
ABSTRACT
Background
The majority of adolescents are currently becoming sexually active before their 18th birthday having to battle with unsafe sexual behaviors, teenage pregnancies, sexually transmitted infections, and school dropouts. The study designed and tested the effect of integrated reproductive health lesson materials in a Problem-Based pedagogy (PBP) to enhance safe sexual behaviors among adolescents in Tanzania.
Methods
Clustered Randomized Controlled Trial was adopted among 660 adolescents in Tanzania. The study consisted of three research arms including pure PBP, Hybrid PBP, and Lecture-Based Pedagogy (LBP). Sexual-risk Behavior Beliefs and Self-esteem Scale adopted from previous studies measured adolescents' sexual behaviors. A Statistical Analysis Software (SAS) version 9.4 was used to analyze data. Descriptive analysis established adolescents' socio-demographic profiles. Generalized Estimating Equation (GEE) determined the effect of interventions on adolescents' intentions to practice safe sexual behaviors at a 95% confidence interval and a significance level of 5%.
Results
Adolescents' mean age was 15 ± 1.869 years. Sums of 57.5% (n = 380) were females. 39.5% of adolescents were sexually active whereas 44.8% of them initiated sexual intercourse by the age between 10 and 12 years. The end-line findings showed that 54.9% of adolescents in the LBP group demonstrated a significant intention to unsafe sexual behaviors against 26.3% and 30.9% of adolescents in the pure PBP and Hybrid PBP groups respectively. The Difference-In-Difference odds ratio for unsafe sexual behavior among adolescents in the Hybrid PBP and pure PBP was less (AOR = 0.30; p < 0.0001; 95%CI: 0.1398, 0.5559) and (AOR = 0.30, p < 0.0002; 95%CI: 0.1386, 0.5487) contrary to a control group respectively.
Conclusion
The integrated RH lesson materials in a PBP can change a spectrum of sexual behavior among adolescents in Tanzania. This study suggests school teachers and health workers work together to facilitate RH lessons using PBP to enhance safe sexual behaviors among adolescents for their healthy adulthood and future investment.
Trial registration: Pan African Clinical Trial Registry identifier: PACTR202009656160779..
| Abbreviations | ||
| CI | = | Confidence Interval |
| D-I-D | = | Difference in Difference |
| GEE | = | Generalized Estimating Equation |
| HIV | = | Human Immunodeficiency Virus |
| IRHC | = | Integrated Reproductive Health Content |
| IRRC | = | Institutional Research Review Committee |
| LBP | = | Lecture-based Pedagogy |
| AOR | = | Adjusted Odds Ratio |
| PBP | = | Problem-Based Pedagogy |
| RH | = | Reproductive Health |
| SAS | = | Statistical Analysis Software |
| SD | = | Standard Deviation |
| SRBBSES | = | Sexual-risk Behavior Beliefs and Self-esteem Scale |
| SRH | = | Sexual and Reproductive Health |
| STIs | = | Sexually Transmitted Infections |
Introduction
Adolescents represent a large cohort that determines a huge opportunity to transform the social and economic fortunes in the globe if they are formed properly during the early years of their lives (Chen, Brody, & Miller, Citation2022). Data on adolescents by United Nations (Citation2019) estimates that of the 7.2 (higher than that reported in 2010) billion world population, 42% (over 3 billion) are younger than 25 years, 18% (1.2 billion) are adolescents aged 10–19 years. About 88% of adolescents live in developing countries whereby Sub-Saharan Africa (SSA) constitutes 18% of them. It is also projected that by 2010–2030 the adolescent population in Sub-Saharan Africa will increase to 1.3 billion (UN, Citation2020). Tanzanian adolescents aged between 10 and 19 years account for 11,858,193 (23%) of the county’s population (N = 51,557,365). Early adolescents (10–14 years) make up 13% while late adolescents (15–19 years) make up 10% of the total population respectively (MoHCDGEC, Citation2018).
A healthy adolescence stage is argued to determine healthy adulthood, which is associated with increased job market opportunities that are believed to increase productivity rates (Chen et al., Citation2022). Increased productivity rates are claimed by scholars to have the potentials of promoting economic growth and prosperity at the individual, family, and national levels in the world (Tadjer, Lafifi, Seridi-Bouchelaghem, & Gülseçen, Citation2020). However, literature has noted that most adolescents are not developed appropriately in their characters, identity, and social responsibilities (Lanari, Mangiavacchi, & Pasqualini, Citation2020). The literature demonstrates that the adolescence stage energies young people out of their control that need close attention from parents, teachers, health care workers, and relatives (Mbachu et al., Citation2020).
The majority of adolescents often demonstrate a sense that they are always right to their desires and act regardless of how beneficial or hazardous they are to live (Moran & Taylor, Citation2022). The stage characterizes them not only to be attention seekers but also to demonstrate reckless behaviors including disputes with their parents, peers, teachers at schools, and other people in families and or unsafe sexual behaviors (Kemigisha, Ivanova, et al., Citation2019). Unsafe sexual behaviors among adolescents, for example, seem to prevail around the globe (Seff & Stark, Citation2022). Unsafe sexual behaviors among adolescents may include such manners as incorrect and inconsistent usage of contraceptive methods, having multiple sexual partners, frequent sexual intercourse, drug abuse before, or while having sexual activity, and or engaging in sexual intercourses for money or material gain (Zou et al., Citation2022).
Adolescents are currently becoming sexually active before their 18th birthday having to battle with unsafe sexual behaviors, teenage pregnancies, sexually transmitted infections (STIs), and school dropouts. Millanzi, Kibusi, and Osaki (Citation2022) have exposed that most adolescents take less negotiating power over safe sexual behaviors and find themselves at a considerable risk of sexual exploitation. Early initiation of unsafe sexual behaviors among adolescents is associated with early and unintended teenage pregnancies (United Nations, Citation2020). Early and unintended pregnancies are also linked with several adverse health outcomes such as new Sexually Transmitted Infections (STIs) including Human Immunodeficiency Virus (HIV) (Sodré, Spindola, Rose, & Martins, Citation2022).
Childbirth among adolescent girls exposes them to a risk of experiencing obstetric complications before, during, and after delivery such as eclampsia, post-partum hemorrhage, fistula, and or premature death (Keats et al., Citation2022). Children born from an adolescent girl are at risk of higher potential deaths, and low birth weights (Chavula, Svanemyr, Zulu, & Sandøy, Citation2021). Likewise, teenage pregnancies are associated with educational outcomes such as interrupting schooling leading to school dropouts (Delprato & Frola, Citation2022). Nevertheless, early and unintended teenage pregnancies are linked with social and economic outcomes including endangering their future economic opportunities such as reduced job market opportunities that would contribute to the economic growth and prosperity at an individual level, family, and nation at large (Davidai, Citation2022).
Some scholars have linked unsafe sexual behaviors among adolescents with limited formal and age-appropriate pedagogies used in facilitating SRH information and educations particularly in developing countries including Tanzania. The implementation of innovative and age-appropriate pedagogies in facilitating SRH learning among adolescents is argued to hold a potential of developing them with appropriate knowledge, self-esteem, and assertiveness skills for safe sexual behaviors than merely the implementation of conventional pedagogies such as lectures, discussions, and or buzzing (Zhang et al., Citation2019). Innovative pedagogies used in facilitating SRH learning among adolescents, appear to develop them with abilities, to make informed, reasoned, and responsible decisions over sexual and reproductive health (SRH) issues than conventional pedagogies can do (Keto, Tilahun, & Mamo, Citation2020).
Literature has shown that innovative pedagogies used in facilitating sexuality education to adolescents have the potentials of enhancing their self-control over the urges to engage in sexual relationships, marry young, and or have children at young ages (Kemigisha, Bruce, et al., Citation2019). Developing adolescents under conventional pedagogies may imply that they will grow up misinformed about comprehensive SRH information and its consequences remain common (Boonstra, Citation2021). To address such a pedagogical gap, scholars and practitioners appear in the frontline in encouraging educators to develop and adopt problem-based pedagogy (PBP) in facilitating various lesson materials in schools (Kwan, Citation2019). The PBP is a learner-centered pedagogy that uses real-life or hypothetically ill-structured problems as the motivator of learning among learners (Utomo, Joyoatmojo, Yutmini, & Suryani, Citation2022).
