
ABSTRACT
Expression of programmed cell death protein 1 (PD-1) and its ligand PD-L1 has been demonstrated to confer a prognostic value in colorectal cancer (CRC), but no studies have investigated whether this association differs according to tumour location. In this study, immunohistochemical expression of PD-1 and PD-L1 was analysed in tissue microarrays with primary tumours from 557 incident CRC cases from a prospective population-based cohort. Univariable and multivariable Cox regression analyses, adjusted for age, sex, TNM stage, differentiation grade and vascular invasion, were applied to determine the impact of biomarker expression on 5-year overall survival (OS), in the entire cohort and in subgroup analysis of right colon, left colon, and rectum. High PD-L1 expression on tumour-infiltrating immune cells was an independent factor of a prolonged OS in the entire cohort (hazard ratio [HR] = 0.49; 95% confidence interval [CI] CI 0.35 – 0.68), and in tumours of the right colon (HR = 0.43; 95% CI 0.25 – 0.74) and the left colon (HR = 0.28; 95% CI 0.13 – 0.61), but not in rectal cancer. Tumour-specific PD-L1-expression was not prognostic, neither in the full cohort nor according to tumour location. High immune cell-specific PD-1 expression was associated with a prolonged OS in the entire cohort and in tumours of the right colon, but not in the left colon or rectum, and only in univariable analysis. In conclusion, these results demonstrate that immune cell-specific PD-L1 and PD-1 expression is prognostic in a site-dependent manner, whereas tumour-specific PD-L1-expression is not prognostic in CRC.
Introduction
Colorectal cancer (CRC) is the second most common cancer in women and the third most common cancer in men worldwide. Despite advances in treatment, CRC is still the third most frequent cause of cancer-related death.Citation1
Programmed cell death protein 1 (PD-1) is expressed by both lymphoidCitation2 and non-lymphoid immune cells,Citation3,Citation4 and is up-regulated upon after engagement of T cell or B cell receptors on naïve lymphocytes.Citation2,Citation4 Activation of PD-1 by its ligand PD-L1 induces down-regulation of lymphocyte proliferation and cytokine production, resulting in lymphocyte deletion.Citation5 Indeed, expression of PD-L1 on tumour cells has been found to suppress CD8+ T cell activity and to be associated with an impaired prognosis is several types of solid cancer.Citation6-Citation8
Immunotherapy has emerged as a promising approach for cancer treatment,Citation9,Citation10 and checkpoint inhibitors, targeting PD-1 or PD-L1, have demonstrated objective response in several types of cancer, including melanoma, non-small cell lung cancer, and renal cell carcinoma, among others.Citation11 In CRC, the clinical benefit of PD-1 or PD-L1 blockade remains uncertain, however, a few studies report a positive effect of anti-PD-1 antibodies in patients with microsatellite instability (MSI) high tumoursCitation12,Citation13 and anti-PD-1 therapies were recently approved by the U.S Food and Drug Administration for treatment of any type of advanced MSI-high cancer.
Despite increasing evidence reporting multiple differences in epidemiology, clinicopathological features, prognosis, and treatment response between proximal and distal CRC, no studies have hitherto evaluated the prognostic impact of PD-1 and PD-L1 expression in relation to primary tumour location (PTL). The aim of this study was therefore to investigate the prognostic impact of immune cell-specific PD-1 and PD-L1 expression, respectively, and tumour-specific PD-L1 expression, in tumours from incident CRC cases in a large, prospective, population-based Swedish cohort, with particular emphasis on the anatomical location of the primary tumour. In light of previous findings regarding tumour-infiltrating T cells and B cells in the herein investigated cohort,Citation14 we hypothesized that the prognostic impact of PD-1 and PD-L1 expression would be of furthermost importance in tumours of the right colon, rather than in tumours of the left colon or the rectum.
Results
Distribution of immune cell-specific PD-1 and PD-L1 expression and tumour cell-specific PD-L1 expression according to primary tumour site
Information on tumour location was available for 555/557 (99.6%) cases in the tissue microarray (TMA), with 201 (36.1%) right-sided colon tumours, 145 (26.0%) left-sided colon tumours, and 209 (37.5%) rectal tumours.
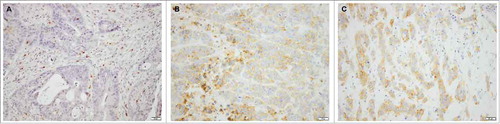
PD-1 expression could be determined in 526 (94.4%) cases, whereby 228 (43.3%) cases were found to have low expression and 298 (56.7%) cases to have high expression of PD-1. Immune cell-specific PD-L1 expression could be evaluated in 536 (96.2%) cases, with 239 (44.6%) cases demonstrating low PD-L1 expression, and 297 (55.4%) cases demonstrating high PD-L1 expression. Tumour cell-specific PD-L1 expression was assessable in 536 (96.2%) cases, with 429 (68.5%) cases displaying negative (0–1%) expression, 52 (8.3%) positive expression in 1–4%, 17 (2.7%) positive expression in 5–9%, 13 (2.1%) positive expression in 10–49%, and 25 (4.0%) cases displaying positive expression in 50–100% of tumour cells. Sample immunohistochemical (IHC) images are shown in .
Figure 1. Immunohistochemical images of PD-1 and PD-L1 staining in colorectal cancer. Sample immunohistochemical images (20x magnification) of (A) PD-1 expression in immune cells, (B) PD-L1 expression in both immune cells and tumour cells, and (C) PD-L1 expression mainly in tumour cells. Unfilled arrows indicate immune cells and filled arrows indicate tumour cells.
Stainings were also evaluated on whole tissue sections and compared with the results from the TMA-based analysis. As demonstrated in Supplementary Table S1, 5/15 cases had a discrepant score in the whole section regarding immune cell-specific PD-1 expression, not differing more than one category, and in 2/15 cases, the difference also affected the dichotomized categories. As shown in Supplementary Table S2, 6/25 cases had a discrepant score in the whole section regarding immune cell-specific PD-L1 expression, not differing more than one category, and in 1/25 cases, the difference also affected the dichotomized categories. Regarding tumour cell-specific PD-L1 expression, a discrepant score was observed in 9/25 cases, differing more than one category in 2/25 cases (Supplementary Table S2).
