
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background: The varicella vaccine (VarV) is not included in the national childhood immunization schedules in China, although 2-dose VarV (VarV2) were recommended for children at 1 and 4 years of age in Hangzhou since 2014. However, the reported incremental vaccine effectiveness (VE) of VarV2 varies widely among studies. We described the epidemiological characteristics of varicella in Hangzhou, assessed the VE of VarV, so as to provide scientific evidence on optimization and adjustment of immunization strategies for varicella prevention in China.
Methods: All varicella cases diagnosed in a hospital in Hangzhou are reported to China Information System for Disease Control and Prevention (CISDCP). The demographic information of reported varicella cases onset from January 1 to December 31, 2019 was extracted from CISDCP on Jan 31, 2020. The demographic information was obtained from the information system of the National Center for Disease Prevention and Control. We conducted a 1:1 matched case–control study to assess the effectiveness of VarV. Participant data were collected with standardized questionnaires. VarV vaccination status was checked by using Hangzhou Immunization Information System (HZIIS).
Results: A total of 11,813 varicella cases were reported in Hangzhou, China, 2019, without any death. Annual estimated incidence of varicella was 120 cases per 100,000 populations in 2019. The overall estimated incidence rate of varicella was high, especially for persons aged 10–19 years old and in suburb areas. The seasonal pattern was apparent, mostly due to the cases among students and children in kindergarten. In total, 218 varicella cases and 218 matched controls were included for evaluating the VE of VarV. VarV vaccination produced a high level of protection against varicella, while VE of VarV2 was even better. VE of VarV1 was 91.0% (95%CI: 81.6%-95.8%), and VE was 98.0% (95.5%-99.2%) for VarV2.
Conclusion: Continuous monitoring and management of varicella cases is necessary, especially in those endemic areas, high-risk populations, and peak periods; a 2-dose VarV strategy is highly recommended, and relevant health institutions should consider the inclusion of VarV in the national immunization program to better control varicella epidemic and reduce the burden of varicella.
1. Introduction
Varicella is a highly contagious disease caused by varicella-zoster virus (VZV) that is mainly transmitted from person to person by direct contact with the varicella or herpes zoster rash, inhalation of aerosolized droplets from respiratory tract secretions of patients with varicella. In the absence of varicella vaccine (VarV), it affects nearly every person by mid-adulthood. At present, with the annual average incidence of varicella from 2005 to 2015 increased by 30%,Citation1 the number of varicella patients is still on the rise in China. The damage and disease burden caused by varicella in China is mainly manifested in the incidence of varicella and the cost of direct medical services and other indirect costs,Citation2 and is becoming increasingly severe. However, unlike the national infectious diseases listed by the Ministry of Health, varicella has not been monitored and managed in a systematic way. The World Health Organization (WHO) has suggested that a systematic disease surveillance system should be established to assess the disease burden of varicella before introducing routine childhood VarV immunization, and sustained and appropriate monitoring should be carried out after the vaccine is included in the immunization program.Citation3 Effective monitoring of the varicella epidemic situation is helpful to access the epidemic trends and understand the epidemiological characteristics of varicella, and further provides the basis for the formulation of prevention and control strategies in the future.Citation1,Citation2,Citation4 In 2019, required by the Hangzhou Bureau of Health, all medical agencies should report varicella cases via China Information System for Disease Control and Prevention (CISDCP) within 24 h.
