
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
The number of surplus frozen human embryos in storage in the United Kingdom (UK) is at its highest level since records began in 1991 and the formation of the UK Human Fertilisation and Embryology Authority (HFEA). This study features a quantitative analysis of data from 1991 to 2019 provided by the HFEA as well as a commentary on observed trends within this data. We also discuss trends relating to the final destiny of surplus embryos. Data analysis show that at least 130,000 stored embryos have been discarded in the UK since 1991, while another 500,000 embryos are currently being stored in a frozen state, of which a significant proportion is likely to be discarded in the future. However, this creates a moral dilemma since UK legislation relating to human embryos is based on the 1984 Warnock Report which recognizes that they have a special moral status.
KEYWORDS:
1. Introduction
During an In Vitro Fertilisation (IVF) cycle in the UK, about 5–34 eggsFootnote1 are retrieved through surgery from a woman, which are then fertilized with the sperm of a man in a laboratory (Diaz-Garcia Citation2023). The eggs are held in a special media and cultured in an incubator until insemination (Diaz-Garcia Citation2017). They are subsequently allowed to develop for two to four days before they are checked to see if any egg has been successfully fertilized. One or two of the embryos are then selected by the fertility expert and transferred into the womb with the aim of starting a pregnancy (Diaz-Garcia Citation2017). The remaining surplus embryos, if there are any, are usually frozen for future use since the UK Human Embryology and Fertilisation Act 1990 (as amended, HFE Act 1990)Footnote2 allows the creation of surplus embryos.
Research also shows that since 1991, there has been a continuous increase in the number of women choosing IVF with the possible creation of supernumerary embryos. Thus, the number of IVF cycles recorded at licensed fertility clinics in the UK grew from around 6,700 in 1991–76,000 cycles in 2021 (HFEA Citation2021). Moreover, the storage limit of human embryos has been raised with the enactment of the UK Health and Care Act 2022. This Act indicates that persons undergoing fertility treatment can store their embryos for their own use for up to 55 years, providing they reconsent every 10 years (UK Parliament Citation2022, schedule 17). The same schedule also indicates that if persons consent to their embryos being used after their death, they can remain in storage for another 10 more years after they have died.
In this context, since the total number of embryos currently in storage in the UK remains unknown, the authors obtained a set of data from the Human Fertilisation and Embryology Authority (HFEA) beginning in 1991 and spanning three decades. These data were then used to present the current situation of embryo storage in the UK. As we proceed, some ethical concerns will emerge from considering the implications of the data. These questions urgently need to be addressed since, without us making a direct judgment of the matter, they may or may not go against interests of individual patients and of the public alike.
2. Methodology
The main body of this paper consists of data analysis employing basic algorithms and plotting, the mathematical details of which are specified with the presentation of data. The public data are drawn from HFEA annual reports available on its official site.Footnote3 In addition, the authors requested certain specific data from the HFEA under the Freedom of Information Act (2000). Between the 4th-25th August 2022, the HFEA provided relevant data from a live register spanning the years 1991–2019, with 2019 being the latest year in which data were available. But it was indicated that one centre was excluded due to data reporting issues. Meanwhile, some data were only available in more recent years due to changes in the information that was collected on register forms, and since the data provided was from a live register, it may not match data provided in previous requests or published elsewhere. The HFEA also replaced all counts of less than 5 with a < 5 because of the significant possibility of the identification of individual patients, to whom a duty of confidentiality is owed. For the sake of expediency during calculation, however, all <5 data points were treated as 3 in this paper. Further, the HFEA indicated that embryos are sometimes discarded for reasons unrecorded on its register and, more generally, embryos may be discarded in the course of treatment. This means the following tables cannot provide a precise account of the situation, but the information obtained can still be useful if it is treated as informed estimates.
3. Results
The first set of data which was acquired was the number of surplus embryos discarded, sorted by six specific reasons of disposal.
Another set of data obtained from the HFEA presents the number of new embryos being stored as well as the various destinations of some of the previously stored embryos. Using these data, an estimation of new embryos being stored every year (i.e. yearly storage surplus) was calculated (T) on which an estimation of the overall storage of embryos at the end of each year was deduced (U) which were rounded to the nearest thousand. Indeed, because of the nature of the data, the precise total number of stored embryos at the end of each year was impossible to determine. But U is nevertheless a valuable index regarding the current situation of frozen embryos in the UK.
4. Discussion
As already noted, more embryos are generally created in IVF treatment in the UK than can be immediately implanted into the woman in order to reduce the burden and risks of retrieving the eggs from the woman through surgery (Bodri et al. Citation2008) and also to save costs. These surplus embryos may then be frozen for a number of reasons including the desire by individuals to have further treatments with thawed embryos in the future.
In this context, when individuals are responsible for bringing into existence embryos through IVF, the embryos are usually seen as belonging to these individuals though this is not generally represented as a form of ownership. Indeed, those responsible for generating the embryos are generally considered to have the authority and responsibility to make decisions about the fate of the embryos which they have created through IVF (Fuscaldo Citation2005, p. 95).