The pedagogy can be implemented in two forms including using pure PBP (Introducing real-life problems to learners without using any other pedagogies such as lectures, demonstrations, or role-play). Hybrid PBP is another form of PBP whereas the problem is introduced to learners using PBP and any other pedagogies such as a lecture. Facilitator-guided small groups are formed and opportunities are provided among learners to resolve ill-structured and real-life problems by using their existing knowledge, and experiences (Millanzi & Kibusi, Citation2020b). According to Wong and Kan (Citation2022) and Pyper (Citation2021), PBP is effective in a diversity of learners in teacher-training programs, higher schools, elementary schools, and middle, and low-income countries.
The PBP is now practiced implemented in a variety of professional schools including medicine, business administration, engineering studies, leadership education, architecture, teacher education, nursing, chemical engineering, law schools, and social work disciplines. Though very few, available comparative scholarly works have demonstrated pieces of evidence of the effect of PBP over the LBP in secondary school students’ learning behaviors by influencing them to take responsibility for their learning with minimal support and guidance from facilitators. The work of Karimi et al. (Citation2019) explored the effect of PBP on improving health-promoting behaviors among girl students where they found that the total girls’ health literacy was significantly improved (p < 0.001) with higher mean scores after intervention than girls in the control group did.
Students guided under PBP have been reported to be able to develop specific, relevant problem-solving skills, life-long learning attitudes challenges handling skills, and completion of tasks in a real problem-driven environment (Kelly, Hyde, & Abdalla, Citation2022). However, there is misguided knowledge as to whether improved curricula and pedagogical practice of the nature of PBP can work in facilitating SRH learning among adolescents in ordinary level secondary schools in Tanzania (Millanzi & Kibusi, Citation2021). Scholars (Baku, Agbemafle, Kotoh, & Adanu, Citation2018; Ivanova et al., Citation2019; Wanje et al., Citation2017) have noted that parents, teachers, and health workers have a positive attitude towards STI screening and the implementation of school-based sexual educational syllabus among adolescents. However, they claim to experience trouble when they try teaching the social and physiological parts of it by using conventional pedagogies such as lectures, discussions, demonstrations, storytelling, and or initiate communication with adolescents about SRH matters.
Although the SRH content varies widely across schools, the outcry among stakeholders links the permanence use of conventional pedagogies in Tanzania with the permanence facilitation of biological than the psychological SRH contents among adolescents (Boti et al., Citation2019; Kemigisha, Bruce, et al., Citation2019). Topics such as the human reproductive system and sexual health behavior are taught in the classroom with great care and respect, taking into consideration the prevailing socio-cultural sensitive issues. Furthermore, school teachers and health workers who are invited to facilitate SRH learning among adolescents in schools, tend to make their own decisions regarding what, how, and when to implement it, which is commonly facilitated by using didactic pedagogies (Seidu et al., Citation2022).
The SRH lesson materials are argued to adopt more western lifestyle contents, problems, scenarios, which hardly reflect the existing contexts of adolescents (Boonstra, Citation2021). The noted SRH pedagogical situation may imply that there is no formal guideline with pedagogical prescriptions to guide teachers, health workers, and other facilitators in facilitating SRH learning among adolescents. In the same context, literature has exposed that, the existing guidelines used in the country seem to lack robust prescriptions about the coverage, dosage, timing, frequency, and its associated pedagogies to facilitate comprehensive and age-appropriate SRH lesson materials among adolescents (Petok & Marcell, Citation2022).
Findings by Frimpong et al. (Citation2021) for example have noted that teachers and or health workers implement the existing curricula materials using conventional teaching and assessment approaches as pedagogical bases in facilitating SRH learning among adolescents. The permanence use of conventional pedagogies in school curricula, project, interventions, and other programs are argued here to lead to pedagogical inadequacies when facilitating SRH learning among adolescents (Kemigisha, Ivanova, et al., Citation2019). On one hand, to continue implementing SRH education programs via conventional pedagogies may imply that teachers, health workers, and or other facilitators might continue experiencing challenges to assist adolescents to develop self-control over sexual temptations, harassment, and peer/parental sexual pressure when they resort to using didactic pedagogies (Jacobs, Citation2022).
On the other hand, developing adolescents under conventional pedagogies may imply that they will grow up misinformed about comprehensive SRH information and its consequences remain common (Boti et al., Citation2019; Chavula et al., Citation2021). Therefore, this study employed a randomized controlled trial (RCT) to test the effect of integrated RH lesson materials in a PBP for shaping safe sexual behavior among adolescents in Tanzania. The integrated RH lesson materials in a PBP that have been developed and tested in this study are going to establish a strong bond and multidisciplinary collaboration and provide a sustainable pedagogical guide for both teachers and health workers in facilitating RH learning among adolescents in schools.
Using a PBP in facilitating SRH learning might enhance adolescents, teachers’ and health workers’ abilities to discuss and facilitate the biological and psychological part of the SRH lesson materials efficiently. This may help to empower adolescents with informed, reasoned, and responsible decisions over sexual behaviors and thus, reduce the rate of early onset of unsafe sexual behaviors among them.
Methods
Methods in this study were performed per Tanzanian University guidelines and regulations.
Study design, and location
The study employed a parallel randomized controlled trial (RCT) in Tanzanian ordinary level secondary schools using a longitudinal design incorporating a multicenter approach from September 2019 to September 2020. Table S1 summarizes the study timelines alongside study activities.
Study population
This study intended to investigate the full range of adolescents between 12 and 19 years in Tanzania's mainland. Adolescents between groups were matched in their ages, school ownership (only government-owned schools), school level (only ordinary level secondary schools), and years of study (Form I, II, and III) to assure their demographic characteristic similarities before the commencement of the study.
Eligibility criteria
The set inclusion criteria such as being at ordinary level secondary school, age between 12 and 19 years, exposed to SRH lesson materials, being not recruited in other projects, and informed consent were used to assess adolescents who suited to join the study. The principal investigator and research assistants obtained written informed consent from adolescents >18 years after briefing them about the aim, advantages, and roles throughout the study. Additionally, written informed consents from adolescents <18 years were given by parents or headteachers of the respective schools on behalf of adolescents’ parents after a thorough communication with them or legally acceptable representatives. The study excluded from four adolescents who were preparing themselves for their final form four examinations. Form four is a level in the ordinary level secondary education system in Tanzania in which students have to sit for the final national examination before graduation and successfully enrollment to advanced levels (Form five and form six).
Sample size determination
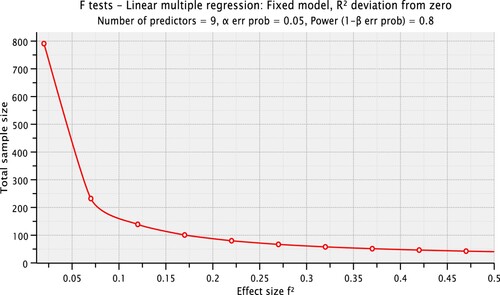
The necessary sample of the study was determined by using G*Power computer software program version 3.1.9.7 as recommended to be used in calculating the desired sample in randomized controlled trials by previous studies (Brydges, Citation2019; Yakubu, Citation2018). On one side, as indicated in , the F-tests set at a statistical test of linear multiple regression with fixed model and R2 deviation from 0 of a prior power of analysis was used to determine the minimum sample size set at α err probability = 0.05, power (1 – β err probability) = 0.80, and small effect size (Cohen’s d) = 0.02 that was a statistical power of the study.
Figure 1. The effect size that was used to calculate the total sample size of the study. Source: Study Plan (2020).
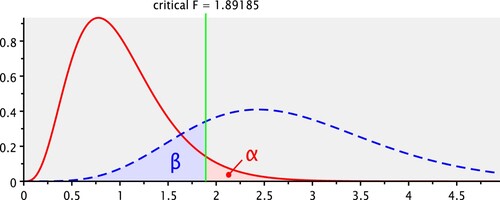
On the other hand, as shown in , with the critical F = 1.89185, a calculated minimum sample size was n = 791. A predicted attrition rate of the desired sample size was set at 10% (n = 79). Therefore. The minimum desired sample size of this study was 791 + 79 = 870 adolescents.
Figure 2. A critical value that was used to define the minimum sample size of the study. Source: Study Plan (2020).
