
ABSTRACT
Background: Maternal exposure to dietary factors during pregnancy may modulate the immunity of offspring by epigenetic programming. But the relationship between intrauterine environment and persistence of protective antibody after hepatitis B vaccination has not been reported. This study was to investigate the 5-year persistence of protective antibody response after primary hepatitis B vaccination, and its relationship with maternal folic acid supplementation. Materials and Methods: A total of 1461 children who completed a 3-dose 10 μg recombinant hepatitis B vaccine at birth and did not infect hepatitis B virus were followed up. Logistic regression and mediation analysis was used to explore the relationship between 5-year persistence of protective antibody and maternal nutrition. Results: Of 1403 children who did not revaccinated during the follow-up, 76.1% had protective hepatitis B surface antibody (anti-HBs) levels. Twenty percent of mothers did not take folate during pregnancy. Mediation analysis showed a total effect of folic acid supplementation on good persistence (odds ratio: 1.10, 95% CI: 1.03-1.17, p = 0.0010), a direct effect was 1.07 (95% CI: 1.01-1.13, p = 0.0128) and an indirect effect was 1.03 (95% CI: 1.00-1.06, p = 0.0672); the proportion of good persistence mediated by primary response was 30.3%. Conclusion: This study indicated a good protective anti-HBs persistence at year 5 after 10 μg recombination hepatitis B vaccination in infants. Maternal folic acid supplementation may improve the persistence of protective antibodies through other pathways. Multi-center cohort studies should be conducted to verify this conclusion.
Introduction
Hepatitis B virus (HBV) infection is the leading cause of chronic viral infection worldwide.Citation1 The outcome of chronic hepatitis B for people exposed to HBV is age-dependent. Among those who undergo acute HBV infection, about 95% of neonates, 20–30% of children aged 1–5 years and less than 5% of adults develop HBsAg carriers.Citation2 Therefore, vaccination, especially universal vaccination in infants and/or adolescents, was recommended by the World Health Organization and integrated into all national immunization programs by 1997 to prevent and control HBV infection.Citation3,Citation4 These programs have resulted in a sharp drop in the rates of acute infection, chronic infection and hepatitis B-related mortality in many parts of the world.Citation1
As a high-hepatitis B endemic area, Hepatitis B vaccine began to be used in 1992 in China, while it was introduced into the universal infant routine immunization in 2002. The schedule involved a three-dose HBV recombinant yeast vaccine (5 μg/dose) administered within 24 hours of birth and at ages 1 and 6 months.Citation5 As a result of this vaccine, the prevalence of HBV surface antigen (HBsAg) for people of 1–59 years decreased from 9.75% in 1992Citation6 to 7.18% in 2006.Citation7 The capital city, Beijing, launched the first vaccination program in China in 1990. Subsequently, a program of high-dose (10 μg) immunization in infants was commenced in 2006 as an alternative to the conventional 5 μg vaccine. Antibody to hepatitis B surface antigen (anti-HBs) concentration ≥10 mIU/mL is considered protective after a primary vaccine series. Better anti-HBs response, including the percentage of protective antibody (anti-HBs>10mIU/ml) and anti-HBs titers, could be achieved for infants with high-dose immunization than those with 5 µg/dose.Citation8 However, anti-HBs titers are known to decline over time,Citation9" and some loss of protection occur each year for children immunized at birth.Citation10 It is still unclear how long a protective antibody response may persist after vaccination.
Epidemiological studies highlighted the importance of the intrauterine environment in early fetal development, which is a critical period that determines the nutrition and health status of individuals throughout their lives.Citation11 Folic acid as its promising role in modulating diverse clinical conditions appears to be a first modern attempt to design a strategy for using food for the prevention or treatment of developmental defects.Citation12 Our former study has shown that maternal folic acid supplementation may increase anti-HBs titers in the primary response.Citation13 Considering primary response after hepatitis B vaccination is strongly associated with the persistence of the protective antibody response.Citation14 The relationship between maternal folic acid supplementation, primary response and persistence of the protective antibody response needs to be clarified.
Using a cohort study of children who completed a 3-dose 10 μg recombinant hepatitis B vaccine regimen with ‘0-1-6’ schedule at birth in Beijing, China, the aims of our study were to evaluate the 5-year persistence of protective antibody response after HBV primary immunization with the high-dose vaccination strategy in a medium-endemic area and explore their relationship with maternal folic acid supplementation.