PD-1 and PD-L1 expression was also compared in cases of rectal cancer in patients who did and did not receive neoadjuvant therapy. There was no significant difference in the expression of PD-L1 in immune cells or tumour cells, whereas the density of PD-1+ immune cells was significantly lower in tumours from cases having received neoadjuvant treatment (Supplementary Table S3).
Associations of immune cell-specific PD-1 and PD-L1 expression and tumour cell-specific PD-L1 expression with clinicopathological factors, according to primary tumour site
For correlation analyses between immune cell-specific PD-1 and PD-L1 expression and clinicopathological factors, cases were divided into groups of low (0–9%) and high (10–100%) PD-1+ and PD-L1+ immune cells, and tumour-cell specific PD-L1 expression was divided into three groups of low (< 1%) and high (1–100%) positive tumour cells. Associations between PD-1 and PD-L1 expression and established clinicopathological characteristics and other investigative biomarkers in relation to PTL are demonstrated in , , and .
Table 1. Associations between PD-1 expression in immune cells and clinicopathological and investigative factors stratified by primary tumour location.
Table 2. Associations between PD-L1 expression in immune cells and clinicopathological and investigative factors stratified by primary tumour location
Table 3. Associations between PD-L1+ tumour cell expression and clinicopathological and investigative factors stratified by primary tumour location
PD-1 expression was significantly associated with lower T-stage (p = 0.015 for the right colon and p < 0.001 for the rectum) and with lower M-stage (p = 0.001) in right-sided colon cancers (). Immune cell-specific PD-L1 expression was significantly associated with lower T-stage in each tumour location (p = 0.017 for the right colon, p = 0.008 for the left colon, and p < 0.001 for the rectum), and with lower N-stage (p = 0.002) and M-stage (p = 0.011) in right-sided colon cancers (). Tumour cell-specific PD-L1 expression was significantly associated with lower age (p = 0.034) and with high differentiation grade (p = 0.040) in patients with right-sided colon cancers ().
Neither PD-1 nor PD-L1 expression in immune cells was associated with BRAF or KRAS mutation status.
PD-1 and PD-L1 expression in immune cells was significantly higher in MSI tumours than in microsatellite stable (MSS) tumours, but only in right-sided tumours (p < 0.001, and p = 0.001, respectively; ,), and PD-L1 expression in tumour cells was significantly higher in MSI tumours in both right-sided colon cancers and rectal caners (p < 0.001 and p = 0.006, respectively; ).
PD-1 expression was significantly associated with immune cell-specific PD-L1 expression, in the entire cohort (p < 0.001) as well as in each tumour subsite (p < 0.001 for all). Furthermore, PD-1 expression correlated with tumour cell-specific PD-L1 expression, in the entire cohort (p < 0.001) and in right-sided and left-sided colon cancers (p < 0.001 and p < 0.001, respectively). Finally, immune cell-specific PD-L1 was associated with tumour cell-specific PD-L1 expression, in the entire cohort (p < 0.001) and in each tumour location (p < 0.001 for all).
Associations of immune cell-specific PD-1 and PD-L1 expression and tumour cell-specific PD-L1 expression with T lymphocyte and B lymphocyte density
Since the prognostic value of B lymphocytes, plasma cells and various subsets of T lymphocytes has previously been shown do differ according to PTL in the herein investigated cohort,Citation14,Citation15 their associations with PD-1 and PD-L1 expression were also examined. There were significant correlations between PD-1 expression and T and B cell infiltration, being most evident in right-sided tumours (). Immune cell-specific PD-L1 expression also correlated significantly with dense infiltration of T cells and B cells, in the entire cohort as well as in right-sided and left-sided colon cancers, and in rectal cancers (). Finally, tumour cell-specific PD-L1 expression was significantly associated with T cell and B cell infiltration in right-sided and left-sided colon cancers ().
Prognostic significance of immune cell-specific PD-1 and PD-L1 expression and tumour cell-specific PD-L1 expression according to primary tumour site
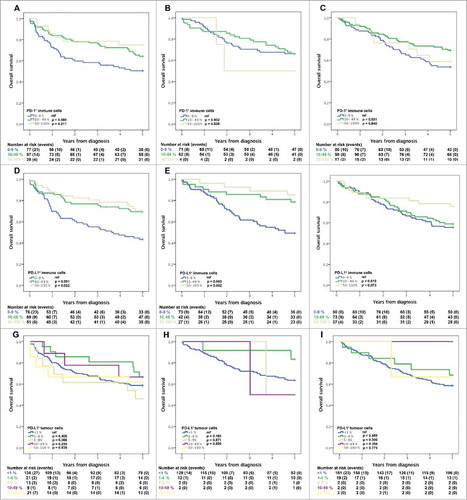
Kaplan-Meier analysis according to all annotated categories demonstrated that PD-1 expression in immune cells was not significantly associated with survival (), whereas intermediate or high expression of PD-L1 in immune cells was significantly associated with an improved 5-year overall survival (OS) in tumours of the right colon () and in the left colon (), but not in the rectum (). Tumour-specific PD-L1 expression was not prognostic in any tumour location ().
Figure 2. Kaplan–Meier estimates of overall survival according to immune cell-specific PD-1 and PDL-1 expression and tumour cell-specific PD-L1 expression, and primary tumour location. Kaplan-Meier analysis of 5-year overall survival in strata of 0–9 %, 10–49 %, and 50–100 % immune cells positive for PD-1 (A, B, C) and PD-L1 (D, E, F) staining, and <1 %, 1–4 %, 5–9 %, 10–49 %, and 50–100 % tumour cells positive for PD-L1 staining (G, H, I), in right-sided (first row) and left-sided (second row) colon cancers, and rectal cancer (third row).
In the entire cohort, the prognostic value of PD-1 expression in immune cells was only significant for low vs negative expression (Supplementary ), whereas intermediate or high PD-L1 expression in immune cells was significantly associated with an improved 5-year OS (Supplementary ), and tumour-specific PD-L1 expression was not prognostic in any tumour location (Supplementary ).
For further survival analyses of immune cell-specific PD-1 and PD-L1 expression, cases were divided into groups of low (0–9% positive cells; n = 239, n = 228, and n = 498, respectively) and high (10–100% positive cells; n = 297, n = 298, and n = 38, respectively) expression.
