Abstract
Purpose: Although it is widely accepted that physical activity (PA) positively, and screen-based media use (SBM) negatively, affects well-being, there is a lack of studies relating PA and SBM to health-related quality of life (HRQoL) in adolescents. We examined these associations in German adolescents for different HRQoL subdomains and explored the role of body satisfaction as a possible mediator. Methods: The 11–17-year-old subsample of the German Health Interview and Examination Survey (2003–2006) was analysed (N = 6813; 51.3% male). Cross-sectional associations of self-reported PA frequency and amount of daily SBM with HRQoL subscale scores (according to KINDL-R) were examined by hierarchical linear regression models, adjusting for the clustering of the sample and for a variety of possible confounders. The size and significance of indirect effects via body (dis)satisfaction (BDS) were examined by mediation analyses. Results: Higher PA frequency was significantly associated with higher HRQoL on nearly all subscales and dose–response-relationships were observable. Variations were greatest in terms of social well-being in boys (effect size d = 0.59) and physical well-being in girls (d = 0.43). Higher SBM was related to lower HRQoL on all subscales in girls and on some subscales in boys, with the largest effects for school functioning in both genders (d = 0.31 and 0.37, respectively). The mediated effects for PA and SBM were significant in both genders, but the sizes and the proportions of total effects mediated by body satisfaction were rather small. Conclusions: Higher PA frequency was associated with higher self-reported HRQoL, and higher SBM was associated with lower self-reported HRQoL in both genders, even after adjusting for relevant covariates. The results support the assumption of independent health impacts of both behaviours, although no causal relationship can be confirmed with these cross-sectional data. Mechanisms other than body satisfaction must largely account for the effects of PA and SBM on well-being.
1. Background
A prevailing sedentary lifestyle consisting of insufficient physical activity (PA) and high levels of sedentary behaviours such as screen-based media use (SBM) substantially accounts for the burden of many non-communicable diseases, including cardiovascular diseases, type 2 diabetes, and some cancers (Lee et al., Citation2012; Proper, Singh, van Mechelen, & Chinapaw, Citation2011).
Children and adolescents in general are the most physically active and healthiest subset of the population. Nevertheless, many youths do not meet current recommendations for PA, and a majority of youths in various countries exceed the recommended maximum amount of SBM of 2 h per day (Currie et al., Citation2012).
Although numerous studies have focused on the physical health benefits of an active lifestyle, subjective perceptions of health and well-being have attracted growing attention in recent decades. Because most non-communicable diseases are less likely in children and adolescents (Boreham & Riddoch, Citation2003), indicators of subjective well-being, such as health-related quality of life (HRQoL), play an especially important role in this age group. Moreover, subjective health complaints and low quality of life are common in adolescents and increase during teenage years (Ravens-Sieberer et al., Citation2009).
HRQoL relates to a person's self-perceived health and consists of ratings of well-being and functionality in important life areas, including physical well-being/functioning, emotional well-being, self-esteem, social functioning, and family relations (Ravens-Sieberer, Erhart, Wille, Bullinger, & the BELLA study group, Citation2008). HRQoL can help in identifying subgroups at higher risk for health problems and in detecting impairments in well-being and functioning early (Ravens-Sieberer et al., Citation2008).
It is widely accepted that PA leads to better well-being, although causality has not been sufficiently proven (Bize, Johnson, & Plotnikoff, Citation2007). Studies in children and adolescents have revealed that PA is related to mental health indicators such as depressive symptoms, anxiety, self-esteem, and cognitive functioning, as evidenced by a recent review of reviews. Furthermore, primary studies on SBM that were also reviewed found negative associations with indicators of mental health (Biddle & Asare, Citation2011). The latter was also observed for self-esteem (Tremblay et al., Citation2011). Studies relating PA or SBM to comprehensive measures of HRQoL in adolescents of the general population, however, are sparse.
Although some research on PA has found that more active adolescents reported notably higher HRQoL than those who were less active (Sanchez-Lopez et al., Citation2009), others found quite low (Breslin et al., Citation2012; Spengler & Woll, Citation2012) or no (Boyle, Jones, & Walters, Citation2010) associations of PA with HRQoL among children or adolescents. Studies that analysed both PA and SBM typically found that PA is positively, and SBM is negatively, related to different HRQoL measures (Chen et al., Citation2005; Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, Janssen, & Boyce, Citation2009; Lacy et al., Citation2012; Mathers et al., Citation2009).
One possible mechanism through which PA or SBM may influence HRQoL is an effect on body satisfaction that subsequently leads to higher self-esteem and well-being (Biddle, Fox, Boutcher, & Faulkner, Citation2000; Rejeski et al., Citation2001). In fact, a recent meta-analysis concluded that exercisers report having a better body image and that exercising interventions lead to improvements in body image (Hausenblas & Fallon, Citation2006). Higher body satisfaction, moreover, is one motive to participate in PA that is frequently expressed by adolescents (Tergerson & King, Citation2002).
However, evidence regarding the relationship of PA with body satisfaction in adolescents is inconclusive (Breslin et al., Citation2012; Fairclough, Ridgers, & Welk, Citation2012; Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009). On the other hand, strong associations between body satisfaction and HRQoL were confirmed in previous studies on adolescents (Jansen, van de Looij-Jansen, de Wilde, & Brug, Citation2008; Mond, van den Berg, Boutelle, Hannan, & Neumark-Sztainer, Citation2011).
For SBM, it has also been supposed that high exposure to media images of ideal bodies may be one factor that leads to body dissatisfaction (BDS), especially in girls, through internalising these media images and making self-comparisons with these ideals (Ricciardelli, McCabe, Holt, & Finemore, Citation2003). However, studies relating SBM to physical self-concept or body satisfaction have found inconsistent results. For example, Iannotti, Janssen, et al. (Citation2009) discovered small negative relations between SBM and body satisfaction among large adolescent samples from North America and Europe, but in other studies, this association was not found or was found only in subsamples (Iannotti, Kogan, et al., Citation2009; Nihill, Lubans, & Plotnikoff, Citation2013; Racine, DeBate, Gabriel, & High, Citation2011).
Both PA and SBM are different aspects of an inactive lifestyle and are independently related to health and well-being (Janssen & LeBlanc, Citation2010; Tremblay et al., 2011). Most previous studies on HRQoL in adolescents are limited in that they only considered PA or SBM (Boyle et al., Citation2010; Breslin et al., Citation2012; Mathers et al., Citation2009; Sanchez-Lopez et al., Citation2009; Spengler & Woll, Citation2012) or that they did not adjust for associations with other potentially important covariates, such as biological maturity, body satisfaction, and risk behaviours (Chen et al., Citation2005; Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009; Lacy et al., Citation2012). Some studies that included a variety of possible confounders focused on more specific aspects of adolescents' well-being, such as self-esteem (Nihill et al., Citation2013; Schmalz, Deane, Birch, & Davison, Citation2007) or mental health (Ussher, Owen, Cook, & Whincup, Citation2007). With the exception of a few studies (Breslin et al., Citation2012; Chen et al., Citation2005; Sanchez-Lopez et al., Citation2009), we could not find research that related PA or SBM to different HRQoL subdomains in their analyses.
