
ABSTRACT
Inflammatory bowel disease (IBD) is a chronic disabling inflammatory process that affects young individuals, with growing incidence. The etiopathogenesis of IBD remains poorly understood. A combination of genetic and environmental factors triggers an inadequate immune response against the commensal intestinal flora in IBD patients. Thus, a better understanding of the immunological mechanisms involved in IBD pathogenesis is central to the development of new therapeutic options.
Current pharmacological treatments used in clinical practice like thiopurines or anti-TNF are effective but can produce significant side effects and their efficacy may diminish over time. In fact, up to one third of the patients do not have a satisfactory response to these therapies. Consequently, the search for new therapeutic strategies targeting alternative immunological pathways has intensified. Several new oral and parenteral substances are in the pipeline for IBD.
In this review we discuss novel therapies targeting alternative pro-inflammatory pathways like IL-12/23 axis, IL-6 pathway or Janus Kinase inhibitors; as well as others modulating anti-inflammatory signalling pathways like transforming growth factor-β1 (TGF-β1). We also highlight new emerging therapies targeting the adhesion and migration of leukocytes into the inflamed intestinal mucosa by blocking selectively different subunits of α4β7 integrins or binding alternative adhesion molecules like MAdCAM-1. Drugs reducing the circulating lymphocytes by sequestering them in secondary lymphoid organs (sphingosine-1-phosphate (S1P) receptor modulators) are also discussed. Finally, the latest advances in cell therapies using mesenchymal stem cells or engineered T regs are reviewed. In addition, we provide an update on the current status in clinical trials of these new immune-regulating therapies that open a new era in the treatment of IBD.
Inflammatory bowel disease (IBD) is a chronic disabling inflammatory process that affects mainly the gastrointestinal tract and may present associated extraintestinal manifestations.Citation1 IBD includes both ulcerative colitis (UC) and Crohn's disease (CD). In UC, the inflammation takes place in the colon and rectum, is limited to the mucosa and always extends in oral direction from the rectum.Citation2 CD can affect any part of the gastrointestinal tract (typically the ileocecal area) and is characterised by transmural inflammation and local complications like stenosis, fistulae and abscesses.Citation3
It predominantly affects young individuals with symptoms like abdominal pain, chronic diarrhea, fever, rectal bleeding and weight loss; alternating flares and periods of remission.Citation3 The prevalence of IBD in western countries is estimated to be up to 0.5% of the general population, with growing incidence.Citation4 The treatment of IBD requires the continuous use of powerful anti-inflammatory drugs (corticosteroids, thiopurines, anti-tumour necrosis factor [anti-TNF] agents etc.) and hospitalisation or surgery to manage its complications.Citation1-Citation3 This results in significantly compromised quality of life as well as a huge economic burden for society with high associated healthcare costs.Citation5 In fact, only the direct costs in Europe are estimated to exceed €5.6 billion annually.Citation6
The etiopathogenesis of the disease remains largely unknown. It is currently considered a polygenic immune disorder involving: 1) individual genetic factors; 2) environmental factors; 3) intestinal flora (microbiome); and 4) immune response. A combination of these factors triggers an inadequate immune response against the commensal flora in genetically predisposed subjects.Citation7,Citation8
Several alterations in some key innate immunity mechanisms have been reported in recent years involving both the recognition and clearance of intracellular organisms and bacteria, such as alterations in the nucleotide-binding oligomerisation domain-containing protein 2 (NOD2)Citation9 or in the autophagy related protein 16L (ATG16L).Citation10 In addition, other factors can contribute to the appearance of recurrent infections and chronic intestinal inflammation, such as: alterations in the intestinal permeabilityCitation11,Citation12; alterations in the mucosal layerCitation13,Citation14; dysfunction in the production of defensins by Paneth cellsCitation15 or alterations in the stress mechanisms of the endoplasmic reticulum.Citation16
CD is considered to be a predominant type 1 T helper cell (Th1)- and Th17-mediated disease with an increased production of IL-17, IFN-γ and TNF-α; while UC has been associated with a dysregulated Th2 response.Citation2
However, the IL-23 pathway – that is crucial to the function of Th17 cells – is altered in both conditions.Citation17 The importance of regulatory T cells (Tregs) and other unconventional T cells like natural killer T cells (NKT), innate lymphoid cells (ILC) or gammadelta (γδ) T cells have been increasingly recognised in IBD pathogenesis, underlining its complexity.Citation7,Citation18-Citation20
This impaired immune response leads to an increased infiltration of leukocytes into the inflamed intestinal mucosa, which contributes to persistent inflammation.Citation21 Understanding the interplay between these cytokines and the different immune cells is central to the development of new therapeutic options in IBD.
Heterogeneity is an important issue in the clinical management of IBD patients since both clinical manifestations, disease location and behavior (phenotypes) and response to different therapies varies widely from patient to patient.Citation1
The current treatment of IBD includes mesalazine (oral and rectal formulations), glucocorticoids (conventional and other forms like budesonide or beclomethasone), antibiotics (typically ciprofloxacine and metronidazole), immunosuppressants (mostly azathioprine/6-mercaptopurine or methotrexate) and anti-TNF agents (infliximab, adalimumab, certolizumab pegol and golimumab). Recently, the anti-integrin antibody vedolizumab and the antibody against IL-12/23 ustekinumab have been approved for IBD.Citation22,Citation23
The introduction of anti-TNF agents into clinical practice (infliximab was first approved in 1998 and 2005 for CD and UC, respectively) both for the induction of remission and as maintanence therapy, has improved the outcomes of IBD patients significantly.Citation24 However these drugs have several limitations: 1) they are injectable (intravenous or subcutaneous) complicating the compliance; 2) they work only in a subset of patients (one third of the patients show no benefit); 3) they are immunogenic, causing allergic reactions and secondary loss of response (in approximately another third of the cases) due to antibody formation; 4) they are expensive; and 5) can lead to reactivation of infections – like tuberculosis or hepatitis B – and may increase the risk of some cancers.Citation25-Citation27 Moreover, the need for surgery remains high despite of the wide use of biologics in clinical practice (the risk of surgery 10 years after diagnosis is still 16% in UC and as high as 47% in CD patients).Citation28,Citation29
Thus, there is an urge for the development of new therapeutic targets for IBD. An increased insight into IBD pathogenesis (and especially the immunological aspects) can provide an excellent opportunity for therapeutic advances. Consequently, the search for new therapeutic strategies targeting alternative inflammatory cytokines and immunological pathways has intensified in the recent years. New oral and parenteral substances regulating alternative immune pathways like IL-12/23 axis, IL-6, Janus Kinase inhibition, TGF-β pathway, as well as the regulation of adhesion/migration of leucocytes or novel cell therapies using mesenchymal stem cells (MSC) or engineered T cells are in the pipeline. Here, we review the most promising of those new coming approaches in immunotherapy for IBD (summarized in and ).
Targeting pro-inflammatory pathways
The interleukin 12-family
The interleukin-12 (IL-12) family of five cytokines are heterodimeric cytokines composed of two covalently linked chains.Citation30 IL-12 and IL-23 are pro-inflammatory and have been found to be pathogenic in animal models of intestinal inflammation and in IBD.Citation31-Citation33
IL-12 consist of the heterodimeric proteins p40 and p35, while IL-23 consists of the heterodimeric proteins p40 and p19. Therefore, the shared p40 protein is a common target of both these cytokines. IL-12 and IL-23 secreted from antigen presenting cells (dendritic cells, macrophages) spark off intestinal inflammation and maintain the inflammatory response by secretion of inflammatory cytokines like IL-6, IL-17 and TNF-α from macrophages, neutrophils and natural killer cells.Citation17,Citation31,Citation33 IL-12 and IL-23 favour Th1 and Th17 differentiation of naïve T-cells, in CD, as opposed to the postulated Th2 domination in UC.Citation17,Citation34 IL-12 and IL-23 signal through heterodimeric receptors: ILRβ1 and IL12Rβ2 for p40 and p35 subunits of IL-12; and IL-23R and ILRβ1 for p19 and p40 subunits of IL-23.Citation32 Even though IL-23 might favour Th17 differentiation in CD, single nucleotide polymorphisms (SNPs) have been found in candidate gene encoding the IL-23 receptor (IL23R), which is associated with both increased and reduced risk for CD and UC.Citation35-Citation37 IL-12 and IL-23 signalling is mediated via Janus kinase (JAK)-signal transducer and activator of transcription (STAT)-proteinsCitation33 and induces expression of interferon gamma (IFN-γ) and IL-17 from Th1 and Th17 cells, respectively.
Given the importance of the IL-23–IL-17 axis and IL-17 overexpression in CD, blocking IL-17 could be beneficial. However, the anti-IL-17A monoclonal antibody secukinumab and anti-IL-17 receptor antibody brodalumab were both ineffective in CD.Citation38,Citation39 This is consistent with a study in mice showing the importance of IL-17 production by γδ T cells (independent of IL-23) for maintenance and protection of the epithelial barrier in the intestinal mucosa.Citation40 Even though IL-23 contributes to tissue damage in IBD, it has an important role controlling infections. In fact, IL-23 and IL-17RA knockout mice have increased susceptibility and mortality to pulmonary infection with Klebsiella pneumoniae and IL-23 knockout mice showed increased mortality after enteric infection with Citrobacter rodentium.Citation41 Moreover, mice with IL-23R deficiency in intestinal epithelial cells have reduced IL-22 induction, leading to increase in pro-inflammatory flagellated bacteria and increased mortality to dextran sodium sulfate colitis.Citation42 In addition, intestinal epithelium derived IL-23 mediates mucosal healing via IL-22.Citation43 Of note, IL-23R have shown opposing roles in different colitis models.Citation44,Citation45
Ustekinumab is a human anti-p40 IgG1 antibody blocking both IL-12 and IL-23. It is administered intravenously, and it has proven to be effective in CD both for induction and maintenance therapy after anti-TNF failure.Citation46 Another antibody against the p40 subunit – briakinumab – has been tested in CD with some clinical benefit,Citation47,Citation48 but the overall quality of the evidence for the outcome clinical remission was rated as low in a recent meta-analysis.Citation49 In fact, briakinumab studies have been discontinued due to limited clinical efficacy.Citation49,Citation50
Concerns have been raised about cardiovascular safety for both ustekinumab and briakinumab,Citation51,Citation52 but a Cochrane review concludes that both drugs are safe.Citation49 The new drug brazikumab – AMG 139/MEDI2070 – blocking the p19 subunit (specific for IL-23) was associated with clinical improvementCitation53 in patients with CD and TNF-antagonist failure. One study with risankizumab (BI 655066) – also targeting the p19 subunit – has shown some efficacy in CD.Citation54 Trials with other drugs targeting the p19 subunit, like mirikizumab (LY3074828) are underway.Citation50,Citation55
IL-6 pathway
IL-6 is a key pleiotropic cytokine with an immunoregulatory role in innate and adaptive immune responses synthesized by a wide variety of immune cells.Citation56 In fact, IL-6 can display pro- and anti-inflammatory properties depending on the context.
IL-6 has a protective role in many infections, where a transient production of IL-6 contributes to host defense and tissue repair.Citation57 In addition IL-6 induces the hepatic synthesis of C-reactive protein and other acute-phase proteins.Citation58 However, an excessive production of IL-6 can contribute to the maintenance of chronic inflammatory diseases like rheumatoid arthritis or IBD.Citation59,Citation60 In fact, IL-6 promotes specific differentiation of naïve CD4-positive cells into Th17 cells and inhibits TGF-β-induced Treg development.Citation61,Citation62 This dysregulation of Th17/Treg balance by IL-6 is considered to be key in the development of autoimmune and chronic inflammatory diseases, like IBD.Citation63
IL-6 can display its effects through a transmembrane receptor (IL-6R) and a soluble form (sIL-6R).Citation64 Blocking the IL-6 pathway ameliorates colitis in mice.Citation65 Both IL-6 and sIL-6R are highly expressed in the colonic mucosa of patients with IBDCitation66 and several studies show that high serum concentration of IL-6 is predictive of relapse in IBD.Citation67 Thus, IL-6 antagonism has been explored as a novel therapeutic target in IBD.
Intravenous tocilizumab, a humanized anti-IL6R antibody, was well tolerated but showed a modest effect in a pilot study including 36 CD patients. Clinical remission was obtained in 20% of treated patients versus none in the placebo group, but no differences in the endoscopic or histological examination were found.Citation68
PF-04236921, a fully human monoclonal IgG2 antibody that binds to IL-6, was given subcutaneously in 3 different doses (10, 50 and 200 mg) on days 1 and 28 in a phase II randomized, double-blind, placebo-controlled trial in 247 subjects with refractory CD.Citation69 Only the 50 mg s.c. arm achieved the primary endpoint (a clinical response defined as a CDAI-70 at week 8 or 12). This occurred in 49% and 47% of treated patients versus 31% and 29%, respectively, in the placebo arm (P <0.05 for both). However, the 200 mg arm was terminated early because of safety concerns. There was a troubling number of adverse events including 1 death because of post-operative respiratory failure and 6 patients experiencing complications like abscess or perforation during the induction study.Citation69 These serious side effects may be due to the pleiotropic functions of IL-6 including epithelial regeneration.Citation70 The inhibition of these beneficial functions – like the stimulation of mucosal healing – can lead to complications, and may limit the use of IL-6 inhibition in the future.