Cox proportional hazards analyses of 5-year OS according to expression of PD-1 and PD-L1 in immune cells and PD-L1 expression in tumour cells, respectively, in relation to tumour subsite are shown in . The time-dependent covariate was non-significant for immune cell-specific PD-1 and PD-L1 expression as well as for tumour cell-specific PD-L1 expression, and therefore, the factor x time interaction term was dropped from the model. The proportional hazard assumption was also considered to be satisfied with graphical evaluation using log-minus-log plots (data not shown). Univariable hazard ratios for factors included in the multivariable analysis are shown in Supplementary Table S4.
Table 4. Cox proportional hazards models for 5-year overall survival in relation to immune cell-specific PD-1 and PD-L1 expression, and tumour cell-specific PD-L1 expression
In univariable Cox regression analysis, high PD-1 expression was confirmed to be associated with an improved 5-year OS in the entire cohort (hazard ratio [HR] = 0.69; 95% confidence interval [CI] 0.52 – 0.91) and in tumours of the right colon (HR = 0.57; 95% CI 0.36 – 0.89), however, these associations did not remain significant in multivariable analysis, after adjustment for age, sex, TNM stage, differentiation grade, and vascular infiltration (). The significant associations between high PD-L1 expression in tumour-infiltrating immune cells and an improved 5-year OS in the entire cohort were confirmed in univariable Cox regression analysis (HR = 0.50; 95% CI 0.38 – 0.66) and remained significant in multivariable analysis, (HR = 0.50; 95% CI 0.36 – 0.71). Furthermore, high immune cell-specific PD-L1 expression was significantly associated with an improved 5-year OS in both right-sided and left-sided tumours in univariable (HR = 0.42; 95% CI 0.27 – 0.66 and HR = 0.30; 95% CI 0.16 – 0.57, respectively) and multivariable analysis (HR = 0.47; 95% CI 0.26 – 0.84 and HR = 0.28; 95% CI 0.13 – 0.62, respectively). When MSI status and BRAF mutation status was included in the adjusted model, PD-L1 remained an independent favourable prognostic factor in right-sided tumours (HR = 0.46; 95% CI 0.24 – 0.87). Survival analysis in strata according to MSI status revealed that the prognostic impact of PD-L1 was only evident for patients with MSS tumours, in both univariable and multivariable Cox regression analysis (data not shown).
Using the classification and regression tree (CRT) derived cut-off for the total number (continuous score) of PD-1+ immune cells, high expression was confirmed to be prognostic in univariable Cox regression analysis in the entire cohort (HR = 0.46; 95% CI 0.25 – 0.85) and in tumours of the right colon (HR = 0.36; 95% CI 0.16 – 0.83), but not in multivariable analysis (data not shown).
Cox regression analyses for immune cell-specific PD-1 and PD-L1 expression, respectively, after exclusion of rectal cancer cases having received neoadjuvant therapy are shown in Supplementary Table S5. In the entire cohort, immune cell-specific PD-L1 expression remained an independent prognostic factor and PD-1 expression was prognostic in univariable but not in multivariable analysis.
Tumour-specific PD-L1 expression was not prognostic for any of the tested cut-offs at 1%, 5%, or 10%, neither in univariable nor in multivariable Cox regression analysis, (Supplementary Table S6).
There was a significant interaction between high PD-L1 expression in immune cells and tumour location in the right and left colon vs. the rectum (p for interaction = 0.019). No significant interactions were observed between PD-1 expression in immune cells or PD-L1 expression in tumour cells and any tumour location.
Survival analysis in strata according to adjuvant chemotherapy in curatively treated stage III patients revealed no prognostic significance of neither immune cell-specific PD-1 or PD-L1 expression nor tumour cell-specific PD-L1 expression (data not shown).
Discussion
Although several studies have investigated the prognostic impact of PD-1 and PD-L1 expression in CRC,Citation16-Citation21 this study is, to the best of our knowledge, the first to investigate whether this association differs by the anatomical location of the primary tumour.
In the entire cohort, high expression of PD-L1 in tumour-infiltrating immune cells was found to be independently associated with an improved prognosis, which is in line with previous findings in CRC.Citation17,Citation19,Citation22 Moreover, in subsite analysis according to PTL, PD-L1 expression was independently associated with a prolonged survival in patients with right-sided and left-sided colon cancers, but not in patients with rectal cancer. These findings further support previous evidence suggesting that proximal and distal CRC may represent different epidemiological, pathological, genetic, and clinical entities.Citation23,Citation24 Right-sided tumours, often defined as proximal to the splenic flexure, are generally poorly differentiated, diagnosed in more advanced tumour stages, displaying different molecular patterns, and carrying a poorer prognosis than left-sided tumours.Citation24,Citation25 Several studies also demonstrate the importance of taking PTL into account when evaluating treatment response,Citation26-Citation28 and retrospective analyses from large phase III trials have demonstrated that patients with right-sided tumours have less benefit from the addition of EGFR-targeted therapy.Citation29
High PD-L1 expression in immune cells correlated significantly with dense CD8+ T cell infiltration, which in the herein investigated cohort has been found to be an independent prognostic factor.Citation14 This may indicate a general activation of the immune response. Nevertheless, the prognostic impact of PD-L1 was independent of CD8+ T cell infiltration, suggesting that PD-L1 expression itself carries a prognostic value. Another explanation to the favourable impact of PD-L1 expression, contradicting results from other types of solid cancer, is that the immune cell infiltration in CRC might be associated with paradoxical features due to the microbiota of the colon. For example, in contrast with the majority of human cancers, the infiltration of FoxP3+ immune cells in CRC has in the herein investigated cohortCitation14 and others,Citation30,Citation31 been found to be an auspicious prognostic factor. It should however be pointed out that the herein described inter-correlations between different subsets of immune cells merely reflect their co-localization in selected tumour regions. Moreover, although there was a good agreement between PD-1 and PD-L1 expression in the TMA cores and whole tissue sections, the latter may not be sufficient for comprehensive mapping of tumour-infiltrating immune cells. Rather, applying the TMA technique for multiple sampling of cores from different tumour blocks, representing both the tumour and adjacent stroma, would likely provide more accurate information.