It is also possible that creating and freezing surplus embryos during IVF has become a normal procedure in the UK with infertile individuals simply agreeing to the practice without further thoughts in their eagerness, and sometimes desperation, to have a child as soon as possible. Some of the patients may not even be informed that they do not have to fertilize all the obtained eggs through IVF.
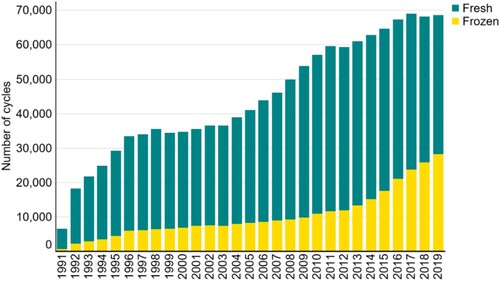
In this regard, statistics indicate that frozen embryos are increasingly being used in fertility treatment in the UK. Accordingly, the 2019 report published by the HFEA identified an 86% surge in the proportion treatment cycles using frozen embryos from 2014–2019, as shown in (HFEA Citation2019, §4):
Figure 1. Number of IVF cycles over time by fresh and frozen embryos, 1991–2019.
4.1. Increasing number of stored frozen embryos
Generally, it is not easy for individuals to decide what to do with their surplus frozen embryos (Fuscaldo Citation2005, p. 93, Fuscaldo et al. Citation2007). For instance, a study by Robert Nachtigall et al. (Citation2005) indicated that 72% of the interviewed couples with an average of 7.1 surplus frozen embryos had not reached a final decision after an average of 4.2-year storage time. In a similar study, it was indicated that more than two thirds of the 77 families interviewed decided to keep their frozen embryos for more than 5 years either passively, because of disagreement or indecision, or actively, in order to (1) maintain embryo potential, (2) avert feelings of loss, or (3) as psychological or genetic ‘insurance’ (Nachtigall et al. Citation2009). This reluctance to make a decision could even last until the storage limit was reached when the embryos had to be destroyed. Indeed, many seemed to actively avoid deciding what to do with their embryos by failing to respond to, or breaking contact with, the clinic (MacCallum and Widdows Citation2012, p. 279, Tonkens Citation2016). As shown in , this reason accounts for up to 42% of the total embryos discarded in 2018. Thus, the data reveal a certain, perhaps unexpected, reluctance of individuals to decide the fate of their stored surplus embryos.
Table 1. The number of embryos discarded by reason between 1991–2019, constructed based on the data provided by HFEA in August 2022. Blank spaces indicate that no data were available. Estimated total disposal in each year is calculated using Equation (1): . *The data points ‘<5’ are averaged to 3 for expedience.
Furthermore, the primary reason for embryos being stored, namely, further pregnancy attempts, does not generally persist in time. In the 2009 Nachtigall study (Citation2009, pp. 2094–5), only 8% of the interviewed families intended to make further pregnancy attempts with their surplus embryos after one year. Indeed, whatever the original motives for storing the embryos, subsequent practical considerations seemed to initiate a re-evaluation of the aims of these individuals. Some may even opt, eventually, for their embryos to be discarded because it was acknowledged that discarding provided a clear and definite outcome (Nachtigall et al. Citation2009, p. 2096).
Such a discrepancy between the number of stored embryos and further uses of embryos in fertility treatment is corroborated by the comparison between the trends of total embryos in storage and usage for treatment over three decades, as shown below in :
Figure 2. The estimated number of embryos in storage (U), embryo usage for treatment (J), yearly storage surplus (T), and new embryos stored (G), 1991–2019. The data were adopted from .
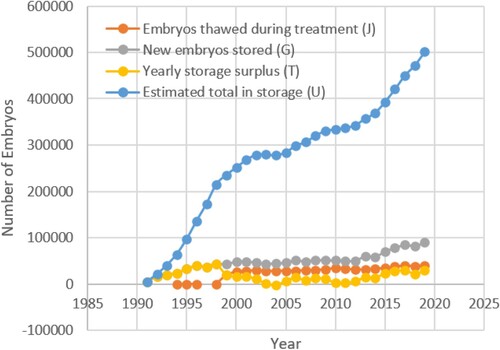
This demonstrates that although a constant increase in the number of embryos thawed for treatment has taken place, which was emphasized in the 2019 HFEA report, it is dwarfed by the consistent increase of the total number of embryos in storage since many more new embryos are frozen than are thawed for treatment or otherwise used. In 2019, for example, about 40,000 embryos were thawed for treatment, which was only about 8% of the total in storage, while more than twice as many new embryos entered into storage in the same year (). Furthermore, to make the comparison of the rates of growth in different categories more obvious, the rate of growth of U, J and G in were calculated and plotted as :
Figure 3. The rates of growth of estimated total in storage (calculated using Equation (4): ), embryo usage for treatment (calculated using Equation (5):
), and new embryos stored (calculated using Equation (6):
), 1991–2019. The data were derived from relevant data in .
