
ABSTRACT
Objectives: To understand why some long-term childhood cancer survivors experience positive adjustment in the long run,[Q1] this study aimed to (1) explore associations between well-being, health status, social support, and emotion regulation (ER) strategies in a cohort of long-term childhood lymphoblastic leukemia (cALL) survivors, (2) identify the individual contribution of each ER strategy to well-being (3) and their interaction with social support.
Methods: We used data from 92 participants from the PETALE cohort (51% female, aged 24 ± 7 years). Measures included well-being (WHO-5), health status (15D), social support (SSQ-6), cognitive reappraisal and expressive suppression (ERQ), and emotional processing and expression (EAC). We modeled the odds of high well-being adjusting for health status in logistic regressions and explored the moderating role of social support with bootstrap techniques. Independent of clinical history, high well-being was associated with better health status, higher social support, more frequent use of cognitive reappraisal and emotional processing.
Results: We found a main contribution of emotional processing to well-being (OR = 2.12, 95% CI = 1.09-5.37). The interaction between low suppression and high social support was significant (OR = .40, 95% CI = .13-.79). Probabilities for high well-being were 96% when expressive suppression was low and social support was high. Results suggest approaching one's own emotions may contribute to well-being in long-term childhood cancer survivors.
Clinical implications: Combining curbing emotional suppression with promoting supportive social environment could be a promising target for future supportive care interventions in survivors.
Introduction
Despite improved 5-year survival rates of 90%, long term childhood acute lymphoblastic leukemia (cALL) survivorship is associated with multiple late adverse effects (Kızılocak & Okcu, Citation2019). Approximately two-thirds of childhood cancer survivors will experience chronic treatment-related side effects known as long-term adverse effects (Canadian Cancer Society, Citation2023; Eiser, Citation2007). As adults, childhood cancer survivors are at risk for chronic and serious health problems. For example, in a sample of 1,713 adult pediatric cancer survivors, the cumulative prevalence of being diagnosed with at least one chronic condition at age 45 was estimated to be 95.5% (Hudson et al., Citation2013). The prevalence is estimated to be 29% for adults aged 25–44 and 48% for those aged 45–64 in the general population (Canadian Institute for Health Information, Citation2011). Long-term adverse effects include cardiac, metabolic, bone, and neurocognitive complications (Hudson et al., Citation2013; Wilson & Ness, Citation2013). These negatively affect the quality of life of this population (Kızılocak & Okcu, Citation2019). From a psycho-behavioral viewpoint, studies have suggested a wide array of long-term negative consequences of cALL inattention-hyperactivity, social withdrawal, and learning difficulties (Jacola et al., Citation2016).
Most of psychosocial research on adjustment to pediatric cancer has focused on psychological risk such as distress, anxiety, and depression (Anestin et al., Citation2018; Oancea et al., Citation2014; Płotka et al., Citation2021). While these studies identified subsets of survivors reporting significant adjustment issues, a consistent result has been that pediatric cancer survivors globally demonstrate positive adjustment once their treatments are completed (Yallop et al., Citation2013; Zebrack & Chesler, Citation2002; Zebrack et al., Citation2012). For example, compared to healthy peers, they were even globally less likely to report abnormal psychosocial well-being and prosocial behavior issues (Yallop et al., Citation2013). Despite the widespread observation of frequent physical late effects, a meta-analysis investigating psychosocial late effects in childhood cancer survivors from 35 studies revealed that in average, survivors did not experience more psychosocial issues such as depression and distress than their healthy peers (Bitsko et al., Citation2016).
This positive adjustment to cancer is referred to as resilience. In the context of cancer, resilience can be defined as the protective attributes and personal characteristics of the individual that are considered modifiable and conducive to adjustment to cancer (Eicher et al., Citation2015). The latter include, for example, seeking social support, optimism, a sense of coherence, and positive emotions, and could be the target of interventions aimed at optimizing resilience (Chmitorz et al., Citation2018; Helmreich et al., Citation2017). In the present study, survivors’ well-being is considered as a manifestation of survivors’ psychological adaptation. A similar operationalization of resilience has been used in studies examining resilience factors (e.g. Barakat et al., Citation2021; Helmreich et al., Citation2017).
It is both curious and encouraging that despite experiencing late adverse effects in the physical sphere, most survivors do not report more frequent or intense psychosocial issues. To date, we do not know why some study participants fare so well on their journey with cancer while a minority experience distress and adjustment difficulties. While risk factors and psychological risk are largely investigated in the childhood cancer survivorship literature (e.g. Anestin et al., Citation2018; Oancea et al., Citation2014; Płotka et al., Citation2021), protective factors and positive adjustment have received little interest so far (Zebrack et al., Citation2012). Exploring positive outcomes in childhood cancer survivors may help for a better understanding of adjustment, which could greatly inform psychosocial interventions. To date, positive adjustment in this population has been studied by examining its potential contributors (e.g. Yi et al., Citation2015; Zebrack et al., Citation2012). Unfortunately, these results are derived from studies that did not control for health status, a major factor in this domain, as better health (or lower levels of long-term effects) could contribute to positive adjustment or well-being (Ngamaba et al., Citation2017).
