
Abstract
Context: In Italy, little is known about the territorial distribution of the frailty status.
Aims: To compare frailty- and multimorbidity-prevalence in the elderly population of two Italian regions.
Methods: This study examined randomized samples of elderly (both community dwelling and institutionalized) assisted by general practitioners. Frailty was evaluated through the CSHA-Scale, multimorbidity through the Charlson-Score. The relation between frailty and multimorbidity was studied through a logistic model. Both crude and standardized prevalences were calculated.
Results: One hundred and sixteen physicians assisted 176,503 patients highly representative of Italian people. In a randomized sample of 4,531 older people, the sex–age-standardized prevalence of Frailty (standard population: Italy) was 25.74% (24.63–26.85%). Age-standardized prevalence for males was 20.08% (18.46–21.71%) and 30.00% (28.54–31.57%) for females. Using the sex–age-standardization pooled sample, the prevalence of frailty was significantly higher in Sicily than Veneto (28.74% [27.03–30.46%] vs 22.30% [20.94–23.67%]. This study did not find differences in the prevalence of multimorbidity: Veneto 20.76% (19.21–22.31%); Sicily 22.05% (20.33–23.77%). Both “to be female” and “to live in Sicily” were shown to be predictors of frailty OR for being female = 1.64 (1.42–1.88); OR for living in Sicily = 1.27 (1.11–1.46). Multimorbidity was an independent frailty-predictor only for those aged < 85: OR of Charlson Index ≥ 4 for ages < 85 = 3.44 (2.88–4.11), OR for ages ≥ 85 = 1.44 (0.97–2.12).
Limitations: (1) This study considered patients assisted by doctors, not a random sample of the general population. (2) The cross-sectional nature of the study limits the interpretation of the relationships between frailty and multi-morbidity. (3) Few covariates were available for our multivariate models.
Conclusions: More than 1/4 of elderly persons are shown to be frail (1/5 of males and 1/3 of females). Frailty is more frequent in Sicily, while multimorbidity does not differ between the two regions. This could be due to regional differences in the organization of care networks dedicated to elderly patients.
Introduction
Frailty and multimorbidity represent the more important hallmarks of ageing and they are a primary concern in the care of older adultsCitation1. Today there is unanimous agreement that frailty should be considered a condition in its own right. Frailty represents an independent risk factor for numerous endpointsCitation2,Citation3 and it must be clearly distinguished from disability and multimorbidity, equally important and independent but often superimposed on itCitation4. The debate on whether incorporating multimorbidities or disabilities in the frailty-scales is still open, because these represent a share of irreversibility that does not conform to the concept of a dynamic condition accepted by other authorsCitation5. Frailty-models adopted by researchers are extremely heterogeneous, so the prevalence of frailty is shown to be very different depending on the definition adopted, on the domains that were considered, and the tools used for measuring itCitation6–9. Few Italian studies evaluated the territorial distribution of the frail elderly patientsCitation10–15, while there is a wide variety of literature about the prevalence of chronic diseasesCitation16. Nevertheless, the identification of frail patients is essential, insofar as the determinants of frailty can be very different from those of the multimorbidityCitation3,Citation5. So, the activation of territorial assistance networks based only on the management of the chronic diseases may be insufficient, frailty being an independent risk factor of death and institutionalizationCitation3,Citation5.
In a previous article we discussed the difficulty in comparing the prevalence of frailty estimated in different settings: this is due to the difference in the analysed populations and the heterogeneity of the diagnostic tools. These factors provide a wide variation in the Italian prevalence of frailty, ranging from 12.7–44.6%Citation17.
By our knowledge our recent cross-sectional study on 2,407 older patients in VenetoCitation17 is the first Italian experience in which the prevalence of frailty was examined through the CSHA Clinical Frailty ScaleCitation18 in a random sample of the population assisted by general practitioners. That research shows that almost one in five elderly in Veneto is affected by frailty, the raw prevalence being 23.18% (21.53–24.91%). In that experience, to be a female acted as a strong and independent risk factor, while age was shown to be a confounder in regards to the multimorbidity: only in elderly individuals aged below 85 year was a significant multimorbidity shown to be an independent predictor of frailtyCitation17.
The study of the territorial distribution of frailty and multimorbidity is essential for welfare. In Italy, the interventions for chronicity are mainly based on the treatment of diseases, and there are also many differences in the ways in which the single regions manage the assistance to elderly people.
The primary objective of our research was to estimate the prevalence of frailty in the older population (i.e. 65+ years) normally assisted by 116 general practitioners in Veneto and Sicily (Italy); our study evaluated both community-dwelling and institutionalized people. Secondary objectives were to compare the prevalence of frailty and multimorbidity in Veneto and Sicily. A third objective was to confirm the relationship between frailty and multimorbidity found in our previous researchCitation17.
Subjects and methods
Our research is an observational cross-sectional study.