The aim of the present paper was to further explore the relationships of SBM and PA with different HRQoL subdomains in a representative sample of German adolescents, taking into account a variety of possible covariates. We expected that PA would be positively, and SBM negatively, related to HRQoL. Body satisfaction was examined as a possible mediator of these relationships. We supposed that potential mediation effects would be strongest for self-esteem among all HRQoL domains.
2. Methods
2.1 Sample and procedures
The data stemmed from the representative German Health Interview and Examination Survey (KiGGS) (Robert Koch-Institut, Citation2008). The aims and methodology of this comprehensive survey comprising verbal and written inquiries and a medical examination are described in detail elsewhere (Kurth et al., Citation2008). In brief, a total of 17,641 boys and girls aged 0–17 years and their parents participated in the survey from May 2003 to May 2006. A stratified multistage probability sample representative of this age group in Germany was obtained from 167 local study centres (sample points). Invited participants were randomly sampled from population registries. The overall response rate was 66.6%. Most non-responders had missed the scheduled appointment with no explanation or were children who refused participation. Analysis of a short non-responder questionnaire revealed very few differences between responders and non-responders in terms of health-relevant variables and indicated good representativeness on the health of children and adolescents living in Germany. Deviations of the net sample from the population structure in terms of age, gender, nationality, and region were corrected by sampling weights (Kurth et al., Citation2008). The present analyses were restricted to adolescents aged 11–17 years (N = 6813; 51.3% male), for whom self-reported PA, SBM, body satisfaction, and HRQoL were assessed. The study was approved by the Charité/Universitätsmedizin Berlin ethics committee and the Federal Office for the Protection of Data.
2.2 Measures
All measures were developed considering established instruments and adapted to the conditions and necessities of the KiGGS survey. All employed instruments were extensively pretested and validated, and the quality of the study was monitored throughout all phases (Kurth et al., Citation2008).
2.2.1 Independent variables
Physical activity. Boys and girls were asked how often they were physically active enough in their leisure time that they sweated or breathed hard. Possible answers were: ‘about every day’, ‘about 3–5 times a week’, ‘about once or twice a week’, ‘about once or twice a month’, or ‘never’. Because the last two categories were rare (5.5% and 10.0%, respectively), they were combined to ‘no regular PA’ (reference) for the analyses. There are no reliability data available for the analysed sample. Other studies, however, showed moderate to good retest reliability for different time periods and supported validity for similar items in other studies on adolescents (Booth, Okely, Chey, & Bauman, Citation2001; Prochaska, Sallis, & Long, Citation2001).
Screen-based media use. The questionnaire asked for the average amount of daily time spent with different screen media (TV/videos, computer/Internet, and gaming consoles). An index for screen time was formed: for TV, computer, and gaming consoles, individual answers were scored with 0 (‘not at all’), 0.5 (‘about half an hour’), 1.5 (‘about 1–2 h’), 3.5 (‘about 3–4 h’), and 5 (‘more than 4 h’) and summed up across these media. The total screen time index was only computed for adolescents with valid answers for all three media. Because the distribution of the SBM index was skewed and to harmonise the analyses, SBM was classified into four groups: below 2 h per day (used as the reference category in the analyses), 2–<3 h/day, 3–<4.5 h/day, and ≥4.5 h/day. Similar SBM items have shown good retest reliability and good criterion-related validity in other applications with adolescent samples (Schmitz et al., Citation2004; Utter, Neumark-Sztainer, Jeffery, & Story, Citation2003). Concerning TV, in our sample, parallel items were answered by parents of 11–13 year olds, and these were plainly correlated with self-reported scores (r = 0.51 and 0.57 for boys and girls, respectively).
2.2.2 Dependent variables
Health-related quality of life. HRQoL was measured with age-specific self-report versions of the revised German KINDL-R questionnaire (Ravens-Sieberer & Bullinger, Citation2000). KINDL-R is a generic HRQoL measure that covers six dimensions of HRQoL with reference to the previous week: physical (e.g. ‘I felt ill’) and emotional well-being (e.g. ‘I had fun and laughed a lot’), self-esteem (e.g. ‘I was proud of myself’), family (e.g. ‘I got along well with my parents’), friends (e.g. ‘I got along well with my friends’), and school (e.g. ‘Doing the schoolwork was easy’). Each dimension was measured by four items and transformed to a score in the range of 0 (lowest HRQoL) to 100 (highest HRQoL). The KINDL-R showed acceptable reliability and validity in different applications, including the KiGGS sample (Bullinger, Brutt, Erhart, & Ravens-Sieberer, Citation2008). For the sample analysed here, Cronbach's alpha was α = 0.82 for the HRQoL total score and, for the subscales, ranged from α = 0.54 for the subscale school to α = 0.73 for family.
Body (dis)satisfaction. To assess BDS, adolescents were asked whether they thought of themselves as ‘much too thin’, ‘slightly too thin’, ‘about the right size’, ‘slightly too fat’, or ‘much too fat’. Because of small group sizes for the extreme categories, the groups were merged to the three categories ‘(much) too thin’, ‘(much) too fat’, and ‘right weight’ (reference category). This item was also used in the international health behaviour in school-aged children survey and showed good retest reliability for a two-week interval (Griebler et al., Citation2010).
2.2.3 Covariates
Research indicates that factors often associated with PA and/or SBM and indicators of well-being include weight status (Griffiths, Parsons, & Hill, Citation2010; Marshall, Biddle, Gorely, Cameron, & Murdey, Citation2004), biological maturity (Hunter Smart et al., Citation2012), sleep (Chen et al., Citation2005; Nelson & Gordon-Larsen, Citation2006), risk behaviours such as smoking and alcohol use (Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009; Nelson & Gordon-Larsen, Citation2006), and socio-demographic variables such as age, socio-economic status (SES), gender, and ethnicity (Van Der Horst, Paw, Twisk, & Van Mechelen, Citation2007). These variables were therefore included as potential covariates or, in case of gender, moderators in our analyses.
Socio-demographic measures. SES and ethnicity were assessed with parent questionnaires. SES was based on parents' education, occupation, and household income (Lange et al., Citation2007). Children whose parents were both immigrants and those who were immigrants themselves and had at least one parent of non-German descent were classified as immigrants (Schenk, Ellert, & Neuhauser, Citation2007) and compared with children of German descent (reference category). Other parameters considered were decimal age and gender.
Anthropometric measures. Standing height was measured to the nearest centimetre using a rigid stadiometer. Weight was measured, with the subjects in their underwear, to the nearest 0.1 kg using a calibrated balance scale. Body weight was quantified using Cole's least mean square method expressing body mass index (BMI) as a standard deviation score (zBMI) (Cole, Citation1990) using age- and gender-specific reference data for German children (Kromeyer-Hauschild et al., Citation2001).