Vaccination is the most effective and reliable method to prevent varicella. In March 1995, the VarV was licensed for use in the United States, with a single dose of VarV vaccinated at 12 months old,Citation5 and converted the VarV vaccination guidelines to 2-dose schedule (at ages 12–15 months and 4–6 years) in 2006.Citation6 Meanwhile, VarV was used to prevent varicella in China since 1997, which was available in Hangzhou with the immunization schedule of 1-dose for children over 1 year old since 1999. Then, 2-dose VarV was recommended for children at 1 and 4 years of age in Hangzhou, China since July, 2014.Citation7 Nonetheless, VarV needs to be paid by vaccine recipients as it was not included in Expanded Program on Immunization (EPI), which is not free. In some countries with high immunization coverage rate, such as America, Canada, Australia, and Uruguay, a sharp decline in the morbidity of varicella and varicella-related hospitalization and complication rates has been reported since the introduction of VarV into routine immunization programs.Citation8,Citation9 After a single dose of VarV, effectiveness against all forms of varicella is around 76% to 85% and reaches up to 100% after two doses.Citation10 Children in Hangzhou had overall high vaccination coverage of 1-dose VarV (VarV1), and the coverage of 2-dose VarV (VarV2) was increasing by year.Citation11 Limited investigations have been done to assess the effectiveness of VarV2 vaccination due to the immunization schedule which is not widely recommended nationwide. Many outbreak investigations reported that the VarV2 immunization schedule provided improved protection against varicella, while same studies showed the vaccine effectiveness (VE) of one dose and two doses were similar, in which varicella VE was calculated using the equation: (1-attack rate among students who received 1- or 2-doses of vaccine/attack rate among unvaccinated students without a history of varicella)×100%.Citation12
In this study, we aim to describe the epidemiological characteristics of varicella in Hangzhou, China; assess overall and incremental vaccine effectiveness of 1-dose and 2-dose VarV vaccination; and delineate the correlation between varicella incidence characteristics and VarV vaccination status, so as to provide scientific evidence on optimization and adjustment of immunization strategies for VarV prevention in China.
2. Materials and methods
2.1. Setting
Hangzhou is an economically developed city in Zhejiang Province of China, with a population of about 9,800,000 in 15 districts. There are approximately 200 vaccination clinics providing VarV vaccination in the city. Since 2005, Hangzhou Center for Disease Control and Prevention (HZCDC) created Hangzhou Immunization Information System (HZIIS), which is a computerized information system that contains immunization data and vaccine’s demographic information for Hangzhou.
2.2. Target population and data resources
Surveillance of varicella in Hangzhou is passive, and since 2019, all practitioners in medical agencies in Hangzhou have been required to report varicella cases by CISDCP within 24 h, once the diagnosis of varicella was made. Confirmed cases are clinically diagnosed cases and laboratory-confirmed cases. The demographic information and the disease onset records of varicella case with disease onset from January 1 to December 31, 2019 were extracted from CISDCP on Jan 31, 2020. The demographic information included gender, date of birth, occupation and current address. The census data were obtained from the information system of the National Center for Disease Prevention and Control.
2.3. Assessment of the effectiveness of VarV vaccination
We used 1:1 matched case–control study to assess the effectiveness of VarV vaccination. The case with disease onset from January 1 to December 31, 2019 born after 2008 in a kindergarten or primary school outbreak was included. For each case, we enrolled a control: a subject with the same gender, age and classroom as the case. We investigated the control to confirm that he had never have varicella disease. Participant data were collected with standardized questionnaires. VarV vaccination status (vaccination date and dose) was checked by using HZIIS.
A sample size of at least 205 pairs of cases and controls was included based on the formula:;
(p0 = 53.4%; α = 0.05; β = 0.10; Uα = 1.96; Uβ = 1.28; OR = 2; p= OR/(1+ OR); p1 = p0OR/[1+ p0(OR-1)]; q1 = 1-p1; q0 = 1-p0.)
2.4. Statistical analysis
Demographic characteristics of varicella cases were analyzed. Overall, age-specific and district-specific estimated incidence rates of varicella were calculated. Data were collected using Microsoft Office Excel (version2010) and were analyzed using SPSS for Windows, version 17.0 (SPSS Inc., Chicago, IL, USA). Pearson chi-squared test was used to compare proportions of incidences. In the matched case–control study, odds ratios (OR) and 95% confidence intervals (CIs) were calculated via Logistic regression. VE of VarV was estimated by using the formula developed by Greenwood and Yule (1 − relative risk [RR]). A value of P< .05 (2-sided) was considered statistically significant.
