (CAMHS), Psychological services, adult mental health and liaison psychiatry which works at the interface of physical and mental health care delivery. There were also differing levels of seniority amongst the staff participants from trainee psychiatrist to director of services.
4.2. System components
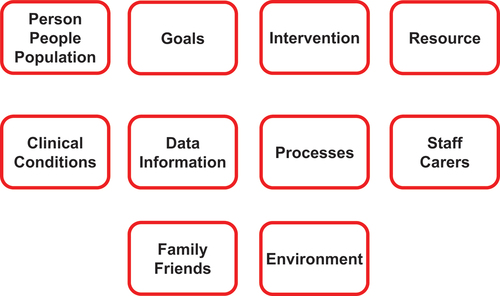
The analysis of participants’ stories appears to confirm the initial hypothesis of the researchers with the exception of one component (Family and Friends). The following is the full list of ten components – Person/People/Population, Goals, Intervention, Resources, Clinical Conditions, Data/Information, Processes, Staff/Carers, Family/Friends and Environment – as shown in . These are briefly described below with sample quotations from participants.
Figure 2. The ten key components of a mental health delivery system.
4.2.1. Person/People/Population
We define this component as the individual person, people, or population for whom the service of interest is developed. In total, the code for this component emerged in 83 quotations in the data either in isolation or together with other system components as discussed in the section on “co-occurrence between system components” below. This may seem an obvious component of a mental health delivery system, but the explicit identification enables a focus on understanding the variations within, and between groups in relation to how the service is set up to be delivered. For example, one staff member emphasised the importance of seeing people with the mental health condition for whom the service was developed – “So Personality Disorder Community Service. So we only work with people really who have a borderline personality disorder, that’s sort of what we’re set up for, so there’s lots of other types of personality disorder, antisocial, narcissistic, both of which we aren’t really set up to treat.” Staff 101. One service user suggested the importance of aligning not just how the service is delivered but also when it is delivered to the people for whom it is setup – “But then maybe they should be having the service after school times for school age people.” Service user. Another service user also emphasised how the thinking of the person may impact how they respond to the service – “One of the things that I do and I don’t know if other people do is I’ve heard lots of other … not in this group, but lots of other people with mental health problems do is you try to reject the person before they can reject you.” Service user.
All these examples highlight the importance of not just identifying service users but understanding, describing, and visualising the variations in and between them to inform a good understanding of the service delivery system.
4.2.2. Clinical conditions
This is the disease, illness or any physical or mental disorder for which a person, people or a defined population need the service system. Codes for conditions occurred 41 times in the data analysis. The identification of the clinical condition as an explicit component of the system is key to designing or redesigning a service that is fit for purpose. The identification of a clinical condition or a group of conditions determines a significant number of other system components including the processes, resources, staffing, information, and many external agencies. Some conditions also have implications for the interface with physical health as one service user experienced – “They say I have to go to BPD [Borderline Personality Disorder Service] and BPD say “No, because the underlying problem is because of your physical problems” Service user. In some cases, service users identify with a particular condition – “I’ve had a diagnosis of bipolar for about 10 years.” Service user.
The way the clinical conditions emerge in staff narratives also gives another perspective on the implications of this key component to service delivery – “… Like we’ve got the personality disorders pathway, it’s a very difficult pathway, extremely difficult, the requirements to get in and everything is hard, so we get more complaints about that and more serious incidents about that because the patients there are a different kind of patient.” Staff 102.
The implications for the service may differ depending on whether it is setup to treat a specific condition or manage a range of conditions – “Sure. So my name is 301. I’m a consultant psychiatrist in general adult psychiatry and I work full-time with the … Adult Locality Team. So the team treats working age adults, so that’s between 18 and 65, with moderate to severe mental health problems, so mainly psychosis, bipolar disorder, major depression and anxiety disorders.” Staff 301.
In mental health services, co-occurring conditions can make diagnosis challenging. Clarity on this component is key to receiving the right referrals from partner organisations.
