
ABSTRACT
Introduction
The European Association of Urology guidelines recommend offering kidney-sparing surgery (KSS) as a primary treatment option to patients with low-risk tumours. Cystoscopy, urinary cytology, and computed tomography urography (CTU) do not always allow correct disease staging and grading, and sometimes there is even a lack of certainty regarding the diagnosis of UTUC. Diagnostic ureteroscopy (d-URS) may therefore be of crucial importance within the diagnostic framework and fundamental in establishing the appropriate therapeutic approach.
Evidence acquisition and synthesis
A systematic review of the literature was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Risk of bias was assessed using Risk of Bias in Non-randomized Studies of interventions (ROBINS-I). Overall, from 3791 identified records, 186 full-text articles were assessed for eligibility. Finally, after a quantitative review of the selected literature, with the full agreement of all authors, 62 studies were considered relevant for this review.
Results
CTU has a sensitivity and specificity for UTUC of 92% and 95% respectively, but is not able to detect small or flat lesions with adequate accuracy. The sensitivity of voided urinary cytology for UTUC is around 67–76% and ranges from 43% to 78% for selective ureteric urine collection. As no technique offers a diagnosis of certainty, d-URS can allow an increase in diagnostic accuracy. In the present review the pros and cons of d-URS were analysed. This technique may provide additional information in the selection of patients suitable for neoadjuvant chemotherapy or KSS, distinguishing between normal tissue and low- and high-grade UTUC thanks to the emerging technologies.
Conclusions
Information obtainable from d-URS and ureteroscopic-guided biopsy can prove extremely valuable when the diagnosis of UTUC is doubtful or KSS is being considered. Notwithstanding concerns remain regarding the potential risk of bladder recurrence, cancer dissemination, and/or delay in radical treatment.
Abbreviations: CLE: confocal laser endomicroscopy; CSS: cancer-specific survival; CTU: CT urography; d-URS: diagnostic ureteroscopy; EAU: European Association of Urology; HR: hazard ratio; IMAGE1S: Storz professional imaging enhancement system; IVR: intravesical recurrence; KSS: kidney-sparing surgery; MFS: Metastasis-free survival; NAC: neoadjuvant chemotherapy; NBI: narrow-band imaging; OCT: optical coherence tomography; RFS: Recurrence-free survival; RNU: radical nephroureterectomy; ROBINS-I: Risk of Bias in Non-randomized Studies of interventions; URS(-GB): Ureteroscopy(-guided biopsy); UTUC: upper tract urothelial carcinoma; UUT: upper urinary tract
Introduction
Upper tract urothelial carcinoma (UTUC) accounts for 5–10% of urothelial carcinomas [Citation1]. To date, radical nephroureterectomy (RNU) with bladder cuff excision still represents the ‘gold standard’ treatment for UTUC. Nevertheless, the European Association of Urology (EAU) guidelines recommend offering kidney-sparing surgery (KSS) as a primary treatment option to patients with low-risk tumours [Citation1,Citation2]. The availability of preoperative predictive tools that yield reliable information on tumour location, size, stage, and grade and any tumour-associated conditions is of fundamental importance in guiding the selection of candidates for such treatment. The EAU guidelines make a Grade-A recommendation for the performance of cystoscopy, urinary cytology, and CT urography (CTU) in the diagnostic evaluation of UTUC. They also advise that diagnostic ureteroscopy (d-URS) and biopsy should be performed in cases in which additional information may have an impact on treatment decisions [Citation1]. In our opinion d-URS represents an extremely useful tool that guarantees the possibility of carrying out a visual study of the conditions of the upper urinary tract (UUT). This means, for instance, identifying the actual number and size of the lesions. It also represents an irreplaceable tool to seek for and possibly biopsy flat lesions not identifiable on the CTU. The possibility of studying the UUT endoscopically is also of fundamental importance to design or evaluate the feasibility of a conservative approach, especially in those conditions in which the lesion is difficult to reach or localise (i.e. lower calyx). Imaging and optical diagnostic techniques and new devices for performing biopsies represent an extraordinary tool for increasing diagnostic accuracy.
However, the procedure is challenging so that not always achieving optimal results. It is then necessary to carry out a risk stratification of patients to reduce costs, complications, and potential risk of bladder recurrence, cancer dissemination, or delay in radical treatment.
A systematic review of the literature was performed with the aim of taking stock of the current knowledge of the strengths and weaknesses of d-URS in UTUC.
