
ABSTRACT
Exposure to pro-vaccination messages from nonmedical peers and others perceived to share a similar value system for society (referred to as worldview outlook) improves vaccination attitudes. Nonetheless, a minority of African American parents have friends and family members who provide them with vaccine advice. The aims of the current study were to identify the presumed worldview outlook of eight types of community figures as perceived by African American parents, and determine parents’ trust in these figures for vaccine advice, and whether trust varied according to the figures’ racial concordance. A cross-sectional survey was administered to 110 African American parents in 2015. Parents perceived the community figures to represent a spectrum of worldview outlooks. Although levels of trust in the community figures differed overall (p < .001), it was high in the school nurse, pediatrician, mother, father, disease survivor, and vaccine scientist. All trusted figures except the father were perceived to hold a communitarian outlook. Parents shown race-concordant figures had higher levels of trust in them than those who were shown race-discordant equivalents (p < .01). These findings suggest that vaccination campaigns geared toward African American parents may be strengthened by including other nonmedical, African American spokespersons who convey their community contributions in messages.
Introduction
Vaccinating a child is an important parental decision that is often not made alone. Parents trust the advice of social contacts to form their own opinions and beliefs about vaccination.Citation1–Citation5 Social contacts may influence parents’ behavior by providing cues as to whether vaccine acceptance or refusal is typical and acceptable among peers.Citation6,Citation7 In fact, the proportion of a parent’s social network recommending against vaccination may be more strongly associated with whether parents vaccinate their children than parents’ own thoughts on childhood vaccination.Citation2 Respected community members’ opinions can help people overcome mistrust, and enhance and reinforce healthcare provider-patient communication.Citation8 Nonetheless, a minority of African American parents receive vaccine advice from family and friends.Citation9,Citation10 Therefore, identifying trusted community members to advocate for vaccines may play an important role in promoting vaccination acceptance among African American parents for their children.
A community member’s ability to impact a parent’s attitude toward vaccination is dependent on how he or she is perceived by the parent.Citation11,Citation12 Studies have shown that people may find others more credible if they can connect with them through mutual worldview outlook – meaning a sense of how society should be organized (the Cultural Cognition Thesis).Citation11,Citation12 In studies, worldview outlook has been defined along two intersecting norm dimensions labelled “group” and “grid” ().Citation12,Citation13 “High group” individuals adhere to a communitarian outlook which holds that the community has a responsibility to help all individuals in solidarity; by contrast, “low group” individuals adhere to an individualistic outlook which deems individuals to have a responsibility primarily to their own interests. “High grid” individuals adhere to a hierarchical view of social order which holds that social privileges and choices are dependent upon an individual’s position in society, and everyone has their rightful role; whereas, “low grid” individuals adhere to an egalitarian outlook which considers individual characteristics irrelevant in terms of merit for social privileges, and everyone is basically equal. In one study, participants had higher odds of changing their attitudes toward the human papillomavirus vaccine if the argument for or against it was thought to have been made by someone with whom they believed to share their same worldview orientation.Citation11
Figure 1. Group-grid worldview typology in accordance with the cultural cognition thesis.
Credibility might be further influenced by the racial or cultural profile of the messenger.Citation5 For instance, racial concordance with health care providers has been associated with greater trust and satisfaction in care among African Americans patients.Citation14–Citation19 Further, some communication literature has also shown that culturally relevant messages are more effective at changing health behavior of minorities including African Americans,Citation20–Citation22 although the data are still inconclusive in terms of the cost-benefit of culturally tailored messaging.Citation23–Citation25
In the current study, we assessed African American parents’ perceptions of the relative cultural worldviews of various types of prominent community figures. We then determined the level of trust African American parents had in these community figures, and whether levels of trust varied according to the community figures’ racial concordance (i.e., also African American or not). The ultimate goal of our inquiry was to identify the types of messengers most suitable to convey vaccination advice to African American parents in public health vaccination campaigns to enhance confidence in national recommendations. In total, there were 110 participants. Most were female, in their twenties and thirties, and had two or more young children ().