Biological maturity. The percentage of adult stature was estimated using the Khamis–Roche method (Khamis & Roche, Citation1994). This measure is based on the actual height and weight of the child and the (self-reported) height of the parents. Age- and gender-specific continuous z-scores of the percentage of adult height already reached were calculated as a measure of maturity relative to same-aged peers (maturational timing).
Smoking. Adolescents were asked if and how often they currently smoked cigarettes. Those who indicated smoking at least sometimes were classified as ‘smoking’ and compared with those who indicated that they were non-smokers (reference category).
Alcohol. Adolescents self-reported whether they had ever drunk alcohol. If ‘yes’, they indicated how many glasses of beer, wine, and/or hard liquor they currently drank. Girls and boys who consumed beer, wine, and/or hard liquor once per week or more frequently were classified as ‘regular drinkers’ compared with those who drank less (reference category).
Sleeping hours. Participants were asked to estimate how many hours they had spent sleeping the night before examination day, and this was used as a continuous measure.
2.3 Statistical analyses
Descriptive statistics were computed and compared between genders using independent t-tests and χ2-tests. To describe associations between PA and SBM, τc rank order correlations were computed. All descriptive statistics were computed using Stata/IC 12.1 (StataCorp LP, College Station, TX, USA) taking into account the clustering of the survey by using robust standard errors adjusted for clustering and by using sampling weights to adjust for deviations from representativeness. For analysing the associations between PA and SBM with HRQoL and BDS, the nested structure of the sample was accounted for by computing hierarchical regression models with the software HLM 6.08 (Scientific Software International, Skokie, IL, USA).
2.3.1 Data screening and missing values
The portion of missing values was below 5% for all analysed variables. Because HLM only allows for individual missing values on the lowest level of the analysis (level 1; i.e. up to five of six HRQoL subscale scores may be missing for one subject), missing values for continuous subject-level predictors (level 2) were estimated by linear regression using all potential variables of the final analyses as predictors. Cases with missing values on categorical variables and those with completely missing information on HRQoL were excluded from the analyses. The excluded cases (3.4%) had significantly lower SES scores and more often were immigrants (p < 0.01) but did not differ on other variables from the analysed sample. Completed data were screened for multicollinearity, distributional assumptions, and outliers, and no problems were discovered.
2.3.2 Main analyses
To analyse the associations of PA frequency and SBM with the HRQoL subscale scores, a three-level hierarchical linear regression model was analysed in which individual HRQoL subscale scores (level 1) were nested in subjects (level 2) and subjects were nested in sample points (level 3). HRQoL intercepts were allowed to vary between sample points (random effects), whereas the slopes of the predictors were fixed. Because significant interactions with gender were revealed for the associations of PA and SBM with HRQoL, all models were computed separately for boys and girls.
All categorical independent measures were entered by using dummy variables to contrast each category with a reference category coded ‘0’. For each contrast, effect size d was computed as model-estimated mean difference divided by person-level SD and interpreted as d = 0.20 (small), d = 0.50 (medium), and d = 0.80 (large).
For the main analyses, crude regression models were computed first to estimate the bivariate associations of the HRQoL subscales with subject-level predictors. All tested covariates were significantly related to PA or SBM and HRQoL for at least some of the HRQoL subscales. In the final adjusted models, the effects for the different HRQoL subscales were adjusted for covariates that were significant in the final models.
2.3.3 Mediation analysis
BDS was analysed as a possible mediator of the effects of PA and SBM on HRQoL. Because effects for feeling ‘too fat’ and ‘too thin’ in general pointed in the same direction, for the mediation analysis (which allows for a binary or continuous mediator), both categories were combined, and those who were dissatisfied with their weight were compared with boys and girls who felt ‘about the right size’. We used the Stata package ‘mediation’ to calculate the mediated effect for BDS as a mediator using 3000 simulation runs for the quasi-Bayesian estimation of confidence intervals (Hicks & Tingley, Citation2011). To simplify the analysis, mediated effects were only calculated for the comparison of the two most extreme categories of PA and SBM.
To further describe the kind of mediating mechanism, the coefficients alpha (the coefficient for the mediator BDS regressed on the independent variable PA/SBM) and beta (the coefficient for the dependent variable HRQoL regressed on the mediator BDS and adjusted for PA/SBM) were additionally calculated (Cerin & Mackinnon, Citation2009). Because BDS was predicted by logistic regression, alpha is expressed as an odds ratio (OR).
3. Results
3.1 Description of the sample
Table gives a description of the sample and compares boys with girls. Boys in general reported more frequent PA (28.2% nearly daily PA vs. 17.3% in girls) but also higher amounts of SBM (M = 3.77 h vs. M = 2.73 h) and regular drinking (29.4% vs. 19.5%) than did girls. Girls more often felt ‘too fat’ (54.5% vs. 35.5%), whereas boys more often were satisfied with their weight but also more often felt ‘too thin’ (20.4% vs. 8.9%) than did girls. With respect to HRQoL, girls reported lower well-being, except on the subscale ‘school’, on which boys reported lower scores. Boys and girls did not differ in age, but girls on average were biological older in terms of the percentage of adult height already reached (M = 97% vs. 93%).
Table 1. Characteristics of the studied KiGGS subsample (11–17 years old) by sex.
Although PA frequency and SBM were significantly related (τc boys = 0.074, τc girls = 0.101, p < 0.001), this association was not very strong. It is therefore confirmed that PA and SBM should be treated as distinct behaviours.
3.2 Associations with HRQoL
Associations of PA with HRQoL were very clear in both the unadjusted and the adjusted models for girls as well as for boys, although most effects considerably decreased when adjusted for SBM and significant covariates (see Tables and ). PA frequency was significantly related to all HRQoL domains, except for ‘school’ in boys and ‘family’ in girls. Higher PA frequency in general was related to higher HRQoL (see Figure (a) and 1(b)), showing small to moderate effect sizes for daily vs. no regular PA in both genders. The largest effects were seen for social and emotional well-being in boys (moderate effects: d = 0.56–0.59) and physical well-being followed by social well-being in girls (small to moderate effects: d = 0.43 and d = 0.32). In both genders, HRQoL was related to PA frequency in a dose–response manner, and for most subscales, significant linear trends were revealed. However, although HRQoL in boys increased quite steadily and the highest scores were reached with daily PA, girls' HRQoL only slightly differed between daily PA and 3–5 times/week.
Figure 1. (a–d) Health-related quality of life (HRQoL) subscale scores as a function of physical activity (PA) frequency and amount of daily screen-based media use (SBM) in girls (N = 3217) and boys (N = 3356). HRQoL scores on a scale from 0 (lowest HRQoL) to 100 (highest HRQoL) are contrasted with irregular PA and SBM less than 2 h per day as references (=0), respectively.
