

ABSTRACT
Purpose
This study examined hope, meaning in life (MIL), and religious/spiritual struggle (RSS) as predictors of the quality of life (QOL) in cancer patients. We hypothesized a positive association of QOL with hope and MIL, whereas a negative association with RSS. The stage of cancer was hypothesized as a moderator variable between QOL and hope. Hope and MIL were assumed as positive predictors and RSS as negative predictor of QOL.
Methods
Data stem from the cross-sectional survey study of 300 cancer patients (Mean age = 50.97 ± 13.50 SD). Herth Hope Index, Meaning in Life Scale, Religious Spiritual Struggle Scale and WHO-QOL-BRIEF were used. The correlation coefficient and partial least square structural equation modeling approach (PLS-SEM) were used for assessing the measurement model and the structural model.
Results
As hypothesized, QOL was found positively associated with Hope and MIL, but negatively associated with RSS. The stage of cancer was hypothesized as a negative moderator. The three predictors significantly predicted QOL in cancer patients and explained 75.3% of the variance in QOL, and the overall model fit was adequate (SRMR = 0.075). Hope and MIL had a positive impact on QOL (β = .356, p < 0.01; β = .355 p < 0.01, respectively), whereas RSS had a negative impact (β = –.102, p < .05). The Stage of cancer did not moderate the path coefficient between the hope and QOL to a significant degree (β = .097, p > 0.01).
Conclusion
In cancer patients, hope and MIL are facilitators of QOL. Addressing religious and spiritual concerns and struggles is critical to overall QOL improvement.
Introduction
To improve the quality of life of cancer patients, psychology has been an essential component of oncological care since 1970 (Lang-Rollin & Berberich, Citation2018). QOL is an individual’s perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards, and concerns (World Health Organization (WHO), Citation1993). Patients who are hopeful about their treatment outcomes outperform those who are pessimists (Blank & Bellizzi, Citation2006). Furthermore, meaning in life is a metaphysical question that is inextricably linked to the fundamental existentialism of being. Finding meaning in life while battling a disease like cancer has been shown to enhance cancer patients’ quality of life by modifying their illness perception and global meaning (Majernikova & Obrocnikova, Citation2017; Whiteford & Olver, Citation2012). These studies found a positive impact of MIL on QOL. Additionally, religion and/or spirituality are possibly important to investigate among cancer patients. A religious metaphor is faith in God, and a spiritual metaphor is connecting to the larger world. However, the religious struggle (Ano & Pargament, Citation2012) involves emotions of abundance and a punishment from God, questioning his decisions negatively and blaming Him for illness and the effect of superstitious powers such as demons and evil forces. Spiritual struggle, on the other hand, is the inability to connect with the larger world, connect with people, and doubt deeds and values to life during cancer survivorship. Religious/spiritual struggle is linked to a sense of symptom burden and a low quality of life (Damen et al., Citation2021). The stage of cancer has been found to have a differential impact on the hope of cancer patients. Some studies have found that the cancer stage does not impact the level of hope, while another study reported that during the advanced stage, the hope decreases (Chen, Citation2003; Duggleby et al., Citation2013; Baczewska et al., Citation2020).
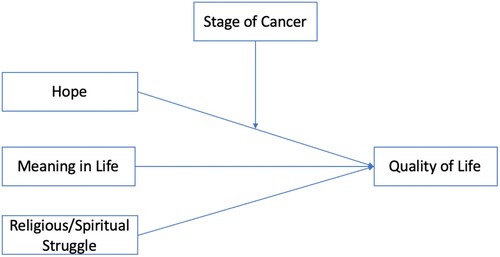
India’s progress in providing palliative care for cancer patients is still in its early stages. In this situation, discovering hope and finding meaning in life can play a crucial role in safeguarding the patient’s QOL. Furthermore, as a country with a multitude of religions, India’s population encompasses a wide range of religious/spiritual beliefs, and dealing with such an illness can pose challenges to their religious and spiritual convictions. The epidemiological investigation revealed that the occurrence of cancer is elevated in the Indo-Gangetic basin (Madhawi et al., Citation2018). This increased incident can be attributed to the presence of high levels of arsenic (oxygen, chlorine, & sulfur) in water and the disposal of heavy metals in the surrounding soil. The sociodemographic study has investigated the impact of limited education and working status on the diminished quality of life experienced by patients in India (Ramasubbu et al., Citation2021). The stage of cancer has been examined as a sociodemographic factor in previous studies (Chen, Citation2003; Duggleby et al., Citation2013; Baczewska et al., Citation2020). But the role of the stage is still unclear. Given the importance of these variables, the current study intends to investigate Hope, MIL, RSS as predictors of QOL among the cancer patients living at Indo-Gangetic region ().
Figure 1. Theoretical framework of the constructs.
Hope
Hope is a multidimensional concept that includes temporality and future, positive readiness and expectancy, and interconnectedness (Herth, Citation1989). Temporality and future refer to an individual’s perception of goals, positive outlook on life, belief in the potentiality of each day, and apprehension about the future. Positive readiness and expectancy represent emotional readiness during challenging times, the purpose of life, valuing life, and recollection of positive memories. Lastly, interconnectedness relates to an individual’s sense of connection with self and broader context. Cancer diagnosis may have a negative impact on patients’ hope for future life expectancy. As the disease progresses, patients begin to fight the impending doom of death and sufferings (Caldeira et al., Citation2016). Interestingly, a few studies (Vartak, Citation2015) are available that examine the role of hope in QOL among Indian cancer patients, with the majority of them focusing on hopelessness and QOL (Ravindran, Citation2019), depression and QOL (Bhattacharyya et al., Citation2017; Shankar et al., Citation2021; Sharma & Purkayastha, Citation2017; Tiwari, Citation2019; Srivastava et al., Citation2016). Hope and cancer are linked in two ways: highly hopeful people actively engage in cancer screening behavior. Those who are suffering demonstrate increased adjustment and decreased distress throughout treatment (Taylor, Citation2000). Patients with high hope are more likely to continue their treatment (Herth, Citation1989). Newtony (Citation1991) writes that ‘hope has been identified as an important component in the quality of life’ (Newtony, Citation1991, p. 57) for women with breast cancer. It serves as a protective factor in improving and maintaining one's QOL (Li et al., Citation2016). Research indicates that hope is a key predictor of quality of life and is positively correlated with it (Cui et al., Citation2014; Soylu et al., Citation2016; Sharour, Citation2010).