Results
Characteristics of children in this study
Among the 4519 infants with primary HB vaccination, 102 infants with HBsAg or hepatitis B core antibody (anti-HBc) positive, anti-HBs < 10 mIU/ml or logic errors were excluded. Among the rest of 4417 infants who obtained protective antibody levels after primary immunization, a stratified sampling was conducted and 1461 infants were enrolled for follow-up. We also excluded 58 children who were revaccinated during the follow-up period. The final analyses included 1403 children. The participants’ selection procedure was shown in . The mean age was 5.6 ± 0.1 years. 52.2% were male and 95.1% were of Han population (.).
Figure 1. Participant's selection procedure.
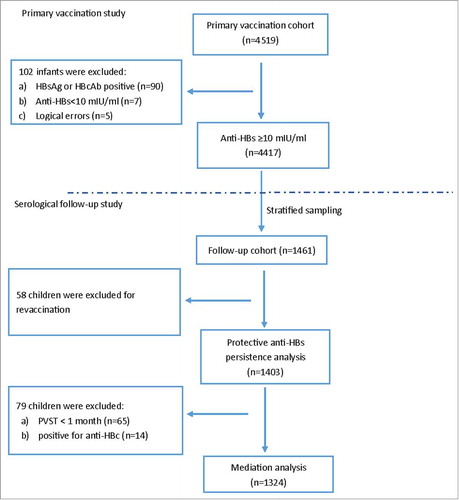
Table 1. Study population characteristics.
Five-year persistence of protective anti-HBs
To assess anti-HBs persistence, we determined the serum anti-HBs titers at year 5 after primary vaccination (). Of the 1403 children, 1068 (76.1%) still had protective anti-HBs concentrations (including 13 individuals positive for anti-HBc but negative for HBsAg and HBV DNA). Additionally, 332 (23.7%) had anti-HBs levels below 10 mIU/ml (including 1 child positive for anti-HBc but negative for HBsAg and HBV DNA) and 3 (0.2%) had undetectable anti-HBs. Nearly half of the children (49.1%) whose primary response was <1,000 mIU/ml did not have protective anti-HBs, but among those children whose primary response was ≥ 1,000 mIU/ml, only 11.5% did not have protective anti-HBs (p < 0.0001). The Geometric mean titer (GMT) of serum anti-HBs at year 5 after primary vaccination was 30.3 mIU/ml (28.0-32.9 mIU/ml). Anti-HBs concentrations were significantly higher in children whose primary response had been ≥ 1,000 mIU/ml than those in children whose primary response had been <1,000 mIU/ml (51.0 mIU/ml vs 9.8 mIU/ml).
Table 2. Serum anti-HBs titers at year 5 after vaccination by groups.
Association of maternal folic acid supplementation with the primary response and the 5-year persistence of the protective anti-HBs
After excluded 14 children who were positive for anti-HBc and 65 subjects whose post-vaccination serologic testing (PVST) were performed at less than one month, 1324 subjects were included in our mediation analysis. A total of 1029 (77.7%) women were given maternal folic acid supplementation during pregnancy. Adjusting for maternal factors, birth conditions and grow factors, maternal folic acid supplementation (odds ratio [OR]: 1.62; 95% CI: 1.20-2.20, p = 0.0017) was positively associated with the 5-year persistence of protective anti-HBs as well as high primary immune response (OR: 1.39; 95% CI: 1.03-1.86, p = 0.0292) (). As expected we also observed children having high primary immune response had a higher probability of having protective anti-HBs at year 5 after primary vaccination (OR: 10.24; 95% CI: 7.53-13.91, p < 0.0001, data not shown). Mediation analysis indicated that the total effect of folic acid supplementation on good persistence was 1.10 (95% CI: 1.03-1.17, p = 0.0010), the direct effect was 1.07 (95% CI: 1.01-1.13, p = 0.0128) and the indirect effect was 1.03 (95% CI: 1.00-1.06, p = 0.0672); with 30.3% of increased risk mediated by primary immune response ().
Table 3. Association of maternal folic acid supplementation with the primary response and the 5-year persistence of the protective anti-HBs.
Table 4. Primary immune response as mediator for association of maternal folic acid supplementation and 5-year persistence of protective anti-HBs.