Whereas immune cell-specific PD-L1 expression was found to be an independent prognostic factor, tumour cell-specific PD-L1 expression was not associated with survival neither in the full cohort nor in subgroup analysis according to PTL, supporting previous reports in CRCCitation16,Citation17,Citation19,Citation22 and other cancers.Citation32-Citation34 Nonetheless, an abundance of studies have reported high PD-L1 expression to be associated with an impaired prognosis due to induction of immune evasion,Citation6,Citation7,Citation35 being the rationale for PD-1/PD-L1 blockade.Citation36,Citation37 Noteworthy, a significant part of studies regarding the prognostic impact of PD-L1 have not discriminated between its expression in tumour cells and tumour-infiltrating immune cells. The results from the present study, with immune cell-specific PD-L1 expression being an independent prognostic factor while its expression in tumour cells was not, are coherent with previous researchCitation16,Citation23-Citation26 and demonstrate that PD-L1 expression in immune cells and tumour cells might carry different prognostic values and might be regulated by distinct mechanisms. Furthermore, although tumour cell-specific PD-L1 expression has been validated as a predictive marker for response to PD-1 or PD-L1 blockade in several cancers,Citation11,Citation38,Citation39 recent studies now suggest that PD-L1 expression in tumour-infiltrating myeloid and T cells also play a critical role in immunosuppression,Citation38,Citation40-Citation43 and should possibly be taken into account in assessment scoring for PD-1/PD-L1 blockade.
Although the favourable impact of PD-L1 expression in tumour-infiltrating immune cells was independent of MSI status in the entire cohort as well as in right-sided tumours, the prognostic impact was only evident in MSS tumours. In contrast, previous studies concerning treatment response from PD-1 or PD-L1 blockade in CRC report clinical benefit only for patients with MSI-high tumours,Citation12,Citation13 possibly explained by the fact that MSI-high tumours generally carry a higher mutational load, resulting in a robust T cell response which can be exploited by relieving the negative pressure. Nevertheless, Droeser et al. found that strong PD-L1 expression in CRC cells correlated with improved survival only in patients with MSS tumours, and that high PD-L1 was associated with an increased CD8+ T cell infiltration.Citation18 They hypothesized that the favourable impact of PD-L1 in MSS tumours might be coupled with the concomitant dense cytotoxic T cell infiltration. This may also explain the results from the present study, as there was a significant correlation between a high density of CD8+ T cells and high PD-L1 expression in MSS tumours.
Immune cell-specific PD-L1 expression was significantly higher in tumours with lower TNM stage, both in the entire cohort and in right-sided tumours. Furthermore, PD-L1 expression in both immune cells and tumour cells was significantly associated with MSI tumours, which is in line with previous research.Citation44 These data further support an auspicious prognostic impact of immune cell-specific PD-L1 expression. Consistent with previous research,Citation45 high PD-L1 expression in tumour cells correlated significantly with older age and female sex. Furthermore, tumour cell-specific expression of PD-L1 was significantly associated with immune cell-specific PD-1 and PD-Ll expression, supporting results from other studies.Citation39
Of note, the majority of previous studies regarding PD-1 and PD-L1 expression in cancer have focused on the predictive value for PD-1/PD-L1 blockade, with the choice of antibody and scoring algorithm depending on the selected PD-1/PD-L1-pathway inhibitor. The aim of this study was to examine the prognostic value of PD-1 and PD-L1 expression in CRC, with particular reference to PTL. Studies regarding the prognostic impact of PD-1 and PD-L1 expression have used different categorical cut-offs,Citation16-Citation21 some also including staining intensity, and no consensus has yet been reached regarding an optimal prognostic cut-off. For evaluation of tumour cell-specific PD-L1 expression, we applied cut-offs commonly used in clinical studiesCitation46 and the prognostic value of PD-1+ immune cells was validated using the total count. The results from the present study, demonstrating that immune cell-specific PD-1 and PD-L1 expression carries the most evident prognostic value in right-sided CRC, are not likely to be disputed by alternative scoring systems.
In the present study, no independent associations between PD-1 expression and prognosis were found, neither in the full cohort, nor in subsite analysis. This is in contrast with a previous study on CRC, where Li et al. demonstrated PD-1 to be an independent prognostic factor for both OS and disease-free survival in patients with MSS tumours.Citation17 Moreover, PD-1 expression has been demonstrated to carry an independent favourable impact in gastric,Citation47 ovarian,Citation48 and head and neck cancer,Citation49 among others. Further studies are warranted to elucidate the prognostic impact of PD-1 expression in CRC, particularly regarding PTL.
Of note, a significant part of studies on CRC regarding PTL exclude the transverse colon altogether, and a rather large proportion of these studies also include rectal cancers into left-sided CRC. However, rectal cancer differs from descending and sigmoid colon cancer in molecular features, treatment approaches, and prognosis.Citation50,Citation51 Thus, we believe that it is more appropriate to apply the herein used definition on future studies.
Nonetheless, there are some limitations to the study. First, although the study cohort is derived from a large, prospective population-based cohort with clinically and histopathologically well-characterised CRC cases, there is a potential risk of selection bias as the study was made retrospectively. Furthermore, previous studies have used different antibodies and various cut-offs to define high and low expression of PD-L1 and PD-1, respectively, making it problematic to compare the results. Finally, several factors have been reported to affect the expression of PD-1 and PD-L1, including chemotherapyCitation52,Citation53 and radiotherapy.Citation22 However, in the present cohort, only 61 (29,8%) of patients with rectal cancer received neoadjuvant treatment, and we found similar results regarding the prognostic value of the investigated biomarkers when excluding neo-adjuvant treated rectal cancer patients. Moreover, while the density of PD-1+ immune cells was significantly lower in tumours from rectal cancer patients having received neoadjuvant treatment, the density of PD-L1+ immune cells and the distribution of tumour cell-specific PD-L1 expression did not differ between treated and untreated cases. However, we did not compare the expression of PD-1 and PD-L1 in pre-treatment biopsies and post-treatment surgical specimens, which would indeed be of relevance in future studies.
Conclusion
This study is, to the best of our knowledge, the first to demonstrate that the prognostic impact of PD-L1 and PD-1 expression differs according to primary tumour site in CRC. Dense infiltration of PD-L1+ immune cells was an independent prognostic factor in right-sided and left-sided colon cancer, but not in rectal cancer. These results need validation, but may be clinically relevant, as they indicate that tumour location might be an important factor to take into consideration in therapeutic decisions, including eligibility for immunotherapy.