Stage of cancer and level of hope
The progression of cancer at different stages may impact the level of hope. However, the research supports mixed findings. Chen (Citation2003) examined the effect of disease metastasis on patients’ level of hope and found that the cancer stage did not significantly affect their hope after the successful treatment (Chen, Citation2003). Similarly, Duggleby et al. (Citation2013) found that stage does not impact cancer patients’ hope (Duggleby et al., Citation2013). Contrarily, some researchers have found an increase in hope at the end of treatment but not a significant increase (Wakiuchi et al., Citation2015). Recently, Baczewska et al. (Citation2020) found that hope was low in those patients who were in the terminal phase of cancer (Baczewska et al., Citation2020). Several studies (Ballard et al., Citation1997; Rustøen & Wiklund, Citation2000; Benzein & Berg, Citation2005) had already examined the role of age in the hope of cancer patients, and therefore, age was not a variable of interest in this study (Ballard et al., Citation1997; Rustøen & Wiklund, Citation2000; Benzein & Berg, Citation2005).
Meaning in life
Meaning in life is a multi-faceted construct that includes perceived harmony and peace, life perspective, purpose and goals, confusion and lessened meaning, and benefits of spirituality (Jim et al., Citation2006). Harmony and peace reflect positive emotions and thoughts such as tranquility, serenity, and comfort. Life perspective, purpose, and goals refer to assigning meaning to oneself regarding the goals. Confusion and lessened meaning show a lack of motivation for confusion about life. The benefits of spirituality reflect seeking meaning through spiritual faith and beliefs. Finding meaning when battling a sickness like cancer has been found to improve patients’ quality of life (QOL) by altering how they perceive their condition and global meaning, although those findings are only applicable to non-Asian contexts (Majernikova & Obrocnikova, Citation2017; Whiteford & Olver, Citation2012). There are numerous meaning sources. Goals is one such source (Baumeister, Citation1991; Emmons, Citation2005; Wong, Citation1998; Klinger, Citation1998). Emmons (Citation2005) states that ‘the development of goals that allow for a greater sense of purpose in life is one of the cornerstones of well-being" (Emmons, Citation2005, p. 734). Some researchers have discovered a positive, statistically significant relationship between meaning in life and QOL in cancer patients (Majernikova & Obrocnikova, Citation2017; Whiteford & Olver, Citation2012; Dobrikova et al., Citation2015).
Religious/spiritual struggle
Religious/spiritual struggle (RSS) is a common experience among cancer patients (Zumstein-Shaha et al., Citation2020). It includes divine conflict, intrapsychic/intrapersonal, and interpersonal conflict (Pargament, Citation2007). The experience of a troubled relationship with God as distant and unresponsive to needs is referred to as divine or supernatural struggle. Interpersonal conflicts are those that occur between individuals in the community over religious or spiritual issues (Pargament et al., Citation1998). During the course of a fatal disease, interaction at a religious place, community, or congregation can become a source of tension and conflict (Becker et al., Citation1993). Facing a fatal disease can evoke fear and guilt. Interactions at religious places may exacerbate these emotions if individuals feel judged or inadequate due to their illness. Intrapersonal struggle is an individuals’ struggle within oneself regarding the meaning, existence, or doubt of existence or moral dilemma (Abu-Raiya et al., Citation2015). Interpersonal conflict also means why good people sometimes suffer unpleasant outcomes (Ellison & Lee, Citation2010, p. 505). Spirituality is defined in the context of palliative care patients, such as cancer patients, as a way of connecting to oneself, others, nature, and the sacred; it is the way individuals express meaning and purpose (Puchalski et al., Citation2009); religion symbolizes belief and practices (Emblen, Citation1992). Despite the fact that India is a multi-religious country, little attention has been paid to RSS. Simha et al. (Citation2013), for example, conducted a qualitative study of the spiritual concerns of Indian cancer patients receiving palliative care and discovered patients who were questioning their karma and previous birth sins. This is referred to as an intrapsychic or intrapersonal struggle (Simha et al., Citation2013). Winkelman et al. (Citation2011) investigated the relationship between spiritual concern and QOL in patients receiving palliative radiotherapy (Winkelman et al., Citation2011). The results showed a significant inverse relationship between psychological QOL and spiritual struggle, spiritual seeking, and total spiritual concern. Doubting God (spiritual struggle) was discovered to be the strongest predictor of the poorest psychological QOL. Overall, neither total spiritual struggle nor spiritual seeking emerged as significant predictors of QOL.
The objective of this study was to examine the association of hope, MIL, and RSS with the QOL of cancer patients with early and advanced malignancy. Furthermore, these variables were investigated as QOL’s predictors. Additionally, the stage of cancer was studied as a moderator variable between the association of hope and QOL (). Thus, the following hypotheses were made: (1) H1: hope and MIL would have a positive association with QOL while RSS would have a negative correlation, (2) H2: RSS was hypothesized to be a negative predictor of QOL, while hope and MIL were hypothesized to be positive predictors and, (3) H3: Stage of cancer was hypothesized as a negative moderator between hope and QOL.
Material and methods
Design
This study followed a cross-sectional survey research design with stratified random sampling of cancer patients of varying stages (0,1, 2, 3, 4) from the Out-Patient Department of radiation oncology and surgical oncology of State Cancer Institute on 06/08/2019. The center was chosen based on reports of patients in various stages of cancer. The first author has extensive experience of data collection in psycho-oncological researches. The inclusion criteria were: (1) a cancer diagnosis at least three months ago; (2) having received or being subjected to chemotherapy, radiation therapy, surgery, or any combination of these treatments; and (3) patients agreeing to participate in the study. Exclusion criteria were: (1) patients experiencing nausea/pain as a side effect of radiation/chemotherapy/surgery on the day of data collection; (2) being unable to vocalize the answer due to surgery or any other reason; and (3) family pressure or reluctance to allow patients to participate in the study. (4) Patients with benign tumors, as previous research has shown that tumor nature influences QOL (Hörnquist et al., Citation1992).