Considering the maternal HBV infection status might be more important for the development of long-term immunity. We also conducted the same analysis after excluding the 179 subjects with unknown maternal HBV infection status. The result showed that the total effect, direct effect and indirect effect were 1.11 (95% CI: 1.03-1.19, p = 0.0012), 1.07 (95% CI: 1.01-1.14, p = 0.0132) and 1.03 (95% CI: 1.00-1.06, p = 0.0908), respectively. Indirect effect could explained 28.52% of the total effect (data not shown).
Discussion
Beijing is a medium endemic area where the prevalence of HBsAg is estimated at 3.49% in 2006.Citation15 A program of high dose immunization of the neonates was commenced an alternative to conventional 5 μg vaccine in 2006. It was the first cohort study evaluating the persistence of protective anti-HBs after 10μg vaccination. Our study showed that the majority (76.1%) of children retained a protective anti-HBs level at 5 years after primary vaccination with 3-dose 10 μg recombinant HB vaccine. The results are consistent with a meta-analysis of 33 studies presented at an international meeting in Milan organized by the Viral Hepatitis Prevention Board in 2011.Citation9 Also, our study showed that the children with high primary immune response had higher anti-HBs titers and proportion of anti-HBs titers ≥ 10 mIU/ml. The results consist with the studies conducted in both high and low endemic areas.Citation9,Citation16
Emerging epidemiological studies emphasize the importance of intrauterine exposure in embryogenesis and adult health. Maternal exposure to dietary factors during pregnancy may modulate the immunity of offspring by epigenetic programming. Studies showed that maternal folic acid supplementation, which was commonly used to prevent neural tube defects (NTDs),Citation17 may have a role in the prevention of pregnancy complications.Citation18–21 In our study we observed that maternal folic acid supplementation was positively associated with 5-year persistence of protective anti-HBs. Considering that folic acid supplementation may increase anti-HBs titers in the primary response from our previous study,Citation13 together with the fact that antibody levels after primary vaccination are strongly associated with the persistence of the protective antibody,Citation14 which was also found in this study, we performed mediation analysis to verify whether or not there is a direct effect of maternal folic acid supplementation on the persistence of the protective antibody response other than the indirect effect by increasing primary response. We found that folic acid may directly increase 5-year persistence of protective anti-HBs (OR = 1.07; 95% CI: 1.03-1.17, p = 0.0010) and the proportion of good persistence mediated by primary response was 30.3%. Considering maternal HBV infection status has a significant impact on the persistence of protective anti-HBs, we also excluded the 179 subjects with unknown maternal HBV infection status and found the consistent results.
Folate deficiency is common in various regions of China, including Beijing, for women of childbearing age.Citation22 Maternal folic acid supplementation may influence the persistence of protective anti-HBs by following ways. On the one hand folate deficiency reduces fetal iron stores even may leading to anemia, perhaps well into the first year of life.Citation23 Experimental studies have shown that iron is a fundamental element for normal development of the immune system. Humoral, cell-mediated and nonspecific immunity that have an important role in various steps of immunogenic mechanisms are influenced by iron deficiency anemia.Citation24 On the other hand folic acid may also affect anti-HBs persistence by providing methyl groups, which is critical for intracellular DNA methylation reactions.Citation25 Folic acid plays a key role in DNA methylation and cell-mediated immunity is especially affected by folate deficiency.Citation26 Appropriate DNA methylation is essential for embryogenesis and adult health.Citation27 DNA methylation, can act in concert with transcription factors and play critical roles in B cell development and differentiation, including differentiation to memory B cells or long-lived plasma cells for the immune memory.Citation28 Thus, our findings that maternal folic acid supplementation may increase the probability of persistence of protective anti-HBs is supported by the demonstrated biological functions of these molecules in regulating immune health.
It is noteworthy that the performance of immune response at the peak after vaccination is the foundation stone for long-term immunity. Our study also supported that primary vaccination are strongly associated with the persistence of protective antibody levels. Logically, it is possible that the maternal folic acid supplementation may impact on long-term immunity via the indirect effect, that is, enhancing the peak level after immunization. Our results showed that the indirect effect of maternal folic acid supplementation on persistent protective antibody was 1.03 (95% CI: 1.00-1.06, p = 0.0672) and p value was around the threshold of 0.05. Our current sample size may have not enough power to detect the effects.
The strengths of this study are as followings. First, all the participants were enrolled through the immunization information management system and had clear immunization records. The detailed immunization information could help us to exclude the participants with revaccination. Secondly, mediation analysis was used to explore the casual relationship between folic acid supplementation, primary response and persistence of the protective antibody response.