Evidence acquisition and synthesis
A comprehensive literature search was performed in May 2020 using the PubMed/MEDLINE database using the following terms: ‘upper tract urothelial carcinoma’ OR ‘UTUC’ OR ‘upper urinary tract’ AND ‘biopsy’ OR ‘bladder recurrence’ OR ‘complications’ OR ‘delay’ OR ‘diagnosis’ OR ‘diagnostic ureteroscopy’ OR ‘confocal laser endomicroscopy’ OR ‘grade’ OR ‘IMAGE1S’ OR ‘imaging’ OR ‘narrow-band imaging’ OR ‘neoadjuvant chemotherapy’ OR ‘optical coherence tomography’ OR ‘stage’.
Publications were filtered for English language and full-text availability and included original articles, clinical trials, case reports, meta-analyses, professional society guidelines, and reviews. Letters to the editor, replies, textbooks, and contributions written in languages other than English were excluded from our research. No filters were applied for the publication date.
Eligible articles were screened according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) criteria [Citation3] ().
Figure 1. PRISMA diagram for study selection
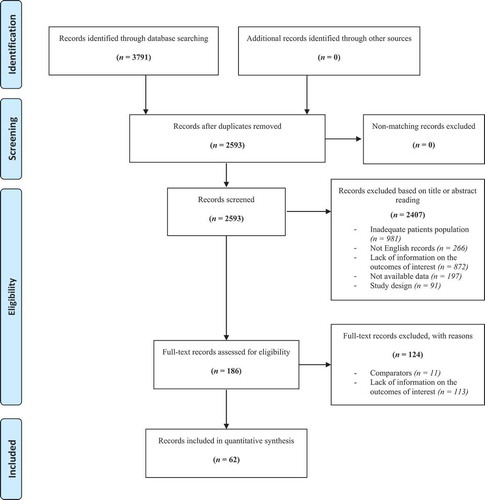
Studies were not excluded a priori based on quality reporting assessment. Because only non-randomised studies were retrieved, we adopted the Risk of Bias in Non-randomized Studies of interventions (ROBINS-I) tool to assess the risk of bias in the included studies for the following domains: confounding bias, selection of participants bias, bias in classification of interventions, bias due to deviation from intended interventions, bias due to missing data, the bias in the measurement of outcomes and bias in the selection of the reported results [Citation4]. We used the ROBINS-I tool to evaluate the risk of bias among the studies included as one of the four levels (low, moderate, serious and critical). The results of our risk of bias assessment for all individual studies are shown in [7,19–21,25–27,30,32–36,38–40,42,43,46–48,55–58,62,63]. The most problematic domains involved uncontrolled, single-arm studies, small sample sizes, outcomes measurement, and confounding.
Table 1. Risk of bias assessment using ROBINS-I
The reported studies had moderate, serious, or critical risk of bias. When using the ROBINS-I assessment, it is recommended to exclude studies with a high-risk of bias from analyses. Nevertheless, considering the rarity of the disease and the various technical details regarding diagnosis and therapy analysed, despite the overall high risk of bias, all the studies have been retained for the purposes of the present review. Moreover, we performed many subgroup analyses to investigate so that it could be a source of further heterogeneity.
Overall, from 3791 identified records, 186 full-text original articles were assessed for eligibility. Finally, 62 records were considered relevant for the present review.
Results
The findings reported in the present review relate to the pros of d-URS, such as histological characterisation of UTUC in select patients eligible for endoscopic treatment and/or neoadjuvant chemotherapy (NAC). The cons of d-URS, i.e. complications, inconclusive diagnosis, risk of cancer dissemination and bladder recurrence, and potential delay in treatment could also affect the prognosis.
Pros
Histopathological confirmation of disease
CTU has the highest diagnostic accuracy among the available imaging techniques, with a sensitivity and specificity of 92% and 95%, respectively [Citation5]. However, CTU may not be able to reliably estimate the actual three-dimensional extension of the disease or to detect small or flat lesions with adequate accuracy, especially in the case of ureteric localisation [Citation6], thus potentially leading to misclassification and undertreatment [Citation7]. The sensitivity of voided urinary cytology for UTUC is around 67–76% and ranges from 43% to 78% for selective ureteric urine collection, being higher for high-grade UTUC [Citation8,Citation9]. Barbotage cytology detects up to 91% of cancers, being as effective as biopsy histology [Citation10].
A d-URS allows exploration of the UUT and is crucial when diagnostic uncertainty exists and in patients who can benefit from KSS [Citation1,Citation11]. A d-URS has the advantage to offer a direct view of the tumour for biopsy and to facilitate selective ureteric sampling for cytology in situ [Citation1,Citation11]. Indeed, in situ collection of urine through the barbotage technique has proven to be sensitive if correctly executed, with better diagnostic performance than that of voided urine cytology [Citation12]. It also enables clarification of the nature of non-specific CTU findings, such as wall thickening, and to re-classify suspicious lesions as benign [Citation13].