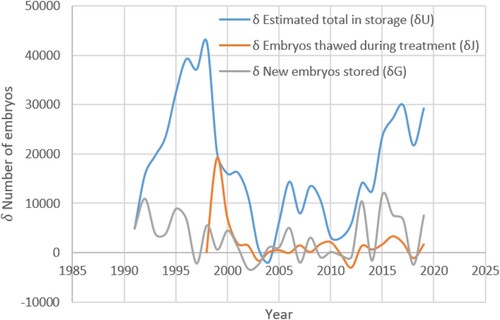
Table 2. The number of embryos stored, donated, thawed, and discarded between 1991–2019, constructed based on the data provided by HFEA in August 2022. Blank spaces indicate that no data were available. The estimated yearly surplus is calculated using Equation (2): . The estimated total embryos in storage at the end of each year is calculated using Equation (3):
. The U values are rounded up or down to the nearest thousand. *The data points ‘<5’ are averaged to 3 for expedience.
This figure indicates that the growth rate of embryos being thawed peaked at about 1999, but then quickly levelled off with only minor rises every year. In contrast, the growth rate of new embryos being stored did not pick up until 2013 which led to another surge in the growth rate of total storage. These gradients indicate that, in recent years, many more individuals have been attracted to embryo freezing than those who eventually use these frozen embryos. Although the general trend suggests that the number of IVF procedures using frozen embryos will probably keep rising, it is very likely that it will still be outmatched by the escalating number of new embryos being stored.
4.2. Embryos donated to other individuals and to research
Other interesting trends obtained from the data were that of the number of embryos donated to other individuals and to research.
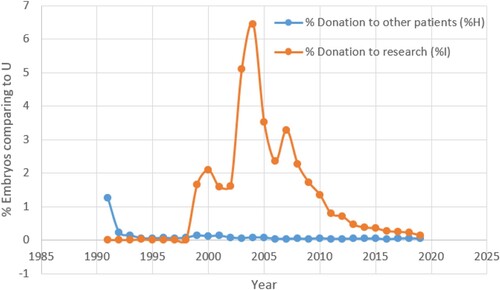
Moreover, relative numbers of embryos donated to other patients and to research were plotted as percentages of the estimated total in storage (U) for each year, as shown in Figure 6:
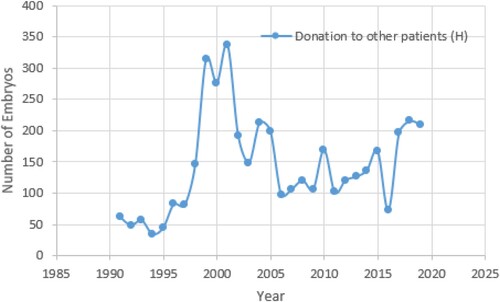
shows that the number of embryos donated to others for gestation was extremely low until it began to increase in 1998–2001, but it then started dwindling again to ca. 100–200 embryos donated every year. From a different perspective, though, the number of embryos donated to other patients is always very low in terms of percentage of the estimated total in storage, as Figure 6 shows. This phenomenon needs further investigation since some studies have suggested that a majority of individuals had a positive attitude towards embryo donation to other couples. For example, a survey conducted in Switzerland indicated that 52% of the participants thought donation of surplus embryos to other couples should be allowed (Mohler-Kuo et al. Citation2009, p. 1935) though a Norwegian study shows a much greater reluctance amongst interviewees (Kvernflaten et al. Citation2022, p. 580). Thus, it is unclear why so few couples donate their surplus frozen embryos to others though some suggestions have been proposed. For example, a study by Sheryl de Lacey (Citation2005) indicated that many patients expressed a willingness to donate their surplus embryos to other patients when first interviewed, but the majority subsequently changed their minds. The reason for such a development, according to the study, was a change in the patients’ perspective when they became parents. Indeed, it was established that parenthood brings about a certain emotional connection between them and their frozen embryos. Donation to other patients was then considered to be more similar to child relinquishment (De Lacey Citation2005).
Figure 4. Number of donated embryos to other individuals from 1991–2019. The data were obtained from relevant date in .
Other research suggests that a number of individuals with surplus embryos make a decision relating to the destiny of these embryos based, in part, on the significance they attach to genetic relatedness (McMahon et al. Citation2000, De Lacey Citation2005). Accordingly, a number of studies indicate that many individuals would prefer that their surplus embryos be destroyed rather than donated to infertile couples even when they support donation in principle (Darlington and Matson Citation1999, Newton et al. Citation2003, MacCallum and Widdows Citation2012, pp. 277–8). This is because they feel connected, in some important and crucial way, to their embryos and do not want other parents raising them as their own.Footnote4 On the other hand, individuals who believe that social, and not genetic, relationships are relevant seem to be more willing to donate their embryos to other couples (Fuscaldo Citation2005, p. 56).