A limitation of this study is that we did not evaluate the immune memory of the people who had anti-HBs < 10 mIU/ml because loss of protective anti-HBs does not necessarily imply loss of protection due to immunological memory. Several studies have shown that the presence of detectable anti-HBs in children before booster immunization is positively associated with the response to the booster dose.Citation29 Subjects with lower anti-HBs responded more poorly to a booster dose than those with higher anti-HBs.Citation30–32 Therefore, factors that protect the persistence of protective anti-HBs may also protect the immune memory.
Conclusions
The 10 μg recombination hepatitis B vaccination strategy has good protective anti-HBs persistence at year 5 after primary vaccination in infants. Maternal folic acid supplementation may improve the persistence of protective antibodies through other pathways. Additional multi-center cohort studies are needed to verify the conclusions.
Materials and methods
Primary vaccination study design
The primary vaccination study was conducted in 2009. A total of 4519 infants completed 3 doses of 10 μg recombinant Hepatitis B vaccine (hansenula polymorpha, Dalian Hissen Bio-pharm. Co., Ltd, Dalian, China) with a ‘0-1-6’ schedule (at birth, 1 and 6 months of age). Children were enrolled using the immunization information management system from 179 community health services centers of all 18 sub-districts in Beijing. All the enrolled infants have clear immunization records. Parents were interviewed using a structured questionnaire that included infants’ demographic characteristics (gender, ethnicity and date of birth), birth condition (prematurity, newborns parity and birth weight) and maternal characteristics during pregnancy (anemia, calcium deficiency, diabetes, hypertension, folic acid supplementation and HBV infection status). The information of anemia, diabetes, hypertension and calcium deficiency was collected based on the physicians’ diagnoses.Citation13
Serological follow-up study
Because the original aim of this follow-up study was to explore the five-persistence of protective anti-HBs for the infants after high-dose primary vaccination. So, we used the rate of five-year persistence of protective anti-HBs to estimate the sample size. Assuming persistence rate of 75%,Citation9 allowable error of 5% and significance level to be 0.05, the estimated sample size was 1191. After adjusting loss to follow-up rate of 15%, the total sample size was 1401. The participants for the follow-up study were selected in 2014 using stratified sampling to ensure that the number of children was proportional to the size of the community health services in the primary vaccination study. Finally a total of 1461 children who reached protective antibody after primary vaccination were enrolled. We also excluded the children who were revaccinated during the follow-up. The participants’ selection procedure was shown in . Questionnaire surveys were conducted among all children's parents to collect the children's growth condition (weight, height, zinc or calcium supplementation and residence at the follow-up period) and the revaccination history.
Laboratory testing and definition
Three milliliters of intravenous blood were collected when the PVST was conducted. Serum was separated and stored at −80 °C for testing anti-HBs, HBsAg and anti-HBc for primary vaccination.Citation13 At 5 years after primary vaccination, another 3 ml of intravenous blood were collected to determine the current level of anti-HBs and to evaluate evidence for previous or current HBV infection. Anti-HBs, HBsAg and anti-HBc were measured using a chemiluminescence micro-particle immunoassay (Architect i2000 analyzer, Abbott, Chicago, IL, USA). The limits of anti-HBs concentration detection were 0.05 and 15,000 mIU/ml. Protective anti-HBs was defined as anti-HBs≥10 mIU/ml. Nested-PCR was used to assay for HBV DNA for children with anti-HBc positivity, while HBsAg-positive and/or anti-HBc-positive individuals were defined as being HBV-infected.
Ethics approval
This study was overseen by The Ethical Committee of the Institute of Basic Medical Sciences Chinese Academy of Medical Sciences and Beijing Center for Disease Prevention and Control.