3. Results
3.1. Demographic characteristics
A total of 11,813 varicella cases were reported in Hangzhou, China, 2019, without any death. Annual estimated incidence of varicella was 120 cases per 100,000 populations in 2019. Of the 11,813 cases, 6,209 (52.6%) were male and 5,604 (47.4%) were female. The majority (7,139, 60.4%) of the cases occurred among students and children in kindergarten. The median age of cases was 15 years (IQR 10–24). A total of 7, 826 cases (66.3%) were <20 years of age, while 10–14 years (2,893, 24.5%) and 15–19 years (2,299, 19.5%) were the main onset age. The incidence of varicella remained relatively stable for children under 8 years old, but increased from 8 years age group to 10–14 years age group, and then declined. The incidence was higher for children in 10–14 years age group (856/100,000) and 15–19 years (701/100,000).
3.2. Geographic distribution
Most of the varicella cases in 2019 occurred in suburb areas (6101, 51.7%), followed by in urban areas (3698, 31.3%) and rural areas (2014, 17.1%). Meanwhile, the incidence rate of varicella was different by geographic areas. It was higher in suburb areas (150/100,000) than in urban areas (117/100,000) and rural areas (78/100,000)(P< .001).
3.3. Seasonal distribution
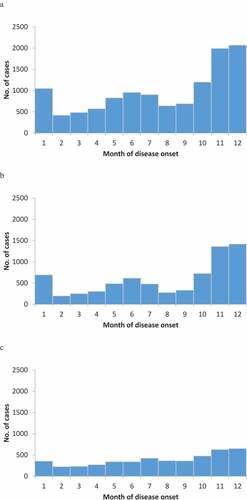
A seasonal pattern was observed for all varicella cases in 2019 (), with the high peak during the winter months and another peak from May to July. The same seasonal trend was seen for the cases among students and children in kindergarten. The seasonality for cases among non-student adults, preschool children and infants was not so apparent.
Figure 1. Number of varicella cases and incidence of varicella by age in Hangzhou, 2019
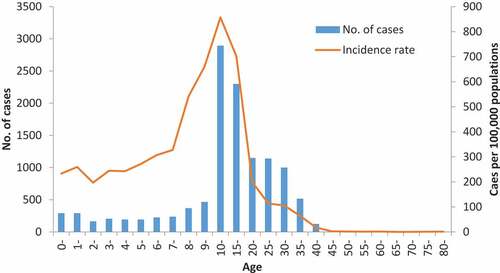
Figure 2. Distributions of varicella cases by month and by occupation in Hangzhou, 2019. (A) All cases (n = 11,813). (B) Cases among students and children in kindergarten (n = 7,139). (C) Cases among non-student adults, preschool children and infants (n = 4,674)
3.4. VarV vaccination effectiveness
In total, 218 varicella cases and 218 matched controls were included for evaluating the VE of VarV. There were 54.1% males (118 pairs) and 45.9% females (100 pairs). The ages were between 6 and 12 years, and the average age was 9.84 ± 1.40 years old. All subjects were from 20 schools, including 1 kindergarten, 17 primary schools and 2 middle schools.
Three hundred and thirty-five subjects (126 cases and 209 controls) had received VarV. The overall vaccination rate of VarV1 was 76.8% (335/436), and which was significantly higher in control group (95.9%, 209/218) than in case group (57.8%, 126/218) (χ2 = 88.77, P< .001). In addition, the overall vaccination rate of VarV2 was 27.1% (118/436), with which was 10.6% (23/218) in case group and 43.6% (95/218) in control group. The vaccination rate of VarV2 was also significantly higher in control group than in case group (χ2 = 60.23, P< .001). VE of VarV1 was 91.0% (95%CI: 81.6%-95.8%), and VE was 98.0% (95.5%-99.2%) for VarV2 ().
Table 1. VarV effectiveness by dose, Hangzhou, China
4. Discussion
Our results showed that the overall estimated incidence rate of varicella was high, especially for persons aged 10–19 years old and in suburb areas. The seasonal pattern was apparent, mostly due to the cases among students and children in kindergarten. Vaccination with the VarV produced a high level of protection against varicella, while VE of VarV2 was even better.