Sample and determination of sample size
The study included 300 cancer patients (). Soper's a-priori sample size calculator for SEM was used to calculate sample size, which takes into account the expected effect size, desired statistical power, number of predictors, number of criterion variables, and the probability level used in the study (Soper, Citation2021). In this study, the expected effect size was 0.15, the desired power of the test was 0.80, the number of predictor variables was three, and the criterion variable was one. The p-value that was chosen was 0.01. The sample size calculation determined that the model structure required a minimum sample size of 200. As a result, this study's sample size is adequate for the structural equation model.
Table 1. Demographic characteristics of the participants (N = 300).
Procedure
The ethics committee of the State Cancer Institute approved this study (Acad.Cell 1468 Dated 30/05/2019). After the approval, potential patients meeting the inclusion criteria were identified from the upcoming appointment registry available in the Out-Patient Department record book of the Radiation Oncology and Surgical Oncology department. The researcher met with the patients at a psycho-oncology clinic, briefed them on the purpose of the study, and obtained their consent. We divided the cancer strata into early and advanced stages. We pre-determined that each stratum would contain 50% of the total sample. After that, we randomly chose participants for each stratum until the required number of patients were recruited. We did this to rule out the effect of sample heterogeneity. First, demographic information such as the patient's age, sex, cancer stage, date of diagnosis, type of cancer, and location were collected. Following that, they were given instructions regarding self-report inventories. All the inventories were administered in English language.
Measures
Hope was measured using the Herth Hope Index (HHI), which is a 4-point rating scale, from strongly disagree to strongly agree, has 12 items (Herth, Citation1992). This scale comprises three subscales: inner sense of temporality and the future (e.g. I believe that each day has potential), inner positive readiness (e.g. I have a sense of direction), and interconnectedness with self and others (e.g. I am able to give and receive love). For the current study, the scale's overall internal consistency (Cronbach’s Alpha α) was strong ( = 0.93), as were its subscales measuring inner sense of temporality and future ( = 0.86), inner positive readiness ( = 0.89), and interconnectedness with self and others ( = 0.79).
The Meaning in Life Scale (MiLS) is a 21-item questionnaire designed specifically for use with cancer patients (Jim et al., Citation2006). Patients rated each statement from 1 to 6 on a 6-point scale (strongly disagree to strongly agree). This scale is comprised of four components: life perspective, purpose and goal, confusion and lessened meaning, harmony and peace, benefits of spirituality. For this study, the internal consistency (α) of these factors was 0.81, 0.82, 0.86, 0.89, respectively, and on the full scale was 0.96.
The Religious Spiritual Struggle Scale (RSS) was used to assess the RSS of the patients (Pargament, Citation2007). This scale has 26 items with a 6-point rating scale ranging from 1 to 6 (strongly disagree to strongly agree). The scale is comprised of three components: divine struggle, intrapsychic struggle, and interpersonal struggle. For the current study, the internal consistency (α) of these factors was 0.88, 0.92 and 0.908, and the overall scale was 0.96.
The WHOQOL-BRIEF (WHO, Citation1993) was used to assess the quality of life of cancer patients (Organization. Division of Mental Health, W. H. O., Citation1996, January 1). It consists of 26 items on a 5-point rating scale ranging from very poor/very dissatisfied/not at all/never to very good/an extreme amount/extremely/ completely/always. This scale consists of four domains of quality of life, namely physical health, psychological health, social relationships, and environment, and two items measure quality of life and general health. The internal consistency of this scale for the current study was 0.91 (α), showing excellent reliability to assess the QOL of cancer patients (George & Mallery, Citation2003).
Statistical analysis
The data were analyzed using SPSS version 25 and Smart PLS 3.3. Demographic characteristics and score on measures were summarized using descriptive statistics (Mean, Standard Deviation, Percentage, Skewness and Kurtosis). Pearson Product moment coefficient of correlation was used to test the association of predictors (Hope, MIL, RSS) and their dimensions with the QOL. In the measurement model, scale items were indicators, and scale dimensions were first-order constructs. In the structural model Hope, MIL, and RSS were second-order constructs/endogenous variables and QOL is exogenous variable/criterion variable. The measurement model was evaluated for reliability and validity of the constructs. Cronbach’s Alpha (α) and Composite reliability (Pc) were used to test the internal consistency. Factor loading of items was confirmed. Convergent validity and discriminant validity were assessed through Average Variance Extracted (AVE) (Fornell & Larcker, Citation1981) and Latent Variable Correlation (LVC), respectively. In the structural model, the collinearity of the predictors was assessed using the variance inflation factor (VIF). Path coefficient (β) was used to test the hypothesized association, and Coefficient of determination (R2) was used to explain the variance in the QOL by the predictor variables. The overall model fit was tested with a Standardized Root-Mean-Square Residual (SRMR). The predictive relevance of the overall model was tested with Stone-Geisser’s predictive relevance (Q2) statistic [111]. Lastly, the magnitude of the effect of the predictors was tested with effect size statistics (f2) (Cohen, Citation1988).
Results
Exploratory data analysis showed no missing values in the data set. Kurtosis and skewness are the measure of shape of the distribution of scores in a data set and both are related with its standard error (Cohen, Citation1988, p. 140). The value of skewness for hope, MIL, RSS and, QOL were –0.032, 0.135, 0.047, –1.228, respectively and of kurtosis –1.604, –1.020, –1.284, and 2.361, respectively (see the Supplementary Table). Converting the values of Skewness and Kurtosis into z score requires division of absolute values by their standard errors. In the present data set the obtained value of skewness (z score) for hope, MIL, RSS, and QOL were .226, 8.709, 0.957, 0.333, respectively. Furthermore, the value of kurtosis was 5.70, 8.402, 3.62, and 4.56 for hope, MIL, RSS, and QOL, respectively. The obtained value between ±1.96 SD is considered within the range (Field, Citation2009, p. 140). In addition to this, the normality of data were also checked by the Kolmogorov–Smirnov (Hope= 0.194, p < 0.01, MIL = 0.135, p < 0.01, RSS= .099, p < 0.01, QOL= .117, p < 0.01) and Shapiro–Wilk tests (Hope= .886, p < 0.01, MIL= 0.941, p < 0.01, RSS= 0.925 p < 0.01 QOL= 0.957, p < 0.01). Since the sample is large, the former statistic was used to interpret the normality. Likewise, the distribution of scores on all the subscales was also tested. All the indices (Skewness, Kurtosis, and Kolmogorov–Smirnov test) denote that the data lack symmetry. Conclusively the use of partial least square structure equation modeling (PLS-SEM) was appropriate as it does not assume data symmetry.