Setting
We considered elderly patients assisted by general practitioners and residents in two Italian regions (Veneto and Sicily). In Italy, the general practitioners assist these types of older adults: (1) patients who are able to autonomously reach the doctor’s office; (2) home-dwelling patients who are unable to walk (followed up with home visits); and (3) institutionalized patients in nursing homes. All these seniors (i.e. aged 65 and over) constituted the population of our study.
Sample
We evaluated the prevalence of frailty and multimorbidity in a randomized sample that was obtained through a central randomization stratified by sex and age. Prevalence of frailty was our primary endpoint.
Data collection
General practitioners from Veneto and Sicily were enrolled on a voluntary basis. Everyone had to use the same professional software (MillewinR)Citation19.
The 116 doctors involved in the initiative were members of the Scientific Society “Societa’ Italiana di Medicina Generale e delle Cure primarie” (SIMG) or sympathizers. Our research was not financed and all the researchers were volunteers.
Data of recruited patients were anonymously collected (only the physicians knew the identity of the patients—see below) and were treated in compliance with the laws that regulate privacy and execution of observational research in Italy.
In particular, Italian laws require each patient to provide informed consent to the attending physician regarding the anonymized treatment of their clinical data at the time of taking charge.
Each researcher received and decrypted a list of centrally randomized patients. If codes were of deceased patients or for other reasons no longer assisted by the doctor, the researcher had to replace them in casual mode in the manner described in Supplementary Appendix A.
Tools
Frailty was measured through the Rockwood’s CSHA Clinical Frailty ScaleCitation18, particularly suitable for the professional routine in a general practice. The CSHA Clinical Frailty ScaleCitation18 allows one to calculate a score ranging from one to seven (one: best state, seven: worst state), the frailty status being defined by a score >4. This instrument was well validated both in reliability and in predictive valueCitation6.
Rockwood does not consider frailty as an “all-or-nothing” statusCitation18. Fitness and frailty status are strictly linked in the theoretical model which provided the CSHA Frailty Scale: in this model patients’ need of help with daily activities is a determinant factor.
The multimorbidity was evaluated through the Charlson Index (CCI)Citation20, defined by the presence/absence of 23 conditions characterized by different prognostic weights; a CCI ≥4 characterizes a condition of multimorbidity with clinical significanceCitation21.
Stages of research
The research took place in two phases.
In the first phase a unique dataset was constructed, represented by the whole population in charge of the recruited physicians.
Anonymized data were extracted from records of individual physicians through a custom SQL query (details on request). This was built to obtain, in addition to the personal data of all assisted patients (sex, date of birth), also the data relevant to the 23 conditions necessary to calculate the Charlson IndexCitation20. Each condition was defined through ICD-9 codesCitation22,Citation23 (see also Supplementary Appendix B). The individual patient data were rigorously anonymous, in compliance with the current Italian legislation.
In the second phase we extracted a random sample of 65+ people from the dataset previously constructed through a central randomization stratified by sex and age (65–74; 75–84; ≥85 years). Then we provided the researchers the anonymous codes of the randomized patients. We provided a utility that matched anonymous codes and patients: each doctor used this utility to identify the patients to evaluate through the CSHA Clinical Frailty ScaleCitation18.
Statistical analysis
We compared the composition in sex and age-decades with the official dataCitation24 to judge whether the population assisted by the physicians involved was representative of the general population of Italy. The comparison was made using both graphic methods and formal statistical tests (see below).
We evaluated the quality of the randomization process comparing the distribution of three classes of age (65–74; 75–84; ≥85) between the entire 65+ aged population and the randomized sample of patients evaluated through the CSHA Clinical Frailty ScaleCitation18. The comparison was made both graphically and through statistical approach (see below).
We calculated the sample size accepting a usual level of confidence (95%) and programming a relative precision of ±30%. The expected prevalence of frailty that we used in the calculations referred to the proportions of frail individuals detected in three age strata by a cross-sectional study cited by RockwoodCitation25,Citation26. After correction for finite populationCitation27 the theoretical sample size corresponded to 3,616 65+ aged individuals. We took into account a drop-out of 20% of physicians, thus increasing the sample size to 4,520 individuals. The prevalence of the 65+ age-stratum in an epidemiological dataset of primary-care medical records is 25.47% (MilleinReteCitation28) so the general population capable of generating 4,520 elderly was 17,746 units. Assuming that a doctor could not examine more than a tenth of his elderly pool, the population necessary to research amounted to 177,464 individuals. That is, admitting that an Italian general practitioner assists 1,500 patients on average, 118 general practitioners seemed to be necessary for our research.
We compared the distribution of age-strata between different populations using both graphic methods and formal (Kolmogorov and Smirnov) statistical testsCitation29,Citation30.
We evaluated the prevalence of the frailty and its 95% CI in our randomized sample through the Agresti’s method for proportionsCitation31.
We standardized the frailty prevalence by sex and five classes of age (≥ 65 < 70, ≥ 70 < 75, ≥ 75 < 80, ≥ 80 < 85, ≥85) using the official data provided by the Italian Official Statistical DataCitation24. We also compared the prevalence of frailty and multimorbidity between Veneto and Sicily by standardizing for age and sex using the pooled sample as a standard population.