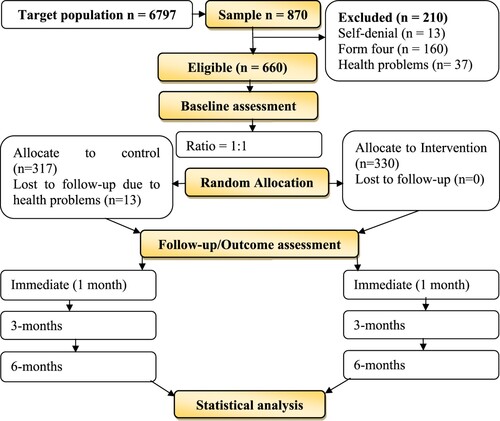
As indicated in , sums of 660 (75.9%) out of 870 adolescents were recruited to participate in the study. However, 210 adolescents were excluded due to different reasons. Among them, 160 (76.2%) were form four adolescents students who were preparing for their final national examination, 13 (6.2%) adolescents declined to join the study, and 73 (34.8%) adolescents due to various health problems.
Figure 3. Study flow diagram showing the recruitment of adolescents, their distribution by research arms, and study timelines. Source: Study plan (2020).
The procedure of random allocation of schools
Twelve (12) public ordinary-level secondary schools (3 schools from each of the 4 sampled districts) were randomly selected using a simple random sampling technique (by lottery method). Via the use of three random allocation cards (each card was written the name of the intervention such as pure PBP, Hybrid PBP, and LBP), immediately after baseline assessment each independent researcher of the study (3 researchers) per district who were labeled the names of schools, drew one out of three cards to identify the school arms. A random numbers table sampling method was employed to achieve a proportion of adolescents per school and class respectively. Criteria such as adolescents’ age were used to cluster adolescents at the class level into the early adolescence group (10–12 years), middle adolescence group (13–16 years), and late adolescence (17–19 years).
Blinding procedure
The study employed a double-blinding design by not letting the research assistants and adolescents know whether they were in a control or intervention group to minimize contamination of information and the adjustment of an intervention. Moreover, the outcome assessor and data analyst were also blinded to the study allocations.
Interventions
The interventions were implemented by 36 trained research assistants who were also having expertise in reproductive health matters and or teaching experiences. Interventions were implemented based on some comprehensive SRH theoretical guides for developing and adapting curriculum-based programs for adolescents (Kirby et al., Citation2011) and PBP development and implementation frameworks from previous studies (Millanzi & Kibusi, Citation2020a, Citation2021).
Training of research assistants
Some research assistants were trained about the integrated RH lesson material in a PBP (pure PBP and Hybrid PBP) and others about the standard RH lesson materials in an LBP alongside their implementations later in September 2019. Sums of 36 research assistants (18 assistants from Dodoma region and the other 18 assistants from Lindi region) with a proportional distribution of 3 assistants from each sampled school, were trained on the RH lesson materials, language, timing, pedagogical experiences, how to appraise the material, and learners’ assessment pedagogies to familiarize them before implementing it. By the end of the training, the skills of the research assistants on the implementation of the RH lesson materials were verified to be adequate through role-plays and return demonstrations.
Schedule and duration of the training about the integrated RH lesson materials among research assistants
The principal investigator based on the negotiation and consensus reached with research assistants made a schedule of training. Moreover, the principal investigator performed the training of research assistants. The training was scheduled to be performed per research arms for 12 days (Six days were used to train assistants at Lindi region and the remaining six days were used to train assistants at Dodoma region). Assistants assigned to each research arm (pure PBP, Hybrid PBP, and LBP) were trained independently for two days of which the first day covered the theoretical part and discussions (questions and answers) whereby the second day was for practices (demonstrations).
The theoretical part of the training covered issues about the structure of the RH lesson materials, nature of the content, scope, dosage, timing, teaching and learning organization, and teaching and learning experiences expected from research assistants and adolescents respectively. The practical part of the training covered issues around demonstrations of teaching and learning experiences that were prescribed in RH lesson materials among research assistants. The practical part of the training was flexible to repetitions to a saturation based on the requests from research assistants.
The training was scheduled to commence at 8:00 am and end up at about 4:00 pm every day alongside some breaks in between sessions as negotiated with research assistants. Separate unoccupied rooms from one among sampled schools in a particular region were used for training research assistants based on the permit from respective headteachers. Research assistants from Lindi region (Lindi municipal council and Kilwa district council) were trained first followed by those from Dodoma region (Dodoma city and Kondoa district council).
Sums of twelve research assistants were trained successfully and were able to demonstrate mastery in implementing the integrated RH lesson materials using pure PBP. Moreover, another group of twelve assistants was trained successfully too and on assessment, they were able to demonstrate mastery on the implementation of the integrated RH lesson materials using Hybrid PBP. Nevertheless, the other twelve research assistants were also trained successfully and managed to demonstrate mastery in implementing standard RH lesson materials using an LBP.
Descriptions of the interventions
As shown in . The intervention was conducted in a parallel design in 12 well-separated secondary schools in Lindi and Dodoma regions, Tanzania mainland. Three secondary schools were sampled from each of the four districts and were randomly allocated to either pure PBP, Hybrid PBP, or LBP. The intervention aimed at empowering adolescents to practice safe sexual behaviors such as delaying sexual debut, reducing the number of sexual partners, staying faithfully, intention to negotiate condom use, and saying ‘NO’ to unsafe sexual behavior. The interventions were delivered by trained research assistants, one per study location. There were no important changes to the methods of delivering the intervention after the commencement of the study.
Table 1. Descriptions of interventions per research arms.
Pure PBP group
Adolescents randomized to the pure PBP group received the same theoretical and practical concepts about SRH taught in the Hybrid PBP and control group but a pure PBP (IRH content + PBP). Adolescents learned by face-to-face delivery method for a maximum of 90 min per session a day and two sessions per week within four months. Sessions were scheduled to be conducted during morning times (half-day sessions) after some negotiations made with the head of the respective schools. The classrooms were set for adolescents to sit in a round style to promote eye contact during presentations. The same facilitator who implemented the material, which would have led to an unbiased interpretation of the results, evaluated the developed reporting checklist that was strictly followed.
The pure PBP teaching and learning of SRH contents integrated classroom and take-home activities whereas adolescents had to learn the contents in groups of 5–8 members. The most intensive components of the content delivery and assessment models were participatory, peer-assisted, inquiry, and peer-evaluation. There was no time devoted for mini-lecture to either introduce problems to fill the gaps within the scenario that appeared to be difficult for adolescents to solve on their own. Sessions commenced with the presentation of a real-life or hypothesized problem in ill-structured scenarios and puzzling pictures as a learning catalyst per each session.
Presentation of the problem was followed by the provision of a minimum of 30 min for self-study about the problem among adolescents to explore and identify potential solutions to solve it. Thirty minutes were then added for adolescents to share and discuss their works within their groups of 5–8 members. Extra time was provided among them to continue analyzing the problem and identify appropriate solutions to address them as a take-home activity (Outside activities).
The session of the second day was for experience and knowledge sharing, discussions, challenging information, and peer-evaluation. Adolescents in their groups had to present their works in the entire class, defend, and address any queries from their colleagues before they are being peer-rated. At the end of each session, 2–5 adolescents were randomly selected to share their experiences about the session including the teaching and learning styles. Their shared experiences were saved and used during analysis. The model of the session’s implementations continued the same to the end of an intervention.
Hybrid PBP group
Adolescents randomized to the Hybrid PBP group received the same theoretical and practical concepts about SRH taught in the pure PBP and control group but the Hybrid PBP (IRHC + Hybrid pedagogy + PBP). Moreover, all teaching and learning activities and procedures provided among adolescents in the Hybrid PBP group were the same as those provided among adolescents in the pure PBP group. An added portion to adolescents in the Hybrid group was that they were provided with a minimum of 10-minutes mini-lectures for introducing, and elaborating the problem in a scenario and to fill its associated gaps that appeared to be difficult for adolescents to address on their own.
LBP (control group)
The study involved an active treatment concurrent control group design. Adolescents randomized in the control group received the same SRH content as those in the pure and Hybrid PBP received via the LBP (IRHC + LBP). Adolescents learned by face-to-face delivery method for a maximum of 90 min per session a day and two sessions per week within four months. Sessions were scheduled to be conducted during morning times (half-day sessions) after some negotiations made with the head of the respective schools. The classrooms were set for adolescents to sit in a round style to promote eye contact during presentations. The same facilitator who implemented the material, which would have led to an unbiased interpretation of the results, evaluated the developed reporting checklist that was strictly followed.