Individual psychological functioning may play a key role in adjustment to adversity such as cancer (Fletcher & Sarkar, Citation2013). Adaptive emotion regulation such as cognitive reappraisal, emotional processing, and emotional expression or disclosure were found to promote positive outcomes in adult cancer patients (Cho et al., Citation2013; Conley et al., Citation2016; Karimzadeh et al., Citation2021; Peh et al., Citation2017). In contrast, maladaptive emotion regulation strategies such as expressive suppression were associated with negative outcomes (Peh et al., Citation2017). Although it is unknown, it is probable that the same processes operate in the context of childhood cancer.
More importantly, theory and research have identified social contexts as key to the functioning of emotion regulation (Zaki & Williams, Citation2013). Sharing and processing emotions in a supportive environment typically helps characterizing, organizing, understanding, and controlling emotions. An essential ingredient of adjustment probably lies in the social sharing of emotions (SSE), i.e. an interaction between appropriate emotional regulation strategies and a supportive social environment. SSE is defined as the re-evocation of emotions in a socially shared language and involves a recipient (Rimé, Citation2009a). SSE most often takes the form of conversations with an interlocutor in which an emotional episode, feelings, and reactions are discussed. It will help with understanding of what happened, strengthening social bonds, and reinforcing social support (Rimé, Citation2017). The search for social support is a primary reason for SSE (Luminet, Citation2008). Through SSE, the individual's social network can effectively help him or her, during an emotional episode, to reinterpret the situation in a more positive light. A second motive corresponds to cognitive articulation, which makes it possible to reorganize the emotional event and to adopt a less emotion-centric point of view (Luminet, Citation2008; Rimé, Citation2009b). In this sense, it seems that for the cognitive work of emotional regulation to take place, the individual must first express his or her emotions to an interlocutor.
There are two types of SSE: a cognitive mode and a socio-affective mode (Rimé, Citation2009b). The socio-affective mode meets the narrator's needs by providing support and comfort. The cognitive mode aims to reconstruct meaning and reframe the emotional episode, enabling the work necessary to achieve emotional recovery (Rimé, Citation2009b). Cognitive reappraisal (Gross & John, Citation2003) and emotional processing (Stanton et al., Citation2000) are two emotional regulation strategies that facilitate this cognitive work.
It is clear, then, that the social support offered by those around the individual who has experienced an emotional episode plays an important role in regulating the emotions associated with it. Although applied to different adversity situations (e.g. Chukwuemeka & Obioha, Citation2024; Coo et al., Citation2022; Demirtas et al., Citation2015), this important idea has only been rarely explored in cancer research, with results in breast cancer survivors suggesting that expressing one’s feeling in a caring and listening environment could favour lower emotional distress (Boinon et al., Citation2014).
In sum, it is unclear why a large part of cancer survivors reports such levels of positive adjustment and well-being while a minority will report low well-being, when both show deteriorated health over the long run (Anestin et al., Citation2018; Bitsko et al., Citation2016; Yallop et al., Citation2013; Yi et al., Citation2015; Zebrack & Chesler, Citation2002; Zebrack et al., Citation2012). Despite the bulk of studies explaining psychosocial risk in this population, we do not know which factors may promote positive adjustment in childhood cancer survivors. The mechanisms explaining the role of these factors also remain unknown. Modeling positive adjustment and resilience in this population is a necessity to identify key targets for future supportive activities (D'Agostino et al., Citation2011). In addition, previous studies identifying resilience factors in this population have not controlled for survivors’ health status, making it impossible to isolate their effect and measure their impact.
The overall objective of this study was to identify individual and social contributors to well-being in long-term cALL survivors. Our first objective was to explore associations between well-being, health status, social support, and emotional regulation components typically related with positive adjustment: cognitive reappraisal, emotional processing, and emotional expression-suppression. Our second objective was to identify the contributing role of each of the ER strategies to well-being, independent of health status. In line with the SSE theory, we also expected social support to moderate the effect of emotion regulation strategies, i.e. enhancing the effect of emotional expression and mitigating the effect of suppression.
Materials and methods
This study was part of the PETALE multidisciplinary cohort description conducted at CHU Sainte-Justine (Montreal, Quebec, Canada) aiming at characterizing late adverse effects in long-term cALL survivors (Marcoux et al., Citation2017). The present study focuses on measures taken at the second recall involving those who necessitated in-depth investigations due to probable sequelae detected at the first recall. The study design is cross-sectional and based on self-reports.
Participants
Full recruitment and data collection process are available in previous reports (Marcoux et al., Citation2017). In summary, survivors had received their diagnosis before the age of 19 years between 1987 and 2010, and were at least 5 years post-diagnosis. They had been treated following Dana-Farber Cancer Institute/cALL Consortium protocols 87–01 to 05-01. Survivors who received hematopoietic stem cells transplant, whose cancer had relapsed or was refractory were excluded. Those who showed extreme phenotypes on at least one of the studied long-term effect health domains were invited to an in-depth investigation (N = 100) ().
Figure 1. Flowchart of participants. cALL, childhood acute lymphoblastic leukemia.