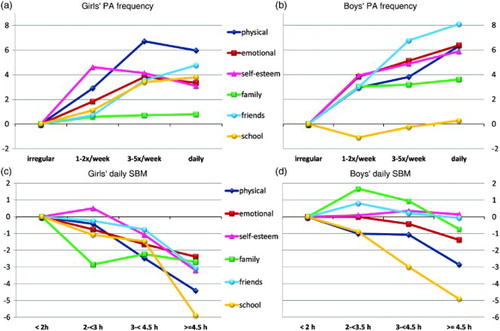
Table 2. Crude and adjusted model of girls' HRQoL scores predicted by PA and SBM: coefficient (s.e.) from three-level hierarchical linear regression (data from KiGGS study 2003–2006, 11–17 year-olds).
Table 3. Crude and adjusted model of boys' HRQoL scores predicted by PA and SBM: coefficient (s.e.) from three-level hierarchical linear regression (data from KiGGS study 2003–2006, 11–17 year-olds).
High SBM generally was related to lower HRQoL in our sample, although associations were more unambiguous in girls. In both genders, SBM effects were slightly reduced after adjustment for PA and covariates. Negative associations of SBM with HRQoL were significant for all HRQoL domains in girls (Table ) and were most obvious for school, friends, and physical well-being. The largest effect for SBM was found with girls' school functioning (d = −0.37) – a steep decline in HRQoL appeared for those in the highest SBM category (Figure (c)). In girls, SBM was related to HRQoL in a dose–response manner and for most subscales was best described by a linear trend, except for the subscale family. The pattern of associations between SBM and HRQoL was less clear in boys (Table ). Only physical well-being, family, and school were significant in the adjusted model, with the largest effects for school (d = −0.31). In general, boys with the highest SBM had the lowest HRQoL scores (Figure (d)), but a clear dose–response relation was only seen with physical well-being and school, which also showed significant linear trends. On the family subscale, a significant quadratic trend was revealed; scores for medium SBM were higher than they were for low SBM, and only boys with the highest SBM showed reduced familial well-being.
For all HRQoL subscales, SBM effects were larger in girls than in boys. The opposite was true for PA, where the effects were larger in boys than in girls, with the exception of the school domain.
No PA–SBM interactions were found for any of the HRQoL subscales, confirming that the effects of PA and SBM were independent of each other in both genders. Interaction effects of PA with gender were significant for the HRQoL domains physical well-being and school (p < 0.05), and for SBM, significant interactions were found in relation to the domains physical well-being, self-esteem, and family (p < 0.05).
3.3 Mediation analysis
Tables and show the results of the mediation analysis for BDS as a potential mediator of the relationships of PA and SBM with HRQoL. No interactions of PA or SBM with BDS were detected in any of the models.
Table 4. Mediation analysis in girls (N = 3217) – PA and SBM effects on HRQoL mediated by BDS (data from KiGGS study 2003–2006, 11–17 year-olds).
Table 5. Mediation analysis in boys (N = 3356) – PA and SBM effects on HRQoL mediated by BDS (data from KiGGS study 2003–2006, 11–17 year-olds).
In general, the results show that more frequent PA was related to a lower risk of BDS, although in boys the contrast of daily vs. irregular PA did not reach significance (p for trend <0.05). Higher use of SBM was associated with significantly higher odds of feeling dissatisfied in both genders, and BDS was related to significantly lower HRQoL scores on all subscales in both genders.
The corresponding mediated effects for BDS were significant for PA and SBM on all HRQoL subscales in boys and girls. However, the size of these effects was rather small. Mediated PA effects in girls accounted for 0.14–0.35 point increases in HRQoL scores for daily vs. irregular PA (see Table ), with the largest value for the self-esteem subscale. In boys, the PA effects explained by mediation ranged from 0.16 to 0.61 point increases in HRQoL (Table ), with the largest effect for physical well-being. The proportions of total PA effects that were mediated exceeded 10% only for those HRQoL subscales on which the PA effect was small and not significant. Thus, our results indicate that only a very small part of the PA effects was mediated by BDS.
Mediation effects for SBM were more pronounced in girls than in boys and were larger than those for PA. Again, however, the size of these indirect effects was rather small. The maximum encountered mediated effect for self-esteem, for example, showed that for the highest compared with the lowest SBM category, the effect mediated by feeling dissatisfied accounted for a 0.64 point decrease in self-esteem, which was roughly 20% of the corresponding total SBM effect. Most other indirect effects were notably lower.
In boys, the mediation of SBM effects was, overall, comparable in size to the mediation results for PA. The largest effect was again found for the subscale physical well-being, where a decrease of 0.33 points could be explained by mediation, which was 11.2% of the total effect for highest vs. lowest SBM. The proportions of the total SBM effect that were mediated on other subscales again exceeded 10% only for those HRQoL subscales on which the effects of SBM were small and non-significant.
4. Discussion
The present paper examined the associations of PA and SBM with HRQoL subdomains in a representative sample of German adolescents and evaluated the mediating role of body satisfaction for these associations. In general, associations of PA with HRQoL showed that more frequent PA in both genders was related to higher HRQoL. High use of screen-based media was associated with lower HRQoL, but these associations were more pronounced in girls than in boys. Mediation analysis indicated significant but rather small indirect effects of PA and SBM on HRQoL via BDS, accounting for only small portions of total effects of PA and SBM.
4.1 PA in relation to HRQoL
Our finding that HRQoL was positively related to PA frequency confirms research with children and adolescents on PA and different measures of HRQoL (Chen et al., Citation2005; Lacy et al., Citation2012; Sanchez-Lopez et al., Citation2009), although some previous studies found only very small effects (Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009; Spengler & Woll, Citation2012) or non-significant effects (Boyle et al., Citation2010).
The variation in results of previous studies might be explained by different assessments of PA and HRQoL as well as by confounders that were accounted for aside from PA, including SBM. Self-report measures likely differ in the specific aspects that they cover. For example, Spengler and Woll (Citation2012) analysed a random subsample (N = 1828, 58.3% response) of our sample but used a different PA questionnaire that measured overall volume of PA in minutes. They did not adjust for SBM and covariates such as zBMI, maturity, sleep, foreign background, smoking, or drinking and reported only very small associations with overall HRQoL score.
Our results indicate that PA frequency is related to HRQoL generally in a dose–response manner. In girls, however, the results indicate that a PA frequency of 3–5 times per week or more, not just the highest (i.e. daily) PA frequency, is associated with the highest HRQoL. Because from adolescence on, girls are found to be less physically active and physical requirements for PA differ between boys and girls, it may be reasonable that for both genders, different kinds and amounts of activities are optimal for subjective well-being. Yet, because we asked only for frequency but not total amount of PA, we cannot draw conclusions about the ideal amount of PA for each gender in terms of well-being.
Only very few studies have discriminated between different HRQoL subdomains when examining associations with PA. We observed the strongest associations between PA frequency and physical and social well-being (friends). This finding is in line with the results of Breslin et al. (Citation2012), who found that children who met the recommendations for PA reported higher social acceptance and peer support as well as fewer physical and emotional symptoms. Our results are also consistent with those of Iannotti, Janssen, et al. (Citation2009), who found the strongest associations of PA with perceived health status and peer relationships in an international comparison.