Janus Kinase inhibitors
The inhibition of JAK by small oral molecules has been tested in several autoimmune diseases like rheumatoid arthritis or myelofibrosis; and lately in IBD.Citation71-Citation74 JAK inhibitors can target signalling pathways used by multiple cytokines contributing to intestinal inflammation in IBD like IL-2, IL-6, IL-12, IL-21, IL-23 or IFN-γ (reviewed in refs. Citation75-Citation77).
JAKs are non-receptor tyrosine kinases expressed in multiple immune cells comprising 4 members: JAK1, JAK2, JAK3, and Tyrosine kinase 2 (TYK2). These proteins are bound to the intracellular domain of several cytokine and hormone receptors where they facilitate signal transduction. The binding of the cytokine to its receptor results in JAK activation and auto-phosphorylation as well as phosphorylation of the receptor chains, forming binding sites and activating STATs. As a result, STATs form homo- or heterodimers and translocate to the nucleus where they modulate the transcription of target genes. There are seven STAT family members (STAT1, STAT2, STAT3, STAT4, STAT5A, STAT5B, and STAT6). Thus, each cytokine will activate different patterns in the JAK-STAT pathway leading to different immunomodulatory effects.Citation76,Citation77
The possibility of inhibiting several pro-inflammatory cytokines interacting with this pathway led to the test of tofacitinib (an oral JAK inhibitor that mainly inhibits JAK1, JAK2 and JAK3) in UC. A phase II randomized, placebo-controlled trial including 194 active UC patients showed that tofacitinib 15 mg oral twice daily produced a statistically significant clinical response at week 8 (primary endpoint), as well as clinical remission and endoscopic response (secondary outcomes) compared with placebo. A dose-dependent increase in both LDL and HDL cholesterol concentrations which reversed after discontinuation of the drug was observed. In addition, 3 patients treated with tofacitinib had an absolute neutrophil count of less than 1500/mm3 during the study period and 2 presented serious adverse events in form of infection.Citation73
The results of two phase III trials testing tofacitinib 10 mg twice daily for the induction of remission in active UC (OCTAVE Induction 1 and 2) have been recently presented.Citation74 More patients receiving tofacitinib achieved remission, mucosal healing and clinical response in both studies compared with placebo at week 8. No differences regarding previous anti-TNF treatment were reported. Tofacitinib showed a quick onset of action (as for week 2) and the rate of serious adverse events was similar across groups. However, increases in serum lipids (cholesterol, LDL and HDL) and creatine kinase levels were reported with tofacitinib.Citation74
A phase III study assessing the effectiveness and safety of tofacitinib in the maintenance of remission in UC has recently been completed and a multicenter open label extension phase III study to address the safety at 12 months is still recruiting patients (NCT01458574 and NCT01470612, respectively).
In contrast to the results of tofacitinib in UC, recent trials in patients with CD have produced disappointing results.Citation78,Citation79 A phase II trial failed to show any significant differences in the percentage of CD patients who achieved clinical responses or clinical remission after 4 weeks administration of tofacitinib (1, 5, or 15 mg) or placebo twice daily. However, the high placebo response and short duration of treatment, together with the biological effects observed with high doses of tofacitinib (significant reductions in CRP and faecal calprotectin), encouraged the continuation of the trials in CD. Consequently, two phase IIb studies evaluated the efficacy and safety of tofacitinib for induction and maintenance treatment in patients with moderate-to-severe CD.Citation79 Again, both primary efficacy endpoints (proportion of patients in clinical remission at week 8 and clinical response or remission at week 26) were not significantly different from placebo.Citation79 Thus, further development of tofacitinib in CD has been discontinued.
Filgotinib (GLPG0634, GS-6034), a novel once daily oral JAK1-selective inhibitor, was also tested in a large multicentre phase II study. Forty seven percent of patients treated with filgotinib 200 mg/day achieved clinical remission at week 10 (primary endpoint) versus 23% in the placebo group.Citation80 However, the proportion of patients achieving endoscopic remission or mucosal healing was similar in both groups. Serious treatment-emergent adverse effects were reported more often in patients treated with filgotinib than in the placebo group (9% versus 4%) and serious infections occured in 3% of patients. In addition, exposure to filgotinib for 20 weeks resulted in 12% increase in mean LDL levels.Citation80
The results of two phase III studies for the induction and long-term maintenance for CD (NCT02914561 and NCT02914600) will help test the efficacy and safety of filgotinib. Moreover, filgotinib has also entered two phase III studies for UC (NCT02914522 and NCT02914535). Another selective oral JAK1/3 inhibitor (JNJ-54781532) has completed a phase IIb trial to investigate its safety and effectiveness in active UC (NCT01959282). The results have not been communicated yet.
Laquinimod
Laquinimod is a new oral medication with several anti-inflammatory properties and a good safety profile that has been already clinically tested in multiple sclerosisCitation81,Citation82 and lupus nephritis.Citation83
Its mechanism of action is not fully understood. Laquinimod suppresses Th1 and Th17-responses (inhibiting the production of TNF-α, IL-17 and IL-12) and induces a Th2 shift (increasing the production TGF-β, IL-10 and IL-4). It can also stimulate the action of Tregs and is able to inhibit leucocyte migration (reviewed in refs. Citation84, Citation85).
A dose escalation multicentre double-blind phase II study evaluated the safety and efficacy of laquinimod as induction therapy in patients with active CD, showing a significant clinical improvement and a favourable safety profile.Citation86 Patients received laquinimod orally (0.5, 1, 1.5 or 2 mg/day) or placebo for 8 weeks with 4-week follow-up. The proportion of patients in clinical remission at week 8 was higher for the laquinimod 0.5 mg (48.3%) and 1 mg (26.7%) groups compared to higher doses of laquinimod or placebo (15.9%).
The incidence of side effects was similar. An elevation of liver enzymes reported in previous MS trials was not observed in the 0.5 mg group. Laquinimod was well tolerated and decreased significantly faecal calprotectin levels.Citation86 Thus, laquinimod is a promising oral drug with a good safety profile and broad-spectrum anti-inflammatory and immune-regulatory properties. A phase III clinical development programme exploring the effect of the most effective dose (0.5 mg/day) along with a lower dose (0.25 mg/day) for the induction and maintenance of remission in moderate to severe CD is planned.Citation86
Targeting anti-inflammatory pathways
The transforming growth factor β (TGF–β) pathway. SMAD7 antisense oligonucleotide
TGF–β1 is a multifunctional cytokine produced by many immune cells. It has been shown to down-regulate immune responses in the intestine and participates in several anti-inflammatory mechanisms. TGF–β1 suppresses the activation macrophages and effector T cells, stimulates the differentiation of Tregs and induces mucosal healing by promoting margination of epithelial cells and production of collagen (reviewed in refs. Citation87-Citation89).
TGF–β1 signals through two transmembrane protein kinase receptors (TGFβR1 and TGFβR2) that, upon activation, phosphorylates SMAD2 and SMAD3 that subsequently associate with SMAD4. This complex translocates to the nucleus where it regulates the expression of target genes. SMAD7 is an intracellular negative regulator of TGF–β1 signaling that prevents the phosphorylation of SMAD2 and SMAD3.Citation90,Citation91
IBD patients present a decreased activity of the anti-inflammatory cytokine TGF–β1 caused by increased levels of SMAD7 secondary to decreased degradation.Citation92 In addition, previous studies showed that specific antisense oligonucleotides for SMAD7 restores TGF–β1 signaling decreasing pro-inflammatory cytokine production.Citation93 Consequently, the inhibition of SMAD7 could be a novel potential therapeutic target in IBD.
Mongersen is a new oral antisense oligonucleotide that targets SMAD7 mRNA facilitating the degradation of SMAD7 and thus, restoring the anti-inflammatory effects of TGF–β1.Citation94 Mongersen is enveloped in a pH-dependent release tablet that makes it optimal to treat ileocolonic CD. Pharmacokinetic studies suggested that it acts locally and is not systemically available in plasma.Citation95
After assessing the safety and tolerability of mongersen in a phase I trial,Citation95 166 patients with moderate-to-severe CD were enrolled in a phase II study. Three oral doses of mongersen (10, 40, or 160 mg/day) or placebo were administered for two weeks. The primary endpoint was defined as CDAI <150 points at week two and maintained for two weeks. Fifty-five and 65% of patients achieved clinical remission in the 40 mg and 160 mg mongersen groups respectively, as compared with 10% in the placebo group (P < 0.001).Citation94
Interestingly, no statistically significant differences were found in the number of participants achieving normalization of CRP levels after treatment, raising the question of its effect on mucosal inflammation. The authors argument that the short duration of the study could have been insufficient to reach CRP normalization.Citation94 In addition, the lack of endoscopic evaluation is a major drawback of the study. To address this issue, a phase Ib randomized study investigated the endoscopic outcomes in 63 CD patients after therapy with a high dose of mongersen (160 mg daily for 4, 8 or 12 weeks), showing endoscopic response in 37% of patients (defined as a reduction in Simple Endoscopic Score for CD of at least 25% in comparison to baseline).Citation96
The rate of adverse events did not differ among groups and most adverse events were considered to be related to complications of the disease in the pivotal phase II study.Citation94 However, the short duration of therapy (2 weeks) may also limit the evaluation of safety in a chronic disease like CD.Citation94
TGF–β1 is a profibrotic agent that can activate fibroblasts and smooth muscle cells and increase the production of collagen, which raises concerns regarding the possible effect of its therapeutic stimulation in the production of strictures and eventually in the incidence of colon cancer.Citation97 Of note, patients with a history of strictures or fistulae were excluded from the main study by Monteleone et al.Citation94
A previous study tried to address this issue. A small open label study including 15 patients treated with mongersen daily for a week showed no association with the development of small bowel strictures at 6 months.Citation98 However, the question regarding the development of fibrosis on the long term needs to be further addressed. A phase II study exploring the efficacy and safety of mongersen in UC has recently been completed (NCT02601300). Two ongoing randomized multicentre phase III trials for induction and maintenance of remission in CD were prematurely discontinued in October 2017 by the sponsor pharma company after assessing overall benefit/risk in an interim futility analysis.
Targeting adhesion, trafficking and migration of immune cells
Adhesion molecules
Lymphocyte migration and retention in the intestinal mucosa and epithelium is mediated by adhesion molecules expressed on lymphocytes, the endothelium, the epithelium and the extracellular matrix (cell adhesion molecules [CAMs], integrins, selectins and cadherins).Citation99 Blocking the adhesion of lymphocytes to the endothelium could alleviate the inappropriate immune reaction in IBD, stopping T-cell recruitment and retention to the inflamed mucosa. Endothelial adhesion molecules are induced during inflammation through cytokine (IL-1 and TNF) activation.Citation100-Citation102
The intercellular adhesion molecule 1 (ICAM-1) antisense oligonucleotide alicaforsen showed no effect in CD given intravenously. However, it is effective in distal UC and pouchitis when used in form of enemas.Citation103-Citation105
Gut activated T-lymphocytes express the α4β7 integrin for specific homing to the intestinal mucosa,Citation106 while the corresponding ligand mucosal vascular addressin cell adhesion molecule (MAdCAM-1) is primarily expressed in the gastrointestinal tract (endothelium and lymphoid tissue).Citation107 Thus, targeting the gut-specific binding between α4β7 expression on effector/memory T-cells and MAdCAM-1 of the inflamed intestinal endothelium is a therapeutic option.
Natalizumab, a monoclonal antibody against human α4 integrin blocks the α4-subunit of α4β1 and α4β7 integrins, inhibiting the adhesion to vascular cell adhesion molecule-1 (VCAM-1) and MAdCAM-1, respectively.Citation108 Therefore, inhibition of lymphocyte – endothelial adhesion is not gut specific for natalizumab. Natalizumab is effective in the treatment of multiple sclerosisCitation109 and in inducing and maintaining remission in CD.Citation110,Citation111 Enthusiasm for natalizumab in the treatment of CD has been curbed due to the increased risk of developing John Cunningham (JC) virus-related progressive multifocal leukoencephalopathy (PML).Citation112 Due to this and also because of the development of vedolizumab, a monoclonal antibody against the α4β7 integrin, natalizumab is no longer a first option for anti-adhesion treatment in IBD.