Statistical analysis
Continuous variables are given as mean ± standard deviation and categorical variables as the absolute value and relative frequency to describe the variables’ distributions where appropriate. Five-year antibody persistence after primary vaccination was evaluated with respect to the percentage of subjects (with 95% confidence intervals (CIs)) who had anti-HBs≥10 mIU/ml. The anti-HBs level was log-transformed to satisfy the normal distribution. GMTs and their CIs were calculated by transforming the results to a common logarithmic scale, assuming asymptotic normality conditions were satisfied on the scale and converting back to the original scale.Citation33 Differences in log-transformed anti-HBs levels were evaluated by analysis of variance, and the chi-squared test was applied to compare the difference in proportion of anti-HBs ≥ 10 mIU/ml with different primary response level. Three logistic regression models were used to examine the association between maternal folic acid supplementation and primary immune response, maternal folic acid supplementation and the protective antibody response at year 5, and primary immune response and the protective antibody response at year 5, respectively. All models were adjusted with birth condition, maternal status and grow factors. Infants born before 37 gestational weeks were grouped as “premature”. Birth weight (<2500 g [low birth weight], 2500–4000 g [normal birth weight] and ≥4000 g [large for gestational age] and the body mass index [underweight, normal and overweight] at 5 year after primary vaccination were defined according to the recommendations of the United States Center for Disease Control and Prevention.Citation34
Mediation analysis is an application of causal modeling.Citation35 It divides the effect of an exposure on the outcome to two parts. One is the direct effect and the other is the indirect effect. The effect of the exposure on the outcome that is not through the intermediate of interest is referred to as a direct effect. The effect of the exposure on the outcome that operates through intermediate of interest is referred to as an indirect effect. And the intermediate of interest is referred to as “mediator”. The sketch map was shown in .
Figure 2. Simple sketch map of mediation.
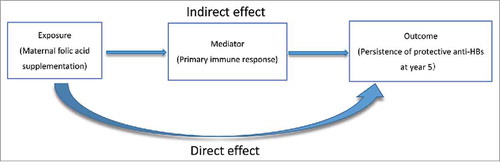
In this study, maternal folic acid supplementation was regarded as the “exposure” variable, while primary immune response was regarded as the “mediator”. The primary immune response was defined as a two-group classification setting: high primary immune response (anti-HBs titers ≥ 1,000 mIU/ml) or not. Firstly, a generalized linear model with binomial probit link function was used to estimate the association between the exposure variable and the mediator. Then, the same model was used to estimate the association of the mediator, the exposure variable and the outcome. Finally, a non-parametric bootstrapping method with up to 10,000 simulations was applied to obtain accurate p values of the estimates of the total effects, direct effects as well as indirect effects. Covariates included in the exposure-mediator and exposure-outcome models were the same with the logistic regression model.
To perform mediation analysis, we also modified the dataset to exclude potential confounding factors. Firstly we excluded children who were positive for anti-HBc. Moreover, our previous analysis showed that anti-HBs titers reach a peak at one month after completion of primary vaccination and then show a negative linear correlation between initial PVST time to log anti-HBs titers.Citation13 Thus, we excluded subjects whose PVST was performed at less than one month and then constructed a linear model of the PVST time and the anti-HBs titers in order to estimate the peak value of the anti-HBs titers in the primary response.
Analyses were implemented with SAS version 9.3 (SAS institute Inc. Cary, NC) and The R package “Mediation” was used for mediation analysis.Citation36 Two-sided statistical tests were performed, and p-values<0.05 were considered to be statistically significant.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.Acknowledgments.
Author contributions
X.Z. and X.P. coded and analyzed the data, wrote the manuscript. L.W. and W.Z. designed the study, guided the writing of the manuscript, and reviewed the manuscript. F.W. and F.C. supervised field work. All authors read and approved the final manuscript.
Acknowledgments
We acknowledge the children, parents and the personnel from the Beijing Center Disease Control and Prevention who participated in the study.
Additional information
Funding
References
- Trepo C, Chan HL, Lok A. Hepatitis B virus infection. Lancet. 2014;384:2053–63. doi:10.1016/S0140-6736(14)60220-8. PMID:24954675.
- Beasley RP. Rocks along the road to the control of HBV and HCC. Ann Epidemiol. 2009;19:231–4. doi:10.1016/j.annepidem.2009.01.017. PMID:19344859.
- Expanded programme on immunization. Global Advisory Group–Part I. Releve Epidemiologique Hebd / Sect. D'hygiene du Secretariat de La Soc. Des Nations = Wkly Epidemiol Rec / Health Sect Secretariat League Nations. 1992;67:11–5. PMID:1736955.
- VanDamme P, Kane M, Meheus A. Integration of hepatitis B vaccination into national immunisation programmes. Brit Med J. 1997;314:1033–6. PMID:WOS:A1997WT15200031.