Results
Perceived worldviews of different community figures
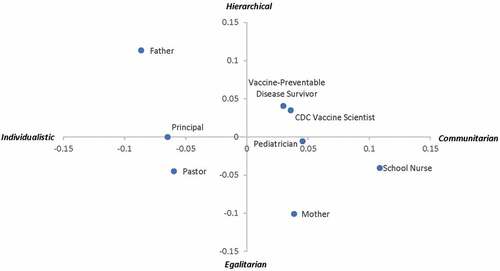
Among all eight example community figures presented to participants, the father was the only one who was perceived by participants to support a hierarchical/individualistic worldview. Participants perceived both of the two medical authority figures, the pediatrician and CDC vaccine scientist, as communitarian, but they considered the scientist to be hierarchical; whereas, they considered the pediatrician to be slightly more egalitarian (). In addition to the pediatrician, participants attributed a communitarian and egalitarian worldview to the school nurse and the mother who had accepted vaccination for her own child.
Figure 2. Participants’ perceived worldview of eight types of community figures.
Levels of trust
Distributions of level of trust for vaccine advice in the eight types of community figures overall differed (p < .001) (). Nonetheless, median levels of trust were 8 or higher for six of the community figures: the school nurse, the pediatrician, the mother, the father, the vaccine-preventable disease survivor, and the CDC vaccine scientist. Levels of trust in the pediatrician and CDC vaccine scientist were the highest, with medians reaching the maximum level of 10 for both figures. Levels of trust in the school principal and pastor were lowest with both medians equal to 5.
Figure 3. Levels of trust in community figures for vaccine advice.
As compared to participants shown images of race-discordant community figures, participants shown race-concordant figures had significantly higher levels of trust in the eight community figures overall (p < .01) (). Average level of trust in the race-concordant medical authority figures (the pediatrician and the CDC vaccine scientist together as a group) was extremely high among study participants (median score of 10). While level of trust in the race-discordant medical authority figures was still high (median of 8.5), it was nonetheless significantly lower than for the race-concordant examples (p < .001). We did not detect a significant difference in levels of trust between the race-concordant and discordant non-medical authority figures as a group (median of 7.3 and 6.5, respectively) (p = .1). However, among individual community figure types, there was higher trust in the race-concordant vaccine-preventable disease survivor (p < .05), and principal as compared with the parallel race-discordant figures (p < .05).
Table 1. Value statements used to assess perceived cultural worldview of community figures.
Table 2. Background of participants.
Table 3. Comparisons of trust in race concordant versus discordant community figures.
Discussion
This study found that while people who are typically viewed as medical authority figures for vaccinations – i.e., pediatricians and CDC scientists – were highly trusted types of individuals for vaccine advice among African American participants, several other nonmedical authority figures were also considered trustworthy, including parents who had accepted vaccination for their own children, school nurses, and vaccine-preventable disease survivors. Community figures who were most trusted were perceived to hold a communitarian worldview with the exception being the father, who was thought to be more individualistic. Overall, race-concordant community figures were trusted more highly for vaccine advice than race-discordant figures. Levels of trust in specific types of race-concordant figures – pediatricians, scientists, vaccine-preventable disease survivors and principals – were significantly higher than in their race-discordant counterparts.