The Pearson Product moment coefficient of correlation showed a significant positive correlation of QOL with hope and MIL. A significant negative correlation was found between RSS and QOL ().
Table 2. Correlation of Hope, MIL, RSS and their dimensions with the QOL.
Step 1: evaluation of measurement model
Internal consistency reliability
Traditionally only Cronbach’s alpha was used for this purpose, but since PLS-SEM is sensitive to the number of items in a scale and it underestimates the reliability when path model is used (Werts et al., Citation1974), the use of composite reliability (Pc) is suggested. In the present research, the composite reliability (Pc) of the first order constructs were as follows: inner sense of temporality and future (0.909), inner positive readiness and expectancy (0.901), inner connectedness with self and others (0.867), life perspective, purpose and goal (0.871), confusion and lessened meaning (0.893), harmony and peace (0.881), benefits of spirituality (0.935), divine struggle (0.913), intrapsychic struggle (0.90), and interpersonal struggle (0.927) (). Further the composite reliability of the criterion (exogenous) variable, QOL is 0.931. The value of .60 and higher shows satisfactory composite reliability; but it should not exceed the 0.95 level (Hair et al., Citation2013).
Table 3. Measurement model.
Construct validity
Construct validity can be measured by both convergent validity and discriminant validity. For convergent validity, the value of AVE 0.50 and above is reported as acceptable (Hair et al., Citation2010). All of the reflective first-order constructs’ AVEs were within an acceptable range (). For discriminant validity, the square root of AVE for each first order construct should be higher than its correlation with the other first-order constructs which is known as Latent Variable Correlation (LVC). The square root of each first order construct was higher than the corresponding LVC ().
Table 4. Discriminant Validity of the first order constructs.
Step 2: evaluation of the structural model
Collinearity assessment
The VIF value of the predictors shall not exceed to 5 (Hair et al., Citation2011). In this study, the VIF did not exceed from the acceptable range (). Thus, no collinearity issue in the second order constructs/predictors was found.
Table 5. Collinearity Assessment of the Second order constructs (predictors).
Coefficient of determination
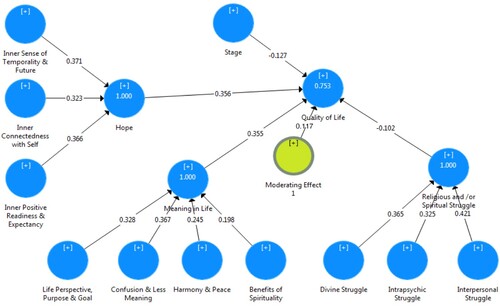
The second step of structural model evaluation is the assessment of coefficient of determination (R2). The PLS Path Model () showed that the overall R2 is 0.753, that denotes a strong coefficient of determination (Hair et al., Citation2011). It suggests that hope, MIL, and RSS can jointly explain 75.3% of the variance in the QOL.
Figure 2. Path Model and Coefficient of Determination.
Path coefficient
It shows the relationship between endogenous and exogenous constructs of the structural model. The significance level of the path model for the present research was obtained by using the bootstrapping procedure with a minimum sample of 5000 (Hair et al., Citation2017) (). The PLS model estimation ( and ) shows that the path coefficient of the three second-order constructs (predictors) hope, MIL, and RSS to quality of life are significant. However, the path coefficient of the moderator variable, that is, the stage of cancer in between hope and quality of life, is not significant.
Figure 3. t-statistics for the model.
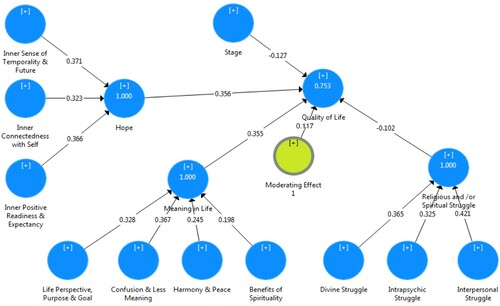
Table 6. Significance testing of the structural model’s path coefficient.
The values of beta (β) for hope and meaning in life were 0.356 (t = 5.064, p < 0.01) and 0.355 (t = 4.944, p < 0.01), respectively. These values indicate their positive impact on cancer patients’ quality of life (QOL). Furthermore, it suggests that hope and MIL have almost equal impacts on the quality of life. But, the value of beta (β) for RSS was –.102 (t = 1.905, p < .05) showed a negative impact on QOL of cancer patients.
Model fit
Standardized Root-Mean-Square Residual (SRMR) is the measure of model fit and the value below 0.08 is considered adequate for the PLS path model (Hu & Bentler, Citation1999). The SRMR value (0.075) showed the adequate overall fit of the present path model ().
Predictive relevance (Q2)
Predictive relevance of the model shows that the results do not only apply to the data which has been obtained in the current research for estimation process, rather the relevance of results outside the current data set i.e. out of sample (Hair et al., Citation2021). The value of Q2 is > 0, it demonstrates good predictive relevance of the model (Chin, Citation1998). Thus, the predictive relevance of the present structural model is good (Hope Q2 = 0.59, MIL Q2 = 0.446, RSS Q2 = 0.530) (). From the effect size (f2) statistics it can be concluded that the predictors namely, hope (f2 = 0.141), meaning in life (f2 = 0.108) and religious and/or spiritual struggle (f2 = 0.025) have medium to large effect size (Fornell & Larcker, Citation1981) (, ).
Figure 4. Predictive relevance of the model.