According to , the number of embryos donated to research, having peaked in 2004 and 2007, decreased to 675 in 2019. At the same time, the percentage of embryos donated to research of the estimated total in storage, seen in , presents a trend that generally follows that observed in its absolute number. Although further research is required to account for these two peaks, it may have resulted from the development of research in Embryonic Stem Cells which began in 1998, when their potential uses in human developmental biology, drug discovery, and transplantation medicine were recognized (Thomson et al. Citation1998). This hypothesis would also explain the subsequent decline in the number of embryos donated to research which began in 2007, which may have arisen because of the development of Induced Pluripotent Stem Cell in 2006 (Takahashi and Yamanaka Citation2006). These are somatic cells taken from human beings and reprogrammed into a pluripotent state, which can then be used in many settings as an alternative to Embryonic Stem Cells. Consequently, the demand for human embryos in stem cell research greatly decreased.
Figure 5. Number of embryos donated to research from 1991–2019. The data were obtained from relevant date in .
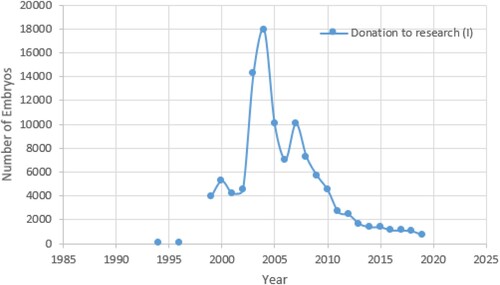
Figure 6. The relative number of embryos donated to other patients (calculated using Equation (7): ) and to research (calculated using Equation (8):
) as percentages of the estimated total in storage (U) from the same year, 1991–2019. These data are derived from relevant data in .
4.3. Embryos discarded
The total number of embryos discarded every year has also shown an overall increase, especially due to the end of storage period and patient request, as shown below in :
Figure 7. The number of estimated total disposal, as well as disposal by various reasons listed, 1996–2019. The data were adopted from . The number of embryos discarded under the reasons ‘no longer required for use in treatment’ and ‘donor sample discarded’ are very small, so they are not plotted in this figure.
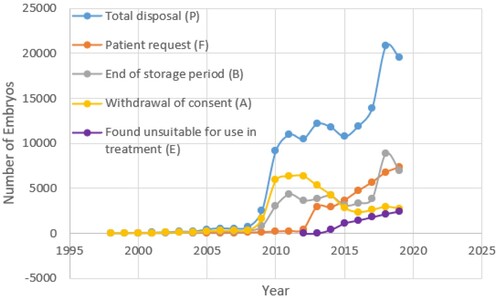
This figure indicates an increase in the total number of embryos being discarded as well as for the different mentioned reasons, with the only exception being the trend of embryos being discarded for ‘withdrawal of consent’. However, the information given by the HFEA in 2022 was ambiguous since ‘withdrawal of consent’ and ‘patient request’ are two terms which may be considered as somewhat similar. In any case, these patterns are not surprising, especially when considered in the context of a steady increase in the total number of surplus embryos shown in . As already noted, and also emphasized in the study by de Lacey (Citation2005), it is a rather common phenomenon that patients change their minds, with time, concerning the destiny of their stored surplus embryos. Indeed, a real difference exists between the idealistic plan of an individual or couple and how reality turns out. Such a change of mind due to new circumstances may account for a considerable proportion of the embryos discarded by ‘withdrawal of consent’ and by ‘patient request’.
4.4. Moral Status of Embryos
A number of studies (Mohler-Kuo et al. Citation2009, Simopoulou et al. Citation2019, p. 2455, Abreu et al. Citation2021) highlight the already mentioned difficulties for individuals to decide the fate of surplus cryopreserved embryos in different countries. These indicate that sociocultural and other factors such as religion, age, treatment period, ethnicity, income, marital status, economic status, and education level are all elements that may influence a couple’s decision-making on what to do with their stored embryos. This also includes how those who created the embryos perceive their moral status. A survey conducted by Mohler-Kuo et al. (Citation2009, p. 1935) indicated that 77% of the participants did not agree that an embryo could just be considered as a pile of cells, with the vast majority (89%) believing that an early embryo deserves some sort of respect. Thus, if the individuals consider their frozen embryos as individual entities worthy of value and worth, or even as having the same moral status as born human children, then it is likely that they would experience internal conflicts when deciding the fate of their embryos. A more recent survey seems to confirm this conjecture when it was reported that ‘couples may consider their embryos as their unborn children or even existing children … hence, the process of grief for the loss when their embryos have to be discarded is a reality’ (Simopoulou et al. Citation2019, p. 2455). Likewise, many other studies have associated negative emotional qualities such as anxiety, distress, and grief to the patients’ decision to dispose their embryos (De Lacey Citation2005, pp. 1664–6, Citation2007, pp. 1753–6, Fuscaldo et al. Citation2007, pp. 3133–4, Takahashi et al. Citation2012, p. 9, Delaunay et al. Citation2023, p. 9). Because of this, Abigail Maguire (Citation2021) indicates:
Current regulatory guidelines by the Human Fertilisation and Embryology Authority state that, when terminating the development of human embryos, a clinic should act with sensitivity, taking account of the embryo’s ‘special status’ and respecting the interests of the gamete providers and recipients.