AJM300 is another drug that targets the α4-subunit of α4β1 and α4β7 integrins, thus blocking binding to VCAM-1 and MAdCAM-1. In contrast to natalizumab, which is administered intravenously, AJM300 is given orally. It has been studied in patients with active UC and was well tolerated (no serious adverse events, including PML); and was better than placebo for induction of clinical response, remission and mucosal healing.Citation113
Targeting α4β7 makes vedolizumab gut-specific. It inhibits the gut homing of lymphocytes by blocking α4β7 binding to MAdCAM-1. Vedolizumab was evaluated in UC and CD in the GEMINI 1 and GEMINI 2 studies, respectively.Citation114,Citation115 Vedolizumab was significantly better for induction and maintenance of remission in UC compared to placebo.Citation114 CD patients receiving vedolizumab were more likely to have a remission, but not a CDAI-100 response, and significantly more patients who had a response to induction therapy and continued to receive vedolizumab were in clinical remission after one year.Citation115 Another study evaluating the effect of vedolizumab found that 21–25% of patients starting vedolizumab for active IBD (21% for CD and 25% for UC) were in clinical remission after 54 weeks.Citation116 Long term efficacy (152 weeks) has been observed for anti-TNF failure and naïve patient with both UC and CD treated with vedolizumab, and patients losing effect with conventional 8-weekly dosing might benefit from increased dosing frequency.Citation117,Citation118 Vedolizumab has an excellent safety profile in both UC and CD: 2830 patients with 4811 person-years of vedolizumab exposure had no cases of PML and no increased risk of infection, serious infection or malignancy.Citation119 Vedolizumab is approved and in clinical use for both UC and CD.
Another antibody against α4β7 integrin – abrilumab (AMG 181/MEDI7183) – has been evaluated in both UC and CD in phase II studies with good safety and promising efficacy profiles.Citation120,Citation121 Anti-MAdCAM-1 therapy targeting the receptor of the α4β7 ligand is theoretically as promising as vedolizumab. The OPERA and TURANDOT studies evaluated the efficacy and safety of PF-00547659, a human monoclonal antibody that binds to MAdCAM-1, in patients with moderate to severe CD and moderate to severe UC, respectively.Citation122,Citation123 In CD, PF-00547659 was not better than placebo, but was safe.Citation122 In UC, the drug was better than placebo for induction of remission after 12 weeks and was safe and well tolerated.Citation123
Etrolizumab, a new agent targeting the β7 subunit of both the α4β7 and αEβ7 integrin, has also been studied. It acts inhibiting both T-cell mucosal recruitment and epithelial retention of intraepithelial lymphocytes through inhibition of α4β7-MAdCAM-1 binding (similar to vedolizumab) and epithelial αEβ7-E-cadherin bindings, respectively. Etrolizumab was more likely to achieve clinical remission at week 10 than placebo in moderately to severely active UC (21% for etrolizumab 100 mg, 10% for etrolizumab 300 mg and loading dose and 0% for placebo). Adverse events were similar in the three groups and no serious opportunistic infections including PML were recorded.Citation124 Several ongoing studies (NCT02136069, NCT02165215, NCT02118584, NCT02403323 and NCT02394028) are evaluating etrolizumab in both UC and CD.Citation125
Sphingosine-1-Phosphate (S1P) pathways
Reducing the circulating lymphocytes by sequestering them in secondary lymphoid organs is an attractive approach to reduce inflammation in the intestinal mucosa. A new class of oral small molecules modulating sphingosine-1-phosphate (S1P) receptor, has recently shown efficacy in IBD.Citation126
Sphingosine derives from the catabolism of endogenous cellular sphingolipids, that are essential constituents of cellular membranes. S1P is the 1-phosphorylated form of sphingosine. S1P can activate a family of five receptors (S1P1–5 receptors) exerting a wide range of immunological functions (reviewed in refs. Citation127-Citation129).
Of interest, the sphingosine 1-phosphate receptor 1 (S1P1) promotes lymphocyte egress from lymphoid organs to blood. A new generation of oral S1P receptor agonists induce internalization and degradation of the S1P1 receptor. That makes lymphocytes incapable of migrating from secondary lymphoid organs reducing the circulating lymphocytes in the blood and as a consequence, in the intestinal mucosa.Citation130-Citation132
Ozanimod is a new oral selective small-molecule agonist for S1P1 and to a lesser extent for S1P5 that reduces circulating lymphocytes by sequestering them in secondary lymphoid organs that showed efficacy in multiple sclerosis.Citation133 A recent double-blind, placebo-controlled phase II trial examined the safety and efficacy of oral 0.5 and 1 mg of ozanimod daily compared with placebo in active UC (TOUCHSTONE). The primary outcome (clinical remission at 8 weeks) was achieved in 16% and 14% respectively, versus 6% in the placebo arm (P = 0.048 and P = 0.14, respectively).Citation126 Significant differences in clinical response at week 8 were achieved only for the 1 mg group. As expected because of the mechanism of action of the drug, absolute lymphocyte counts in blood decreased after treatment (32% and 49% from baseline in patients who received 0.5 mg and 1 mg, respectively). Mucosal healing – but not histological remission – was achieved in both ozanimod groups.Citation126
Ozanimod showed a good safety profile. No important differences were observed in the most commonly reported adverse events between groups. Of note, 4 patients treated with ozanimod had an increase in the alanine aminotransferase level of more than three times the upper limit.Citation126 Since most patients that received 1 mg had lymphocyte counts below the lower limit of the normal range at week 8, future long-term studies are needed to assess the risk of infections.Citation126 Ozanimod has recently entered two phase III trials for induction and/or maintenance in UC (NCT02435992 and NCT02531126) that are still recruiting (as for January 2018); as well as a phase II multicentre study in moderately to severely active CD (NCT02531113).
Moreover, similar agents such as another S1P1 agonist etrasimod (APD334) have entered phase II trials for UC (NCT02447302 and NCT02536404). Amiselimod (MT-1303), an S1P1/S1P5 agonist, has recently completed two phase II trials for CD (NCT02389790 and NCT02378688). The results are awaited.
Cellular therapy
Mesenchymal stem cells (MSCs)
MSCs are nonhematopoietic multipotent cells that can be isolated from the connective tissues of most organs including the bone marrow (BM), adipose tissue and the umbilical cord. MSCs have self-renewal ability, can differentiate into various cell types and exert several interesting immunomodulatory properties (excellent reviews in refs. Citation134 and Citation135).
Since they constitute a heterogeneous group of cells, the International Society for Cellular Therapy proposed 3 criteria to define human MSCs: 1. must be plastic-adherent when maintained in standard culture conditions; 2. must express CD105, CD73 and CD90, and lack expression of CD45, CD34, CD14 or CD11b, CD79α or CD19 and HLA-DR surface molecules; and 3. must differentiate to osteoblasts, adipocytes and chondroblasts in vitro.Citation136
MSCs can inhibit Th1 and Th17 cell proliferation and promote Treg differentiation accompanied by a systemic reduction in pro-inflammatory cytokines (Il-6, IL-17 and IFN-γ) and an elevation of anti-inflammatory cytokines like TGF-β and IL-10.Citation137-Citation142
MSC also have the unique ability to migrate selectively into various sites of tissue injury and inflammation (like the intestinal mucosa), where they actually can be detected several days after intravenous injection in mice.Citation141,Citation143,Citation144 Locally, MSCs promote tissue repair and wound healing through stimulation of angiogenesis and inhibition of apoptosis,Citation145,Citation146 restoring the epithelial barrier integrityCitation147 and secreting potent growth factors like vascular endothelial growth factor (VEGF) and TGF-β1.Citation144
Those interesting features prompted the study of MSCs in mice models of colitis with promising results.Citation137-Citation141 In human studies, MSCs have been administered mainly by two methods: intravenously (i.v.) for the treatment of luminal IBD, or by local injection for perianal fistulizing CD.
A recent meta-analysis suggests that systemic infusion of MSCs is a relatively well tolerated therapy for luminal IBD. A total of 40.5% of patients (95% CI 7.5% – 78.5%) achieved remission after MSCs infusion. However, the studies included had high heterogeneity and risk for bias.Citation148
The first report using allogeneic BM-derived MSCs by systemic infusion in CD was published in abstract form by Onken J et al. in 2006.Citation149 Four out of 10 patients with active luminal CD refractory to steroids showed clinical response (one even achieved clinical remission).Citation149 The same approach using allogeneic BM-derived MSCs obtained from the sternum or the iliac crest and cultured for 5–6 weeks also showed some clinical efficacy. Moreover, an important number of the IBD patients treated were able to taper off steroids after treatment (34 out of 50 IBD patients).Citation150
A subsequent study revealed that 5 out of 7 IBD patients (3 UC and 4 CD) achieved clinical remission at 3 months after the infusion of MSC derived from BM and umbilical cord.Citation151 The use of 4 weekly infusions of BM-derived MSCs was effective in active luminal CD refractory to immunomodulators (clinical response in 12/15 patients, clinical remission in 8/15 and endoscopic improvement in 7/15 at day 42).Citation152 Most of those studies used doses that ranged from 1–8 × 106 MSC/kg.
An alternative approach for the use of MSCs in IBD has been its combination with standard therapy. Knyazev et al. recently reported that the addition of BM-derived MSCs to conventional therapy in UC patients decreased fecal calprotectin and histological indexes at 2, 6 and 12 months.Citation153 The same group reported that the addition of MSCs to infliximab decreased the relapse rate in luminal CD at 3 years.Citation154 However, both studies have been published only in abstract form, complicating further investigations regarding study design, methods and safety issues.
Serious adverse events related to allogenic MSCs are relatively uncommon and injections appear to be safe, as recently confirmed in a meta-analysis.Citation155 Commonly reported non-serious adverse events after infusion are headache, diarrhea, mild transfusion-reactions or dysgeusia, all of them self-limited.Citation152 Of note, the study by Forbes et al. reported an adenocarcinoma arising in a dysplasia associated lesion in one patient. After retrospective chart reviews, the authors suggested the possibility that the cancer was present prior to MSC infusion.Citation152 However, further large controlled trials are needed to address the long-term safety of allogeneic MSCs treatment in IBD.
Only two small studies used injections of autologous MSCs in refractory CD, showing a more modest effect and worse safety profile.Citation156,Citation157 Although clinical response was achieved in both studies, a worsening of the disease was reported in almost half of the patients,Citation156,Citation157 and two serious events possibly related to the treatment were noted (appendicitis and Clostridium difficile colitis).Citation157
Several trials are ongoing in both UC and CD, mostly using allogenic MSCs derived from the BM or the umbilical cord (NCT 02000362, NCT 02150551), both recruiting by January 2018. A phase II study exploring the use of BM-derived MSC in active CD has recently been completed (NCT00294112). Results for this novel therapeutic approach are awaited.
In addition, the use of local injection of MSCs has shown efficacy in the treatment of refractory perianal CD fistulas. The review of these studies is out of the scope of the present work (see recent extensive reviews in Citationrefs. 135, Citation148, Citation158).
T cell engineering
Tregs are a subset of T lymphocytes that are able to suppress the activation and effector function of multiple immune cells involved in intestinal inflammation and help maintain immune tolerance. Tregs are characterized by the expression of the transcription factor Foxp3 and the production of potent anti-inflammatory cytokines like IL-10 and TGF-β. They are considered to play a major role in the pathogenesis of IBD (reviewed in refs. Citation18 and Citation159).
Several studies using mice models resembling IBD support an anti-inflammatory role for Tregs.Citation160,Citation161 In most human studies a decreased number of Tregs in the peripheral blood of IBD patients is observed, while greater numbers accumulate in active inflammatory lesions suggesting an increased migration in active phases.Citation162-Citation164 However, Tregs' suppressive function is not compromised in IBD patients compared to healthy controls.Citation162 Furthermore, some studies showed that effector T cells that accumulated in the intestine of patients are partially resistant to Tregs,Citation165 which might suggest an effect of the intestinal inflammatory milieu in the function of Tregs in IBD.Citation18
Treg cell therapy has already shown efficacy in other inflammatory diseases like graft versus host diseaseCitation166 and type 1 diabetes.Citation167 The first study testing the efficacy of Tregs in IBD was published by Desreumaux et al. in 2012 in a phase I/IIa study including 20 CD refractory patients (Crohn's And Treg Cells Study [CATS1]).Citation168 Ovalbumin-specific type 1 Tregs (ova-Tregs) were isolated from patients' peripheral blood mononuclear cells, exposed to ovalbumin, and administrated intravenously in a single injection in escalating doses. In order to promote gut migration of ova-Tregs, patients ingested an ovoalbumin enriched diet (a meringue cake). The injections of ova-Tregs were well tolerated and 40% of the patients had a clinical response at weeks 5 and 8 (CDAI reduction of 100 points), but only 10% of patients achieved clinical remission (CDAI ≤150) and the clinical effect after a single dose was transient.Citation168 In addition, no information about the numbers of ova-Tregs that reached the intestinal mucosa or their stability and plasticity features was provided in this study. The results from a phase IIb multicenter placebo-controlled clinical trial with ova-Tregs in refractory CD (CATS29) are expected during 2018 (NCT02327221).