Note. As all questionnaires were missing for these survivors and the frequency of missing data was low, we decided not to impute missing data.
Procedure
Survivors and their parents if needed completed questionnaires on their psychological health and adjustment between April 2014 and April 2016 during their visit at the hospital or at home (return envelope to be sent within three weeks). Ethical approval was given by CHU Sainte-Justine ethical board (#2013-479, 3607) in accordance with the Declaration of Helsinki. Written consent was obtained from all participants (Marcoux et al., Citation2017).
Measures
Demographic and Clinical Information. Sociodemographic and clinical history were abstracted from medical files. Variables of interest were sex, first language, age, ethnicity, marital status, employment, age at diagnosis, age at the end of treatment, ALL risk status, treatment protocol, and radiotherapy.
Well-being. The World’s Health Organization Well-Being Index (WHO-5) (WHO, Citation1998) was used to measure survivors’ well-being. The WHO-5 is composed of 5 items (this sample α = .91) and uses a 6-point Likert scale (e.g. I have felt cheerful in good spirits, 0 = never, 5 = all the time). Items are summed to generate a global score and multiplied by 4 to obtain a 0–100 score, with higher scores reflecting higher well-being. As recommended, we used a cut point of > 50 to define high well-being (Topp et al., Citation2015).
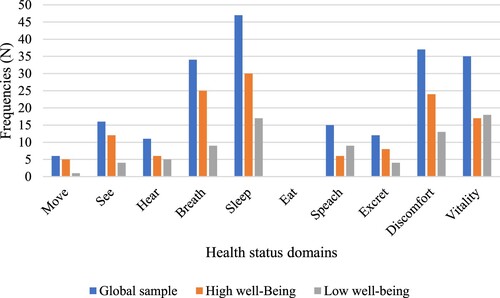
Health Status. We used the 15D (Sintonen, Citation2001), and its adapted forms for younger individuals 16D (Apajasalo et al., Citation1996), 17D (Apajasalo et al., Citation1996), to assess survivors’ health functional status (Rondeau et al., Citation2021). The 15D aims to assess functional health status in 15 health domains. Each 1-item domain is measured with five options, from no issue (e.g. I am able to walk normally (without difficulty) indoors, outdoors and on stairs) to severe issue (e.g. I am completely bed-ridden and unable to move about). To avoid spurious associations with well-being, items on depression and psychological distress items were discarded (). As a global score we used a count variable reflecting the number of health domains with at least a mild physical difficulty. We considered the 10 health domains common to the 15D-16D-17D: mobility, vision, hearing, breathing, sleeping, eating, speech, excretion, discomfort, and vitality. A description of this count variable in the present sample is available in .
Figure 2. Frequencies of health function issues in 92 cALL survivors.
Note. cALL, childhood acute lymphoblastic leukemia. We used a count variable reflecting the number of health domains with at least a mild physical issue. A cut-point on the WHO-5 well-being index of > 50 for high-well being was used (Topp et al., Citation2015).
Social Support. We used the Social Support Questionnaire-Short Form (SSQ-6) (Sarason et al., Citation1987). The SSQ-6 is a 6-item instrument with two scores for each item: the perceived availability of support (SSQ-Number) and satisfaction toward social support (SSQ-Satisfaction). For the study, we used SSQ-Number (α = .92). Respondents indicate the name of the people they can rely on in different situations (e.g. Who accepts you totally including both your worst and best points?) The global score is computed by summing up the number of people reported for each item (range: 0-54).
Cognitive Reappraisal and Expressive Suppression. We used the Emotion Regulation Questionnaire (ERQ) (Gross & John, Citation2003). The ERQ is a 10-item instrument including two subscales, cognitive reappraisal (6 items, α = .84, e.g. When I want to feel more positive emotions (such as joy or amusement), I change what I’m thinking about), and expressive suppression (4 items, α = .84, e.g. When I am feeling negative emotions, I make sure not to express them). Items are responded on a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree), and are averaged within each subscale.
Emotional Processing and Emotional Expression. The Emotional Approach Coping Scales were used to measure emotional processing and emotional expression (EAC) (Stanton et al., Citation2000). The EAC includes two subscales, each designed to measure emotional processing (4 items, α = .83, e.g. I take time to figure out what I’m really feeling.) and emotional expression (4 items, α = .85, e.g. I take time to express my emotions). Both subscales use a 4-point Likert scale (1 = I don’t do it at all, 4 = I do it a lot).
Statistical analyses
After describing variables and exploring bivariate associations using standard procedures, we modeled the odds of reporting high well-being with multivariate logistic regressions. We entered each of the emotional regulation strategies in turn, social support, as well as its interaction with the emotional regulation strategy. We computed four models for cognitive reappraisal, expressive suppression, emotional processing, and emotional expression, respectively. All models were adjusted for health status. We used the PROCESS syntax version 3.5 for SPSS version 25. Bootstrapping was used to estimate the distribution of effects and 95% confidence intervals (95% CIs) with 5000 resamples. Results were significant if the 95% CIs of the estimate did not include 1.00. The full dataset and analyses procedures are available in Supplementary Material.