4.2.3. Goals
“Goals” are the outcomes desired by a person with a condition or the results desired by the service in relation to the condition. “Goals” as a code occurred 23 times in the data but were also identified as a key system component because of their importance to the objective of the study. It is often the case in qualitative analysis where the frequency of occurrence of a theme does not constitute the only grounds for its importance, but also its meaning in context (Chenail, Citation2012). This component makes it important for the goals of key stakeholders to be externalised for mutual agreements to be reached. Some of such conflicting goals were identified in our data:
So we’re at the point where I’m trying to work with him to set a goal that involves getting out and about, getting involved more in the community and everything is met with a ‘No I can’t do that because … ’ or ‘No I don’t want to do that’, so the challenge there is about trying to find what his motivation actually is. Staff 101.
… I thought ‘Do you think I’m never going to work at my age and I’m going to live like this? I’m going back to work. I don’t care what I do’. So that sort of encouraged me that I wanted an endpoint to … Service user
4.2.4. Interventions
Interventions refer to drug treatments, physical activity, psychological therapies, or other forms of defined activities and support which a person needs to manage their condition(s) effectively. In all the focus groups and interview data, the code for this system component occurred 34 times. The recognition of “Interventions” as a system component resulted from several mentions of different interventions that the participants had experienced as service users or staff. These included interventions such as Cognitive Analytical Therapy, Cognitive Behavioural Therapy (CBT) Group therapy and psychotherapy as may be seen from the following sample quotations:
… and said that I had BPD symptoms or some BPD behaviours and that I really needed analytical therapy, might be cognitive analytical therapy, but unfortunately they had no access. She had no ability to send me for that so she put me on the waiting list for CBT, and it’s only through a friend who applied to St Columba Group Therapy Centre. Service user
… And patient themselves has to be an active participant in that, so you can’t really do psychotherapy to somebody, it has to be a mutual, collaborative endeavour. So they have to be somewhat motivated to explore these issues, understand these issues, make changes. Staff in focus group
4.2.5. Processes
Processes are the activities that are done in collaboration with the person who has a condition, to achieve the desired goals. During the focus groups and interviews the facilitators probed for process information by encouraging participants to describe activities that took place where and who was involved? What was needed? And, what happened next? Participants did not describe all processes in equal detail. Researchers had to identify certain activities which will inevitably involve several specific tasks to be completed. For example, “admission” is a process that will require several specific tasks to be completed. “Referrals” and “appointments” are other examples. Two example quotations from the data are provided here to illustrate how these emerged from participant stories.
she said ‘Well I think you really need to have an inpatient admission’ and she referred me to a colleague of hers who worked in the NHS and I had an appointment with that consultant and we had quite a chat, he talked to me about how I felt, what I thought about an admission and it was agreed that I would be admitted within the week really. Service user
So the first point we hear about them is that there is some kind of referral process which happens and as part of the referral process it can be very multiagency, so we can have the police, ambulance services and A&E staff, obviously the medical and surgical teams and the nursing staff as well. Staff in focus group
A significant part of service provision involves a range of processes and hence a key component of the system.
4.2.6. Resources
Resources are defined as money, material, staff (non-clinical), and other assets that are needed by a person or service to function effectively. In all, 78 codes or references to resources were identified in the data. Resources are key to the functioning of a delivery system and seemed to more strongly expressed in our data from the staff perspective. The inadequacy of resources of all kinds appeared to be the main challenge. The following quotations from two staff and a service user illustrate precisely how resources as system component played out in the narratives.
… The resources at the moment are nowhere near adequate for that. So lots of people, in my view, get care that probably isn’t the best care for them, it might even sometimes be making them worse because there’s no psychotherapy available. Staff in focus group
So I need a room, I need bits of paper, I need a patient that turns up roughly on time, roughly when expected and isn’t totally in crisis or is not made worse. So sometimes we see people from a long way away but the journey makes them worse than they would have been if they’d never seen anyone. Staff in focus group
Talking about it slightly differently, we know that the budget for mental health services is 0.04% or something ridiculous, how are we ever going to get anywhere without any money? Service user
4.2.7. Data/Information
Data and information represent the facts, statistics, and current knowledge about the conditions which may be provided to a person with the condition and/or used by staff and/or carers in doing their work. This includes all data and information requirements for processes and procedures, decision support and skill acquisition. 43 quotations were identified in the data to have elements relating to this component. Three example quotations are given below.