The most intensive components of the content delivery and assessment models were teacher-led, questions and answers, and tests. Sessions commenced with a formal presentation of SRH terms, information and facts, concepts, pictures, and procedures followed by questions projected by the facilitator to adolescents and answers from adolescents. There was no time provided to adolescents for neither self-study, take-home activities nor after each session’s evaluation (for sharing their experiences about the implemented session). There were no important changes to the methods of delivering the intervention after the commencement of the study.
Criteria for discontinuing or modifying allocated intervention
Adolescents who dropped out without or with notification to the researcher or assistants at any point were discontinued from the study. Adolescents who requested to quit the study were discontinued.
Strategies to improve adherence to the intervention
Roll calls were taken at both the beginning and end of each session of the intervention. After each day’s session, adolescents were assigned simple works to do as homework to be shared in the next session. Examples of simple works adolescents were assigned included preparing storytelling about sexual coercions events encountered in life, finding real-life strategies to solve a presented problem in a scenario, finding a more relevant source of information over the provided ones, and or attaching meaning of the RH lesson materials in own body changes. One of the secondary school teachers of each study center was involved to help facilitate adherence and response rate of adolescents. Adolescents who adhered to the intervention regimen were provided with either a notebook, ruler, pen, pencil, or a rubber.
Data collection instruments
The study collected primary data using 15 items pre-tested Sexual-risk Behavior Beliefs and Self-esteem Scale (SRBBSES) adopted from previous studies (Fisher et al., Citation2018). Unis, Johansson, and Sällström (Citation2015), recommended the adopted instrument when a researcher intends to assess sexual behavior among young people. The items had ‘Yes-No’ responses of which ‘Yes’ had a value of 1 point while the ‘No’ response had a ‘0’ point. For sexual behavior ‘Yes’ response represented the presence of any of the mentioned sexual behavior in an item whereas ‘No’ represented no sexual behavior. Items were statistically transformed to compute a new end-point variable, which was dichotomized into ‘Yes’ (reported sexual behavior) and ‘No’ (did not report any sexual behavior). The study adhered to research ethical issues that would occur among recruited adolescents. For example, adolescents who reported to have been coerced to have sexual intercourse with someone in the past 12 months or within the time of the study (n = 11), his/her information was kept securely and confidentially, reported to the headteacher of the respective school and then linked to the hospital services to health checkups and treatment if required.
A sample of items included in an SRBBSES
Some young people have a boy or girlfriend whom they trust and have sex with him/her. Have you ever had sexual intercourse in your whole life with someone you love and trust?
Some young people are forced to have sexual intercourse against their will by a boy/girlfriend, a stranger, a relative, or an older person. Has this ever happened to you with any of the mentioned people?
Some young sexual partners use contraceptives such as condoms to avoid a pregnancy. Have you or your partners do this?
Some young people are forced or willingly watch sexual videos or photos through different media such as smartphones, the internet, magazines, movies, cinema, and or Television. Has this ever happened to you?
Some young people receive money or gifts in exchange for sexual intercourse. Has this ever happened to you?
Some people experience genital sores, bruises, rashes, or ulcers that need treatment. Has this ever happened to you during the past12/6 months?
Some people experience bad-smelling and abnormal genital discharge (Bloodstained or pus) that need to be treated. Has this ever happened to you during the past 12/6 months?
Validity of the research tools
The questionnaires were anonymously filled after being translated from English into the Swahili language to facilitate understanding of the items among adolescents. The inter-rater design revealed a content validity index of >0.8 and face validity of ≥95% which were highly recommended by previous studies (Shi, Mo, & Sun, Citation2012).
Reliability of the research tools
The questionnaires were pretested among 240 adolescents to determine a Cronbach’s alpha for their internal consistency reliability. Exploratory factor analysis was first performed for data reduction to get high weighed items above the suggested statistical thresholds (>0.3) as recommended by authors from previous studies (Hajjar, Citation2018; Lima, Barreto, & Assunção, Citation2012; Taherdoost, Sahibuddin, & Jalaliyoon, Citation2014; Ul Hadia, Abdullah, & & Sentosa, Citation2016). The correlation coefficient was set at a cut-off point of ≥0.30 whereas, the Kaiser-Meyer-Oklin (KMO) value of ≥0.05 and p < 0.05 was used to assess sampling adequacy and was set at a cut-off point of ≥0.60. Moreover, Bartlett’s test of sphericity was used to support the factorability of the correlation matrix and examine whether the original data were appropriate for factor analysis.
Sums of 15 items for sexual behavior were subjected to the factor analysis. The suitability of data for factor analysis was assessed whereas, an inspection of the correlation matrix revealed the presence of coefficients of ≤0.30. The KMO was 0.603, which was approximately equivalent to the cut-off point of 0.6; p < 0.05, and Bartlett’s test of sphericity was statistically significant [(χ2 = 5281.036 (2278); p < 0.01)]. A Cronbach Alpha was significantly above the recommended measurements (0.823; M = 10.60 ± 6.159; variance = 37.937).
Data analysis
Data were analyzed using SAS computer software program version 9.4. The main analytical strategy to minimize bias, missing data, and inequality of information that would occur during the allocation of adolescents to the intervention groups and lost to follow-ups, the intention-to-treat analysis opted. Descriptive analysis was used to establish sociodemographic characteristic profiles of adolescents alongside the proportions of sexual behaviors against them. Inferential statistics were determined through Difference-in-difference (D-I-D) analysis by comparing changes in outcomes over time between the population involved in the intervention and the population that is not (the control group).
The generalized estimating equation (GEE) model accounted for the repeated measures of the outcome variables that were opted to determine the effect of interventions on adolescents’ sexual behaviors. The general fixed effect D-I-D GEE model was presented using the following equation:
1)Whereas the chance of having outcome for subjects with characteristics x at time t, Time is a dummy variable for a period, equal to 1 when the outcome measurement was made in the post-period (end-line) and 0 for baseline measurements. Treatment is a dummy variable for subject treatment arm membership. The composite variable Time* Treatment is the interaction between time and treatment. In the model above, the parameter β0 represents the intercept, the log odds of having an event of interest in the Control treatment arm at the baseline measurement. The β1 is the change in log odds (log odds ratio) of having an event of interest in the Control treatment arm between baseline and end-line.
The parameter β2 indicates the difference in log odds of having an event of interest between the treatment and Control treatment arm at baseline, whereas the coefficient β3 (Interaction) measures the difference in slopes between the two treatment arms (Hybrid PBP versus Control or Pure PBP versus Control). Sociodemographic characteristic profiles of adolescents were controlled during analysis to discriminate the effect of integrated RH lesson materials in a PBP on sexual behaviors among them. The D-I-D GEE model presented above does not mean that it differs significantly from a more conventional GEE approach to regression. It is just a specification used in this study.
Ethics statement
Ethics approval and consent to participate: all methods were carried out by relevant guidelines and regulations: approved by the University of Dodoma (UDOM) Institutional Research Review Committee (IRRC). Ethics Clearance to reach schools: approved by education officers of the respective schools in the sampled study locations.
Results
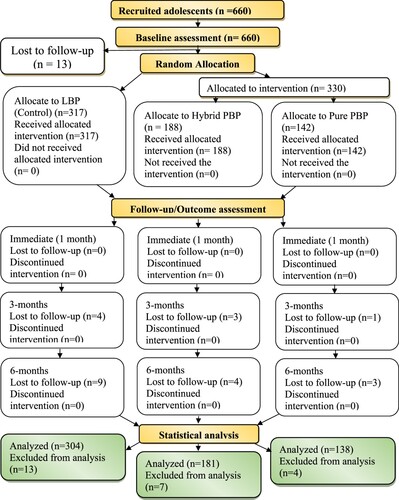
indicates that the attrition rate among adolescents in the pure PBP was 2.8%, while in the Hybrid PBP was 3.7% and the LBL group was 8.2%.
Figure 4. Study flow diagram indicating adolescents’ adherence to the interventions and lost to follow-ups by research arms throughout the study timelines. Source: Study plan (2020).