Although it is possible that girls and boys with better physical well-being simply engage in more PA because of better overall functioning, a positive impact of PA on physical well-being is likely. PA, especially on a regular basis, results in various physical adaptations that may enhance well-being, although dose–response issues are unclear (Biddle et al., Citation2000).
The link between PA and better social well-being related to friends seems reasonable, because PA in adolescents, especially boys, is often performed together with peers or in team sports (Wickel & Eisenmann, Citation2007). It is therefore likely that for the social dimension of well-being, time spent together during physical activities is critical. This may also explain why these effects were more pronounced in males than in females.
According to other studies (Breslin et al., Citation2012), more frequent PA was also related to higher self-esteem scores in our sample, although the effect sizes were small. Stronger indications of causal influences of PA on self-esteem were reported by Schmalz et al. (Citation2007). They revealed a significant lagged effect of PA on self-esteem after two years in early adolescent girls, whereas no indication was found for an effect of self-esteem on later PA. A review on exercise interventions also concluded that exercise leads to increased self-esteem in youths, at least in the short run (Ekeland, Heian, Hagen, Abbott, & Nordheim, Citation2004). It therefore seems justified to assume that PA has a positive impact on self-esteem in adolescents.
4.2 SBM in relation to HRQoL
The found association of high SBM with lower HRQoL in our sample is in accord with the results of previous studies (Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009; Lacy et al., Citation2012; Mathers et al., Citation2009). Consistent with our findings, Lacy et al. (Citation2012) found larger associations in girls than in boys, whereas no gender-specific results were reported in other studies.
Hardly any research has examined SBM in relation to HRQoL subdomains. In general, the effects in our sample were largest for school functioning in both genders. This result is in line with studies relating SBM to lower academic performance (Strasburger, Jordan, & Donnerstein, Citation2010; Tremblay et al., Citation2011). High media consumption may lead to a lack of time for school work and therefore interfere with school functioning. On the other hand, adolescents with lower school success may turn to other interests in their leisure time and therefore have higher SBM.
Although the effect size was small, we found that high SBM related to lower self-esteem in girls. This finding confirms results from other studies (Nihill et al., Citation2013; Racine et al., Citation2011; Tremblay et al., Citation2011). One possible explanation for this result would be that the negative impact of media images on girls' body image generalises to general self-esteem. This hypothesis is discussed in more detail below as part of the mediation analysis.
Boys' familial well-being was only reduced in the group with the highest SBM but was heightened for those in the medium categories. Some other studies also reported small positive associations of SBM with social relationships, although primarily for peers (Chen et al., Citation2005; Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009). It might be the social component of SBM that affects social well-being. Watching TV or engaging in computer use or console gaming together, at least for some boys, may be one kind of family or peer activity that positively affects social well-being. In girls, on the other hand, social well-being was highest in those with the lowest SBM, indicating no such social benefit or, rather, differing needs concerning the quality of social interactions.
However, we did not differentiate between different kinds of media in our study. The effects of SBM on health and well-being can also result from specific media content and not only from being sedentary (Brown & Cantor, Citation2000). This may explain some of the gender differences found in the results (Olds, Maher, Ridley, & Kittel, Citation2010). Further research would benefit from analysing patterns of results for different types of media in relation to HRQoL subdomains in boys and girls.
4.3 Mediation by BDS
A positive impact on body image is one supposed effect of an active lifestyle and was hypothesised as a possible mediator for farther-reaching effects on improved self-esteem and quality of life (Biddle et al., Citation2000; Rejeski et al., Citation2001). We found only small indications of body satisfaction mediating the effects of higher PA frequency on HRQoL, and the relation of PA with BDS was less clear than that of SBM with BDS.
Our result is in contrast to results from a meta-analysis that revealed conspicuously better body image in exercisers of different ages (Hausenblas & Fallon, Citation2006). However, other studies found only small (Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009) or no associations (Breslin et al., Citation2012; Fairclough et al., Citation2012) of PA with body image in children and adolescents. It is likely that specific forms of PA (i.e. structured exercise and sports) affect body image more strongly than does the broader concept of PA that was investigated here.
BDS may be one mechanism that explains lower HRQoL and especially lower self-esteem in female heavy media users. Gender differences in our results indicate that the assumption that idealised media images of female bodies could have a negative impact on girls' body image and in turn on self-esteem may be partly true. Self-esteem, as expected, was the HRQoL dimension with the largest mediation effect, accounting for more than 20% of the total SBM effect in girls. However, all mediated effects were rather small, and most of the SBM-HRQoL association could not be explained by these indirect effects. Furthermore, in boys, effects on physical well-being generally were more pronounced than were effects on self-esteem for both PA and SBM.
We are not aware of other studies that have examined whether the effects of SBM are mediated by body satisfaction. Overall, the links between SBM and BDS that we revealed in our study seem to stand out from other studies in their magnitude. One reason may be that we adjusted our analyses for actual weight status, which was not done in most other research (Iannotti, Janssen, et al., Citation2009; Iannotti, Kogan, et al., Citation2009; Racine et al., Citation2011).
Because direct associations of PA and SBM with HRQoL were more manifest than were associations with BDS and only small proportions of PA and SBM effects were partially mediated by BDS, the hypothesis that body satisfaction mediates the effects of PA or SBM on HRQoL altogether received only partial support from our study. Other mechanisms must therefore account for large parts of the relationships of SBM and PA with HRQoL and should be investigated in future studies. It may be, for example, that adolescents with low PA and high SBM have fewer social contacts and support (although this may also be a reason for high media use or an alternative way to make contact). SBM is also associated with less balanced nutrition (Pearson & Biddle, Citation2011), which might also lead to lower well-being independent of weight status. Other potential mediating variables that were supposed for PA are mastery experiences and self-confidence, a positive environment, and physiological mechanisms as a result of somatic adaptations (Biddle et al., Citation2000). These mediating variables remain to be studied in adolescents. Nevertheless, we identified body satisfaction as a strong predictor of HRQoL. Further research should analyse whether BDS causally affects HRQoL domains and whether promotion of body satisfaction therefore may generalise to increased general well-being.
4.4 Strengths and limitations
Some strengths of our study should be highlighted. In contrast to previous studies, we studied both PA and SBM in relation to a comprehensive HRQoL measure and considered independent associations of both PA and SBM, as different but not opposite aspects of inactivity, with HRQoL subdomains while controlling for a variety of meaningful covariates and differentiating results by gender. We used a large and representative sample, covering a broad age range from early to late adolescence. The applied questionnaires were extensively pretested and validated (Kurth et al., Citation2008). We are not aware of other studies that tested the possible mediating role of body satisfaction on HRQoL effects.