Interestingly, studies also indicate that the more parents believe that embryos have a moral status, the less likely they are to favour donation to other couples (Mohler-Kuo et al. Citation2009). This reflects a paradox since parents who believe that their embryos have some or full moral status may eventually be the ones who are more likely to discard them (MacCallum and Widdows Citation2012, pp. 278–9).
In this regard, Lord Alton from the UK House of Lords indicated in 2012 that embryos were, unfortunately, being created and thrown away in an ‘industrial’ scale in the UK, adding: ‘It happens on a day-by-day basis with casual indifference’.Footnote5 This is in the context of UK legislation relating to human embryos being based on the 1984 Warnock Report which recognized that they have an undefined ‘special’ moral status (Warnock Citation1984). Indeed, for a significant minority of persons in the UK this special moral status means that they actually have a full moral status. Regardless, this ‘special’ status implies that human embryos are at least not purely assemblies of cells, whatever else one may take them to be. Such a conception of embryos necessarily calls for more attention to the ethical concerns around the ‘industrial’ scale of creation and disposal of embryos.
4.5. Future Developments in the UK
As previously mentioned, the storage limit of human embryos has been raised with the enactment of the UK Health and Care Act 2022. This will enable persons undergoing infertility treatment to store their embryos for their own use for up to 55 years, providing they reconsent every 10 years (UK Parliament Citation2022, schedule 17). Moreover, the same document indicates that, provided the persons consent to their embryos being used in the event of their death, they can remain in storage for up to 10 years after they have died.
However, after analysing the previous data, it is unlikely that this legislative change will effectively mitigate the difficulty the patients encounter during the decision-making process. Rather, this extension seems to be simply delaying the problem. It is also possible that this change may exacerbate the ever-rising total number of embryos being stored, and consequently make the question about their destiny even more morally weighty. Another potential outcome of this act is that the number of embryos left in storage by persons who have died will increase. In that scenario, the ethical question may no longer only be the moral status of the frozen embryos, but also who, if anyone, has the right to determine their fate.
4.6. Addressing the ever-increasing number of embryos being stored in the UKFootnote6
It is very likely, based on the data presented, that the rise in the number of embryos being stored will eventually result in an increasing number of embryos being discarded. This is a cause for concern because the human embryo officially retains a special moral status in the UK. Therefore, it is important to try and reduce the overall number of stored embryos being destroyed in order to address the moral challenge of discarding an increasing number of entities which have a special moral status. This goal may be attained in a number of ways.
4.6.1. Improving discussion with individuals before IVF takes place
To begin with, it is important that individuals fully understand the choices that are open to them before IVF takes place in order to make an informed decision. Indeed, Nachtigall et al. (Citation2005, p. 433) found that many couples ‘are initially focused on the immediate goal of achieving a pregnancy … and do not anticipate that having surplus embryos will present a challenge in the future’. In this context, another fertility specialist, Richard Kennedy, stated that patients should be encouraged to reflect on what should happen with their surplus embryos before IVF takes place. With respect to the very high numbers of embryos already being stored in 2003, he indicated:
These figures do raise the question of why we are creating all these extra embryos and I think we should be pro-actively discussing the future of these embryos before the embryos are created.Footnote7
4.6.2. Only creating embryos which are certain to be implanted into a woman
Relating to the discussion taking place before IVF treatment is initiated, it may also be possible to clearly inform individuals that they do not have to fertilize all the eggs obtained through fertility treatment. Indeed, it may be appropriate to only create a small number of embryos which will definitely be implanted into a woman at a later stage, thus avoiding the storage of surplus embryos which may eventually be discarded.
4.6.3. Storing frozen eggs
In order to reduce the number of embryos being stored, it may also be possible to just store unfertilized egg cells, which are not generally considered to have the same moral status as embryos. Egg vitrification is a kind of ‘flash freezing’ procedure in which eggs are quickly immersed into liquid nitrogen, thus cooling them to – 196°C so that they become ‘glass-like’ or ‘vitrified’. Moreover, studies show that eggs frozen with vitrification had a survival rate of up to 91% (Cao et al. Citation2009, Rezazadeh Valojerdi et al. Citation2009) which brings their survival rates very close to those of frozen embryos.