Because this study found that most of the trusted vaccine advisors were perceived to value community benefit, it could be useful in vaccination ad campaigns to convey how vaccine spokespersons contribute to society in addition to having them share their opinions about vaccines. The typical medical authorities for vaccine information, pediatricians and vaccine scientists, were both perceived by participants to be communitarian in their worldview outlook, and indeed, to hold relatively similar worldviews to each other. Prior studies suggest that different types of messengers are necessary to convey different types of pro-vaccine messages – for example, supportive family messages versus healthcare provider endorsement.Citation26,Citation27 Thus, vaccination ad campaigns may be more persuasive if they include other nonmedical, trusted community figures such as other parents, vaccine-preventable disease survivors and school nurses, who represent a broader set of worldviews. Furthermore, because a previous study found that African American adults often hold egalitarian/communitarian worldviews themselves,Citation12 it may be particularly useful to include mothers and school nurses in messages directed toward African American audiences as our study suggests these types of community figures are also perceived to be relatively egalitarian and communitarian. Inclusion of community figures who are not medical authorities may be particularly useful in vaccination campaigns for reaching parents who are more vaccine hesitant given that vaccine hesitant parents and refusers may have lower levels of trust in, and more negative experiences with the medical system.Citation28–Citation30
Our study suggests that like parents of other races,Citation10,Citation31,Citation32 African American parents trust medical authorities for vaccine advice. Nonetheless, qualitative studies have repeatedly demonstrated that though this may be true, African Americans’ attitudes toward vaccination are multi-faceted and often impacted by deep-seated fears of experimentation.Citation1,Citation10,Citation33 This may explain our finding that trust in the race-concordant CDC vaccine scientist and pediatrician were both significantly higher than in the race-discordant equivalents. This is consistent with other studies which have suggested that racial concordance improves patients’ trust in medical authorities and satisfaction with care.Citation14–Citation19 Previous studies suggest that distrust in physicians leads some African Americans to avoid seeking care, forego treatment and withdraw altogether from care.Citation34 That said, it is not possible, or even desirable to have all patients treated exclusively by race-concordant healthcare providers; an alternate solution may be to supplement healthcare provider recommendations with advice from other messengers who are perceived by patients to be of similar background and experience. Among suggested cultural competency techniques to reduce health disparities are to use community health workers for education and communication, and to involve family members and community leaders in counseling.Citation8 Inclusion of nonmedical, trusted community figures may be particularly useful for reaching parents most likely to refuse vaccines; in one study, African Americans who were more racially conscious had lower trust in influenza vaccine, and the vaccine process, higher suspicions of influenza vaccine risk, less confidence in the influenza vaccine’s benefits, and greater vaccine hesitancy.Citation7
Because the purpose of this study was to help identify potentially effective messengers broadly for public health vaccination campaigns in predominantly African American communities, it was intentionally conducted amongst a population of parents without regard to their baseline views on vaccination. Few parents in this study reported refusing or delaying any childhood vaccination for a disease other than influenza (2.7%) which is consistent with the low percentage nationally of exemptions from school-required vaccinations (2.2%).Citation35 While this rate is low, multiple studies have demonstrated that parental attitudes toward vaccination should be considered along a continuum of vaccine acceptance since some parents who have accepted vaccines in the past may still harbor concerns that portend future vaccine refusal.Citation29,Citation30,Citation36 Parents with concerns about vaccines who are at risk for refusal but are not adamant refusers have been subcategorized as “Fence-sitters” and “Worrieds” in one classification system, and as “Cautious Acceptors,” “Hesitants” and “Late/Selective” vaccinators in another.Citation29,Citation30 Our study likely included many parents in these categories given that 30.9% responded affirmatively when asked specifically whether they had ever refused or delayed influenza vaccination (a percentage similar to the national percentage of children who are not vaccinated against influenza each year (~40%)).Citation37 This suggests the importance of vaccination campaigns reaching parents along the spectrum of vaccine acceptance especially for vaccines that are frequently and inaccurately perceived as more risky such as influenza vaccine, or those that are newer, such as human papillomavirus vaccine whose rate of uptake continues to lag behind that of other adolescent vaccines.Citation38
Despite our relatively small sample size, we found that the probability of equivalent levels of trust in the race-concordant and discordant examples of the pediatrician to be extremely low (p < .001), likely in part because the difference in ratings was substantial at 20% (large effect size). It is possible that our small sample size limited our ability to detect small differences in trust in other community figures by racial concordance. Our study was also limited by the fact it was conducted in a Supplemental Nutrition Program for Women, Infants and Children Supplemental Nutritional (WIC) center and a healthcare center collocated with an academic hospital in an urban setting, and may not be generalizable to other settings. Active WIC enrollees have higher immunizations rates than non-enrollees,Citation39 and participants recruited from a healthcare center may have a higher degree of trust in medical professionals than others who were not recruited by virtue of avoiding medical visits. Those parents who avoid medical visits may have lower levels of trust in physicians and scientists, and it may be even more important to identify alternative, non-medical community figures to disseminate vaccination messages to this group. Our study is further limited by our use of still images (rather than videos or interactive media) of hypothetical community figures. Clearly, how real people convey health messages is an important determinant of their credibility with parents. In one study, when physicians were more patient-centered in their communication, patients perceive themselves to be more personally similar, and had greater trust in the physicians.Citation18 It is possible that some of the differences in parental trust in race-concordant versus discordant community figures might have been less if parents were presented with videos in which race-concordant and discordant figures were both able to present content in a manner that was perceived to be culturally, and personally relevant to participants. Finally, similar to other surveys, trust in community figures for vaccine advice was assessed using a single item.Citation31,Citation40,Citation41 Future studies whose aim is to fine tune the assessment of trust in vaccine advisors may develop and test a scale to possibly assess this construct more precisely.