Patients and methods
Patients
The study cohort consists of all incident cases of CRC in the Malmö Diet and Cancer Study from 1991 up until December 31st 2008 (n = 626), from which 557 cases were available for TMA construction.Citation14,Citation15,Citation54,Citation55 The Malmö Diet and Cancer Study is a prospective population-based cohort with the primary aim to investigate associations between various dietary factors and cancer incidence.Citation56 The project, including non- participants in the European Prospective Investigation into Cancer (EPIC) cohort, enrolled 18326 women (60.2%) and 12120 (39.8%) men, with a total of 30446 participants (from a background population of 74,138).
Information on CRC incidence was obtained through the Swedish Cancer Registry up until 31 December 2007, and from The Southern Swedish Regional Tumour Registry for the period of 1 January – 31 December 2008. Clinical and treatment data were obtained from medical charts. Histopathological data were obtained from pathology records. TNM staging was performed according to the American Joint Committee on Cancer. Right colon was defined as appendix, caecum, ascending and 2/3 of transverse colon, whereas left colon was defined as the left colic flexure, descending and sigmoid colon, corresponding to the midgut fetal origin versus the hindgut as well as different innervation and blood supply.
Median age at diagnosis was 71 (range 50 – 86) years. Information on vital status and cause of death was obtained from the Swedish Cause of Death Registry up until 31 December 2013. Follow-up began at CRC diagnosis and ended at death, emigration or 31 December 2013, whichever came first. Median follow-up time was 5.97 (range 0–21.69) years for the full cohort (n = 626) and 10.05 (range 5.03- 21.69) years for patients alive (n = 274). MSI screening status was assessed by IHC as previously described,Citation57 and KRAS and BRAF mutation status was determined by pyrosequencing as previously described.Citation58
All EU and national regulations and requirements for handling human samples have been fully complied with during the conduct of this project; i.e. decision no. 1110/94/EC of the European Parliament and of the Council (OJL126 18,5,94), the Helsinki Declaration on ethical principles for medical research involving human subjects, and the EU Council Convention on human rights and Biomedicine. The study was approved of by the Ethics committee of Lund University (ref nr 51/90, 445/07 and 530/08). Written informed consent has been obtained from each subject.
Tissue microarray construction
All tumours with available slides or paraffin blocks were histopathologically re-evaluated on haematoxylin and eosin stained slides by a senior pathologist (KJ). Cases with an insufficient amount of tumour material were excluded, whereby a total number of 557 (89.0%) cases were available for TMA construction. Representative and non-necrotic areas were marked, and TMAs were constructed with duplicate tissue cores (1 mm) taken from each primary tumour and mounted in a recipient block, using a semi-automated arraying device (TMArrayer, Pathology Devices, Westminister, MD, USA). Four µm sections from this block were subsequently cut using a microtome and mounted on glass slides.
Immunohistochemistry
For IHC analysis of PD-L1, 4 μm TMA-sections were pre-treated with Flex TRS High, pH 9, and subsequently stained in an Autostainer Plus (Dako; Glostrup, Denmark) with the anti-PD-L1 antibody (clone E1L3N, rabbit, dilution 1:200, Cell Signalling Technologies, Danvers, MA 01923, USA). For analysis of PD-1, TMA-sections were pre-treated using Flex TRS Low, pH 6,1, and stained with the anti-PD-1-antibody (ab52587, clone NAT105, mouse, dilution 1:50, AbCam; Cambridge, UK). Endothelial cells and normal colonic mucosa were used as negative internal controls. The density of B cells (CD20+), plasma cells (CD138+, IGKC+) and T lymphocytes (CD3+, CD8+, FoxP3+) was analysed as previously described.Citation14,Citation15
Evaluation of PD-1 and PD-L1 expression
Immune cell-specific PD-L1 and PD-1 expression was annotated as the estimated percentage of stained cells and categorized as 0–9%, 10–49% and 50–100% stained immune cells. PD-L1 expression on tumour cells was annotated as the estimated percentage of stained cells and categorized as < 1%, 1–4%, 5–9%, 10–49%, and 50–100% stained tumour cells. Cells with linear membranous staining were counted as positive. Staining intensity was not accounted for, as only minor variations were observed. For PD-1 expression, the total number of positive immune cells was also counted. The annotated score in the TMA was also compared with whole tissue sections by blinded analysis of 15 cases with 5 representing each category of PD-1 expression in immune cells, and 25 cases with 5 cases representing each category of PD-L1 expression in tumour cells and 7, 7, and 11 cases, respectively, of categories 0, 1, and 2 for PD-L1+ immune cells.
All stainings were evaluated independently by two observers (KJ and JB) blinded to clinical outcome, one being a board-certified pathologist (KJ). Discrepant cases were re-evaluated and discussed in order to reach consensus.
Statistical analysis
Chi-square tests and Mann Whitney U tests were used to evaluate associations between categories of PD-1 and PD-L1 expression and established clinicopathological characteristics and other investigative biomarkers. Kaplan-Meier analysis and log rank test were applied to illustrate differences in five-year OS with respect to categories of PD-1 and PD-L1 expression. CRT analysis was applied to determine the optimal prognostic cut-off for PD-1+ immune cell count. Cox regression proportional hazard models were used to estimate hazard ratios for death within 5 years in both univariable and multivariable analysis, adjusted for age, sex, T-stage, N-stage, M-stage, differentiation grade, and vascular invasion.
The proportional hazard assumption was tested using Cox regression with a time-dependent covariate analysis, whereby the proportional hazard assumption was considered to be satisfied when the factor x time interaction was non-significant.
To estimate the interaction effect between tumour location and PD-1 and PD-L1 expression, an interaction variable was constructed with tumour location (right/other, left/other, or rectal/other, respectively) x immune cell-specific PD-1 or PD-L1 expression, or tumour cell-specific PD-L1 expression, respectively (low/high).
All calculations were performed using SPSS version 24.0 (SPSS Inc, Chicago, IL). All statistical tests were two-sided and p-values < 0.05 were considered statistically significant.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
2018ONCOIMM0062R-file006.docx
Download MS Word (152.3 KB)Additional information
Funding
References
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. PMID:25651787.