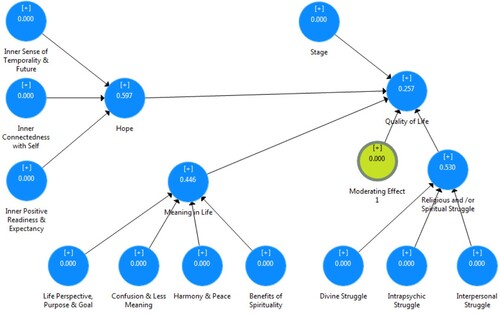
Table 7. Predictive relevance and effect size of the structural model.
Discussion
Our study revealed a significant positive correlation among various dimensions of hope, the total hope score, and the overall quality of life (QOL) for cancer patients. Furthermore, the stage of cancer did not emerge as a significant moderator between the two. The measurement of hope in our study encompassed three specific aspects: cognitive-temporal (inner sense of temporality and future), affective-behavioural (inner positive readiness and expectancy), and interconnectedness with self and others. The results could indicate that cancer patients engage in visualizing their goals, planning, and executing actions as they navigate through their illness journey. Identifying achievable pathways towards significant goals becomes crucial for individuals facing diseases like cancer (Chin, Citation1998). This process could facilitate the acceptance of illness and foster positive behavior towards treatment, imparting a sense of purpose in their lives and the ability to connect with others, which overall positively impacts their quality of life (Berendes et al., Citation2010). These trends align with the findings from studies conducted in China, which also highlighted hope as a significant positive psychological factor contributing to the preservation of cancer patients’ quality of life. The presence of hope among these patients fosters positive thoughts related to their cancer experience, leading to more favorable outcomes (Zhang et al., Citation2020).
Cancer patients who can discover situational meaning amidst their struggles with illness and successfully integrate this meaning with the broader purpose and significance of their lives tend to cope more effectively (Bernard et al., Citation2017). In our study, we identified a positive association and impact of MIL on the QOL of cancer patients. How these patients perceive their current life situation enables them to derive harmony and peace, which contributes to their overall well-being. Additionally, they could find benefit in spirituality, as it serves as one of the sources of meaning-making during times of suffering. The integration of these aspects could collectively enhance their QOL. Studies conducted with Slovak cancer patients have reported comparable positive effects of MIL (Majernikova & Obrocnikova, Citation2017). These findings underscore the importance of discovering purpose and significance in life as a valuable element in improving the overall QOL of individuals dealing with cancer.
A significant negative correlation was observed between RSS and QOL of the patients. RSS was found to have an adverse impact on their QOL Cancer patients’ interpersonal struggle may reveal feelings of abandonment by others, with some perceiving individuals with religious faith or spiritual beliefs advocating rituals for seeking forgiveness and appeasing God as spiritual hypocrites. The perception arises from the observation that these individuals do not consistently embody the principles they advocate, leading to interpersonal conflicts. Interestingly, patients’ divine struggle could demonstrate a sense of abundance or punishment by God with disease perceived as a consequence of evil forces, as reported in the questionnaire and endorsed by participants. A related study by Simha et al. (Citation2013) showed interpersonal struggle among Hindu cancer patients, such as questioning the Karma of previous birth or sins (Simha et al., Citation2013). Similarly, among cancer patients receiving palliative care in the United States, Damen et al. (Citation2021) found bivariate association between RSS, perceived burden of symptoms, and QOL (Damen et al., Citation2021).
Therefore, hypothesis 1, which suggests a positive correlation between hope, MIL, and QOL has been confirmed. Additionally, the hypothesis proposing a negative association between RSS and QOL has also been validated. Hypothesis 2, indicating that hope, MIL and RSS predict QOL, has been supported by the study’s results. However, hypothesis 3, proposing that the stage of cancer would negatively moderate the association between hope and QOL in patients, did not find support in the present study.
Conclusion
The presence of hopefulness and sense of meaning in life contributes to an improved quality of life for individuals with cancer. However, some patients experience unresolved internal religious or spiritual conflicts through their illness journey. These struggles have a negative impact on their quality of life, highlighting a lack of spiritual or religious support within the palliative care they receive.
Implications
The results have important theoretical implications. In the Asian context, mostly the correlation of hopelessness and quality of life (Ravindran, Citation2019) and the correlation between depression and quality of life (Bhattacharyya et al., Citation2017; Shankar et al., Citation2021; Sharma & Purkayastha, Citation2017; Tiwari, Citation2019) in cancer patients have been examined so far. The present study bridges this gap in the literature by adopting a positive perspective and depicting the positive correlation between hope and QOL among cancer patients. It has also strengthened and supported some researchers who tried to study the correlation between hope and quality of life (Lang-Rollin & Berberich, Citation2018) in the Indian scenario. Moreover, this research will benefit a specific group of people Medical Counselors. The findings, in particular, can be effectively used by chaplains, psychiatric social workers, and nursing staff who provide support to patients. The healthcare team, which includes nurses, doctors, and other support staff, frequently encounter patients’ religious or spiritual questions and supportive needs. In palliative care settings, chaplains often offer consultation and support to the medical staff, as mentioned in a study by Liberman et al. (Citation2020). According to this study, addressing spiritual needs of patients is linked to improved clinical outcomes, especially an enhanced quality of life. Addressing spiritual needs entails resolving religious and/or spiritual conflict while developing Spiritual Care Interventions (SCI). Furthermore, in a multi-faith, multi-religion country like India, designing the spiritual intervention to address spiritual and/or religious struggle requires interfaith experts.
Limitations
The main limitation of this study is that the findings cannot be generalized across cultures. Understanding the concept of quality of life, for instance, is subject to cultural variation. The use of self-report inventories is also constrained by social desirability. As a result, a mixed-method approach could have provided a richer understanding of concepts such as religious or spiritual struggle, which is a more personalized experience. The working status of the person (employed/unemployed), nature of employment, and income of patients, as well as their impact on hope, could not be tapped in this study because the majority of the patients were from the middle or lower middle class, which could impact cancer patients’ quality of life (Jo & Son, Citation2004).
