
ABSTRACT
Allergen immunotherapy (AIT) is a very useful therapy for allergic rhinitis. However, some patients do not achieve the expected results. The aim of the study was to investigate the potential factors that could affect the result, either good or poor, from AIT.
Methods: A retrospective analysis of 1624 patients with allergic rhinitis who underwent AIT and 1519 matched patients who underwent only symptomatic therapy (without AIT) was performed. Symptoms, medications scores and quality of life related to allergic diseases before and after therapy were recorded. Cluster analysis on all of the patients was performed to find any associations between responsiveness to therapy and the analyzed parameters. Responsiveness to therapy was assessed by the Mailing criteria.
Results: A total of 1266 (77.8%) patients from the AIT group met the criterion of 30% or greater improvement, and 1061 (65.2%) of these patients met the threshold of 60% or greater improvement according to the Mailing criteria. Patients who had a frequently better response to AIT were highly represented in the two clusters. There were subjects with a short history of allergic rhinitis and concomitant allergy to grass pollen or house dust mites. Patients with a prolonged duration of allergic rhinitis before therapy and with polysensitization were more frequently worse responders to AIT.
Conclusion: Responsiveness to therapy, including that to AIT, is difficult to assess. However, there were associations suggesting that short-term allergic rhinitis and monovalent allergies to grass pollen or mites could correspond to a better response to AIT.
Introduction
Allergen immunotherapy (AIT) is one of the most important tools used for the treatment of some allergic diseases. In recent years, many studies have confirmed the clinical safety and efficacy of AIT in the treatment of different types of allergies in children and adults.Citation1,Citation2 Allergic rhinitis and some cases of allergic asthma and hypersensitivity to wasp or bee venom are the most popular indications for AIT use.Citation1,Citation2 Many guidelines recommend such therapy as the basic way to improve allergy symptoms and to stop the further development of allergies and the transformation of allergic rhinitis to bronchial asthma; AIT may also be indicated to prevent new sensitizations.Citation2,Citation3 However, many questions in research areas addressing new vaccination methods, desensitization to new allergens, methods assessing the efficacy of AIT (searching for new immunological and/or clinical parameters), and explanations for why some patients who are correctly prescribed AIT have no response to the treatment remain. Answering the last question is not easy. Many factors influence AIT, including the suitable recognition of causative allergens, sufficient duration of AIT and administration of adequate cumulative doses of allergens during the course of AIT.Citation3,Citation4
Unfortunately, many other unrecognized factors could be responsible for the efficiency or lack of efficiency following AIT. There are only a few studies that have analyzed this problem. Patients who are nonresponders are frequently not assessed for why they did not respond to AIT. Sometimes, AIT failing to be effective can lead to patients withdrawing from proper treatment.
The aim of the study was to find other potential factors that influence the response to AIT, either good or poor, in patients with allergic rhinitis.
Results
In the final analysis, 1266 (77.8%) patients from the AIT group met the criterion of showing 30% or better improvement, and 1061 (65.2%) of these patients showed 60% or better improvement. Compared to the AIT group, the control group had significantly fewer participants who met the criteria of 30% and 60% improvement: 351 (23.1%) for 30% and 212 (14%) for 60%.
The detailed changes in the analyzed parameters are presented in .
Table 1. Changes in the analyzed parameters in the patients after AIT and in those in the control group
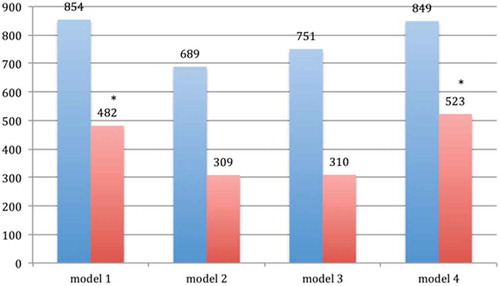
Based on the cluster analysis, four models were evaluated. The characteristics of the models are as follows:
Model 1: predominantly men, frequently younger than 35 years of age, with moderate or mild intermittent allergic rhinitis, with better response to treatment (more patients achieved ≥30% or ≥60% improvement from baseline), and high prevalence of allergy to grass pollen and/or house dust mites but also having allergies to other allergens, and short duration of allergic rhinitis before therapy;
Model 2: predominantly women, smokers or former smokers, with moderate or mild perennial allergic rhinitis, high prevalence of allergy to tree pollen and/or house dust mites, and worse response to treatment based on many of the analyzed parameters (<30% improvement from baseline);
Model 3: predominantly women, with polysensitization, high prevalence of allergy to mugwort and/or house dust mites and/or cats and/or Alternaria, prolonged history of allergic rhinitis before therapy, and worse response to treatment (<30% improvement from baseline); and
Model 4: predominantly young patients, with severe perennial allergic rhinitis and a spectrum of allergy similar to that described in model 1, with good response to treatment (≥30% improvement from baseline), and short duration of disease.