- Keir ME, Butte MJ, Freeman GJ, Sharpe AH. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. 2008;26:677–704. doi:10.1146/annurev.immunol.26.021607.090331. PMID:18173375.
- Gordon SR, Maute RL, Dulken BW, Hutter G, George BM, McCracken MN, Gupta R, Tsai JM, Sinha R, Corey D, et al. PD-1 expression by tumour-associated macrophages inhibits phagocytosis and tumour immunity. Nature. 2017;545(7655):495–9. doi:10.1038/nature22396. PMID:28514441.
- Lim TS, Chew V, Sieow JL, Goh S, Yeong JP, Soon AL, Ricciardi-Castagnoli P. PD-1 expression on dendritic cells suppresses CD8(+) T cell function and antitumor immunity. Oncoimmunology. 2016;5(3):e1085146. doi:10.1080/2162402X.2015.1085146. PMID:27141339.
- Francisco LM, Sage PT, Sharpe AH. The PD-1 pathway in tolerance and autoimmunity. Immunol Rev. 2010;236:219–42. doi:10.1111/j.1600-065X.2010.00923.x. PMID:20636820.
- Nomi T, Sho M, Akahori T, Hamada K, Kubo A, Kanehiro H, Nakamura S, Enomoto K, Yagita H, Azuma M, et al. Clinical significance and therapeutic potential of the programmed death-1 ligand/programmed death-1 pathway in human pancreatic cancer. Clinical cancer research : an official journal of the American Association for Cancer Research. 2007;13(7):2151–7. doi:10.1158/1078-0432.CCR-06-2746. PMID:17404099.
- Muenst S, Schaerli AR, Gao F, Daster S, Trella E, Droeser RA, et al. Expression of programmed death ligand 1 (PD-L1) is associated with poor prognosis in human breast cancer. Breast Cancer Res Treat. 2014;146(1):15–24. doi:10.1007/s10549-014-2988-5. PMID:24842267.
- Thompson RH, Gillett MD, Cheville JC, Lohse CM, Dong H, Webster WS, Krejci KG, Lobo JR, Sengupta S, Chen L, et al. Costimulatory B7-H1 in renal cell carcinoma patients: Indicator of tumor aggressiveness and potential therapeutic target. PNAS. 2004;101(49):17174–9. doi:10.1073/pnas.0406351101. PMID:15569934.
- Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age. Nature. 2011;480(7378):480–9. doi:10.1038/nature10673. PMID:22193102.
- Restifo NP, Dudley ME, Rosenberg SA. Adoptive immunotherapy for cancer: harnessing the T cell response. Nat Rev Immunol. 2012;12(4):269–81. doi:10.1038/nri3191. PMID:22437939.
- Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–54. doi:10.1056/NEJMoa1200690. PMID:22658127.
- Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, Desai J, Hill A, Axelson M, Moss RA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. 2017;18(9):1182–91. doi:10.1016/S1470-2045(17)30422-9. PMID:28734759.
- Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015;372(26):2509–20. doi:10.1056/NEJMoa1500596. PMID:26028255.
- Berntsson J, Svensson MC, Leandersson K, Nodin B, Micke P, Larsson AH, Eberhard J, Jirström K. The clinical impact of tumour-infiltrating lymphocytes in colorectal cancer differs by anatomical subsite: A cohort study. Int J Cancer. 2017;141(8):1654–66. doi:10.1002/ijc.30869. PMID:28677162.
- Berntsson J, Nodin B, Eberhard J, Micke P, Jirstrom K. Prognostic impact of tumour-infiltrating B cells and plasma cells in colorectal cancer. Int J Cancer. 2016;139(5):1129–39. doi:10.1002/ijc.30138. PMID:27074317.
- Wang L, Ren F, Wang Q, Baldridge LA, Monn MF, Fisher KW, Sheng W, Zhou X, Du X, Cheng L. Significance of Programmed Death Ligand 1 (PD-L1) Immunohistochemical Expression in Colorectal Cancer. Mol Diagn Ther. 2016;20(2):175–81. doi:10.1007/s40291-016-0188-1..
- Li Y, Liang L, Dai W, Cai G, Xu Y, Li X, Li Q, Cai S. Prognostic impact of programed cell death-1 (PD-1) and PD-ligand 1 (PD-L1) expression in cancer cells and tumor infiltrating lymphocytes in colorectal cancer. Mol Cancer. 2016;15(1):55. doi:10.1186/s12943-016-0539-x. PMID:27552968.
- Droeser RA, Hirt C, Viehl CT, Frey DM, Nebiker C, Huber X, Zlobec I, Eppenberger-Castori S, Tzankov A, Rosso R, et al. Clinical impact of programmed cell death ligand 1 expression in colorectal cancer. European journal of cancer (Oxford, England : 1990). 2013;49(9):2233–42. doi:10.1016/j.ejca.2013.02.015. PMID:23478000.
- Lee KS, Kwak Y, Ahn S, Shin E, Oh HK, Kim DW, Kang SB, Choe G, Kim WH, Lee HS. Prognostic implication of CD274 (PD-L1) protein expression in tumor-infiltrating immune cells for microsatellite unstable and stable colorectal cancer. Cancer Immunol Immunother : CII. 2017;66(7):927–39. doi:10.1007/s00262-017-1999-6. PMID:28405764.
- Lee LH, Cavalcanti MS, Segal NH, Hechtman JF, Weiser MR, Smith JJ, Garcia-Aguilar J, Sadot E, Ntiamoah P, Markowitz AJ, et al. Patterns and prognostic relevance of PD-1 and PD-L1 expression in colorectal carcinoma. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2016;29(11):1433–42. doi:10.1038/modpathol.2016.139. PMID:27443512.
- Kollmann D, Schweiger T, Schwarz S, Ignatova D, Chang YT, Lewik G, Schoppmann SF, Hoetzenecker W, Klepetko W, Guenova E, et al. PD1-positive tumor-infiltrating lymphocytes are associated with poor clinical outcome after pulmonary metastasectomy for colorectal cancer. Oncoimmunology. 2017;6(9):e1331194. doi:10.1080/2162402X.2017.1331194. PMID:28932634.