A recent study aimed to define the optimal population for Treg cell therapy comparing CD4+CD25+CD127loCD45RA+ and CD4+CD25+CD127loCD45RA−Treg subsets. Tregs were isolated from CD patients' blood, expanded in vitro and tested in a xenotransplant model of human intestine. The study showed that CD45RA+ Tregs do not convert to a Th17 phenotype in vitro, express gut homing molecules (like α4β7integrin) and suppress activation of lymphocytes isolated from inflamed mucosa of CD patients. Thus, the authors propose CD4+CD25+CD127loCD45RA+ as the most appropriate from which to expand Tregs for T cell therapy in future studies.Citation169
Some authors have pointed the possibility of manipulating γδ T cells to treat IBD. γδ T cells are unconventional T cells with interesting immunoregulatory and tissue healing properties recently implicated in CD pathogenesis.Citation20 γδ T cells have shown a protecting function against colitis in several murine modelsCitation170,Citation171 and appeared safe and effective in clinical trials in cancer immunotherapy.Citation172 However, no clinical studies to treat IBD have been published to this date.
Thus, although cellular therapies are emerging as safe and effective therapies, many unresolved questions like type of cells to use, adequate doses and long-term effects need to be addressed in larger clinical trials.
Other immune-regulating therapies
Finally, other therapeutic approaches have shown immune-modulating and anti-inflammatory properties in IBD. Promising candidates that showed efficacy in clinical trials are: fecal microbiota transplantationCitation173,Citation174; antibiotics with immune-regulating properties like metronidazole or ciprofloxacinCitation175-Citation178; modulation of mucosal immunity by helminthsCitation179,Citation180; dietary induction of Tregs by short fatty acids or prebioticsCitation181-Citation183; substitution of phosphatidylcholine to increase the mucus layerCitation184; or certain herbs and plants with immune-regulating characteristics like: curcumin, artemisia absinthium, myrrh, chamomile or wheatgrass.Citation185
Concluding remarks and future perspectives
IBD is a chronic disabling inflammatory process that affects young individuals, with growing incidence. The etiopathogenesis of IBD remains poorly understood, but recent studies show that improved understanding of the immunological mechanisms involved in IBD pathogenesis is key to the development of new therapeutic options.
Current pharmacological treatments used in clinical practice like thiopurines or anti-TNF are effective. However, some of these drugs have significant side effects like infections or an increased risk for certain cancers and their efficacy may diminish over time. In fact, up to one third of the patients do not have a satisfactory response to these therapies.
Consequently, the search for new therapeutic strategies targeting alternative immunological pathways has intensified. New therapies targeting alternative pro-inflammatory pathways like IL-12/23 axis, IL-6 pathway or Janus Kinase inhibitors are on its way. Alternatively, some emerging oral substances that aim to stimulate canonical immune-modulating pathways, like the TGF-β pathway, have shown clinical efficacy. The inhibition of adhesion and migration of leukocytes into the inflamed intestinal mucosa has also received much attention. Molecules like vedolizumab are currently approved for IBD and other approaches targeting alternative adhesion or migration mechanisms are in advanced phases in clinical trials. Finally, the possibility of engineering immune-modulating cells like MSCs or Tregs is a promising alternative approach, but cell therapies still need to prove safety and efficacy in larger clinical trials.
In conclusion, several novel treatment strategies for IBD are on their way and will certainly expand our therapeutic armamentarium in the next future. However, IBD is a very heterogeneous disorder where patients have different genetic and environmental backgrounds and can display a wide variety of clinical phenotypes. In addition, IBD treatment is still based basically on clinical and endoscopical findings and patients may have unpredictable responses to different therapies. This makes it difficult for the clinician to choose the appropiate drug according to risk factors and clinical course.
A better understanding of the immunopathogenesis of IBD is crucial to help the clinician to select the most appropiate therapeutic approach to maximize cost-efficacy and minimize risks and undesirable side-effects derived from the immune-regulation (like infections or the inhibition of other protective properties like epithelial healing). Furthermore, a combination of some of these novel drugs with the ones currently in use could be a plausible startegy to improve therapeutic outcomes by targeting different pathways.
Thus, it will be crucial to include an examination of immune responses before and after therapy and integrate these data with other genetic, serologic and mucosal variables to tailor our therapeutic decisions towards a real personalized medicine in IBD. We are in the opening of a new era in the treatment of IBD and immunotherapy is definitely going to play a major role in the next future.
Table 1. Novel drugs, therapeutic targets and current status in clinical studies.
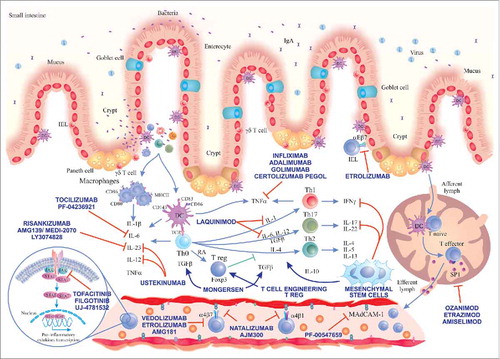
Figure 1. Immunological pathways targeted by the main novel therapies for IBD. A loss of intestinal barrier integrity takes place in IBD, leading to translocation of bacteria that triggers an exaggerated immune response with secondary activation of Th cell responses (Th1, Th2, Th17). We show the main drugs inhibiting IL-6 pathway, IL-12/23 axis, Jak inhibitors, laquinimod and stimulators of TGF-β1 pathway (mongersen). Drugs inhibiting TNF-α already approved for use in IBD and cell therapies using MSCs and Tregs and their main immune-modulation functions are depicted in the centre. Substances targeting different adhesion molecules are described in the blood vessel and in the gut epithelium (etrolizumab). On the bottom right, we show the mechanism of action of drugs reducing the circulating lymphocytes by sequestering them in secondary lymphoid organs (sphingosine-1-phosphate receptor modulators). Main abbreviations: IEL, intraepithelial lymphocyte; DC, dendritic cell; JAK, Janus kinase; STAT, signal transducer and activator of transcription; IL, interleukin; Th, T helper lymphocyte; TGF-β, transforming growth factor-beta; RA, retinoic acid; IFNγ, interferon gamma; S1P, sphingosine-1-phosphate.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgements
We would like to thank Dr. Miriam Giambelluca for her contribution and technical suggestions in the elaboration of the figure in this article; and Dr. Arne Kristian Sandvik for reviewing this manuscript.
References
- Abraham C, Cho JH. Inflammatory Bowel Disease. N Engl J Med. 2009;361:2066–78. doi:10.1056/NEJMra0804647. PMID:19923578.
- Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet. 2012;380:1606–19. doi:10.1016/S0140-6736(12)60150-0. PMID:22914296.
- Baumgart DC, Sandborn WJ. Crohn's disease. Lancet. 2012;380:1590–605. doi:10.1016/S0140-6736(12)60026-9. PMID:22914295.
- Molodecky NA, Soon IS, Rabi DM, Ghali WA, Ferris M, Chernoff G, Benchimol EI, Panaccione R, Ghosh S, Barkema HW, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54.e42. doi:10.1053/j.gastro.2011.10.001. PMID:22001864.
- Rocchi A, Benchimol EI, Bernstein CN, Bitton A, Feagan B, Panaccione R. Inflammatory bowel disease: a Canadian burden of illness review. Can J Gastroenterol. 2012;26(11):811–817. doi:10.1155/2012/984575. PMID:23166905.
- Burisch J, Jess T, Martinato M, Lakatos PL. The burden of inflammatory bowel disease in Europe. Journal of Crohn's and colitis. 2013;7:322. doi:10.1016/j.crohns.2013.01.010.
- de Souza HS, Fiocchi C. Immunopathogenesis of IBD: current state of the art. Nat Rev Gastroenterol Hepatol. 2016;13:13–27. doi:10.1038/nrgastro.2015.186. PMID:26627550.
- de Souza HSP, Fiocchi C, Iliopoulos D. The IBD interactome: an integrated view of aetiology, pathogenesis and therapy. Nat Rev Gastroenterol Hepatol. 2017;14:739–49. doi:10.1038/nrgastro.2017.110. PMID:28831186.
- Hugot J-P, Chamaillard M, Zouali H, Lesage S, Cezard J-P, Belaiche J, Almer S, Tysk C, O'Morain CA, Gassull M, et al. Association of NOD2 leucine-rich repeat variants with susceptibility to Crohn's disease. Nature. 2001;411:599–603. doi:10.1038/35079107. PMID:11385576.
- Hampe J, Franke A, Rosenstiel P, Till A, Teuber M, Huse K, Albrecht M, Mayr G, De La Vega FM, Briggs J, et al. A genome-wide association scan of nonsynonymous SNPs identifies a susceptibility variant for Crohn disease in ATG16L1. Nat Genet. 2007;39:207–11. doi:10.1038/ng1954. PMID:17200669.
- Zeissig S, Burgel N, Gunzel D, Richter J, Mankertz J, Wahnschaffe U, Kroesen AJ, Zeitz M, Fromm M, Schulzke JD. Changes in expression and distribution of claudin 2, 5 and 8 lead to discontinuous tight junctions and barrier dysfunction in active Crohn's disease. Gut. 2007;56:61–72. doi:10.1136/gut.2006.094375. PMID:16822808.
- Barrett JC, Lee JC, Lees CW, Prescott NJ, Anderson CA, Phillips A, Wesley E, Parnell K, Zhang H, Drummond H, et al. Genome-wide association study of ulcerative colitis identifies three new susceptibility loci, including the HNF4A region. Nat Genet. 2009;41:1330–4. doi:10.1038/ng.483. PMID:19915572.
- Buisine MP, Desreumaux P, Debailleul V, Gambiez L, Geboes K, Ectors N, Delescaut MP, Degand P, Aubert JP, Colombel JF, et al. Abnormalities in mucin gene expression in Crohn's disease. Inflamm Bowel Dis 1999;5:24–32. doi:10.1097/00054725-199902000-00004. PMID:10028446.
- Braun A, Treede I, Gotthardt D, Tietje A, Zahn A, Ruhwald R, Schoenfeld U, Welsch T, Kienle P, Erben G, et al. Alterations of phospholipid concentration and species composition of the intestinal mucus barrier in ulcerative colitis: a clue to pathogenesis. Inflamm Bowel Dis. 2009;15:1705–20. doi:10.1002/ibd.20993. PMID:19504612.
- Wehkamp J, Salzman NH, Porter E, Nuding S, Weichenthal M, Petras RE, Shen B, Schaeffeler E, Schwab M, Linzmeier R, et al. Reduced Paneth cell α-defensins in ileal Crohn's disease. Proc Natl Acad Sci U S A. 2005;102:18129–34. doi:10.1073/pnas.0505256102. PMID:16330776.
- Kaser A, Lee AH, Franke A, Glickman JN, Zeissig S, Tilg H, Nieuwenhuis EE, Higgins DE, Schreiber S, Glimcher LH, et al. XBP1 links ER stress to intestinal inflammation and confers genetic risk for human inflammatory bowel disease. Cell. 2008;134:743–56. doi:10.1016/j.cell.2008.07.021. PMID:18775308.
- Neurath MF. Cytokines in inflammatory bowel disease. Nat Rev Immunol. 2014;14:329–42. doi:10.1038/nri3661. PMID:24751956.
- Mayne CG, Williams CB. Induced and natural regulatory T cells in the development of inflammatory bowel disease. Inflamm Bowel Dis. 2013;19:1772–88. doi:10.1097/MIB.0b013e318281f5a3. PMID:23656897.
- Peters CP, Mjosberg JM, Bernink JH, Spits H. Innate lymphoid cells in inflammatory bowel diseases. Immunology letters. 2016;172:124–31. doi:10.1016/j.imlet.2015.10.004. PMID:26470815.
- Catalan-Serra I, Sandvik AK, Bruland T, Andreu-Ballester JC. Gammadelta T Cells in Crohn's Disease: A New Player in the Disease Pathogenesis? Journal of Crohn's & colitis. 2017;11:1135–45.
- Danese S, Panes J. Development of drugs to target interactions between leukocytes and endothelial cells and treatment algorithms for inflammatory bowel diseases. Gastroenterology. 2014;147:981–9. doi:10.1053/j.gastro.2014.08.044. PMID:25220794.
- Gomollon F, Dignass A, Annese V, Tilg H, Van Assche G, Lindsay JO, Peyrin-Biroulet L, Cullen GJ, Daperno M, Kucharzik T, et al. 3rd european evidence-based consensus on the diagnosis and management of crohn's disease 2016: part 1: diagnosis and medical management. Journal of Crohn's & colitis. 2017;11:3–25. doi:10.1093/ecco-jcc/jjw168.
- Harbord M, Eliakim R, Bettenworth D, Karmiris K, Katsanos K, Kopylov U, Kucharzik T, Molnar T, Raine T, Sebastian S, et al. third european evidence-based consensus on diagnosis and management of ulcerative colitis. part 2: Current management. Journal of Crohn's & colitis. 2017;11:769–84. doi:10.1093/ecco-jcc/jjx009..
- Cohen BL, Sachar DB. Update on anti-tumor necrosis factor agents and other new drugs for inflammatory bowel disease. BMJ (Clinical research ed). 2017;357:j2505. doi:10.1136/bmj.j2505. PMID:28630047.