Grahn et al. [Citation14] compared the performance of CTU and visual assessment during d-URS in 148 patients with suspected UTUC. The d-URS showed a similar sensitivity (89% vs 84%; P = 0.36), but greater specificity (51% vs 85%; P < 0.001) and accuracy (74% vs 84%; P = 0.04) than CTU.
Gallioli et al. [Citation7] found that, among patients with positive CTU and d-URS, the lesions differed in dimensions, number or site in 45/107 (42.1%) cases.
Grading, staging, and biopsy for histopathology
Ureteroscopic-guided biopsy (URS-GB) correctly determines tumour grade in most cases, but stage assessment using URS-GB is notoriously difficult.
Subiela et al. [Citation15] conducted a systematic review and meta-analysis including 23 studies on the diagnostic accuracy of URS-GB in predicting stage and grade at final pathology. The authors reported a grade concordance between URS-GB and final pathology of 66% (95% CI 55–77%) for low-grade tumours and 97% (95% CI 94–98%) for high-grade tumours. They also found that identification of high-grade and subepithelial invasion at URS-GB had a moderate (positive predictive value [PPV] 60%, 95% CI 54–66%) and strong correlation (PPV 94%, 95% CI 84–100%) with invasive UTUC at final pathology, respectively. Notwithstanding, undergrading and understaging rates at prior URS-GB compared with final pathology were found in 32% (95% CI 25–38%) and 46% (95% CI 38–54%) of cases, respectively.
It is evident that, to date, the accuracy of URS-GB has been limited by several factors, including insufficient tissue quality and crush artefacts; even if there is no unanimity over whether low biopsy volume in URS-GB affects tumour biopsy grading. Some authors try to overcome these limitations by describing detailed methods for URS inspection and URS-GB, while others have sought to find the best device to obtain an adequate biopsy sample.
In 1997, Tawfiek et al. [Citation16] described in detail their technique to inspect the UUT and perform URS-GB for handling and processing the samples. In a series of 45 patients, Guarnizo et al. [Citation17] proposed a multi-biopsy approach that was able to achieve a diagnostically accurate diagnosis of UTUC in 89% of cases.
Golan et al. [Citation18] proposed a technique to achieve maximal tissue preservation in which the specimen was mounted on filter paper prior to embedding in paraffin.
With the current diagnostic devices, an ideal method to procure adequate tissue sampling is still missing. Basket and 3-F cup biopsy forceps represent the two most commonly used biopsy tools [Citation19]. Basket devices can be front loaded and allow the ensnarement of a piece or even the whole specimen from its base. Thanks to their flexibility they are also more likely to reach those lesions localised in calyces that require considerable deflection of the instrument. Conversely, flat lesions could not be sampled with this tool. Larger diameter forceps can capture large specimens and also flat lesions, but they need to be introduced in the ureteroscope by backloading as the tip of the device is not compatible with the diameter of the working channel. Unfortunately, they bestow stiffness to the flexible ureteroscope, so that sampling of lesions could be impossible if deflection is needed. Furthermore, they require the use of a double lumen ureteroscope or the placement of ureteric access sheath to allow the insertion of the ureteroscope because of the consequent lack of irrigation fluid [Citation20,Citation21] ( [19–21]).
Table 2. Overview of biopsy devices during operative ureteroscopies used in UTUC in the included studies
Kleinmann et al. [Citation19] evaluated the pathological result obtained in 504 URS-GB performed for suspicion of UTUC. The 2.4-F basket device proved to be superior to the 3-F cup forceps for disease confirmation (94% vs 63%, respectively; P < 0.001) and correct assessment of grade (93% vs 80%, respectively; P < 0.033).
Breda et al. [Citation20] found BIGopsy forceps and the 2.2-F nitinol basket to be superior to 3-F forceps in obtaining an adequate specimen for the pathology examination of UTUC. In addition, for papillary lesions, the basket biopsy provided larger specimens in comparison to the other biopsy devices, while for flat or sessile lesions, the BIGopsy forceps provided larger, deeper, and less distorted specimens than the 3-F forceps.
In a multi-institutional retrospective study on 145 patients, Lama et al. [Citation21] evaluated URS-GB using backloaded cup forceps, a nitinol basket, or standard cup forceps. The ability to distinguish low- and high-grade UTUC prior to RNU was statistically higher using the backloaded cup forceps (P = 0.02). The authors also reported that, compared with the standard cup forceps, the backloaded cup forceps showed a significantly higher subjective score for biopsy quality (P = 0.01), quality of basement membrane thickness (P = 0.02), and role of biopsy size in accurate diagnosis (P = 0.04). However, no subjective differences were noticed between the backloaded cup forceps and nitinol basket biopsies.