Conclusion
In addition to healthcare professionals, African American parents also trust other community figures for vaccine advice. They perceive these community figures to hold an array of culture worldviews. In future studies, it may be useful to determine the impact of mobilizing many different types of community figures as pro-vaccination spokespeople to appeal to the broadest African American audience.
Patients and methods
This study protocol was deemed exempt from review by the Children’s National Medical Center institutional review board (IRB) on the basis of the information being recorded in such a manner that participants could not be identified directly or through identifiers linked to the participants. Participants were informed about the study purpose, their rights, confidentiality and study contacts by research staff following an oral script prior to beginning the survey.
Participants and setting
Participants were recruited from a pediatric ambulatory care center and a WIC office co-located with a teaching hospital in Washington, D.C. All participants were recruited between August to December 2015, and were self-identified African American, English-speaking parents and legal guardians (hereafter referred to collectively as parents) who were age 18 years or older. Because the study intended to assess normative beliefs among acculturated African Americans, participants were excluded if they had lived in the United States for less than 10 years.
Survey administration
African American parents were approached in waiting rooms prior to their child’s appointment. For parents who were interested and eligible to participate, a survey was administered while parents awaited the child’s healthcare visit. To ensure adequate participation of parents with low literacy skills, the survey was administered via a face-to-face interview by research staff. The survey consisted of two parts – one assessed the relative cultural worldview that parents attributed to eight community figures, and the second assessed parental levels of trust in each of these figures. The following community figures were represented: school nurse, church pastor, school principal, pediatrician, “mother whose own child got the vaccine,” “father whose own child got the vaccine,” “disease survivor who could have been protected if she had gotten the vaccine,” and a “Centers for Disease Control and Protection (CDC) vaccine scientist.” The included community figures were selected based on previous studies’ findings of people potentially influential in parents’ vaccination decisions.Citation5,Citation6,Citation31,Citation40,Citation42 Parents were shown labelled images of the figures in a stereotypical pose (e.g., school nurse in scrubs examining a child, pastor in church, school principal in a classroom, pediatrician in a white coat examining a child, mother/father hugging a child, disease survivor at a rally, and scientist with a microscope). We first pilot tested the survey with ten parents who met inclusion criteria, and interviewed them for feedback after the survey. In the pilot phase, local politician was dropped as one of the community figures based on universally very low levels of trust in this community figure; whereas, father of a vaccinated child – which was not originally included – was added upon participants’ suggestion.
To determine perceived, relative cultural worldviews of the community figures, participants were asked to choose the one community figure from the eight who they thought was most likely to endorse each of 25 different value statements using two adapted, validated scales, based upon group-grid typology.Citation12 These scales had previously been tested in populations of diverse racial and ethnic backgrounds, including over 400 African American adults. A few of the items were modified slightly or dropped after pilot testing for comprehension and to reduce response burden. lists the value statements included in the final survey. Each value statement was representative of a cultural norm attributed to a particular worldview – communitarian, individualistic, hierarchical, and egalitarian. For the individualistic-communitarian scale, 7 items measured individualistic worldview and 4 items measured communitarian worldview. The hierarchical-egalitarian scale was comprised of 7 items measuring hierarchical worldview and 7 items measuring egalitarian worldview.
To evaluate level of trust in the community figures, participants were asked, “How much would you trust each of the following types of people in a video describing why they think a vaccine is good for your child?” This item was adapted from two previously published surveys that together included nearly 600 African American adults.Citation31,Citation40 Response options were on a scale of 1 (not at all) to 10 (very much). To assess the influence of racial concordance on levels of trust, the first half of all participants were shown African American example images (race concordant) and the second half of all participants were shown white example images (race discordant). Neither group was told that an aim of the study was to examine the effect of racial concordance on their opinions. Participants were simply told to react to figures based on their community “role,” while the race of the figures depicted in the images was to appear to participants as incidental.