- Ding NS, Hart A, De Cruz P. Systematic review: predicting and optimising response to anti-TNF therapy in Crohn's disease – algorithm for practical management. Aliment Pharmacol Ther. 2016;43:30–51. doi:10.1111/apt.13445. PMID:26515897.
- Dulai PS, Thompson KD, Blunt HB, Dubinsky MC, Siegel CA. Risks of serious infection or lymphoma with anti-tumor necrosis factor therapy for pediatric inflammatory bowel disease: a systematic review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2014;12:1443–51; quiz e88-9. doi:10.1016/j.cgh.2014.01.021. PMID:24462626.
- Dulai PS, Siegel CA. The risk of malignancy associated with the use of biological agents in patients with inflammatory bowel disease. Gastroenterol Clin North Am. 2014;43:525–41. doi:10.1016/j.gtc.2014.05.010. PMID:25110257.
- Frolkis AD, Dykeman J, Negrón ME, deBruyn J, Jette N, Fiest KM, Frolkis T, Barkema HW, Rioux KP, Panaccione R, et al. Risk of Surgery for Inflammatory Bowel Diseases Has Decreased Over Time: A Systematic Review and Meta-analysis of Population-Based Studies. Gastroenterology. 2013;145:996–1006. doi:10.1053/j.gastro.2013.07.041. PMID:23896172.
- Gionchetti P, Dignass A, Danese S, Magro Dias FJ, Rogler G, Lakatos PL, Adamina M, Ardizzone S, Buskens CJ, Sebastian S, et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn's Disease 2016: Part 2: Surgical Management and Special Situations. Journal of Crohn's & colitis. 2017;11:135–49. doi:10.1093/ecco-jcc/jjw169..
- Trinchieri G, Pflanz S, Kastelein RA. The IL-12 Family of Heterodimeric Cytokines: New Players in the Regulation of T Cell Responses. Immunity. 2003;19:641–4. doi:10.1016/S1074-7613(03)00296-6. PMID:14614851.
- McGovern D, Powrie F. The IL23 axis plays a key role in the pathogenesis of IBD. Gut. 2007;56:1333–6. doi:10.1136/gut.2006.115402. PMID:17872562.
- Abraham C, Dulai PS, Vermeire S, Sandborn WJ. Lessons Learned From Trials Targeting Cytokine Pathways in Patients With Inflammatory Bowel Diseases. Gastroenterology. 2017;152:374–88.e4. doi:10.1053/j.gastro.2016.10.018. PMID:27780712.
- Vignali DAA, Kuchroo VK. IL-12 family cytokines: immunological playmakers. Nat Immunol. 2012;13:722. doi:10.1038/ni.2366. PMID:22814351.
- Yadav V, Varum F, Bravo R, Furrer E, Bojic D, Basit AW. Inflammatory bowel disease: exploring gut pathophysiology for novel therapeutic targets. Translational research : the journal of laboratory and clinical medicine. 2016;176:38–68. doi:10.1016/j.trsl.2016.04.009. PMID:27220087.
- Duerr RH, Taylor KD, Brant SR, Rioux JD, Silverberg MS, Daly MJ, Steinhart AH, Abraham C, Regueiro M, Griffiths A, et al. A Genome-Wide Association Study Identifies IL23R as an Inflammatory Bowel Disease Gene. Science. 2006;314:1461–3. doi:10.1126/science.1135245. PMID:17068223.
- Silverberg MS, Cho JH, Rioux JD, McGovern DP, Wu J, Annese V, Achkar JP, Goyette P, Scott R, Xu W, et al. Ulcerative colitis-risk loci on chromosomes 1p36 and 12q15 found by genome-wide association study. Nat Genet. 2009;41:216–20. doi:10.1038/ng.275. PMID:19122664.
- Pidasheva S, Trifari S, Phillips A, Hackney JA, Ma Y, Smith A, Sohn SJ, Spits H, Little RD, Behrens TW, et al. Functional Studies on the IBD Susceptibility Gene IL23R Implicate Reduced Receptor Function in the Protective Genetic Variant R381Q. PLOS ONE. 2011;6:e25038. doi:10.1371/journal.pone.0025038. PMID:22022372.
- Hueber W, Sands BE, Lewitzky S, Vandemeulebroecke M, Reinisch W, Higgins PD, Wehkamp J, Feagan BG, Yao MD, Karczewski M, et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn's disease: unexpected results of a randomised, double-blind placebo-controlled trial. Gut. 2012;61:1693–700. doi:10.1136/gutjnl-2011-301668. PMID:22595313.
- Targan SR, Feagan B, Vermeire S, Panaccione R, Melmed GY, Landers C, Li D, Russell C, Newmark R, Zhang N, et al. A Randomized, Double-Blind, Placebo-Controlled Phase 2 Study of Brodalumab in Patients With Moderate-to-Severe Crohn's Disease. Am J Gastroenterol. 2016;111:1599–607. doi:10.1038/ajg.2016.298. PMID:27481309.
- Lee Jacob S, Tato Cristina M, Joyce-Shaikh B, Gulen Muhammet F, Cayatte C, Chen Y, Blumenschein Wendy M, Judo M, Ayanoglu G, McClanahan Terrill K, et al. Interleukin-23-Independent IL-17 Production Regulates Intestinal Epithelial Permeability. Immunity. 2015;43:727–38. doi:10.1016/j.immuni.2015.09.003. PMID:26431948.
- Maloy KJ, Kullberg MC. IL-23 and Th17 cytokines in intestinal homeostasis. Mucosal Immunol. 2008;1:339. doi:10.1038/mi.2008.28. PMID:19079198.
- Aden K, Rehman A, Falk-Paulsen M, Secher T, Kuiper J, Tran F, Pfeuffer S, Sheibani-Tezerji R, Breuer A, Luzius A, et al. Epithelial IL-23R Signaling Licenses Protective IL-22 Responses in Intestinal Inflammation. Cell Rep. 2016;16:2208–18. doi:10.1016/j.celrep.2016.07.054. PMID:27524624.
- Macho-Fernandez E, Koroleva EP, Spencer CM, Tighe M, Torrado E, Cooper AM, Fu YX, Tumanov AV. Lymphotoxin beta receptor signaling limits mucosal damage through driving IL-23 production by epithelial cells. Mucosal Immunol. 2015;8:403–13. doi:10.1038/mi.2014.78. PMID:25183367.
- Cox JH, Kljavin NM, Ota N, Leonard J, Roose-Girma M, Diehl L, Ouyang W, Ghilardi N. Opposing consequences of IL-23 signaling mediated by innate and adaptive cells in chemically induced colitis in mice. Mucosal Immunol. 2012;5:99–109. doi:10.1038/mi.2011.54. PMID:22089030.
- Eken A, Singh AK, Treuting PM, Oukka M. IL-23R+ innate lymphoid cells induce colitis via interleukin-22-dependent mechanism. Mucosal Immunol. 2014;7:143–54. doi:10.1038/mi.2013.33. PMID:23715173.
- Sandborn WJ, Gasink C, Gao L-L, Blank MA, Johanns J, Guzzo C, Sands BE, Hanauer SB, Targan S, Rutgeerts P, et al. Ustekinumab Induction and Maintenance Therapy in Refractory Crohn's Disease. N Engl J Med. 2012;367:1519–28. doi:10.1056/NEJMoa1203572. PMID:23075178.
- Mannon PJ, Fuss IJ, Mayer L, Elson CO, Sandborn WJ, Present D, Dolin B, Goodman N, Groden C, Hornung RL, et al. Anti–Interleukin-12 Antibody for Active Crohn's Disease. N Engl J Med. 2004;351:2069–79. doi:10.1056/NEJMoa033402. PMID:15537905.
- Panaccione R, Sandborn WJ, Gordon GL, Lee SD, Safdi A, Sedghi S, Feagan BG, Hanauer S, Reinisch W, Valentine JF, et al. Briakinumab for treatment of Crohn's disease: results of a randomized trial. Inflamm Bowel Dis. 2015;21:1329–40. PMID:25989338.
- MacDonald JK, Nguyen TM, Khanna R, Timmer A. Anti-IL-12/23p40 antibodies for induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2016;11:Cd007572. PMID:27885650.
- Baker KF, Isaacs JD. Novel therapies for immune-mediated inflammatory diseases: What can we learn from their use in rheumatoid arthritis, spondyloarthritis, systemic lupus erythematosus, psoriasis, Crohn's disease and ulcerative colitis? Ann Rheum Dis. 2018;77:175–87. doi:10.1136/annrheumdis-2017-211555. PMID:28765121.
- Ryan C, Leonardi CL, Krueger JG, Kimball AB, Strober BE, Gordon KB, Langley RG, de Lemos JA, Daoud Y, Blankenship D, et al. Association between biologic therapies for chronic plaque psoriasis and cardiovascular events: a meta-analysis of randomized controlled trials. Jama. 2011;306:864–71. PMID:21862748.
- Tzellos T, Kyrgidis A, Trigoni A, Zouboulis CC. Association of ustekinumab and briakinumab with major adverse cardiovascular events: An appraisal of meta-analyses and industry sponsored pooled analyses to date. Dermato-endocrinology. 2012;4:320–3. doi:10.4161/derm.23100. PMID:23467502.
- Sands BE, Chen J, Feagan BG, Penney M, Rees WA, Danese S, Higgins PDR, Newbold P, Faggioni R, Patra K, et al. Efficacy and Safety of MEDI2070, an Antibody Against Interleukin 23, in Patients With Moderate to Severe Crohn's Disease: A Phase 2a Study. Gastroenterology. 2017;153:77–86.e6. doi:10.1053/j.gastro.2017.03.049. PMID:28390867.
- Feagan BG, Sandborn W, Panés J, Ferrante M, Louis E, D'Haens GR, Franchimont D, Kaser A, Dewit O, Seidler U, et al. 812a Efficacy and Safety of Induction Therapy With the Selective IL-23 Inhibitor BI 655066, in Patients With Moderate-to-Severe Crohn's Disease: Results of a Randomized, Double-Blind, Placebo-Controlled Phase II Study. Gastroenterology. 2016;150:S1266. doi:10.1016/S0016-5085(16)34278-0..
- Coskun M, Vermeire S, Nielsen OH. Novel Targeted Therapies for Inflammatory Bowel Disease. Trends in pharmacological sciences. 2017;38:127–42. doi:10.1016/j.tips.2016.10.014. PMID:27916280.
- Hunter CA, Jones SA. IL-6 as a keystone cytokine in health and disease. Nat Immunol. 2015;16:448–57. doi:10.1038/ni.3153. PMID:25898198.
- Tanaka T, Narazaki M, Ogata A, Kishimoto T. A new era for the treatment of inflammatory autoimmune diseases by interleukin-6 blockade strategy. Semin Immunol. 2014;26:88–96. doi:10.1016/j.smim.2014.01.009. PMID:24594001.
- Heinrich PC, Castell JV, Andus T. Interleukin-6 and the acute phase response. Biochem J. 1990;265:621–36. doi:10.1042/bj2650621. PMID:1689567.
- Calabrese LH, Rose-John S. IL-6 biology: implications for clinical targeting in rheumatic disease. Nat Rev Rheumatol. 2014;10:720. doi:10.1038/nrrheum.2014.127. PMID:25136784.
- Gross V, Andus T, Caesar I, Roth M, Scholmerich J. Evidence for continuous stimulation of interleukin-6 production in Crohn's disease. Gastroenterology 1992;102:514–9. doi:10.1016/0016-5085(92)90098-J. PMID:1370661.
- Korn T, Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 Cells. Annu Rev Immunol. 2009;27:485–517. doi:10.1146/annurev.immunol.021908.132710. PMID:19132915.
- Bettelli E, Carrier Y, Gao W, Korn T, Strom TB, Oukka M, Weiner HL, Kuchroo VK. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature. 2006;441:235–8. doi:10.1038/nature04753. PMID:16648838.
- Kimura A, Kishimoto T. IL-6: regulator of Treg/Th17 balance. Eur J Immunol. 2010;40:1830–5. doi:10.1002/eji.201040391. PMID:20583029.
- Wolf J, Rose-John S, Garbers C. Interleukin-6 and its receptors: a highly regulated and dynamic system. Cytokine. 2014;70:11–20. doi:10.1016/j.cyto.2014.05.024. PMID:24986424.
- Yamamoto M, Yoshizaki K, Kishimoto T, Ito H. IL-6 is required for the development of Th1 cell-mediated murine colitis. Journal of immunology (Baltimore, Md : 1950). 2000;164:4878–82. doi:10.4049/jimmunol.164.9.4878. PMID:10779797.
- Hosokawa T, Kusugami K, Ina K, Ando T, Shinoda M, Imada A, Ohsuga M, Sakai T, Matsuura T, Ito K, et al. Interleukin-6 and soluble interleukin-6 receptor in the colonic mucosa of inflammatory bowel disease. J Gastroenterol Hepatol. 1999;14:987–96. doi:10.1046/j.1440-1746.1999.01989.x. PMID:10530495.