Case selection for conservative endoscopic treatment
The main factors that correlate with the oncological outcomes of URS treatment are pathological grade, tumour size, and tumour focality [Citation2], although recent studies suggest that tumour burden plays a secondary role [Citation22,Citation23]. Therefore, risk stratification based on these factors is essential to limit the risk of under- and overtreatment, with current guidelines recommending elective conservative treatment only in the case of small (<2 cm), unifocal, low-grade disease [Citation24]. In this context, endoscopic exploration of the UUT plays a key role in selecting those patients who are fit for KSS of UTUC, together with urinary cytology and cross-sectional imaging. Golan et al. [Citation25], in their retrospective study on 116 patients who underwent d-URS for suspected UTUC on CTU, found that RNU was spared in 42% of cases, without reporting disease progression in any of those cases. Tsivian et al. [Citation26] found a lower rate of RNU (89% vs 69%; P = 0.01) and misdiagnosis (15.5% vs 2.1%; P = 0.02) in patients evaluated with routine d-URS. Gallioli et al. [Citation7] reported a change in the indication of elective treatment after d-URS in 37/76 (48.1%) cases ( [7,25,26]).
Table 3. Summary of published studies focussed on case selection for conservative endoscopic treatment
Given its ability to consistently evaluate tumour dimension, focality, and growth pattern through direct visualisation, and to yield tumour grading via histopathology and in situ cytology, URS represents an essential tool for risk stratification and case selection for conservative endoscopic treatment.
Case selection for neoadjuvant chemotherapy
Several retrospective studies have shown the promising role of NAC in the treatment of high-risk locally advanced UTUC in comparison to RNU alone [Citation24]. It must always be borne in mind that deterioration in renal function following RNU may render a patient ineligible for further cisplatin-based combination chemotherapy in 49% of cases [Citation27], strengthening the role of NAC as opposed to adjuvant chemotherapy. However, the criteria for candidate selection remain unclear, although they commonly include high-grade pathology or locally advanced disease (cT2–T4N0M0) [Citation28].
In this setting, URS can provide histopathological diagnosis, confirm the urothelial nature of the disease, and yield information about its grade, which has been shown to correlate with a higher stage and worse outcomes [Citation29]. Furthermore, it helps candidate selection by detecting the presence of high-risk features such as high-grade tumour sessile growth patterns or large tumour burdens [Citation30].
In the challenge to select those patients who will respond to NAC, the retrieval of a biopsy specimen could in the future provide a molecular fingerprint of the disease. It could also provide information regarding DNA repair genes, expression of tyrosine kinase receptors, immune checkpoint inhibitors molecular targets and regulation of apoptosis; this would allow the medical oncologist to select the best NAC or immunotherapy for patients in a truly tailored approach [Citation31]. [27,30,31] summarises the results of NAC for UTUC based on the included studies.
Table 4. Results of NAC for UTUC in the included studies
New diagnostic technologies to increase diagnostic accuracy
Various new techniques have been developed to enhance diagnostic accuracy and risk stratification, including narrow-band imaging (NBI), the Storz professional imaging enhancement system (IMAGE1S), optical coherence tomography (OCT), and confocal laser endomicroscopy (CLE) ( [32–36]).
Table 5. Overview of optical/imaging techniques used during URS inspecting the UUT
Traxer et al. [Citation32] reported a 22.7% increase in the tumour detection rate in the UUT when using NBI compared with white light. Emiliani et al. [Citation33] reported CLARA and CLARA+CHROMA to offer better quality compared with white light and other IMAGE1S modalities.
OCT might enhance the staging accuracy of d-URS. Bus et al. [Citation34] reported concordance of lesion staging with OCT and final histopathology in 83% of cases.
CLE provides real-time in vivo microscopy of tissue, allowing the distinction between benign tissue and UTUC [Citation35]. Breda et al. [Citation36] reported concordance between CLE images and final histopathological results in 100% and 83% of cases of high- and low-grade UTUC, respectively, and in one out of one case of carcinoma in situ.
Cons
Risk of complications
During URS, lesions of the UUT can occur, ranging from mucosal abrasion to false passage, perforation and fluid extravasation, intussusception, and ureteric avulsion [Citation37]. Bleeding is usually self-limited; nevertheless, life-threatening haemorrhagic complications and perirenal haematoma formation have been published as a result of forniceal or renal parenchyma rupture [Citation38].
Among the early postoperative complications, UTI has been reported in 1–2.6% of cases, with severe sepsis in 0.06–0.3% [Citation39,Citation40], the latter probably linked to the development of high intrarenal pressures during the procedure [Citation41]. Local oedema, ureteric spasm, or blood clot can lead to acute obstruction of the UUT and renal colic. VUR may occur after URS, but the use of small-calibre flexible and semi-rigid ureteroscopes has obviated ureteric dilatation in most cases and has likely reduced the incidence of reflux overall [Citation37].