Patients who received AIT, especially for grass pollen and/or house dust mites, were highly represented in models 1 and 4 ().
Figure 1. Flow chart of the process used to obtain data
The detailed data described in the cluster models are presented in .
Table 2. Description of individual cluster models
A similar cluster analysis, but one that was limited to patients who received AIT (n = 1624), revealed six further models (A–F) that are mentioned below. In this analysis, the additional criteria of changes of ≥30% and ≥60% in specific IgE (decreasing) and IgG4 (increasing) between baseline and after AIT were used.
Of all the analyzed patients (n = 1456) who underwent AIT, the criterion of ≥30% for specific IgE was met in 945 (64.9%) patients and the criterion of ≥60% was met in 459 (31.5%). For specific IgG4, these criteria of 30% and 60% improvement were met in 1178 (80.9%) and 874 (60.1%) patients, respectively.
There were the following models:
Model A (n = 257): patients <18 years of age, moderate/mild allergic rhinitis without asthma, no family history of allergies, short duration of allergic rhinitis, allergy to grass pollen;
Model B (n = 212): men, moderate/mild allergic rhinitis, significant increase in the concentration of IgG4, allergy to grass pollen and/or birch;
Model C (n = 223): patients >18 years of age, severe allergic rhinitis, allergic asthma, prolonged duration of allergic disease, no changes in specific IgE concentration against desensitized allergen during AIT;
Model D (n = 211): women, moderate/mild rhinitis without asthma and with atopic dermatitis, allergy to house dust mites, significantly increased concentrations of IgG4 and SCIT;
Model E (n = 356): men over 35 years of age, severe allergic rhinitis, atopic dermatitis, prolonged duration of allergy, polysensitization, SLIT;
Model F (n = 365): patients <18 years of age, moderate/mild allergic rhinitis, prolonged duration of allergy, SCIT, significantly increased concentration of IgG4;
The patients with a good response to AIT (criterion: improvement ≥ 30%) were highly represented in model A (69%), model B (72%) and model F (78%). Patients with a very good response (criterion: improvement ≥ 60%) were highly represented in model F (77%).
Patients who did not respond to AIT were highly represented in model E (83%) and model D (74%). In model C, the proportions of responding and nonresponding patients were 43% and 57%, respectively.
Type of allergic disease
A total of 76% of patients with allergic rhinitis (severe, moderate/mild), 63% with allergic rhinitis with concomitant asthma and only 39% with allergic rhinitis and concomitant atopic dermatitis with or without asthma met the criterion of a 30% minimum improvement.
Duration of allergic rhinitis
Patients with a short-term history of allergic rhinitis before therapy (cutoff: < 3 years) had a higher odds of obtaining good results of AIT according to the criteria, OR (odds ratio) = 2.35 (95%CI: 2.18–2.47), than those who had a longer medical history of it.
Monosensitization vs. polysensitization
Monosensitized patients had a higher odds of obtaining good results of AIT than polysensitized patients, OR = 3.11 (95%CI: 2.98–3.32).
Methods of AIT
After AIT, 210 (12.9%) patients received sublingual immunotherapy (SLIT), and 1414 (87.1%) received injection immunotherapy (SCIT). The criterion of a minimum improvement of 30% was met in 139 (66.2%) patients after undergoing SLIT and 1046 after undergoing SCIT (74%). For the criterion of a minimum improvement of 60%, 108 (51.4%) patients met the criterion after undergoing SLIT and 989 (70%) patients met the criterion after undergoing SCIT.