Furthermore, this study is based on patients with malignant types of cancer, and those with benign tumors were excluded. The nature of the tumor could also influence the QOL (Hörnquist et al., Citation1992). A comparison study of hope, MIL, RSS, and QOL in patients with benign and malignant cancers could have provided additional insight into the current study. The facets-wise study of WHO-QOL could add another perspective. Patients with higher socioeconomic status who report in private hospitals and self-finance their treatment were also excluded from this study. In the current study, the majority of the patients’ treatment was covered by a government scheme. Does self-financing or reliance on a scheme have an impact on the quality of life of cancer patients? As one aspect of the WHO-QOL brief scale is Environmental health, which encompasses items assessing financial resources. Patients who depends on government aid in India may experience delays in receiving assistance, while those who are financially affluent can access treatment promptly. This discrepancy can have an impact on their quality of life. Such questions were not addressed in this study, but they may be addressed in the future.
Summary of the key findings
Our study highlighted several important findings. Even in the face of illness, maintaining hope appears to positively contribute to QOL of cancer patients. The stage of the diseases did not significantly moderate the relationship between hope and QOL. This implies that hope remains relevant across different stages of the disease. Meaning in life is equally essential for the QOL of the patients. While hope and MIL contribute positively to QOL, it is essential to recognize that the RSS has a negative association. In summary, fostering hope and nurturing a sense of meaning enhance the lives of individuals facing cancer. Acknowledging and supporting individuals dealing with religious and spiritual struggles is equally vital.
Open Scholarship

This article has earned the Center for Open Science badge for Open Materials. The materials are openly accessible at https://osf.io/utpqd/?view_only=583dac7e6bc44642bfc92e837b863681.
Competing interest
The authors declare that they have no conflict of interest.
Ethical statement
Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki and was approved by an Institutional Review Board/Ethics Committee. ☑
The study received an exemption from an Institutional Review Board/Ethics Committee. ☑
Supplemental Material
Download MS Word (90.9 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abu-Raiya, H., Pargament, K. I., & Exline, J. J. (2015). Understanding and addressing religious and spiritual struggle in health care. Health and Social Work, 40(4), 126–134. https://doi.org/10.1093/hsw/hlv055
- Ano, G. G., & Pargament, K. I. (2012). Predictors of spiritual struggle: An exploratory study. Mental Health, Religion, and Culture, 16(4), 419–434. https://doi.org/10.1080/13674676.2012.680434
- Baczewska, B., Block, B., Kropornicka, B., Niedzielski, A., Malm, M., Lukasiewicz, J., Wojciechowska, K., Poleszak, W., Zwolak, A., & Makara-Studzińska, M. (2020). Hope of recovery in patients in the terminal phase of cancer under palliative and hospice care in Poland. BioMed Research International, https://doi.org/10.1155/2020/7529718
- Ballard, A., Green, T., McCaa, A., & Logsdon, M. C. (1997). A comparison of the level of hope in patients with newly diagnosed and recurrent cancer. Oncology Nursing Forum, 24(5), 899–904.
- Baumeister, R. F. (1991). Meanings of life. Guilford Press.
- Becker, P. E., Ellingson, S. J., Flory, R. W., Griswold, W., Kniss, F., & Nelson, T. (1993). Straining at the tie that binds: Congregational conflict in the 1980s. Review of Religious Research, 34(3), 193–209. https://doi.org/10.2307/3700594
- Benzein, E., & Berg, A. (2005). The level of and relation between hope, hopelessness and fatigue in patients and family members in palliative care. Palliative Medicine, 19(3), 234–e240. https://doi.org/10.1191/0269216305pm1003oa
- Berendes, D., Keefe, F. J., Somers, T. J., Kothadia, S. M., Porter, L. S., & Cheavens, J. S. (2010). Hope in the context of lung cancer: Relationships of hope to symptoms and psychological distress. Journal of Pain & Symptom Management, 40(2), 174–182. https://doi.org/10.1016/j.painsymman.2010.01.014
- Bernard, M., Strasser, F., Gamondi, C., Braunschweig, G., Forster, M., Kaspers-Elekes, K., Walther, S. V., & Borasio, G. D. (2017). Relationship between spirituality, meaning in life, psychological distress, wish for hastened death, and their influence on quality of life in palliative care patients. Journal of Pain & Symptom Management, 54(4), 514–522. https://doi.org/10.1016/j.jpainsymman.2017.07.019
- Bhattacharyya, S., Bharracherjee, S., Mandal, T., & Das, D. K. (2017). Depression in cancer patients undergoing chemotherapy in a tertiary care hospital of north Bengal, India. Indian Journal of Public Health, 61(1), 14–18. https://doi.org/10.4103/0019-557X.200252
- Blank, T. O., & Bellizzi, K. M. (2006). After prostate cancer: Predictors of well-being among long-term prostate cancer survivors. Cancer, 106(10), 2128–2135. https://doi.org/10.1002/cncr.21865
- Caldeira, S., Fiona, T., Emília, C. C., & Margarida, V. (2016). Nursing diagnosis of spiritual distress in women with breast cancer prevalence and major defining characteristics. Cancer Nursing, 39(4), 321–327. https://doi.org/10.1097/NCC.0000000000000310
- Chen, M. (2003). Pain and hope in patient with cancer: A role for cognition. Cancer Nursing, 26(1), 61–67. https://doi.org/10.1097/00002820-200302000-00009
- Chin, W. W. (1998). The partial least squares approach to structural equation modeling. In G. A. Marcoulides (Ed.), Modern methods for business research (pp. 295–336). Lawrence Erlbaum Associates.
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed). Lawrence Erlbaum Associates.