4.6.4. Adopting frozen embryos
Another option providing a real alternative to surplus embryos being discarded is to encourage more couples to consider adopting frozen embryos since fertility experts believe this number could be increased. For example, even in 2003, Ian Craft, who was a director of a fertility centre in London indicated: ‘It surprises me that so few couples agree to donate spare embryos if you consider the desperation of infertile couples to have children’, adding:
There are very few babies to adopt and so I would have thought these couples, who have been through infertility treatment themselves and who have completed their families, would be more sympathetic to others.Footnote8
4.6.5. Freezing of pre-zygotes
Finally, it may be possible to consider changing the law in the UK to something similar to the German Citation1990 Embryo Protection Act. This explicitly forbids the creation of surplus embryos during an IVF treatment cycle (German Bundestag Citation1990, §1.1.2–1.1.5). It also states that it is only possible to fertilize the number of eggs from a woman (to a maximum of three eggs) that can immediately be transferred back into her in one treatment cycle.
However, the German Act also defines an embryo as a fertilized egg after fusion of the pronuclei, which takes place about 10–24 hrs after the sperm cell first penetrates the egg. Pre-nuclear fertilized eggs are where the male pronucleus containing the chromosomes and the female pronucleus are separated. Actually, the early fertilized egg normally still has one set of chromosomes from the sperm cell and the other set from the egg, but it is in a replicated state (Leone Citation2008, p. 18). And only when the fertilized egg begins to develop, with the formation and then expulsion of a polar body (containing an extra set of chromosomes from the egg), does the egg have only one set of chromosomes from the mother. This happens about 2–8 hours after sperm penetration (Van Den Bergh et al. Citation1995, Leone Citation2008, p. 19). Thus, it is not until the expulsion of the polar body that the fertilized egg has the normal two sets of the 23 chromosomes, with one set coming from the man and the other from the woman. Nevertheless, the pronuclei remain separated for a few more hours. This pronuclear stage is reversible to some extent,Footnote9 suggesting that the fertilized egg may not yet have become an organism.Footnote10
As a result, the cryopreservation of fertilized eggs at the pronuclear stage for subsequent use is permitted under German law since they are not considered to be embryos (Kliebisch et al. Citation2016). The rationale behind this legislation was to avoid the ethical dilemmas of unwanted surplus embryos and their eventual destruction since these have, according to German legislation, the moral status of individual persons.
And although this legislation may not be perfect, it may be worth considering in order to address the creation of surplus embryos during IVF in the UK. But if this solution was considered, an amendment to UK legislation would be required since Section 4A (9) of the Human Fertilisation and Embryology Act 1990 (as amended) defines an ‘embryo’ as ‘a live embryo, including an egg that is in the process of fertilization or is undergoing any other process capable of resulting in an embryo’.
5. Conclusion
The data presented in this study have shown that the total number of embryos in storage is continually increasing in the UK. Moreover, the number of embryos being donated to others for gestation remains extremely low for reasons that remain unclear, though it may benefit from more discussion and publicity. In addition, the number of embryos donated for research has decreased dramatically between 2007 and 2019 which may reflect the development of Induced Pluripotent Stem Cells in research.
The data also indicates that at least 130,000 embryos have, so far, been discarded after treatment in the UK since 1991, and ca. 500,000 embryos are currently being stored. Based on the data analysis, it is likely that most of the stored embryos will eventually be destroyed. Human embryos are, however, recognized by the 1984 Warnock Report as having a ‘special’ moral status which, though undefined, position them at least above inanimate objects. But in the current situation where very large number of embryos are created and discarded, they do seem to be treated exactly as inanimate objects. Thus, it seems impossible to remain indifferent to the status quo without grave concerns and further discussion regarding this dilemma. Failure to do so objectively entails a serious lack of moral prudence and responsibility.
6. Limitations of Research
Both the process and the analysis of acquired data follow very basic statistical operations, which make them as unbiased as possible. Nevertheless, we acknowledge some limitations to our research. First, the raw data provided by the HFEA have unsatisfying quality before 1999, which makes the analysis output an educated guess and it is likely an underestimation due to data loss during the early years reported by the HFEA. Second, this paper is not a literature review and so the discussion features only a limited scope of the vast scholarship in this area. We have only presented the studies that we deem the most relevant to the theme of our paper. Meanwhile some particular points, such as the objective moral status of embryos and the gender discrepancy in perceived status of embryos, are not exhaustively explored since they exceed the scope of this paper. Third, we did not have the space to provide a comprehensive legal comparison between UK and other countries worldwide. Further research into the ethics of frozen embryos and their legal status in different countries should be encouraged. Research in such fields will greatly improve the quality of discussion on this sensitive moral issue within the UK.
Acknowledgement
The authors would like to acknowledge the assistance of Ms. Fiona Thomson in the preparation of this article. We are grateful to the HFEA staff who provided assistance in any form. We also thank the two anonymous reviewers whose comments helped improve this paper.
The views expressed in this article are those of the authors and do not necessarily reflect the positions of the professional organizations with which they are affiliated.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Zishang Yue
Zishang Yue is from Henan, China. He holds a MChem Chemistry (University of Edinburgh, 2021) and a MSc Science and Religion (University of Edinburgh, 2022). He is currently a postgraduate researcher in DPhil Theology and Religion (University of Oxford), with research interests in mediaeval metaphysics, quantum interpretations, and bioethics.