Type of allergen
The criteria of 30% and 60% improvement were most often obtained by patients after AIT with allergies to grass pollen (84% and 78%, respectively), birch (72% and 63%, respectively) and house dust mites (72% and 63%, respectively). Patients who underwent AIT with allergies to Alternaria obtained the worst results, 47% and 38%, respectively; those with allergies to cats, 51% and 32%, respectively; and those with allergies to mugwort, 54% and 28%, respectively.
Discussion
The obtained results confirm the importance of AIT in the treatment of allergic rhinitis with or without concomitant allergic asthma. Consistent with other authors and guidelines, the patients in our study achieved success after AIT when they clearly met the AIT qualification criteria.Citation1,Citation4 The efficacy criteria that were used were similar according to the Mailing criteria.Citation5 Most of the studied patients met the criteria of showing a 30% minimum improvement, and many of them also showed a 60% or better improvement. This can be proof that there is a need to find more restrictive parameters to assess the efficacy of AIT. The Mailing criteria and the newer EAACI recommendation (>20% improvement) seem to be insufficient. Would the Mailing criterion of an improvement of better than 60% be a better tool? What kind of detailed parameters should be used to calculate the final improvement? These questions still need further investigation.
However, based on the above criteria, typical symptomatic treatment without AIT was presented as yielding a very poor efficacy regardless of the type of analyzed allergy compared to immunotherapy.
In the first cluster analysis, the associations between a good response to AIT and severe or moderate and short-term allergic rhinitis and concomitant allergy to grass pollen and/or house dust mites were noticed. These observations are consistent with the present guidelines and recommendations for AIT.Citation6-Citation8 In contrast, polysensitization and prolonged time of allergic rhinitis before therapy were connected with a worse result after AIT.
The analysis that focused on only patients who underwent immunotherapy revealed associations between a ‘good response’ to AIT and a relatively young age of patients, a short history of allergic rhinitis, concomitant allergy to grass pollen and/or house dust mites and a significant increase in the serum concentration of IgG4. On the other hand, patients who were polysensitized, had concomitant atopic dermatitis and a prolonged duration of allergic rhinitis seemed to be worse responders to AIT. These results generally align with other opinions, except for those on atopic dermatitis.Citation2-Citation4 Perhaps, the coexistence of atopic dermatitis with intensive and nonspecific IgE reactions can impair the induction of immune tolerance during AIT.
There are only a few studies that have tried to analyze the characteristics of patients who are good responders to AIT. Goth et al. performed a cluster analysis that revealed a positive correlation between serum Th1/Th2 cytokines and other cytokines/chemokines in highly responsive patients following SLIT.Citation9 Gueguen et al. confirmed that a combination of 5 markers predominantly expressed by blood DCs (i.e., C1Q and CD141) or that are shared with lymphoid cells (i.e., FcγRIIIA, GATA3 and RIPK4), reflect changes in the balance of regulatory/proallergic responses in the peripheral blood and can be used to monitor the efficacy of AIT as early as after 2 months of treatmentCitation10. However, this study analyzed only immunological parameters without clinical features.
It seems that injection with AIT was more effective than the sublingual treatment and that its efficacy was especially visible for the criterion of ≥60% improvement. However, it should be noted that the group that received SLIT had a significantly smaller number of patients in this study, which may affect the statistical analysis. Therefore, further studies with a larger group of patients who underwent SLIT are needed.
There are some limitations to this study: this was a retrospective analysis that included the possibility of therapy assessment by patients and doctors, and the relatively low number of patients treated for allergies to Alternaria and cats could have influenced the negative final results of whether patients responded to AIT for those allergens.
Taking these limitations into account, it seems that such findings and further studies, especially prospective studies, could provide new information for the better identification of patients who would respond well to AIT to obtain a better treatment effect.
Material and methods
Patients
This study was a multicentre, retrospective, randomized analysis of patients who underwent AIT for allergic rhinitis and/or concomitant asthma. The following were the inclusion criteria:
age between 12 and 75 years;
confirmed allergic rhinitis to common allergens: D. pteronyssinus, D. farinae and/or hazel, birch, alder, grass, and mugwort pollen, as well as combinations of the above allergens, or cats;
intermittent or persistent allergic rhinitis according to ARIACitation12 without significant improvement after symptomatic treatment and qualified AIT;
completion of a minimum of three years of preseasonal, coseasonal or perennial SLIT or SCIT;
lack of other chronic diseases;
consent for data publication; and
ability to complete the survey.