… And the thing is that I’m taking a lot of different drugs and actually I think somebody who had a prescription or had that qualification in knowing how all the medications interact would actually be really bloomin’ helpful. Service user
… I missed the appointment, a few days later I got a letter, a copy of a letter that was sent to the GP, she copies me on her letters, saying ‘He’s missed his appointment, one appointment, I am therefore discharging him completely’. And this was somebody who has been to them saying ‘I think my wife is going to kill me or I might kill her’, blah, blah, blah, didn’t turn up for an appointment, there was no phone call, there was no nothing, just dismissed completely. Service user
… . When I started in this service I sort of had quite a lot of autonomy to do what I think is right with the OT part of the service and on a practical level … well the library service was really, really helpful, because in terms of gathering evidence for me, helping me with literature searches. Staff 101
4.2.8. Staff/Carers
These are the people who are directly involved in the provision of care. These are the frontline staff and/or carers who are distinct from other staff in the service such as managers or administrative staff. This system component emerged in the greatest number of quotations − 118. Some of the elements identified as part of this system component include, psychiatrists, clinical psychologists, OTs and many more. The following quotations are a few examples.
I was diagnosed with bipolar three years ago and had a very severe form of mania and I was taken to … where I remained for a while and I had excellent care and since then I’m seeing the psychiatrist once a month. Service user
I’m recently seeing the clinical psychologist and now I’m on a waiting list which has taken a while to get some talking treatment, but my experience has just been amazing, I wouldn’t be here if they … like all the time they’ve been with me so for me I’ve been very fortunate. Service user
Yeah. So in terms of people so I lead the OT and support work team, with our team, so to do that we need an experienced lead OT and then at least one other occupational therapist and we need … We’ve currently got three support workers, … Staff 101
I suppose they’ve got some motivation that they’ve even agreed to come, so I guess sometimes the psychiatrist might say ‘Oh I think you need this therapy’ and they say ‘Oh no, I don’t want that’, or ‘It’s not going to help me.’ Staff in focus group
4.2.9. Family/Friends
These are the friends and family of the person or people for whom the service is developed. This component seemed to be important in this context of mental health. It was clearly identified in several quotations but not as many as some of the other components. In line with the characteristics of qualitative data analysis, we did not identify systems components only based on the number of occurrences but also on what may be considered important as expressed by some participants. The perception of this component seems to differ from the perspectives of service users and staff. Whilst service users are likely to mention family or friends in the context of support, staff could also see this as a contributing factor in a service user’s challenges. Example quotations from service users and staff are given below.
So eventually I came out and they asked my mother if she’d have me because I don’t think anybody else could and because my mother was a bit frightened the crisis team came every day. So they were really helpful, they were really supportive. Service user
This isn’t me personally but my friend was on a waiting list to get CBT like I was from … , but she also contacted Mind and they got back to her quicker, she’s been on the … waiting list for about three months and Mind got back to her in a month … Service user
So they grew up with difficult family circumstances or being abused or being rejected or neglected and that those experiences have shaped the way they interact with other people … Staff in focus group
Note that a friends or family under this component will not have responsibility for caring for the service user. They are, through their relationship with the service user, part of a network of people that make a difference to him or her. When a friend or family has a responsibility to provide care and is an unpaid non-professional, he or she will be a carer and therefore part of the “Staff/Carers” component described above.
4.2.10. Environment/External agencies
This represents everything else that can have an impact on the service but is not directly within it. For example, policy, schools, the council or even the weather. Of all the systems components identified, this one seems to be the least intuitive. It was clear from both service user and staff stories that there were several elements that impacted on what happened within the mental health service delivery system, but which are not part of the day-to-day running of the service. They are not the responsibility of the mental health Trust and are not controlled by them. There were about 100 quotations from the data with references to police, GP, charities commissioners. The following are a few examples.