Calum MacKellar
Calum MacKellar lives in Edinburgh, UK. He is the Director of Research of the Scottish Council on Human Bioethics and a visiting lecturer in Bioethics at St Mary’s University in Twickenham, London.
Notes
1 The actual number of eggs retrieved from each individual varies greatly depending on factors such as age, lifestyle, medical conditions, etc. (Diaz-Garcia Citation2023).
2 The first version of this Act was enacted in 1990, and it was then revised in 2008.
3 https://www.hfea.gov.uk/about-us/publications/research-and-data/ (accessed 9 May 2024)
4 See Fuscaldo (Citation2005, p. 116), McMahon et al. (Citation2000), and de Lacey (Citation2005). Moreover, it is likely that very few individuals would generate embryos for the specific purpose of donation to other patients.
5 David Alton, quoted in Doughty, Steve; ‘1.7 million embryos created for IVF have been thrown away, and just 7 per cent lead to pregnancy’, Daily Mail, 31st December 2012.
6 The proposals in this section only represent possible ways in which the problem might be solved, and the authors do not officially endorse any of them. Each of the proposals may or may not create new ethical concerns which would need to be addressed further.
7 Richard Kennedy, quoted in Templeton, Sarah-Kate; ‘Spare embryos “should be donated to infertile couples”’, The Sunday Herald, 21st September 2003.
8 Ian Craft, quoted in the Sarah-Kate Templeton article (see footnote 1).
9 It is possible to take the pronuclei out of the fertilized egg and put them, or other pronuclei from another couple, back in.
10 However, it should be noted that the cell produced by sperm-egg fusion can no longer be considered an ‘egg’ in any meaningful sense. The process of producing a zygote cannot be ‘reversed’ (meiosis II has been completed and a number of other irreversible changes have taken place) but it can be disrupted by removing the pronuclei, leaving a cellular cytoplasm that, while significantly different from that of an egg, is still sufficient to support development if new pronuclei are transplanted. Only when a true zygote is formed and cell division takes place is there no possibility of reversibility.
11 In this regard, it may be noted that in 2003 the HFEA indicated that there were 51,346 frozen embryos stored in the UK in March 1999. This figure increased to 97,719 in March 2001 and to 116, 252 by March 2003 (source: same as footnote 1).
References
- Abreu, C.W.D.P.A., et al., 2021. Final destination of surplus cryopreserved embryos: what decision should be made? JBRA assisted reproduction, 25 (2), 276–281. doi: 10.5935/1518-0557.20200085
- Bodri, D., et al., 2008. Complications related to ovarian stimulation and oocyte retrieval in 4052 oocyte donor cycles. Reproductive BioMedicine online, 17 (2), 237–243. doi: 10.1016/S1472-6483(10)60200-3
- Cao, Y.-X., et al., 2009. Comparison of survival and embryonic development in human oocytes cryopreserved by slow-freezing and vitrification. Fertility and sterility, 92 (4), 1306–1311. doi: 10.1016/j.fertnstert.2008.08.069
- Darlington, N., and Matson, P., 1999. The fate of cryopreserved human embryos approaching their legal limit of storage within a West Australian in-vitro fertilization clinic. Human reproduction, 14 (9), 2343–2344. doi: 10.1093/humrep/14.9.2343
- De Lacey, S., 2005. Parent identity and “virtual” children: why patients discard rather than donate unused embryos. Human reproduction, 20 (6), 1661–1669. doi: 10.1093/humrep/deh831
- De Lacey, S., 2007. Decisions for the fate of frozen embryos: fresh insights into patients’ thinking and their rationales for donating or discarding embryos. Human reproduction, 22 (6), 1751–1758. doi: 10.1093/humrep/dem056
- Delaunay, C., et al., 2023. (De)bonding with embryos: the emotional choreographies of Portuguese IVF patients. Social science & medicine [online], 321, Available from: https://doi.org/10.1016/j.socscimed.2023.115770.
- Diaz-Garcia, C. 2017. 7 Steps of IVF Process [online]. IVI UK. Available from: https://www.ivi.uk/blog/our-ivf-process-in-7-simple-steps/ [Accessed 16 Jan 2024].
- Diaz-Garcia, C. 2023. The average number of eggs retrieved during IVF [online]. IVI UK. Available from: https://www.ivi.uk/blog/average-number-eggs-retrieved-during-ivf/ [Accessed 16 Jan 2024].
- Fuscaldo, G. 2005. Genetic ties: are they morally binding? The University of Melbourne. Available from: https://onlinelibrary.wiley.com/doi/10.1111j.1467-8519.2006.00478.x [Accessed 16 Jan 2024].
- Fuscaldo, G., et al., 2007. How to facilitate decisions about surplus embryos: patients’ views. Human reproduction, 22 (12), 3129–3138. doi: 10.1093/humrep/dem325
- German Bundestag. 1990. Act for the Protection of Embryos 1990 (Germany). Available from: https://www.rki.de/SharedDocs/Gesetzestexte/Embryonenschutzgesetz_englisch.pdf?__blob=publicationFile.