- Cui FQ, Wang XJ, Cao L, Liang XF, Lu Y, Lu YS, et al. Progress in hepatitis B prevention through universal infant vaccination – China, 1997–2006 (Reprinted from MMWR, vol 56, pg 441–445, 2007). Jama-J Am Med Assoc. 2007;298:506–+. PMID:WOS:000248438100009.
- Xia GL, Liu CB, Cao HL, Bi SL, Zhan MY, Su CA, et al. Prevalence of hepatitis B and C virus infections in the general Chinese population. Results from a nationwide cross-sectional seroepidemiologic study of hepatitis A, B, C, D, and E virus infections in China, 1992. Int Hepatol Commun. 1996;5:62–73. doi:10.1016/S0928-4346(96)82012–3. PMID:WOS:A1996UT28500011.
- Liang X, Bi S, Yang W, Wang L, Cui G, Cui F, Zhang Y, Liu J, Gong X, Chen Y et al. Epidemiological serosurvey of hepatitis B in China–declining HBV prevalence due to hepatitis B vaccination. Vaccine. 2009;27:6550–7. doi:10.1016/j.vaccine.2009.08.048. PMID:19729084.
- Zhang L, Zhang W, Zhai XJ, Li YP, Li J, Yan BY, Li YT, Zhu FC, Huang T, Li LQ, et al. Comparison on the antibody response after primary immunization of 5 µg and 10 µg hepatitis B vaccine made by recombinant DNA techniques among newborns. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua Liuxingbingxue Zazhi. 2012;33:305–8.
- FitzSimons D, Hendrickx G, Vorsters A, Van Damme P. Hepatitis B vaccination: A completed schedule enough to control HBV lifelong? Milan, Italy, 17–18 November 2011. Vaccine. 2013;31:584–90. doi:10.1016/j.vaccine.2012.10.101. PMID:23142301.
- Lu CY, Chiang BL, Chi WK, Chang MH, Ni YH, Hsu HM, Twu SJ, Su IJ, Huang LM, Lee CY. Waning immunity to plasma-derived hepatitis B vaccine and the need for boosters 15 years after neonatal vaccination. Hepatology. 2004;40:1415–20. doi:10.1002/hep.20490. PMID:15565627.
- China TmohotPsRo. The report of children's nutrition development aged 0–6 years old in China Acta Nutrimenta Sinica 2013;35:1–4.
- Barua S, Kuizon S, Junaid MA. Folic acid supplementation in pregnancy and implications in health and disease. J Biomed Sci. 2014;21:77.
- Xiao M, Qiu Q, Pang X, Liang X, Li L, Cui F, Wang F, Zhang G, Li H, Wang L et al. Immune response in infants after universal high-dose hepatitis B vaccination: A community-based study in Beijing, China. Vaccine. 2015;33:5878–83. doi:10.1016/j.vaccine.2015.06.018. PMID:26117148.
- Schonberger K, Riedel C, Ruckinger S, Mansmann U, Jilg W, Kries RV. Determinants of Long-term protection after hepatitis B vaccination in infancy: A meta-analysis. Pediatr Infect Dis J. 2013;32:307–13. doi:10.1097/INF.0b013e31827bd1b0. PMID:23249904.
- Wu J, Zhang W, Han LL, Lin CY, Lin H, Xing YL, Gao P, Gong XH, Liu LR, Huang F, et al. A sero-epidemiologiecal study on hepatitis B among general population in Beijing. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua Liuxingbingxue ZazhiCochraneCochrane. 2007;28:555–7. PMID:17939383.
- Boxall EH, J AS, El-Shuhkri N, Kelly DA. Long-term persistence of immunity to hepatitis B after vaccination during infancy in a country where endemicity is low. The Pediatr Infect Dis J. 2004;190:1264–9. doi:10.1086/423818. PMID:15346336.
- De-Regil LM, Pena-Rosas JP, Fernandez-Gaxiola AC, Rayco-Solon P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database of Syst Rev. 2015:Cd007950. doi:10.1002/14651858.CD007950.pub3. PMID:26662928.
- Bukowski R, Malone FD, Porter FT, Nyberg DA, Comstock CH, Hankins GD, Eddleman K, Gross SJ, Dugoff L, Craigo SD, et al. Preconceptional folate supplementation and the risk of spontaneous preterm birth: A cohort study. PLoS Med. 2009;6:e1000061. doi:10.1371/journal.pmed.1000061. PMID:19434228.