- Hecht M, Buttner-Herold M, Erlenbach-Wunsch K, Haderlein M, Croner R, Grutzmann R, Hartmann A, Fietkau R, Distel LV. PD-L1 is upregulated by radiochemotherapy in rectal adenocarcinoma patients and associated with a favourable prognosis. European journal of cancer (Oxford, England : 1990). 2016;65:52–60. doi:10.1016/j.ejca.2016.06.015. PMID:27468145.
- Lee GH, Malietzis G, Askari A, Bernardo D, Al-Hassi HO, Clark SK. Is right-sided colon cancer different to left-sided colorectal cancer? – a systematic review. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2015;41(3):300–8. doi:10.1016/j.ejso.2014.11.001. PMID:25468456.
- Gervaz P, Bucher P, Morel P. Two colons-two cancers: paradigm shift and clinical implications. J Surg Oncol. 2004;88(4):261–6. doi:10.1002/jso.20156. PMID:15565587.
- Hansen IO, Jess P. Possible better long-term survival in left versus right-sided colon cancer – a systematic review. Dan Med J. 2012;59(6):A4444. PMID:22677242.
- Holch JW, Ricard I, Stintzing S, Modest DP, Heinemann V. The relevance of primary tumour location in patients with metastatic colorectal cancer: A meta-analysis of first-line clinical trials. European journal of cancer (Oxford, England : 1990). 2017;70:87–98. doi:10.1016/j.ejca.2016.10.007. PMID:27907852.
- Sunakawa Y, Ichikawa W, Tsuji A, Denda T, Segawa Y, Negoro Y, Shimada K, Kochi M, Nakamura M, Kotaka M, et al. Prognostic Impact of Primary Tumor Location on Clinical Outcomes of Metastatic Colorectal Cancer Treated With Cetuximab Plus Oxaliplatin-Based Chemotherapy: A Subgroup Analysis of the JACCRO CC-05/06 Trials. Clin Colorectal Cancer. 2017;16(3):e171−e80. doi:10.1016/j.clcc.2016.09.010. PMID:27856123.
- Boeckx N, Koukakis R, Op de Beeck K, Rolfo C, Van Camp G, Siena S, Tabernero J, Douillard JY, André T, Peeters M. Primary tumor sidedness has an impact on prognosis and treatment outcome in metastatic colorectal cancer: results from two randomized first-line panitumumab studies. Annals of oncology : official journal of the European Society for Medical Oncology. 2017;28(8):1862–8. doi:10.1093/annonc/mdx119. PMID:28449055.
- Arnold D, Lueza B, Douillard JY, Peeters M, Lenz HJ, Venook A, Heinemann V, Van Cutsem E, Pignon JP, Tabernero J, et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Annals of oncology : official journal of the European Society for Medical Oncology. 2017;28(8):1713–29. doi:10.1093/annonc/mdx175. PMID:28407110.
- Frey DM, Droeser RA, Viehl CT, Zlobec I, Lugli A, Zingg U, Oertli D, Kettelhack C, Terracciano L, Tornillo L. High frequency of tumor-infiltrating FOXP3(+) regulatory T cells predicts improved survival in mismatch repair-proficient colorectal cancer patients. Int J Cancer. 2010;126(11):2635–43. PMID:19856313.
- Salama P, Phillips M, Grieu F, Morris M, Zeps N, Joseph D, Platell C, Iacopetta B. Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2009;27(2):186–92. doi:10.1200/JCO.2008.18.7229. PMID:19064967.
- Kim HR, Ha SJ, Hong MH, Heo SJ, Koh YW, Choi EC, et al. PD-L1 expression on immune cells, but not on tumor cells, is a favorable prognostic factor for head and neck cancer patients. Sci Rep. 2016;6:36956. doi:10.1038/srep36956. PMID:27841362.
- Webb JR, Milne K, Kroeger DR, Nelson BH. PD-L1 expression is associated with tumor-infiltrating T cells and favorable prognosis in high-grade serous ovarian cancer. Gynecol Oncol. 2016;141(2):293–302. doi:10.1016/j.ygyno.2016.03.008. PMID:26972336.
- Cho J, Lee J, Bang H, Kim ST, Park SH, An JY, Choi MG, Lee JH, Sohn TS, Bae JM, et al. Programmed cell death-ligand 1 expression predicts survival in patients with gastric carcinoma with microsatellite instability. Oncotarget. 2017;8(8):13320–8. doi:10.18632/oncotarget.14519. PMID:28076847.
- Thompson RH, Dong H, Lohse CM, Leibovich BC, Blute ML, Cheville JC, et al. PD-1 is expressed by tumor-infiltrating immune cells and is associated with poor outcome for patients with renal cell carcinoma. Clinical cancer research : an official journal of the American Association for Cancer Research. 2007;13(6):1757–61. doi:10.1158/1078-0432.CCR-06-2599. PMID:17363529.
- Hirano F, Kaneko K, Tamura H, Dong H, Wang S, Ichikawa M, Rietz C, Flies DB, Lau JS, Zhu G, et al. Blockade of B7-H1 and PD-1 by monoclonal antibodies potentiates cancer therapeutic immunity. Cancer Res. 2005;65(3):1089–96. PMID:15705911.
- Iwai Y, Ishida M, Tanaka Y, Okazaki T, Honjo T, Minato N. Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade. PNAS. 2002;99(19):12293–7. doi:10.1073/pnas.192461099. PMID:12218188.
- Herbst RS, Soria JC, Kowanetz M, Fine GD, Hamid O, Gordon MS, Sosman JA, McDermott DF, Powderly JD, Gettinger SN, et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature. 2014;515(7528):563–7. doi:10.1038/nature14011. PMID:25428504.
- Taube JM, Klein A, Brahmer JR, Xu H, Pan X, Kim JH, Chen L, Pardoll DM, Topalian SL, Anders RA. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clinical cancer research : an official journal of the American Association for Cancer Research. 2014;20(19):5064–74. doi:10.1158/1078-0432.CCR-13-3271. PMID:24714771.
- Juneja VR, McGuire KA, Manguso RT, LaFleur MW, Collins N, Haining WN, Freeman GJ, Sharpe AH. PD-L1 on tumor cells is sufficient for immune evasion in immunogenic tumors and inhibits CD8 T cell cytotoxicity. J Exp Med. 2017;214(4):895–904. doi:10.1084/jem.20160801. PMID:28302645.