However, some limitations should also be considered. First, based on the present cross-sectional analyses, we cannot draw conclusions about the causality of the found effects. Concerning PA, it was argued not only that PA could increase well-being but also that well-being could motivate further PA. Therefore, the associations may well be reciprocal (Biddle et al., Citation2000). The same could be true for SBM. Only longitudinal and experimental research will help to determine the foundations of these relationships. In addition, mediation effects generally cannot satisfactorily be verified by cross-sectional research. Nevertheless, examining hypothesised associations and possible mediating mechanisms cross-sectionally can help to refute causal hypotheses. The KiGGS study, furthermore, is going to be continued as a cohort study, which implies that results from the reported survey may be verified longitudinally and may allow for more sound conclusions.
Both PA and SBM were self-reported by adolescents in our study. It is well recognised that the accuracy of PA and SBM self-reports in children and adolescents is limited (Biddle, Gorely, Pearson, & Bull, Citation2011; Lubans et al., Citation2011). In particular, the PA item was rather crude and not able to represent the full picture of this complex behaviour (Pettee Gabriel, Morrow, & Woolsey, Citation2012), and no exact information on the reliability and validity of the employed self-report measures is available. The use of more accurate objective measures (e.g. accelerometers or timekeepers) is preferable, but is often not feasible in comprehensive health surveys such as the KiGGS. However, as Masse and de Niet (Citation2012) pointed out, most PA self-report measures are suitable for accurately ranking subjects according to their PA levels, a feature that is needed in studies relating PA to health outcomes.
Reliability in terms of internal consistency was debatable for some HRQoL subscale scores, and this may have resulted in larger measurement errors. Therefore, the results for family and friends should particularly be interpreted with caution. However, internal consistency was only slightly lower than it was in a study on the psychometric properties of this instrument (Bullinger et al., Citation2008), in which altogether good scale properties as well as convergent and discriminant validity were confirmed.
4.5 Conclusions
In sum, we found positive associations of PA and negative associations of SBM with HRQoL independent from each other and from relevant covariates such as body mass, age, or maturational timing, with low-to-moderate effect sizes for PA and generally lower effects for SBM. Whereas PA associations were more pronounced in boys, SBM associations were more consistent in girls. Although the sizes of the found effects were only low to moderate, some differences in HRQoL scores between PA categories were of the same magnitude as differences between healthy children and those with chronic conditions or handicaps (Ravens-Sieberer et al., Citation2008).
We found only small indirect effects indicating that PA and SBM affect HRQoL indirectly via body satisfaction, but large portions of these effects are left unexplained.
Future studies on PA and well-being should concentrate on establishing causal effects and exploring which mediating mechanisms account for the found associations. Because the patterns of the results were more divergent with respect to SBM, it may be fruitful to distinguish between different types of SBM (i.e. TV, computer, and video games) to shed further light on the found gender differences in relation to the associations of SBM and well-being.
Acknowledgements
The KiGGS study was funded by the German Federal Ministry of Health, the Ministry of Education and Research, and the Robert Koch Institute. It was designed and carried out at the Robert Koch Institute. We acknowledge support for the Article Processing Charge by the Deutsche Forschungsgemeinschaft and the Open Access Publication Funds of Bielefeld University Library.
References
- Biddle, S. J. H., & Asare, M. (2011). Physical activity and mental health in children and adolescents: A review of reviews. British Journal of Sports Medicine, 45(11), 886–895. doi: 10.1136/bjsports-2011-090185
- Biddle, S. J. H., Fox, K. R., Boutcher, S. H., & Faulkner, G. E. (2000). The way forward for physical activity and the promotion of psychological well-being. In S. J. H. Biddle, K. R. Fox, & S. H. Boutcher (Eds.), Physical activity and psychological well-being (pp. 154–195). London: Routledge.
- Biddle, S. J. H., Gorely, T., Pearson, N., & Bull, F. C. (2011). An assessment of self-reported physical activity instruments in young people for population surveillance: Project ALPHA. International Journal of Behavioral Nutrition and Physical Activity, 8, 1. doi: 10.1186/1479-5868-8-1
- Bize, R., Johnson, J. A., & Plotnikoff, R. C. (2007). Physical activity level and health-related quality of life in the general adult population: A systematic review. Preventive Medicine, 45(6), 401–415. doi: 10.1016/j.ypmed.2007.07.017
- Booth, M. L., Okely, A. D., Chey, T., & Bauman, A. (2001). The reliability and validity of the physical activity questions in the WHO health behaviour in schoolchildren (HBSC) survey: A population study. British Journal of Sports Medicine, 35(4), 263–267. doi: 10.1136/bjsm.35.4.263
- Boreham, C., & Riddoch, C. (2003). Physical activity and health through the lifespan. In J. McKenna & C. Riddoch (Eds.), Perspectives on health and exercise (pp. 11–30). Basingstoke: Palgrave Macmillan.
- Boyle, S., Jones, G., & Walters, S. (2010). Physical activity, quality of life, weight status and diet in adolescents. Quality of Life Research, 19(7), 943–954. doi: 10.1007/s11136-010-9659-8
- Breslin, G., Gossrau-Breen, D., McCay, N., Gilmore, G., McDonald, L., & Hanna, D. (2012). Physical activity, gender, weight status, and wellbeing in 9- to 11-year-old children: A cross sectional survey. Journal of Physical Activity and Health, 9(3), 394–401.
- Brown, J. D., & Cantor, J. (2000). An agenda for research on youth and the media. Journal of Adolescent Health, 27 (2, Supplement 1), 2–7. doi: 10.1016/S1054-139X(00)00139-7
- Bullinger, M., Brutt, A. L., Erhart, M., & Ravens-Sieberer, U. (2008). Psychometric properties of the KINDL-R questionnaire: Results of the BELLA study. European Child and Adolescent Psychiatry, 17(Suppl 1), 125–132. doi: 10.1007/s00787-008-1014-z
- Cerin, E., & Mackinnon, D. P. (2009). A commentary on current practice in mediating variable analyses in behavioural nutrition and physical activity. Public Health Nutrition, 12(8), 1182–1188. doi: 10.1017/S1368980008003649
- Chen, X., Sekine, M., Hamanishi, S., Wang, H., Gaina, A., Yamagami, T., & Kagamimori, S. (2005). Lifestyles and health-related quality of life in Japanese school children: A cross-sectional study. Preventive Medicine, 40(6), 668–678. doi: 10.1016/j.ypmed.2004.09.034
- Cole, T. J. (1990). The LMS method for constructing normalized growth standards. European Journal of Clinical Nutrition, 44(1), 45–60.
- Currie, C., Zanotti, C., Morgan, A., Currie, D., de Looze, M., Roberts, C., … Barnekow, V. (Eds.). (2012). Social determinants of health and well-being among young people: Health Behaviour in School-Aged Children (HBSC) study: International report from the 2009/2010 survey. Copenhagen: WHO Regional Office for Europe.