Ethics statement
Ethical approval was given by CHU Sainte-Justine ethical board (#2013-479, 3607) in accordance with the Declaration of Helsinki.
Results
In descriptive analyses, we found a majority of survivors with high well-being (73%, ). Notably, well-being subgroups did not differ on sociodemographic characteristics or clinical history.
Table 1. Sociodemographic and clinical characteristics of 92 cALL survivors.
When describing health status (), we found that participants presented a mean number of affected domains of 2.32 (SD = 1.94). The most frequent issues were on domains of Sleeping (51.1%), Discomfort and pain (40.2%), Vitality (38.0%), and Breathing (37.0%). Bivariate comparisons revealed that high well-being was associated with better health status, and less frequent issues on speech, discomfort, and vitality domains. This provides further justifications for controlling for health status in subsequent explanatory models. High well-being was also associated with higher social support, and a more frequent use of cognitive reappraisal and emotional processing ().
Table 2. Health status and psychosocial description of the study sample.
In multivariate models adjusted for health status, we found one main contribution of emotional processing (OR = 2.12, 95% CI = 1.09-5.37), with higher emotional processing contributing to higher odds of well-being (). Other main effects were nonsignificant. When looking into interactions with social support, we found the term expressive suppression x social support to be associated with well-being OR = .40, 95% CI = .13-.79) (). Other interaction terms were not associated with well-being (, Tables S1-S2).
Table 3. Summary of logistic regression moderation analysis predicting the odds of belonging to the high well-being subgroup depending on emotional processing controlling for health status (n = 92).
Table 4. Summary of logistic regression moderation analysis predicting the odds of high well-being by expressive suppression, social support, and their interaction (n = 92).
To interpret the significant interaction, we plotted high well-being group membership as a function of suppression for three contrasted levels of social support (). A subgroup was composed of participants benefiting from high social support and who reported low suppression (i.e. high expression). This combination (high social support and low suppression) increased the odds to report high well-being. Impressively, the probabilities to belong to the high well-being subgroup with this combination were of 96% (logit = 3.16). When suppression was high, the odds to show high well-being were the same regardless of the level of social support. The probabilities to belong to the high well-being subgroup were consistently around 70-71% (logit = .83; .88) for survivors with low, medium, and high social support.
Figure 3. Social support moderates the contribution of expressive suppression to well-being in a group of 92 cALL survivors.
Note. ERQ, Emotion Regulation Questionnaire. Models are adjusted for health status; As per the PROCESS output, Low social support = 11 people, Medium social support = 19 people, High social support = 30 people.
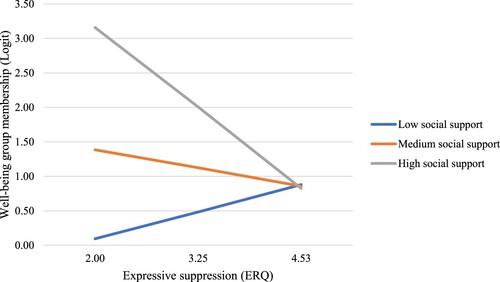
To yield additional details on the interaction, we used the Johnson-Neyman technique to probe the interaction (Hayes, Citation2020). This analysis showed that the interaction was significant only when social support counted 23 people or more (high social support condition represented in ).
Discussion
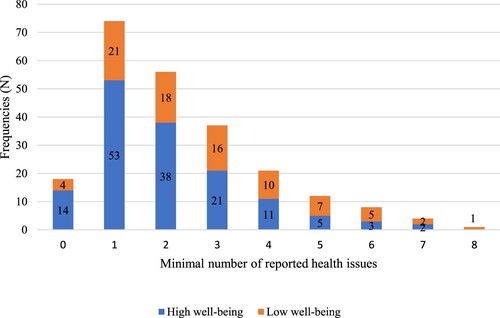
In this study we led unique analyses aiming at probing the contribution of emotional regulation strategies and social support on long-term cALL survivors’ well-being. Most participants in this sample reported high well-being (73%), despite presenting with health function issues. Interestingly, studies of well-being in the general population report averages of around 70 on the WHO-5 well-being index (Quebec National Institute of Public Health, Citation2023). In the present sample, the average is 61.78, suggesting a somewhat lower level of well-being than in the general population. Seventy-four (80.43%) survivors reported at least one health issue and 56 (60.87%) reported at least two health issues (). We found well-being to be essentially unrelated with clinical history and sociodemographic description. High well-being was associated with better health function, higher social support, and a more frequent use of emotional processing and cognitive reappraisal. We found emotional processing to contribute positively to well-being independently of health function. Finally, higher social support appeared to moderate the contribution of lower suppression to high well-being.
Figure 4. Number of health function issues reported by 92 cALL survivors on the 15D.
Note. cALL, childhood acute lymphoblastic leukemia. A cut-point on the WHO-5 well-being index of > 50 for high-well being was used (Topp et al., Citation2015).