Adolescents’ sociodemographic characteristics profiles by research groups
indicates that the mean age of the adolescents was 15 ± 1.869 years with a minimum of 12 years and a maximum of 19 years. The most dominating age group was 13–16 years with 72.5% (n = 103) of adolescents were found in a pure PBP, 66.5% (n = 125) in a Hybrid PBP and 73.5% (n = 233) in a LBP group. Female adolescents were many (57.5%) between groups compared to males with 58.5% (n = 83) of female adolescents in a pure PBP, 58.5% (n = 110) in a Hybrid PBP and 56.5% (n = 179) in a LBP group. On the other hand, 58.3% (n = 377) of adolescents were sexually active by engaging in at least one unsafe sexual behavior including sexual relationship (39.9%), sexual intercourse (5.7%) multiple sexual partners (8.7%), and condom use (4.0%).
Table 2. Adolescents’ sociodemographic characteristics profiles by research groups (n = 660).
The proportions of adolescents’ sexual behavior between groups across the study timelines
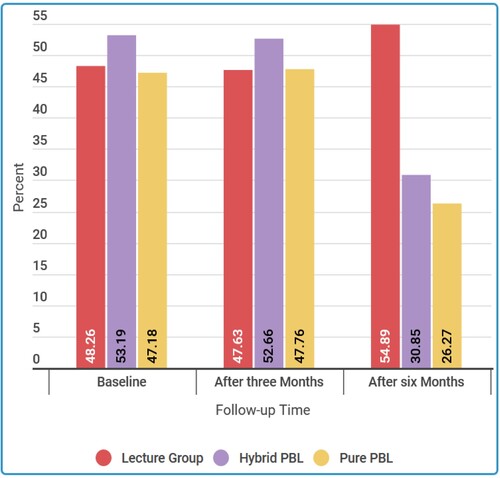
Findings of the GEE descriptive statistical analysis model in indicate that the proportions of adolescents’ sexual behavior were significantly similar at baseline. However, the majority of adolescents in the pure PBP intervention (26.3%) demonstrated a significant decrease in sexual behavior followed by adolescents in the Hybrid PBP intervention (30.9%); against their counterparts in the LBP group who demonstrated a high proportion of engaging in unsafe sexual behaviors (54.9%).
Figure 5. Proportions of adolescents’ overall sexual behavior between groups across the study timelines. Source: Filed data (2020).
Proportions of adolescents’ sexual behavior by sexual indicators between groups over the study timelines
shows that there was no significant difference in the indicators of baseline sexual behavior between groups (χ2 = 2.331; p > 0.05). However, the findings of the 6-months post-intervention show a significant decrease in adolescents’ sexual behavior and its associated indicators by 7.89% (from 49.46% at baseline to 41.57% at end-line) (χ2 = 12.672; p < 0.01). Sums of 41.57% (n = 259) of adolescents (pure PBP = 26.27%, Hybrid PBP = 30.85% and LBL group = 54.89%) were sexually active within 6-months after the commencement of the study. They engaged in at least one unsafe sexual behavior including sexual relationships (28.89%), sexual intercourse (6.26%), multiple sexual partners (4.33%), and low use of a condom (2.09%). Findings may imply that the intervention demonstrated a significant effect on shaping safe sexual behavior among adolescents.
Table 3. Proportions of adolescents’ sexual behavior and its associated sexual indicators between groups.
Empirical based parameter estimates (β) and odds ratio (OR) of the adjusted GEE for D-I-D analysis of the overall sexual behavior among adolescents
At baseline, the proportion of adolescents involved in sexual behaviors was not significantly different between groups (p > 0.05). However, the post-test findings in show that the magnitude of the D-I-D Odds ratio (AOR) for Hybrid PBP was (AOR = 0.30; P < 0.01; 95%CI: 0.1398, 0.5559). This implies that the proportion of adolescents engaged in sexual behaviors decreased at a higher rate from baseline to end-line in the Hybrid PBP group as compared to adolescents in the control group.
Table 4. The effect of integrated RH lesson material in a PBP on sexual behavior among adolescents.
Similarly, there was a significantly higher decrease in the proportion of adolescents involved in sexual behaviors moving from the baseline to end-line among adolescents in the Pure PBP group compared to those in control (AOR = 0.30; p < 0.01; 95%CI: 0.1386, 0.5487). The decrease of sexual behaviors was observed to be statistically significant by the study timelines among adolescents exposed in the pure PBP (AOR = −1.2148; p < 0.01; 95%CI: −0.0899, −3.4583) and those in the Hybrid PBP (AOR = −1.2125; p < 0.01; 95%CI: −0.9389, −3.3436) against adolescents in the control group. Thus, the integrated RH lesson materials in a PBP had a significant positive effect on reducing the proportion of sexual behaviors among adolescents in ordinary level secondary schools than the LBP.
Discussion
The interventions (pure PBP and Hybrid PBP) demonstrated a significant effect on self-reported sexual behaviors over the control group (LBP). The effect probably would be fueled by the nature of integrated RH lesson materials in a PBP because the implementation of the reproductive lesson materials started with facilitating biological materials followed by the psychological materials by the style of introducing problem first then learning process. The adopted theory and model would also catalyze self-directed and small group learning in the round table style among adolescents that are the requirements of active and inquiry learning for behavioral outcomes. The prescribed PBP lesson materials used real-life and hypothetical scenarios, illustrations, and outside activities to motivate adolescents to learn and therefore make them blend their classroom learning activities to real-life problem-solving skills.
The integrated RH lesson materials in a PBP were prototyped first through the involvement and frequent consultations with experts in curriculum development, SRH, and teaching. The prototyping process would assure adolescents get age-appropriate SRH lesson materials, in the right dose, frequency, and time to enhance the development of intentions for safe sexual behaviors. The trained research trainers who also had expertise in SRH matters and or teaching did the implementation process of integrated RH lesson materials in a PBP by using a prescribed facilitator guide that was developed by the principal investigator. The use of trained research trainers would control intervention bias from the principal investigator and thus, make clear discrimination of the effect of the pure PBP and Hybrid PBP over the LPB. However, the effect of the intervention was significantly prominent with the use of Hybrid PBP than pure PBP over the LBP.
The effect of Hybrid PBP over the pure PBP would probably be more prominent because trained research trainers would implement the PBP material more comfortably as it involved lecturing (common pedagogy) than it has been with the use of pure PBP alone (New to them). Combining Lecture (common pedagogy) and PBP would make it easy for the trainers and adolescents to adopt new learning environment than it has been with the use of Pure PBP alone. The sustainability of the effect of pure PBP and Hybrid PBP on self-reported sexual behaviors among adolescents was significantly prominent at six months of follow-up against the control (LBP). This means that the retention span of self-reported sexual behaviors among adolescents is six months before being exposed to new training.
The six-month retention span would be attributed to an active engagement of adolescents in solving real-life and or hypothetical problems, illustrations & scenarios. With this remark, the study findings provide robust evidence that the interventions (pure PBP and Hybrid PBP) were significantly more effective in enhancing adolescents’ self-reported intentions to practice safe sexual behaviors than the LPB group did. Inline of findings on adolescents’ sexual behaviors observed in this study, some previous studies for example Alabi and Oni (Citation2017), Landry, Turner, Vyas, and Wood (Citation2017), and Kazdouh, El-ammari, Bouftini, Fakir, and Achhab (Citation2019) in Nigeria, the United States, and Morocco respectively, argued that many adolescents initiate unsafe sexual behaviors very early in the course of their lives. Factors such as exposure to media have been mentioned to have the potentials of catalyzing unsafe sexual behaviors among adolescents. Moreover, media have been critiqued to disseminate uncontrolled SRH information and education in the form of a picture, cinema, and videos which is not valid and age-appropriate among adolescents (Deep, Salleh, & Othman, Citation2019). Similarities of these findings imply that controlling SRH information and education disseminated by media may help developing adolescents in culturally contextualized and ethical competencies against unsafe sexual behaviors towards their healthy adulthood.
Similarly, Keto et al. (Citation2020) exposed that sex of adolescents is closely linked with sexual activeness and early initiation of unsafe sexual behaviors among them. They uncovered that despite male adolescents initiating unsafe sexual behaviors at the adolescence stage, adolescent girls were sexually active more than males. Male adolescents who were economically well off spent some money in exchange for sexual intercourse with girls. This might probably be true than the same to be done by girls who in the developing world become the recipients of gifts, money, or other materials. Similarities of findings between the two studies might be attributed to the study population of which both, studied adolescents.