my most recent experience though was I got told that I needed to be put on a waiting list for CBT and during that period on the waiting list I found somewhere else that offered it on a voluntary kind of payment basis and so they are helping me at the moment rather than actually the mental health services themselves. Service user
My GP referred me to Complex Cases because I’d seen them before, because they used to deal with people who had severe physical illnesses that caused mental health difficulties. Service user
she was on the phone to somebody screaming for help, ‘She needs help! She needs help!’ and then the help didn’t come but the police did. So I was dragged away without hardly any clothes on, without any shoes on and into the local police station at Parkside and I ended up in …, and for a long time I didn’t know who I was or where I was. Service user
But remember we are a commissioned service so we are answerable to our commissioner which is the CCG, and indirectly … Staff 102
4.2.11. Co-occurrence between system components
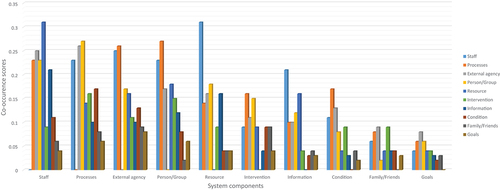
From the data analysis, we also found that participant stories did not only help to identify the key components of the system. The stories revealed how these components may be related. This was based on the co-occurrence analysis of the system components. This analysis, which is a feature of the Atlas.ti qualitative analysis software, uses the quotations, and the codes which represent the system components. A quotation can have multiple codes assigned to it depending on the system elements contained in it. For example, if the codes for “Staff/Carers” and “Data/Information” appear in the same quotation, then they are said to co-occur. The co-occurrence analysis looks at all the quotations in the dataset and quantifies the frequency by which any two pairs of system components co-occur. In other words, this analysis seeks to answer the question “which system components do participants talk about together?” This is one of the benefits of storytelling as methodology as participants are not intentional about revealing these relationships between system components. below shows a summary of the results of the co-occurrence analysis. It is important to emphasise that this is not a measure of which system component is more important.
Figure 3. Co-occurrence analysis of system components.
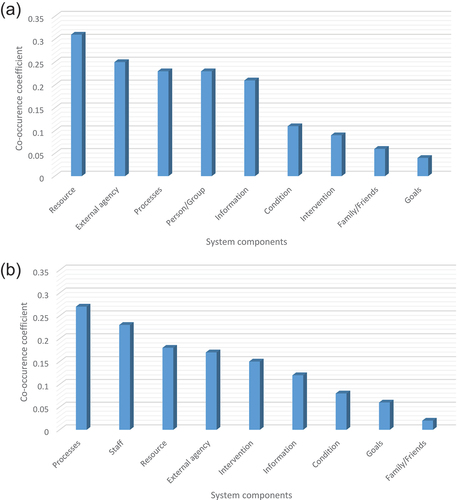
shows two examples in detail. (a) shows the co-occurrence between the “Staff” components and the other nine components. (b) shows the co-occurrence between the “Person” component and the other components. What these figures show is that when participants spoke about the “Staff” component, their references appear to be more frequently referring to “Resources”. Similarly, when participants spoke about the “Person” component, their references appear to be more frequently referring to “Processes”. We emphasise again that this is not about which component is more important than the other. Rather, these raise several interesting questions which we explore under the discussion section.
Figure 4. Co-occurrence between “Staff” component and other components (a) and co-occurrence between “Person/Group” component and other components (b).
4.2.12. Validation of system components
The mental health system components identified above were validated in subsequent focus groups and interviews with the goal to find out if anything was missing. The general feedback from participants is that components do capture all aspects of mental health delivery reasonably well. A few quotes from participants in response to the question “are we missing anything?” are presented below.