The diagnosis of allergic rhinitis and the decision of performing AIT were made based on positive diagnostic skin tests and a medical history that confirmed the relation between allergic nasal symptoms and the expected allergen (allergens).
Additionally, nasal provocation tests (NPT) were performed using an anterior active rhinomanometry (Rhinotest MP-500, Germany) or acoustic rhinometry (acoustic rhinometer, GM Instruments A1, ProVita, Poland). NPT were used when there was doubt about which expected allergen induced the nasal symptoms. NPT were assessed based on the guidelines of the European Academy of Allergy and Immunology: positive symptoms score and/or decrease in nasal resistance.Citation13
Patients were considered as polysensitized when their clinical rhinitis symptoms were induced by more than one of the allergen groups mentioned above.
The exclusion criteria were a lack of completion of AIT, lack of consent and lack of full therapy documentation.
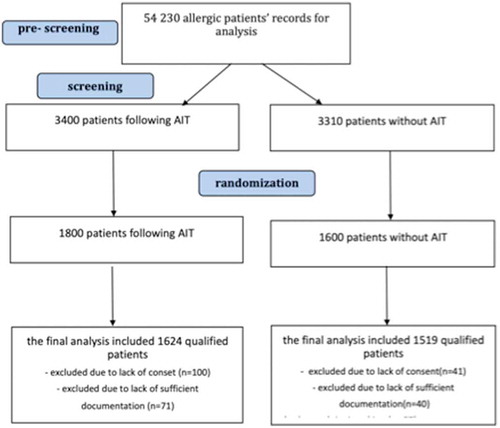
The control group comprised patients who fulfilled all inclusion criteria except point 4. They were only on symptomatic therapy without AIT. The prescreening and screening steps for the patients included in the further analysis are shown in a flow chart (). The final number of included patients was based on a power calculation that took into account the expected effect size, the standard deviation of the outcomes and the ordinal variables for the comparative study.
Figure 2. Distribution of patients after AIT in the individual models after cluster analysis
The randomization procedure (random selection) relied on the use of computer-generated numbers by means of a coin-flip generator (Excel, version 14.3.0, 2015, Microsoft Corporation, USA). In total, 1624 patients were included in the AIT-administered study group, and 1519 were included in the control group. The patient characteristics of both groups are presented in .
Table 3. Patient characteristics of the study and control groups
Method of analysis
The following patient data were analyzed:
medical history, especially history that was focused on allergic diseases;
medical examination with laryngological and dermatological assessments;
results of skin prick tests with inhalant allergens: D. pteronyssinus, D. farinae, pollen from grass and cereals, birch, hazel, alder, mugwort, and plantain, Alternaria, Cladosporium, cats and dogs. A positive result of the test was based on the presence of wheals of 3 mm or greater in diameter and concomitant wheals of 5 mm or greater in diameter from histamine;Citation14
results of specific IgE (sIgE) and IgG4 against allergens in blood serum mentioned above (uni-CAP, Thermo Fisher, Sweden), which were measured before and after therapy; the results were considered positive when the sIgE concentration was greater than 0.35 kU/L, which was according to the manufacturer’s recommendation; IgG4 was measured in mg/L. These results were analyzed only when AIT was performed.