The fact that well-being was associated with better health status was expected. Late adverse effects associated with cALL treatments may have deleterious effects on well-being because of their disabling effects on physical and psychosocial functioning regarding psychosocial development (Kızılocak & Okcu, Citation2019). In a study interviewing adolescents and young adults survivors of cALL, participants reported that late adverse effects had reduced their faculties, which in turn limited their participation in activities with their peers (Andrés-Jensen et al., Citation2020).
Similarly, we found high well-being to be associated with larger social support. This is also a well-identified phenomenon in a wide variety of clinical conditions (Gariépy et al., Citation2016). The stress-buffering hypothesis proposes that social support may serve as a protective factor against stress by modifying the appraisal or the individual’s response to the stressor (Cohen & Wills, Citation1985). Associations between social support and markers of resilience, such as benefit finding and well-being, have been found in several samples of pediatric cancer survivors (e.g. Orbuch et al., Citation2005; Teall et al., Citation2013).
When modeling the odds of higher well-being, we carefully adjusted for health status so that the results could highlight the target phenomenon of reporting well-being independent of possible health deterioration. In previous work, health status had not been controlled for, which has been a major limitation when interpreting the contributions of psychosocial factors on well-being. Here, we found a unique contribution of emotional processing to well-being. This emotion regulation strategy refers to acknowledging, exploring, and understanding one's stressor-related emotions and is conceptualized as an approach-oriented coping strategy. It was found to promote positive adjustment in cancer survivors (Stanton, Citation2010). For example, in a sample of young adults with cancer, a greater use of emotional processing was associated with higher levels of resilience. The authors suggest that emotional processing reflects survivors’ attempts to represent their cancer experience in a positive way, which may increase resilience (Darabos et al., Citation2021). This strategy is in sharp contrast with just expressing one’s emotions without processing, which may instead increase emotion dysregulation by intensifying rumination, worry or maladaptive thoughts (Hoyt et al., Citation2013). Here, emotional processing was associated with a kind of resilience as the relation was independent of health deterioration.
We expected that social support would moderate the contribution of emotion regulation strategies, specifically expression and suppression. Consistently, we found that the combination of high social support and low suppression increased dramatically the probabilities to report high well-being, and this was especially true in people with a large social network. In high suppression individuals we did not find any impact of social support. This result suggests that social support does not overly mitigate suppression as we anticipated. Instead, it may be particularly beneficial in participants who do not use suppression so much. It could be that social support be beneficial when emotional expression is not inhibited. This finding is in line with the theory of social sharing of emotions (SSE) (Rimé, Citation2009a). In our sample, it appears that when survivors expressed (did not suppress) their emotions to a large support network, i.e. when they performed SSE, probabilities for high well-being were clearly higher. This finding is compatible with previous research on SSE in the context of adult cancer, where perceptions of uncompassionate attitudes and avoidance within the close social network were associated with higher emotional distress (Boinon et al., Citation2014). Together with our findings, the results suggest that efficient SSE would promote resilience in cancer survivors, as associations were independent from health function.
If confirmed in future research, we should encourage expression or mitigate suppression before improving social support, as it appears there would be little benefit increasing social networks in people using predominantly suppression as social sharing cannot occur under these circumstances. This approach has the potential to influence well-being positively including in groups with deteriorated health. Although not a direct consequence of our results, interventions should also educate relatives to respond appropriately to emotional disclosure in a sensitive manner, especially in those who use predominantly suppression strategies, as this would encourage them to disclose their internal states.
Study limitations
We should recognize the limitations of this study. First, the study is cross-sectional, which did not allow us to identify causal associations. Although the direction of interpretations is sensible, it is possible that well-being influence emotional regulation strategies including emotional expression/suppression. Second, the sample selection criteria probably inflated the variability in health status function (selection of extreme phenotypes). This limits the generalization of results to other cALL or cancer survivors’ population. Finally, to avoid spurious associations when using standard health function indices, we chose to use a count variable independent of psychological functioning. For the sake of generalizability, we performed the same analyses using the standard index scores (15D-16D-17D). These analyses fully replicated the present results and are available in Supplementary Material (Tables S3-S6).
Clinical implications
If replicated, these results suggest that resilience could be promoted in survivors by supporting emotional processing. In high emotional suppressing survivors, a combined action on mitigating suppression and increasing social networks may also lead to improved resilience, independent of health deterioration.
Conclusions
In a cohort of 92 cALL survivors, high psychological well-being was associated with better health function, higher social support and more frequent cognitive reappraisal and emotional processing. Independent of health function, we found a beneficial output of using emotional processing on well-being. We also found that large social network was beneficial in those using less frequently emotional suppression strategies.
Acknowledgments
We would like to thank the survivors who took part to the study and the clinical research team.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by an Institutional Review Board/Ethics committee. See details under Methods.