We studied the relation between frailty and multimorbidity through a logistic regression model considering age, sex, residence, and comorbidity as covariates.
Analyses were done using STATA14 SE and PASS 2008 software.
Results
Compliance of researchers
The first phase of the research took place over 42 days; the second over 102 days (for details see Supplementary Appendix C)
One hundred and forty-five general practitioners agreed to be recruited; 116 doctors completed the research, so the general drop-out rate corresponded to 20.0% (i.e. exactly as expected).
Population of patients assisted by primary care physicians
The whole population assisted corresponded to 176,503 individuals (Veneto: n = 82,919; Sicily: n = 93,584, with a prevalence of 25.29% of subjects aged 65+ (n = 44,630, Veneto n = 21,825; Sicily n = 22,825).
The distribution of five age classes of this population was almost perfectly comparable to that of the Italian population illustrated by the official ISTAT dataCitation24 (Kolmogorov-Smirnov test, p = 1.00—details on request).
The sample of older people evalutated for frailty and multimorbidity
The researchers evaluated the frailty status of 4,531 individuals (, Supplementary Appendix D). Of the 4,531 individuals included in our research, 2,584 (57.03%) were females. The distribution in sex and age classes in the 4,531 evaluated subjects is illustrated in Supplementary Appendix E.
Table 1. Characteristics of the analysed sample.
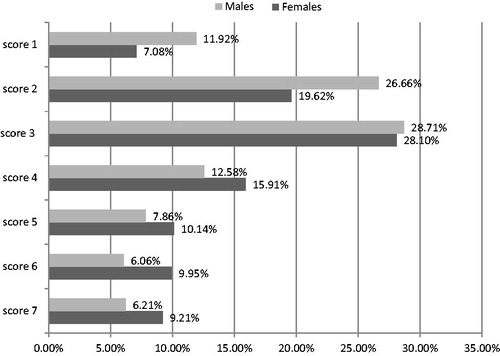
The distribution of CSHA Clinical Frailty Scale’sCitation18 scores in the sample is illustrated in ; the distribution of these values is shown to be roughly bimodal.
Figure 1. Distribution of the Rockwoods scores in the 4,531 65+ evaluated.
Crude prevalence of frailty
The crude prevalence of Frailty (CSHA Clinical Frailty ScaleCitation18 score >4) stratified by sex and three age-strata is illustrated in ; for the full sample corresponds to 25.35% (24.11–26.64%): this estimation can be considered as the primary result of our study.
Table 2. Age- and sex-distribution of the prevalence of Frailty Status (so defined by a Rockwood score > 4) in the sample of 4,531 elderly individuals evaluated with the Rockwood Clinical Frailty Scale (% value and 95% confidence intervals).
The crude prevalence of the state of frailty in five age-strata is illustrated in Supplementary Appendix F. Frailty is shown to be more frequent in women with respect to men both in the whole sample and in the age-strata (Supplementary Appendix F).
illustrates the prevalence of the state of frailty in some common chronic diseases.
Table 3. Prevalence of the state of frailty in some common chronic diseases.
Prevalence of frailty standardized over Italian distribution of ages and sex
Using as standard population the official data of Italy (ISTAT 2017Citation24) and sex and five age-classes as covariates, the standardized prevalence of frailty corresponds to 25.74% (24.63–26.85%). Females were shown be significantly frailer than males, being the prevalence of Frailty 30.00% (28.54–31.57%) and 20.08% (18.46–21.71%), respectively (see also Supplementary Appendix E).
Comparison of Veneto’s and Sicily’s frailty prevalence adjusted for age and sex
Using the whole sample as a standard population, the standardized prevalence of frailty is shown to be higher in Sicily than Veneto, corresponding to 28.74% (27.03–30.46%) and 22.30% (20.94–23.67%), respectively (p < 0.0001)
Crude prevalence of significant multimorbidity
The prevalence of significant multimorbidity (i.e. of a Charlson Score ≥ 4) in the sample is 21.39%.
Supplementary Appendix G shows the distribution of the Charlson Score’s values.
Age- and sex-standardized prevalence of multimorbidity (reference: Italian distribution)
Using as a standard population the official data of Italy (ISTAT 2017Citation24) and sex and five age-classes as covariates, the standardized prevalence of multimorbidity corresponds to 21.47% (20.30–22.64%), without significant differences between males and females: 20.77% (19.01–22.53%) and 22.00% (20.43–23.58%), respectively.
Comparison of age- and sex-adjusted prevalence of multimorbidity between Veneto and Sicily
Using the whole sample as standard population, the standardized prevalence of significant multimorbidity is shown to not be different between the two regions, corresponding to 20.76% (19.21–22.31%) in Veneto and 22.05% (20.33–23.77%) in Sicily (p = 0.623).
Distribution of standardized prevalences of frailty and multimorbidity in different classes of age
illustrates the prevalence of frailty and significant multimorbidity in five mutually exclusives categories.