Ureteric strictures can occur as a late postoperative complication subsequent to ureteric lesions. Although the incidence of strictures has been reported to be <1% [Citation39,Citation40], the use of post-ureteroscopic lesion scores has revealed the incidence to be considerably higher [Citation42,Citation43] ( [38–40,42,43]).
Table 6. Intra- and postoperative complications rate reported in the studies included in our review during operative URS
Cancer dissemination
The potential role of URS in cancer dissemination was initially explored by Kulp et al. [Citation44] in 1994, who reported on a series of 13 patients who underwent URS prior to RNU. In the surgical specimens, no tumour cells were noted in vascular or lymphatic spaces. Conversely, Lim et al. [Citation45] described a case of suspicious lymphatic invasion that the authors attributed to high intrarenal pressures during URS.
Comparing patients with and without d-URS, Hendin et al. [Citation46] found no significant differences in overall 5-year survival (87% vs 76%,) or metastasis-free survival (MFS) (67% vs 71%). Ishikawa et al. [Citation47], in a multi-institutional study of 208 patients, found the 5-year cancer-specific survival (CSS) to be comparable in the d-URS and control groups (88.3% vs 78.1%). Gurbuz et al. [Citation48] explored the recurrence-free survival (RFS) of patients with and without d-URS prior to RNU and found comparable results at 5-year follow-up (72% vs 69%; P = 0.17).
Guo et al. [Citation49] published a meta-analysis that confirmed the above findings. Despite the paucity of data and the retrospective design of all the eight studies included, the authors concluded from that meta-analysis that URS is not associated with overall survival, MFS, or RFS. [46–48] summarises the results of the studies concerning cancer dissemination included in the review.
Table 7. Summary of included studies analysing cancer dissemination
Bladder recurrence
In recent years, the risk of intravesical recurrence (IVR) after URS prior to RNU has been addressed. The hypothesis is that the manipulation of the ureteroscope and the irrigation back-flow may increase the risk of or seeding [Citation45]. Audenet et al. [Citation50] showed that the majority of bladder tumours following RNU are clonally related, supporting the hypothesis that IVR is caused by neoplastic cell implantation rather than being a second primary tumour.
Two meta-analyses have summarised the current evidence. Marchioni et al. [Citation51] found an IVR rate of 39.2–60.7% and 16.7–46% in patients with and without URS prior to RNU, respectively. The pooled analysis found a significant association between URS and IVR (hazard ratio [HR] 1.56; P < 0.001). Guo et al. [Citation49] similarly found that IVR rates were lower in patients without a history of bladder cancer who underwent URS (HR 1.81). The main limitations of these two meta-analyses are the retrospective design of all the included studies, the lack of data about the URS, and the bladder cuff management technique [Citation52] with no postoperative administration of mitomycin C [Citation53].
Conversely, Ishikawa et al. [Citation47] found that IVR at 2-year follow-up was comparable (60% vs 58.7%) in patients who underwent URS prior to RNU and controls. Similar results were reported by Lee et al. [Citation54].
Sung et al. [Citation55] found that the interval between URS and RNU does not seem to affect the IVR rate, while Lee et al. [Citation56], reported that patients who underwent URS and RNU in a single session had an IVR comparable to that in a non-URS group.
Yoo et al. [Citation57] found the IVR rate to be significantly higher in patients with renal pelvic (but not ureteric) tumours who underwent URS-GB prior to RNU (60.4%; HR 2.06; P = 0.01). A possible explanation is that the endoscopic manipulation could have increased the shedding of cancer cells from the renal pelvis into the bladder. [47,55–58] summarises the results of bladder recurrence for UTUC based on the included studies.
Table 8. Overview of IVR after URS prior to RNU in the included studies
Delay in radical treatment
One of the main criticisms regarding the systematic implementation of URS for UTUC is that it may lead to a delay in radical surgical treatment. It has been shown that a delay in bladder cancer treatment is associated with a higher pathological stage, and the window of time between diagnosis and cystectomy should not exceed 12 weeks [Citation58]. This threshold does not apply to UTUC [Citation59,Citation60]. Nison et al. [Citation61] reported on a significant delay in surgical treatment following URS (median 79.5 days) compared with a non-URS group (median 44.5 days; P = 0.04). However, the 5-year CSS, MFS, and RFS were comparable between the groups. Boorjian et al. [Citation62] retrospectively compared the results in 121 patients who underwent RNU without URS (n = 34), with URS-GB (n = 75), or with URS + laser ablation (n = 12). They found no significant difference in postoperative disease status between the three groups.
Gurbuz et al. [Citation48], in a multi-institutional retrospective study, confirmed that endoscopic ablation prior to RNU is not associated with poorer CSS and disease-free survival. The study demonstrated patient selection for laser ablation to be the key in guaranteeing good oncological outcomes even after endoscopic management failure. [48,62–63] summarises the results of the studies concerning delay in radical treatment included in the review.