Supplemental Material
Download Zip (49.5 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The full dataset is available in Supplementary material attached to this article.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Andrés-Jensen, L., Larsen, H. B., Johansen, C., Frandsen, T. L., Schmiegelow, K., & Wahlberg, A. (2020). Everyday life challenges among adolescent and young adult survivors of childhood acute lymphoblastic leukemia: An in-depth qualitative study. Psycho-oncology, 29(10), 1630–1637. https://doi.org/10.1002/pon.5480
- Anestin, A. S., Lippé, S., Robaey, P., Bertout, L., Drouin, S., Krajinovic, M., Michon, B., Rondeau, É, Samoilenko, M., Laverdière, C., Sinnett, D., & Sultan, S. (2018). Psychological risk in long-term survivors of childhood acute lymphoblastic leukemia and its association with functional health status: A PETALE cohort study. Pediatric Blood & Cancer, 65(11), e27356. https://doi.org/10.1002/pbc.27356
- Apajasalo, M., Rautonen, J., Holmberg, C., Sinkkonen, J., Aalberg, V., Pihko, H., Siimes, M. A., Kaitila, I., Mäkelä, A., Erkkilä, K., & Sintonen, H. (1996a). Quality of life in pre-adolescence: a 17-dimensional health-related measure (17D). Quality of Life Research, 5(6), 532–538. https://doi.org/10.1007/BF00439227
- Apajasalo, M., Sintonen, H., Holmberg, C., Sinkkonen, J., Aalberg, V., Pihko, H., Siimes, M. A., Kaitila, I., Mäkelä, A., Rantakari, K., Anttila, R., & Rautonen, J. (1996b). Quality of life in early adolescence: a sixteen-dimensional health-related measure (16D). Quality of Life Research, 5(2), 205–211. https://doi.org/10.1007/BF00434742
- Barakat, L. P., Madden, R. E., Vega, G., Askins, M., & Kazak, A. E. (2021). Longitudinal predictors of caregiver resilience outcomes at the end of childhood cancer treatment. n/a(n/a). https://doi.org/10.1002/pon.5625.
- Bitsko, M. J., Cohen, D., Dillon, R., Harvey, J., Krull, K., & Klosky, J. L. (2016). Psychosocial late effects in pediatric cancer survivors: A report from the children's oncology group. Pediatric Blood & Cancer, 63(2), 337–343. https://doi.org/10.1002/pbc.25773
- Boinon, D., Sultan, S., Charles, C., Stulz, A., Guillemeau, C., Delaloge, S., & Dauchy, S. (2014). Changes in psychological adjustment over the course of treatment for breast cancer: the predictive role of social sharing and social support. Psycho-Oncology, 23(3), 291–298. https://doi.org/10.1002/pon.3420
- Canadian Cancer Society. (2023). Watching for Late Effects. Canadian Cancer Society. https://cancer.ca/en/living-with-cancer/your-child-has-cancer/after-treatment/watching-for-late-effects
- Canadian Institute for Health Information. (2011). Seniors and the Health Care System: What Is the Impact of Multiple Chronic Conditions? https://secure.cihi.ca/free_products/air-chronic_disease_aib_en.pdf
- Chmitorz, A., Kunzler, A., Helmreich, I., Tüscher, O., Kalisch, R., Kubiak, T., Wessa, M., & Lieb, K. (2018). Intervention studies to foster resilience - A systematic review and proposal for a resilience framework in future intervention studies. Clinical Psychology Review, 59, 78–100. https://doi.org/10.1016/j.cpr.2017.11.002
- Cho, D., Park, C. L., & Blank, T. O. (2013). Emotional approach coping: gender differences on psychological adjustment in young to middle-aged cancer survivors. Psychology & Health, 28(8), 874–894. https://doi.org/10.1080/08870446.2012.762979
- Chukwuemeka, N. A., & Obioha, C. W. (2024). Emotion regulation strategies on psychological distress and psychological well-being of caregivers of mentally challenged children: moderating role of social support. Psychology, Health & Medicine, 79–91. https://doi.org/10.1080/13548506.2023.2289473
- Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. https://doi.org/10.1037/0033-2909.98.2.310
- Conley, C. C., Bishop, B. T., & Andersen, B. L. (2016). Emotions and emotion regulation in breast cancer survivorship. Healthcare, 4, 56. https://doi.org/10.3390/healthcare4030056
- Coo, S., García, M. I., Prieto, F., & Medina, F. (2022). The role of interpersonal emotional regulation on maternal mental health. Journal of Reproductive and Infant Psychology, 40(1), 3–21. https://doi.org/10.1080/02646838.2020.1825657
- D'Agostino, N. M., Penney, A., & Zebrack, B. (2011). Providing developmentally appropriate psychosocial care to adolescent and young adult cancer survivors. Cancer, 117(10), 2329–2334. https://doi.org/10.1002/cncr.26043
- Darabos, K., Renna, M. E., Wang, A. W., Zimmermann, C. F., & Hoyt, M. A. (2021). Emotional approach coping among young adults with cancer: Relationships with psychological distress, posttraumatic growth, and resilience. Psycho-oncology, 30(5), 728–735. https://doi.org/10.1002/pon.5621
- Demirtas, O., Özdevecioğlu, M., & Capar, N. (2015). The relationship between cognitive emotion regulation and Job stress: Moderating role of social support. Asian Social Science, 11(12), 168–173. https://doi.org/10.5539/ass.v11n12p168
- Eicher, M., Matzka, M., Dubey, C., & White, K. (2015). Resilience in adult cancer care: An integrative literature review. Oncology Nursing Forum, 42(1), E3–E16. https://doi.org/10.1188/15.ONF.E3-E16
- Eiser, C. (2007). Beyond survival: Quality of life and follow-up after childhood cancer. Journal of Pediatric Psychology, 32(9), 1140–1150. https://doi.org/10.1093/jpepsy/jsm052
- Fletcher, D., & Sarkar, M. (2013). Psychological resilience. European Psychologist, 18(1), 12–23. https://doi.org/10.1027/1016-9040/a000124
- Gariépy, G., Honkaniemi, H., & Quesnel-Vallée, A. (2016). Social support and protection from depression: systematic review of current findings in Western countries. British Journal of Psychiatry, 209(4), 284–293. https://doi.org/10.1192/bjp.bp.115.169094
- Gross, J. J., & John, O. P. (2003). Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348
- Hayes, A. F. (2020). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Press.