Figure 2. Prevalences of mutually exclusive combinations of frailty and serious comorbidity.
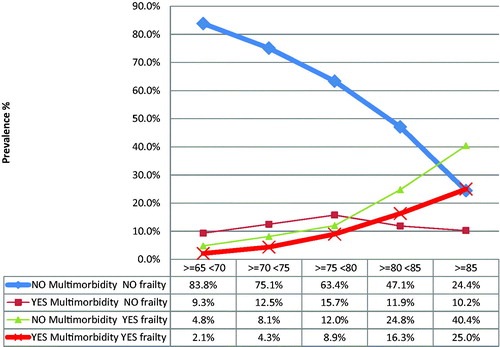
Values were standardized by age and sex using Italian people as a standard population. As can be seen, the prevalence of frailty is shown to increase with age, while the prevalence of significant multimorbidity tends to decrease.
In detail, the proportions of patients without frailty and without significant multimorbidity (that is with Charlson score < 4 and Frailty score ≤ 4) showed a strong and progressive decrease with the advance in age. At the same time, the proportions of frail/not multimorbid patients (that is, with Charlson score < 4 and Frailty score > 4) and frail/multimorbid patients (Charlson Score ≥ 4 and Frailty score > 4) were shown to increase with advancing age. On the other hand, the proportion of multimorbid/not frail patients (Charlson Score ≥ 4 and Frailty score ≤ 4) was shown to increase with age up to the age group ≥ 75 < 80, and then to decrease (). In the last age-stratum (≥ 85 years) a quarter of individuals (24.4%) were shown to be neither frail nor multimorbid; another quarter (25.0%) were shown to be both frail and multimorbid, another 40.4% were shown to be frail, but not multimorbid, and the last 10.2% were shown to to be multimorbid, but not frail.
Multivariate logistic regression model
We explored the details of the relationship between frailty and multimorbidity through three models of logistic regression () in which the condition of frailty was the outcome and age, sex, residence, and multimorbidity were the predictors. The model with interaction shows the best goodness of fit and the best response to model-diagnostics (). To be a female shows to be strongly associated to the frailty status: OR = 1.53 (1.31–1.79). To be a resident in Sicily compared to be in Veneto is shown to also be a strong predictor of frailty: OR = 1.43 (1.23–1.66). Multimorbidity status (i.e. a Charlson score ≥4) is shown to be an independent frailty-predictor, but not in the most advanced ages: the variable “age” acts in fact as an important confounder towards multimorbidity. The statistical study of the interaction age/multimorbidity demonstrates for the multi-morbid subjects (i.e. with Charlson score ≥4) OR of frailty = 3.44 (2.88–4.11) for <85 people and OR = 1.44 (0.97–2.12) for ≥85 people (see footnote of for details).
Table 4. Univariate and multivariate logistic regression models exploring the relationship between frailty (i.e. Rockwood score > 4) and comorbidity (i.e. Charlson Score ≥ 4).
Discussion
Frailty and multimorbidity prevalence
The identification of frail patients appears essential, insofar as the determinants of frailty can be very different from those of the multimorbidityCitation3,Citation5. So, the activation of territorial assistance networks based only on the management of the chronic diseases may be insufficient, fraility being a risk factor of death and institutionalizationCitation3,Citation5.
Maybe, the better way to draw a sample is from the general population identified by the electoral lists, but this procedure exposes to the risk of low compliance. A good compromise is to extract a sample from a pool of people which is representative of the Italian population in terms of sex and age.
By our knowledge this research represents, after our previous communicationCitation17, the second Italian experience in which the prevalence of frailty was examined through the CSHA Clinical Frailty ScaleCitation18 in a large sample of patients assisted by general practitioners: this sample is representative by sex and age of structure of the entire population.
The CSHA Clinical Frailty Scale is not widely used in prevalence studies. As we already discussed in our previous articleCitation17, to our knowledge there are only two other studies aimed at estimating the prevalence of frailty through this tool.
There is no agreement in the literature on the model for the definition of frailty and on the measuring instrument: we thought that the CHSA scale could be a rational choice for its ease and rapidity of use. The evaluation of the state of frailty does not require the presence of the patient at the general practice, because a physician who knows her patients can assign the score based on her memory.
Our standardized data demonstrate that a quarter of the older people (25.74%) are shown to be frail and frailty is shown to be more common in women (30.00%) than men (20.08%), as also shown in other researchCitation32,Citation33. The proportions of frail patients in different age groups in the entire sample are very similar to the one we already reported in the cohort of VenetoCitation17.
As we already notedCitation17, other experiences which evaluated frailty with the same scale and in a similar strata of populationCitation34,Citation35 were based on interviews or questionnaires, providing a high risk of healthy user bias. In our research the doctor, who knew the patients very well, evaluated frailty of the random sample with a simple tool that did not need the collaboration of the patient. Moreover, the randomized choice of the sample allowed us to evaluate institutionalized or non-walkable patients who would not have been reached through interviews or questionnaires targeted towards the community-dwelling population.