VZV is highly contagious. Although it is less readily transmitted than measles, with the routine use of measles vaccine, the incidences of measles in 2017 and 2018 in China were 0.43/100,000 and 0.28/100, 000,Citation13 respectively, much lower than the incidence of varicella. Nevertheless, as other vaccine-preventable diseases such as measles are controlled, varicella may represent a considerable preventable disease burden in the population, with significant health-care and societal costs. In the absence of universal VarV immunization, the burden of varicella would be substantial with a total of 5.5 million (95% CI: 4.7–6.4) varicella cases occurring annually across Europe.Citation14 In Taiwan, the implementation of a routine childhood VarV vaccination program which provided free VarV1 vaccination for all 1-year-old children had resulted in 87% decline in morbidity (881.49 to 115.17 per 100,000).Citation15 A major reduction is expected in the number of hospitalizations among children aged 3–4 years; public campaigns for the immunization of children younger than 4 years old with VarV2 lead to cost savings and are cost-effective because the vaccine price results in a benefit–cost ratio greater than 1.Citation16 In Hangzhou, with the high vaccination rate of VarV1, the morbidity was similar to Taiwan, and extremely higher than the average annual incidence in mainland China. The overall prevalence in Hangzhou was higher than the previously reported and the rates nationwide or in some other provinces during the same period,Citation17 which indicated that varicella is a growing and serious public health problem. A rising trend was also observed in the whole country and in other Chinese provinces.Citation17 Another possible reason is that in most provinces of China, varicella was not identified as a national notifiable disease, so the reported cases were much fewer than real cases.Citation2 Thus, varicella cases should be monitored effectively so as to access the epidemic trends and understand the epidemiological characteristics of varicella, and further provides the basis for the formulation of prevention and control strategies in the future.
The reasons for the incidence differences may relate to properties of VZV, climate models, geographical locations, population density and risk of exposureCitation18 and other potential factors.Citation19 Consistent with several previous studies, Citation1 the number of female cases is always lower than the number of male cases, which may be due to males participating in more activities, having much worse health habits, and having more opportunities to be infected. Several features in suburb areas maybe the reasons for the epidemic of varicella,Citation20 including poor awareness of vaccines or disease-related knowledge, more frequently population migration, accompanied by the low average economic income of families, which hinders the use of VarV, a voluntarily self-paid vaccine.Citation21 The onset of varicella shows a strong seasonality in temperate settings and in most tropical settings, with peak incidence during winter and spring,Citation22 which is approximately coincident with findings of studies in other areas,Citation17 and it is similar to most of the respiratory infectious diseases. In our study, we found two incidence peaks, the high peak during the winter months and another short peak from May to July. These were not only epidemiological characteristics of varicella but also due to the children congregate in schools and kindergartens. Children gather in schools and kindergartens undoubtedly increase the spread of VZV in these groups, which make them the main population for varicella. The seasonal trend for cases among non-student adults, preschool children and infants was not so apparent. Additionally, the majority of patients were teenagers aged 10–19 years old, consistent with results found in previous studies.Citation1,Citation17 Thus, education and health administrative departments should place the importance on improving the awareness of students, parents, and teachers around varicella and VarV vaccination, and strengthening the monitoring of epidemic situations in schools and kindergartens.