Table 9. Overview of delay in radical treatment and reported outcomes
Conclusions
A d-URS is an extremely valuable tool in cases of suspected UTUC, especially when the diagnosis is equivocal or when KSS can be considered. Although nowadays URS can be considered a safe procedure, it is not without risks, some of which can endanger the patient’s life. Risks can be related to the presence of neoplastic disease, which translates into the potential risk of bladder recurrence, cancer dissemination, and/or delays in radical treatment. Some technical devices or precautions can aid in obtaining correct information, above all concerning the grade of the disease. The latest techniques such as NBI, IMAGE1S, CLE, and OCT can also provide information of value in optimising patient selection for KSS. NAC could represent an ‘ace up our sleeve’, but accurate staging and grading remain crucial for appropriate therapeutic decision making, and d-URS can be of decisive importance for this purpose.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Rouprêt M, Babjuk M, Compérat E, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2017 Update. Eur Urol. 2018;73(1):111–122.
- Seisen T, Peyronnet B, Dominguez-Escrig JL, et al. Oncologic Outcomes of Kidney-sparing Surgery Versus Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: a Systematic Review by the EAU Non-muscle Invasive Bladder Cancer Guidelines Panel. Eur Urol. 2016;70(6):1052–1068.
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: explanation and Elaboration. PLOS Med. 2009;6(7):e1000100.
- Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
- Janisch F, Shariat SF, Baltzer P, et al. Diagnostic performance of multidetector computed tomographic (MDCTU) in upper tract urothelial carcinoma (UTUC): a systematic review and meta-analysis. World J Urol. 2020;38(5):1165–1175.
- Wang LJ, Wong YC, Ng KF, et al. Tumor Characteristics of Urothelial Carcinoma on Multidetector Computerized Tomography Urography. J Urol. 2010;183(6):2154–2160.
- Gallioli A, Territo A, Mercadé A, et al. The impact of ureteroscopy following computed tomography urography in the management of upper tract urothelial carcinoma. J Urol. 2020;205(2):392–399.
- Williams SK, Denton KJ, Minervini A, et al. Correlation of upper-tract cytology, retrograde pyelography, ureteroscopic appearance, and ureteroscopic biopsy with histologic examination of upper-tract transitional cell carcinoma. J Endourol. 2008;22(1):71–76.
- Mandalapu RS, Remzi M, de Reijke TM, et al. Update of the ICUD-SIU consultation on upper tract urothelial carcinoma 2016: treatment of low-risk upper tract urothelial carcinoma. World J Urol. 2017;35(3):355–365.
- Malm C, Grahn A, Jaremko G, et al. Diagnostic accuracy of upper tract urothelial carcinoma: how samples are collected matters. Scand J Urol. 2017;51(2):137–145.
- Clements T, Messer JC, Terrell JD, et al. High-grade ureteroscopic biopsy is associated with advanced pathology of upper-tract urothelial carcinoma tumors at definitive surgical resection. J Endourol. 2012;26(4):398–402.
- Messer J, Shariat SF, Brien JC, et al. Urinary cytology has a poor performance for predicting invasive or high-grade upper-tract urothelial carcinoma. BJU Int. 2011;108(5):701–705.
- Türkvatan A, Erden A, Ölçer T, et al. Hypertrophic renal papillae mimicking urothelial tumor. Eur J Radiol Extra. 2009;69(3):e121–e123.
- Grahn A, Melle-Hannah M, Malm C, et al. Diagnostic accuracy of computed tomography urography and visual assessment during ureterorenoscopy in upper tract urothelial carcinoma. BJU Int. 2017;119(2):289–297.
- Subiela JD, Territo A, Mercadé A, et al. Diagnostic accuracy of ureteroscopic biopsy in predicting stage and grade at final pathology in upper tract urothelial carcinoma: systematic review and meta-analysis. Eur J Surg Oncol. 2020;46(11):1989–1997.
- Tawfiek E, Bibbo M, Bagley DH. Ureteroscopic biopsy: technique and specimen preparation. Urology. 1997;50(1):117–119.
- Guarnizo E, Pavlovich CP, Seiba M, et al. Ureteroscopic biopsy of upper tract urothelial carcinoma: improved diagnostic accuracy and histopathological considerations using a multi-biopsy approach. J Urol. 2000;163(1):52–55.
- Golan S, Gerber G, Margel D, et al. A novel technique to improve the processing of minute ureteroscopic biopsies. Pathol Oncol Res. 2018;24(1):89–94.
- Kleinmann N, Healy KA, Hubosky SG, et al. Ureteroscopic biopsy of upper tract urothelial carcinoma: comparison of basket and forceps. J Endourol. 2013;27(12):1450–1454.