Our standardized data also show that about one fifth of Italian older people (21.47%) are affected by significant multi-morbidity, without differences between the two sexes and between the two regions.
Notably, frailty progressively increases with advancing age, becoming one of the first geriatric problems in the more aged groups. Over the age of 85, for example, it affects 65.4% of patients, being much more frequent than multimorbidity (35.2%)
This result could be explainedCitation17 by both the cross-sectional nature of our analysis and the fact that likely multimorbidity influences the prognosis to a greater extent than frailty: our sample could be constituted of self-selected people with better survival (less sick subjects).
Interestingly our study shows that the prevalence of frailty is significantly higher in Sicily than Veneto (28.74% vs 22.30%), while the prevalence of severe multimorbidity is similar in the two regions (22.05% vs 20.76%).
Furthermore, official data show that Sicily has a higher standardized mortality rate than Veneto (99.01 vs 85.33 deaths per 10,000 inhabitants in 2015Citation36).
These data are conventionally related to socioeconomic differences between the two regions. In Veneto, one of the most important Italian industrial regional economies, the gross domestic product per capita in purchasing power standards (GDP per capita in PPS) was €32,300 in 2016, amounting to 114% of the Italian averageCitation37. In the same period, in Sicily GDP per capita in PPS amounted to €17,500, equal to 62% of the national oneCitation38.
Despite our study not being intended for evaluating frailty as a predictor of death, the results make us suppose that the difference in the prevalence of frailty could be one of the determinants of the excess of mortality in Sicily. This hypothesis is biologically in accord with the demonstrated relationship between frailty and negative outcomes such as death and the need for institutional careCitation18.
The difference in mortality rate between Sicily and Veneto increases with increasing age, and the difference in the prevalence of frailty between the two regions shows a similar trend. This overlap is clearly visible up to the age-stratum of 80–84 years for men () and 75–79 years for women (Supplementary Appendix L, Figures L1 and L2), limits beyond which the prevalence of frailty in Sicily and Veneto converge.
While the prevalence of frailty in the two regions tends to converge in the upper strata of age ( and ), in the same strata the difference in mortality rate tends to remain notable, and also to increase.
This suggests that the difference of prevalence of frailty could explain almost partially the excess of mortality in Sicily, but that other determinants could be involved, such as the different efficacy in managing frailty by the two regions.
Obviously, this is only a hypothesis, which can be confirmed only by a longitudinal study.
In Italy, a domiciliary care service intended for non-self-sufficient people and frail subjects is available, which integrates health and social services (“Assistenza Domiciliare Integrata”, ADI): each physician can activate this service informing the Local Health Unit about the need of social and healthcare of a patient. In 2015, in Sicily, ADI was distributed to ∼9,800 elderly people (≥65 years old) more than VenetoCitation39, despite the resident elderly population being around 54,000 more in Veneto than SicilyCitation40. The proportion of elderly people in ADI was similar in the two regions (approximatively 88% of the total)Citation39, but Veneto had high rates of treated cases with low care intensity, while Sicily was one of the regions with the highest rates of treated cases with high care intensityCitation41. This situation makes us suppose that, maybe, in Sicily physicians dispense ADI as an intervention mainly aimed to severe morbidity or disability, while in Veneto the same service is dispensed also taking into greater account other criteria such as socioeconomic needs.
Our study shows that a substantial proportion of elderly people are frail without having severe multimorbidity, particularly at older ages, and our logistic regression model shows that severe multimorbidity is not a significant determinant of frailty in people aged ≥85. For these reasons, physicians who dispense ADI as an intervention primarily aimed to severe morbidity do not reach non-comorbid elderly people whose main determinant of death and other negative outcomes is frailty. Furthermore, in Sicily, residential care facilities cannot likely address socio-sanitary needs of the patients not reached by ADI, since the number of beds for non-self-sufficient elderly people in these structures is dramatically lower in Sicily than Veneto (51.7 vs 268.8 beds for non-self-sufficient elderly people per 10,000 resident elderly people)Citation39.
These data and our results suggest that some of the determinants of the excess of mortality in Sicily could be the higher prevalence of frailty and a less effective management of needs of frail older adults.
Frailty must be evaluated as routine practice
Non-geriatric physicians are more familiar with the problems related to multimorbidity compared to the problems related to the frailty, because the frailty is often associated with psycho-social determinantsCitation5 that do not belong to the physical domain, which is the main object of the medical profession. For this reason, also the territorial epidemiological research was focused on the prevalence of diseases instead of the prevalence of frailty. However, now it is known that frailty status is an important predictor of death and other important clinical endpoints, so the approach to older patients in primary care must be absolutely integrated by a systematic assessment of frailty. Although our research was not aimed at this objective, our data suggest that differences in prevalence and management of frailty could result in different risk of death in different regions.