Statistical methods
A mean communitarian score for each figure was calculated based on the number of times that figure was chosen as the one most likely to endorse one of the communitarian value statements divided by the total number of communitarian value statements. Mean individualistic, hierarchical and egalitarian scores were similarly calculated. To assess internal consistency of the scales, we calculated Cramér’s V for each pairing of variables in each of the four scales. Cramér’s V ranged from 0.32–0.44 for the communitarian scale, 0.33–0.46 for the individualistic scale, 0.36–0.57 for the hierarchical scale, and 0.35–0.53 for the egalitarian scale, indicating strong to very strong correlation among all of variables included in the same scale. A figure’s “group” score was determined by mean communitarian score minus mean individualistic score. A figure’s “grid” score was determined by mean hierarchical score minus mean egalitarian score. Overall perceived, relative cultural worldviews of the eight community figures were plotted on a group-grid graph.
Non-parametric tests were used to examine levels of trust in the community figures. Medians and interquartile ranges (IQRs) were calculated for trust in each type of community figure, and were compared using the Friedman’s chi-square test which is analogous to a repeated measures ANOVA test for non-parametrically distributed data.Citation43 Next, pairwise comparisons for levels of trust in race-concordant versus discordant figures were performed for: 1) each individual figure’s score, 2) all eight figures’ combined mean score, 3) the two medical authority figures’ (pediatrician, and CDC vaccine scientist) combined mean score, and 4) the other six non-medical authority figures’ combined mean score. All pairwise comparisons were performed using the Wilcoxon rank-sum test. All statistical analyses were completed using Stata software version 13.1 (College Station, TX).
Abbreviations
| CDC | = | Centers for Disease Control and Prevention |
| IQR | = | interquartile range |
| WIC | = | Supplemental Nutrition Program for Women, Infants and Children Supplemental Nutritional |
Disclosure of potential conflicts of interest
Dr. Haimowitz has no financial interest or benefit that has arisen from the direct applications of this research to disclose. Dr. Fu and Ms. Thompson have received funding to support immunization research projects from Pfizer.
Additional information
Funding
References
- Quinn S, Jamison A, Musa D, Hilyard K, Freimuth V. Exploring the continuum of vaccine hesitancy between African American and white adults: Results of a qualitative study. PLoS Curr. 2016 Dec;8. doi:10.1371/currents.outbreaks.3e4a5ea39d8620494e2a2c874a3c4201.
- Brunson EK. The impact of social networks on parents’ vaccination decisions. Pediatrics. 2013;131(5):e1397–1404. doi:10.1542/peds.2012-2452.
- Kennedy A, Sapsis KF, Stokley S, Curtis CR, Gust D. Parental attitudes toward human papillomavirus vaccination: evaluation of an educational intervention, 2008. J Health Commun. 2011;16(3):300–13. doi:10.1080/10810730.2010.532296.
- Serpell L, Green J. Parental decision-making in childhood vaccination. Vaccine. 2006;24(19):4041–46. doi:10.1016/j.vaccine.2006.02.037.
- Galbraith-Gyan KV, Lechuga J, Jenerette CM, Palmer MH, Moore AD, Hamilton JB. HPV vaccine acceptance among African-American mothers and their daughters: an inquiry grounded in culture. Ethn Health. 2017;1–18. doi:10.1080/13557858.2017.1332758.
- Benin AL, Wisler-Scher DJ, Colson E, Shapiro ED, Holmboe ES. Qualitative analysis of mothers’ decision-making about vaccines for infants: the importance of trust. Pediatrics. 2006;117(5):1532–41. doi:10.1542/peds.2005-1728.
- Quinn SC, Jamison A, Freimuth VS, An J, Hancock GR, Musa D. Exploring racial influences on flu vaccine attitudes and behavior: results of a national survey of White and African American adults. Vaccine. 2017;35(8):1167–74. doi:10.1016/j.vaccine.2016.12.046.
- Brach C, Fraser I. Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med Care Res Rev. 2000;57(Suppl 1):181–217. doi:10.1177/1077558700057001S09.
- Fu LY, Zimet GD, Latkin CA, Joseph J. Social networks for HPV vaccine advice among African American parents. J Adolesc Health. In press.