Needless to say, Nalukwago et al. (Citation2018) in Uganda observed approximately the same findings of this study that close parenthood plays a key role in controlling, moderating, and thus, delaying the onset of unsafe sexual behaviors among adolescents. The absence of close parenting to adolescents for example may lead them to be misinformed about SRH matters to high incidences of early onset of unsafe sexual behaviors among adolescents. Zou et al. (Citation2022) emphasized that adolescents who have little parental connectedness and communication about SRH matters, and or missing parental sexual security are sometimes end up engaging in unsafe sexual behaviors.
The study observed that the more adolescents were engaging and interacting with social groups, the less they demonstrate sexual behaviors than adolescents who are not. They also encounter social challenges from peer colleagues, adults, and other strange people that might probably catalyze them to develop non-cognitive skills in addressing them with minimal support from parents or caregivers.
On contrary, findings on the link between social cohesion and unsafe sexual behaviors among adolescents differ from those observed by Bingenheimer and Ahiadeke (Citation2016) in Ghana. They argued that if adolescents are exposed to their peers and other groups, are prone to engage in unsafe sexual behaviors due to a sense of imitating others’ behaviors. Owing to differences in socio-economic, and cultural backgrounds children have to interact and share, which may lead them to adopt and practice others’ behaviors. However, be it a contagious behavior or not, the findings of these studies give light that the majority of adolescents lack soft skills to make conscious, informed, and reasoned decisions over sexual behaviors. The difference in findings might be significant due to differences in geographical locations, social-cultural norms, and the methodological approaches between the two studies.
Tallying with the findings of this study, the effect of drug abuse on sexual behaviors found Xu, Chen, Yu, Joseph, and Stanton (Citation2017) who described the prevalence of risky sexual behaviors among Chinese adolescents. They found that 25.0% of the adolescents practiced sexual intercourse under the influence of alcohol and or other psychoactive drugs. Drug abuse among adolescents, therefore, can be considered in this study to be a positive predictor of unsafe sexual behaviors among adolescents that need to be addressed accordingly. Some adolescents in developed nations are driven to abuse them as boosters to sex, as a fashion to their partners, and or as a means to control shyness when approaching girls. The similarities of findings are significant as both studies revealed how drug abuse can predict unsafe sexual behavior among adolescents around the globe.
Although there are very few intervention studies about the effect of PBP on shaping safe sexual behaviors among adolescents, the findings of this study match with those found by Sudarsih and Ade (Citation2018) in Indonesia. They found that adolescents demonstrated a significant change in their unsafe sexual behaviors from 72.2% before to 62.2% after being exposed to a PBP intervention. This may imply that implementation of PBP that engages adolescents in a first position in solving real-life problems about SRH, they can easily be developed to be critical thinkers, problem-solvers, and autonomous individuals to make conscious, informed, and reasoned decisions over unsafe sexual behaviors. Similarities of these findings might be attributed to the fact that both studies examined the effect of PBP on adolescents’ sexual behaviors with almost similar methodological approaches.
Parallel to the work of Panjaitan (Citation2019) and Zhang et al. (Citation2019) on the best model of preventing adolescents’ unwanted pregnancy revealed that the implementation of problem-based pedagogy is more effective than other models such as LBP. Adolescents exposed to a PBP demonstrated self-control over sexual emotions, sexual coercion, and sexual temptations than when they demonstrated in other preventive models such as lectures and group discussions. These findings add new knowledge that, SRH lesson materials that are integrated into a PBP work better and positively in enhancing safe sexual behavior change among adolescents. The resemblance of findings between these two studies is bringing hope that integrating RH lesson materials in a PBP may hit a target of shaping safe sexual behaviors among adolescents.
Nevertheless, Yusra, Purwanto, and Dahlan (Citation2021) argued similarly to the argument of this study that the implementation of classroom-guided PBP can improve the negative attitude towards premarital and thus, shape safe sexual behaviors among adolescents. Adolescents developed under the PBP model tend to demonstrate intentions to stop sexual behaviors or not to initiate new ones. These findings provide an understanding to teachers, health workers, and or other facilitators of SRH information and education among adolescents that integrated RH lesson materials in a PBP can shape safe sexual behaviors among adolescents.
Strengths of the study
This study explored an important issue given robust evidence, which suggests that curriculum-based sex education interventional programs or projects are potential in shaping safe sexual behavior among adolescents. The study has advocated multidisciplinary strategies by developing integrated RH lesson materials in a PBP to guide teachers and or health workers in facilitating SRH learning among adolescents in Tanzania. Needless to say, this study has managed to develop procedural prescriptions about how to develop the integrated RH lesson materials in a PBP alongside its implementation and evaluation.
The study has managed to demonstrate the mechanisms to be adhered to produce and measure outcome variables such as adolescents’ SRH knowledge, soft skills, and sexual behaviors in the Tanzanian context. The current study has addressed the methodological gap by adopting sequential mixed methods through phenomenological design and randomized controlled trials to examine the effectiveness of integrated RH lesson materials in a PBP on adolescents’ SRH knowledge, soft skills, and sexual behaviors.
Conclusion
The two forms of PBP pedagogies appeared to be effective in enhancing self-reported sexual behavior change among adolescents than the LBP could do. These findings may imply that if schools through teachers work together with health workers in integrating and implementing RH lesson materials in a PBP, adolescents’ intentions to practice safe sexual behaviors can be developed for their healthy adulthood and future investment.
The implication of the study
The findings of this study might add new knowledge on the best ways to develop, adopt and evaluate innovative SRH pedagogies in a PBP via a randomized controlled trial to enhance its facilitation among adolescents. Moreover, findings might provide a path towards developing a sustainable, interdisciplinary, and formal SRH guideline to assist and guide teachers and or health workers during the facilitation of SRH learning among adolescents. Adolescents may also benefit from the findings of this study because they are going to be oriented on necessary soft skills to be adhered to against sexual storms and stresses in their day-to-day living.
Policy implication
Findings of this study give light to policymakers of the country that revisions and transformation of pedagogical approaches in secondary school curricula are very potential for successful facilitation of SRH learning among adolescents. Integrating RH lesson materials in a PBP may be a substitute to conventional pedagogies such as lectures, discussions, or demonstrations.
Limitation of the study
There was a lack of reliable evidence on actual comprehensive sexual education lesson content delivered in schools in the absence of video recording of sessions or active observation by the evaluation team. Thus, this study was unable to verify the completeness of the content in lessons during delivery or ensure that all research assistants did not use other components from other pedagogical approaches. As an attempt to address the limitation, there were unscheduled visits to the intervention centers by the research team including the principal investigator to oversee the research trainers’ adherence to the PBP procedural prescriptions during the facilitation of SRH learning to adolescents.
Nevertheless, verifiable research trainers’ reports and students’ oral feedbacks and notebooks for session activities were used as proxy evidence to confirm research trainers’ adherence to the PBP procedural prescriptions. This helped to ensure full and appropriate implementation of the integrated RH lesson materials in a PBP and therefore appropriate and comprehensive facilitation of SRH information and education among adolescents.
Desirability bias was another limitation faced by this study as the questionnaires included sensitive questions (items) that would lead adolescents to answer them in a manner they felt to be socially inappropriate. They would over or under respond to the questions by fearing what has been prohibited by the socio-cultural norms. It was impossible to determine in what direction such a bias operated. To minimize this limitation, the principal investigator and research trainers described the aims and benefits adolescents would get from participating in the study, and thus, anonymity procedures would be adhered to assure their dignity throughout the study. All consented adolescents were separated from their parents and or teachers for privacy and confidentiality and to make them feel free and comfortable to express themselves about SRH matters.
They were seated in a separate unoccupied room and each of them got seated on a sparse single chair and desk and were assured of their privacy, confidentiality, and security of the information they provided. The principal investigator and research assistants were available to address inquiries from adolescents throughout the data collection procedure. This helped to minimize the desirability bias and thus, have accurate and real-life SRH experiences from adolescents.
Informed consent
Written informed consent was obtained from all participants and written informed consent was obtained from parents/teachers or legally acceptable representatives for minors (below 18 years of age) as one of the criteria to participate in the study.