- Ekeland, E., Heian, F., Hagen, K. B., Abbott, J., & Nordheim, L. (2004). Exercise to improve self-esteem in children and young people. Cochrane Database of Systematic Reviews, (1), Art. No.: CD003683. doi:10.1002/14651858.CD003683.pub2. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003683.pub2/otherversions
- Fairclough, S. J., Ridgers, N. D., & Welk, G. (2012). Correlates of children's moderate and vigorous physical activity during weekdays and weekends. Journal of Physical Activity and Health, 9(1), 129–137.
- Griebler, R., Molcho, M., Samdal, O., Inchley, J., Dür, W., & Currie, C. (Eds.). (2010). Health Behaviour in School-Aged Children: A World Health Organization cross-national study. Research protocol for the 2009/2010 survey. Vienna/Edinburgh: Ludwig-Boltzmann Institute for Health Promotion Research (LBIHPR)/Child and Adolescent Health Research Unit (CAHRU), University of Edinburg.
- Griffiths, L. J., Parsons, T. J., & Hill, A. J. (2010). Self-esteem and quality of life in obese children and adolescents: A systematic review. International Journal of Pediatric Obesity, 5(4), 282–304. doi: 10.3109/17477160903473697
- Hausenblas, H. A., & Fallon, E. A. (2006). Exercise and body image: A meta-analysis. Psychology and Health, 21(1), 33–47. doi: 10.1080/14768320500105270
- Hicks, R., & Tingley, D. (2011). Causal mediation analysis. Stata Journal, 11(4), 605–619.
- Hunter Smart, J. E., Cumming, S. P., Sherar, L. B., Standage, M., Neville, H., & Malina, R. M. (2012). Maturity associated variance in physical activity and health-related quality of life in adolescent females: A mediated effects model. Journal of Physical Activity and Health, 9, 86–95.
- Iannotti, R. J., Janssen, I., Haug, E., Kololo, H., Annaheim, B., & Borraccino, A. (2009). Interrelationships of adolescent physical activity, screen-based sedentary behaviour, and social and psychological health. International Journal of Public Health, 54(Suppl 2), 191–198. doi: 10.1007/s00038-009-5410-z
- Iannotti, R. J., Kogan, M. D., Janssen, I., & Boyce, W. F. (2009). Patterns of adolescent physical activity, screen-based media use, and positive and negative health indicators in the U.S. and Canada. Journal of Adolescent Health, 44(5), 493–499. doi: 10.1016/j.jadohealth.2008.10.142
- Jansen, W., van de Looij-Jansen, P. M., de Wilde, E. J., & Brug, J. (2008). Feeling fat rather than being fat may be associated with psychological well-being in young Dutch adolescents. Journal of Adolescent Health, 42(2), 128–136. doi: 10.1016/j.jadohealth.2007.07.015
- Janssen, I., & LeBlanc, A. (2010). Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 7(1), 40. doi: 10.1186/1479-5868-7-40
- Khamis, H. J., & Roche, A. F. (1994). Predicting adult stature without using skeletal age: The Khamis–Roche method. Pediatrics, 94(4), 504–507.
- Kromeyer-Hauschild, K., Wabitsch, M., Kunze, D., Geller, F., Geiß, H. C., Hesse, V., … Hebebrand, J. (2001). Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben [Percentiles of body mass index in children and adolescents evaluated from different regional German studies]. Monatsschrift für Kinderheilkunde, 149(8), 807–818. doi: 10.1007/s001120170107
- Kurth, B. M., Kamtsiuris, P., Holling, H., Schlaud, M., Dolle, R., Ellert, U., … Wolf, U. (2008). The challenge of comprehensively mapping children's health in a nation-wide health survey: Design of the German KiGGS-Study. BMC Public Health, 8(1), 196. doi: 10.1186/1471-2458-8-196
- Lacy, K., Allender, S., Kremer, P., de Silva-Sanigorski, A., Millar, L., Moodie, M., … Swinburn, B. A. (2012). Screen time and physical activity behaviours are associated with health-related quality of life in Australian adolescents. Quality of Life Research, 21(6), 1085–1099. doi: 10.1007/s11136-011-0014-5
- Lange, M., Kamtsiuris, P., Lange, C., Schaffrath Rosario, A., Stolzenberg, H., & Lampert, T. (2007). Messung soziodemographischer Merkmale im Kinder- und Jugendgesundheitssurvey (KiGGS) und ihre Bedeutung am Beispiel der Einschätzung des allgemeinen Gesundheitszustands [Sociodemographic characteristics in the German Health Interview and Examination Survey for children and adolescents (KiGGS) – Operationalisation and public health significance, taking as an example the assessment of general state of health]. Bundes – gesundheitsblatt – Gesundheitsforschung – Gesundheitsschutz, 50(5), 578–589. doi: 10.1007/s00103-007-0219-5
- Lee, I. M., Shiroma, E. J., Lobelo, F., Puska, P., Blair, S. N., & Katzmarzyk, P. T. (2012). Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet, 380(9838), 219–229. doi: 10.1016/S0140-6736(12)61031-9
- Lubans, D. R., Hesketh, K., Cliff, D. P., Barnett, L. M., Salmon, J., & Dollman, J. (2011). A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obesity Reviews, 12(10), 781–799. doi: 10.1111/j.1467-789X.2011.00896.x
- Marshall, S. J., Biddle, S. J. H., Gorely, T., Cameron, N., & Murdey, I. (2004). Relationships between media use, body fatness and physical activity in children and youth: A meta-analysis. International Journal of Obesity and Related Metabolic Disorders, 28(10), 1238–1246. doi: 10.1038/sj.ijo.0802706
- Masse, L. C., & de Niet, J. E. (2012). Sources of validity evidence needed with self-report measures of physical activity. Journal of Physical Activity and Health, 9(Suppl 1), S44–55.
- Mathers, M., Canterford, L., Olds, T., Hesketh, K., Ridley, K., & Wake, M. (2009). Electronic media use and adolescent health and well-being: Cross-sectional community study. Academic Pediatrics, 9(5), 307–314. doi: 10.1016/j.acap.2009.04.003
- Mond, J., van den Berg, P., Boutelle, K., Hannan, P., & Neumark-Sztainer, D. (2011). Obesity, body dissatisfaction, and emotional well-being in early and late adolescence: Findings from the Project EAT study. Journal of Adolescent Health, 48(4), 373–378. doi: 10.1016/j.jadohealth.2010.07.022
- Nelson, M. C., & Gordon-Larsen, P. (2006). Physical activity and sedentary behavior patterns are associated with selected adolescent health risk behaviors. Pediatrics, 117(4), 1281–1290. doi: 10.1542/peds.2005-1692
- Nihill, G. F. J., Lubans, D. R., & Plotnikoff, R. C. (2013). Associations between sedentary behavior and self-esteem in adolescent girls from schools in low-income communities. Mental Health and Physical Activity, 6(1), 30–35. doi: 10.1016/j.mhpa.2012.02.003
- Olds, T., Maher, C., Ridley, K., & Kittel, D. (2010). Descriptive epidemiology of screen and non-screen sedentary time in adolescents: A cross sectional study. International Journal of Behavioral Nutrition and Physical Activity, 7(1), 92. doi: 10.1186/1479-5868-7-92
- Pearson, N., & Biddle, S. J. H. (2011). Sedentary behavior and dietary intake in children, adolescents, and adults: A systematic review. American Journal of Preventive Medicine, 41(2), 178–188. doi: 10.1016/j.amepre.2011.05.002
- Pettee Gabriel, K. K., Morrow, J. R.Jr, & Woolsey, A. L. (2012). Framework for physical activity as a complex and multidimensional behavior. Journal of Physical Activity and Health, 9(Suppl 1), S11–18.