- Kleinovink JW, Marijt KA, Schoonderwoerd MJA, van Hall T, Ossendorp F, Fransen MF. PD-L1 expression on malignant cells is no prerequisite for checkpoint therapy. Oncoimmunology. 2017;6(4):e1294299. doi:10.1080/2162402X.2017.1294299. PMID:28507803.
- Noguchi T, Ward JP, Gubin MM, Arthur CD, Lee SH, Hundal J, Selby MJ, Graziano RF, Mardis ER, Korman AJ, et al. Temporally Distinct PD-L1 Expression by Tumor and Host Cells Contributes to Immune Escape. Cancer Immunol Res. 2017;5(2):106–17. doi:10.1158/2326-6066.CIR-16-0391. PMID:28073774.
- Powles T, Eder JP, Fine GD, Braiteh FS, Loriot Y, Cruz C, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515(7528):558–62. doi:10.1038/nature13904. PMID:25428503.
- Masugi Y, Nishihara R, Yang J, Mima K, da Silva A, Shi Y, Inamura K, Cao Y, Song M, Nowak JA, et al. Tumour CD274 (PD-L1) expression and T cells in colorectal cancer. Gut. 2017;66(8):1463–73. doi:10.1136/gutjnl-2016-311421. PMID:27196573.
- Rosenbaum MW, Bledsoe JR, Morales-Oyarvide V, Huynh TG, Mino-Kenudson M. PD-L1 expression in colorectal cancer is associated with microsatellite instability, BRAF mutation, medullary morphology and cytotoxic tumor-infiltrating lymphocytes. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2016;29(9):1104–12. doi:10.1038/modpathol.2016.95. PMID:27198569.
- Brunnstrom H, Johansson A, Westbom-Fremer S, Backman M, Djureinovic D, Patthey A, Isaksson-Mettävainio M, Gulyas M, Micke P. PD-L1 immunohistochemistry in clinical diagnostics of lung cancer: inter-pathologist variability is higher than assay variability. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2017;30(10):1411–21. doi:10.1038/modpathol.2017.59. PMID:28664936.
- Wu Y, Cao D, Qu L, Cao X, Jia Z, Zhao T, Wang Q, Jiang J. PD-1 and PD-L1 co-expression predicts favorable prognosis in gastric cancer. Oncotarget. 2017;8(38):64066–82. doi:10.18632/oncotarget.19318. PMID:28969052.
- Darb-Esfahani S, Kunze CA, Kulbe H, Sehouli J, Wienert S, Lindner J, Budczies J, Bockmayr M, Dietel M, Denkert C, et al. Prognostic impact of programmed cell death-1 (PD-1) and PD-ligand 1 (PD-L1) expression in cancer cells and tumor-infiltrating lymphocytes in ovarian high grade serous carcinoma. Oncotarget. 2016;7(2):1486–99. doi:10.18632/oncotarget.6429. PMID:26625204.
- Badoual C, Hans S, Merillon N, Van Ryswick C, Ravel P, Benhamouda N, Levionnois E, Nizard M, Si-Mohamed A, Besnier N, et al. PD-1-expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2013;73(1):128–38. doi:10.1158/0008-5472.CAN-12-2606. PMID:23135914.
- Yamauchi M, Morikawa T, Kuchiba A, Imamura Y, Qian ZR, Nishihara R, Liao X, Waldron L, Hoshida Y, Huttenhower C, et al. Assessment of colorectal cancer molecular features along bowel subsites challenges the conception of distinct dichotomy of proximal versus distal colorectum. Gut. 2012;61(6):847–54. doi:10.1136/gutjnl-2011-300865. PMID:22427238.
- Li FY, Lai MD. Colorectal cancer, one entity or three. Journal of Zhejiang University Science B. 2009;10(3):219–29. doi:10.1631/jzus.B0820273. PMID:19283877.
- Sheng J, Fang W, Yu J, Chen N, Zhan J, Ma Y, et al. Expression of programmed death ligand-1 on tumor cells varies pre and post chemotherapy in non-small cell lung cancer. Sci Rep. 2016;6:20090. doi:10.1038/srep20090. PMID:26822379.
- Zhang P, Su DM, Liang M, Fu J. Chemopreventive agents induce programmed death-1-ligand 1 (PD-L1) surface expression in breast cancer cells and promote PD-L1-mediated T cell apoptosis. Mol Immunol. 2008;45(5):1470–6. doi:10.1016/j.molimm.2007.08.013. PMID:17920123.
- Larsson A, Johansson ME, Wangefjord S, Gaber A, Nodin B, Kucharzewska P, Welinder C, Belting M, Eberhard J, Johnsson A, et al. Overexpression of podocalyxin-like protein is an independent factor of poor prognosis in colorectal cancer. Br J Cancer. 2011;105(5):666–72. doi:10.1038/bjc.2011.295. PMID:21829192.
- Eberhard J, Gaber A, Wangefjord S, Nodin B, Uhlen M, Ericson Lindquist K, Jirström K. A cohort study of the prognostic and treatment predictive value of SATB2 expression in colorectal cancer. Br J Cancer. 2012;106(5):931–8. doi:10.1038/bjc.2012.34. PMID:22333599.
- Berglund G, Elmstahl S, Janzon L, Larsson SA. The Malmo Diet and Cancer Study. Design and feasibility. J Intern Med. 1993;233(1):45–51. doi:10.1111/j.1365-2796.1993.tb00647.x. PMID:8429286.
- Wangefjord S, Brandstedt J, Lindquist KE, Nodin B, Jirstrom K, Eberhard J. Associations of beta-catenin alterations and MSI screening status with expression of key cell cycle regulating proteins and survival from colorectal cancer. Diagn Pathol. 2013;8:10. doi:10.1186/1746-1596-8-10. PMID:23337059.
- Wangefjord S, Sundstrom M, Zendehrokh N, Lindquist KE, Nodin B, Jirstrom K, Eberhard J. Sex differences in the prognostic significance of KRAS codons 12 and 13, and BRAF mutations in colorectal cancer: a cohort study. Biol Sex Differ. 2013;4(1):17. doi:10.1186/2042-6410-4-17. PMID:24020794.