Consent for publication
Not applicable.
Supplemental Material
Download MS Word (40.1 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data presented in the study will be made available at the time of publication via institutional contact address http://repository.udom.ac.tz. Currently, data are owned by a third party (the Ministry of education, science, and technology, Tanzania – a sponsor) due to some sensitive information gathered from the sampled schools.
Additional information
Funding
References
- Alabi, O. T., & Oni, I. O. (2017). Teenage pregnancy in Nigeria: Causes, effect, and control. International Journal of Academic Research in Business and Social Sciences, 7(2), 17–32.
- Baku, E. A., Agbemafle, I., Kotoh, A. M., & Adanu, R. M. K. (2018). Parents ‘ experiences and sexual topics discussed with adolescents in the Accra Metropolis, Ghana : A qualitative study. Hindawi: Advances in Public Health, 2018, 12.
- Bingenheimer, J. B., & Ahiadeke, C. (2016). Peer influences on sexual activity among adolescents in Ghana. Study Family Planning, 46(1), 1–19. doi:10.1111/j.1728-4465.2015.00012.x
- Boonstra, H. D. (2021). Advancing sexuality education in developing countries: Evidence and implications. Evidence-Based Approaches to Sexuality Education, 14(3), 370–380.
- Boti, N., Hussen, S., Shegaze, M., Shibru, S., Shibiru, T., Zerihun, E., … Temtime, Z. (2019). Effects of comprehensive sexuality education on the comprehensive knowledge and attitude to condom use among first-year students in Arba Minch University: A experimental quasi-experimental study. BMC Research Notes, 1–7.
- Brydges, C. R. (2019). Effect size guidelines, sample size calculations, and statistical power in gerontology. Innovation in Aging, 3(4), 1–8. doi:10.1093/geroni/igz036
- Chavula, M. P., Svanemyr, J., Zulu, J. M., & Sandøy, I. F. (2021). Experiences of teachers and community health workers implementing sexuality and life skills education in youth clubs in Zambia. Global Public Health, 20(2), 1–15. doi:10.1080/17441692.2021.1893371
- Chen, E., Brody, G. H., & Miller, G. E. (2022). What are the health consequences of upward mobility? Annual Review of Psychology, 73(1), 599–628. doi:10.1146/annurev-psych-033020-122814
- Davidai, S. (2022). How do people make sense of wealth and poverty? Current Opinion in Psychology, 43, 42–47. doi:10.1016/j.copsyc.2021.06.010
- Deep, S., Salleh, B. M., & Othman, H. (2019). Study on problem-based learning towards improving soft skills of students in effective communication class. International Journal of Innovation and Learning, 25(1), 17–34. doi:10.1504/IJIL.2019.096512
- Delprato, M., & Frola, A. (2022). Zones of educational exclusion of out-of-school youth. International Journal of Educational Development, 88, 102532. doi:10.1016/j.ijedudev.2021.102532
- Duby, Z., Jonas, K., Appollis, T. M., Maruping, K., Mathews, C., Duby, Z., … Maruping, K. (2021). “Condoms Are boring”: navigating relationship dynamics, gendered power, and motivations for condomless Sex amongst adolescents and young people in South Africa. International Journal of Sexual Health, 33(1), 40–57. doi:10.1080/19317611.2020.1851334
- Fisher, T. D., Davis, C. M., Yarber, W. L., Davis, S. L., Nemerofsky, A. G., & Carran, D. T. (2018). Handbook of sexuality-related measures. 1–3. doi:10.4324/9781315881089.ch3
- Frimpong, J. B., Budu, E., Adu, C., Mohammed, A., Tetteh, J. K., Seidu, A., & Ahinkorah, B. O. (2021). Comprehensive HIV/AIDS knowledge and safer sex negotiation among adolescent girls and young women in sub-Saharan Africa. Journal of Biosocial Science, 1–13. doi:10.1017/S0021932021000493
- Hajjar, S. T. E. L. (2018). Statistical analysis: Internal consistency reliability and construct validity. International Journal of Quantitative and Qualitative Research Methods, 6(1), 27–38. ISSN2056-3639.
- Ivanova, O., Rai, M., Mlahagwa, W., Tumuhairwe, J., Bakuli, A., Nyakato, V. N., & Kemigisha, E. (2019). A cross-sectional mixed-methods study of sexual and reproductive health knowledge, experiences, and access to services among refugee adolescent girls in the Nakivale refugee settlement, Uganda. Reproductive Health, 16(1), 1–11. doi:10.1186/s12978-019-0698-5
- Jacobs, A. J. (2022). Sexual and Reproductive Issues I: Education; Reproductive Choices. 90(ILB), 221–238. doi:10.1007/978-3-030-87698-2_12.
- Karimi, N., Saadat-Gharin, S., Tol, A., Sadeghi, R., Yaseri, M., & Mohebbi, B. (2019). A problem-based learning health literacy intervention program on improving health-promoting behaviors among girl students. Journal of Education and Health Promotion, 8(251), 1–19.
- Kazdouh, H. E., El-ammari, A., Bouftini, S., Fakir, S. E., & Achhab, Y. E. (2019). Perceptions and intervention preferences of Moroccan adolescents, parents, and teachers regarding risks and protective factors for risky sexual behaviors leading to sexually transmitted infections in adolescents: Qualitative findings. Reproductive Health, 16(138), 1–17.
- Keats, E. C., Akseer, N., Thurairajah, P., Cousens, S., Bhutta, Z. A., Ali, H., … Zhu, Z. (2022). Multiple-micronutrient supplementation in pregnant adolescents in low- and middle-income countries: A systematic review and a meta-analysis of individual participant data. Nutrition Reviews, 80(2), 141–156. doi:10.1093/nutrit/nuab004
- Kelly, D., Hyde, S., & Abdalla, M. E. (2022). Mapping health, social, and health system issues and applying a social accountability inventory to a problem-based learning medical curriculum. Medical Education Online, 27, 1. doi:10.1080/10872981.2021.2016243
- Kemigisha, E., Bruce, K., Ivanova, O., Leye, E., Coene, G., Ruzaaza, G. N., … Michielsen, K. (2019). Evaluation of school based comprehensive sexuality education program among very young adolescents in rural Uganda. BMC Public Health, 19, 1. doi:10.1186/s12889-019-7805-y
- Kemigisha, E., Ivanova, O., Ruzaaza, G. N., Ninsiima, A. B., Kaziga, R., Bruce, K., … Michielsen, K. (2019). Process evaluation of a comprehensive sexuality education intervention in primary schools in South Western Uganda. Sexual and Reproductive Healthcare, 21, 51–59. doi:10.1016/j.srhc.2019.06.006
- Keto, T., Tilahun, A., & Mamo, A. (2020). Knowledge, attitude, and practice towards risky sexual behaviors among secondary and preparatory students of Metu town, southwestern Ethiopia. BMC Public Health, 20(1), 1–8. doi:10.1186/s12889-020-09371-4
- Kirby, D., Coyle, E., Alton, K., Rolleri, F., & Robin, L., & L, E. (2011). Reducing Adolescent Sexual Risk A Theoretical Guide For Developing And Adapting Curriculum-Based Programs. ETR Associates 4 Carbonero Way Scotts Valley, California 95066. www.efsc.org.