- Cui, J., Fang, F., Shen, F., Song, L., Zhou, L., Ma, X., & Zhao, J. (2014). Quality of life in patients with advanced cancer at the end of life as measured by the McGill quality of life questionnaire: A survey in China. Journal of Pain and Symptom Management, 48(5), 893–902. https://doi.org/10.1016/j.jpainsymman.2014.02.016
- Damen, A., Exline, J., Pargament, K., Yao, Y., Chochinov, H., Emanuel, H., Handzo, G., Elikie, D. J., & Fitchett, G. (2021). Prevalence, predictors and correlates of religious and spiritual struggles in palliative cancer patients. Journal of Pain and Symptom Management, 62(3), 139–137. https://doi.org/10.1016/j.joainsymman.2021.04.024
- Dobrikova, P., Pcolkova, D., AlTurabi, L. K., & West Jr., D. J. (2015). The effect of social support and meaning in life on the quality of life care for terminally ill patients. American Journal of Hospice & Palliative Medicine, 32(7), 767–771. https://doi.org/10.1177/1049909114546208
- Duggleby, W., Ghosh, S., & Cooper, D. (2013). Hope in newly diagnosed cancer patients. Journal of Pain and Symptom Management, 46(5), 661–670. https://doi.org/10.1016/jpainsymman.2012.12.004
- Ellison, C. G., & Lee, J. (2010). Spiritual struggles and psychological distress: Is there a dark side of religion? Social Indicators Research, 98(3), 501–517. https://doi.org/10.1007/s11205-009-9553-3
- Emblen, J. D. (1992). Religion and spirituality defined according to current use in nursing literature. Journal of Professional Nursing, 8(1), 41–47. https://doi.org/10.1016/8755-7223(92)90116-g
- Emmons, R. A. (2005). Striving for the sacred: Personal meaning, life meaning, and religion. Journal of Social Issues, 61(4), 731–745. https://doi.org/10.1111/j.1540-4560.2005.00429.x
- Field, A. (2009). Discovering statistics using SPSS (3rd ed.). Sage Publications Ltd.
- Fornell, C., & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18(1), 39–50. https://doi.org/10.2307/3151312
- George, D., & Mallery, P. (2003). Reliability analysis. SPSS for windows, step by step: A simple guide and reference (4th ed.). Allyn & Bacon.
- Hair, J. F., Astrachan, C. B., Moisescu, O. I., Radomir, L., Sarstedt, M., Vaithilingam, S., … Ringle, C. M. (2021). Executing and interpreting applications of PLS-SEM: Update for family business researches. Journal of Family Business Strategy,12(3), 100392. https://doi.org/10.1016/j.jfbs.2020.100392.
- Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis (7th ed). Prentice Hall.
- Hair, J. F., Hult, G. T. M., Ringle, C. M., & Sarstedt, M. (2013). A primer on partial least squares structural equation modeling (PLS-SEM). Sage.
- Hair, J. F., Hult, G. T. M., Ringle, C. M., & Sarstedt, M. A. (2017). Primer on partial least squares structural equation modeling (PLS-SEM) (2nd ed.). SAGE.
- Hair, J. F., Sarstedt, M., Ringle, C. M., & Mena, J. A. (2011). An assessment of the use of partial least square structural equation modeling in marketing research. Journal of Academy Marketing Science, 40(3), 414–433. https://doi.org/10.1007/s11747-011-0261-6
- Herth, K. (1992). Abbreviated instrument to measure hope: Development and psychometric evaluation. Journal of Advance Nursing, 17(10), 1251–1259. https://doi.org/10.1111/j.1365-2648.1992.tb01843.x
- Herth, K. A. (1989). The relationship between level of hope and level of coping response and other variables in patients with cancer. Oncology Nursing Forum, 16(1), 67–72. https://pubmed.ncbi.nlm.nih.gov/2911529/
- Hörnquist, J. O., Hansson, B., & Åkerlind, I. (1992). Severity of disease and quality of life: A comparison in patients with cancer and benign disease. Quality of Life Research, 1(2), 135–141. https://doi.org/10.1007/BF00439721
- Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteriaversus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. https://doi.org/10.1080/10705519909540118
- Jim, H. S., Purnell, J. Q., Richardson, S. A., Golden-Kruetz, D., & Anderson, B. L. (2006). Measuring meaning in life following cancer. Quality of Life Research Journal, 15(8), 1355–1371. https://doi.org/10.1007/s11136-006-0028-6
- Jo, K. H., & Son, B. K. (2004). The relationship of uncertainty, hope and quality of life in patients with breast cancer. Journal of Korean Academy of Nursing, 34(7), 118–193. https://doi.org/10.4040/jkan.2004.34.7.1184
- Klinger, E. (1998). The search for meaning in evolutionary perspective and its clinical implications. In P. T. P. Wong & P. S. Fry (Eds.), The human quest for meaning: A handbook of psychological research and clinical applications (pp. 27–50). Lawrence Erlbaum Associates Publishers.
- Lang-Rollin, I., & Berberich, G. (2018). Psycho-oncology. Dialogues in Clinical Neuroscience, 20(1), 13–22. https://doi.org/10.31887/DCNS.2018.20.1/ilangrollin
- Li, M. Y., Yang, Y. L., Liu, L., & Wang, L. (2016). Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: A cross-sectional study. Health and Quality of Life Outcomes, 14(1), 73. https://doi.org/10.1186/s12955-016-0481-z
- Liberman, T., Kozikowski, A., Carney, M., Kline, M., Axelrud, A., Ofer, A., Rossetti, M., & Pekmezaris, R. (2020). Knowledge, attitudes, and interactions with chaplains and nursing staff outcomes: A survey study. Journal of Religion & Health, 59(5), 2308–2322. https://doi.org/10.1007/s10943-020-01037-0
- Madhawi, R., Pandey, A., Raj, S., Mandal, M., Devi, S., Sinha, P. K., & Singh, R. K. (2018). Geographical pattern of carcinoma gallbladder in bihar and its association with river Ganges and arsenic levels: Retrospective individual consecutive patient data from regional cancer centre. South Asian Journal of Cancer, 7(3), 167–170. https://doi.org/10.4103/sajc.sajc_37_18
- Majernikova, L., & Obrocnikova, A. (2017). Relationship between the quality of life and the meaning of life in cancer patients. Nursing in 21stCentury, 16(2), 13–17. https://doi.org/10.1515/pielxxiw-2017-0012
- Newtony, M. L. (1991). Every tomorrow, a vision of hope. Oncology Nursing Forum, 9(3), 117–126. https://doi.org/10.1300/J077v09n03_10
- Organization. Division of Mental Health, W. H. O. (1996, January 1). WHOQOL-BREF : introduction, administration, scoring and generic version of the assessment : field trial version, December 1996. WHOQOL-BREF : Introduction, Administration, Scoring and Generic Version of the Assessment : Field Trial Version, December 1996. Retrieved January 6, 2023, from https://apps.who.int/iris/handle/10665/63529
- Pargament, K. I. (2007). Spiritually integrated psychotherapy: Understanding and addressing the scared. Guildford Press.