- HFEA. 2019. Fertility treatment 2019: trends and figures. Human Fertilisation and Embryology Authority (HFEA). Available from: https://www.hfea.gov.uk/about-us/publications/research-and-data/fertility-treatment-2019-trends-and-figures/ [Accessed 18 Jan 2024].
- HFEA 2021. Fertility treatment 2021: preliminary trends and figures. Human Fertilisation and Embryology Authority (HFEA). Available from: https://www.hfea.gov.uk/about-us/publications/research-and-data/fertility-treatment-2021-preliminary-trends-and-figures/ [Accessed 18 Jan 2024].
- Kliebisch, T.K., et al., 2016. The German middleway as precursor for single embryo transfer: a retrospective data-analysis of the Düsseldorf University Hospital's Interdisciplinary Fertility Centre – UniKiD. Geburtshilfe und Frauenheilkunde, 76 (6), 690–698. doi: 10.1055/s-0042-105747
- Kvernflaten, B., et al., 2022. Kin or research material? Exploring IVF couples’ perceptions about the human embryo and implications for disposition decisions in Norway. Journal of bioethical inquiry, 19 (4), 571–585. doi: 10.1007/s11673-022-10214-7
- Leone, S., 2008. The pre-zygote identity as a moral issue. Human reproduction & genetic ethics, 14 (1), 15–21. doi: 10.1558/hrge.v14i1.15
- MacCallum, F., and Widdows, H., 2012. Ethical issues in embryo donation. In: G. Pennings, J.B. Appleby, and M. Richards, eds. Reproductive donation: practice, policy and bioethics. Cambridge: Cambridge University Press, 270–288.
- Maguire, A., 2021. An examination into the embryo disposal practices of human fertilization and embryology authority licenced fertility centers in the United Kingdom. Cambridge quarterly of healthcare ethics, 30 (1), 161–174. doi: 10.1017/S096318012000064X
- McMahon, C.A., et al., 2000. Mothers conceiving through In vitro fertilization: siblings, setbacks, and embryo dilemmas after five years. Reproductive technologies, 10 (3), 131–135.
- Mohler-Kuo, M., et al., 2009. Attitudes of couples towards the destination of surplus embryos: results among couples with cryopreserved embryos in Switzerland. Human reproduction, 24 (8), 1930–1938. doi: 10.1093/humrep/dep103
- Nachtigall, R.D., et al., 2005. Parents’ conceptualization of their frozen embryos complicates the disposition decision. Fertility and sterility, 84 (2), 431–434. doi: 10.1016/j.fertnstert.2005.01.134
- Nachtigall, R.D., et al., 2009. How couples who have undergone In vitro fertilization decide what to Do with surplus frozen embryos. Fertility and sterility, 92 (6), 2094–2096. doi: 10.1016/j.fertnstert.2009.06.027
- Newton, C.R., et al., 2003. Embryo donation: attitudes toward donation procedures and factors predicting willingness to donate. Human reproduction, 18 (4), 878–884. doi: 10.1093/humrep/deg169
- Rezazadeh Valojerdi, M., et al., 2009. Vitrification versus slow freezing gives excellent survival, post warming embryo morphology and pregnancy outcomes for human cleaved embryos. Journal of assisted reproduction and genetics, 26 (6), 347–354. doi: 10.1007/s10815-009-9318-6
- Simopoulou, M., et al., 2019. Discarding IVF embryos: reporting on global practices. Journal of assisted reproduction and genetics, 36 (12), 2447–2457. doi: 10.1007/s10815-019-01592-w
- Takahashi, S., et al., 2012. The decision-making process for the fate of frozen embryos by Japanese infertile women: a qualitative study. BMC medical ethics, 13 (1), 9. doi: 10.1186/1472-6939-13-9
- Takahashi, K., and Yamanaka, S., 2006. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell, 126 (4), 663–676. doi: 10.1016/j.cell.2006.07.024
- Thomson, J.A., et al., 1998. Embryonic stem cell lines derived from human blastocysts. Science, 282 (5391), 1145–1147. doi: 10.1126/science.282.5391.1145
- Tonkens, R., 2016. The moral unacceptability of abandoning human embryos. Monash bioethics review, 34 (1), 52–69. doi: 10.1007/s40592-016-0060-4
- UK Parliament. 2022. Health and care act 2022 (UK). Available from: https://www.legislation.gov.uk/ukpga/2022/31/contents [Accessed 4 Jan 2024].
- Van Den Bergh, M., et al., 1995. Second polar body extrusion is highly predictive for oocyte fertilization as soon as 3 hr after intracytoplasmic sperm injection (ICSI). Journal of assisted reproduction and genetics, 12 (4), 258–262. doi: 10.1007/BF02212928
- Warnock, M. 1984. Report of the committee of inquiry into human fertilisation and embryology. Great Britain Committee of Inquiry into Human Fertilisation and Embryology, ed. London: H.M.S.O (9314).