- Kwan, C. Y. (2019). A thorny path: The developmental course of problem-based learning for health sciences education in Asia. Advances in Health Sciences Education, 24(5), 893–901. doi:10.1007/s10459-019-09920-6
- Lanari, D., Mangiavacchi, L., & Pasqualini, M. (2020). Adolescent sexual behaviour and academic performance of Italian students. Genus, 76, 1. doi:10.1186/s41118-020-00093-4
- Landry, M., Turner, M., Vyas, A., & Wood, S. (2017). Social media and sexual behavior among adolescents: Is there a link? JMIR Public Health and Surveillance, 3(2), e28. doi:10.2196/publichealth.7149
- Lima, E. d. P., Barreto, S. M., & Assunção, AÁ. (2012). Factor structure, internal, consistency and reliability of the posttraumatic stress disorder checklist (PCL): an exploratory study. Trends in Psychiatry and Psychotherapy, 34(4), 215–222. doi:10.1590/S2237-60892012000400007
- Mbachu, C. O., Agu, I. C., Eze, I., Agu, C., Ezenwaka, U., Ezumah, N., & Onwujekwe, O. (2020). Exploring issues in caregivers and parent communication of sexual and reproductive health matters with adolescents in ebonyi state, Nigeria. BMC Public Health, 20(1), doi:10.1186/s12889-019-8058-5
- Millanzi, W. C., & Kibusi, S. M. (2020a). Exploring the effect of problem-based facilitatory teaching approach on metacognition in nursing education: A quasi-experimental study of nurse students in Tanzania. Nursing Open, 1–15. doi:10.1002/nop2.514
- Millanzi, W. C., & Kibusi, S. M. (2020b). Exploring the effect of problem-based facilitatory teaching approach on metacognition in nursing education: A quasi-experimental study of nurse students in Tanzania. Nursing Open, 7(5), 1431–1445. doi:10.1002/nop2.514
- Millanzi, W. C., & Kibusi, S. M. (2021). Exploring the effect of problem-based facilitatory teaching approach on motivation to learn: A quasi-experimental study of nursing students in Tanzania. BMC Nursing, 20(1), 3. doi:10.1186/s12912-020-00509-8
- Millanzi, W. C., Kibusi, S.,M., & Osaki, K. M. (2022). Effect of integrated reproductive health lesson materials in a Problem-Based Pedagogy on soft skills for safe sexual behaviour among adolescents: A school-based randomized controlled trial in Tanzania. PLoS One, 17(2):e0263431. doi:10.1371/journal.pone.0263431
- MoHCDGEC. (2018). National Adolescent Health and Development Strategy 2018–2022. 2057, 1–41. https://tciurbanhealth.org/wp-content/uploads/2017/12/020518_Adolescent-and-Develo pment-Strategy-Tanzania_vF.pdf.
- Moran, D., & Taylor, L. K. (2022). Outgroup prosocial behaviour among children and adolescents in conflict settings. Current Opinion in Psychology, 44, 69–73. doi:10.1016/j.copsyc.2021.08.030
- Nalukwago, J., Crutzen, R., Borne, B. V. D., Bukuluki, P. M., Bufumbo, L., Zikusooka, A., … Alaii, J. (2018). Adolescents discussing sexual behaviors With Key influencing audiences. Global Journal of Health Science, 10(8), 91–106. doi:10.5539/gjhs.v10n8p91
- Panjaitan, A. A. (2019). Model of prevention of adolescent unwanted pregnancy in Indonesia: Review article. International Journal of Research in Law Economic and Social Sciences, 1(2), 60–73.
- Pascoe, L. (2020). Negotiating HIV and pregnancy prevention and sexual pleasure amongst heterosexual men and women in South Africa. International Journal for Research Intervention and Care, 23(1), 115–130.
- Petok, W. D., & Marcell, A. V. (2022). The acquisition of sexual and reproductive health knowledge. Psychological and Medical Perspectives on Fertility Care and Sexual Health, 1, 3–20. doi:10.1016/B978-0-12-822288-1.00014-2
- Pyper, J. S. (2021). Problem-Based learning as a professional learning model helped me with the sudden demand ofremote learning, and I believe is helping me offer students ownership and their own voice in their learning. Acedemia Letters, 563, 1–6.
- Ringrose, J., Regehr, K., & Whitehead, S. (2021). Teen girls’ experiences negotiating the ubiquitous dick Pic: Sexual double standards and the normalization of image based sexual harassment. Sex Roles, 85(9–10), 558–576. doi:10.1007/s11199-021-01236-3
- Seff, I., & Stark, L. (2022). The role of social norms: A case study of intimate partner violence Among adolescent girls in Nigeria. Child Behavioral Health in Sub-Saharan Africa, 157–180. doi:10.1007/978-3-030-83707-5_9
- Seidu, A. A., Ameyaw, E. K., Ahinkorah, B. O., Baatiema, L., Dery, S., Ankomah, A., & Ganle, J. K. (2022). Sexual and reproductive health Education and its association with ever use of contraception: A cross - sectional study among women in urban slums, Accra. Reproductive Health, 19(7), 1–10.
- Shi, J., Mo, X., & Sun, Z. (2012). Content validity index in scale development. Journal of Central South University (Medical Sciences), 37(2), 152–155.
- Sodré, C. P., Spindola, T., Rose, E., & Martins, C. (2022). Prevention of sexually transmitted infections among young people and the importance of health education A prevenção das infecções sexualmente transmissíveis entre jovens e a importância. Enfemeria Global, 65, 102–115.
- Sudarsih, S., & Ade, P. (2018). Effect Of problem-based instruction (PBI) learning method on behavior prevention of HIV/AIDS prevention in adolescent. International Journal of Nursing and Midwifery Science (IJNMS), 2(2), 197–204. e-ISSN: 2597-9345.
- Tadjer, H., Lafifi, Y., Seridi-Bouchelaghem, H., & Gülseçen, S. (2020). Improving soft skills based on students’ traces in problem-based learning environments. Interactive Learning Environments, doi:10.1080/10494820.2020.1753215
- Taherdoost, H., Sahibuddin, S., & Jalaliyoon, N. (2014). Exploratory factor analysis: Concepts and theory. 2nd International Conference on Mathematical, Computational and Statistical Sciences, 375–382. doi:10.2139/ssrn.3205035.
- Ul Hadia, N., Abdullah, N., & & Sentosa, I. (2016). An easy approach to exploratory factor analysis: Marketing perspective. Journal of Educational and Social Research, 6(1), 215–223.
- UN. (2019). World Population Prospects 2019. Population Division, Department of Economic and Social Affairs, June, 46. https://population.un.org/wpp/Publications/.
- UN. (2020). World Fertility and Family Planning 2020: Highlights. In World Fertility and Family Planning 2020: Highlights. doi:10.18356/9789210043694.
- Unis, B., Johansson, I., & Sällström, C. (2015). Rural high school students ‘ sexual behavior and self-esteem. Open Journal of Nursing, 5, 24–35. doi:10.4236/ojn.2015.51004
- United Nations. (2020). World Fertility and Family Planning 2020: Highlights. https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Jan/un_2020_worldfertilityfamilyplanning_highlights.pdf.
- Utomo, S. W., Joyoatmojo, S., Yutmini, S., & Suryani, N. (2022). Problem-based learning model with a scientific approach to improve higher order thinking skills. International Journal of Learning and Change, 14(1), 87. doi:10.1504/IJLC.2022.119515
- Wanje, G., Masese, L., Avuvika, E., Baghazal, A., Omoni, G., & Mcclelland, R. S. (2017). Parents ‘ and teachers ‘ views on sexual health education and screening for sexually transmitted infections among in-school adolescent girls in Kenya : a qualitative study. Reproductive Health, 14(95), 1–11.
- Wong, F. M. F., & Kan, C. W. Y. (2022). Online problem-based learning intervention on self-directed learning and problem-solving through group work : A waitlist controlled trial. International Journal of Environmental Research and Public Health, 19(720), 1–16.
- Xu, Y., Chen, X., Yu, B., Joseph, V., & Stanton, B. (2017). The effects of self-efficacy in bifurcating the relationship of perceived benefit and cost with condom use among adolescents: A cusp catastrophe modeling analysis. Journal of Adolescence, 61, 31–39. doi:10.1016/j.adolescence.2017.09.004
- Yakubu, I. (2018). Determinants of adolescent pregnancy in sub-Saharan Africa : a systematic review. Reproductive Health, 15(15), 1–11.
- Yusra, T., Purwanto, E., & Dahlan, U. A. (2021). The effectiveness of classroom guidance with problem-based learning and jigsaw techniques to improve negative attitudes towards premarital sexual behavior. Jurnal Bimbingan Konseling, 10(9), 7–12.
- Zhang, Y., Xu, G., Hou, J., Shi, P., Chang, S., Wu, A., … Shi, J. (2019). Problem-based learning could tackle the issue of insufficient education and adherence in people living with HIV/AIDS. Frontiers in Pharmacology, 10, 1–7. doi:10.3389/fphar.2019.00001
- Zou, S., Cao, W., Jia, Y., Wang, Z., Qi, X., Shen, J., & Tang, K. (2022). Sexual and reproductive health and attitudes towards sex of young adults in China. BMJ Sexual and Reproductive Health, 48(e1), E13–E21. doi:10.1136/bmjsrh-2020-200766