data on the patient’s clinical symptoms monitored during AIT or symptomatic treatment during the allergen exposure period (seasonal for pollen allergy, perennial for other allergens). The severity of ocular, nasal and asthmatic symptoms was recorded using a VAS scale of 10 cm increments. Each symptom was categorized as ‘mild’ (VAS: 0–30 cm), ‘moderate’ (VAS: >30 cm and ≤ 70 cm), or ‘severe’ (VAS > 70 cm);Citation15 patients filled in a diary every day, and the data were averaged and presented with standard deviation every month; the patients recorded the use of medications on their diary cards, and a specific weekly score was assigned (1 point: used only nasal corticosteroids or eye drops at a minimum of one day per week; 2 points: the previous therapy plus one tablet of levocetirizine at a minimum of one per day; 3 points: the previous therapies plus one 4 mg methylprednisolone tablet at a minimum of one per day). SMS were calculated for each patient after every year of treatment; and
results of questionnaires: RSS and/or ASS, RQLQ and/or QOL. The questionnaires were administered after every year of treatment (AIT or only symptomatic therapy)Citation11,Citation12,Citation16,Citation17
Analysis procedures 2–6 were used before the start of treatment and after 3 or 5 years of therapy for each patient (AIT or only symptomatic therapy). The efficacy of therapy was assessed based on the criterion of a minimum of 30% (mild) or 60% (strong) improvement at the same time for all parameters: SMS, RSS, ASS and RQLQ and QOL compared between the start of treatment and after treatment (3–5 years later).
Statistical analysis
The statistical analysis was performed using Statistica version 8.12 (SoftPOl, Poland). Student’s t-test for unpaired data was used to analyze differences in the medication and symptom scores and differences in the changes in IgE and IgG4 serum concentrations before and just after AIT. ANOVA or the Wilcoxon test was used to analyze other differences between groups. A cluster analysis was performed to identify the factors (models) associated with responding to AIT or symptomatic therapy. The k-means method was used. In the cluster analysis, the following parameters were taken into consideration: sex, age, type of allergic disease, type of allergen (allergens), monosensitization or polysensitization, mean duration of disease before treatment, mean duration of treatment, type of AIT, mean time of AIT, mean time of symptomatic treatment, and percent change in the results of the SMS, RSS, ASS, RQLQ and QOL before and after treatment. Odds ratios with the 95%CI were calculated for some of the parameters.
Differences were considered significant at P< .05. The study was approved by the local ethics committees of the Medical University of Silesia in Poland. All patients signed an informed consent form.
Conclusion
AIT is significantly more effective than symptomatic therapy in the treatment of allergic rhinitis. The association between a better response to AIT and a short-term history of allergic rhinitis with concomitant allergy to grass pollen and/or house dust mites was noticed.
Patients with coexisting atopic dermatitis, polysensitization, allergies to Alternaria, mugwort or cats and a prolonged duration of allergic disease seem to have a worse response to AIT.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Abbreviations
| AIT | = | Allergen immunotherapy |
| ASS | = | Asthma Symptom Score |
| HDM | = | House dust mites |
| NPT | = | Nasal provocation test |
| PANN | = | Persistent allergic rhinitis |
| QOL | = | Asthma-related quality of life |
| RSS | = | Rhinitis symptom score |
| RQLQ | = | Rhinoconjunctivitis quality of life questionnaire |
| SANN | = | Intermittent allergic rhinitis |
| SCIT | = | Injection allergen immunotherapy |
| sIgE | = | Allergen-specific immunoglobulin E |
| SMS | = | Combined symptoms medication score |
| SLIT | = | Sublingual allergen immunotherapy |
| TCRS | = | Combined rhinitis score |
| VAS | = | Visual analog scale |
Related Research Data
References
- Nurmatov U, Dhami S, Arasi S, Roberts G, Pfaar O, Muraro A, Ansotegui IJ, Calderon M, Cingi C, Durham S, et al. Allergen immunotherapy for allergic rhinoconjunctivitis: a systematic overview of systematic reviews. Clin Transl Allergy. 2017 Aug 8;7:24. doi:10.1186/s13601-017-0159-6. eCollection 2017.
- Jutel M, Agache I, Bonini S, Burks AW, Calderon M, Canonica W, Cox L, Demoly P, Frew AJ, O’Hehir R, et al. International consensus on allergy immunotherapy. J Allergy Clin Immunol. 2015 Sep;136(3):556–68. doi:10.1016/j.jaci.2015.04.047. [ Epub 2015 Jul 7].
- Jutel M, Agache I, Bonini S, Burks AW, Calderon M, Canonica W, Cox L, Demoly P, Frew AJ, O’Hehir R, et al. International consensus on allergen immunotherapy II: mechanisms, standardization, and pharmacoeconomics. J Allergy Clin Immunol. 2016 Feb;137(2):358–68. doi:10.1016/j.jaci.2015.12.1300.