- Helmreich, I., Kunzler, A., Chmitorz, A., König, J., Binder, H., Wessa, M., & Lieb, K. (2017). Psychological interventions for resilience enhancement in adults. Cochrane Database of Systematic Reviews, 2017(2), CD012527. https://doi.org/10.1002/14651858.CD012527
- Hoyt, M. A., Stanton, A. L., Bower, J. E., Thomas, K. S., Litwin, M. S., Breen, E. C., & Irwin, M. R. (2013). Inflammatory biomarkers and emotional approach coping in men with prostate cancer. Brain, Behavior, and Immunity, 32, 173–179. https://doi.org/10.1016/j.bbi.2013.04.008
- Hudson, M. M., Ness, K. K., Gurney, J. G., Mulrooney, D. A., Chemaitilly, W., Krull, K. R., Green, D. M., Armstrong, G. T., Nottage, K. A., Jones, K. E., Sklar, C. A., Srivastava, D. K., & Robison, L. L. (2013). Clinical ascertainment of health outcomes among adults treated for childhood cancer. Jama, 309(22), 2371–2381. https://doi.org/10.1001/jama.2013.6296
- Jacola, L. M., Edelstein, K., Liu, W., Pui, C.-H., Hayashi, R., Kadan-Lottick, N. S., Srivastava, D., Henderson, T., Leisenring, W., Robison, L. L., Armstrong, G. T., & Krull, K. R. (2016). Cognitive, behaviour, and academic functioning in adolescent and young adult survivors of childhood acute lymphoblastic leukaemia: a report from the Childhood Cancer Survivor Study. The Lancet Psychiatry, 3(10), 965–972. https://doi.org/10.1016/S2215-0366(16)30283-8
- Karimzadeh, Y., Rahimi, M., Goodarzi, M. A., Tahmasebi, S., & Talei, A. (2021). Posttraumatic growth in women with breast cancer: emotional regulation mediates satisfaction with basic needs and maladaptive schemas. European Journal of Psychotraumatology, 12(1), 1943871. https://doi.org/10.1080/20008198.2021.1943871
- Kızılocak, H., & Okcu, F. (2019). Late effects of therapy in childhood acute lymphoblastic leukemia survivors. Turkish Journal of Hematology, 36(1), 1–11. https://doi.org/10.4274/tjh.galenos.2018.2018.0150
- Luminet, O. (2008). Psychologie des émotions: confrontation et évitement (2 ed.). De Boeck Supérieur.
- Marcoux, S., Drouin, S., Laverdière, C., Alos, N., Andelfinger, G. U., Bertout, L., … Levy, E. (2017). The PETALE study: Late adverse effects and biomarkers in childhood acute lymphoblastic leukemia survivors. Pediatric Blood & Cancer, 64(6), 6–20. https://doi.org/10.1002/pbc.26361
- Ngamaba, K. H., Panagioti, M., & Armitage, C. J. (2017). How strongly related are health status and subjective well-being? Systematic review and meta-analysis. European Journal of Public Health, 27(5), 879–885. https://doi.org/10.1093/eurpub/ckx081
- Oancea, S. C., Brinkman, T. M., Ness, K. K., Krull, K. R., Smith, W. A., Srivastava, D. K., Robison, L. L., Hudson, M. M., & Gurney, J. G. (2014). Emotional distress among adult survivors of childhood cancer. Journal of Cancer Survivorship, 8(2), 293–303. https://doi.org/10.1007/s11764-013-0336-0
- Orbuch, T. L., Parry, C., Chesler, M., Fritz, J., & Repetto, P. (2005). Parent-child relationships and quality of life: Resilience among childhood cancer survivors*. Family Relations, 54(2), 171–183. https://doi.org/10.1111/j.0197-6664.2005.00014.x
- Peh, C. X., Liu, J., Bishop, G. D., Chan, H. Y., Chua, S. M., Kua, E. H., & Mahendran, R. (2017). Emotion regulation and emotional distress: the mediating role of hope on reappraisal and anxiety/depression in newly diagnosed cancer patients. Psycho-Oncology, 26(8), 1191–1197. https://doi.org/10.1002/pon.4297
- Płotka, A., Chęcińska, A., Zając-Spychała, O., Więckowska, B., Kramer, L., Szymańska, P., Adamczewska-Wawrzynowicz, K., Barełkowska, M., Wachowiak, J., & Derwich, K. (2021). Psychosocial late effects in adolescent and young adult survivors of childhood cancer diagnosed with leukemia, lymphoma, and central nervous system tumor. Journal of Adolescent and Young Adult Oncology, 10(4), 443–453. https://doi.org/10.1089/jayao.2020.0086
- Quebec national institute of public health. (2023). Information sheet 14 - World Health Organization Well-Being Index (WHO-5). Quebec National Institute of Public Health. https://www.inspq.qc.ca/en/post-disaster-mental-health-impacts-surveillance-toolkit/standardized-measurement-instruments/information-sheets-standardized-measurement-instruments-recommended/well-being
- Rimé, B. (2009a). Le partage social des émotions (2nd ed.). Presses Universitaires de France. https://www.cairn.info/le-partage-social-des-emotions–9782130578543-page-67.htm
- Rimé, B. (2009b). Emotion elicits the social sharing of emotion: Theory and empirical review. Emotion Review, 1(1), 60–85. https://doi.org/10.1177/1754073908097189
- Rimé, B. (2017). The social sharing of emotion in interpersonal and in collective situations. In J. A. Holyst (Ed.), Cyberemotions: Collective emotions in cyberspace (pp. 53–69). Springer International Publishing. https://doi.org/10.1007/978-3-319-43639-5_4.