- Pargament, K. I., Smith, B. W., Koenig, H. G., & Perez, L. (1998). Patterns of positive and negative religious coping with major life stressors. Journal for the Scientific Study of Religion, 37(4), 710–724. https://doi.org/10.2307/1388152
- Puchalski, C., Ferrell, B., Virani, R., Otis-Green, S., Baird, P., Bull, J., Chochinov, H., Handzo, G., Nelson-Becker, H., Prince-Paul, M., Pugliese, K., & Sulmasy, D. (2009). Improving the quality of spiritual care as a dimension of palliative care: The report of the consensus conference. Journal of Palliative Medicine, 12(10), 885–904. https://doi.org/10.1089/jpm.2009.0142
- Ramasubbu, S. K., Pasricha, R. K., Nath, U. K., Rawat, V. S., & Das, B. (2021). Quality of life and factors affecting it in adult cancer patients undergoing cancer chemotherapy in a tertiary care hospital. Cancer Reports, 4(2), e1312. https://doi.org/10.1002/cnr2.1312
- Ravindran, O. S. (2019). A comparative study on perceived stress, coping, quality of life, hopelessness between cancer patients and survivors. Indian Journal of Palliative Care, 25(3), 414–420.
- Rustøen, T., & Wiklund, I. (2000). Hope in newly diagnosed patients with cancer. Cancer Nursing, 23(3), 214–219.
- Shankar, A., Dracham, C., Ghoshal, S., & Grover, S. (2021). Prevalence of depression and anxiety disorder in cancer patients: An institutional experience. Indian Journal of Cancer, 53(3), 432–434. https://doi.org/10.4103/0019-509X.200651
- Sharma, N., & Purkayastha, A. (2017). Factors affecting quality of life in breast cancer patients: A descriptive cross-sectional study with review of literature. Journal of Mid-Life Health, 8(2), 75–83. https://doi.org/10.4103/jmh.JMH_15_17
- Sharour, L. H. J. A. (2010). Psychosocial predictors of quality of life among Jordanian colorectal cancer patients: A mixed method study. Doctoral thesis submitted to Giffith University, School of Nursing and Midwifery. http://doi.org/10.259041912/2514
- Simha, S., Noble, S., & Chaturvedi, S. K. (2013). Spiritual concerns in Hindu cancer patients undergoing palliative care: A qualitative study. Indian Journal of Palliative Care, 19(2), 99–105. https://doi.org/10.4103/0973-1075.116716
- Soper, D. S. (2021). A-priori sample size calculator for structural equation models [Software]. https://www.danielsoper.com/statcalc
- Soylu, C., Babacan, T., Sever, A. R., & Altundag, K. (2016). Patients understanding of treatment goals and disease course and their relationship with optimism, hope, and quality of life: A preliminary study among advanced breast cancer outpatients before receiving palliative treatment. Supportive Care in Cancer, 24(8), 3481–3488. https://doi.org/10.1016/j.vhri.2013.01.011
- Srivastava, V., Ansari, M. A., Kumar, A., Shah, A. G., Meena, R. K., Sevach, P., … Singh, O. M. (2016). Study of anxiety and depression among breast cancer patients from north India. Clinical Psychiatry, 2(1), 1–7. https://doi.org/10.21767/2471-9854.100017.
- Taylor, J. D. (2000). Confronting breast cancer: Hope and health. In C. R. Snyder (Ed.), Handbook of hope: Theory, measures, and applications (pp. 355–371). Academic Press.
- Tiwari, A. (2019). Prevalence of depression and anxiety among cancer patients in small town in India: Single center study. International Journal of Radiation Oncology, Biology, Physics, 103(4), 1018. https://doi.org/10.1016/j.ijrobp.2018.11.060.
- Vartak, J. (2015). The role of hope and social support on resilience in cancer patients. Indian Journal of Mental Health, 2(1), 35–42. https://doi.org/10.30877/IJMH.2.1.2015.35-42
- Wakiuchi, J., Marchi, J. A., Norila, L. S., Mareon, S. S., & Sales, C. A. (2015). Patients undergoing chemotherapy. Acta Paulista de Enfermagem (Paulista Nursing Act), 28(3), 202–208. https://doi.org/10.1590/1982-0194201500035
- Werts, C. E., Linn, R. L., & Joreskog, K. G. (1974). Quantifying unmeasured variables. In H. M. Blalock, Jr. (Ed.), Measurement in the social sciences (pp. 270–292). Aldine Publishing Corporation.
- Whiteford, H. S., & Olver, L. N. (2012). The multidimensionality of spiritual-wellbeing: Peace, meaning and faith and their association with quality of life and coping in oncology. Psycho-Oncology, 21(6), 602–610. https://doi.org/10.1002/pon.1937
- Winkelman, W. D., Lauderdale, B. A. K., Balboni, M. J., Phelps, A. C., Peteet, J. R., Block, S. D., Kachnic, L. A., Wheele, J. J., & Balboni, T. A. (2011). The relationship of spiritual concerns to the quality of life of advanced cancer patients: Preliminary findings. Journal of Palliative Medicine, 14(9), 1022–1028. https://doi.org/10.1089/jpm.2010.0536
- Wong, P. T. P. (1998). Implicit theories of meaningful life and the development of the personal meaning profile (PMP). In P. T. P. Wong & P. S. Fry (Eds.), The human quest for meaning: A handbook of psychological research and clinical applications (pp. 111–140). Lawrence Erlbaum Associates Publishers.
- World Health Organization (WHO). (1993). Study protocol for the World Health Organization project to develop a quality of life assessment instrument (WHOQOL). Quality of Life Research, 2(2), 153–159. https://doi.org/10.1007/BF00435734
- Zhang, Y., Cui, C., Wang, Y., & Wang, L. (2020). Effects of stigma, hope and social support on quality of life among Chinese patients diagnosed with oral cancer: A cross-sectional study. Health & Quality of Life Outcomes, 18(1), 112. https://doi.org/10.1186/s12955-020-01353-9
- Zumstein-Shaha, M., Ferrell, B., & Economou, D. (2020). Nurses’ response to spiritual needs of cancer patients. European Journal of Oncology Nursing, 48, 101792. https://doi.org/10.1016/j.ejon.2020.101792