- Louis E, Belaiche J, van Kemseke C, Franchimont D, de Groote D, Gueenen V, Mary JY. A high serum concentration of interleukin-6 is predictive of relapse in quiescent Crohn's disease. Eur J Gastroenterol Hepatol. 1997;9:939–44. doi:10.1097/00042737-199710000-00004..
- Ito H, Takazoe M, Fukuda Y, Hibi T, Kusugami K, Andoh A, Matsumoto T, Yamamura T, Azuma J, Nishimoto N, et al. A pilot randomized trial of a human anti-interleukin-6 receptor monoclonal antibody in active Crohn's disease. Gastroenterology. 2004;126:989–96; discussion 47. doi:10.1053/j.gastro.2004.01.012. PMID:15057738.
- Danese S, Vermeire S, Hellstern P, Panaccione R, Rogler G, Fraser G, Kohn A, Desreumaux P, Leong RW, Comer GM, et al. Randomised trial and open-label extension study of an anti-interleukin-6 antibody in Crohn's disease (ANDANTE I and II). Gut. 2017;1–9. doi:10.1136/gutjnl-2017-314562.
- Kuhn KA, Manieri NA, Liu T-C, Stappenbeck TS. IL-6 Stimulates Intestinal Epithelial Proliferation and Repair after Injury. PLOS ONE. 2014;9:e114195. doi:10.1371/journal.pone.0114195. PMID:25478789.
- Fleischmann R, Kremer J, Cush J, Schulze-Koops H, Connell CA, Bradley JD, Gruben D, Wallenstein GV, Zwillich SH, Kanik KS. Placebo-Controlled Trial of Tofacitinib Monotherapy in Rheumatoid Arthritis. N Engl J Med. 2012;367:495–507. doi:10.1056/NEJMoa1109071. PMID:22873530.
- Verstovsek S, Kantarjian H, Mesa RA, Pardanani AD, Cortes-Franco J, Thomas DA, Estrov Z, Fridman JS, Bradley EC, Erickson-Viitanen S, et al. Safety and Efficacy of INCB018424, a JAK1 and JAK2 Inhibitor, in Myelofibrosis. N Engl J Med. 2010;363:1117–27. doi:10.1056/NEJMoa1002028. PMID:20843246.
- Sandborn WJ, Ghosh S, Panes J, Vranic I, Su C, Rousell S, Niezychowski W. Tofacitinib, an Oral Janus Kinase Inhibitor, in Active Ulcerative Colitis. N Engl J Med. 2012;367:616–24. doi:10.1056/NEJMoa1112168. PMID:22894574.
- Sandborn WJ, Su C, Sands BE, D'Haens GR, Vermeire S, Schreiber S, Danese S, Feagan BG, Reinisch W, Niezychowski W, et al. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2017;376:1723–36. doi:10.1056/NEJMoa1606910. PMID:28467869.
- Coskun M, Salem M, Pedersen J, Nielsen OH. Involvement of JAK/STAT signaling in the pathogenesis of inflammatory bowel disease. Pharmacol Res. 2013;76:1–8. doi:10.1016/j.phrs.2013.06.007. PMID:23827161.
- Ghoreschi K, Laurence A, O'Shea JJ. Janus kinases in immune cell signaling. Immunol Rev. 2009;228:273–87. doi:10.1111/j.1600-065X.2008.00754.x. PMID:19290934.
- O'Shea JJ, Plenge R. JAK and STAT signaling molecules in immunoregulation and immune-mediated disease. Immunity. 2012;36:542–50. doi:10.1016/j.immuni.2012.03.014. PMID:22520847.
- Sandborn WJ, Ghosh S, Panes J, Vranic I, Wang W, Niezychowski W. A phase 2 study of tofacitinib, an oral Janus kinase inhibitor, in patients with Crohn's disease. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2014;12:1485–93.e2. doi:10.1016/j.cgh.2014.01.029. PMID:24480677.
- Panés J, Sandborn WJ, Schreiber S, Sands BE, Vermeire S, D'Haens G, Panaccione R, Higgins PDR, Colombel J-F, Feagan BG, et al. Tofacitinib for induction and maintenance therapy of Crohn's disease: results of two phase IIb randomised placebo-controlled trials. Gut. 2017;66(6):1049–1059. doi:10.1136/gutjnl-2016-312735.
- Vermeire S, Schreiber S, Petryka R, Kuehbacher T, Hebuterne X, Roblin X, Klopocka M, Goldis A, Wisniewska-Jarosinska M, Baranovsky A, et al. Clinical remission in patients with moderate-to-severe Crohn's disease treated with filgotinib (the FITZROY study): results from a phase 2, double-blind, randomised, placebo-controlled trial. Lancet. 2017;389:266–75. doi:10.1016/S0140-6736(16)32537-5. PMID:27988142.
- Comi G, Jeffery D, Kappos L, Montalban X, Boyko A, Rocca MA, Filippi M. Placebo-Controlled Trial of Oral Laquinimod for Multiple Sclerosis. N Engl J Med. 2012;366:1000–9. doi:10.1056/NEJMoa1104318. PMID:22417253.
- Vollmer TL, Sorensen PS, Selmaj K, Zipp F, Havrdova E, Cohen JA, Sasson N, Gilgun-Sherki Y, Arnold DL. A randomized placebo-controlled phase III trial of oral laquinimod for multiple sclerosis. J Neurol. 2014;261:773–83. doi:10.1007/s00415-014-7264-4. PMID:24535134.
- Jayne D, Appel G, Chan TM, Barkay H, Weiss R, Wofsy D. LB0003 A Randomized Controlled Study of Laquinimod in Active Lupus Nephritis Patients in Combination with Standard of Care. Ann Rheum Dis. 2013;72:A164–A. doi:10.1136/annrheumdis-2013-eular.528..
- Bruck W, Wegner C. Insight into the mechanism of laquinimod action. J Neurol Sci. 2011;306:173–9. doi:10.1016/j.jns.2011.02.019. PMID:21429524.
- Thöne J, Linker RA. Laquinimod in the treatment of multiple sclerosis: a review of the data so far. Drug Design, Development and Therapy. 2016;10:1111–8. doi:10.2147/DDDT.S55308. PMID:27042003.
- D'Haens G, Sandborn WJ, Colombel JF, Rutgeerts P, Brown K, Barkay H, Sakov A, Haviv A, Feagan BG. Laquinimod for Crohn's Disease I. A phase II study of laquinimod in Crohn's disease. Gut. 2015;64:1227–35. doi:10.1136/gutjnl-2014-307118. PMID:25281416.
- Gorelik L, Flavell RA. Transforming growth factor-beta in T-cell biology. Nat Rev Immunol. 2002;2:46–53. doi:10.1038/nri704. PMID:11905837.
- Letterio JJ, Roberts AB. Regulation of immune responses by TGF-beta. Annu Rev Immunol. 1998;16:137–61. doi:10.1146/annurev.immunol.16.1.137. PMID:9597127.
- Sedda S, Marafini I, Dinallo V, Di Fusco D, Monteleone G. The TGF-beta/Smad System in IBD Pathogenesis. Inflamm Bowel Dis. 2015;21:2921–5. doi:10.1097/MIB.0000000000000542. PMID:26230862.
- Heldin CH, Miyazono K, ten Dijke P. TGF-beta signalling from cell membrane to nucleus through SMAD proteins. Nature. 1997;390:465–71. doi:10.1038/37284. PMID:9393997.
- Derynck R, Zhang Y, Feng XH. Smads: transcriptional activators of TGF-beta responses. Cell 1998;95:737–40. doi:10.1016/S0092-8674(00)81696-7. PMID:9865691.
- Monteleone G, Del Vecchio Blanco G, Monteleone I, Fina D, Caruso R, Gioia V, Ballerini S, Federici G, Bernardini S, Pallone F, et al. Post-transcriptional regulation of Smad7 in the gut of patients with inflammatory bowel disease. Gastroenterology. 2005;129:1420–9. doi:10.1053/j.gastro.2005.09.005. PMID:16285943.
- Monteleone G, Kumberova A, Croft NM, McKenzie C, Steer HW, MacDonald TT. Blocking Smad7 restores TGF-beta1 signaling in chronic inflammatory bowel disease. J Clin Invest. 2001;108:601–9. doi:10.1172/JCI12821. PMID:11518734.
- Monteleone G, Neurath MF, Ardizzone S, Di Sabatino A, Fantini MC, Castiglione F, Scribano ML, Armuzzi A, Caprioli F, Sturniolo GC, et al. Mongersen, an Oral SMAD7 Antisense Oligonucleotide, and Crohn's Disease. N Engl J Med. 2015;372:1104–13. doi:10.1056/NEJMoa1407250. PMID:25785968.
- Monteleone G, Fantini MC, Onali S, Zorzi F, Sancesario G, Bernardini S, Calabrese E, Viti F, Monteleone I, Biancone L, et al. Phase I clinical trial of Smad7 knockdown using antisense oligonucleotide in patients with active Crohn's disease. Molecular therapy : the journal of the American Society of Gene Therapy. 2012;20:870–6. doi:10.1038/mt.2011.290. PMID:22252452.
- Feagan B, Sands B, Rossiter G, Li X, Usiskin K, Zhan X, Colombel JF. PD-008 A Study of Oral Mongersen (GED-0301) on Endoscopy and Clinical Activity (Stool Frequency and Abdominal Pain) in Crohn's Disease. Inflamm Bowel Dis. 2017;23:S8–S.
- Li C, Kuemmerle JF. Mechanisms that mediate the development of fibrosis in patients with Crohn's disease. Inflamm Bowel Dis. 2014;20:1250–8. doi:10.1097/MIB.0000000000000043. PMID:24831560.
- Zorzi F, Calabrese E, Monteleone I, Fantini M, Onali S, Biancone L, Pallone F, Monteleone G. A phase 1 open-label trial shows that smad7 antisense oligonucleotide (GED0301) does not increase the risk of small bowel strictures in Crohn's disease. Aliment Pharmacol Ther. 2012;36:850–7. doi:10.1111/apt.12051. PMID:22971085.
- Lobaton T, Vermeire S, Van Assche G, Rutgeerts P. Review article: anti-adhesion therapies for inflammatory bowel disease. Aliment Pharmacol Ther. 2014;39:579–94. doi:10.1111/apt.12639. PMID:24479980.
- Jones SC, Banks RE, Haidar A, Gearing AJ, Hemingway IK, Ibbotson SH, Dixon MF, Axon AT. Adhesion molecules in inflammatory bowel disease. Gut 1995;36:724–30. doi:10.1136/gut.36.5.724. PMID:7541009.
- Souza HS, Elia CCS, Spencer J, MacDonald TT. Expression of lymphocyte-endothelial receptor-ligand pairs, α4β7/MAdCAM-1 and OX40/OX40 ligand in the colon and jejunum of patients with inflammatory bowel disease. Gut. 1999;45:856–63. doi:10.1136/gut.45.6.856. PMID:10562584.
- Oshima T, Jordan P, Grisham MB, Alexander JS, Jennings M, Sasaki M, Manas K. TNF-alpha induced endothelial MAdCAM-1 expression is regulated by exogenous, not endogenous nitric oxide. BMC Gastroenterol. 2001;1:5. doi:10.1186/1471-230X-1-5. PMID:11481030.
- Yacyshyn BR, Chey WY, Goff J, Salzberg B, Baerg R, Buchman AL, Tami J, Yu R, Gibiansky E, Shanahan WR. Double blind, placebo controlled trial of the remission inducing and steroid sparing properties of an ICAM-1 antisense oligodeoxynucleotide, alicaforsen (ISIS 2302), in active steroid dependent Crohn's disease. Gut. 2002;51:30–6. doi:10.1136/gut.51.1.30. PMID:12077088.
- Vegter S, Tolley K, Wilson Waterworth T, Jones H, Jones S, Jewell D. Meta-analysis using individual patient data: efficacy and durability of topical alicaforsen for the treatment of active ulcerative colitis. Aliment Pharmacol Ther. 2013;38:284–93. doi:10.1111/apt.12369..
- Jairath V, Khanna R, Feagan BG. Alicaforsen for the treatment of inflammatory bowel disease. Expert opinion on investigational drugs. 2017;26:991–7. doi:10.1080/13543784.2017.1349753. PMID:28670932.
- Mora JR, Bono MR, Manjunath N, Weninger W, Cavanagh LL, Rosemblatt M, von Andrian UH. Selective imprinting of gut-homing T cells by Peyer's patch dendritic cells. Nature. 2003;424:88–93. doi:10.1038/nature01726. PMID:12840763.
- Briskin M, Winsor-Hines D, Shyjan A, Cochran N, Bloom S, Wilson J, McEvoy LM, Butcher EC, Kassam N, Mackay CR, et al. Human mucosal addressin cell adhesion molecule-1 is preferentially expressed in intestinal tract and associated lymphoid tissue. Am J Pathol 1997;151:97–110. PMID:9212736.