- Catov JM, Bodnar LM, Olsen J, Olsen S, Nohr EA. Periconceptional multivitamin use and risk of preterm or small-for-gestational-age births in the Danish National Birth Cohort. Am J Clin Nutr. 2011;94:906–12. doi:10.3945/ajcn.111.012393. PMID:21795441.
- Li Z, Ye R, Zhang L, Li H, Liu J, Ren A. Periconceptional folic acid supplementation and the risk of preterm births in China: A large prospective cohort study. Int J Epidemiol. 2014;43:1132–9. doi:10.1093/ije/dyu020. PMID:24603317.
- Saccone G, Sarno L, Roman A, Donadono V, Maruotti GM, Martinelli P. 5-Methyl-tetrahydrofolate in prevention of recurrent preeclampsia. J Matern Fetal Neonatal Med. 2016;29:916–20. doi:10.3109/14767058.2015.1023189. PMID:25777577.
- Ronnenberg AG, Goldman MB, Aitken IW, Xu X. Anemia and deficiencies of folate and vitamin B-6 are common and vary with season in Chinese women of childbearing age. J Nutr. 2000;130:2703–10. PMID:11053510.
- Allen LH. Anemia and iron deficiency: Effects on pregnancy outcome. Am J Clin Nutr. 2000;71:1280S–4S. PMID:10799402.
- Ekiz C, Agaoglu L, Karakas Z, Gurel N, Yalcin I. The effect of iron deficiency anemia on the function of the immune system. Hematol J Official J Eur Haematol Assoc. 2005;5:579.
- Lu Y, Cheng Y, Yan W, Nardini C. Exploring the molecular causes of hepatitis B virus vaccination response: An approach with epigenomic and transcriptomic data. BMC Med Genomics. 2014;7:12. doi:10.1186/1755-8794-7-12. PMID:24612962.
- Dhur A, Galan P, Hercberg S. Folate status and the immune system. Prog Food Nutrition Sci. 1991;15:43–60. PMID:1887065.
- Barua S, Kuizon S, Junaid MA. Folic acid supplementation in pregnancy and implications in health and disease. J Biomed Sci. 2014;21:77. doi:10.1186/s12929-014-0077-z. PMID:25135350.
- Zan H, Casali P. Epigenetics of peripheral B-cell differentiation and the Antibody Response. Front Immunol. 2015;6:631. doi:10.3389/fimmu.2015.00631. PMID:26697022.
- McMahon BJ, Dentinger CM, Bruden D, Zanis C, Peters H, Hurlburt D, Bulkow L, Fiore AE, Bell BP, Hennessy TW. Antibody levels and protection after hepatitis B vaccine: results of a 22-year follow-up study and response to a booster dose. J Infect Dis. 2009;200:1390–6. doi:10.1086/606119. PMID:19785526.
- Salama, II, Sami SM, Salama SI, Foud WA, Abdel Hamid AT, Said ZN. Persistence of protection to hepatitis B vaccine and response to booster dose among children and adolescents in Dakahleya- Egypt. Egyp J Immunol / Egyp Assoc Immunologists. 2014;21:13–26. PMID:25204041.
- Wang LY, Lin HH. Short-term response to a booster dose of hepatitis B vaccine in anti-HBs negative adolescents who had received primary vaccination 16 years ago. Vaccine. 2007;25:7160–7. doi:10.1016/j.vaccine.2007.07.022. PMID:17707557.
- Zinke M, Kappes R, Kindler K, Paulus-Koschik A, Goering U, Disselhoff J, Soemantri P, Grunert D, Laakmann KH, Gunasekaran R, et al. Immune memory to hepatitis B virus in 4-9-year old children vaccinated in infancy with four doses of hexavalent DTPa-HBV-IPV/Hib vaccine. Human Vaccines. 2009;5:592–8. PMID:19535920.
- Nauta J. Statistics in clinical vaccine trials. Springer Sci Bus Media. 2010.
- Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, Wei R, Curtin LR, Roche AF, Johnson CL. 2000 CDC growth charts for the united states: Methods and development. Vital Health Statist Ser 11, Data Nat Health Survey. 2002:1–190. PMID:12043359.
- Gelfand LA, Mensinger JL, Tenhave T. Mediation analysis: A retrospective snapshot of practice and more recent directions. J Gen Psychol. 2009;136:153.
- Tingley D, Teppei H, Mit Y, Keele L, State P, Imai K. Mediation: R package for causal mediation analysis. J Stat Softw. 2015;59:1689–91.