No, especially within mental health. I think that’s been important because I think you would have had an easier job if you’d have just gone to clinicians or you’d … but I think we get very blinkered in mental health and within the NHS generally to kind of patient … it becomes very much about the clinician and the system rather than about the patient and that’s not a good thing. Staff 403
Well I do spend quite a lot of time thinking about service delivery and the various components of the service I work in fit together. But I suppose this is a different paradigm or a different model or just a different framework, because I’m not really used to it it’s requiring a paradigm shift in my own head which is enjoyable. Staff 404
… I sometimes use diagrams and draw something, and this reminds me of one that I sometimes do which is that a person is saying something about I’ve got low self-esteem, or I’ve got no confidence, so I represent that as a raft and then the various components that go to kind of help support it as it floats. … . That’s just what I thought when I saw this, I thought these are all things that … they’re all supporting a mental health service, I mean you could put the patient there and they’re all supporting, but actually it’s kind of symbiotic isn’t it … Staff 404
5. Discussions
5.1. Results in context
This paper has shown that the stories that service users tell of their experiences of receiving care in a mental health delivery system, together with the stories that staff tell of their experiences providing care in the same system give us a unique window into the system. Through these stories we can identify the key components of the delivery system – People, Goals, Conditions, Interventions, Processes, Resources, Staff/Carers, Data/Information, Family/Friends and Environment. In addition, their stories also reveal interesting associations between these components. These findings are an important step towards a better understanding of mental health delivery systems and how to describe them. This system understanding and description is vital to creating a shared understanding between stakeholders to facilitate improvement efforts.
It has been argued that “ … of all the things that we try to measure in mental health services research, the most difficult and dangerous is describing the services” (Bickman, Citation2000). This study is a first step towards opening the “Black box” of mental health delivery systems (Bickman, Citation2000) and developing a systematic way of describing them. Research efforts in mental health have predominantly focused on neuroscience and clinical research to discover causes and treatment of mental disorders (Minas & Cohen, Citation2007). With the alarming state of mental health globally, it has become imperative to give attention to research into mental health delivery systems (Minas & Cohen, Citation2007; Vigo, Citation2021). The findings reported here are timely. They begin to focus attention on the delivery system as a whole and not only on an intervention or process. They present the system as complex with implications for system understanding and systems design.
In the global context, mental health remains a priority for the World Health Organisation (WHO). With its comprehensive mental health action plan (WHO, Citation2021a), health systems building blocks (WHO, Citation2010) and emerging synthesis of the evidence of the impact of COVID-19 on mental health (WHO, Citation2022), it seeks to lead the way in guiding nations in the best course of action. The research reported in this paper complements these initiatives in at least two ways: First research. The comprehensive mental health action plan sets several targets for 2030. One of these is for the output global research on mental health to be doubled. We will argue that this cannot mean double of the same but also to promote research into new areas of understanding that can make a difference to service user experience. Second, service delivery. The health systems building blocks, for example, emphasises the importance of health service delivery from the top down. In this study, we take the counter perspective. We begin with the users’ stories as a window into the delivery system. The two perspectives, however, seem mutually complementary.
5.2. Implications for system understanding – facilitating shared understanding
Identifying the components of a system is a necessary first step to understanding how it works. Despite the volumes of work published on mental health services research, the question “what is a mental health service or system” has received little or no attention. Bickman acknowledged that perhaps we do not know what the services actually are (Bickman, Citation2000). The absence of a shared understanding of what the system is can hinder several efforts at improving care. This is because without a shared model of the system all decisions and policies will be based on mental models which are highly unreliable (Forrester, Citation1971). A formal model of a system exposes hidden assumptions and facilitates genuine attempts to improve care.
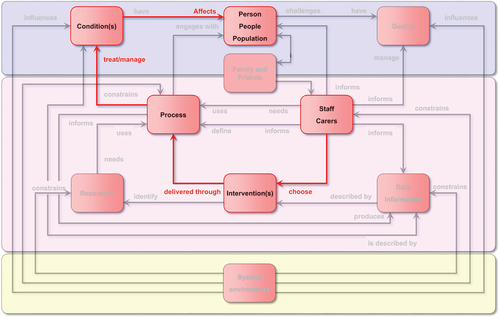
With a formal model or representation of a system, several narratives can be explored, and issues examined in a transparent way. The representation of components and their interactions in is informed by the “things and happenings” concepts used by Douglas Ross in his Structured Analysis language (Ross, Citation1977). These have been confirmed in the context of mental health using empirical data (Komashie & Clarkson, Citation2018). The components represent entities or “things” in the system and the interactions between them are actions or “happenings” that occur. In the most basic form, these are noun-verb representations. also highlights an example of how a shared narrative may be constructed around the components of a mental health service system. This example focuses on how “Staff” may choose or develop “Interventions” that are delivered through “Processes” to treat “Conditions” that affect a “Person”. This simple scenario can lead to several questions to inform a useful and transparent discussion about the system. At the same time, the diagram shows other possible links that remind stakeholders of other possible influences on the chosen scenario. For example, it may be important to note that the “Environment” may still influence the “Condition” or constrain the “Staff or Carers”.