- Joseph NP, Clark JA, Bauchner H, Walsh JP, Mercilus G, Figaro J, Bibbo C, Perkins RB. Knowledge, attitudes, and beliefs regarding HPV vaccination: ethnic and cultural differences between African-American and Haitian immigrant women. Womens Health Issues. 2012;22(6):e571–579. doi:10.1016/j.whi.2012.09.003.
- Kahan DM, Braman D, Cohen GL, Gastil J, Slovic P. Who fears the HPV vaccine, who doesn’t and why? An experimental study of the mechanisms of cultural cognition. Law Hum Behav. 2010;34:501–16. doi:10.1007/s10979-009-9201-0.
- Kahan DM, Braman D, Gaastil J, Slovic P, Mertz CK. Culture and identity-protective cognition: explaining the white-male effect in risk perception. J Empirical Legal Studies. 2007;4(3):465–505. doi:10.1111/j.1740-1461.2007.00097.x.
- Douglas M, Wildavsky A. Risk and culture: an essay on the selection of technical and environmental dangers. Berkeley: University of California Press; 1982.
- Johnson RL, Saha S, Arbelaez JJ, Beach MC, Cooper LA. Racial and ethnic differences in patient perceptions of bias and cultural competence in health care. J Gen Intern Med. 2004;19(2):101–10.
- Laveist TA, Nuru-Jeter A. Is doctor-patient race concordance associated with greater satisfaction with care? J Health Soc Behav. 2002;43(3):296–306.
- Saha S, Komaromy M, Koepsell TD, Bindman AB. Patient-physician racial concordance and the perceived quality and use of health care. Arch Intern Med. 1999;159(9):997–1004.
- Cooper LA, Roter DL, Johnson RL, Ford DE, Steinwachs DM, Powe NR. Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med. 2003;139(11):907–15.
- Street RL Jr., O’Malley KJ, Cooper LA, Haidet P. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6(3):198–205. doi:10.1370/afm.821.
- Cooper-Patrick L, Gallo JJ, Gonzales JJ, Vu HT, Powe NR, Nelson C, Ford DE. Race, gender, and partnership in the patient-physician relationship. JAMA. 1999;282(6):583–89.
- Nierkens V, Hartman MA, Nicolaou M, Vissenberg C, Beune EJAJ, Hosper K, van Valkengoed IG, Stronks K, Derrick GE. Effectiveness of cultural adaptations of interventions aimed at smoking cessation, diet, and/or physical activity in ethnic minorities. a systematic review. PLoS One. 2013;8(10):e73373. doi:10.1371/journal.pone.0073373.
- Larkey LK, Hecht M. A model of effects of narrative as culture-centric health promotion. J Health Commun. 2010;15(2):114–35. doi:10.1080/10810730903528017.
- Dutta MJ, Collins W, Sastry S, Dillard S, Anaele A, Kumar R, Roberson C, Robinson T, Bonu T. A culture-centered community-grounded approach to disseminating health information among African Americans. Health Commun. 2018;1–10. doi:10.1080/10410236.2018.1455626.
- Melvin CL, Jefferson MS, Rice LJ, Nemeth LS, Wessell AM, Nietert PJ, Hughes-Halbert C. A systematic review of lifestyle counseling for diverse patients in primary care. Prev Med. 2017;100:67–75. doi:10.1016/j.ypmed.2017.03.020.
- Mosdol A, Lidal IB, Straumann GH, Vist GE. Targeted mass media interventions promoting healthy behaviours to reduce risk of non-communicable diseases in adult, ethnic minorities. Cochrane Database Syst Rev. 2017;2:Cd011683.
- Liu J, Davidson E, Bhopal R, White M, Johnson M, Netto G, Deverill M, Sheikh A. Adapting health promotion interventions to meet the needs of ethnic minority groups: mixed-methods evidence synthesis. Health Technol Assess. 2012;16(44):1–469. doi:10.3310/hta16440.
- Hopfer S. Effects of a narrative HPV vaccination intervention aimed at reaching college women: a randomized controlled trial. Prev Sci. 2012;13(2):173–82. doi:10.1007/s11121-011-0254-1.
- Hopfer S, Clippard JR. College women’s HPV vaccine decision narratives. Qual Health Res. 2011;21(2):262–77. doi:10.1177/1049732310383868.