VarV is the most effective way to control the varicella epidemic and offer protection against varicella.Citation23 Sero-conversion, efficacy, and effectiveness measure different aspects of the ability of a vaccine to protect a child. VE is critical for the success of immunization programs. This study showed that VarV vaccination produced a high level of protection against varicella, VarV2 vaccination has a strong incremental VE and reduced risk of varicella infection, with VE of VarV1 was 91.0% and 98.0% for VarV2, which was consistent with some other scholars’ findings.Citation24,Citation25We found a much higher VE of VarV1 than most studies demonstrated that which was usually 70%-90% effective in preventing varicella.Citation26 Compared 1-dose VarV vaccination, some studies involving outbreak investigation have demonstrated that 2-dose VarV conferred better protection against varicella.Citation27 The VE of VarV2 estimate of 98% in our study was similar to 97% in the United States and 97% in Spain,Citation28,Citation29 similar to 94% reported from a case–control study in Spain,Citation30 but much higher than 84.6% of VarV2 VE observed in a population-based observational study.Citation31 One reason for this maybe that observational studies conducted during outbreaks, when infection pressure is high, tend to underestimate vaccine performance.Citation32 Eligible case–control studies were also considered to be reliable, having low selection bias, adjusted OR and moderate heterogeneity. Overall, our results provide strong evidence supporting a VarV2 vaccination schedule among healthy children. Several studies indicated that VarV2 are highly effective, and produce stronger protection than 1-dose.Citation33,Citation34 In addition, previous literatures have documented increased VE when vaccine coverage rate was higher.Citation35 The immunization coverage rate of at least 1-dose VarV and that of the second dose was higher in Hangzhou. This likely is the explanation for the higher incremental VE in our study. Due to the principle of voluntary choice and self-funded payments, and the neglected risk of varicella compared to other infectious diseases such as measles and mumps, the vaccination rate of VarV in many parts of China is relatively low and does not reach the 80% level that the WHO recommends.Citation7 In view of the current high prevalence of varicella, relevant health institutions should consider the inclusion of VarV in the national immunization program, and recommend VarV2 immunization schedules to better control the spread of varicella.
The strength of the present study was the use of CISDCP and HZIIS for data collection. All varicella cases diagnosed in a hospital in Hangzhou are reported to CISDCP. HZIIS is a modern surveillance system that maintains all immunization data, which were collected after the persons contacted an immunization clinic. Yet, this study has two limitations. Most of the diagnosis of varicella cases was made clinically by the characteristic rash. In vaccines who have breakthrough varicella, clinical diagnosis maybe more difficult because of mild rashes. Thus, the existing surveillance systems do not capture cases that do not seek medical care, and a few cases are affected by underreporting and under ascertainment. Another limitation is that we obtained only one-year-reported data, which was not sufficient to develop an understanding of the long-term epidemic characteristics and periodical trend changes. Therefore, with the development of disease surveillance, more data should be collected and analyzed in the future.
In conclusions, to better control varicella epidemic and reduce the burden of varicella, continuous monitoring and management of varicella cases is necessary, especially in those endemic areas, high-risk populations, and peak periods; a 2-dose VarV strategy is highly recommended, for 2-dose VarV vaccination provided superior protection than 1-dose VarV vaccination; and health authorities should widely disseminate disease knowledge among the people and consider the inclusion of VarV in the national immunization program to increase the 2-dose VarV inoculation rate and the overall immunity level.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Ethical considerations
This program was approved by the ethics committee of the HZCDC. Data were de-identified when extracted from HZIIS and CISDCP and were not linked to individual identifiers. All of the participants included in the case–control study were given a brief oral description of the aims of the present study, and verbal consent was obtained from the participants.
Acknowledgments
We wish to thank the staff at county-level Center for Disease Control and Prevention and in vaccination clinics in Hangzhou, for their disease surveillance, control, and vaccination service.
Additional information
Funding
References
- Siu HT, Li JC, Wang M,Liu YM, Yin DP. Varicella epidemiology in China, 2005-2015. Chin J Vaccines Immun. 2019;2:155–59.
- Yin D, Song L, Zhang X, Li FJ, Cao LS, Zhang SL, Fan CX, Zhang GM, Zhou YQ, Zheng JS, et al. The investigation on the incidence of varicella in Shandong, Gansu and Hunan provinces in 2007. Chin J Vaccines Immunization. 2009;15(2):119–22.
- World Health Organization. Varicella and herpes zoster vaccines: WHO position paper, June 2014-Recommendations. Vaccine. 2016;34(2):198–99. doi:10.1016/j.vaccine.2014.07.068.