Figure 5. Example of exploring interactions between system components showing how “Staff can choose Interventions delivered through processes to treat a condition that affects a person”.
5.3. Implication for service design – stories provide a window into the care delivery system
Focus groups and interviews have often been used to explore specific set of issues like people’s views and experiences of a service to make a value judgement (Kitzinger, Citation1994). To our knowledge, this is the first study of its kind that combines storytelling with focus group methodology not for the purpose of making value judgements on a health service but as window into the system itself. Interestingly, the analysis of the participant stories did not only confirm the original system components, but also revealed different levels of associations between system components that could lead to further explorations.
As presented in the section on “co-occurrence between system components” above, some of the associations are to be expected yet intriguing all the same. For example, the “Staff” component having the highest co-occurrence with the “Resources” component could be because of the obvious implications of resource availability on staff ability to do their work. Could there be other reasons? To fully understand a particular service situation, these could be very useful questions to explore.
5.4. Implications for service design – a model of mental health delivery systems
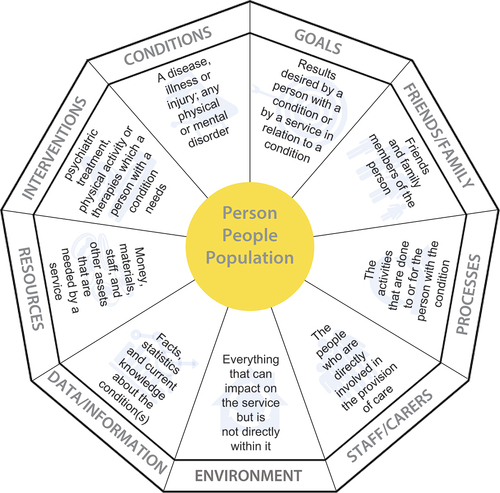
During our focus groups and interviews, participants regularly expressed the need for the person, people, or population to be at the centre of any visual representation of the delivery service. The need for a model of mental health delivery services has been recognised in the mental health service research literature for decades (Bickman, Citation2000; Burns & Priebe, Citation1996). In reflecting on the implications of our results for mental health service design, we found it appropriate to develop a model of the system that incorporates all the components and has the service users at the heart of it. The result is , our proposed model of mental health delivery systems. In any service design or redesign exercise, a project team using this model can easily ask if some part of the system is being left out and if that was appropriate.
Figure 6. A proposed model of mental health delivery systems showing the ten key components with the person at the centre.
The use of this model in identifying the components of a mental health system strongly complements the application of a systems approach to improvement (Clarkson et al., Citation2017, Citation2018). Systems approaches have received increasing recognition in recent decades as an effective way of dealing with the complexities in improving health and care system (Komashie, Hinrichs-Krapels, et al., Citation2021; Komashie, Ward, et al., Citation2021). A systems approach essentially involves four key perspectives on People, Systems, Design and Risk. The People perspective is about understanding the interactions among people, at personal, group and organisational levels. Systems is about addressing complexity in real world problems with highly interconnected technical and social elements. Design is about focusing on improvement by identifying the right problem to solve. Risk emphasises the need to manage risk, based on the timely identification of threats and opportunities (Clarkson et al., Citation2017). The work reported in this paper provides one model for supporting explorations in the People and Systems perspectives.
5.5. Limitations and further work
The main limitation of this work is in the focus on service users and staff as participants to the exclusion of other stakeholders. There are several other stakeholders (e.g., commissioners, and policy makers) whose perspectives would have been useful, but resource and time limitations did not allow the inclusion of more stakeholders. However, we believe that service users and staff are key to the delivery system and provide a useful starting point. In addition, the choice of quotations in the qualitative analysis was not an exact science. There is therefore a subjective element to the size of a quotation based on what was considered meaningful or useful for the analysis. Though different quotation lengths may not have had significant impact on the system components, we believe the results of the co-occurrence analysis could be slightly different.