- Ghosh S, Panaccione R. Anti-adhesion molecule therapy for inflammatory bowel disease. Ther Adv Gastroenterol. 2010;3:239–58. doi:10.1177/1756283X10373176. PMID:21180606.
- Miller DH, Khan OA, Sheremata WA, Blumhardt LD, Rice GPA, Libonati MA, Willmer-Hulme AJ, Dalton CM, Miszkiel KA, O'Connor PW. A Controlled Trial of Natalizumab for Relapsing Multiple Sclerosis. N Engl J Med. 2003;348:15–23. doi:10.1056/NEJMoa020696. PMID:12510038.
- Sandborn WJ, Colombel JF, Enns R, Feagan BG, Hanauer SB, Lawrance IC, Panaccione R, Sanders M, Schreiber S, Targan S, et al. Natalizumab Induction and Maintenance Therapy for Crohn's Disease. N Engl J Med. 2005;353:1912–25. doi:10.1056/NEJMoa043335. PMID:16267322.
- Targan SR, Feagan BG, Fedorak RN, Lashner BA, Panaccione R, Present DH, Spehlmann ME, Rutgeerts PJ, Tulassay Z, Volfova M, et al. Natalizumab for the treatment of active Crohn's disease: results of the ENCORE Trial. Gastroenterology. 2007;132:1672–83. doi:10.1053/j.gastro.2007.03.024. PMID:17484865.
- Pagnini C, Arseneau KO, Cominelli F. Natalizumab in the treatment of Crohn's disease patients. Expert opinion on biological therapy. 2017;17:1433–8. PMID:28832222.
- Yoshimura N, Watanabe M, Motoya S, Tominaga K, Matsuoka K, Iwakiri R, Watanabe K, Hibi T. Safety and Efficacy of AJM300, an Oral Antagonist of alpha4 Integrin, in Induction Therapy for Patients With Active Ulcerative Colitis. Gastroenterology. 2015;149:1775–83.e2. doi:10.1053/j.gastro.2015.08.044. PMID:26327130.
- Feagan BG, Rutgeerts P, Sands BE, Hanauer S, Colombel J-F, Sandborn WJ, Van Assche G, Axler J, Kim H-J, Danese S, et al. Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2013;369:699–710. doi:10.1056/NEJMoa1215734. PMID:23964932.
- Sandborn WJ, Feagan BG, Rutgeerts P, Hanauer S, Colombel J-F, Sands BE, Lukas M, Fedorak RN, Lee S, Bressler B, et al. Vedolizumab as Induction and Maintenance Therapy for Crohn's Disease. N Engl J Med. 2013;369:711–21. doi:10.1056/NEJMoa1215739. PMID:23964933.
- Stallmach A, Langbein C, Atreya R, Bruns T, Dignass A, Ende K, Hampe J, Hartmann F, Neurath MF, Maul J, et al. Vedolizumab provides clinical benefit over 1 year in patients with active inflammatory bowel disease – a prospective multicenter observational study. Aliment Pharmacol Ther. 2016;44(11–12):1199–1212. doi:10.1111/apt.13813.
- Loftus EV, Jr., Colombel JF, Feagan BG, Vermeire S, Sandborn WJ, Sands BE, Danese S, D'Haens GR, Kaser A, Panaccione R, et al. Long-term Efficacy of Vedolizumab for Ulcerative Colitis. Journal of Crohn's & colitis. 2017;11:400–11.
- Vermeire S, Loftus EV, Jr., Colombel JF, Feagan BG, Sandborn WJ, Sands BE, Danese S, D'Haens GR, Kaser A, Panaccione R, et al. Long-term Efficacy of Vedolizumab for Crohn's Disease. Journal of Crohn's & colitis. 2017;11:412–24.
- Colombel JF, Sands BE, Rutgeerts P, Sandborn W, Danese S, D'Haens G, Panaccione R, Loftus EV, Jr., Sankoh S, Fox I, et al. The safety of vedolizumab for ulcerative colitis and Crohn's disease. Gut. 2016.
- Sandborn WJ, Cyrille M, Hansen MB, Feagan BG, Loftus JEV, Rogler G, Vermeire S, Cruz ML, Yang J, Sullivan BA, et al. OP034 Efficacy and safety of abrilumab in subjects with moderate to severe ulcerative colitis: results of a phase 2b, randomised, double-blind, multiple-dose, placebo-controlled study. Journal of Crohn's and Colitis. 2017;11:S21–S2. doi:10.1093/ecco-jcc/jjx002.033..
- Sandborn WJ, Cyrille M, Berner Hansen M, Feagan BG, Loftus JEV, Vermeire S, Cruz ML, Mo M, Sullivan BA, Reinisch W. OP035 Efficacy and safety of abrilumab (AMG 181/MEDI 7183) therapy for moderate to severe Crohn's disease. Journal of Crohn's and Colitis. 2017;11:S22–S3. doi:10.1093/ecco-jcc/jjx002.034..
- Sandborn WJ, Lee SD, Tarabar D, Louis E, Klopocka M, Klaus J, Reinisch W, Hebuterne X, Park DI, Schreiber S, et al. Phase II evaluation of anti-MAdCAM antibody PF-00547659 in the treatment of Crohn's disease: report of the OPERA study. Gut. 2017;1–12.
- Vermeire S, Sandborn WJ, Danese S, Hebuterne X, Salzberg BA, Klopocka M, Tarabar D, Vanasek T, Gregus M, Hellstern PA, et al. Anti-MAdCAM antibody (PF-00547659) for ulcerative colitis (TURANDOT): a phase 2, randomised, double-blind, placebo-controlled trial. Lancet. 2017;390:135–44. doi:10.1016/S0140-6736(17)30930-3. PMID:28527704.
- Vermeire S, O'Byrne S, Keir M, Williams M, Lu TT, Mansfield JC, Lamb CA, Feagan BG, Panes J, Salas A, et al. Etrolizumab as induction therapy for ulcerative colitis: a randomised, controlled, phase 2 trial. Lancet. 2014;384:309–18. doi:10.1016/S0140-6736(14)60661-9..
- Argollo M, Fiorino G, Hindryckx P, Peyrin-Biroulet L, Danese S. Novel therapeutic targets for inflammatory bowel disease. J Autoimmun. 2017;85:103–16. doi:10.1016/j.jaut.2017.07.004. PMID:28711286.
- Sandborn WJ, Feagan BG, Wolf DC, D'Haens G, Vermeire S, Hanauer SB, Ghosh S, Smith H, Cravets M, Frohna PA, et al. Ozanimod Induction and Maintenance Treatment for Ulcerative Colitis. N Engl J Med. 2016;374:1754–62. doi:10.1056/NEJMoa1513248. PMID:27144850.
- Spiegel S, Milstien S. The outs and the ins of sphingosine-1-phosphate in immunity. Nat Rev Immunol. 2011;11:403–15. doi:10.1038/nri2974. PMID:21546914.
- Fyrst H, Saba JD. An update on sphingosine-1-phosphate and other sphingolipid mediators. Nat Chem Biol. 2010;6:489–97. doi:10.1038/nchembio.392. PMID:20559316.
- Nielsen OH, Li Y, Johansson-Lindbom B, Coskun M. Sphingosine-1-Phosphate Signaling in Inflammatory Bowel Disease. Trends Mol Med. 2017;23:362–74. doi:10.1016/j.molmed.2017.02.002. PMID:28283249.
- Mandala S, Hajdu R, Bergstrom J, Quackenbush E, Xie J, Milligan J, Thornton R, Shei GJ, Card D, Keohane C, et al. Alteration of lymphocyte trafficking by sphingosine-1-phosphate receptor agonists. Science. 2002;296:346–9. doi:10.1126/science.1070238. PMID:11923495.
- Pappu R, Schwab SR, Cornelissen I, Pereira JP, Regard JB, Xu Y, Camerer E, Zheng YW, Huang Y, Cyster JG, et al. Promotion of lymphocyte egress into blood and lymph by distinct sources of sphingosine-1-phosphate. Science. 2007;316:295–8. doi:10.1126/science.1139221. PMID:17363629.
- Thangada S, Khanna KM, Blaho VA, Oo ML, Im DS, Guo C, Lefrancois L, Hla T. Cell-surface residence of sphingosine 1-phosphate receptor 1 on lymphocytes determines lymphocyte egress kinetics. J Exp Med. 2010;207:1475–83. doi:10.1084/jem.20091343. PMID:20584883.
- Cohen JA, Arnold DL, Comi G, Bar-Or A, Gujrathi S, Hartung JP, Cravets M, Olson A, Frohna PA, Selmaj KW. Safety and efficacy of the selective sphingosine 1-phosphate receptor modulator ozanimod in relapsing multiple sclerosis (RADIANCE): a randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2016;15:373–81. doi:10.1016/S1474-4422(16)00018-1. PMID:26879276.
- Mao F, Tu Q, Wang L, Chu F, Li X, Li HS, Xu W. Mesenchymal stem cells and their therapeutic applications in inflammatory bowel disease. Oncotarget. 2017;8:38008–21. doi:10.18632/oncotarget.16682. PMID:28402942.
- Gregoire C, Lechanteur C, Briquet A, Baudoux E, Baron F, Louis E, Beguin Y. Review article: mesenchymal stromal cell therapy for inflammatory bowel diseases. Aliment Pharmacol Ther. 2017;45:205–21. doi:10.1111/apt.13864. PMID:27878827.
- Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A, Prockop D, Horwitz E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006;8:315–7. doi:10.1080/14653240600855905. PMID:16923606.
- Li L, Liu S, Xu Y, Zhang A, Jiang J, Tan W, Xing J, Feng G, Liu H, Huo F, et al. Human umbilical cord-derived mesenchymal stem cells downregulate inflammatory responses by shifting the Treg/Th17 profile in experimental colitis. Pharmacology. 2013;92:257–64. doi:10.1159/000354883. PMID:24280970.
- Choi YS, Jeong JA, Lim DS. Mesenchymal stem cell-mediated immature dendritic cells induce regulatory T cell-based immunosuppressive effect. Immunol Invest. 2012;41:214–29. doi:10.3109/08820139.2011.619022. PMID:22017637.
- Gonzalez MA, Gonzalez-Rey E, Rico L, Buscher D, Delgado M. Adipose-derived mesenchymal stem cells alleviate experimental colitis by inhibiting inflammatory and autoimmune responses. Gastroenterology. 2009;136:978–89. doi:10.1053/j.gastro.2008.11.041. PMID:19135996.
- He XW, He XS, Lian L, Wu XJ, Lan P. Systemic infusion of bone marrow-derived mesenchymal stem cells for treatment of experimental colitis in mice. Dig Dis Sci. 2012;57:3136–44. doi:10.1007/s10620-012-2290-5. PMID:22752635.
- Liang L, Dong C, Chen X, Fang Z, Xu J, Liu M, Zhang X, Gu DS, Wang D, Du W, et al. Human umbilical cord mesenchymal stem cells ameliorate mice trinitrobenzene sulfonic acid (TNBS)-induced colitis. Cell Transplant. 2011;20:1395–408. doi:10.3727/096368910X557245. PMID:21396175.
- Gonzalez-Rey E, Anderson P, Gonzalez MA, Rico L, Buscher D, Delgado M. Human adult stem cells derived from adipose tissue protect against experimental colitis and sepsis. Gut. 2009;58:929–39. doi:10.1136/gut.2008.168534. PMID:19136511.
- Devine SM, Cobbs C, Jennings M, Bartholomew A, Hoffman R. Mesenchymal stem cells distribute to a wide range of tissues following systemic infusion into nonhuman primates. Blood. 2003;101:2999–3001. doi:10.1182/blood-2002-06-1830. PMID:12480709.
- Hayashi Y, Tsuji S, Tsujii M, Nishida T, Ishii S, Iijima H, Nakamura T, Eguchi H, Miyoshi E, Hayashi N, et al. Topical implantation of mesenchymal stem cells has beneficial effects on healing of experimental colitis in rats. J Pharmacol Exp Ther. 2008;326:523–31. doi:10.1124/jpet.108.137083. PMID:18448866.
- Kachgal S, Putnam AJ. Mesenchymal stem cells from adipose and bone marrow promote angiogenesis via distinct cytokine and protease expression mechanisms. Angiogenesis. 2011;14:47–59. doi:10.1007/s10456-010-9194-9. PMID:21104120.
- Akiyama K, Chen C, Wang D, Xu X, Qu C, Yamaza T, Cai T, Chen W, Sun L, Shi S. Mesenchymal-stem-cell-induced immunoregulation involves FAS-ligand-/FAS-mediated T cell apoptosis. Cell Stem Cell. 2012;10:544–55. doi:10.1016/j.stem.2012.03.007. PMID:22542159.
- Yabana T, Arimura Y, Tanaka H, Goto A, Hosokawa M, Nagaishi K, Yamashita K, Yamamoto H, Adachi Y, Sasaki Y, et al. Enhancing epithelial engraftment of rat mesenchymal stem cells restores epithelial barrier integrity. J Pathol. 2009;218:350–9. doi:10.1002/path.2535. PMID:19291714.