- Fu LY, Zimet GD, Latkin CA, Joseph JG. Associations of trust and healthcare provider advice with HPV vaccine acceptance among African American parents. Vaccine. 2017;35(5):802–07. doi:10.1016/j.vaccine.2016.12.045.
- Gust D, Brown C, Sheedy K, Hibbs B, Weaver D, Nowak G. Immunization attitudes and beliefs among parents: beyond a dichotomous perspective. Am J Health Behav. 2005;29:81–92.
- Leask J, Kinnersley P, Jackson C, Cheater F, Bedford H, Rowles G. Communicating with parents about vaccination: a framework for health professionals. BMC Pediatr. 2012;12:154. doi:10.1186/1471-2431-12-34.
- Ojeaga A, Alema-Mensah E, Rivers D, Azonobi I, Rivers B. Racial disparities in HPV-related knowledge, attitudes, and beliefs among African American and white women in the USA. J Cancer Educ. 2019;34(1):66–72.
- Perkins RB, Apte G, Marquez C, Porter C, Belizaire M, Clark JA, Pierre-Joseph N. Factors affecting human papillomavirus vaccine use among White, Black and Latino parents of sons. Pediatr Infect Dis J. 2013;32(1):e38–44. doi:10.1097/INF.0b013e31826f53e3.
- Sanders Thompson VL, Arnold LD, Notaro SR. African American parents’ HPV vaccination intent and concerns. J Health Care Poor Underserved. 2012;23(1):290–301. doi:10.1353/hpu.2012.0007.
- Jacobs EA, Rolle I, Ferrans CE, Whitaker EE, Warnecke RB. Understanding African Americans’ views of the trustworthiness of physicians. J Gen Intern Med. 2006;21(6):642–47. doi:10.1111/j.1525-1497.2006.00485.x.
- Mellerson JL, Maxwell CB, Knighton CL, Kriss JL, Seither R, Black CL. Vaccination coverage for selected vaccines and exemption rates among children in Kindergarten - United States, 2017–18 school year. MMWR Morb Mortal Wkly Rep. 2018;67(40):1115–22. doi:10.15585/mmwr.mm6740a3.
- Opel DJ, Mangione-Smith R, Taylor JA, Korfiatis C, Wiese C, Catz S, Martin DP. Development of a survey to identify vaccine-hesitant parents: the parent attitudes about childhood vaccines survey. Hum Vaccin. 2011;7(4):419–25.
- Centers for Disease Control and Prevention. Estimates of flu vaccination coverage among children-United States, 2017–18 flu season. 2018 [ accessed 2018 Dec. 18]. www.cdc.gov/flu/fluvaxview/coverage-1718estimates-children.htm#figure1.
- Walker TY, Elam-Evans LD, Yankey D, Markowitz LE, Williams CL, Mbaeyi SA, Fredua B, Stokley S. National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years - United States, 2017. MMWR Morb Mortal Wkly Rep. 2018;67(33):909–17. doi:10.15585/mmwr.mm6733a1.
- Birkhead GS, Cicirello HG, Talarico J. The impact of WIC and AFDC in screening and delivering childhood immunizations. J Public Health Manag Pract. 1996;2:26–33.
- Cunningham-Erves J, Talbott LL, O’Neal MR, Ivankova NV, Wallston KA. Development of a theory-based, sociocultural instrument to assess black maternal intentions to vaccinate their daughters aged 9 to 12 against HPV. J Cancer Educ. 2016;31(3):514–21. doi:10.1007/s13187-015-0867-3.
- Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Sources and perceived credibility of vaccine-safety information for parents. Pediatrics. 2011;127(Suppl 1):S107–112. doi:10.1542/peds.2010-1722P.
- Thomas T, Blumling A, Delaney A. The influence of religiosity and spirituality on rural parents’ health decision making and human papillomavirus vaccine choices. ANS Adv Nurs Sci. 2015;38(4):E1–e12. doi:10.1097/ANS.0000000000000094.
- Friedman M. The use of ranks to avoid the assumption of normality implicit in the analysis of variance. J Am Stat Assoc. 1937;32(200):675–701. doi:10.1080/01621459.1937.10503522.