The current work has provided a high-level system description but opens several potential questions for further exploration. For example, what is the most useful way of describing each of the components in detail? We intend to explore each system component in detail and develop diagrammatic approaches for visualising them.
6. Conclusions
This paper has shown that the stories that service users tell of their experience receiving care in a mental health delivery system, together with staff stories about their experience providing care in the same system, gives us a unique window into the delivery system. It also shows that the ten key components namely, Staff, Resources, Environment, Person/Groups, Processes, Data/Information, Conditions, Interventions, Family/Friends, and Goals, sufficiently represent a mental health delivery system. All these components are vital to the delivery of good quality and safe care and need to be considered in any service design work. The results show that all these components have different levels of association with each other based on the analysis of how frequently they occurred together in participants’ narratives. It was found for instance that service users in the service who were represented as the person/group component have the strongest association with processes whilst staff had the strongest association with resources. These associations are not meant to show which components are more or less important, but they might be useful in helping service designers better understand the complex inter-component interactions. We have also demonstrated that the interaction between system components may represent a taxonomy for visual communication about the relationship between system components.
Acknowledgments
This research was supported by The Healthcare Improvement Studies Institute (THIS Institute), University of Cambridge. THIS Institute is supported by the Health Foundation, an independent charity committed to bringing about better health and healthcare for people in the UK. The authors also want to thank all the service users and staff who participated in the focus groups and interviews and the members of the Service User Advisory Group (SUAG) for their contribution to the study.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- ATLAS.ti. (2019). ATLAS.ti 8 Qualitative Data Analysis Software. http://atlasti.com/
- Bickman, L. (2000). The most dangerous and difficult question in mental health services research. Mental Health Services Research, 2(2), 71–72. https://doi.org/10.1023/A:1010100119789
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
- Britten, N. (1995). Qualitative research: Qualitative interviews in medical research. BMJ, 311(251), 251–253. https://doi.org/10.1136/bmj.311.6999.251
- Burns, T., & Priebe, S. (1996). Mental health care systems and their characteristics: A proposal. Acta Psychiatrica Scandinavica, 94(6), 381–385. https://doi.org/10.1111/J.1600-0447.1996.TB09878.X
- Chenail, R. J. (2012). Conducting qualitative data analysis: Reading line-by-line, but analyzing by meaningful qualitative units. Qualitative Report, 17(1), 266–269. https://doi.org/10.46743/2160-3715/2012.1817
- Clarkson, P. J., Bogle, D., Dean, J., Tooley, M., Trewsby, J., Vaughan, L., Adams, E., Dudgeon, P., Platt, N., & Shelton, P. (2017). Engineering better care: A systems approach to health and care design and continuous improvement. http://www.raeng.org.uk/news/news-releases/2017/september/healthcare-professionals-and-engineers-partner-to
- Clarkson, P. J., Dean, J., Ward, J., Komashie, A., & Bashford, T. (2018). A systems approach to healthcare: From thinking to practice. Future Health Care Journal, 5(3), 151–155. https://doi.org/10.7861/futurehosp.5-3-151
- Elliott, C., & Deasley, P. (2007). Creating systems that work: Principles of engineering systems for the 21st century. The Royal Academy of Engineering, 293074. http://www.raeng.org.uk/publications/reports/rae-systems-report
- Fadlallah, R., El-Jardali, F., Nomier, M., Hemadi, N., Arif, K., Langlois, E. V., & Akl, E. A. (2019). Using narratives to impact health policy-making: A systematic review. Health Research Policy and Systems, 17(1). https://doi.org/10.1186/s12961-019-0423-4