A tool to assess the condition of frailty within the primary care setting must be validated in terms of predictability and reproducibility, but it must also be very simple, and usable without excessive loss of time during the daily care practice. Frailty is very easy to measure with the scale we used: so, by our opinion, the use of the CSHA Clinical Frailty ScaleCitation18 should become part of the routine of general practitioners.
Strengths of our research
We analysed a stratified random sample that is highly representative of a population; this population was representative of the general population of Italy. For this reason, we are reasonably confident about our inferences.
The randomization of the sample and the evaluation of the frailty by the general practitioners allowed us to produce representative data of the entire elderly population normally followed in the primary care setting.
The tool we used for estimating frailty (CSHA Clinical Frailty ScaleCitation18) is very simple to apply (only a few seconds for every known patient), it provides reproducible results, and it is well predictive of important geriatric outcomes.
Limitations of our research
This work was not funded, and it was conducted with volunteer doctors.
The best approach for a prevalence study should be to extract a random sample directly from the general population by means of electoral or telephone directories, but these methods can be very expensive, and they can expose to risk of poor compliance and healthy users biasCitation17.
However, the population followed up by the volunteer doctors is perfectly comparable to that of the general population in terms of age- and sex-structure.
To assess the robustness of our results, we compared the frailty prevalence of Veneto with the one of Palermo (that is the city that contributed to a greater extent to the Sicilian sample). This sensitivity analysis confirmed our results (see Supplementary Appendix H).
The cross-sectional nature of our research suggests caution in the aetiopathogenetic interpretation of the relationships between frailty and multimorbidity in different age classes. However, we implemented a study in “real life” conditions, and our evaluation suggests a more extensive management of needs of older adults.
Our analyses should have been adjusted for other factors related to the condition of morbidity, such as being or not being institutionalized. We are planning a second phase of the research aimed at evaluating the individual frailty determinants in the recruited sample; on this occasion we will take into account other important covariates (i.e. such as the admission to a nursing home).
The datum of a very similar multi-morbidity in the two Italian regions was widely expected, given that the ethnic group is common. Although in our discussion we hypothesized that the differences in mortality rates between the two regions can be explained by different prevalence in terms of frailty, the reasons why Sicilian seniors are more frail than elderly people in Veneto remain to be investigated. Our research will continue in a subsequent step, in the verification and comparison of the determinants of frailty in the two regions, in order to answer this question.
Finally, frailty was not evaluated through instrumental investigations such as the measurement of gripping force, but the Rockwood scale was already validated in terms of reproducibility and predictability.
Conclusions
Our research shows that almost a quarter of elderly people in Italy are affected by frailty (almost one third for females and almost one fifth for males). Often physicians focus more on morbidity than on psychosocial needs of older people. Nevertheless, the individualization of frail individuals is important because frailty is a predictor of death and other geriatric endpoints, but often it is also a reversible condition.
Physicians should pay close attention both to frailty and comorbidity. Frailty is easy to measure with the scale we used. The use of the CSHA Clinical Frailty ScaleCitation18 should become part of the routine of the general clinical practice.
Transparency
Declaration of funding
There is no funding to declare.
Declaration of financial/other relationships
The authors and JDA peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
For Veneto
Pirolo Giulio3, Balzan Corrado3, Barilla Giuseppe3, Buzzatti Agostino3, Cassol Maria Antonia3, Mazzorana Michela3, Scarrocchia Luisa3, Zollino Maria Luciana3, Cabri Giovanni4, Dolci Alberto4, Tonello Paolo4, Franchini Carlo Andrea5, Fracasso Isabella5, Casalena Michele5, Dima Catia5, Givanni Silvana5, Marrocchella Raffaella5, Menini Ernesto5, Micchi Alessio5, Pastori Caterina5, Sciortino Maurizio5, Cancian Maurizio6, De Conto Umberto6, Antiga Gianluigi6, Camarotto Antonio6, Camerotto Antonio6, Dalla Zentil Giovanni6, Mulato Giuseppe6, Pantaleoni Nicola6, Peccolo Franco6, Penco Claudio6, Pieropan Franco6, Pregnolato Umberto6, Redetti Marina7, Zorgno Nadia6, Musto Martina7, Michieli Raffaella7, Bergamasco Giulio7, Blundetto Emanuela7, De Zan Antonio7, Moressa Maria Pia7, Ongaro Andrea7, Severi Sandro7, Spinardi Francesco7, Franco Novelletto Bruno8, Bordin Anna8, De Gobbi Riccardo8, Fanton Livio8, Fraccaro Bianca Maria8, Franzoso Federico8, Merola Gennaro8, Bordin Anna8, and Simioni Giuliana8.