- Hua Z, Han Z, Rong O, Zeng Q, Hu L, Qiu H, Sharma M, Ye M. Spatiotemporal epidemiology of varicella in Chongqing, China, 2014-2018. Int J Environ Res Public Health. 2020;17(2):662. doi:10.3390/ijerph17020662.
- Prevention of varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Centers for disease control and prevention. MMWR Recomm Rep. 1996 Jul 12;45(RR–11):1–36.
- Prevention of varicella: recommendations for use of varicella vaccines in children, including a recommendation for a routine. 2-dose varicella immunization schedule. Pediatrics. 2007 Jul;120(1):221–31. doi: 10.1542/peds.2007-1089
- Xu Y, Liu S, Che X, Liu Y, Zhang X, Du J, Zhang X, Wang J, Xu E. Seroepidemiology of varicella in Hangzhou, China in the vaccine era. Hum Vaccin Immunother. 2018;14(10):2464–71. doi:10.1080/21645515.2018.1477909.
- Varela FH, Pinto LA, Scotta MC. Global impact of varicella vaccination programs. Hum Vaccin Immunother. 2019;15(3):645–57. doi:10.1080/21645515.2018.1546525.
- Lopez AS, Zhang J, Marin M. Epidemiology of varicella during the 2-dose varicella vaccination program-United States, 2005-2014. Morb Mortal Wkly Rep. 2016;65(34):902–05. doi:10.15585/mmwr.mm6534a4.
- Marin M, Marti M, Kambhampati A, Jeram SM, Seward JF. Global varicella vaccine effectiveness: a meta-analysis. Pediatrics. 2016;137(3):e20153741–e20153741. doi:10.1542/peds.2015-3741.
- Liu Y, Xu E, Che X, Wang J, Gu WW, Xu YY, Du J, Zhang XP, Zhang XC. Coverage of two doses of varicella attenuated live vaccine in Hangzhou city of Zhejiang province. Chin J Vaccines Immunization. 2018;24(4):453–56.
- Suo L, Lu L, Wang Q, Yang F, Wang X, Pang X, Marin M, Wang C. Varicella outbreak in a highly-vaccinated school population in Beijing, China during the voluntary two-dose era. Vaccine. 2017;35(34):4368–73. doi:10.1016/j.vaccine.2017.06.065.
- Ma C, Su Q, Hao L. Epidemiology of measles in China, 2017-2018. Chin J Vaccines Immunization. 2020;26(1):5–8.
- Riera MM, Bollaerts K, Heininger U, Hens N, Gabutti G, Gil A, Nozad B, Mirinaviciute G, Flem E, Souverain A, et al. Estimation of the burden of varicella in Europe before the introduction of universal childhood immunization. BMC Infect Dis. 2017;17(1):353. doi:10.1186/s12879-017-2445-2.
- En TW, Ting AW, Yi HS. Change of epidemiological characteristics and disease burden of varicella due to implementation of mass immunization program in Taiwan from 2000 to 2012[C]. World Academy Sci Eng Tech Int J Med Health Sci. 2017;11(2). https://publications.waset.org/abstracts/56517/change-of-epidemiological-characteristics-and-disease-burden-of-varicella-due-to-implementation-of-mass-immunization-program-in-taiwan-from-2000-to-2012.
- Peña Blasco G, Blasco Pérez-Aramendía MJ. A cost-benefit analysis of varicella vaccination in Aragón. Arch Argent Pediatr. 2017;115(5):432–38. doi:10.5546/aap.2017.eng.432.
- ZJ L, Wang Y, Wang DM. Epidemiological characteristics of varicella in Guizhou, 2013-2017. Mod Prev Med. 2019;46:3101–03.
- Plotkin SA, Orenstein WA, Offit PA. Vaccines [M]. 7th ed. Philadelphia (PA): Elsevier; 2018. p. 1145–80.
- Sumi A. Role of temperature in reported chickenpox cases in northern European countries: denmark and Finland. BMC Res Notes. 2018;11(1):377. doi:10.1186/s13104-018-3497-0.