- Forrester, J. W. (1971). Counterintuitive behavior of social systems a new approach to social systems. Technological Forecasting and Social Change, 22(3), 1–22. https://doi.org/10.1016/S0040-1625(71)80001-X
- Karni, R., & Kaner, M. (2007). An engineering tool for the conceptual design of service systems. In D. Spath & K.-P. Fähnrich (Eds.), Advances in Services Innovations (pp. 65–83). Springer Berlin Heidelberg. https://doi.org/10.1007/978-3-540-29860-1_4
- Kitzinger, J. (1994). The methodology of focus groups: The importance of interaction between research participants. Sociology of Health & Illness, 16(1), 103–121. https://doi.org/10.1111/1467-9566.ep11347023
- Kitzinger, J. (1995). Qualitative Research: Introducing focus groups. BMJ, 311(299), 299–302. https://doi.org/10.1136/bmj.311.7000.299
- Klein, J. H., Connell, N. A. D., & Meyer, E. (2007). Operational research practice as storytelling. The Journal of the Operational Research Society, 58(12), 1535–1542. https://doi.org/10.1057/palgrave.jors.2602277
- Komashie, A., & Clarkson, P. J. (2018). Designing mental health delivery systems: Describing the relationship between system components. Proceedings of International Design Conference, DESIGN, 6, 2669–2680. https://doi.org/10.21278/idc.2018.0413
- Komashie, A., Hinrichs-Krapels, S., & Clarkson, P. J. (2021). Systems approaches to healthcare systems design and care delivery: An overview of the literature. Proceedings of the Design Society, 1(August), 2941–2950. https://doi.org/10.1017/pds.2021.555
- Komashie, A., Ward, J., Bashford, T., Dickerson, T., Kaya, K. G., Liu, Y., Kuhn, I., Gunay, A., Kohler, K., Boddy, N., O’Kelly, E., Masters, J., Dean, J., Meads, C., & Clarkson, P. J. (2021). A systems approach to healthcare design, delivery and improvement: A systematic review and meta-analysis. British Medical Journal Open, 11(X), XX. https://doi.org/10.1136/bmjopen-2020-037667
- The Lancet Regional Health – Europe. (2022). Preparing for a hotter world. The Lancet Regional Health - Europe, 19, 100484. https://doi.org/10.1016/j.lanepe.2022.100484
- Minas, H., & Cohen, A. (2007). Why focus on mental health systems? International Journal of Mental Health Systems, 1(1), 1–7. https://doi.org/10.1186/1752-4458-1-1
- Nyumba, T., Wilson, K., Derrick, C. J., Mukherjee, N., & Geneletti, D. (2018). The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods in Ecology and Evolution, 9(1), 20–32. https://doi.org/10.1111/2041-210X.12860
- Puckett, K. (2016). Narrative theory: A critical introduction. Cambridge University Press.
- Ross, D. T. (1977). Structured Analysis (SA): A language for communicating ideas. IEEE Transactions on Software Engineering, SE-3(1), 16–34. https://doi.org/10.1109/TSE.1977.229900
- Sinnott, C., Kelly, M. A., & Bradley, C. P. (2017). A scoping review of the potential for chart stimulated recall as a clinical research method. BMC Health Services Research, 17(1), 1–11. https://doi.org/10.1186/s12913-017-2539-y
- Taylor, B., Henshall, C., Kenyon, S., Litchfield, I., & Greenfield, S. (2018). Can rapid approaches to qualitative analysis deliver timely, valid findings to clinical leaders? A mixed methods study comparing rapid and thematic analysis. British Medical Journal Open, 8(10), 5–7. https://doi.org/10.1136/bmjopen-2017-019993
- Vigo, D. (2021). Dawn of a new day for mental health systems. International Journal of Mental Health Systems, 15(1), 1–3. https://doi.org/10.1186/s13033-021-00475-x
- WHO. (2009). Improving health systems and services for mental health. In Mental health policy and service guidance package. http://apps.who.int/iris/bitstream/handle/10665/44219/9789241598774_eng.pdf?sequence=1%0Ahttp://www.who.int/mental_health/policy/services/mhsystems/en/index.html
- WHO. (2010). Monitoring the Building Blocks of Health Systems : a Handbook of Indicators and their measurement strategies. https://apps.who.int/iris/handle/10665/258734
- WHO. (2021a). Comprehensive Mental Health Action Plan 2013 - 2030. https://www.who.int/initiatives/mental-health-action-plan-2013-2030
- WHO. (2021b). WHO Mental Health atlas 2020. https://www.who.int/publications/i/item/9789240036703
- WHO. (2022). Mental Health and COVID-19: Early evidence of the pandemic ’ s impact. World Health Organization: Scientific Brief, 2(March), 1–11. https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1