For Sicily
Amodeo Angela10, Amodeo Vincenzo10, Arezio Palma Carmela11, Aulicino Maria Caterina12, Blunda Gaetano13, Bongiorno Mario10, Calderone Rosa Maria10, Calì Claudia10, Campo Francesco13, Carlino Vincenzo10, Caudo Giacomo11, Cincotta Gaetano11, Cirrito Francesco10, Consiglio Girolamo10, D’Alessandro Rosario10, D’Aratro Vincenzo10, Di Carlo Vittorio10, Di Gregorio Carmelo14, Disclafani Giuseppe10, Di Silvestre Baldassare10, Dolce Antonino Felice10, Fasulo Serenella10, Galvano Luigi10, Gattuso Salvatore10, Giammalva Maria Giuseppa10, Giardina Giovanni15, Giarrusso Paolo10, Giusa Paolo14, Greco Andrea10, Greco Rosa Vincenza10, Gurgone Francesco17, Iraci Tindaro10, La Spia Emanuele10, La Verde Francesco16, Liberti Grace10, Litrico Angelo14, Lo Bue Giuseppe10, Lo Giudice Domenico13, Lombardo Francesco Paolo10, Longo Santi10, Magliozzo Francesco10, Mannina Giuseppe13, Manno Maria Vincenza10, Merlino Giovanni10, Milazzo Vito13, Paradisi Vincenza14, Parlapiano Calogero10, Polizzi Rosaria10, Progno Mariassunta10, Quartetti Giovanni10, Rodolico Pasquale10, Salamone Francesco10, Salvo Anna14, Salvo Nicolò10, Santoro Giuseppe17, Sferlazza Concetta10, Simonetti Maria Teresa10, Spallina Antonio10, Spicola Luigi10, Terzo Maurizio13, Vicari Maria Grazia10, Violini Emanuela16, and Zafonte Rita10.
1 SIMG (Societa’ Italiana di Medicina Generale e delle Cure Primarie); 2 SVEMG (Scuola Veneta di Medicina Generale); 3 General practitioner, Belluno; 4 General practitioner, Vicenza; 5 General practitioner, Verona; 6General practitioner, Treviso; 7 General practitioner, Venezia; 8 General practitioner, Padova; 9 FIMMG (Federazione Italiana Medici di Medicina Generale), Palermo; 10 General practitioner, Palermo; 11 General practitioner, Messina; 12 General practitioner, Siracusa; 13 General practitioner, Trapani; 14 General practitioner, Catania; 15 General practitioner, Agrigento; 16 General practitioner, Caltanissetta; 17 General practitioner, Enna.
Previous presentation
This work was presented at this meeting in a oral communication: Societa’ Italiana di Medicina Generale e delle Cure Primarie, Centro Congressi (Florence, Italy), November 30, 2018.
Supplemental Material Appendices
Download MS Word (3.1 MB)Acknowledgements
We are grateful for the important contribution in the recruitment of researchers to: Musto Martina1,2, Carraro Alessandro2, Pirolo Giulio1–3, Ioverno Enrico1,2,4, Franchini C. Andrea1,2,5, De Conto Umberto1,2,6, Galvano Luigi1,9, and Li Puma Giusy9. We thank for participating actively as researchers of “Italian Study Group on the Elderly”:
Related Research Data
References
- Weiss CO. Frailty and chronic diseases in older adults. Clin Geriatr Med. 2011;27:39–52.
- Hogan DB, MacKnight C, Bergman H, et al. ommittee. Canadian Initiative on Frailty and Aging. Models, definitions, and criteria of frailty. Aging Clin Exp Res. 2003;15:(Suppl):1–29.
- Abellan van Kan G, Rolland Y, Houles M, et al. The assessment of frailty in older adults. Clin Geriatr Med. 2010;26:275–286.
- Wong CH, Weiss D, Sourial N, et al. Frailty and its association with disability and comorbidity in a community-dwelling sample of seniors in Montreal: a cross-sectional study. Aging Clin Exp Res. 2010;22:54–62.
- de Vries NM, Staal JB, van Ravensberg CD, et al. Outcome instruments to measure frailty: a systematic review. Ageing Res Rev. 2011;10:104–114.
- Ravaglia G, Forti P, Lucicesare A, et al. Development of an easy prognostic score for frailty outcomes in the aged. Age Ageing. 2008;37:161–166.
- Ensrud KE, Ewing SK, Taylor BC, et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch Intern Med. 2008;168:382–389.
- Rothman MD, Leo-Summers L, Gill TM. Prognostic significance of potential frailty criteria. J Am Geriatr Soc. 2008;56:2211–2216.
- Hilmer SN, Perera V, Mitchell S, et al. The assessment of frailty in older people in acute care. Australas J Ageing. 2009;28:182–188.
- Liotta G, O'Caoimh R, Gilardi F, et al. Assessment of frailty in community-dwelling older adults residents in the Lazio region(Italy): A model to plan regional community-based services. Arch GerontolGeriatr. 2017;68:1–7.
- Roppolo M, Mulasso A, Gobbens RJ, et al. A comparisonbetween uni- and multidimensional frailty measures: prevalence, functionalstatus, and relationships with disability. Clin Interv Aging. 2015;22:1669–1678.