- Breda A, Territo A, Sanguedolce F, et al. Comparison of biopsy devices in upper tract urothelial carcinoma. World J Urol. 2019;37(9):1899–1905.
- Lama DJ, Safiullah S, Patel RM, et al. Multi-institutional evaluation of upper urinary tract biopsy using backloaded cup biopsy forceps, a nitinol basket, and standard cup biopsy forceps. Urology. 2018;117:89–94.
- Villa L, Haddad M, Capitanio U, et al. Which patients with upper tract urothelial carcinoma can be safely treated with flexible ureteroscopy with holmium:YAG laser photoablation? Long-term results from a high volume institution. J Urol. 2018;199(1):66–73.
- Scotland KB, Kleinmann N, Cason D, et al. Ureteroscopic management of large ≥2 cm upper tract urothelial carcinoma: a comprehensive 23-year experience. Urology. 2018;121:66–73.
- Rouprêt M, Babjuk M, Burger M, et al. EAU Guidelines on Upper Urinary Tract Urothelial Carcinoma. 2020; presented at the 35th EAU Annual Congress, Amsterdam. Available at: https://uroweb.org/guideline/upper-urinary-tract-urothelial-cell-carcinoma.
- Golan S, Nadu A, Lifshitz D. The role of diagnostic ureteroscopy in the era of computed tomography urography. BMC Urol. 2015;15(1):74.
- Tsivian A, Tsivian M, Stanevsky Y, et al. Routine diagnostic ureteroscopy for suspected upper tract transitional-cell carcinoma. J Endourol. 2014;28(8):922–925.
- Lane BR, Smith AK, Larson BT, et al. Chronic kidney disease after nephroureterectomy for upper tract urothelial carcinoma and implications for the administration of perioperative chemotherapy. Cancer. 2010;116(12):2967–2973.
- Martini A, Daza J, Poltiyelova E, et al. Pathological downstaging as a novel endpoint for the development of neoadjuvant chemotherapy for upper tract urothelial carcinoma. BJU Int. 2019;124(4):665–671.
- Brien JC, Shariat SF, Herman MP, et al. Preoperative hydronephrosis, ureteroscopic biopsy grade and urinary cytology can improve prediction of advanced upper tract urothelial carcinoma. J Urol. 2010;184(1):69–73.
- Porten S, Siefker-Radtke AO, Xiao L, et al. Neoadjuvant chemotherapy improves survival of patients with upper tract urothelial carcinoma. Cancer. 2014;120(12):1794–1799.
- Tse J, Ghandour R, Singla N, et al. Molecular predictors of complete response following neoadjuvant chemotherapy in urothelial carcinoma of the bladder and upper tracts. Int J Mol Sci. 2019 Feb ;13(20):793.
- Traxer O, Geavlete B, de Medina SG, et al. Narrow-band imaging digital flexible ureteroscopy in detection of upper urinary tract transitional-cell carcinoma: initial experience. J Endourol. 2011 Jan;25(1):19–23.
- Emiliani E, Talso M, Baghdadi M, et al. Evaluation of the Spies TM modalities image quality. Int Braz J Urol. 2017;43(3):476–480.
- Bus MT, de Bruin DM, Faber DJ, et al. Optical coherence tomography as a tool for in vivo staging and grading of upper urinary tract urothelial carcinoma: a study of diagnostic accuracy. J Urol. 2016;196(6):1749–1755. .
- Bui D, Mach KE, Zlatev DV, et al. A Pilot Study of In Vivo Confocal Laser Endomicroscopy of Upper Tract Urothelial Carcinoma. J Endourol. 2015 Dec;29(12):1418–1423.
- Breda A, Territo A, Guttilla A, et al. Correlation between confocal laser endomicroscopy (Cellvizio ®) and histological grading of upper tract urothelial carcinoma: a step forward for a better selection of patients suitable for conservative management. Eur Urol Focus. 2018;4(6):954–959.
- Johnson DB, Pearle MS. Complications of ureteroscopy. Urol Clin North Am. 2004;31(1):157–171.
- Whitehurst LA, Somani BK. Perirenal hematoma after ureteroscopy: a systematic review. J Endourol. 2017;31(5):438–445.
- Somani BK, Giusti G, Sun Y, et al. Complications associated with ureterorenoscopy (URS) related to treatment of urolithiasis: the Clinical Research Office of Endourological Society URS Global Study. World J Urol. 2017;35(4):675–681.
- Baş O, Tuygun C, Dede O, et al. Factors affecting complication rates of retrograde flexible ureterorenoscopy: analysis of 1571 procedures-a single-center experience. World J Urol. 2017;35(5):819–826.