- Prochaska, J. J., Sallis, J. F., & Long, B. (2001). A physical activity screening measure for use with adolescents in primary care. Archives of Pediatrics and Adolescent Medicine, 155, 554–559. doi: 10.1001/archpedi.155.5.554
- Proper, K. I., Singh, A. S., van Mechelen, W., & Chinapaw, M. J. (2011). Sedentary behaviors and health outcomes among adults: A systematic review of prospective studies. American Journal of Preventive Medicine, 40(2), 174–182. doi: 10.1016/j.amepre.2010.10.015
- Racine, E. F., DeBate, R. D., Gabriel, K. P., & High, R. R. (2011). The relationship between media use and psychological and physical assets among third- to fifth-grade girls. Journal of School Health, 81(12), 749–755. doi: 10.1111/j.1746-1561.2011.00654.x
- Ravens-Sieberer, U., & Bullinger, M. (2000). KINDLR-Questionnaire for measuring health-related quality of life in children and adolescents. Revised version retrieved 27 February, 2012, from http://kindl.org/cms/wp-content/uploads/2009/11/ManEnglish.pdf
- Ravens-Sieberer, U., Erhart, M., Wille, N., Bullinger, M., & the BELLA study group. (2008). Health-related quality of life in children and adolescents in Germany: Results of the BELLA study. European Child and Adolescent Psychiatry, 17(Suppl. 1), 148–156. doi: 10.1007/s00787-008-1016-x
- Ravens-Sieberer, U., Torsheim, T., Hetland, J., Vollebergh, W., Cavallo, F., Jericek, H., … HBSC Positive Health Focus Group. (2009). Subjective health, symptom load and quality of life of children and adolescents in Europe. International Journal of Public Health, 54(Suppl 2), 151–159. doi: 10.1007/s00038-009-5406-8
- Rejeski, W. J., Shelton, B., Miller, M., Dunn, A. L., King, A. C., & Sallis, J. F. (2001). Mediators of increased physical activity and change in subjective well-being: Results from the Activity Counseling Trial (ACT). Journal of Health Psychology, 6(2), 159–168. doi: 10.1177/135910530100600206
- Ricciardelli, L. A., McCabe, M. P., Holt, K. E., & Finemore, J. (2003). A biopsychosocial model for understanding body image and body change strategies among children. Journal of Applied Developmental Psychology, 24(4), 475–495. doi: 10.1016/S0193-3973(03)00070-4
- Robert Koch Institut. (2008). Public Use File KiGGS, The German Health Survey for children and adolescents 2003–2006. Berlin: Author.
- Sanchez-Lopez, M., Salcedo-Aguilar, F., Solera-Martinez, M., Moya-Martinez, P., Notario-Pacheco, B., & Martinez-Vizcaino, V. (2009). Physical activity and quality of life in schoolchildren aged 11–13 years of Cuenca, Spain. Scandinavian Journal of Medicine and Science in Sports, 19(6), 879–884. doi: 10.1111/j.1600-0838.2008.00839.x
- Schenk, L., Ellert, U., & Neuhauser, H. (2007). Kinder und Jugendliche mit Migrationshintergrund in Deutschland [Children and adolescents in Germany with a migration background. Methodical aspects in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS)]. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz, 50(5), 590–599. doi: 10.1007/s00103-007-0220-z
- Schmalz, D. L., Deane, G. D., Birch, L. L., & Davison, K. K. (2007). A longitudinal assessment of the links between physical activity and self-esteem in early adolescent non-Hispanic females. Journal of Adolescent Health, 41(6), 559–565. doi: 10.1016/j.jadohealth.2007.07.001
- Schmitz, K. H., Harnack, L., Fulton, J. E., Jacobs, D. R. Jr, Gao, S., Lytle, L. A., & Coevering, P. V. (2004). Reliability and validity of a brief questionnaire to assess television viewing and computer use. Journal of School Health, 74(9), 370–377. doi: 10.1111/j.1746-1561.2004.tb06632.x
- Spengler, S., & Woll, A. (2012). The more physically active, the healthier? The relationship between physical activity and health-related quality of life in adolescents: The MoMo-Study. Journal of Physical Activity and Health. Advance online publication. Retrieved from http://journals.humankinetics.com/jpah-in-press/jpah-in-press/the-more-physically-active-the-healthier-the-relationship-between-physical-activity-and-health-related-quality-of-life-in-adolescents-the-momo-study
- Strasburger, V. C., Jordan, A. B., & Donnerstein, E. (2010). Health effects of media on children and adolescents. Pediatrics, 125(4), 756–767. doi: 10.1542/peds.2009-2563
- Tergerson, J. L., & King, K. A. (2002). Do perceived cues, benefits, and barriers to physical activity differ between male and female adolescents? Journal of School Health, 72(9), 374–380. doi: 10.1111/j.1746-1561.2002.tb03562.x
- Tremblay, M. S., LeBlanc, A. G., Kho, M. E., Saunders, T. J., Larouche, R., Colley, R. C., … Connor Gorber, S. (2011). Systematic review of sedentary behaviour and health indicators in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 8, 98. doi: 10.1186/1479-5868-8-98
- Ussher, M., Owen, C., Cook, D., & Whincup, P. (2007). The relationship between physical activity, sedentary behaviour and psychological wellbeing among adolescents. Social Psychiatry and Psychiatric Epidemiology, 42(10), 851–856. doi: 10.1007/s00127-007-0232-x
- Utter, J., Neumark-Sztainer, D., Jeffery, R., & Story, M. (2003). Couch potatoes or French fries: Are sedentary behaviors associated with body mass index, physical activity, and dietary behaviors among adolescents? Journal of the American Dietetic Association, 103(10), 1298–1305. doi: 10.1016/S0002-8223(03)01079-4
- Van Der Horst, K., Paw, M. J., Twisk, J. W., & Van Mechelen, W. (2007). A brief review on correlates of physical activity and sedentariness in youth. Medicine and Science in Sports and Exercise, 39(8), 1241–1250. doi: 10.1249/mss.0b013e318059bf35
- Wickel, E. E., & Eisenmann, J. C. (2007). Contribution of youth sport to total daily physical activity among 6- to 12-yr-old boys. Medicine and Science in Sports and Exercise, 39(9), 1493–1500. doi: 10.1249/mss.0b013e318093f56a