- Dave M, Mehta K, Luther J, Baruah A, Dietz AB, Faubion WA, Jr. Mesenchymal Stem Cell Therapy for Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. Inflamm Bowel Dis. 2015;21:2696–707. doi:10.1097/MIB.0000000000000543. PMID:26230863.
- Onken J, Gallup D, Hanson J, Pandak M, Custer L. Successful outpatient treatment of refractory Crohn's disease using adult mesenchymal stem cells. Abstract 121. American College of Gastroenterology Conference. Las Vegas, NV, 2006.
- Lazebnik LB, Konopliannikov AG, Kniazev OV, Parfenov AI, Tsaregorodtseva TM, Ruchkina IN, Khomeriki SG, Rogozina VA, Konopliannikova OA. [Use of allogeneic mesenchymal stem cells in the treatment of intestinal inflammatory diseases]. Terapevticheskii arkhiv. 2010;82:38–43. PMID:20387674.
- Liang J, Zhang H, Wang D, Feng X, Wang H, Hua B, Liu B, Sun L. Allogeneic mesenchymal stem cell transplantation in seven patients with refractory inflammatory bowel disease. Gut. 2012;61:468–9. doi:10.1136/gutjnl-2011-300083. PMID:21617158.
- Forbes GM, Sturm MJ, Leong RW, Sparrow MP, Segarajasingam D, Cummins AG, Phillips M, Herrmann RP. A phase 2 study of allogeneic mesenchymal stromal cells for luminal Crohn's disease refractory to biologic therapy. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2014;12:64–71. doi:10.1016/j.cgh.2013.06.021. PMID:23872668.
- Knyazev O, Kagramanova A, Churikova A, Konoplyannikov A, Khomeriki S, Parfenov A, Ruchkina I. P575. The use of mesenchymal stromal cells in order to achieve deep (biological) remission of Ulcerative Colitis. Journal of Crohn's and Colitis. 2015;9:S367–S8. doi:10.1093/ecco-jcc/jju027.693..
- Knyazev O, Fadeeva N, Kagramanova A, Shcherbakov P, Ruchkina I, Parfenov A, Konoplyannikov A. P485. The combined of mesenchymal stem cells and infliximab reduces the recurrence rate of Crohn's disease. Journal of Crohn's and Colitis. 2016;10:S346–S.
- Lalu MM, McIntyre L, Pugliese C, Fergusson D, Winston BW, Marshall JC, Granton J, Stewart DJ. Safety of Cell Therapy with Mesenchymal Stromal Cells (SafeCell): A Systematic Review and Meta-Analysis of Clinical Trials. PLOS ONE. 2012;7:e47559. doi:10.1371/journal.pone.0047559. PMID:23133515.
- Duijvestein M, Vos AC, Roelofs H, Wildenberg ME, Wendrich BB, Verspaget HW, Kooy-Winkelaar EM, Koning F, Zwaginga JJ, Fidder HH, et al. Autologous bone marrow-derived mesenchymal stromal cell treatment for refractory luminal Crohn's disease: results of a phase I study. Gut. 2010;59:1662–9. doi:10.1136/gut.2010.215152. PMID:20921206.
- Dhere T, Copland I, Garcia M, Chiang KY, Chinnadurai R, Prasad M, Galipeau J, Kugathasan S. The safety of autologous and metabolically fit bone marrow mesenchymal stromal cells in medically refractory Crohn's disease – a phase 1 trial with three doses. Aliment Pharmacol Ther. 2016;44:471–81. doi:10.1111/apt.13717. PMID:27385373.
- Dave M, Jaiswal P, Cominelli F. Mesenchymal stem/stromal cell therapy for inflammatory bowel disease: an updated review with maintenance of remission. Curr Opin Gastroenterol. 2017;33:59–68. doi:10.1097/MOG.0000000000000327. PMID:28134690.
- Fantini MC, Monteleone G. Update on the Therapeutic Efficacy of Tregs in IBD: Thumbs up or Thumbs down? Inflamm Bowel Dis. 2017;23:1682–8. doi:10.1097/MIB.0000000000001272. PMID:28906289.
- Elinav E, Waks T, Eshhar Z. Redirection of regulatory T cells with predetermined specificity for the treatment of experimental colitis in mice. Gastroenterology. 2008;134:2014–24. doi:10.1053/j.gastro.2008.02.060. PMID:18424268.
- Huber S, Schramm C, Lehr HA, Mann A, Schmitt S, Becker C, Protschka M, Galle PR, Neurath MF, Blessing M. Cutting edge: TGF-beta signaling is required for the in vivo expansion and immunosuppressive capacity of regulatory CD4+CD25+ T cells. Journal of immunology (Baltimore, Md : 1950). 2004;173:6526–31. doi:10.4049/jimmunol.173.11.6526. PMID:15557141.
- Maul J, Loddenkemper C, Mundt P, Berg E, Giese T, Stallmach A, Zeitz M, Duchmann R. Peripheral and intestinal regulatory CD4+ CD25(high) T cells in inflammatory bowel disease. Gastroenterology. 2005;128:1868–78. doi:10.1053/j.gastro.2005.03.043. PMID:15940622.
- Saruta M, Yu QT, Fleshner PR, Mantel PY, Schmidt-Weber CB, Banham AH, Papadakis KA. Characterization of FOXP3+CD4+ regulatory T cells in Crohn's disease. Clinical immunology (Orlando, Fla). 2007;125:281–90. doi:10.1016/j.clim.2007.08.003. PMID:17897887.
- Takahashi M, Nakamura K, Honda K, Kitamura Y, Mizutani T, Araki Y, Kabemura T, Chijiiwa Y, Harada N, Nawata H. An inverse correlation of human peripheral blood regulatory T cell frequency with the disease activity of ulcerative colitis. Dig Dis Sci. 2006;51:677–86. doi:10.1007/s10620-006-3191-2. PMID:16614988.
- Fantini MC, Rizzo A, Fina D, Caruso R, Sarra M, Stolfi C, Becker C, Macdonald TT, Pallone F, Neurath MF, et al. Smad7 controls resistance of colitogenic T cells to regulatory T cell-mediated suppression. Gastroenterology. 2009;136:1308–16, e1-3. doi:10.1053/j.gastro.2008.12.053. PMID:19192480.
- Trzonkowski P, Bieniaszewska M, Juscinska J, Dobyszuk A, Krzystyniak A, Marek N, Mysliwska J, Hellmann A. First-in-man clinical results of the treatment of patients with graft versus host disease with human ex vivo expanded CD4+CD25+CD127- T regulatory cells. Clinical immunology (Orlando, Fla). 2009;133:22–6. doi:10.1016/j.clim.2009.06.001. PMID:19559653.
- Marek-Trzonkowska N, Mysliwiec M, Dobyszuk A, Grabowska M, Techmanska I, Juscinska J, Wujtewicz MA, Witkowski P, Mlynarski W, Balcerska A, et al. Administration of CD4+CD25highCD127- regulatory T cells preserves beta-cell function in type 1 diabetes in children. Diabetes Care. 2012;35:1817–20. doi:10.2337/dc12-0038. PMID:22723342.
- Desreumaux P, Foussat A, Allez M, Beaugerie L, Hebuterne X, Bouhnik Y, Nachury M, Brun V, Bastian H, Belmonte N, et al. Safety and efficacy of antigen-specific regulatory T-cell therapy for patients with refractory Crohn's disease. Gastroenterology. 2012;143:1207–17.e1-2. doi:10.1053/j.gastro.2012.07.116. PMID:22885333.
- Canavan JB, Scotta C, Vossenkamper A, Goldberg R, Elder MJ, Shoval I, Marks E, Stolarczyk E, Lo JW, Powell N, et al. Developing in vitro expanded CD45RA+ regulatory T cells as an adoptive cell therapy for Crohn's disease. Gut. 2016;65:584–94. doi:10.1136/gutjnl-2014-306919. PMID:25715355.
- Inagaki-Ohara K, Chinen T, Matsuzaki G, Sasaki A, Sakamoto Y, Hiromatsu K, Nakamura-Uchiyama F, Nawa Y, Yoshimura A. Mucosal T cells bearing TCRgammadelta play a protective role in intestinal inflammation. Journal of immunology (Baltimore, Md : 1950). 2004;173:1390–8. doi:10.4049/jimmunol.173.2.1390. PMID:15240735.
- Hoffmann JC, Pawlowski NN, Grollich K, Loddenkemper C, Zeitz M, Kuhl AA. Gammadelta T lymphocytes: a new type of regulatory T cells suppressing murine 2,4,6-trinitrobenzene sulphonic acid (TNBS)-induced colitis. Int J Colorectal Dis. 2008;23:909–20.
- Fisher JP, Heuijerjans J, Yan M, Gustafsson K, Anderson J. gammadelta T cells for cancer immunotherapy: A systematic review of clinical trials. Oncoimmunology. 2014;3:e27572. doi:10.4161/onci.27572. PMID:24734216.
- Gallo A, Passaro G, Gasbarrini A, Landolfi R, Montalto M. Modulation of microbiota as treatment for intestinal inflammatory disorders: An uptodate. World J Gastroenterol. 2016;22:7186–202. doi:10.3748/wjg.v22.i32.7186. PMID:27621567.
- Narula N, Kassam Z, Yuan Y, Colombel JF, Ponsioen C, Reinisch W, Moayyedi P. Systematic Review and Meta-analysis: Fecal Microbiota Transplantation for Treatment of Active Ulcerative Colitis. Inflamm Bowel Dis. 2017;23:1702–9. doi:10.1097/MIB.0000000000001228. PMID:28906291.
- Arnold GL, Beaves MR, Pryjdun VO, Mook WJ. Preliminary study of ciprofloxacin in active Crohn's disease. Inflamm Bowel Dis. 2002;8:10–5. doi:10.1097/00054725-200201000-00002. PMID:11837933.
- Sutherland L, Singleton J, Sessions J, Hanauer S, Krawitt E, Rankin G, Summers R, Mekhjian H, Greenberger N, Kelly M, et al. Double blind, placebo controlled trial of metronidazole in Crohn's disease. Gut 1991;32:1071–5. doi:10.1136/gut.32.9.1071. PMID:1916494.
- Prantera C, Zannoni F, Scribano ML, Berto E, Andreoli A, Kohn A, Luzi C. An antibiotic regimen for the treatment of active Crohn's disease: a randomized, controlled clinical trial of metronidazole plus ciprofloxacin. Am J Gastroenterol 1996;91:328–32. PMID:8607501.
- Prantera C, Lochs H, Grimaldi M, Danese S, Scribano ML, Gionchetti P. Rifaximin-extended intestinal release induces remission in patients with moderately active Crohn's disease. Gastroenterology. 2012;142:473–81.e4. doi:10.1053/j.gastro.2011.11.032. PMID:22155172.
- Sandborn WJ, Elliott DE, Weinstock J, Summers RW, Landry-Wheeler A, Silver N, Harnett MD, Hanauer SB. Randomised clinical trial: the safety and tolerability of Trichuris suis ova in patients with Crohn's disease. Aliment Pharmacol Ther. 2013;38:255–63. doi:10.1111/apt.12366. PMID:23730956.
- Weinstock JV. Helminths and mucosal immune modulation. Ann N Y Acad Sci. 2006;1072:356–64. doi:10.1196/annals.1326.033. PMID:17057216.
- Wong C, Harris PJ, Ferguson LR. Potential Benefits of Dietary Fibre Intervention in Inflammatory Bowel Disease. Int J Mol Sci. 2016;17:919. doi:10.3390/ijms17060919..
- Nie Y, Lin Q, Luo F. Effects of Non-Starch Polysaccharides on Inflammatory Bowel Disease. Int J Mol Sci. 2017;18:1372. doi:10.3390/ijms18071372.
- Mitsuyama K, Saiki T, Kanauchi O, Iwanaga T, Tomiyasu N, Nishiyama T, Tateishi H, Shirachi A, Ide M, Suzuki A, et al. Treatment of ulcerative colitis with germinated barley foodstuff feeding: a pilot study. Aliment Pharmacol Ther. 1998;12:1225–30. doi:10.1046/j.1365-2036.1998.00432.x. PMID:9882030.
- Karner M, Kocjan A, Stein J, Schreiber S, von Boyen G, Uebel P, Schmidt C, Kupcinskas L, Dina I, Zuelch F, et al. First multicenter study of modified release phosphatidylcholine “LT-02” in ulcerative colitis: a randomized, placebo-controlled trial in mesalazine-refractory courses. Am J Gastroenterol. 2014;109:1041–51. doi:10.1038/ajg.2014.104. PMID:24796768.
- Langhorst J, Wulfert H, Lauche R, Klose P, Cramer H, Dobos GJ, Korzenik J. Systematic review of complementary and alternative medicine treatments in inflammatory bowel diseases. Journal of Crohn's & colitis. 2015;9:86–106. doi:10.1093/ecco-jcc/jju007.