- Solfrizzi V, Scafato E, Lozupone M, Italian Longitudinal Study on Aging Working Group, et al. Additive Role of a Potentially Reversible Cognitive Frailty Model and Inflammatory State on the Risk of Disability: The Italian Longitudinal Study on Aging. Am J Geriatr Psychiatry. 2017;25:1236–1248.
- Roppolo M, Mulasso A, Rabaglietti E. Cognitive Frailty in Italian Community-dwelling older adults: prevalence rate and its association with disability. J Nutr Health Aging. 2017;21:631–636.
- Bilotta C, Casè A, Nicolini P, et al. Socialvulnerability, mental health and correlates of frailty in older outpatientsliving alone in the community in Italy. Aging Ment Health. 2010;14:1024–1036.
- Perna S, Francis MD, Bologna C, et al. et alPerformance of Edmonton Frail Scale on frailty assessment: its association with multi-dimensional geriatricconditions assessed with specific screening tools. BMC Geriatr. 2017;4:172.
- Saugo M, Pigato M, Avossa F, Gennaro N, et al. Relazione Socio Sanitaria Della Regione Del Veneto – Anno. 2015. Available from: https://www.ser-Veneto.it/Public/RSSR_Veneto_2015.pdf.
- Battaggia A, Scalisi A, Franco Novelletto B, et al. Prevalence of frailty in older people in Veneto (Italy). J Drug Assess. 2019;8(1):1–12.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495. PubMed
- Millennium SRL. [cited 2018 Jun 15]. Available from: https://www.millewin.it/
- Charlson ME, Charlson RE, Peterson JC, et al. The Charlson comorbidity index is adapted to predict costs of chronic disease in primary care patients. J Clin Epidemiol. 2008;61:1234–1240.
- Johnston MC, Marks A, Crilly MA, et al. Charlson index scores from administrative data and case-note review compared favourably in a renal disease cohort. Eur J Public Health. 2015;25:391–396.
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383.
- Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619.
- Statistiche Demografiche ISTAT http://demo.istat.it/pop2017/index.html
- Rockwood K, Howlett SE, MacKnight C, et al. Prevalence, attributes, and outcomes of fitness and frailty in community-dwelling older adults: report from the Canadian study of health and aging. J Gerontol A Biol Sci Med Sci. 2004;59:1310–1317.
- Hogan DB, Fox RA. A prospective controlled trial of a geriatric consultation team in an acute-care hospital. Age Ageing. 1990;19:107–113.
- West Chester UniversityWCU Courses Server Roger Bove, Berenson directory(access: [cited 2018 Jun 15]. Available from: http://courses.wcupa.edu/rbove/Berenson/10th%20ed%20CD-ROM%20topics/section8_7.pdf
- Scuola Veneta di Medicina generaleMilleinRete – il database della Medicina Generale del Veneto( [cited 2018 Jun 15]. Available from: https://www.svemg.it/milleinrete-il-database-della-medicina-generale-del-veneto/
- Kolmogorov AN. Sulla determinazione empirica di una legge di distribuzione. Giornale Dell’ Istituto Italiano Degli Attuari. 1933;4:83–91.
- Smirnov NV. Estimate of deviation between empirical distribution functions in two independent samples. Bulletin Moscow University. 1933. 2:3–16.
- Agresti A, Coull BA. Approximate is better than “exact” for interval estimation of binomial proportions. Am Stat. 1998;52:119–126.
- Fried LP, Tangen CM, Walston J, et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–M156.
- Syddall H, Roberts HC, Evandrou M, et al. Prevalence and correlates of frailty among community-dwelling older men and women: findings from the Hertfordshire Cohort Study. Age Ageing. 2010;39:197–203.
- Ge L, Yap CW, Heng BH. Prevalence of frailty and its association with depressive symptoms among older adults in Singapore. Aging Ment Health. 2018;16:1–6.
- Chang CI, Chan DC, Kuo KN, et al. Prevalence and correlates of geriatric frailty in a northern Taiwan community. J Formos Med Assoc. 2011;110:247–257.
- ISTAT – Mortalita’ per territorio di residenza. Available from: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_CMORTE1_RES#
- Growth – Internal Market, Industry, Entrepreneurshio and SMEs –Veneto. Available from: https://ec.europa.eu/growth/tools-databases/regional-innovation-monitor/base-profile/veneto
- Growth – Internal Market, Industry, Entrepreneurshio and SMEs –Sicily. Available from: https://ec.europa.eu/growth/tools-databases/regional-innovation-monitor/base-profile/sicily
- Rapporto Osservasalute 2017: Stato di salute e qualità dell’assistenza nelle regioni italiane. Available from: https://www.sanitainformazione.it/appuntamenti-della-sanita/rapporto-osservasalute-2017-salute-qualita-dellassistenza-nelle-regioni-italiane/
- ISTAT – Popolazione residente al 1 gennaio. Available from: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1#
- La babele dell’assistenza domiciliare in Italia: chi la fa, come si fa (2017). A cura di Davide L. Vetrano, Ketty Vaccaro. Available from: http://www.italialongeva.it/wp-content/uploads/2017/07/RicercaAdi.pdf