- Osther PJ, Pedersen KV, Lildal SK, et al. Pathophysiological aspects of ureterorenoscopic management of upper urinary tract calculi. Curr Opin Urol. 2016;26(1):63–69.
- Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol. 2013;189(2):580–584.
- Schoenthaler M, Buchholz N, Farin E, et al. The Post-Ureteroscopic Lesion Scale (PULS): a multicenter video-based evaluation of inter-rater reliability. World J Urol. 2014;32(4):1033–1040.
- Kulp DA, Bagley DH. Does Flexible ureteropyeloscopy promote local recurrence of transitional cell carcinoma? J Endourol. 1994;8(2):111–113.
- Lim DJ, Shattuck MC, Cook WA. Pyelovenous lymphatic migration of transitional cell carcinoma following flexible ureterorenoscopy. J Urol. 1993;149(1):109–111.
- Hendin BN, Streem SB, Levin HS, et al. Impact of diagnostic ureteroscopy on long-term survival in patients with upper tract transitional cell carcinoma. J Urol. 1999;161(3):783–785.
- Ishikawa S, Abe T, Shinohara N, et al. Impact of diagnostic ureteroscopy on intravesical recurrence and survival in patients with urothelial carcinoma of the upper urinary tract. J Urol. 2010;184(3):883–887.
- Gurbuz C, Youssef RF, Shariat SF, et al. The impact of previous ureteroscopic tumor ablation on oncologic outcomes after radical nephrouretectomy for upper urinary tract urothelial carcinoma. J Endourol. 2011;25(5):775–779.
- Guo RQ, Hong P, Xiong GY, et al. Impact of ureteroscopy before radical nephroureterectomy for upper tract urothelial carcinomas on oncological outcomes: a meta-analysis. BJU Int. 2018;121(2):184–193.
- Audenet F, Isharwal S, Cha EK, et al. Clonal relatedness and mutational differences between upper tract and bladder urothelial carcinoma. Clin Cancer Res. 2019;25(3):967–976.
- Marchioni M, Primiceri G, Cindolo L, et al. Impact of diagnostic ureteroscopy on intravesical recurrence in patients undergoing radical nephroureterectomy for upper tract urothelial cancer: a systematic review and meta-analysis. BJU Int. 2017;120(3):313–319.
- Xylinas E, Rink M, Cha EK, et al. Impact of distal ureter management on oncologic outcomes following radical nephroureterectomy for upper tract urothelial carcinoma. Eur Urol. 2014;65(1):210–217.
- O’Brien T, Ray E, Singh R, et al. Prevention of bladder tumours after nephroureterectomy for primary upper urinary tract urothelial carcinoma: a prospective, multicentre, randomised clinical trial of a single postoperative intravesical dose of mitomycin C (The ODMIT-C Trial). Eur Urol. 2011;60(4):703–710.
- Lee HY, Yeh HC, Wu WJ, et al. The diagnostic ureteroscopy before radical nephroureterectomy in upper urinary tract urothelial carcinoma is not associated with higher intravesical recurrence. World J Surg Oncol. 2018;16(1):135.
- Sung HH, Jeon HG, Han DH, et al. Diagnostic ureterorenoscopy is associated with increased intravesical recurrence following radical nephroureterectomy in upper tract urothelial carcinoma. PLoS One. 2015;10(11):e0139976.
- Lee JK, Kim KB, Park YH, et al. correlation between the timing of diagnostic ureteroscopy and intravesical recurrence in upper tract urothelial cancer. Clin Genitourin Cancer. 2016;14(1):e37–e41.
- Yoo S, You D, Song C, et al. Risk of intravesical recurrence after ureteroscopic biopsy for upper tract urothelial carcinoma: does the location matter? J Endourol. 2017;31(3):259–265.
- Fahmy NM, Mahmud S, Aprikian AG. Delay in the surgical treatment of bladder cancer and survival: systematic review of the literature. Eur Urol. 2006;50(6):1176–1182.
- Waldert M, Karakiewicz PI, Raman JD, et al. A delay in radical nephroureterectomy can lead to upstaging. BJU Int. 2010;105(6):812–817.
- Sundi D, Svatek RS, Margulis V, et al. Upper tract urothelial carcinoma: impact of time to surgery. Urol Oncol. 2012;30(3):266–272.
- Nison L, Rouprêt M, Bozzini G, et al. The oncologic impact of a delay between diagnosis and radical nephroureterectomy due to diagnostic ureteroscopy in upper urinary tract urothelial carcinomas: results from a large collaborative database. World J Urol. 2013;31(1):69–76.
- Boorjian S, Ng C, Munver R, et al. Impact of delay to nephroureterectomy for patients undergoing ureteroscopic biopsy and laser tumor ablation of upper tract transitional cell carcinoma. Urology. 2005;66(2):283–287.