- Varicella. [accessed 2015 April 15]. https://www.who.int/immunization/diseases/varicella/en/4
- Hu Y, Chen Y, Wang Y. Knowledge, attitude and practice of pregnant women towards varicella and their children’s varicella vaccination: evidence from three districts in Zhejiang Province, China. Int J Env Res Public Health. 2017;14(10):pii: E1110.
- Backround paper on varicella vaccines- SAGE working group. [accessed 2014 April]. http://www.who.int/immunization/sage/meetings/2014/april/presentations_background_docs/en/
- Smith NTA, Saadia TA, Norowitz KB. Negative IgG varicella zoster virus antibody status: immune responses pre and post re-immunization. Infect Dis. 2018;7:175–81.
- Wang Y, Zhang L, Sun X. Effectiveness and failure rate of the varicella vaccine in an outbreak in Jiangsu, China: a 1:2 matched case-control study. Hum Vaccin Immunother. 2019;10(7):1–7. doi:10.1080/21645515.2019.1690331.
- Pan X, Shu M, Ma R, Fang T, Dong H, Sun Y, Xu G. Varicella breakthrough infection and effectiveness of 2-dose varicella vaccine in China. Vaccine. 2018;36(37):5665–70. doi:10.1016/j.vaccine.2018.05.025.
- Huang W-C, Huang L-M, Chang I-S, Tsai F-Y, Chang L-Y. Varicella breakthrough infection and vaccine effectiveness in Taiwan. Vaccine. 2011;29(15):2756–60. doi:10.1016/j.vaccine.2011.01.092.
- Thomas CA, Shwe T, Bixler D, Del Rosario M, Grytdal S, Wang C, Haddy LE, Bialek SR. Two-dose varicella vaccine effectiveness and rash severity in outbreaks of varicella among public school students. Pediatric Infect Dis J. 2014;33(11):1164–68. doi:10.1097/INF.0000000000000444.
- Shapiro ED, Vazquez M, Esposito D, Holabird N, Steinberg SP, Dziura J, LaRussa PS, Gershon AA. Effectiveness of 2 doses of varicella vaccine in children. J Infect Dis. 2011;203(3):312–15. doi:10.1093/infdis/jiq052.
- Perella D, Wang C, Civen R. Varicella vaccine effectiveness in preventing community transmission in the 2-dose era. Pediatrics. 2016;137(4):e20152802.
- Cenoz MG, Martinez AV, Guevara M, Ezpeleta C, Barricarte A, Castilla J. Effectiveness of one and two doses of varicella vaccine in preventing laboratory-confirmed cases in children in Navarre Spain. Hum Vaccin Immunother. 2013;9(5):1172–76. doi:10.4161/hv.23451.
- Siedler A, Rieck T, Tolksdorf K. Strong additional effect of a second varicella vaccine dose in children in Germany, 2009-2014. J Pediatr. 2016;173:202–206.e2. doi:10.1016/j.jpeds.2016.02.040.
- Yin M, Xu X, Liang Y, Ni J. Effectiveness, immunogenicity and safety of one vs. two-dose varicella vaccination: a meta-analysis. Expert Rev Vaccines. 2018;17(4):351–62. doi:10.1080/14760584.2018.1433999.
- Zhu S, Zeng F, Xia L. Incidence rate of breakthrough varicella observed in healthy children after 1 or 2 doses of varicella vaccine: results from a meta-analysis. Am J Infect Control. 2018;46(1):e1–e7. doi:10.1016/j.ajic.2017.07.029.
- Wutzler P, Bonanni P, Burgess M, Gershon A, Sáfadi MA, Casabona G. Varicella vaccination-The global experience. Expert Rev Vaccines. 2017;16(8):833–43. doi:10.1080/14760584.2017.1343669.
- Spackova M, Wiese PM, Dehnert M, Matysiak-Klose D, Heininger U, Siedler A. Comparative varicella vaccine effectiveness during outbreaks in daycare centres. Vaccine. 2010;28(3):686–91. doi:10.1016/j.vaccine.2009.10.086.