- Calderón MA, Casale TB, Togias A, Bousquet J, Durham SR, Demoly P. Allergen-specific immunotherapy for respiratory allergies: from meta-analysis to registration and beyond. J Allergy Clin Immunol. 2011 Apr;127(4):859. doi:10.1016/j.jaci.2011.01.057.
- Mailing HJ. Immunotherapy as an effective tool in allergy treatment. Allergy. 1998;53:461–72. doi:10.1111/j.1398-9995.1998.tb04082.x.
- Dhami S, Nurmatov U, Arasi S, Khan T, Asaria M, Zaman H, Agarwal A, Netuveli G, Roberts G, Pfaar O, et al. Allergen immunotherapy for allergic rhinoconjunctivitis: a systematic review and meta-analysis. Allergy. 2017 Nov;72(11):1597–631. doi:10.1111/all.13201.
- Dhami S, Kakourou A, Asamoah F, Agache I, Lau S. Jutel M, Muraro A, Roberts G, Akdis CA, Bonini M, et al. Allergen immunotherapy for allergic asthma: a systematic review and meta-analysis. Allergy. 2017;72(12):1825–48. doi:10.1111/all.13208.
- Qi S, Chen H, Huang N, Li W, Liu G, Wang Y, Hu L, Wang X, Zhang W, Zhu R. Early intervention improves clinical responses to house dust mite immunotherapy in allergic rhinitis patients. Int Arch Allergy Immunol. 2016;171(3–4):234–40. doi:10.1159/000452333.
- Gotoh M, Kaminuma O, Nakaya A, Katayama K, Motoi Y, Watanabe N, Saeki M, Nishimura T, Kitamura N, Yamaoka K, et al. Identification of biomarker sets for predicting the efficacy of sublingual immunotherapy against pollen-induced allergic rhinitis. Int Immunol. 2017;29(6):291–300. doi:10.1093/intimm/dxx034.
- Gueguen C, Bouley J, Moussu H, Luce S, Duchateau M, Chamot-Rooke J, Pallardy M, Lombardi V, Nony E, Baron-Bodo V, et al. Changes in markers associated with dendritic cells driving the differentiation of either TH2 cells or regulatory T cells correlate with clinical benefit during allergen immunotherapy. Allergy Clin Immunol. 2016;137(2):545–58. doi:10.1016/j.jaci.2015.09.015.
- Canonica G W, Baena-Cagnani CE, Bousquet J, Bousquet PJ, Lockey RF, Malling HJ, Passalacqua G, Potter P, Valovirta E Recommendations for standardization of clinical trials with allergen specific immunotherapy for respiratory allergy. A statement of a world allergy organization (WAO) taskforce. Allergy. 2007 Mar;62(3):317–24. doi:10.1111/j.1398-9995.2007.01456.x.
- Bousquet J, Khaltaev N, Cruz AA. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the world health organization, GA(2)LEN and AllerGen). Allergy. 2008;63:8–160.
- Auge J, Vent J, Agache I, Airaksinen L, Campo Mozo P, Chaker A, Cingi C, Durham S, Fokkens W, Gevaert P, et al. EAACI position paper on the standardization of nasal allergen challenges. Allergy. 2018;8:1597–608. doi:10.1111/all.2018.73.issue-8.
- Heinzerling LM, Burbach GJ, Edenharter G, Bachert C, Bindslev-Jensen C, Bonini S, Bousquet J, Bousquet-Rouanet L, Bousquet PJ, Bresciani M, et al. GA(2)LEN skin test study I: GA(2)LEN harmonization of skin prick testing: novel sensitization patterns for inhalant allergens in Europe. Allergy. 2009;64:1498–506.
- Bousquet PJ, Combescure C, Neukirch F. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy. 2007;62:367–72. doi:10.1111/j.1398-9995.2007.01456.x.
- Global Initiative for asthma. Gina report. Global strategy for Asthma Management and Prevention 2008. [accessed 2019 Jan 21]. http://www.ginasthma.org
- Juniper E, Styles J Measurement of helath- related quality of life & asthma control. [accessed 2018 Dec 10]. http://www.qotech.co.uk