- Rondeau, É, Desjardins, L., Laverdière, C., Sinnett, D., Haddad, É, & Sultan, S. (2021). French-language adaptation of the 16D and 17D Quality of Life measures and score description in two Canadian pediatric samples. Health Psychology and Behavioral Medicine, 9(1), 619–635. https://doi.org/10.1080/21642850.2021.1948416
- Sarason, I. G., Sarason, B. R., Shearin, E. N., & Pierce, G. R. (1987). A brief measure of social support: Practical and theoretical implications. Journal of Social and Personal Relationships, 4(4), 497–510. https://doi.org/10.1177/0265407587044007
- Sintonen, H. (2001). The 15D instrument of health-related quality of life: properties and applications. Annals of Medicine, 33(5), 328–336. https://doi.org/10.3109/07853890109002086
- Stanton, A. L. (2010). Regulating Emotions during Stressful Experiences: The Adaptive utility of coping through emotional approach. In S. Folkman (Ed.), The Oxford handbook of stress, health, and coping (pp. 369–386). Oxford University Press.
- Stanton, A. L., Kirk, S. B., Cameron, C. L., & Danoff-Burg, S. (2000). Coping through emotional approach: Scale construction and validation. Journal of Personality and Social Psychology, 78(6), 1150–1169. https://doi.org/10.1037/0022-3514.78.6.1150
- Teall, T., Barrera, M., Barr, R., Silva, M., & Greenberg, M. (2013). Psychological resilience in adolescent and young adult survivors of lower extremity bone tumors. Pediatric Blood & Cancer, 60(7), 1223–1230. https://doi.org/10.1002/pbc.24441
- Topp, C. W., Østergaard, S. D., Søndergaard, S., & Bech, P. (2015). The WHO-5 Well-Being Index: a systematic review of the literature. Psychotherapy and Psychosomatics, 84(3), 167–176. https://doi.org/10.1159/000376585
- Wilson, C. L., & Ness, K. K. (2013). Bone mineral density deficits and fractures in survivors of childhood cancer. Current Osteoporosis Reports, 11(4), 329–337. https://doi.org/10.1007/s11914-013-0165-0
- World Health Organization Regional Office for Europe. (1998). Use of Well-Being Measures in Primary Health Care: The DepCare Project. https://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf
- Yallop, K., McDowell, H., Koziol-McLain, J., & Reed, P. W. (2013). Self-reported psychosocial wellbeing of adolescent childhood cancer survivors. European Journal of Oncology Nursing, 17(6), 711–719. https://doi.org/10.1016/j.ejon.2013.06.007
- Yi, J., Zebrack, B., Kim, M. A., & Cousino, M. (2015). Posttraumatic growth outcomes and their correlates Among young adult survivors of childhood cancer. Journal of Pediatric Psychology, 40(9), 981–991. https://doi.org/10.1093/jpepsy/jsv075
- Zaki, J., & Williams, W. C. (2013). Interpersonal emotion regulation. Emotion, 13(5), 803–810. https://doi.org/10.1037/a0033839
- Zebrack, B. J., & Chesler, M. A. (2002). Quality of life in childhood cancer survivors. Psycho-oncology, 11(2), 132–141. https://doi.org/10.1002/pon.569
- Zebrack, B. J., Stuber, M. L., Meeske, K. A., Phipps, S., Krull, K. R., Liu, Q., Yasui, Y., Parry, C., Hamilton, R., Robison, L. L., & Zeltzer, L. K. (2012). Perceived positive impact of cancer among long-term survivors of childhood cancer: a report from the childhood cancer survivor study. Psycho-oncology, 21(6), 630–639. https://doi.org/10.1002/pon.1959
